


Introduction
As the country with the largest elderly population in the world, China has approximately 249 million individuals aged 60 and above (Zhang et al. Reference Zhang, Li and Gao2021). Elderly patients are at a heightened risk of developing cancer due to the disease’s subtle onset and atypical early symptoms. According to global cancer statistics, there were 19.29 million new cancer cases worldwide in 2020. This number is projected to increase to 28.4 million by 2040, with 64% of patients aged 60 years or older – a proportion significantly higher than that of younger aged groups (Sung et al. Reference Sung, Ferlay and Siegel2021). Elderly cancer patients often experience a range of psychological and physical symptoms throughout the onset, progression, and treatment of the disease. These symptoms frequently interact and exacerbate one another, leading to a substantial symptom burden that adversely affects patients’ functional status, quality of life, and overall prognosis. Given China’s large population and the accelerating aging trend, the incidence of cancer among older adults is expected to rise steadily. Consequently, assessing the health-related quality of life (HRQOL) of elderly cancer patients has become a critical priority for healthcare professionals (Zhang et al. Reference Zhang, Guo and Song2023).
The European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ)-C30 questionnaire is a widely used instrument for assessing HRQOL of cancer patients. However, it does not adequately address the specific needs of elderly patients, resulting in limited sensitivity and precision (Li et al. Reference Li, Hu and Zhou2024). To fill this gap, the EORTC developed the QLQ-ELD14 as a supplementary module to the QLQ-C30, incorporating age-related issues relevant to cancer patients. Developed through a multicultural, interdisciplinary collaboration, the QLQ-ELD14 has been validated across 10 countries and regions, demonstrating strong psychometric properties and high patient compliance (Wheelwright et al. Reference Wheelwright, Darlington and Fitzsimmons2013). Nevertheless, most validation studies have been conducted in European populations; despite its robust validation in European cohorts, the applicability of the QLQ-ELD14 in Asian contexts – particularly in China – remains unexplored. Therefore, this study aims to adapt the QLQ-ELD14 to the Chinese context through rigorous translation and back-translation, guided by cultural and linguistic considerations, and to evaluate its reliability and validity among elderly Chinese patients.
Methods
Introduction of the EORTC QLQ-ELD14
The EORTC QLQ-ELD14 is a specialized quality of life assessment tool developed by the EORTC (Li et al. Reference Li, Hu and Zhou2024). This scale serves as a supplementary module to the core QLQ-C30 questionnaire and evaluates 7 key dimensions: physical functioning and independence, family and social roles, concerns about the future, the pursuit of life goals, disease-related symptoms, joint stiffness, and family support. Each item is rated on a 4-point Likert scale, ranging from 1 (“never”) to 4 (“always”), and the responses are standardized and converted to a score between 0 and 100. Higher scores in the dimensions of maintaining life goals and family support indicate better patient functioning, whereas elevated scores in the other dimensions suggest more severe symptoms or a poorer quality of life. Comprising 14 items, the QLQ-ELD14 exhibits strong psychometric properties, demonstrating robust internal consistency with a Cronbach’s α exceeding 0.7.
Translation and cultural adaptation of the scale
With authorization obtained from the original author, the scale was translated into Chinese following the modified Brislin cross-cultural research translation model (Wheelwright et al. Reference Wheelwright, Darlington and Fitzsimmons2013). The process involved the following steps: (1) Initial translation: Two bilingual experts – native Chinese speakers with advanced English proficiency – independently translated the original English scale into 2 Chinese versions, designated as Versions A and B. (2) Back-translation: Two additional bilingual experts, similarly qualified, independently back-translated Versions A and B into English, producing Versions CA and DB. (3) Review and reconciliation: The 4 bilingual experts and researchers compared all versions (A, B, CA, DB) with the original scale, resolving discrepancies through discussion to produce a consolidated Chinese version, T. (4) Secondary back-translation: Version T was independently back-translated into English by 2 bilingual experts, resulting in Versions E and F. (5) Final validation: The experts reviewed Versions E and F against the original scale, confirming that discrepancies were minimal before finalizing the Chinese version, T1.
An expert panel comprising 5 individuals with extensive experience in oncology care, expertise in quality-of-life assessment, and familiarity with the Chinese language and culture was convened. The panel undertook a comprehensive review of the instructions, items, and scoring methods of the EORTC QLQ-ELD14 scale. All panel members held academic degrees at or above the bachelor’s level and included 1 chief physician, 1 associate chief physician, 2 associate chief nursing officers, and 1 associate professor. This study involved 2 rounds of expert consultations on the initial translated version (T1) of the scale. Based on the feedback from the experts, modifications were made to enhance cultural adaptation and clarity, resulting in the Chinese version of the EORTC QLQ-ELD14 (T2).
Pilot survey
A convenience sampling method was employed to select 15 elderly cancer patients receiving chemotherapy at the day ward, breast oncology department, and radiation oncology department of a specialized hospital in Tianjin between June 2024 and July 2024. Inclusion criteria were: (1) age ≥60 years; (2) a confirmed diagnosis of malignant tumor via clinical cytology or pathology; and (3) informed consent and voluntary participation in the study. Exclusion criteria included: (1) impairments in hearing or language expression that hinder communication; (2) persistent coma; and (3) current participation in other clinical trials. Prior to data collection, researchers explained the study’s purpose and filling procedures to the participants and addressed any questions. Feedback obtained during this process was incorporated to refine the Chinese version of the EORTC QLQ-ELD14, which was subsequently used for the formal survey.
Validation of reliability and validity
From July 2024 to February 2025, elderly cancer patients visiting a tertiary hospital in Tianjin were selected as study subjects using a convenience sampling method. The inclusion and exclusion criteria mirrored those employed in the pilot survey. According to Kendal’s sample size estimation method, the required sample size should be 5–10 times the number of items on the scale. Taking into account a projected 20% loss to follow-up, a total of 260 patients were included in this study.
A self-administered questionnaire was employed to gather general demographic and clinical information from the study participants. The questionnaire included variables known to potentially impact health outcomes and quality of life in elderly cancer patients, such as age (in years), gender (male/female), and marital status (married, single, divorced, widowed). To ensure face validity, the questionnaire was reviewed and validated by experts in geriatric oncology.
The Chinese version of the EORTC QLQ-ELD14 scale comprises 14 items across 7 dimensions, utilizing a 4-point Likert scale (not at all = 1, a little = 2, quite a bit = 3, very much = 4). Higher scores on the “maintenance of life goals” and “family support” dimensions indicate better patient functioning, whereas higher scores on the other dimensions reflect more severe symptoms or a poorer quality of life.
QLQ-C30 was selected as a benchmark to evaluate the consistency of the QLQ-ELD14 scale with well-established measure (Schurr et al. Reference Schurr, Loth and Lidington2023). This scale comprises 30 items across 15 dimensions, including 5 functional domains – physical functioning (PF), role functioning (RF), emotional functioning (EF), social functioning (SF), and cognitive functioning (CF) – 3 symptom domains – fatigue (FA), pain (PA), and nausea/vomiting (NV) – 1 quality of life (QL) dimension, and 6 single items – dyspnea (DY), appetite loss (AP), insomnia (IN), constipation (CO), diarrhea (DI), and financial difficulties (FI) (Li et al. Reference Li, Ye and Du2025). All scores are linearly transformed to a 0–100 scale. For the 5 functional domains and the QL dimension, higher scores indicate better functioning and quality of life. Conversely, for symptom domains and the 6 single items, higher scores reflect more severe symptoms and poorer quality of life. The EORTC QLQ-C30 summary score is calculated as the average of 13 dimension scores, excluding FI and the QL dimension. Prior to computing the summary score, scores for symptom domains and single items are transformed using the formula: 100 minus the original score.
Two uniformly trained team members distributed the questionnaires and collected data through an on-site survey. Prior to distribution, participants were informed about the study’s purpose and significance, provided informed consent, and had their questions addressed promptly. The questionnaires were collected and reviewed on-site. In total, 260 questionnaires were distributed, of which 248 were valid, yielding a valid response rate of 95.4%.
Item analysis: (1) The critical ratio (CR) was employed to assess the discriminative ability of each item in the Chinese version of the EORTC QLQ-ELD14. Total scores for 248 participants were ranked from lowest to highest. The top 27% constituted the low group, while the bottom 27% formed the high group. An independent samples t-test was performed between 2 groups. Items with a CR value greater than 3.000 and a P-value less than 0.05 were considered to have good discrimination. (2) Correlation analysis was conducted to examine the relationship between each item score and the total scale score. Items with a correlation coefficient less than 0.2 or a P-value greater than 0.05 were removed.
Reliability: (1) Cronbach’s α coefficient was used to evaluate the internal consistency reliability of the total scale and each dimension. A Cronbach’s α coefficient >0.800 indicated good scale reliability. (2) The intraclass correlation coefficient (ICC) was used to evaluate the test–retest reliability of the scale. After an interval of 2 weeks, 20 subjects were conveniently selected for repeated measurements. An ICC >0.700 indicated good stability of the scale.
Validity assessment: (1) Content validity: Five experts in psychology or nursing were invited to conduct 2 rounds of consultation on the Chinese version of the EORTC QLQ-ELD14. Experts rated each item’s relevance using a 4-point Likert scale: 1 (“not relevant”), 2 (“weakly relevant”), 3 (“moderately relevant”), and 4 (“strongly relevant”). Based on these ratings, the scale-level content validity index (S-CVI) and item-level content validity index (I-CVI) were calculated. A scale is considered to have good content validity when S-CVI ≥ 0.800 and I-CVI ≥ 0.780. (2) Construct validity: Exploratory factor analysis (EFA) was employed to assess the construct validity of the Chinese version of the EORTC QLQ-ELD14. The Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity were first performed. A KMO value greater than 0.8 and a statistically significant Bartlett’s test (P < 0.05) indicate that the data are suitable for factor analysis. Items with factor loading exceeding 0.450 were considered to load significantly on a given factor. (3) Criterion-related validity: The widely used Chinese version of the EORTC QLQ-C30, which has demonstrated a moderate correlation with the EORTC QLQ-ELD14, was chosen as the criterion scale. The correlation coefficient between the Chinese EORTC QLQ-ELD14 and the EORTC QLQ-C30 was calculated. A higher correlation coefficient indicates greater criterion-related validity of the scale.
Statistical methods
Data were entered concurrently by 2 independent individuals using Excel spreadsheets. Frequencies and percentages were calculated using SPSS version 26.0 to summarize the demographic and clinical characteristics of the sample.
Item homogeneity: The Spearman correlation coefficient was employed to examine the relationship between each individual item on the scale and the total score, ensuring that each item consistently contributes to the overall measurement.
Item discrimination: The CR method was utilized by ranking the total scale scores. Items were compared between the high-scoring group (top 27%) and the low-scoring group (bottom 27%) using a non-parametric test to assess each item’s ability to differentiate between the groups.
Validity: Construct validity was evaluated through EFA, while the Spearman correlation coefficient was used to assess scale criterion validity. Non-parametric tests were conducted to analyze differences in scale scores between various groups, and expert evaluation was employed to measure the CVI for content validity.
Reliability: Reliability was assessed using Cronbach’s α coefficient to evaluate the consistency of the scale content, alongside test–retest reliability to determine the stability of the scale. Twenty patients were randomly selected from the 248 subjects and asked to complete the EORTC QLQ-ELD14 scale again 1 week after the initial assessment. The correlation coefficient between the 2 assessments was calculated to establish test–retest reliability. The significance level for all analyses was set at α = 0.05.
Results
General participant characteristics
The study comprised 248 elderly cancer patients, with a mean age of 69.22 ± 6.61 years. Additional demographic and clinical information is provided in Table 1.
Demographic and clinical characteristics of the study population (n = 248)

Table 1 Long description
The table summarizes demographic and clinical characteristics for 248 participants, reporting counts and percentages for each category. Women made up 140 participants (56.5%) and men 108 (43.5%). Most were married (195, 78.6%) and most lived with a spouse or family (210, 84.7%), while 38 (15.3%) lived alone. Education was most often high school (86, 34.7%) or middle school (72, 31.5%), with fewer having college or higher education (27, 14.9%). Monthly household income per capita was most commonly in the five thousand range (82, 33.1%), followed by under three thousand (67, 27.0%), the three thousand range (55, 22.2%), and eight thousand or more (44, 17.7%). Half had employee medical insurance (125, 50.4%), 103 (41.5%) had urban and rural resident insurance, and 20 (8.1%) had no insurance. A history of chemotherapy was reported by 172 participants (69.4%). Breast cancer was the most frequent cancer type (70, 28.2%), followed by gastric (52, 21.0%), colorectal (45, 18.1%), liver (40, 16.1%), cervical (21, 8.1%), and other types (20, 8.5%). Time since diagnosis clustered within the first 18 months, with 84 (33.9%) diagnosed within 6 months, 69 (27.8%) between 6 and 12 months, 72 (29.0%) between 12 and 18 months, and 23 (9.3%) at 18 months or more.
Item analysis results
The CR analysis indicated that the CR values for the 14 items of the Chinese version of the EORTC QLQ-ELD14 ranged from 4.448 to 15.271, all exceeding the threshold of 4.000. Differences between high- and low-scoring groups were statistically significant (all P < 0.001), demonstrating strong discrimination for each item between 2 groups. Pearson correlation analysis revealed that the correlation coefficients between individual item scores and the total scale score ranged from 0.380 to 0.767 (all P < 0.001), indicating that each item adequately reflects the underlying construct measured by the scale. Based on these results, all items from the original scale were retained.
Validity
Content validity: The I-CVI for the Chinese version of the EORTC QLQ-ELD14 ranged from 0.800 to 1.000, surpassing the generally accepted threshold of 0.78 for acceptable item-level content validity. Furthermore, the S-CVI was 0.980, exceeding the common standard of 0.90 for excellent scale-level content validity. These findings indicate that the content validity of the scale is robust, demonstrating a high degree of relevance to the construct being measured.
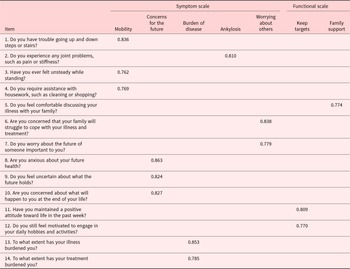
Construct validity: EFA was performed on the 14 items of the Chinese version of the EORTC QLQ-ELD14 scale. The KMO measure was 0.945, and Bartlett’s test of sphericity yielded a χ2 value of 7029.629 (df = 435, P < 0.01), indicating that the data were suitable for factor analysis. Using principal component analysis with varimax orthogonal rotation, 7 underlying factors were extracted: mobility (3 items), worries about the future (3 items), burden of disease (2 items), joint stiffness (1 item), worries about others (2 items), maintaining goals (2 items), and family support (1 item). The resulting factor structure was consistent with the original scale design, accounting for 83.912% of the cumulative variance. All items demonstrated factor loading greater than 0.45 on their respective factors, supporting their retention in the scale (see Table 2).
Item factor loading of the EORTC QLQ-ELD14
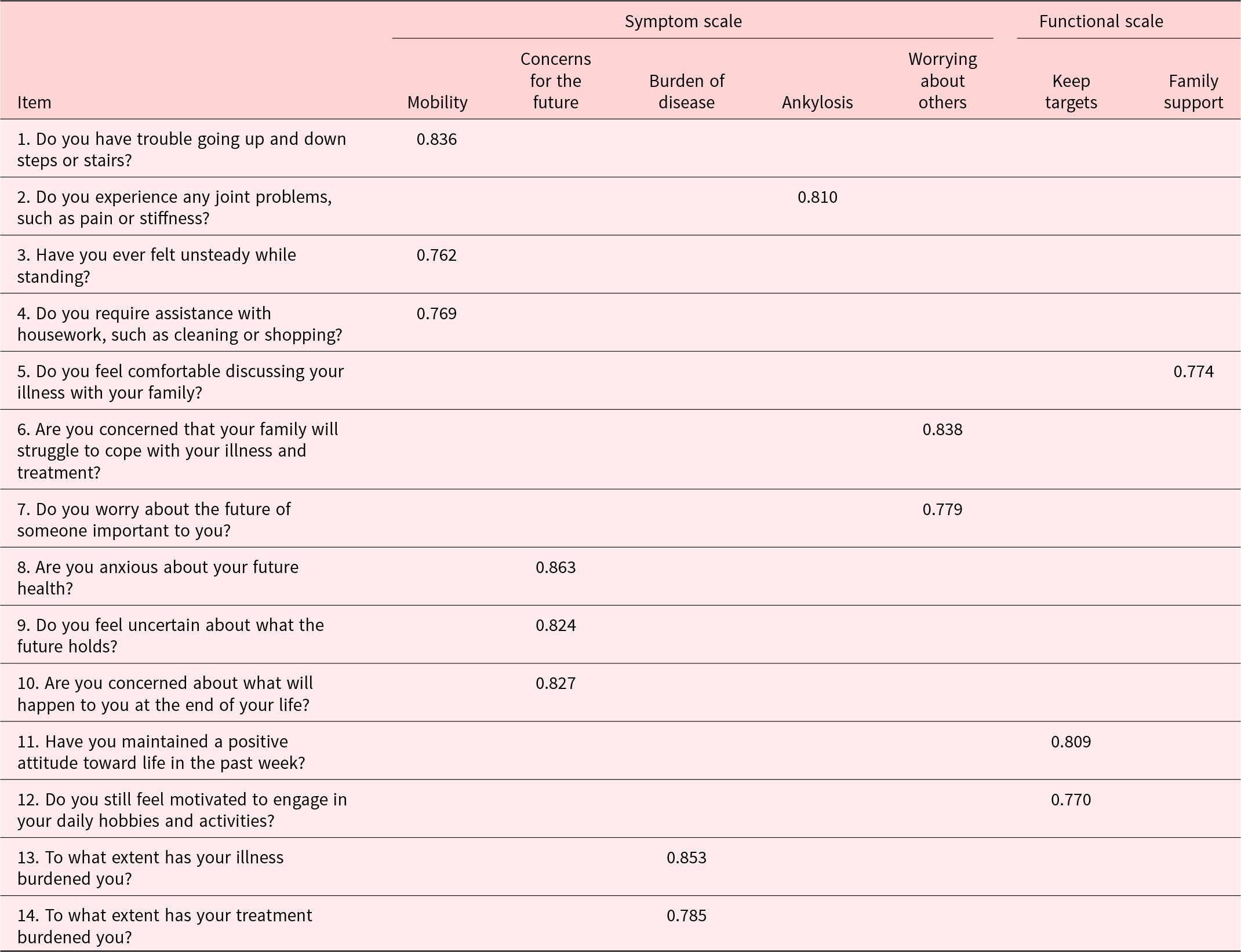
Table 2 Long description
The table lists factor loadings for 14 questionnaire items mapped to seven scales, grouped as symptom scales (Mobility, Concerns for the future, Burden of disease, Ankylosis) and functional scales (Worrying about others, Keep targets, Family support). Mobility items load strongly: stairs 0.836, unsteady standing 0.762, and needing help with housework 0.769. Concerns for the future has the highest values overall, with anxious about future health 0.863, uncertain about the future 0.824, and end of life concerns 0.827. Burden of disease items load highly, especially illness burden 0.853 and treatment burden 0.785. Ankylosis is represented by joint pain or stiffness at 0.810. Functional scales show strong loadings for worrying about others, including family coping 0.838 and worry about someone important 0.779, while keep targets includes positive attitude 0.809 and motivation for hobbies 0.770; family support includes comfort discussing illness with family 0.774. Each item is shown loading on a single scale in this table, so cross-loadings and overall model fit are not provided and should not be inferred.
Criterion-related validity: The correlation coefficient between the total scores of the Chinese version of the EORTC QLQ-ELD14 and the EORTC QLQ-C30 was 0.936 (P < 0.01). For the 7 dimensions of the EORTC QLQ-ELD14, the correlation coefficients with the corresponding dimensions of the QLQ-C30 ranged from 0.795 to 0.876 (all P < 0.01). These high correlation values indicate that the Chinese version of the EORTC QLQ-ELD14 demonstrates strong criterion-related validity, confirming its effectiveness in measuring constructs consistent with an established criterion scale.
Reliability
The overall Cronbach’s α coefficient for the scale was 0.958. The Cronbach’s α coefficients for all 7 dimensions exceeded 0.800, indicating high internal consistency. The test–retest reliability of the scale was 0.849 (P < 0.01), with the 7 dimensions demonstrating reliability coefficients ranging from 0.813 to 0.856 (all P < 0.01). These findings suggest that the Chinese version of the EORTC QLQ-ELD14 demonstrates excellent reliability, both in terms of internal consistency and temporal stability.
Discussion
The quality of research instruments significantly influences the accuracy and reliability of research data. Reliability and validity are essential indicators for evaluating these tools’ quality (Tack et al. Reference Tack, Senff and Kimball2025). In this study, we employed Cronbach’s α coefficient and test–retest reliability to assess the scale’s consistency. The Chinese version of the EORTC QLQ-ELD14 demonstrated excellent internal consistency, with a Cronbach’s α of 0.958 across all 7 dimensions, each exceeding 0.951. The test–retest reliability was 0.849, indicating that the scale provides stable and consistent measurements over time.
Regarding validity, we assessed content validity, structural validity, and criterion-related validity (Lormans et al. Reference Lormans, de Graaf and van der Baan2025; Shinkai et al. Reference Shinkai, Narita and Murayama2025). The Chinese version of the EORTC QLQ-ELD14 showed strong content validity, with an I-CVI ranging from 0.800 to 1.000 and an S-CVI of 0.980, confirming that the instrument effectively captures the intended content. EFA identified 7 factors consistent with the original scale structure, accounting for 82.913% of the total variance. All items exhibited factor loading above 0.450, indicating that each item is appropriately associated with its respective factor.
The shift toward a patient-centered medical model has expanded the focus from solely evaluating survival rates to also considering patients’ quality of life (QOL) (Heß et al. Reference Heß, Meng and Schulte2022). According to the World Health Organization, QOL is defined as individuals’ perceptions of their position in life within the context of their culture and value systems, as well as in relation to their goals, expectations, standards, and concerns (The World Health Organization Quality of Life Assessment 1998). For elderly cancer patients, QOL is influenced not only by the cancer itself and its treatment but also by non-cancer factors such as comorbidities, functional impairments, and the burden of multiple medications. Therefore, addressing and managing QOL in this population is essential (Rios et al. Reference Rios, de Oliveira and da Costa2021). The development and application of scientifically validated assessment tools are critical for effective intervention. Currently, there is a lack of specific QOL assessment instruments tailored for elderly cancer patients in China. To address this gap, the Chinese version of the EORTC QLQ-ELD14 was rigorously translated and culturally adapted. This process involved forward translation, back-translation, expert consultation, and cognitive interviews, followed by comprehensive tests of reliability and validity. During cultural adaptation, expert input was used to modify the scale’s response options and language expressions to enhance participants’ understanding and response accuracy. The final scale comprises 7 dimensions and 14 items that assess physical, psychological, and daily life aspects, providing a comprehensive evaluation of QOL. Its demonstrated reliability and validity confirm that the Chinese version of the EORTC QLQ-ELD14 is a scientifically sound tool for assessing QOL for elderly cancer patients in China. Clinicians can utilize this instrument to gain in-depth insights into patients’ health status, facilitating the development of personalized care plans and optimized treatment strategies. Additionally, nursing managers can employ the tool to improve service quality and ultimately enhance the health and well-being of this vulnerable patient population.
The Chinese version of the EORTC QLQ-ELD14 scale exhibits strong reliability and validity among elderly cancer patients in China. Its concise format – designed for ease of understanding and completion within 3–5 minutes – renders it a practical tool for clinical applications. However, a notable limitation of the study is that it was conducted in a single tertiary hospital in Tianjin, which may restrict the generalizability of the findings to the broader population of elderly cancer patients throughout China. To address this limitation, the study recommends that future research expand both the sample size and geographic scope. Future work should include participants from diverse regions and various levels of healthcare facilities to ascertain whether the scale retains its psychometric properties across a more heterogeneous sample. Such wider-ranging research would enhance the robustness and applicability of the Chinese version of the EORTC QLQ-ELD14 in different clinical contexts, ultimately improving its utility in both research and practice nationwide.
Conclusion
This study rigorously validated the Chinese version of the EORTC QLQ-ELD14 as a reliable, valid, and clinically feasible instrument for assessing the quality of life for elderly cancer patients in China. The scale demonstrates high internal consistency, robust psychometric properties, and a rapid administration time, establishing it as an essential tool for integrating geriatric-specific quality of life assessments into routine oncology care. Given that the current validation was conducted in a tertiary hospital setting, future multicenter studies across diverse regions and healthcare tiers are necessary to confirm its generalizability. We advocate for the immediate adoption of this scale in both clinical practice and research to address unmet needs in geriatric oncology care, ultimately facilitating tailored interventions that prioritize the holistic well-being of elderly cancer patients in China and culturally similar contexts.
Acknowledgments
Not applicable.
Author contributions
Study design: Y.L., W.H.Y.; data acquisition: S.R.J., S.R.; data analysis and interpretation: S.R.J., W.Q.; manuscript preparation: Y.L., W.H.Y.; manuscript editing: W.Y., S.R.; all authors have read and approved the submitted manuscript.
Funding
The study was funded by Tianjin Key Medical Discipline Construction Project (Grant No. TJYXZDXK-3-003A).
Competing interests
The authors declare no conflicts of interest. All co-authors have reviewed and approved the manuscript’s contents, and there are no financial interests to disclose.
Ethical approval
The study was conducted by the Declaration of Helsinki, and the Ethics Committee of Tianjin Medical University Cancer Institute and Hospital approved the study.


 Open access
Open access