


Introduction
Suicide represents a significant public health challenge in Europe, marked by profound and persistent variations. The continent has the world’s second highest age-standardized male suicide mortality rate (17.1 per 100,000 population in 2019) (WHO, 2021), with Eastern Europe bearing the heaviest burden globally (35.9 per 100,000 population) (GBD 2021 Suicide Collaborators, 2025). To achieve international targets for reducing suicide mortality (WHO, 2013; UN, 2015), effective prevention requires strategies tailored to local contexts (Ilic and Ilic, Reference Ilic and Ilic2022), which hinges on a precise understanding of how suicide risk evolves in the long term.
A nuanced understanding of long-term suicide trends requires disentangling three interwoven temporal dimensions: age, period and cohort (APC) effects. An age effect captures suicide risk variation intrinsic to specific life stages (e.g., adolescence, late adulthood), reflecting biological maturation or socially structured transitions. Period effects reflect historical events or policies, such as economic crises or legislative changes that simultaneously impact all age groups. In contrast, a cohort effect represents the enduring influence of formative exposures (e.g., social, economic or technological shifts) shared by a generation, which can shape its lifetime risk trajectory (Hobcraft et al., Reference Hobcraft, Menken and Preston1982). International work, including studies from Australia and the United States, demonstrated that young generations can experience heightened risk for suicide (Spittal et al., Reference Spittal, Mitchell, Clapperton, Laughlin, Sinyor and Page2024; Hou et al., Reference Hou, Li, Liu and Caine2025). In Europe, the post-war ‘baby boomer’ cohorts have displayed increased suicide ideation relative to preceding generations (Cabello et al., Reference Cabello, Rico-Uribe, Martinez-Ávila, Sánchez-Niubò, Caballero, Borges, Mellor-Marsá, Haro, Prina, Koskinen and Ayuso-Mateos2021). Failure to account for cohort effects may, thus, leave key vulnerabilities unaddressed.
However, comprehensive and updated APC analyses across Europe’s diverse subregions are scarce. Most existing studies are largely limited to individual countries, such as the UK (Surtees and Duffy, Reference Surtees and Duffy1989) and Switzerland (Ajdacic–Gross et al., Reference Ajdacic–Gross, Bopp, Gostynski, Lauber, Gutzwiller and Rössler2006), and even these analyses are largely outdated, typically relying on data prior to 2010. Consequently, there is a significant gap in our understanding of contemporary generational shifts in suicide risk within the European context. An updated, subregionally stratified APC analysis is crucial both to uncover latent cohort-driven trends masked by aggregate rates and to inform the contextually relevant prevention strategies across Europe.
Our aim, therefore, was to investigate the role of APC effects on long-term suicide rates across European subregions, using nationally representative data from countries with complete mortality registration for the period 1990–2019.
Methods
Data source
Suicide mortality data (1990–2019) were extracted from the WHO Mortality Database (accessed on 25 February 2025), in which the causes of death were coded by the International Classification of Diseases (ICD), 8th, 9th and 10th Revisions (WHO, 2025). In this study, we identified suicide deaths by codes E950-959 in ICD-8 and ICD-9, and X60-X84, Y87.0 in ICD-10. Notably, only data coded by ICD-10 provide information on suicide means. Corresponding historical population estimates were obtained from United Nations’ World Population Prospects2024 to estimate suicide mortality rates (UN, 2024). We applied gender- and age-specific suicide mortality data for individuals aged 15–84 years. Ages under 15 years were omitted due to the low suicide rate, with the total number of suicides accounting for less than 1% of all suicide deaths between 1990 and 2019. Ages 85+ years were omitted due to the aggregation of older age groups in the source data which precluded precise cohort classification. Although more recent records are available for certain countries, the observation window was restricted to 1990–2019 to maximize cross-national comparability. Analyses were restricted to countries with complete gender- and age-specific suicide mortality data throughout the study period (annual data availability is summarized in Figure S1).
Statistical analysis
Sex, calendar year, matrices of certified deaths and estimated population sizes were utilized to calculate age-specific suicide rates in 5-year age intervals (e.g., 15–19 years), expressed per 100,000 population. We merged the suicide data and population estimates of corresponding countries under the classification of the United Nations Geoscheme to calculate subregional suicide mortality rates of Western, Eastern, Northern and Southern Europe (the list of included countries is provided in Table S1) (UN, 2021). Annual age-standardized suicide mortality rates (ASMRs) between 1990 and 2019 were calculated by the direct standardization method, with the World Health Organization standard population used as the reference (Ahmad et al., Reference Ahmad, Boschi-Pinto, Lopez, Murray, Lozano and Inoue2001). Both standardization and the computation of 95% confidence intervals were performed using the R package epitools (Aragon et al., Reference Aragon, Fay, Wollschlaeger, Omidpanah and Omidpanah2017). For countries providing detailed ICD-10 cause-of-death data between 2010 and 2019, we summarized the gender-specific distribution of suicide means at both national and subregional levels (details of suicide means classification were shown in Table S2).
The APC analysis was conducted using the APC Web Tool (Rosenberg et al., Reference Rosenberg, Check and Anderson2014). The tool fits a log-linear Poisson regression model, where the logarithm of the mortality rate is modelled as an additive function of APC effects:
 \begin{equation*}{\rho _{ca}} = \mu + \left( {{\alpha _L} + {\pi _L}} \right)\left( {a - \bar a} \right) + {\tilde \alpha _a} + \left( {{\pi _L} + {\gamma _L}} \right)\left( {c - \bar c} \right) + {\tilde \pi _{c + a - A}} + {\tilde \gamma _c}\end{equation*}
\begin{equation*}{\rho _{ca}} = \mu + \left( {{\alpha _L} + {\pi _L}} \right)\left( {a - \bar a} \right) + {\tilde \alpha _a} + \left( {{\pi _L} + {\gamma _L}} \right)\left( {c - \bar c} \right) + {\tilde \pi _{c + a - A}} + {\tilde \gamma _c}\end{equation*} In this formulation, μ represents the intercept (the fitted log rate at the reference age and cohort);  ${\alpha _L}$,
${\alpha _L}$,  ${\pi _L}$ and
${\pi _L}$ and  ${\gamma _L}$ denote the linear slopes (drifts) associated with APC, respectively;
${\gamma _L}$ denote the linear slopes (drifts) associated with APC, respectively;  ${\tilde \alpha _a}$,
${\tilde \alpha _a}$,  ${\tilde \pi _{c + a - A}}$ and
${\tilde \pi _{c + a - A}}$ and  $\tilde \gamma $ represent the nonlinear deviations for age group a, period c + a − A and cohort c; and
$\tilde \gamma $ represent the nonlinear deviations for age group a, period c + a − A and cohort c; and  $\bar a$ and
$\bar a$ and  $\bar c$ are the reference age and cohort, typically set to the centroids of the observed data. To address the exact linear dependency between APC, the software constrains cohort deviations to be orthogonal to the linear trend (Rosenberg et al., Reference Rosenberg, Check and Anderson2014). The longitudinal age curve, which describes the age-specific trend for a reference birth cohort adjusted for period effects, is given by the estimating function
$\bar c$ are the reference age and cohort, typically set to the centroids of the observed data. To address the exact linear dependency between APC, the software constrains cohort deviations to be orthogonal to the linear trend (Rosenberg et al., Reference Rosenberg, Check and Anderson2014). The longitudinal age curve, which describes the age-specific trend for a reference birth cohort adjusted for period effects, is given by the estimating function  $\mu + \left( {{\alpha _L} + {\pi _L}} \right)\left( {a - \bar a} \right) + {\tilde \alpha _a}$.
$\mu + \left( {{\alpha _L} + {\pi _L}} \right)\left( {a - \bar a} \right) + {\tilde \alpha _a}$.
Suicide deaths and population estimates were aggregated into 5-year age groups and 5-year calendar periods, covering the age range from 15 to 84 years and the period from 1990 to 2019. The birth cohort for each group was calculated as the difference between the midpoint of each calendar period and the midpoint of the corresponding age group. We set 2000–2004 as the reference period and the 1955 birth group as the reference cohort. The APC model generated longitudinal age curve, along with period relative risks (RRs) reflecting temporal trends common to all ages and cohorts, and cohort RRs capturing deviations in suicide mortality among individuals born in specific years, relative to the reference cohort. It should be noted that the estimated period and cohort effects derived from statistical decompositions under the model’s identifiability constraints should be viewed primarily as descriptive indicators of temporal patterns and birth-cohort differences. To assess temporal trends, net drift (the overall annual percentage change in suicide mortality) and local drift (the age-specific annual percentage change) were calculated for the three decades between 1990 and 2019. The Wald chi-square test was used to evaluate the statistical significance of the model parameters and functions, with a two-sided p-value less than 0.05 considered statistically significant. All analyses were performed using R version 4.3.1 and Python version 3.9.11.
Sensitivity analysis
To evaluate the robustness of our findings, we conducted a sensitivity analysis by varying the reference specifications. Using the manual input feature of the APC Web Tool, we defined two alternative scenarios: a historical-reference model (period: 1995–1999; age: 65–69; cohort ≈1930) and a contemporary-reference model (period: 2010–2014; age: 25–29; cohort ≈1985). For each sensitivity model, we extracted the corresponding estimates, including the longitudinal age curve, period and cohort rate ratios. The stability of our results was assessed by visually comparing functional shapes and temporal trends against the primary model (period: 2000–2004; age: 45–49; cohort: 1955), while verifying the consistency in the direction.
Results
Descriptive results
In 2019, 47,793 male and 13,111 female suicide deaths were recorded across the study regions (Table 1). Male fatalities were most prevalent in Eastern Europe (37.36% of the total), while Western Europe bore the highest female burden (40.73%). For both sexes, crude suicide mortality generally increased with age, peaking at 80–84 years in most regions, except Northern Europe where male suicide rate peaked at 50–54 years.
Suicide deaths and mortality rates per 100,000 in European subregions by sex and age group, 2019

* Mortality rates were measured with age standardized mortality rate for all age groups.
# The values in brackets (%) represent the proportion of age-specific suicide deaths among individuals of the same sex.
Figure 1 illustrates ASMRs from 1990 to 2019. For men, Eastern Europe displayed the highest ASMR, peaking at 77.81 (95% CI: 77.17–78.45) per 100,000 population in the mid-1990s, 2.5 times higher than in other regions at that time, before gradually declining to 22.93 (95% CI: 22.58–23.28) per 100,000 population by 2019. Western and Northern Europe exhibited moderate but consistent declines, from 29.32 (95% CI: 28.93–29.72) per 100,000 population and 24.44 (95% CI: 23.91–24.98) per 100,000 population in 1990 to 17.67 (95% CI: 17.38–17.96) and 18.30 (95% CI: 17.87–18.75) per 100,000 population, respectively, by 2019. Southern Europe maintained the lowest rates, with male ASMRs remaining below 20 per 100,000 population throughout the study period. Female ASMRs were much lower across all regions. Eastern Europe reported the highest female suicide rates in 1994, peaking at 13.35 (95% CI: 13.10–13.60) per 100,000 population, then dropping to 3.79 (95% CI: 3.65–3.93) per 100,000 population in 2019. Similarly, Southern Europe maintained the lowest female ASMR throughout the period.
Age-standardized mortality rates for suicide (per 100,000 people) in European subregions by sex (1990–2019). (A) Age-standardized mortality rates for suicide (per 100,000 people) in European subregions for males (1990–2019). (B) Age-standardized mortality rates for suicide (per 100,000 people) in European subregions for females (1990–2019).

Country-specific ASMR and net drift
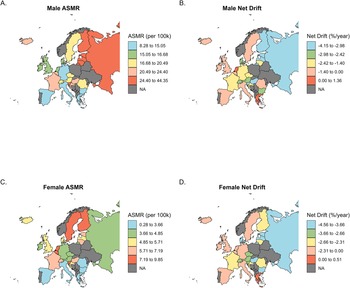
Figure 2 shows country-specific ASMRs in 2019 and net drift values from 1990 to 2019 for suicide among males (Fig. 2A, 2B) and females (Fig. 2C, 2D) across Europe. For men, the highest ASMRs were concentrated in Eastern European countries, including Russia, and in Western European outliers such as France and Iceland. Female ASMRs were substantially lower than men but showed a different regional pattern: the highest rates were observed in Norway, Sweden and the Netherlands, while most Eastern European countries fell in the lower quantiles for female suicide rates.
Country-specific age-standardized suicide mortality rates in 2019 and net drift between 1990 and 2019, by sex. (A) Male ASMRs per 100,000 population in 2019. Countries are grouped into five quantile intervals: 8.28–15.05, 15.05–16.68, 16.68–20.49, 20.49–24.40 and 24.40–44.35. (B) Male net drift in ASMRs (% from 1990 to 2019, categorized as: −4.15 to −2.98, −2.98 to −2.42, −2.42 to −1.40, −1.40 to 0.00 and 0.00 to 1.36. (C) Female ASMRs per 100,000 population in 2019. Intervals: 0.28–3.66, 3.66–4.85, 4.85–5.71, 5.71–7.19 and 7.19–9.85. (D) Female net drift in ASMRs (%) from 1990 to 2019: −4.56 to −3.66, −3.66 to −2.66, −2.66 to −2.31, −2.31 to 0.00 and 0.00 to 0.51. Countries with unavailable data are indicated as NA.

Net drift, representing the average annual percentage change in suicide mortality, revealed declines in most countries. The most notable improvements were observed in Eastern Europe (e.g., Russia, Latvia) and parts of Northern Europe (e.g., Finland) for both men and women. Notably, Greece was the only country with evidence of increasing suicide mortality, with positive net drift for both men (1.10%, 95% CI: 0.86%–1.34%) and women (0.50%, 95% CI: 0.01%–1.00%), which corresponds to a cumulative increase of roughly 38% and 16% for men and women, respectively, from 1990 to 2019.
APC effects on suicide mortality across European subregions
All relevant parameters in the subregional APC models were statistically significant. Figure 3 presents APC effects on suicide mortality across four European subregions by sex, and individualized plots for each region can be found in Figures S44–S47. Age effects, illustrated by the longitudinal age curve within the reference cohort, varied considerably across regions and between sexes (Fig. 3, Panels A and E). Among men, suicide rates were highest in Eastern Europe, with a pronounced peak at 25–30 years (111.79 per 100,000 population; 95% CI: 104.61–119.45), followed by a notable decline with advancing age. In other subregions, male suicide rates were substantially lower and more stable across most age groups, with a gradual decline at older ages in Northern Europe, but substantial increase from age 60 in Western and Southern Europe. For women, age-specific rates were lower overall and age patterns less distinct. In Eastern Europe, female suicide rates peaked at 15–20 years (15.49 per 100,000 population; 95% CI: 14.16–16.94), while in other regions, rates tended to peak around age 50.
Age, period, cohort and local drift effects on suicide mortality by sex and European subregion, 1990–2019. (A) Longitudinal age curve of male suicide mortality (per 100,000 people) for the reference cohort (born in 1955), adjusted for period effects, across four subregions of Europe. (B) Period rate ratios (RRs) for male suicide mortality relative to the 2000–2004 period, across four subregions of Europe. (C) Cohort rate ratios (RRs) for male suicide mortality (reference group: 1955 birth cohort), across four subregions of Europe. (D) Local drift values for male suicide mortality: age group-specific annual percent change (%) in suicide mortality rates, across four subregions of Europe. (E) Longitudinal age curve of female suicide mortality (per 100,000 people) for the reference cohort (born in 1955), adjusted for period effects, across four subregions of Europe. (F) Period rate ratios (RRs) for female suicide mortality relative to the 2000–2004 period, across four subregions of Europe. (G) Cohort rate ratios (RRs) for female suicide mortality (reference group: 1955 birth cohort), across four subregions of Europe. (H) Local drift values for female suicide mortality: age group-specific annual percent change (%) in suicide mortality rates, across four subregions of Europe.

Period effects, reflected in adjusted RRs from 1990 to 2019 (Fig. 3, Panels B and F) and referenced to the 2000–2004 period, exhibited a downward trend for both sexes across all subregions. Notably, men in Eastern Europe experienced a transient increase in period risk during 1995–1999 (RR: 1.06; 95% CI: 1.03–1.10), representing a 15% relative increase compared to the 1990–1994 period (RR: 0.92; 95% CI: 0.89–0.96). Additionally, the period risk for males in Southern Europe showed a marginal, non-significant increase, rising from an RR of 0.91 (95% CI: 0.88–0.93) in 2005–2009 to 0.93 (95% CI: 0.91–0.96) in 2010-2014. For the whole period, the period RR reduction was most pronounced in Eastern Europe, where the most recent period (2015–2019) demonstrated the lowest RR of around 0.40 for both sexes, representing a 60% reduction in mortality risk attributable to period-specific factors.
Cohort effects (Fig. 3, Panels C and G), referenced to the 1955 birth cohort, showed that more recent birth cohorts faced progressively lower suicide mortality in nearly all subregions and both sexes. The decline was particularly striking in Eastern Europe. For males, the cohort RR plummeted from 5.53 (95% CI: 4.28–7.13) in the 1910 cohort to 0.20 (95% CI: 0.15–0.26) in the 2000 cohort, indicating that the suicide risk for the youngest cohort was less than 4% of that experienced by the earliest cohort. Similarly, for females, the RR dropped from 9.42 (95% CI: 8.24–10.77) to 0.31 (95% CI: 0.25–0.38) over the same period. A slight upward trend was observed in female cohorts born after 1980 in Northern Europe, with the point estimate increasing from 0.73 (95% CI: 0.68–0.78) in the 1980 cohort to 0.90 (95% CI: 0.7–1.04) in the 2000 cohort. Upon examining national-specific cohort risk ratios, an upward trend was observed in Greece. Among females, the RR increased from 1.48 (95% CI: 1.11–1.97) in the 1980 cohort to 2.23 (95% CI: 1.39–3.60) in the 1995 cohort (Figure S22), reflecting a substantial 50.7% surge in risk for these younger generations. A similar, though less pronounced, increase was noted among males in Greece, with the RR rising from 1.21 (95% CI: 1.06–1.38) in 1980 to 1.44 (95% CI: 1.15–1.80) in 1995 (Figure S22). In the United Kingdom, the RR for females also showed a marked increase, from 1.28 (95% CI: 1.12–1.46) in 1995 to 1.76 (95% CI: 1.46–2.13) in the 2000 cohort (Figure S29), indicating a 37.5% escalation in risk within a single 5-year cohort interval.
Local drift estimates, representing the annual percentage change in age-specific suicide mortality rates (Fig. 3, Panels D and H), indicated a persistent decrease across nearly all age groups and subregions. Among men, the largest declines occurred in 45–60 age groups in Eastern Europe, with annual decreases exceeding 3%, while in other subregions, the most significant improvements occurred among the youngest and oldest age groups. For women, local drift was generally negative as well; however, in Northern Europe, adolescent females (aged 15–19 years) experienced a positive annual change (0.76%, 95% CI: 0.31%–1.21%), which projects to a concerning 22.8% increase in suicide rates for this group over a 30-year period. Furthermore, improvements among younger women were less pronounced compared to their male counterparts.
The results of sensitivity analyses (Figures S36–S43) demonstrated the robustness of key APC estimable functions to alternative reference specifications. Across all alternative reference settings, the trends in period and cohort RRs remained consistent, showing largely parallel trajectories in most regions except Eastern Europe, where greater variation was observed in both males and females. For the longitudinal age curves (age-specific suicide rates adjusted for period and cohort deviations), while absolute levels differed across reference cohorts, the overall age-dependent patterns – including the location of peaks and inflection points – were preserved.
Suicide means between 2010 and 2019
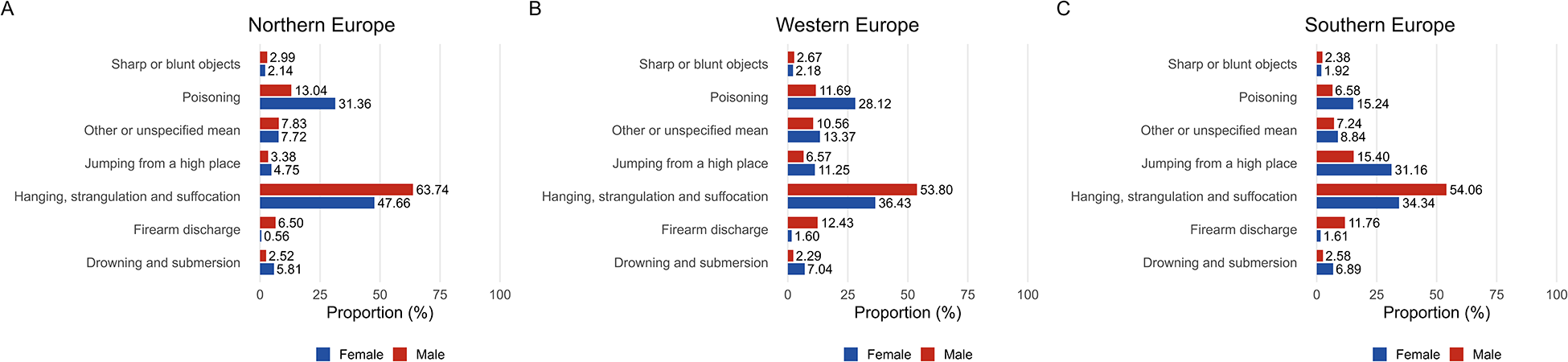
The analysis of suicide means was restricted to countries providing detailed ICD-10 data between 2010 and 2019. Due to the unavailability of granular data for Russia, the Eastern European subregion was excluded leaving Northern, Western and Southern Europe as the primary focus (Fig. 4 and Figure S2). Across all three regions, hanging, strangulation and suffocation were the predominant means of suicide for both sexes, accounting for 53.8%–63.7% among men and 34.3%–47.7% among women.
Proportional distribution of suicide means by sex in North, West and South Europe between 2010 and 2019. (A) Proportional distribution of suicide means in Northern Europe by sex (2010–2019). (B) Proportional distribution of suicide means in Western Europe by sex (2010–2019). (C) Proportional distribution of suicide means in Southern Europe by sex (2010–2019).

Other methods exhibited distinct regional and sex-related patterns. Firearm-related deaths were markedly more prevalent among men, particularly in Western (12.43%) and Southern Europe (11.76%), and these proportions are four to six times higher than those among women in the same regions. In contrast, jumping from a high place was substantially more frequent among women in Southern Europe (31.16%). Poisoning was the second most common method among women in Northern (31.36%) and Western Europe (28.12%).
Discussion
This study examined the evolution of suicide mortality across Europe through the lenses of APC effects and revealed a substantial reduction from 1990 to 2019. However, notable regional and demographic variations remain. Age-specific risk for men peaked in early adulthood and declined in Eastern Europe, while in other regions it was lower and more stable, increasing after age 60 in Western and Southern Europe; for women, age-specific risk was generally lower than that in men, with peaks in early adulthood in Eastern Europe and at midlife elsewhere. Both period and cohort effects reflected continued improvement, especially in Eastern Europe, although an upward trend was observed among female generations born after 1980 in Northern Europe and male generations born after 1995 in Southern Europe.
A primary and concerning finding of this study is the rising suicide risk among adolescent and young adult females in countries such as the Netherlands, the United Kingdom, Ireland and Sweden. This shift is evidenced by positive local drift values and adverse cohort effects for generations born after 1980 in the UK, a finding that corroborates and provides a structural context for broader surveillance data reporting an 8.5% annual escalation in suicide rates among young British females since 2012 (Bertuccio et al., Reference Bertuccio, Amerio, Grande, La Vecchia, Costanza, Aguglia, Berardelli, Serafini, Amore, Pompili and Odone2024). However, our findings suggest that this landscape is shifting. While our ecological design cannot establish causality of increasing suicide, this descriptive finding highlights a demographic subgroup becoming increasingly vulnerable. The potential drivers are likely multifactorial, constituting a critical knowledge gap for future etiological research. Individual-level studies are needed to test hypotheses concerning the growing burden of digital-age social isolation (Hazler and Denham, Reference Hazler and Denham2002; Primack et al., Reference Primack, Shensa, Sidani, Whaite, Lin, Rosen, Colditz, Radovic and Miller2017), evolving presentations of self-harm behaviours (Lurigio et al., Reference Lurigio, Danielle and And Meyers2024; López-Cuadrado et al., Reference López-Cuadrado, Mortier, Alonso and Martínez-alés2025) and seasonal affective disorders in Northern Europe (Pjrek et al., Reference Pjrek, Baldinger-Melich, Spies, Papageorgiou, Kasper and Winkler2016). Such evidence will be essential to inform any future targeted interventions.
In stark contrast to the emerging pattern in young women, our analysis confirms that midlife individuals, particularly men, continue to bear the greatest absolute burden of suicide. This demographic’s vulnerability is deeply intertwined with socio-economic challenges and psychiatric morbidity, resulting in a profound loss of both health and economic productivity (Qin et al., Reference Qin, Syeda, Canetto, Arya, Liu, Menon, Lew, Platt, Yip and Gunnell2022). Within the Europe Union, individuals aged 30–49 account for over 55% of total suicide-related productivity loss (Łyszczarz, Reference Łyszczarz2021). Despite this, middle-aged suicide remains a relative ‘knowledge gap’ compared to other age groups (Qin et al., Reference Qin, Syeda, Canetto, Arya, Liu, Menon, Lew, Platt, Yip and Gunnell2022). While proactive strategies, such as England Suicide Prevention Strategy, have begun to prioritize this group through multidisciplinary approaches involving financial support and employer engagement (Department of Health & Social Care, 2023), such targeted policy focus remains inconsistent across the rest of Europe. Targeted interventions are, therefore, needed to effectively address this enduring public health crisis, especially outside of Eastern Europe where issues have been more notable.
The temporal alignment between macroeconomic instability and suicide trends is observable in two illustrative cases from our period effect analysis. First, the finding that Greece was the only country with a consistently positive net drift for both sexes (Figure S13) aligns with the protracted socio-economic shocks of the Great Recession and the sovereign debt crisis. These crises abruptly terminated decades of economic growth, imposing severe fiscal constraints on the health system and driving a rapid rise in unemployment (Kentikelenis et al., Reference Kentikelenis, Karanikolos, Papanicolas, Basu, Mckee and Stuckler2011), which sustained a long-term upward trajectory in psychological distress (Vandoros et al., Reference Vandoros, Hessel, Leone and Avendano2013).
Second, in Eastern Europe, our period effect analysis identified sharp suicide spikes in Russia during 1991 and 1998, coinciding with the dissolution of the Soviet Union and the subsequent economic crash. These periods of profound societal disorganization and economic insecurity created a high-risk environment, particularly for males (Gavrilova et al., Reference Gavrilova, Semyonova, Evdokushkina and Gavrilov2000; Värnik and Mokhovikov, Reference Värnik, Mokhovikov, Wasserman and Wasserman2009; Minagawa, Reference Minagawa2013). This pattern stands in contrast to the stable suicide trends observed during the peaceful ‘Velvet Divorce’ of Czechoslovakia (Lochmannová et al., Reference Lochmannová, Majdan and Šafr2025). These observations suggest that the degree of harmony and stability accompanying political change may play a critical role in shaping suicide trends: abrupt and disruptive transitions are associated with elevated suicide risks, whereas peaceful and consensual changes are not.
Although suicide methods across Europe remained relatively stable between 2010 and 2019, this pattern primarily reflects the 15–84 age range. At the extremes of age, however, the epidemiology of suicide means diverges significantly. While hanging is the primary method among older adults (≥65 years), firearm use is disproportionately prevalent compared to the general population, with persistent high use among the oldest-old (≥80 years) (Cho et al., Reference Cho, Kim, Son, Jang, Kim, Lee, Lee, Oh, Kang, Tsai, Shinn, Fond, Boyer, Solmi, Woo, Yon and Fusar-Poli2025). While method-specific restrictions – such as limiting paracetamol pack sizes or installing barriers at jumping hotspots – have yielded dramatic declines in suicides by those specific means (Okolie et al., Reference Okolie, Wood, Hawton, Kandalama, Glendenning, Dennis, Price, Lloyd, John and Group1996; Hawton et al., Reference Hawton, Bergen, Simkin, Dodd, Pocock, Bernal, Gunnell and Kapur2013), the ubiquity of materials used for hanging presents a distinct prevention challenge. Nevertheless, two targeted avenues for prevention are supported by evidence. First, approximately 10% of hangings occur within controlled settings, such as psychiatric hospitals and prisons, where the systematic removal of ligature points and the implementation of safer cell designs remain critical and feasible preventive priorities (Gunnell et al., Reference Gunnell, Bennewith, Hawton, Simkin and Kapur2005). Second, qualitative research indicates that the choice of hanging is often driven by the misconception that it is a ‘clean, quick and easy’ method (Biddle et al., Reference Biddle, Donovan, Owen-Smith, Potokar, Longson, Hawton, Kapur and Gunnell2010). Public health messages must be meticulously designed to dispel the ‘clean and easy’ misconception by conveying the harsh realities of hanging, while strictly avoiding instructional details that could inadvertently facilitate an attempt (Biddle et al., Reference Biddle, Donovan, Owen-Smith, Potokar, Longson, Hawton, Kapur and Gunnell2010).
To effectively mitigate individual suicidal crises, prevention strategies must integrate macroeconomic stability, clinical systemic improvements and rapid-response mechanisms. First, robust social safety nets serve as a primary buffer against economic distress. While financial stress and unemployment significantly elevate suicide risk, evidence-based policies such as minimum wage increases and active labour market programs have proven protective (Stuckler et al., Reference Stuckler, Basu, Suhrcke, Coutts and Mckee2009; Gertner et al., Reference Gertner, Rotter and Shafer2019; Roelfs and Shor, Reference Roelfs and Shor2023). This is exemplified by Finland and Sweden, where sustained social welfare investment during severe recessions in the 1990s decoupled soaring unemployment from suicide rates. Evidence-based economic interventions can mitigate this risk (Jäntti et al., Reference Jäntti, Martikainen, Valkonen, Cornia and Paniccià2000; Catalano and Bellows, Reference Catalano and Bellows2005; Stuckler et al., Reference Stuckler, Basu, Suhrcke, Coutts and Mckee2009). Meanwhile, healthcare systems must shift towards proactive and integrated mental health services. Given that nearly half of suicide decedents visit primary care shortly before death (Luoma et al., Reference Luoma, Martin and Pearson2002; Stene-Larsen and Reneflot, Reference Stene-Larsen and Reneflot2017), systematic improvements – such as 24-hour crisis care and multidisciplinary reviews – are essential (While et al., Reference While, Bickley, Roscoe, Windfuhr, Rahman, Shaw, Appleby and Kapur2012). However, mental health resources across Europe remain unevenly distributed; Eastern Europe, in particular, faces chronic underfunding and severe workforce shortages compared to the European Union average (Winkler et al., Reference Winkler, Guerrero, Kågström, Petrášová, Pashoja, Qirjako, Hristakeva, Germanov, Kuzman, Kuharić, Havlíková, Eek, Maron, Őri, Wernigg, Fanaj, Krasniqi, Sile, Brinkmane, Levickaitė, Grigaitė, Manusheva, Kalpak, Ivanovic, Chihai, Mihaela, Gondek, Todzia-Kornaś, Mihai, Molnar, Letovancová, Kopcová, Suvalo, Khudoba, Ismayilova, Muradova, Makhashvili, Dumbadze, Panteleeva, Popkov, Al Tayara, Van Voren and Thornicroft2025). Third, immediate crisis intervention is vital for interrupting the brief peak window of suicidal intent. Professional, clinically integrated services – exemplified by France’s national ‘3114’ helpline – transform reactive tools into operational hubs that coordinate local prevention networks and mobilize stakeholders (Notredame et al., Reference Notredame, Wathelet, Morgiève, Grandgenèvre, Debien, Mannoni, Pauwels, Ducrocq, Leaune, Binder, Berrouiguet, Walter, Courtet, Vaiva and Thomas2025). Furthermore, suicide prevention must address a persistent ‘gender paradox’: while men exhibit higher mortality rates, women report higher rates of ideation and non-fatal attempts (Berardelli et al., Reference Berardelli, Rogante, Sarubbi, Erbuto, Cifrodelli, Concolato, Pasquini, Lester, Innamorati and Pompili2022; Moloney et al., Reference Moloney, Amini, Sinyor, Schaffer, Lanctôt and Mitchell2024; GBD 2021 Suicide Collaborators, 2025). Of particular concern is the rising trend of non-fatal self-harm among young women, evidenced by sharp increases in hospital admissions in Spain (2018–2023) and a near-tripling of rates among females aged 15–24 in Denmark (Reuter Morthorst et al., Reference Reuter Morthorst, Soegaard, Nordentoft and Erlangsen2016; López-Cuadrado et al., Reference López-Cuadrado, Mortier, Alonso and Martínez-alés2025). Simultaneously, men remain less likely to proactively seek help, challenging traditional ‘help-seeking’ models such as routine healthcare and counselling (Stene-Larsen and Reneflot, Reference Stene-Larsen and Reneflot2017). Therefore, future suicide prevention strategies must move beyond merely ‘providing equitable services’ and actively address issues of equitable access.
The interpretation of European suicide trends must account for variations in national ascertainment mechanisms. While the transition to ICD-10 primarily improved method granularity without significantly biasing total estimates (Gjertsen et al., Reference Gjertsen, Bruzzone, Vollrath, Pace and Ekeberg2013; Hensley et al., Reference Hensley, Esie, Ta and Matheson2026), suicide statistics remain susceptible to misclassification. Instead, data accuracy depends more heavily on national ascertainment mechanisms. The propensity for suicide to be ‘hidden’ within accidental deaths or drug-related fatalities varies by nation, influenced by religious stigmas and legal frameworks (Pritchard and Hansen, Reference Pritchard and Hansen2015; Schmeckenbecher et al., Reference Schmeckenbecher, Kapusta, Krausz and Emilian2024). Consequently, our descriptive findings may represent a conservative underestimation, requiring caution in cross-sectional comparisons. Despite cross-sectional variations, the longitudinal validity of these trends remains robust. A salient example is the 2018 legal shift in England and Wales; although lowering the evidentiary standard from a ‘criminal’ to a ‘civil’ threshold triggered an internal reclassification of deaths, it did not fundamentally alter overall suicide statistics, as both ‘undetermined’ and ‘intentional’ deaths are included in the National Statistics definition. However, the upward trend commenced in 2017, predating the legal change and confirming that the observed shifts reflect genuine social drivers rather than procedural artefacts (Office for National Statistics, 2021). Finally, our strict inclusion protocol prioritized data integrity and internal validity over geographical representativeness, which may inevitably introduce selection bias by excluding countries with less developed surveillance infrastructure. These excluded populations may systematically differ in their suicide epidemiology; thus, caution is required when generalizing our subregional findings to the broader European context.
This study has several limitations. First, data accuracy is subject to national variations in death certification and the classification of undetermined deaths. While suicides may be underreported or misclassified across jurisdictions, our longitudinal approach ensures meaningful comparative utility, as temporal trends remain informative of underlying suicide dynamics provided national registration protocols stay relatively consistent. Second, the ecological design precludes individual-level causal inferences; observed population-level associations between socio-economic shifts and suicide trends should not be interpreted as direct causality. Third, our analytical scope established specific boundary conditions, by excluding populations under 15 and over 85 – as well as countries lacking complete registration (e.g., Ukraine). Consequently, these findings may not be generalizable to the youngest or oldest-old populations, nor to regions with less robust surveillance, whose suicide dynamics may distinctively differ from the cohorts studied. Fourth, methodological constraints inherent to APC modelling must be acknowledged. Our sensitivity analyses demonstrated that key interpretations were robust to alternative model specifications. However, the models may not fully capture sudden, short-term shocks from socio-political crises or abrupt improvements in vital registration. Finally, our stratified analyses were exploratory, prioritizing the identification of ‘emerging risks’ over discrete hypothesis testing. Consequently, formal multiple-comparison corrections were omitted to minimize Type II errors, potentially increasing Type I error risks in smaller strata. Despite these limitations, this comprehensive analysis provides crucial insights into the evolving patterns of suicide mortality in Europe, delineating both persistent public health challenges and emerging at-risk populations that require differentiated and evidence-informed prevention strategies.
Conclusion
In conclusion, notable regional and gender differences in suicide mortality rate were observed across Europe between 1990 and 2019. Eastern Europe consistently had the highest suicide rates but with marked declines over time. While men showed greater absolute risks, women demonstrated less pronounced age-specific and regional differences. Patterns by suicide method also varied substantially by region and sex. These findings provide a comprehensive overview of the changing epidemiology of suicide in Europe. This refined understanding serves as a vital prerequisite for developing the next generation of effective, evidence-based preventive interventions.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796026100663.
Availability of data and materials
The suicide statistic data used in this study are publicly available on the World Health Organization Mortality Database website (https://www.who.int/data/data-collection-tools/who-mortality-database). Population estimates can be found on United Nations’ World Population Prospects 2024 (https://population.un.org/wpp/). The code used in this analysis is available from corresponding authors, JL and FH, upon reasonable request.
Acknowledgements
None.
Author contributions
All authors contributed to the study design. JL and FH conceived the study. BZ and JL curated the data, performed content analysis and drafted the initial manuscript. BZ and MZ cross-checked the data quality. JL and FH reviewed and revised the manuscript and related materials. All authors actively participated in discussing and interpreting the results. JL and FH attest that all listed authors meet the authorship criteria and that no individuals meeting the criteria have been omitted. BZ and MX contributed equally to this work and are joint first authors. FH (fengsu_hou@szu.edu.cn) and JL (lijinghua@um.edu.mo) are co-corresponding authors.
Financial support
FH is supported by the National Natural Science Foundation of China (grant ID 72374095) and Guangdong Basic and Applied Basic Research Foundation (grant ID 2022A1515011533). JL is supported by The Start-up Research Grant of the University of Macau (SRG2025-00031-FHS). The funders had no role in the study design, data collection, data analysis, data interpretation or writing.
Competing interests
We declare no competing interests.
Ethical standards
Ethical approval and inform consent can be waived since this study was based on aggregated regional and national/territorial-level health statistic data. JL and FH affirm that this manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.






 Open access
Open access