


Introduction
In the clinical management of schizophrenia, long-term maintenance treatment with antipsychotic medications is widely advocated as the standard practice for sustaining therapeutic effects and preventing relapse. However, this conventional paradigm has increasingly been challenged by emerging findings. First, long-term use of antipsychotics can cause adverse effects, including metabolic abnormalities (e.g. hyperprolactinemia, weight gain) and extrapyramidal symptoms (Zito & Marder, Reference Zito and Marder2020). These side effects are common and can significantly compromise patients’ physical and mental well-being (Read & Williams, Reference Read and Williams2019; Schneider-Thoma et al., Reference Schneider-Thoma, Chalkou, Dörries, Bighelli, Ceraso, Huhn and Leucht2022). They frequently contribute to patients’ reluctance to adhere to medication regimens, posing ongoing challenges for psychiatrists in clinical practice. Second, accumulating evidence from cohort studies and systematic reviews suggests that chronic exposure to antipsychotics may be associated with reductions in brain volume (Haijma et al., Reference Haijma, Van Haren, Cahn, Koolschijn, Hulshoff Pol and Kahn2013; Ho et al., Reference Ho, Andreasen, Ziebell, Pierson and Magnotta2011; van Erp et al., Reference van Erp, Walton, Hibar, Schmaal, Jiang, Glahn and Turner2018), raising additional concerns about the long-term safety and outcomes of continuous treatment.
Conversely, evidence suggests that antipsychotic dose reduction/discontinuation (DRD) may lead to better social functional outcomes compared to continued treatment (Wunderink et al., Reference Wunderink, Nienhuis, Sytema, Slooff, Knegtering and Wiersma2007). A 7-year open-label randomized controlled trial (RCT) found that patients in the DRD group had twice the rate of recovery compared to those maintained on antipsychotics (40.4% vs. 17.6%), with this advantage particularly evident in functional recovery (46.2% vs. 19.6%) (Wunderink et al., Reference Wunderink, Nieboer, Wiersma, Sytema and Nienhuis2013). These findings have prompted further exploration into the potential negative impact of sustained antipsychotic treatment on functional outcomes.
A subset of patients with psychotic disorders can safely discontinue antipsychotic treatment. A systematic review of 10 RCTs reported that 45.7% of patients remained relapse-free 12 months after antipsychotic discontinuation, with this proportion remaining at 39.4% at 18–24 months (Kishi et al., Reference Kishi, Ikuta, Matsui, Inada, Matsuda, Mishima and Iwata2019). Similarly, in the Chicago cohort (Harrow, Jobe, & Faull, Reference Harrow, Jobe and Faull2012) and the Danish OPUS cohort (Wils et al., Reference Wils, Gotfredsen, Hjorthøj, Austin, Albert, Secher and Nordentoft2017), approximately one-third of participants achieved significant symptom remission following antipsychotic discontinuation. Notably, a 10-year follow-up cohort (Morgan et al., Reference Morgan, Lappin, Heslin, Donoghue, Lomas, Reininghaus and Dazzan2014) found that roughly 19% of patients remain symptom-free without medication after an initial episode of schizophrenia. Among those with good functional recovery, some successfully avoided relapse and no longer required ongoing antipsychotic intervention. However, predictive factors allowing early identification of patients likely to achieve favorable functional outcomes after antipsychotic discontinuation remain inadequately understood.
Existing research has highlighted several predictors associated with positive outcomes after discontinuation, including sociodemographic variables and clinical characteristics (e.g. the severity of positive and negative symptoms, responsiveness to antipsychotic treatment, number of hospitalizations, and total illness duration), with socioeconomic status and occupational engagement being particularly relevant (Spellmann et al., Reference Spellmann, Riedel, Schennach, Seemüller, Obermeier, Musil and Möller2012). The OPUS cohort identified female sex, absence of substance use disorder, milder negative symptoms, higher scores on the Global Assessment of Functioning (GAF) scale, and employment as factors linked to sustained remission without relapse following antipsychotic discontinuation (Wils et al., Reference Wils, Gotfredsen, Hjorthøj, Austin, Albert, Secher and Nordentoft2017). Additionally, duration of untreated psychosis (DUP) <30 days and favorable social and occupational functioning during the initial 2 years of follow-up have also emerged as potential prognostic indicators (Hui et al., Reference Hui, Honer, Lee, Chang, Chan, Chen and Chen2018).
In this study, the term functional remission (FR) refers to real-world social and occupational functioning independent of symptomatic status, as defined by the Functional Remission of General Schizophrenia (FROGS) scale (Llorca et al., Reference Llorca, Lançon, Lancrenon, Bayle, Caci, Rouillon and Gorwood2009). Although terminology in the literature varies, functional disability in schizophrenia is increasingly recognized as dynamic rather than static (Harvey & Bellack, Reference Harvey and Bellack2009), and the construct of FR has been supported in prior validation studies. The Functional Remission in patients with Schizophrenia after Antipsychotic Discontinuation (FURSAD) study hypothesizes that FR is associated with specific sociodemographic and clinical variables, including sex, marital status, history of alcohol abuse, clinical remission status, age at onset, years of education, baseline Positive and Negative Syndrome Scale (PANSS) score, antipsychotic dosage, and duration of medication discontinuation.
In summary, this FURSAD study aims to characterize patients with schizophrenia who successfully achieved FR after at least 1 year of antipsychotic discontinuation. Utilizing a rigorous retrospective, non-interventional design informed by real-world clinical data, this study further seeks to develop and validate a machine-learning-based clinical decision-making tool to assist clinicians in identifying patients likely to benefit from safe antipsychotic discontinuation. Ultimately, this research aims to facilitate a personalized treatment strategy in schizophrenia, balancing precision maintenance therapy with timely and informed decisions regarding dose reduction or discontinuation.
Methods
The FURSAD study was a retrospective, real-world study (NCT05667961 at ClinicalTrials.gov) that complied with the Helsinki Declaration of 1975, as revised in 2008. The study protocol has been peer-reviewed and published (Lu et al., Reference Lu, Dong, Zhai, Gao, Luo, Feng and Liu2024).
Participants and functioning assessments
Participants were discharged patients from the Shanghai Mental Health Center (SMHC) who met the inclusion criteria: (1) aged 18–65 years, (2) diagnosed with schizophrenia (ICD-10), (3) discontinued antipsychotics for ≥1 year, and (4) provided informed consent. Participants were allocated into the functional remission (FR) group or functional non-remission (FNR) group based on functioning assessments.
FR was assessed using the FROGS scale, a clinician-rated instrument specifically developed to evaluate functional outcomes in schizophrenia (Rouillon et al., Reference Rouillon, Baylé, Gorwood, Lancrenon, Lançon and Llorca2013). The scale includes 19 items and has been increasingly adopted in cross-cultural schizophrenia research (Bošnjak Kuharić et al., Reference Bošnjak Kuharić, Jambrošić Sakoman, Lovrić Makarić, Savić, Papić and Herceg2024; De Page et al., Reference De Page, Palmers, Vandenbussche, Salsac and Titeca2020; Wang, Zhou, Mao, & Qu, Reference Wang, Zhou, Mao and Qu2020).
FR was defined using empirically validated cutoffs for three key dimensions: social functioning ≥33, daily life ≥12, and treatment dimension ≥12 (Boyer et al., Reference Boyer, Richieri, Guedj, Faget-Agius, Loundou, Llorca and Lançon2013; Gorwood, Mallet, & Lancrenon, Reference Gorwood, Mallet and Lancrenon2018). The specific items comprising each FROGS dimension and the scoring details are provided in the Supplementary Methods. These cutoffs have demonstrated robust sensitivity (88.5%) and specificity (81.1%) in identifying patients with satisfactory functional status, using GAF >60 as the gold standard. (Boyer et al., Reference Boyer, Richieri, Guedj, Faget-Agius, Loundou, Llorca and Lançon2013; Gorwood et al., Reference Gorwood, Bouju, Deal, Gary, Delva, Lancrenon and Llorca2019).
Initially, we considered complementing FROGS with the self-reported World Health Organization Quality of Life – Brief Version (WHOQoL-BREF) (Vahedi, Reference Vahedi2010). However, over 90% of participants exceeded the functional recovery threshold on the WHOQoL-BREF, indicating limited discriminative ability. Therefore, FROGS alone was retained as the primary measure of FR, ensuring both reliability and clinical relevance.
Measures
Data were collected from two sources: (1) post-discharge information, primarily gathered through telephone interviews and online questionnaires; and (2) inpatient information, primarily retrieved from the hospital information system (HIS). A detailed overview of the collected variables is provided in Supplementary Table S1.
Structured telephone interviews using standardized questionnaires were conducted by trained evaluators to obtain post-discharge clinical information. To address potential recall bias or limited insight among some patients – who may be unable to accurately recall their treatment course or report their functional status – researchers will, when necessary and with appropriate consent, conduct interviews with both participants and their caregivers. Interviews explored details on antipsychotic maintenance, dose reduction, and discontinuation, as well as the reasons and decision-making process behind discontinuation. This study phase employs the Reasons for Antipsychotic Discontinuation Interview (RAD-I), a semi-structured tool (Matza et al., Reference Matza, Phillips, Revicki, Ascher-Svanum, Kaiser, Stauffer and Kinon2011), to explore the specific reasons for medication discontinuation and identify the primary decision-makers. All evaluators involved had a minimum of 2 years’ experience in clinical research assessment and underwent formal inter-rater reliability training prior to study commencement.
Following the interview, a separate team of trained researchers, blinded to patient grouping, independently reviewed the HIS records to extract detailed inpatient data using a standard approach. The collected data included:
-
• Baseline sociodemographic information, including sex, employment status, marital status, years of education, age at illness onset, and age at last hospitalization;
-
• Clinical characteristics during hospitalization, including total illness duration (from first onset to medication discontinuation), duration of last hospitalization, number of hospitalizations, history of smoking and alcohol use, family history of psychiatric disorders, history of severe physical illness, modified electroconvulsive therapy (MECT), and discharge status (improved/not recovered).
Symptom severity was assessed using the PANSS (Kay, Fiszbein, & Opler, Reference Kay, Fiszbein and Opler1987) and Clinical Global Impression-Severity (CGI-S) scale (Leucht, Reference Leucht2014) as part of the inpatient clinical practice. These scales were administered by psychiatrists from the same clinical research team, all of whom had extensive experience and underwent regular rater-training and inter-rater reliability calibration.
In addition to PANSS-total, PANSS-positive, PANSS-negative, and PANSS-general psychopathology scores, we also included PANSS-6 (sum of P1, P2, P3, N1, N4, and N6) (Hieronymus, Kølbæk, Correll, & Østergaard, Reference Hieronymus, Kølbæk, Correll and Østergaard2021; Kølbæk et al., Reference Kølbæk, Dines, Hansen, Opler, Correll, Mors and Østergaard2021; Østergaard et al., Reference Østergaard, Lemming, Mors, Correll and Bech2016; Østergaard et al., Reference Østergaard, Foldager, Mors, Bech and Correll2018) and PANSS five-factor model (Citrome et al., Reference Citrome, Castelli, Hasebe, Terahara, Faden and Komaroff2024; Fong et al., Reference Fong, Ho, Wan, Siu and Au-Yeung2015; Lançon, Auquier, Nayt, & Reine, Reference Lançon, Auquier, Nayt and Reine2000; Woodward et al., Reference Woodward, Jung, Smith, Hwang, Barr, Procyshyn and Honer2014), consisting of positive symptoms (POS, sum of P1, P3, G9, P6, P5, and G1), negative signs (NEG, sum of N6, N1, N2, N4, G7, N3, and G16), disorganization (DIS, sum of N7, G11, G10, P2, N5, G5, G12, G13, and G15), excitement (EXC, sum of G14, P4, P7, and G8), and emotional distress (EMO, sum of G2, G6, G3, and G4).
-
• Inpatient medication regimen, including antipsychotic types, formulations, and daily dosage standardized to olanzapine equivalents using World Health Organization Defined Daily Dose methodology (Leucht, Samara, Heres, & Davis, Reference Leucht, Samara, Heres and Davis2016), antipsychotic polypharmacy (APP), and concomitant medications.
Blinding and confidentiality
Data collection was blinded with respect to patient group assignments. Each participant received an initial screening number (e.g. T0001), and those who met criteria were assigned study numbers (e.g. G01 for FR, B01 for FNR). Researchers responsible for grouping patients were only provided with basic information (i.e. name, age, sex, contact), while another team of researchers collected HIS data independently, ensuring objectivity and confidentiality.
Statistical analysis
The study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) (von Elm et al., Reference von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke2007) guidelines and the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) (Collins, Reitsma, Altman, & Moons, Reference Collins, Reitsma, Altman and Moons2015). Data analysis was performed using IBM SPSS Statistics Version 27 and R (version 4.4.1) within RStudio (2024.04.2).
Between-group comparisons were conducted using independent samples t-tests for normally distributed continuous variables (mean ± SD), and Mann–Whitney U tests for non-normally distributed data. Effect sizes were reported as Cohen’s d (t-tests) and Rosenthal’s r (Mann–Whitney U tests). Categorical variables were analyzed via Pearson’s χ 2 tests or Fisher’s exact tests when cell counts were <5, with Phi coefficients used as effect-size measures. Variables significantly differing between groups (P < 0.05) were considered potential predictors.
Predictive modeling employed logistic regression, a supervised learning algorithm suitable for binary classification (e.g. disease occurrence, FR occurrence). In clinical predictive modeling, logistic regression establishes a probabilistic relationship between input features and the target variable, predicting the likelihood of an event occurring, with the output representing a probability value between 0 and 1.
Potential predictors were selected using least absolute shrinkage and selection operator (LASSO) regression (glmnet package) (Friedman, Hastie, & Tibshirani, Reference Friedman, Hastie and Tibshirani2010), a regularization technique enhancing model generalizability. Selected predictors were then incorporated into a binary logistic regression model to predict FR after antipsychotic discontinuation. Multicollinearity among predictors was assessed using the variance inflation factor (VIF) (car package) (Fox & Weisberg, Reference Fox and Weisberg2018). Model performance was validated via 10-fold cross-validation (caret package) (Kuhn, Reference Kuhn2008). Discriminative ability was evaluated using receiver operating characteristic (ROC) curves (pROC package) (Robin et al., Reference Robin, Turck, Hainard, Tiberti, Lisacek, Sanchez and Müller2011). Calibration was assessed using calibration plots (rms package). Clinical utility was evaluated using decision curve analysis (rmda package) (Vickers & Elkin, Reference Vickers and Elkin2006). The final prediction model was visualized as a nomogram, providing an interpretable clinical tool to aid psychiatrists in optimizing individualized treatment strategies.
Results
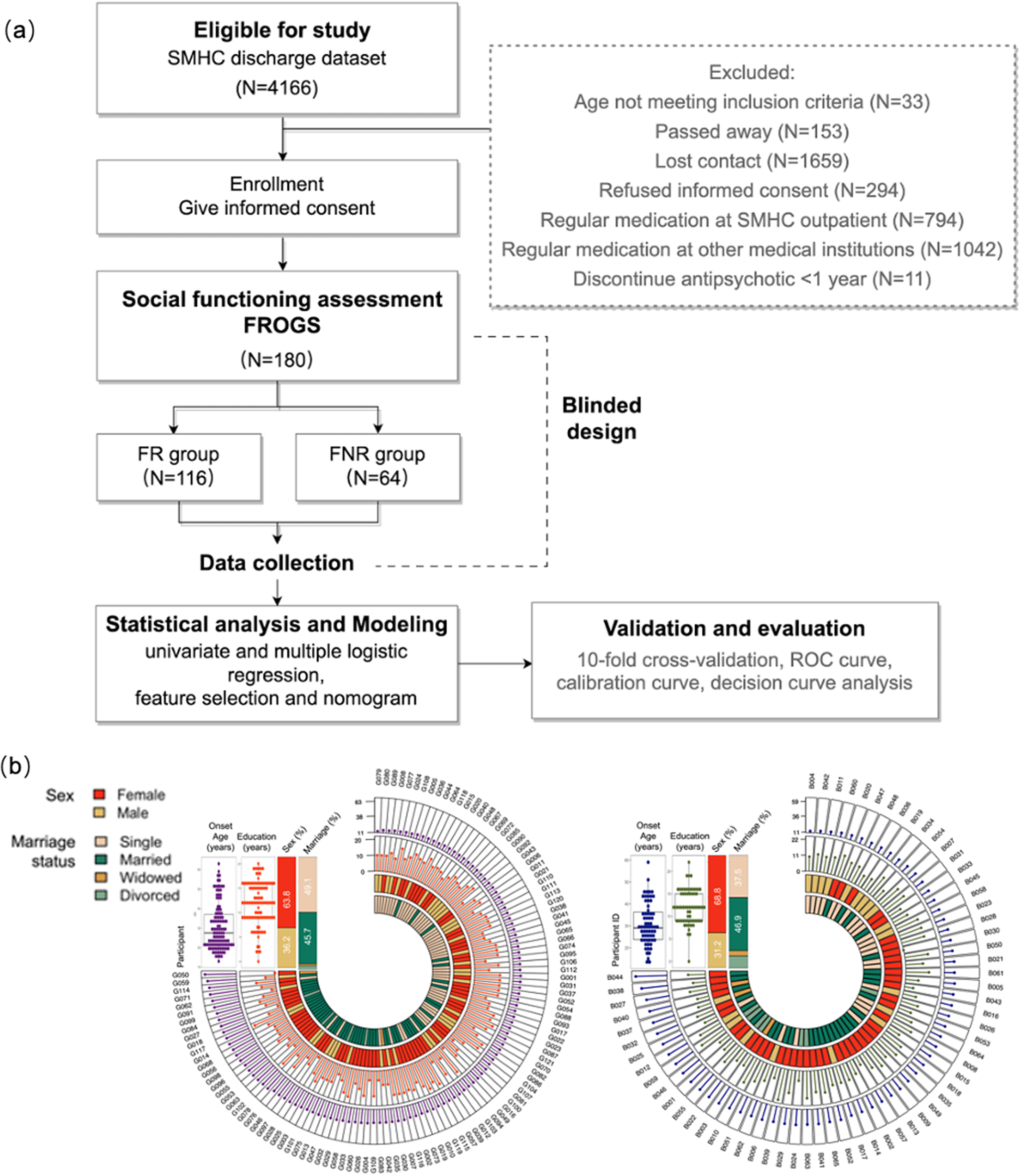
A total of 4,166 discharged patients were initially screened. Of these, 33 did not meet the age criteria, 153 had passed away, 1,659 could not be contacted, and 294 declined participation after contact. Among the remaining individuals, 1,836 were excluded because they continued antipsychotic treatment in outpatient follow-up, and 11 had discontinued antipsychotics for <1 year. Ultimately, 180 patients met the inclusion criteria for ≥1-year antipsychotic discontinuation and were included in the analyses (FR: N = 116; FNR: N = 64). The full screening flow is presented in Figure 1a. Sample size and statistical power calculations are specified in the Supplementary Methods.
(a) Flow chart of the study. (b) Sociodemographic profiles of the FR (left) and FNR (right) group.

Figure 1. Long description
The top panel is a vertical flowchart starting with ‘Eligible for study S M H C discharge dataset N equals 4166’ at the top. Arrows lead downward through ‘Enrollment Give informed consent’, ‘Social functioning assessment F R O G S N equals 180’, then split into ‘F R group N equals 116’ and ‘F N R group N equals 64’. Both groups proceed to ‘Data collection’, then to ‘Statistical analysis and Modeling univariate and multiple logistic regression, feature selection and nomogram’ and ‘Validation and evaluation 10-fold cross-validation, R O C curve, calibration curve, decision curve analysis’. To the right, a dashed box lists exclusions: ‘Age not meeting inclusion criteria N equals 33’, ‘Passed away N equals 153’, ‘Lost contact N equals 1659’, ‘Refused informed consent N equals 294’, ‘Regular medication at S M H C outpatient N equals 794’, ‘Regular medication at other medical institutions N equals 1042’, ‘Discontinue antipsychotic less than 1 year N equals 11’. ‘Blinded design’ is noted between assessment and data collection. The bottom panel has two radial charts. The left chart represents the F R group, the right chart the F N R group. Each chart has three concentric rings: innermost for sex (red for female, yellow for male), middle for marriage status (orange for single, dark green for married, brown for widowed, light green for divorced), and outermost for individual identifiers. Box plots above each chart show onset age and education years, with F R group showing median onset age near 20 and education around 12 years, F N R group with similar distributions. The charts visually compare demographic distributions between groups.
Between-group comparison of characteristics in patients
Figure 1b illustrates the baseline sociodemographic profiles in the FR and FNR groups. No statistically significant differences were observed in age at onset (FR 30.5 ± 11.9 vs. FNR 30.9 ± 9.7), years of education (FR 12.0 ± 4.4 years vs. FNR 12.1 ± 3.8 years), sex (FR 63.8% female vs. FNR 68.8% female), or marital status (single: FR 49.1% vs. FNR 37.5%; married: FR 45.7% vs. FNR 46.9%; widowed: FR 1.7% vs. FNR 4.7%; divorced: FR 3.4% vs. FNR 10.9%).
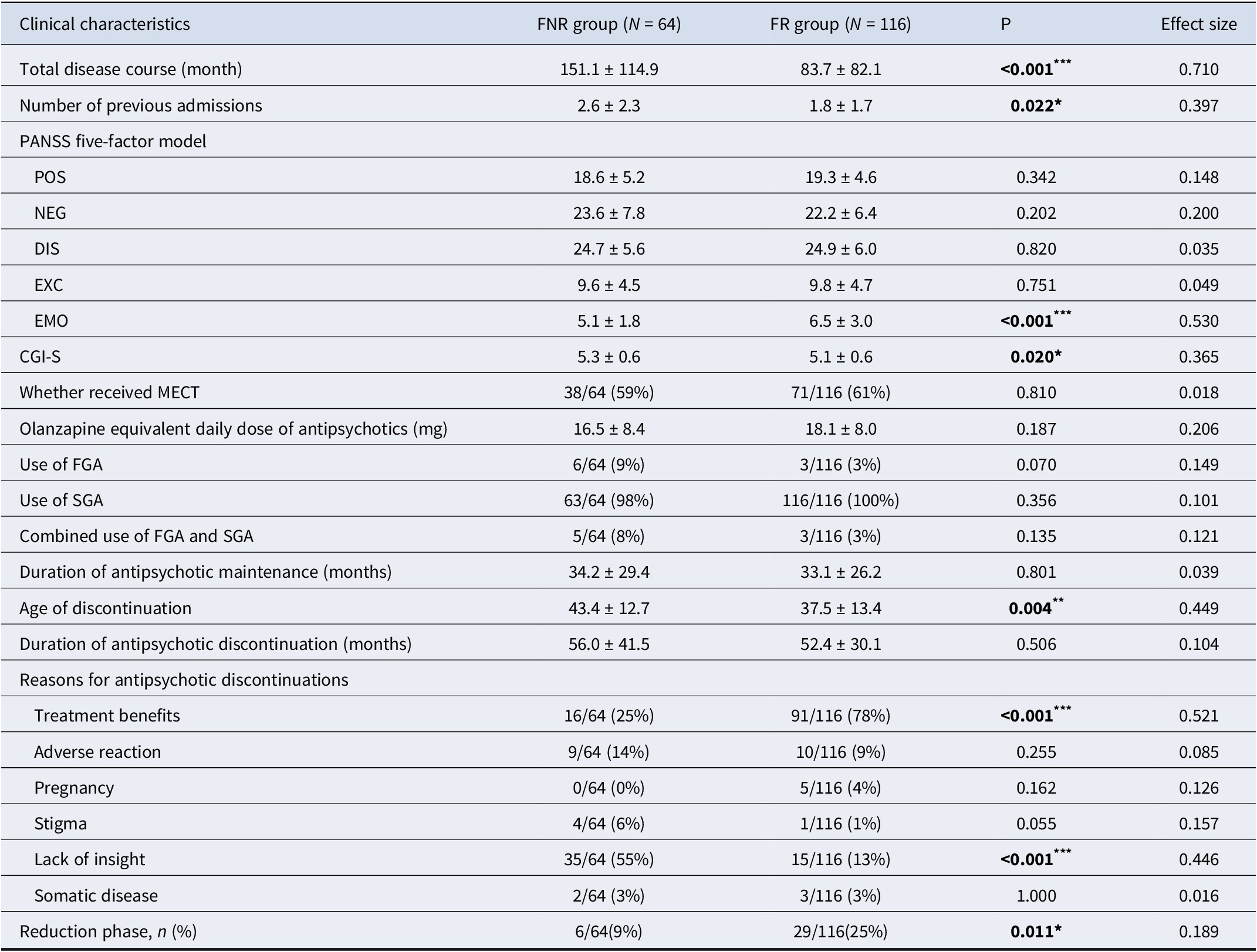
Between-group comparisons were conducted on 54 variables spanning sociodemographic characteristics, clinical characteristics, and symptom severity scores during hospitalization, medication regimens during hospitalization, and patterns of antipsychotic maintenance and discontinuation after discharge. Selected significant characteristics are shown in Table 1 (see Supplementary Tables S2–S6 for complete results).
Clinical characteristics between the FNR and FR groups

Table 1. Long description
The table lists clinical characteristics in the first column, with F N R group data in the second, F R group in the third, P values in the fourth, and effect sizes in the fifth. For total disease course, F N R group shows 151.1 plus or minus 114.9 months, F R group 83.7 plus or minus 82.1 months, P less than 0.001, effect size 0.710. Number of previous admissions: F N R 2.6 plus or minus 2.3, F R 1.8 plus or minus 1.7, P 0.022, effect size 0.397. P A N S S five-factor model subscales: POS, NEG, DIS, EXC, EMO. EMO shows F N R 5.1 plus or minus 1.8, F R 6.5 plus or minus 3.0, P less than 0.001, effect size 0.530. CGI-S: F N R 5.3 plus or minus 0.6, F R 5.1 plus or minus 0.6, P 0.020, effect size 0.365. MECT received: F N R 59 percent, F R 61 percent, P 0.810. Olanzapine equivalent dose: F N R 16.5 plus or minus 8.4 mg, F R 18.1 plus or minus 8.0 mg, P 0.187. Use of F G A: F N R 9 percent, F R 3 percent, P 0.070. Use of S G A: F N R 98 percent, F R 100 percent, P 0.356. Combined F G A and S G A: F N R 8 percent, F R 3 percent, P 0.135. Antipsychotic maintenance duration: F N R 34.2 plus or minus 29.4 months, F R 33.1 plus or minus 26.2 months, P 0.801. Age of discontinuation: F N R 43.4 plus or minus 12.7, F R 37.5 plus or minus 13.4, P 0.004, effect size 0.449. Antipsychotic discontinuation duration: F N R 56.0 plus or minus 41.5 months, F R 52.4 plus or minus 30.1 months, P 0.506. Reasons for discontinuation: treatment benefits F N R 25 percent, F R 78 percent, P less than 0.001, effect size 0.521; adverse reaction F N R 14 percent, F R 9 percent, P 0.255; pregnancy F N R 0 percent, F R 4 percent, P 0.162; stigma F N R 6 percent, F R 1 percent, P 0.055; lack of insight F N R 55 percent, F R 13 percent, P less than 0.001, effect size 0.446; somatic disease F N R 3 percent, F R 3 percent, P 1.000; reduction phase F N R 9 percent, F R 25 percent, P 0.011, effect size 0.189. Statistically significant differences are marked by asterisks, with effect sizes interpreted as small, medium, or large per Cohen's d, Rosenthal's r, or Phi coefficient.
Note: ***P < 0.001, **P < 0.01, and *P < 0.05 indicate statistical significance. Effect sizes: Cohen’s d – small (0.2), medium (0.5), large (0.8); Rosenthal’s r and Phi coefficient – small (0.1), medium (0.3), and large (0.5).
Characteristics of patients with functional remission after antipsychotic discontinuation
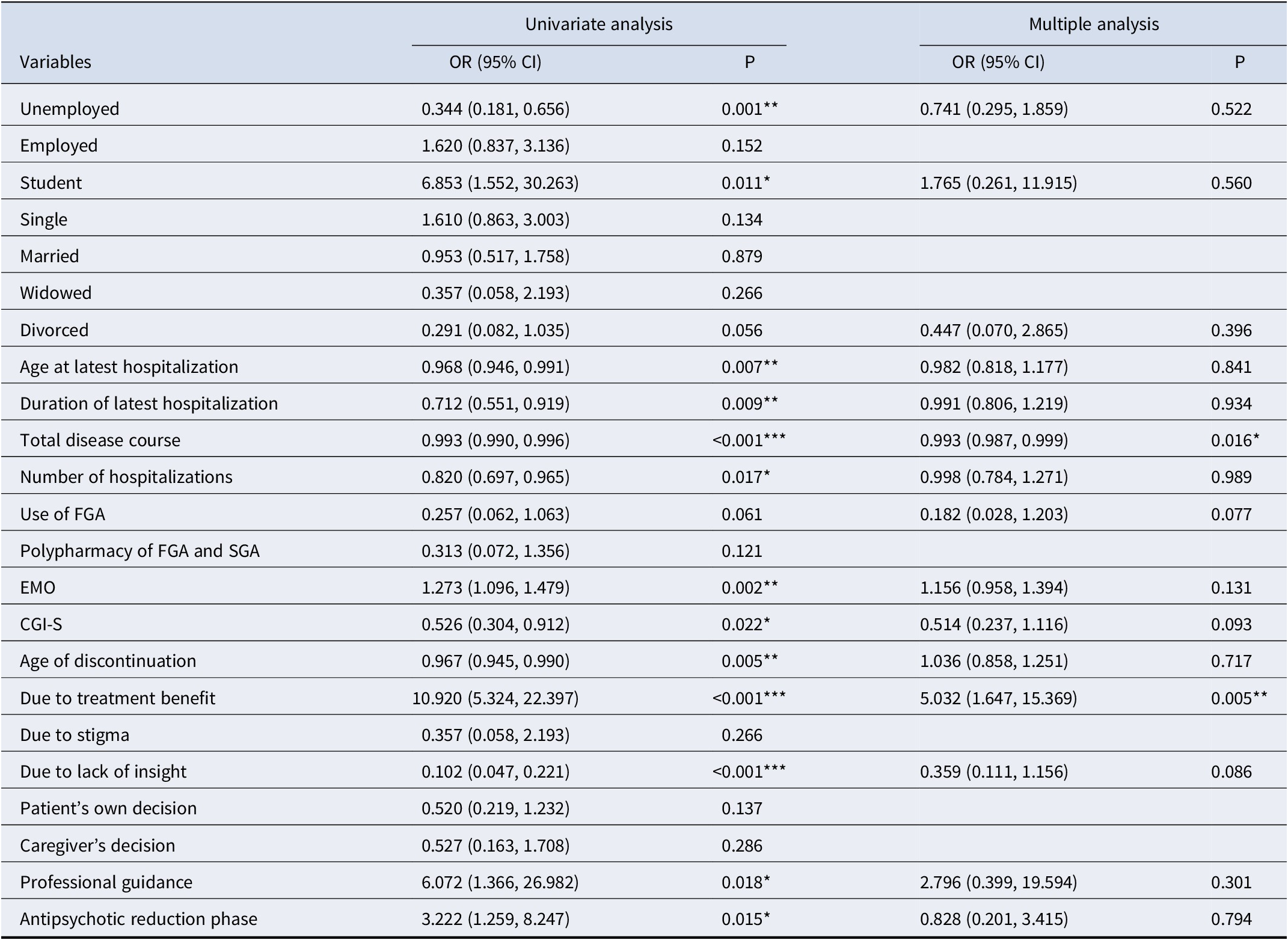
Variables with statistically significant results in between-group comparisons were subsequently analyzed using univariate and multiple logistic regression (Table 2). The univariate logistic analyses identified five protective factors (student, high PANSS-EMO score, antipsychotic discontinuation due to treatment benefits, antipsychotic discontinuation under medical supervision, and having a dose reduction process before discontinuation) and eight risk factors (unemployment, older age at the last admission, longer duration of the latest hospitalization, longer total disease course, more hospitalization times, higher CGI-S score, older age at discontinuation, and antipsychotic discontinuation due to lack of insight) associated with FR after antipsychotic discontinuation.
Influencing factors for functional remission after antipsychotic discontinuation

Table 2. Long description
The table has columns for variables, univariate analysis odds ratio with 95 percent confidence interval, univariate P value, multiple analysis odds ratio with 95 percent confidence interval, and multiple analysis P value. From top to bottom, variables listed are Unemployed, Employed, Student, Single, Married, Widowed, Divorced, Age at latest hospitalization, Duration of latest hospitalization, Total disease course, Number of hospitalizations, Use of F G A, Polypharmacy of F G A and S G A, E M O, C G I dash S, Age of discontinuation, Due to treatment benefit, Due to stigma, Due to lack of insight, Patient’s own decision, Caregiver’s decision, Professional guidance, and Antipsychotic reduction phase. Statistically significant P values are bolded and marked with asterisks: triple asterisk for P less than 0.001, double asterisk for P less than 0.01, and single asterisk for P less than 0.05. Notable significant findings in univariate analysis include Unemployed (O R 0.344, P 0.001), Student (O R 6.853, P 0.011), Age at latest hospitalization (O R 0.968, P 0.007), Duration of latest hospitalization (O R 0.712, P 0.009), Total disease course (O R 0.993, P less than 0.001), Number of hospitalizations (O R 0.820, P 0.017), E M O (O R 1.273, P 0.002), C G I dash S (O R 0.526, P 0.022), Age of discontinuation (O R 0.967, P 0.005), Due to treatment benefit (O R 10.920, P less than 0.001), Due to lack of insight (O R 0.102, P less than 0.001), Professional guidance (O R 6.072, P 0.018), and Antipsychotic reduction phase (O R 3.222, P 0.015). In multiple analysis, only Total disease course (O R 0.993, P 0.016) and Due to treatment benefit (O R 5.032, P 0.005) remain statistically significant. The note states that use of S G A was excluded from univariate analysis due to complete separation, as all individuals in the functional remission group had received S G A.
Note: The variable ‘use of SGA’ was excluded from univariate logistic regression analysis due to complete separation, as all individuals in the functional remission group had received SGA. ***P < 0.001, **P < 0.01, and *P < 0.05 indicate statistical significance.
Multiple logistic analysis revealed that discontinuation due to treatment benefits was an independent protective factor (P = 0.005, OR = 5.032, 95% CI = 1.647–15.369), whereas a longer total disease course was identified as an independent risk factor (P = 0.016, OR = 0.993, 95% CI = 0.987–0.999) for FR after discontinuation.
Establishment and validation of the FURSAD model
Independent predictors with high discriminative value were first screened using LASSO regression (Supplementary Figure S1). Six variables were ultimately included in the final model: total disease course, CGI-S, PANSS-EMO score, use of FGA during maintenance treatment, antipsychotic discontinuation due to perceived treatment benefits, and antipsychotic discontinuation due to lack of insight. VIF values ranged from 1.00 to 1.80, indicating minimal multicollinearity among predictors. The logistic regression coefficients, standard errors, and significance levels for all predictors are provided in Supplementary Table S7.
A binary logistic regression model was developed to predict the probability of FR in patients with schizophrenia after antipsychotic discontinuation. The likelihood ratio test indicated overall statistical significance (χ2 = 78.88, P < 0.0001), suggesting that the selected predictors collectively contributed to outcome variability. The independent variables explained 48.7% of the outcome variance (Nagelkerke R 2 = 0.487). The model also exhibited excellent calibration (Brier score = 0.139, close to the ideal value of 0, indicating good fit).
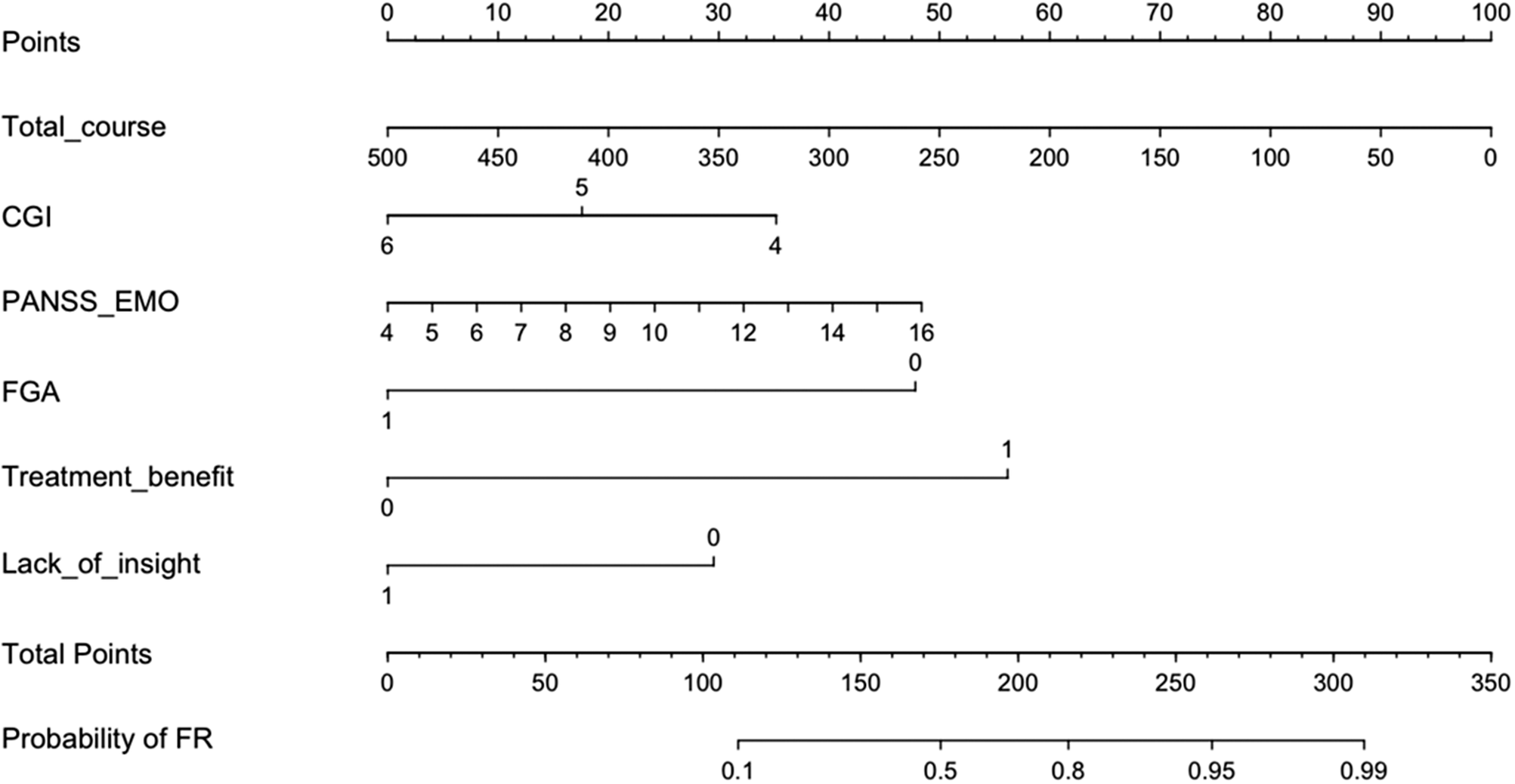
To facilitate clinical interpretation, a nomogram was created based on the logistic regression model (Figure 2). In addition, a dynamic nomogram was developed to demonstrate how the FURSAD model can be applied in specific clinical scenarios for individualized predictions (Supplementary Figure S2). The FURSAD prediction tool has also been developed into a currently accessible online calculator (https://fursad.shinyapps.io/FURSAD_DynNom/). By inputting patient-specific information for the six independent predictors, clinicians can quickly estimate the individual probability of FR approximately 4.5 years after antipsychotic discontinuation, along with 95% confidence intervals.
The FURSAD prediction nomogram. Total_course refers to the total duration of illness (months); PANSS_EMO represents the total score of the emotional distress dimension of the PANSS; FGA indicates prior use of first-generation antipsychotics during the maintenance phase (yes = 1, no = 0); Treatment_benefit refers to antipsychotic discontinuation due to therapeutic benefit (yes = 1, no = 0); Lack_of_insight refers to antipsychotic discontinuation due to lack of insight (yes = 1, no = 0).

Figure 2. Long description
From top to bottom, the nomogram displays: Points scale from 0 to 100; Total_course scale from 500 to 0; C G I scale from 6 to 4; P A N S S underscore E M O scale from 4 to 16; F G A scale from 1 to 0; Treatment_benefit scale from 0 to 1; Lack_of_insight scale from 1 to 0; Total Points scale from 0 to 350; Probability of F R scale from 0.1 to 0.99. Each variable is aligned horizontally, allowing calculation of total points and mapping to relapse probability.
Model performance and clinical utility
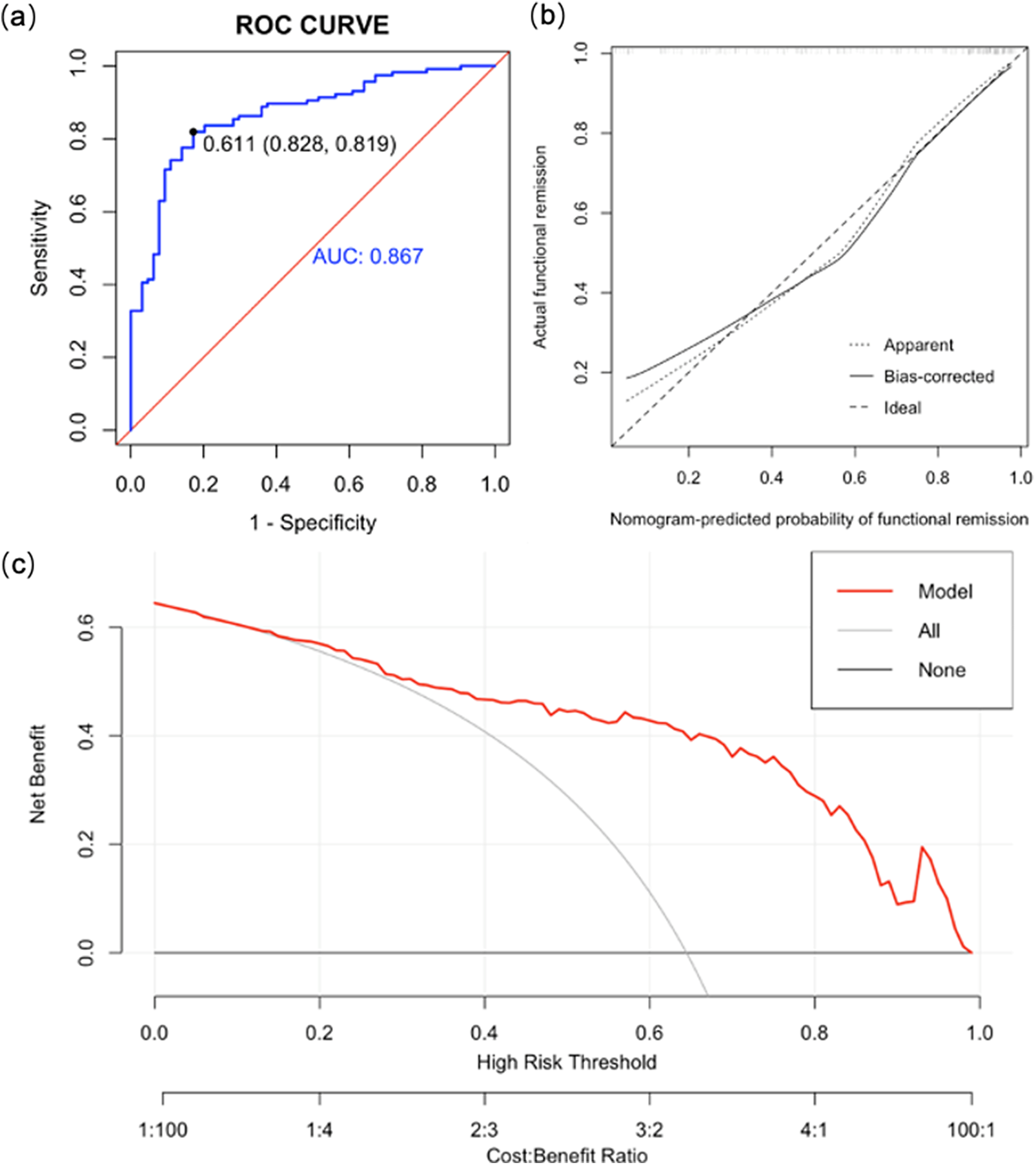
The ROC curve analysis indicated robust discriminative ability, with an area under the curve (AUC) of 0.867 (95% CI: 0.813–0.921), sensitivity of 82.8%, and specificity of 81.9% (Figure 3a). The calibration curves of the nomogram further indicated high predictive accuracy and reliability (Figure 3b). The apparent calibration curve closely approximated the ideal diagonal line, indicating a good fit to the training data with high consistency between predicted and actual outcomes. The bias-corrected calibration curve, representing the model’s generalizability, aligns even more closely with the ideal curve after adjustment, suggesting an improvement in the model’s robustness. Decision curve analysis (DCA) was conducted to evaluate the clinical utility of the predictive model across different risk thresholds (Figure 3c). The results demonstrated that utilizing the model (red line) provides greater net clinical benefit than the default strategies, assuming all (gray line) or no (black line) patients achieve FR, at risk thresholds above approximately 15% (corresponding to a loss-to-benefit ratio of approximately 3:17). Finally, internal validation of the FURSAD prediction model via 10-fold cross-validation yielded an average AUC of 0.843 (95% CI = 0.633–0.964, Supplementary Figure S3), suggesting satisfactory stability and satisfactory generalizability of the model.
(a) ROC curve of prediction model. (b) Calibration curve of prediction model. (c) Decision curve of prediction model.

Figure 3. Long description
Panel a, top-left, is a line graph with x-axis labeled 1 minus Specificity from 0 to 1 and y-axis labeled Sensitivity from 0 to 1. The ROC curve is shown in blue, rising steeply then leveling, with a diagonal red reference line. A black point marks 0.611 with confidence interval 0.828, 0.819. The blue text A U C 0.867 is at lower right. Panel b, top-right, is a calibration curve with x-axis labeled Nomogram-predicted probability of functional remission from 0 to 1 and y-axis labeled Actual functional remission from 0.2 to 1. Three lines are shown: dotted for Apparent, solid for Bias-corrected, dashed for Ideal. The solid line closely follows the diagonal. Panel c, bottom, is a decision curve with x-axis labeled High Risk Threshold from 0 to 1 and Cost to Benefit Ratio from 1 to 100 to 100 to 1. The y-axis is Net Benefit from 0 to 0.6. Three lines are shown: red for Model, gray for All, black for None. The red line starts high and decreases, gray curves downward, black remains flat at zero. Legend at top right of panel c identifies line colors.
Discussion
To the best of our knowledge, the FURSAD study is the first to develop a nomogram specifically aimed at predicting FR in individuals with schizophrenia following antipsychotic discontinuation. After systematically examining multiple factors potentially associated with FR, we identified key prognostic determinants, emphasizing the roles of discontinuation motives and the characteristics of the disease course in shaping long-term functional outcomes. Participants in the study had maintained antipsychotics for approximately 3 years before discontinuation and remained off medication for an average of 4.5 years at assessment.
The prevalence of FR after antipsychotic discontinuation remains debated. In this study, 64.4% of patients achieved FR, whereas 35.6% did not. Prior studies reported widely varying remission rates, ranging from as low as 25% in a 10-year follow-up study by Wils et al. (Reference Wils, Gotfredsen, Hjorthøj, Austin, Albert, Secher and Nordentoft2017) to 29% in the cohort study by Üçok & Kara (Reference Üçok and Kara2020). These discrepancies likely stem from methodological differences, diverse inclusion criteria, and heterogeneity in patient characteristics.
Our findings align with existing evidence suggesting that longer illness duration correlates with declining cognitive and social adaptation, thereby reducing the likelihood of functional remission (Dahlan et al., Reference Dahlan, Midin, Shah, Nik Jaafar, Abdul Rahman, Baharudin and Sidi2014; Lipskaya-Velikovsky, Kotler, Easterbrook, & Jarus, Reference Lipskaya-Velikovsky, Kotler, Easterbrook and Jarus2015; van Dee, Schnack, & Cahn, Reference van Dee, Schnack and Cahn2023). Additionally, higher CGI-S scores at admission, reflecting greater global illness severity, were linked to poorer functional outcomes post-discontinuation, consistent with prior reports that acute symptom burden predicts later psychosocial functioning (Burton et al., Reference Burton, Tso, Carrión, Niendam, Adelsheim, Auther and McFarlane2019; van Dee, Schnack, & Cahn, Reference van Dee, Schnack and Cahn2023; Wu et al., Reference Wu, Ye, Li, Wu, Wang, Yuan and Xiao2022).
Discontinuation motivated by perceived treatment benefit emerged as a strong protective factor. This aligns with evidence that symptomatic remission is closely tied to improvements in daily functioning, social participation, and health service utilization (Helldin et al., Reference Helldin, Kane, Karilampi, Norlander and Archer2007). Conversely, lack of insight was identified as a significant risk factor for impaired functional recovery, in line with extensive clinical and epidemiological research (Chong et al., Reference Chong, Siu, Kwan, Chang, Lee, Chan and Lo2018; Escobedo-Aedo et al., Reference Escobedo-Aedo, Forjan-González, Sánchez-Escribano Martínez, Ruiz-Ruano, Sánchez-Alonso, Mata-Iturralde and Lopez-Morinigo2022). A meta-analysis of 42 studies (N = 4,562) confirmed that better baseline insight predicts superior social functioning (van Dee, Schnack, & Cahn, Reference van Dee, Schnack and Cahn2023). Patients with preserved insight demonstrate greater illness awareness and stronger self-management capacities, allowing them to detect early relapse signs and seek timely intervention even after discontinuation.
Use of FGAs during maintenance treatment was negatively associated with FR. This finding aligns with real-world prescribing patterns, in which FGAs are rarely used (only 5% in our sample) and typically reserved for clinically complex or treatment-resistant cases. Prior evidence also indicates higher EPS risk with FGAs compared with SGAs (Carbon, Kane, Leucht, & Correll, Reference Carbon, Kane, Leucht and Correll2018; Monteleone et al., Reference Monteleone, Cascino, Rossi, Rocca, Bertolino, Aguglia and Maj2022) and more progressive gray-matter loss in FGA-treated patients relative to those treated exclusively with SGAs in longitudinal MRI studies (Vita et al., Reference Vita, De Peri, Deste, Barlati and Sacchetti2015). Together, these data suggest that FGA use may serve as a proxy for underlying illness severity or chronicity, helping explain its association with reduced FR.
Interestingly, a higher score on the PANSS emotional distress dimension (PANSS-EMO) also predicted FR. Although seemingly counterintuitive, prior studies suggest that emotional symptoms may facilitate aspects of personal recovery, such as connectedness, hope, self-identity formation, meaning, and empowerment (Best, Law, Pyle, & Morrison, Reference Best, Law, Pyle and Morrison2020; Leamy et al., Reference Leamy, Bird, Le Boutillier, Williams and Slade2011). Emotional awareness may motivate active symptom management, help-seeking, and engagement with social and clinical resources. Large cohort studies similarly indicate that emotional symptoms can be predictive of functional improvement (Law, Shryane, Bentall, & Morrison, Reference Law, Shryane, Bentall and Morrison2016; Petkari et al., Reference Petkari, Salazar-Montes, Kallert, Priebe, Fiorillo, Raboch and Cervilla2011), supporting the integration of emotional distress assessments into personalized treatment strategies.
Strengths and limitations
Real-world retrospective studies on antipsychotic discontinuation strike an optimal balance between scientific rigor and ethical feasibility, addressing key limitations of RCTs, which typically represent only a subset (~20%) of patients in routine clinical practice (Taipale et al., Reference Taipale, Schneider-Thoma, Pinzón-Espinosa, Radua, Efthimiou, Vinkers and Luykx2022). The FURSAD study employs a blinded design for group allocation and assessment, enhancing methodological robustness. By relying on routinely collected clinical information, the model allows for rapid and practical risk estimation. Furthermore, rigorous internal validation ensures the model’s stability and reliability, minimizing overfitting risks.
Nonetheless, several limitations should be considered. First, our subjects were recruited from a single specialized medical center. While comprehensive inpatient clinical data ensures reliability, the studied population may exhibit greater illness severity and treatment complexity than community-based cohorts. Additionally, requiring successful telephone follow-up for participants may introduce sampling bias, as participants with higher treatment engagement and educational attainment are more likely to complete the follow-up. Patients lost to follow-up, who are likely to present with more severe clinical profiles or poorer treatment adherence, may be underrepresented, which can affect the model’s broader applicability.
Furthermore, symptom severity during inpatient care is inherently dynamic, and the PANSS and CGI-S ratings used in this study, although obtained at a standardized time point within the first 3 days of the last hospitalization, may not fully capture fluctuations across the entire inpatient course. This reliance on early-stage inpatient symptom severity introduces an additional methodological limitation.
To mitigate potential follow-up bias, we adopted two strategies. First, we ensured comparability between the FR and FNR groups in terms of illness onset, year of antipsychotic discontinuation, and follow-up duration, thereby minimizing variation in both the maintenance and discontinuation periods. Second, discontinuation duration was included as a covariate in the regression model; analyses revealed no significant group differences in maintenance or cumulative discontinuation durations, indicating balanced disease-course-related variables across groups and thus reducing potential bias in model predictions.
Conclusions
The FURSAD study underscores the critical role of discontinuation motives and illness trajectory on long-term functional outcomes in patients diagnosed with schizophrenia. The resulting nomogram facilitates shared decision-making by enabling clinicians to estimate the individualized likelihood of achieving FR 4.5 years after treatment cessation, especially among patients treated with antipsychotics for approximately 3 years who are contemplating discontinuation. Future investigations should employ large-scale, multicenter prospective designs in real-world clinical contexts. Broader, multicenter studies conducted in diverse real-world settings will further refine predictive models through larger sample sizes and robust external validation cohorts, ultimately supporting personalized clinical decision-making in the management of schizophrenia.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0033291726104024.
Acknowledgments
The authors would like to thank Dr. Hua Jin (University of California, San Diego) for his suggestions on the study design.
Author contribution
Conceptualization: C.L., Y.D., D.L.; Investigation: Y.D., Z.Z., T.G., M.L., D.C., J.C., J.X., Y.Z., X.M., Z.W.; Methodology: C.L., T.F.; Supervision: D.L.; Writing – original draft: C.L., Y.D., Writing – review and editing: C.L., Y.D., Z.Z., T.G., M.L., D.C., J.C., J.X., Y.Z., X.M., Z.W., Q.X., X.L., T.F., D.L.
Funding statement
This work was sponsored by the MSD China Investigator Initiated Studies Grant (#100154). It was also supported by the National Natural Science Foundation of China (82371504), Shanghai Science and Technology Innovation Project (23ZR1454700), Shanghai Mental Health Center Specific Disease Cohort Study Project (2025-SFDL01), and the Shanghai Mental Health Center Project (2024-YJ06, 2025-YJ01). The founders had no role in the study design, analysis, or in the writing of the report or the decision to submit the report for publication.
Competing interests
The authors declare no competing interests related to this work.
Declaration of AI usage
AI-assisted language tools were used only for English language editing. All research content, including study design, analyses, and interpretation, was produced by the authors, who remain fully responsible for the manuscript.



 Open access
Open access