


Introduction
Mental health and psychosocial support (MHPSS) programmes are essential to humanitarian aid, including those focused on the psychological well-being and social functioning of children, adolescents and youth affected by conflict. This review systematically synthesizes the current literature to identify and evaluate the efficacy, design and implementation challenges of MHPSS interventions for young people in conflict and post-conflict settings. The supplementary materials for this review are available at: https://osf.io/9et73.
Children in conflicts
The global situation for humanitarian aid is increasingly defined by the severe impact of armed conflict on civilians, with children, adolescents and youth being particularly affected. According to UNICEF,Footnote 1 over 473 million children are living in conflict zones, representing nearly one in six children worldwide. Living in such areas is often severely damaging to individuals and communities. UNICEF’s executive director highlighted the year 2024 as one of the most challenging years on record due to the unprecedented number of children affected and the severe impact on their lives.Footnote 2
Children in conflict zones experience international law violations and violence directly and indirectly. They are confronted with loss of family members, friends and familiar support structures, as well as injuries and the loss of, or lack of access to, essential services such as health care and education. In addition, children in conflict areas are exposed to profound immediate and lasting trauma. The origins of such trauma and stress range from direct warfare exposure to the effects of challenges in caregiving associated with adults’ emotional distress. This often results in mental disorders such as post-traumatic stress disorder (PTSD) or more general post-traumatic stress symptoms (PTSS), as well as anxiety and depression.Footnote 3 For children who are internally displaced or forced to migrate, the trauma stemming from exposure to conflict-related violence is compounded by the loss of their home, parents and relatives, identity, and social networks – losses that are themselves significant sources of trauma directly linked to the conflict, and that often lead to a heightened risk of chronic stress and anxiety.Footnote 4 The omnipresent exposure to violence and loss can fundamentally alter a child’s cognitive, emotional and social development.Footnote 5
The Uppsala Conflict Data Program (UCDP) – which uses a different typology than international humanitarian law’s terminology when it comes to conflict classification – categorizes conflicts into three groups:Footnote 6 State-based armed conflict (both inter-State and intra-State), non-State armed conflict and one-sided violence. State-based armed conflict involves the use of armed forces by at least two parties, one of which is the government of a State. An inter-State conflict involves two or more States, and an intra-State conflict occurs between a State government and an organized, non-State opposition within the State’s territory. Non-State armed conflicts involve the use of armed force between two organized, non-State groups that is persistent and results in battle-related deaths (e.g., drug cartels). One-sided violence refers to the use of armed force by a State government or an organized non-State group against unarmed civilians, often targeting specific groups based on identity.Footnote 7 This article will refer to the UCDP’s classification, without this implying that the contexts referred to constitute armed conflicts to which international humanitarian law would be applicable.
The situation of children affected by conflict is a core humanitarian issue which may also amount to a serious violation of their fundamental children’s and human rights as established by international law, in particular but not limited to the United Nations Convention on the Rights of the Child (CRC).Footnote 8 Given that these laws are readily violated in conflicts, the question emerges: if conflict and harm is unavoidable, how can children be assisted in recovering from trauma and to prevent or mitigate (mental) health problems from arising?
The role of mental health and psychosocial support in conflicts
In response to the growing number of conflicts and humanitarian crises occurring around the world, MHPSS has emerged as a critical component that is relevant not only to acute humanitarian aid but also to the broader humanitarian–development–peace nexus, including development, peacebuilding and transitional justice efforts, as described by, for example, the German Federal Ministry for Economic Cooperation and Development.Footnote 9 The Inter-Agency Standing Committee (IASC) defines MHPSS as a layered system of care that promotes psychological well-being, reduces distress and prevents long-term mental health problems.Footnote 10 It integrates four levels of support: (1) basic services and security to meet essential needs, (2) community and family support, (3) non-specialized care by trained workers, and (4) specialized clinical services.Footnote 11 This multi-tiered approach combines community-led initiatives with formal health systems to strengthen resilience and recovery.
The base of the pyramid focuses on integrating mental health and psychosocial considerations into basic services and security. This includes ensuring that the provision of food, shelter, water and sanitation is carried out in a way that is dignified, culturally sensitive and safe. Tier 2 builds upon this foundation by strengthening existing community and family support; this involves community-led initiatives, activation of social networks, and support for positive coping mechanisms and communal healing practices. This is followed by the provision of focused, non-specialized support to individuals and families, often delivered by trained front-line workers who are not necessarily mental health specialists. Key interventions at this level include psychological first aid, stress management programmes, and structured psychosocial activities in settings like schools or other child-friendly spaces. Finally, the top of the pyramid consists of specialized clinical services for individuals with severe mental health conditions. This is a crucial, though less prevalent, level of care provided by qualified mental health professionals such as psychiatrists and psychologists. The IASC model stresses that these four tiers are not sequential steps but rather are complementary services that should be provided simultaneously to meet the diverse and dynamic needs of a population in crisis.
Aim and scope of review
While numerous studies have documented the devastating impacts of conflict on children’s lives and well-being, a significant evidence gap exists with regard to what MHPSS interventions work best in what specific context. Existing literature is often fragmented, with studies varying widely in methodology, context and focus. There is a particular lack of robust evidence on the effectiveness of non-specialized, community-based MHPSS interventions, which are the most widely implemented in humanitarian settings.
The primary aim of the present systematic mapping review is twofold: to synthesize the scientific literature on the documented impacts of conflict on the well-being of children, adolescents and youth, and to likewise synthesize the literature on state-of-the-art approaches to addressing these challenges. The review focuses specifically on studies examining MHPSS interventions targeting children, adolescents and youth affected by conflict. A core objective is to critically assess the methodological quality of the evidence beyond simply synthesizing findings; such comprehensive, up-to-date review is urgently needed to inform evidence-based, scalable MHPSS intervention practices and policies, strengthen MHPSS provision for children, adolescents and young people in ongoing conflicts, and inform further discussions, research and development of MHPSS responses benefiting children and young people in conflict zones.
Methodology
This systematic mapping review with narrative synthesis was conducted following the PRISMA 2020 guidelines.Footnote 12 Given the heterogeneity of populations, interventions, outcomes and study designs, a mapping approach was chosen to synthesize what types of interventions exist, how they have been studied and where gaps remain. In multiple phases, the relevant literature addressing MHPSS interventions for children, adolescents and youth affected by conflict was identified, screened and analyzed. The process of this systematic mapping review followed a “funnel” structure, beginning with broad searches in databases using key terms (see the supplementary materials) and progressively narrowing down the results based on set criteria to arrive at a collection of relevant studies. Figure 1 describes these steps in more detail.
PRISMA flow diagram.

Figure 1 Long description
The diagram shows the PRISMA flow process with three main sections: Identification, Screening and Included. Identification: - Records identified from various databases: Databases (n=13,624), PubMed (n=5,009), Scopus (n=450), Web of Science (n=7,385), PsychIndex (n=780). - Records removed before screening: Duplicates removed (n=5,281) and other reasons such as publication year (n=13). Screening: - Records screened (n=8,330). - Records excluded due to automated pre-screening (n=7,421). - Records assessed for eligibility (n=909). - Reports excluded for reasons such as not being a primary source (n=161), not involving IDPs or children in war-like conflict (n=84) and no in-country intervention (n=206). Included: - Articles included in review (n=56).
Prior to the identification of relevant articles, criteria were defined related to population, intervention focus, setting, language, and publication characteristics. The population of interest for this review comprised children, adolescents and youth, defined as individuals under 25, consistent with the United Nations (UN) definition of youth, which traces back to the International Youth Year in 1985.Footnote 13 This definition has been in use by the UN ever since, and current UN statistics are also based on it. While the target population was individuals under 25, two studies were retained where participants slightly exceeded this threshold (up to age 30) because the majority of the study sample fell within the defined age range. The population included specifically internally displaced people (IDPs) and individuals residing in conflict zones; however, parents, caretakers and other stakeholders who are in contact with children and young people in conflict zones were also included.
The intervention focus was narrowed down to MHPSS, including trauma-related interventions, social support, and community-based mental health programmes. The articles included in the review are peer-reviewed primary studies, published after 1990 and in English. Another inclusion criterion was that the studies reported on in-country interventions, meaning those delivered within the country where the conflict occurred or was ongoing. This also includes populations displaced to safer areas within the country, who continue to face the consequences of conflict exposure as well as additional displacement-related stressors. Both active conflict and post-conflict settings were considered. Exclusion criteria were interventions delivered outside the conflict-affected country or region (e.g., resettlement countries) and reviews or meta-analysis.
Four databases were searched: PubMed (n=5,009), Scopus (n=450), Web of Science (n=7,385) and PsychIndex (n=780). The searches were conducted using Boolean strings with similar key terms but specified for each database. The first string included the population, the second narrowed down the context, the next included MHPSS terms, and lastly the age was specified to receive relevant outcomes in the database. The search strategy combined four main concept blocks. The population block included terms such as “child”, “adolescent”, “young adult”, “refugee” and “internally displaced people”, while the context block covered exposures related to armed conflict, war, forced migration, violence, abduction, kidnapping, threat and resilience. The outcome block focused on MHPSS, mental health, psychosocial support, trauma, community-based interventions and social support, and finally, a youth filter was applied with terms such as “adolescent”, “young adult”, “youth”, “young people”, “under 25”, and “under 18”. As an example, the PubMed search string was: (child*[tiab] OR adolescent*[tiab] OR “young adult”[tiab] OR refugee*[tiab] OR “internally displaced people”[tiab] OR “internal displacement”[tiab]) AND (armed conflict[tiab] OR war[tiab] OR frontline[tiab] OR “forced migration”[tiab] OR abduction[tiab] OR kidnapping[tiab] OR threat[tiab] OR violence[tiab] OR resilience[tiab]) AND (MHPSS[tiab] OR “mental health”[tiab] OR “social support”[tiab] OR trauma[tiab] OR “community based intervention”[tiab]) AND (adolescent*[tiab] OR “young adult”[tiab] OR youth[tiab] OR “under 25”[tiab] OR “under 18”[tiab]). Strings were adapted for Scopus, Web of Science and PsychIndex. Full search strings for each database are provided in the supplementary materials.
The initial number of search results across all databases was 13,624. These were imported into Zotero reference management software, and its duplication detection feature was used to merge identical records. Afterwards, 8,343 articles remained. Thirteen records were excluded because they were published before 1990. The next step included an automated pre-screening based on a custom Python script, developed using Cursor (an AI-assisted coding environment), to perform keyword-based filtering of titles and abstracts. The script matched titles and abstracts against the same concept blocks used in the database searches (population, context, MHPSS and age terms) and flagged records that did not contain sufficient keyword overlap for exclusion. Importantly, this step served only as a pre-screening aid; all flagged exclusions and retained records were subsequently verified manually by the researchers. The script is accessible in the supplementary materials.
After the automated exclusion, 3,182 records were left. A manual screening of titles and abstracts was then conducted, and it narrowed down the results to 1,179. From these, 748 articles were selected for the full-text screening, which then further narrowed the number down to 264 eligible studies that aligned with our focus on children, adolescents and youth in conflict zones. Lastly, studies were assessed for alignment with the criterion of in-country implementation. This resulted in a final sample of fifty-six studies that met all inclusion requirements. Throughout the screening process, one author led the identification and extraction of studies, while all co-authors independently double-checked each study before final inclusion. Disagreements were resolved through consensus discussion. References of all included studies were also screened to identify additional relevant papers.
For data extraction, an Excel spreadsheet was developed to systematically extract key information from each study. Extracted data included population demographics, conflict type and setting, the type, duration and delivery method of the MHPSS intervention, study design and methods, mental health or psychosocial outcome measured, and key findings and limitations. Intervention duration was categorized as short (up to four weeks), medium (four to eight weeks) or long (more than eight weeks).
Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT, version 2018).Footnote 14 The fifty-six included studies comprised randomized controlled trials (n=16), non-randomized studies (n=7), quantitative descriptive studies (n=24), qualitative studies (n=8), and one mixed-methods study. All studies met both screening criteria (S1 and S2). Across the category-specific quality criteria (Q1–Q5), the majority of ratings were positive. Where criteria could not be fully verified based on the available reporting, most commonly with regard to representativeness of the sample (Q2) and the control of potential influencing variables (Q4), ratings of “can’t tell” were assigned. In these cases, the assessment gave the benefit of the doubt to the authors, assuming sound research practices where reporting was limited rather than absent. “No” ratings were rare and concentrated on Q4, reflecting the scarcity of blinding of outcome assessors, as well as limited long-term follow-up beyond six months. Detailed MMAT ratings for each study are provided in the supplementary materials.
Results
The following sections provide an overview of the findings from the fifty-six included studies, summarizing study characteristics, geographic and conflict contexts, intervention types, and measured outcomes. Results are organized to first provide an overview of included studies, followed by impacts on MHPSS, reported outcomes, and effectiveness. For an overview of all studies, see Table 1.
Structural overview of the incorporated studies

Table 1 Long description
The table lists incorporated studies and summarizes, for each study, the target group, age range, sample size, conflict setting and type, conflict duration, intervention type, delivery location, program duration, provider, timing relative to conflict onset, and whether delivered individually, in groups, or to families. Most studies focus on children, adolescents, or young adults, with ages spanning early childhood through young adulthood and occasional adult caregiver or provider samples. Sample sizes vary widely, from small pilots of about ten to several dozen participants to very large multi-country datasets in the tens of thousands. Many studies are set in protracted, internationalized intra-state conflicts, with repeated entries from Palestine and additional studies from Sierra Leone, Congo, Ukraine, Lebanon, Afghanistan, Kashmir, Uganda, Burundi, Colombia, Israel, and others; a few rows report not available values for setting or conflict details. Interventions most commonly include focused psychological support and skills-building, with additional approaches such as basic psychosocial support, family and caregiver support, capacity-building for providers, assessment or screening tools, psychological first aid, and creative or recreational activities. Delivery is frequently group-based and occurs in community and school settings, with some online programs, refugee camp settings, and family-based formats; providers range from lay health workers and paraprofessionals to mental health professionals, educators, community or NGO staff, and researchers. Timing is often during or after conflict exposure, with fewer interventions spanning before, during, and after.
Study context and demographics
The publication year of the included studies ranges from 2000 to 2024, with a peak between 2015 and 2022. Studies are geographically diverse, but with a focus on the global South (>80%); for an overview, see Figure 2. The geographic distribution concentrates in South Asia (n∼12, predominantly India) and the Middle East and North Africa region (n∼20, predominantly Palestine and Israel). Additionally, research was conducted in sub-Saharan Africa, including Sierra Leone, Uganda and the Democratic Republic of the Congo, as well as East and Southeast Europe (n∼5, Ukraine and Bosnia). Other countries chosen for research were Afghanistan, Colombia, South Africa, Indonesia and Brazil, along with some multi-country settings.
Distribution of conflicts by country. Left: global distribution. Right: zoomed in on most studied region.

Figure 2 Long description
A) The left map displays global distribution of conflict studies. Countries are shaded based on the number of studies: few studies (ongoing) are marked with light shading, few studies (ended) with medium shading, many studies (ongoing) with dark shading and many studies (ended) with very dark shading. The legend indicates the number of studies ranging from 1 to 10. Notable regions with many studies include parts of South Asia, the Middle East and sub-Saharan Africa. B) The right map zooms into the Middle East and North Africa, highlighting specific countries with similar shading categories. The legend remains consistent, showing the number of studies from 1 to 10. Countries like Palestine and Israel are prominently marked, indicating a high concentration of studies. The maps visually represent the focus and frequency of conflict-related research across different regions.
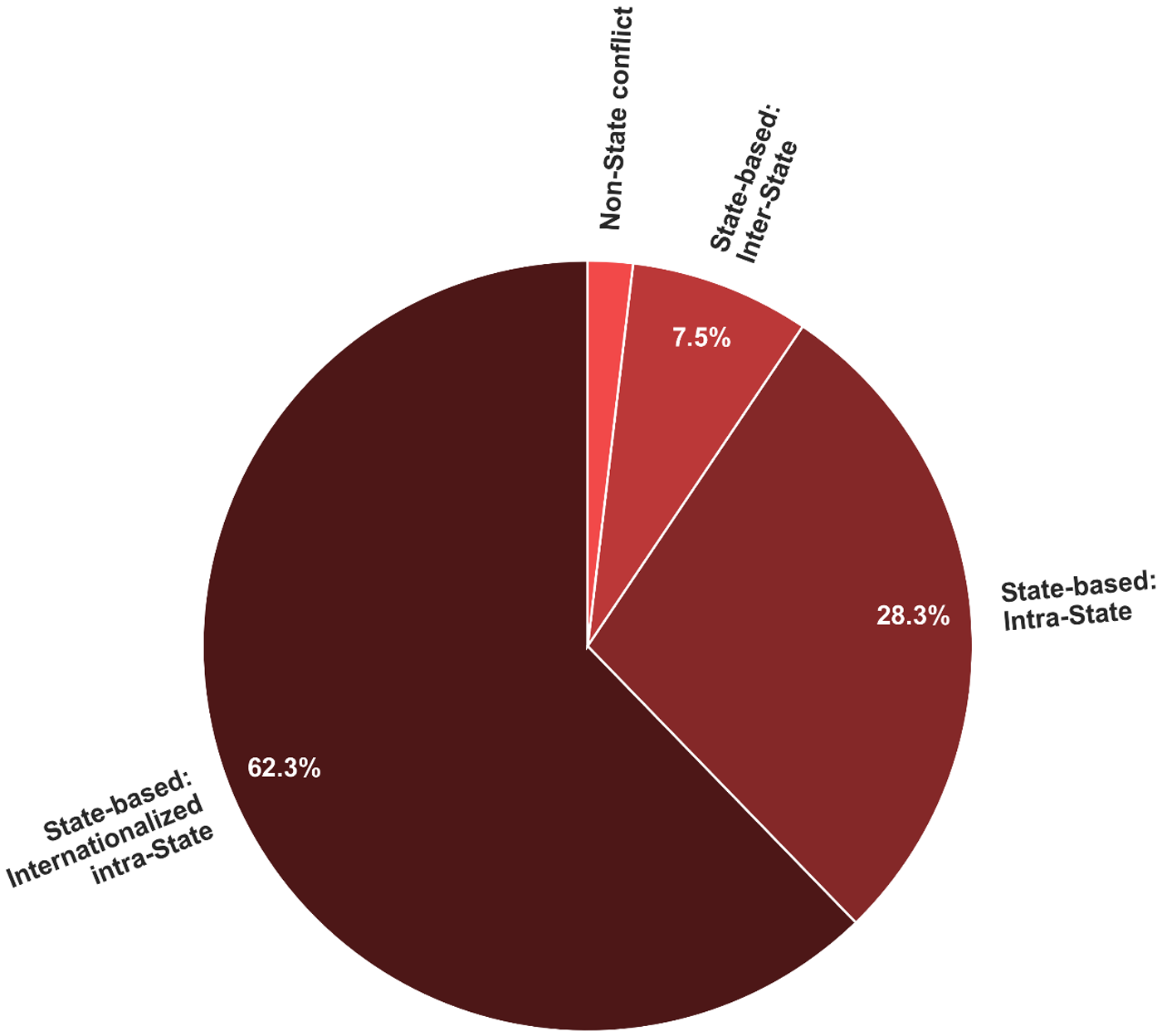
Across the studies included, most interventions are conducted in state-based conflicts as defined by the UCDP. As indicated above, the UCDP uses a typology which is different from international humanitarian law for the purposes of conflict classification and for determining whether that body of rules applies. Specifically, thirty-three studies took place in internationalized intra-State conflicts, fifteen in intra-State conflicts, and four in inter-State conflicts, as visualized by Figure 3. One study addresses non-State violence, and three do not specify the conflict type. In connection with this, (internal) forced displacement as well as host–refugee integration is a recurring topic in the included studies.
Types of conflicts covered by the included studies.

Figure 3 Long description
The pie chart contains four slices with text labels and percentage values. Slice labels and values: State-based: Internationalized intra-State, 62.3 percent. State-based: Intra-State, 28.3 percent. State-based: Inter-State, 7.5 percent. Non-State conflict, 1.9 percent.
The sample sizes (participants in interventions) are not normally distributed and range from ten to 29,292. The median is 190 participants. Eleven studies have fewer than fifty participants, fifteen studies have between fifty and 199 participants, and twenty-three studies include 200 or more participants. Larger samples are more common in school-based trials, while smaller are more prevalent in pilot psychosocial programmes. The age of intervention participants ranges from early childhood (2–7, n=3) to early adulthood (>20, n=13). Most studies focus on school-aged children and adolescents (6–18, n=36), and some include mixed-age groups spanning children, adolescents and adults, or are not specified (n=9). For an overview, see Figures 4, 5 and 6.
Age range spans by intervention type.

Figure 4 Long description
Horizontal bar graph with intervention types listed on the vertical axis and Age on the horizontal axis. Horizontal axis label: Age. Tick labels: 0, 10, 20, 30, 40, 50, 60, 70, 80. Vertical axis label: Intervention type. Bars and labeled age ranges: Capacity building for providers: 19 to 81. Family and caregiver support: 0 to 70. Community based care: 0 to 50. Basic psychosocial support: 0 to 50. Focused psychological support: 16 to 30. Skills building: 6 to 23. Social and emotional learning: 6 to 21. Toy assisted therapy: 7 to 11. Creative expression: 11 to 17. Psychological first aid: 6 to 15. Specialized clinical care: 7 to 18. Self help: 16 to 23. Part icipatory assessment slash research methods: 7 to 11. Assessment slash screening tools: 6 to 11. Recreational activities: 16 to 19. Protective factors education: 10 to 13.
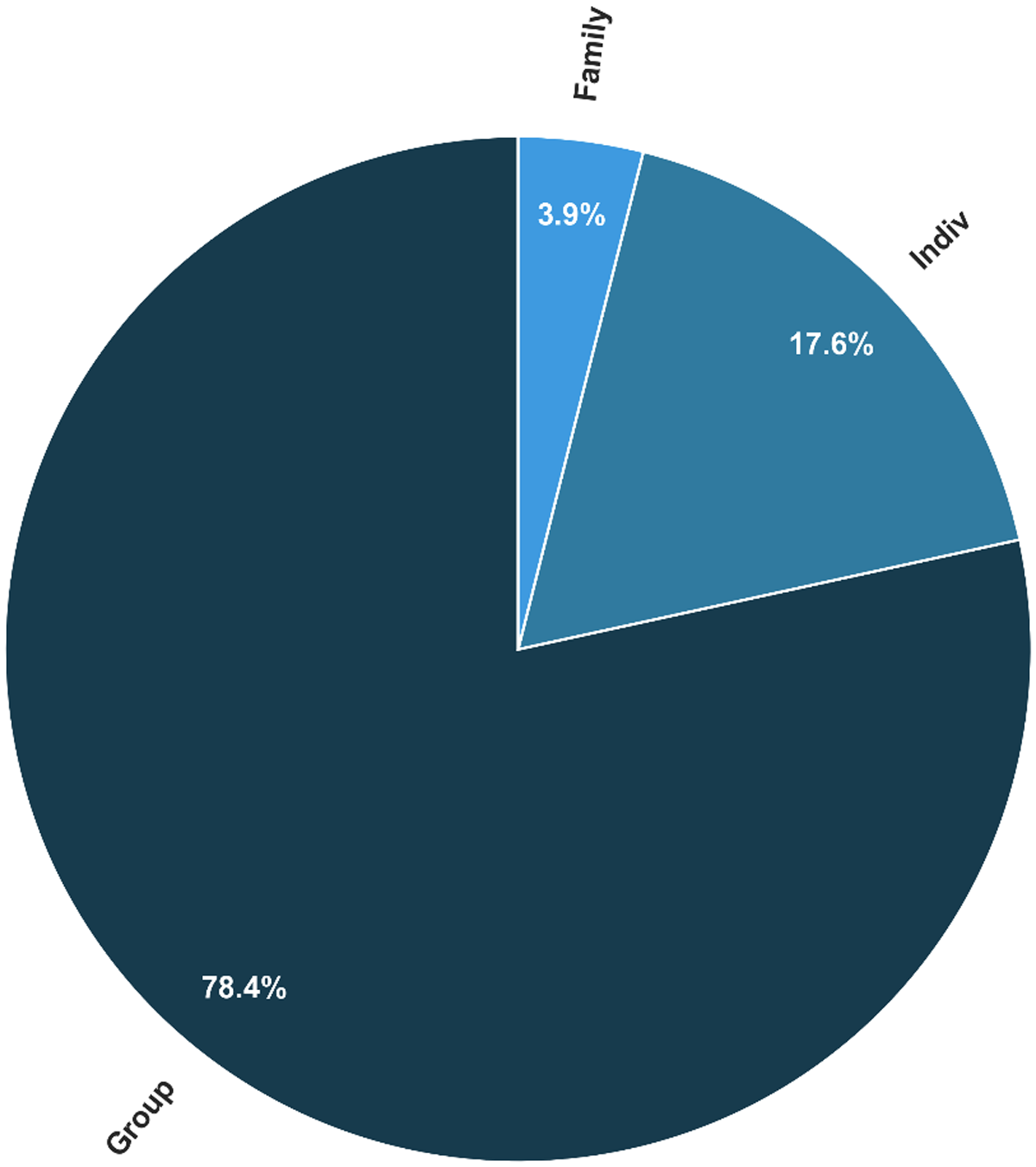
Individual versus group interventions.

Intervention locations; intervention timing relative to conflict; provider type versus location matrix.

Figure 6 Long description
The image contains two pie charts and a heatmap. The first pie chart represents intervention timing relative to conflict, with segments labeled as 'before' at 30.9 percent, 'during' at 45.6 percent and 'after' at 23.5 percent. The second pie chart shows intervention locations, with 'community' at 48.0 percent, 'government' at 5.9 percent, 'online' at 5.9 percent, 'refugee camps' at 3.9 percent and 'school' at 36.3 percent. The heatmap displays intervention provider types versus locations. Rows represent providers such as 'community and NGO', 'educational staff', 'lay health workers', 'mental health professionals', 'mixed', 'paraprofessionals', 'researchers and technical', 'supervisors and peers' and 'trained facilitators'. Columns represent locations including 'SOS children's village', 'community', 'family', 'government', 'group relations', 'online', 'refugee camps' and 'school'. The color intensity indicates the count, ranging from 0 to 8. Notable values include 'community and NGO' at 'community' with a count of 8 and 'lay health workers' at 'school' with a count of 3. The pie charts and heatmap together illustrate the distribution and timing of interventions across different locations and providers.
Key impacts on well-being and mental health
The impact of conflict on child, adolescent and youth well-being that is emphasized in the studies can be categorized into four key areas: physical health impacts, mental health impacts, social and relational impacts, and educational and developmental impacts. Only a few studies directly assess physical health; one study reports an injury during an intervention which had an impact on the physical health of a participant (ankle fracture during a bouldering (climbing) intervention). Mental health impacts are emphasized in the studies, and a high baseline prevalence of PTSS can be identified, as well as common comorbidities such as anxiety, depression, and somatic symptoms. Regarding the social and relational impacts, the review of the studies shows that a breakdown in peer, family and community networks can be identified, for example due to mistrust between groups in inter-group conflict zones. In addition, stigma and prejudice are mentioned in connection to studies in school environments and in the context of displacement. Lastly, studies with school-based approaches highlight that exposure to conflict is linked to concentration difficulties and reduced educational progression rates. These changes were identified through classroom engagement scores before and after the intervention.
Intervention type and design variety
The intervention types are characterized by a strong methodological variety. Forty-six unique intervention labels are used in the studies, and only Teaching Recovery Techniques (TRT) psychosocial intervention (n=4), the Youth Readiness Intervention (YRI) (n=3) and coping strategies (n=2) are recurring intervention types. Additionally, cultural tailoring is common in effective programmes. The programmes are either based on psychosocial (school-based, group therapy, arts, sport-based), clinical (trauma-focused cognitive behavioural therapy (TF-CBT), trauma recovery techniques, narrative therapy), family/community (parenting programmes, community resilience training), tech-based (app-based resilience, online support) or mixed-model interventions (combing education, mental health, and children’s, adolescents’ and youth’s environment). The approaches also vary greatly (thirty-five unique approaches), but they can be generalized into broader categories such as community (e.g., local professionals), children’s, adolescents’ and youth’s direct environment (e.g., teachers, family), and external professionals. In some studies, diverse agents deliver services and interventions to children, adolescents and youth, allowing a mix of local and external involvement through a clinical psychologist or researchers. This is primarily seen in the TRT interventions, the YRI or the JoyPop App. Nineteen studies also include trained local professionals and therefore appear repeatedly; nevertheless, delivery settings and facilitator training are highly heterogeneous. As with the intervention types, the study designs show variation, although a pattern can be identified as randomized controlled trials (n=15) are mostly applied in CBT and psychosocial trials, while qualitative approaches (n=6) are primarily used in community programmes.
Measured outcomes
The measured outcomes can be separated into psychological outcomes, social outcomes, behavioural outcomes and overall intervention effectiveness (i.e., whether the intervention achieved its intended objectives and produced measurable improvements, assessed from both a programme evaluation and psychological research perspective).
Twenty-nine studies target psychological outcomes, and while most programmes address PTSS, the follow-up sustainability is mixed, mentioning no significant improvement in the case of writing therapy but improved mood regulation with app-based tools. However, a reduction in PTSS, depression, anxiety and distress, along with improved emotion regulation, coping and resilience, is identified by studies mentioning psychological outcomes. Some 60–70% of studies record reduced rates of anxiety, with the most significant reductions being found in randomized controlled trials (effect sizes medium to large). Some interventions mention these successes in the short term but not at follow-up, and others only for specific symptoms, while still others show no significant change (e.g., depressive symptoms remain unchanged despite PTSS improvement). Effects were either measured during or immediately after the intervention; only nine studies measure effects after ≥6 months, and no study assesses effects one year after the intervention. Most studies are evaluated shortly after the end of the testing period. The studies evaluating psychological outcomes use a variety of validated measures, including CPSS,Footnote 15 UCLA PTSD RI,Footnote 16 SCARED,Footnote 17 Kessler K-6,Footnote 18 WEMWBS,Footnote 19 DERS,Footnote 20 WHODAS IIFootnote 21 and WHOQOL-100;Footnote 22 however, the same measure is rarely used for multiple studies and in some cases a scale is adjusted to fit the needs of the intervention participants or environment (e.g. shortened, culturally adapted, translated).
Thirteen studies address social outcomes that are mainly measured in community-driven interventions. These outcomes range from increased prosocial behaviour and improved peer/family relations to better communication, improved community cohesion and reduced prejudice. The implementation of community-led programmes has been demonstrated to have a positive impact on collective resilience, even in the context of ongoing conflict. Social outcomes are assessed at the individual, family and community levels. While psychological outcomes are primarily measured by standard clinical scales and context-adapted measures, studies use self-reports or reports from teachers or caregivers to assess social outcomes.
Seven studies measure outcomes regarding the intervention participants’ behaviour. Indicators for this were school attendance, aggression, violent involvement, and activity participation; however, the definition and scope of these terms differ, especially for violence and aggression. Some studies assess level of aggression as an individual behavioural tendency and use standardized self-report scales such as Strengths and Difficulties Questionnaires to measure anger expression and frequency of aggressive behaviour, thereby focusing on internal processes and aggressive acts such as hitting or shouting. Others emphasize more socially situated definitions, involving social conflict behaviours within the peer, school or community environment; examples of these behaviours may include domestic violence, bullying and interpersonal violence.
Table 2 provides an overview of the outcome domains assessed across the fifty-six studies. PTSS and trauma-related symptoms were the most frequently measured (n=30), followed by depression (n=17), social and prosocial functioning (n=17), and behavioural outcomes (n=11). Resilience and coping (n=11), family and parenting outcomes (n=10), and functional impairment (n=10) were moderately represented. Anxiety (n=9), general psychological distress (n=8), well-being and quality of life (n=7), and emotion regulation (n=6) were less commonly assessed. Ten studies relied exclusively on qualitative methods without standardized outcome measures.
Outcome domains assessed across the fifty-six included studies

Table 2 Long description
The table lists outcome domains reported across 56 included studies and the number of studies assessing each domain. PTSS and trauma outcomes are the most frequently assessed, appearing in 30 studies. Depression and social or prosocial functioning are next, each assessed in 17 studies. Behavioural outcomes and resilience or coping are each assessed in 11 studies, while family or parenting and functional impairment are each assessed in 10. Anxiety appears in 9 studies, general psychological distress in 8, well-being or quality of life in 7, and emotion regulation in 6. Ten studies are categorized as qualitative only, meaning they did not use standardized measures.
Overall effectiveness
The effectiveness of interventions can be divided into four categories. Studies were classified as “positive” when the authors reported that the intervention had a beneficial effect on their assessed outcome variables; “mixed” when improvements were observed on some outcomes but not others, or when effects were not sustained at follow-up; “null/negative” when no measurable benefits were found or adverse effects were reported; and “not reported” when outcome information was insufficient to determine effectiveness. This qualitative approach was adopted because the heterogeneity of study designs, outcome variables and assessment methods precluded a meaningful quantitative comparison. Across the fifty-six studies, twenty-five report positive effects on children’s, adolescents’ and youth’s symptoms and/or functioning. Eleven studies show mixed effects, with improvements on some outcomes while others are unchanged or not sustained at follow-up. Two studies report null or negative findings, meaning that they either failed to show measurable benefits or produced (short-term) setbacks for participants. One of these studies, for example, documented no psychological gain and noted a temporary increase in depression symptoms right after a session. It is important to note that temporary increases in distress can be a recognized occurrence during therapeutic interventions, particularly those involving trauma-related content, and do not necessarily indicate harm. In eighteen studies, outcome information is not reported or cannot be determined from the available data.
To summarize the findings, the studies cluster around internationalized intra-State conflicts (n=33) and school-age samples (n=36), with primarily moderate to high numbers of participants. Methodological heterogeneity is evident, with forty-six intervention labels. Psychological symptoms dominate measurement (n=29) while social outcomes, behaviour and well-being are comparatively under-measured.
Discussion
Across diverse conflict settings, MHPSS interventions for children, adolescents and youth are most promising when delivered as part of multilayered systems that integrate universal school/community activities, targeted group programmes, and indicated counselling with referral pathways. Consistent but typically modest improvements are observed in PTSS, emotion regulation, functioning, and peer relations, with effects often attenuating over time without reinforcement. Programmes adapted to local context and delivered by trained teachers, lay workers or non-governmental organization (NGO) staff are feasible and scalable in low-resource and protracted-conflict environments. Evidence demonstrates that lay health workers can be effectively trained in less than four months, with interventions successfully reaching large populations with low dropout rates. In addition, cultural adaptation processes involving community members result in high acceptability and effectiveness even in protracted conflicts.Footnote 23
What works for children, adolescents and youth in conflict settings
Effective MHPSS interventions for children, adolescents and youth in conflict-affected settings share several core characteristics.
Based on the reviewed literature, a promising and scalable framework is a multilayered, stepped-care model that provides a continuum of support.Footnote 24 Such a model typically begins with community or school-based psycho-education; this is followed by more targeted group interventions and care, with the option of more intensive services for those with greater needs.
Group programmes delivered in school or community settings are particularly effective, yielding short-term benefits in reducing PTSS and improving social functioning and resilience.Footnote 25 Task-sharing, which involves trained teachers and lay workers delivering interventions under supervision, is a critical component of this success. This approach makes care feasible and effective in low- and middle-income countries and fragile contexts.Footnote 26
Furthermore, the inclusion of family and caregiver components significantly amplifies the impact of these interventions. Supporting caregiver well-being and parenting skills can reduce family violence and likely help sustain improvements over time.Footnote 27 Alongside core skills training, adjunctive approaches such as structured physical activity, arts, or narrative therapy can enhance engagement and promote well-being;Footnote 28 digital and hybrid support have also demonstrated their feasibility and have the potential to improve emotion regulation and access to care, as long as they are implemented with strong safeguarding and inclusion measures.Footnote 29 Relating these findings to the IASC multilayered model of care, structured physical activity, arts-based activities and psycho-education correspond to Tiers 1–2 (basic services and community support), group-based programmes such as TRT and classroom coping skills align with Tier 3 (focused non-specialized support), and evidence-based therapies such as TF-CBT and the YRI represent Tier 4 (specialized clinical services). Distinguishing between these levels is important, as the evidence base, required training and specific needs of the target populations differ across tiers.
Age-, culture- and trauma-informed fit
Successful interventions in conflict settings are not “one-size-fits-all”. According to the literature, effectiveness is dependent on tailoring programmes to be age-appropriate, culturally sensitive and trauma-informed.
For children in the early stages of development, interventions are most effective when they focus on dyadic play, attachment, and symbolic tools. These approaches reduce stress, strengthen the bond between caregivers and children, and provide a foundation for emotional resilience in conflict settings.Footnote 30 For older children, classroom-based coping skills and prosocial routines have shown to be both implementable and effective. Programmes such as Cognitive Behavioural Intervention for Trauma in Schools have been shown to reduce PTSS and improve social skills in the short term, and are therefore a crucial intervention with regard to MHPSS.Footnote 31 Programmes for adolescents and young adults also need to be tailored to their age, and the review has shown that for these age groups, more structured, evidence-based therapies like CBT, TF-CBT and the YRI are effective. These interventions reduce PTSS and improve emotion regulation and overall functioning.Footnote 32 The studies reviewed indicate that CBT interventions use systematic sessions to help young people identify and change harmful emotional responses, behaviours and thought patterns while teaching them practical coping strategies for daily challenges.Footnote 33 TF-CBT builds on these approaches by addressing trauma specifically through educational components that help youth understand trauma reactions;Footnote 34 it establishes safe environments where participants can build confidence and uses group formats that allow youth to learn from their peers as they practice new problem-solving and coping skills together.Footnote 35 The YRI is delivered in group settings, typically consisting of 10–12 sessions, and integrates family and community involvement.Footnote 36 Studies show that the YRI helps youth develop better emotional regulation abilities, improve their relationships with others and gain the skills needed for participation in school and work.Footnote 37 To maintain these benefits long-term, however, booster sessions are often necessary since the positive effects decrease after a short period of time (e.g., six months for YRI outcomes).Footnote 38
At the core of effective interventions are trauma-informed principles. These principles include creating a sense of safety, establishing stability and taking a phased approach to skill-building that minimizes the risk of re-traumatization. Protocols such as TF-CBT are based on these principles to ensure that they are effective and safe for participants.Footnote 39
Along with age, interventions should be tailored to new contexts because structuring them for specific settings improves their acceptability and effectiveness. Cultural norms can influence the success of an intervention, as demonstrated by a study in which acceptance and commitment therapy is shown to be more effective than TF-CBT for a group of Afghan girls.Footnote 40 This suggests that interventions must align with local values and practices.Footnote 41
Contextual influences and heterogeneity
Beyond individual factors, effects were shaped in similar ways by setting, timing, delivery platform and family systems. In the Middle East, school-based group interventions are common, but the timing of these interventions is sensitive: immediate post-escalation delivery sometimes produces null or transiently adverse outcomes. Research by Karam et al. Footnote 42 in Lebanon emphasizes that an immediate, daily, classroom-based intervention had no significant long-term effect, and had adverse effects on some participants; similarly, the TRT delivered immediately after the 2008 Israel–Hamas war showed only modest overall effectiveness and was associated with a temporary increase in psychological distress.Footnote 43 In contrast, interventions delivered with a delay of a few months, such as a later TRT delivery, showed more positive outcomes.Footnote 44 This suggests that practitioners should exercise caution with regard to immediate intensive trauma-processing interventions and instead focus first on stabilization and safety, allowing children’s natural coping mechanisms to stabilize before structured emotional processing is introduced. Importantly, this does not preclude early trauma-informed or skills-based interventions, which can be safely delivered alongside stabilization efforts.Footnote 45
In sub-Saharan Africa, trials emphasized task-sharing and functional outcomes. TF-CBT reduces PTSS and psychosocial distress among adolescents in the Democratic Republic of the Congo, and the YRI shows educational and functional gains, though durability varies.Footnote 46 In South Asia, lay health worker models are feasible and effective in protracted conflicts. The fit of the modality matters, underscoring the importance of cultural and gender-sensitive therapeutic approaches.Footnote 47 In Ukraine, studies demonstrate the feasibility of caregiver and youth groups, which improve caregiver mental health and reduce family violence. This indicates the importance of family-level mechanisms when the threat is sustained.Footnote 48 Several studies report stronger benefits for girls and younger cohorts at the individual level, which is consistent with the need for age- and gender-tailored interventions.Footnote 49
Disability status alters exposure patterns, but not PTSS prevalence. For example, adolescents with sensory impairments in Lebanon have lower sensory exposure to trauma but similar PTSS rates to those without such impairments, pointing to the importance of inclusive access and support.Footnote 50
Family and community systems are found to consistently moderate outcomes. Close and supportive relationships with caregivers are associated with lower PTSS and better functioning, while caregiver and parenting programmes have been shown to enhance and sustain improvements in children.Footnote 51 School and peer contexts are also influential: teacher-delivered programmes can reduce symptoms, though attitudinal outcomes may be vulnerable to social desirability, which underscores the importance of multi-informant measurement.Footnote 52 Finally, heterogeneity in conflict intensity, displacement, and family functioning contribute to preventive or treatment effects. This implies that delivery should be more tailored (e.g., stepped care or reassignment for non-responders) in routine practice.Footnote 53 Notably, while roughly a third of studies described referral pathways for participants requiring more intensive support, systematic adverse event monitoring was rarely reported. Where safeguards were mentioned, they typically involved supervision of facilitators and protocols for referring participants with severe symptoms. This underscores the need for standardized safeguarding and adverse event reporting in future MHPSS research in conflict settings.
Implications for practice and research
The findings provide significant implications for future mental health programmes for children, adolescents, and youth in conflict settings. They involve multilayered, adaptable approaches that emphasize accessibility, cultural relevance and long-term sustainability. Based on the review of the study sample, the following recommendations have been identified:
1. Programmes and interventions should consider a stepped-care model that links psycho-education at community or school level with more targeted, evidence-based interventions for those in need. These interventions, such as TF-CBT, should be delivered by task-sharing with trained non-specialists, like teachers, NGO staff and lay health workers, who are supervised by specialists. This approach expands the reach of care significantly and creates a ripple effect.
2. Interventions must be tailored to the specific needs of different age groups – for example, they should use play-based and dyadic caregiver–child work for early childhood, focus on classroom and prosocial routines for older children, and apply CBT for adolescents and young adults. Programmes should also culturally adapt their content, adjusting language, focus and pacing, and should incorporate the close environment of the child, such as by improving family well-being and reducing children’s exposure to domestic violence and dysfunction.
3. Practitioners should thoughtfully integrate safe and culturally appropriate practices and adjustments into their programmes to enhance reach and effectiveness. This can include incorporating physical activities, such as bouldering interventions or art-based therapies, as supplementary interventions. Furthermore, secure digital platforms can be utilized to extend services, for example by offering remote support; it should be noted, however, that access to digital services is inconsistent between conflict regions, limiting comprehensive application. Additionally, it is non-negotiable that any use of technology must be paired with robust data privacy safeguards to protect sensitive information and build trust within the community.
Although the existing research has made valuable contributions in high-pressure environments, the quality of the evidence base is constrained by important methodological considerations that influence the certainty and generalizability of its findings. Specifically, the evidence base would be strengthened by more long-term follow-up, as current studies often lack the data required to assess the durability of effects and the need for future booster strategies. Furthermore, studies would benefit from more consistent reporting of essential implementation data (e.g., training, supervision, fidelity) to facilitate confident scale-up. The reliability of findings is also influenced by the possibility of allegiance and expectancy bias introduced when researchers are involved in both the delivery and evaluation of an intervention; this is a common challenge inherent to resource-constrained settings. Finally, increased attention to standardized adverse event reporting is needed to fully evaluate the safety profile of these programmes and ensure that ethical standards are consistently met.
Future research should prioritize longitudinal follow-up to assess the durability and effectiveness of treatments and interventions, especially in settings with ongoing or re-escalating conflict, with follow-up periods of 12–24 months. To optimize intervention design, studies should move beyond simple efficacy comparisons and instead use, for example, factorial or SMART (Sequential, Multiple Assignment, Randomized Trial) designs. Through this, multilayered MHPSS interventions can be optimized and used for diverse children, adolescents and youth in dynamic conflict settings, since factorial designs tell us which inputs and combinations matter, and SMART designs tell us how to adapt over time, and for whom.
Research–practice gap
In MHPSS, the rapid and dynamic nature of real-world service delivery differs greatly from the pace of scientific research, resulting in a notable gap between what front-line workers do and the scientific evidence. This disconnect is amplified by the volatility and dynamics of conflict, which create significant challenges for research implementation, often forcing front-line helpers to adjust programmes rapidly in response to immediate security situations, population displacement, and constantly evolving needs.
Although multilayered MHPSS programmes are being implemented on a large scale across communities and schools, with reported uptake and perceived benefits, the supporting evidence does not meet scientific standards. Studies with control groups and long-term outcome data are rarely available.Footnote 54 This operational reality makes it necessary to fundamentally shift toward greater collaboration between researchers and fieldworkers – particularly civil society and humanitarian actors that are often at the forefront of providing MHPSS to children, adolescents and youth in conflict settings.
In addition to the previously mentioned limitations of scientific practices, many frequently used approaches are evaluated using pragmatic pre-post designs without control groups. Although this methodology reflects the ethical considerations and operational difficulties inherent in conflict settings, it ultimately restricts the strength of causal inference.Footnote 55 In addition, while task-sharing models (using non-specialists to give care) are practical and effective in real-world settings, the research studies rarely mentioned the necessary quality checks; these include independent checks of results, fidelity checks, and analysis of who benefits most (moderator analyses). It is essential to include these quality checks when managing programme quality and tailoring delivery to scale up the programme.Footnote 56 Furthermore, front-line staff typically prioritize outcomes related to functional well-being, school participation, and safety, while in contrast, much research relies on self-report symptom scales, which often have limited cross-cultural validation and incorporate few multi-informant or functional endpoints.Footnote 57 This means that studies often overlook objective feedback from parents and teachers, failing to measure real-life improvements in daily behaviour and social engagement. Lastly, essential economic evidence necessary for informing policy and scaling up remains scarce, with few exceptions.Footnote 58 In addition, the observation that frequent, unplanned adjustments to programme timing and maintenance (often due to factors such as fluctuating funding or sudden security crises) co-occur with a fading of positive effects at follow-up highlights a crucial knowledge gap. Rather than accepting this decline, researchers and practitioners should collaborate to experimentally evaluate planned sustainability strategies, such as scheduled booster sessions, in order to identify the most effective and scalable methods for sustaining long-term programme benefits in conflict settings.Footnote 59
In order to close the gap between implementation and evidence, there must be urgent collaboration between MHPSS providers and scientists in conflict areas, most often civil society and humanitarian organizations. Due to instability and rapid changes in conflict settings, future efforts must move away from inflexible, traditional research designs. Prioritizing hybrid effectiveness–implementation studies, which evaluate a programme’s impact and the real-world factors affecting its delivery simultaneously, is essential. This means incorporating independent assessments, practical functional outcomes, clear documentation of adaptations, cost reporting, and robust designs that specifically assess timing and maintenance within the fluid operational realities of large-scale service delivery. This approach ensures that research informs practice at the speed required by humanitarian work and vice versa.
Limitations
This review’s findings are subject to several limitations. The review is based exclusively on English-language studies, which means it likely omits relevant research published in other languages, especially of the studied locations.
The heterogeneity of interventions, comparators and outcomes across the included studies restricted the ability to make direct and solid comparisons. Additionally, incomplete reporting on, for example, adaptations and adverse events limited the capacity to draw definitive conclusions about the implementation of these interventions. Furthermore, several included studies originate from the same conflict contexts and, in some cases, from overlapping research programmes (e.g., Betancourt, McBain, and Newnham in Sierra Leone, and Diab and Qouta in Palestine). While these studies examine different outcome variables and measures, their shared samples and settings mean that certain conflicts and populations are disproportionately represented in the evidence base while others remain under-explored. This uneven coverage should be considered when interpreting the breadth of the findings, and future research should aim to address these gaps by expanding investigations across a wider range of conflict settings.
Conclusion
This systematic mapping review shows that children and adolescents exposed to conflict experience severe and complex disruptions to their psychological, social and developmental well-being. The evidence strongly supports the short-term effectiveness of multilayered MHPSS systems that integrate universal and community- and school-based activities with more targeted therapeutic and clinical services. Interventions implemented through task-sharing, in which trained teachers, lay workers and NGO staff deliver structured psychosocial care under specialist supervision, have been shown to be feasible and scalable in contexts of ongoing conflict and limited resources. Family and caregiver engagement consistently enhances and sustains the benefits of interventions, emphasizing the central role of the child’s immediate environment in recovery and increased resilience.
The review further emphasizes that meaningful engagement and effectiveness require culturally adapted, age-appropriate and trauma-informed approaches. Dyadic and play-based interventions promote secure attachment and emotional regulation for younger children, while structured, evidence-based therapies such as TF-CBT and the YRI are most beneficial for adolescents and young adults.
Despite frequently evidenced moderate to large short-term improvements in symptoms of post-traumatic stress, anxiety, and emotional functioning, few studies have assessed outcomes beyond six months, and evidence of sustained long-term benefits is limited. The ability to draw definitive conclusions about overall programme effectiveness is restricted by methodological heterogeneity, inconsistent outcome reporting and the scarcity of follow-up data. Furthermore, there is a significant gap between scientific research and field implementation. Real-world MHPSS programmes evolve rapidly in response to shifting conflict dynamics and children’s, adolescents’ and youth’s needs, and academic research lags behind in evaluating these adaptive practices. The current literature primarily reflects interventions such as CBT and the YRI, but in the field there has been a growing interest in body-oriented methods (e.g., yoga-based approaches), which show preliminary promise.Footnote 60 This trend is currently under-represented in the systematic evidence base, and closing this divide will require hybrid effectiveness–implementation studies that assess intervention impact and contextual delivery factors simultaneously. These studies must be supported by transparent reporting on fidelity, cost and sustainability.
Ultimately, the findings affirm that protecting the mental health of children, adolescents and youth in conflict settings demands coordinated, scalable and contextually grounded approaches that combine psychosocial care with education, family support and community resilience-building. Strengthening collaboration among civil society and humanitarian actors, researchers and policy-makers can help MHPSS transition to an evidence-based and ethically responsible framework that mitigates the long-term psychological impact of conflict on future generations.







 Open access
Open access