


Introduction
Care of the injured patient has made great strides in recent decades. This is due in part to the proliferation of trauma centers, advances in evidence-based care, and improved oversight and standardization from organizations such as the American College of Surgeons (ACS; Chicago, Illinois USA). Prehospital care is at the forefront of current interest due to potential for significant improvements in patient outcomes. Much emphasis is placed on the “Golden Hour,” or the idea that providing appropriate care in the initial hour after injury can have significant impacts in minimizing harm. Reference Clark1 This focus has sparked an increase in contemporary research aimed at unraveling the relationships between transportation methods, durations, and patient outcomes. Reference Rudman, Fritz and Thomas2 As the field advances, understanding how these variables intersect is essential for optimizing prehospital protocols.
Previous studies frequently correlate worse morbidity and mortality with longer trauma transport times, Reference Harmsen, Giannakopoulos, Moerbeek, Jansma, Bonjer and Bloemers3–Reference Boland, Lu, Silver, Byrd, Guyette and Brown9 though others suggest these effects may vary by patient group. Reference Björkman, Setälä, Pulkkinen, Raatiniemi and Nurmi10 It remains an open question to what extent prehospital providers should “stay-and-play” or “scoop-and-run;” these decisions are confounded injury severity, distance from the trauma center, and local Emergency Medical Services (EMS) capabilities. Reference Nirula, Maier, Moore, Sperry and Gentilello11–Reference Haas and Nathens13
Similarly, studies demonstrate increased survival odds with helicopter transport for some patient populations due to more advanced care, faster transport, and access to resources not available on ground ambulances. Reference Schneider, Ewing and Cull14–Reference Elkbuli, Dowd, Sanchez, Shaikh, Sutherland and McKenney27 Other studies show mixed results or no improvement. Reference Galvagno, Sikorski and Hirshon28–Reference Talving, Teixeira and Barmparas31 The decision to utilize Helicopter Emergency Medical Services (HEMS) over Ground Emergency Medical Services (GEMS) is a complex triage process influenced by more than just injury severity. Clinicians and first responders must weigh pros, such as the potential for advanced on-board critical care and the ability to bypass geographic obstacles, against cons, such as weather constraints, the significant cost differences between modalities, and the regional saturation of HEMS assets. These considerations have prompted the development of triage algorithms and scores. Reference Brown, Smith and Gestring32–Reference Brown, Forsythe, Stassen and Gestring36
The purpose of this study was to examine the effects of both timing and mechanism of transport on the outcomes of traumatically injured patients presenting to a Level-1 trauma center in St. Louis, Missouri (USA). Aspects of prehospital trauma care that may be improved to increase survival of traumatic injury are highlighted. Finally, potential steps to improve outcomes of this patient population are presented.
Methods
A retrospective analysis was performed using the trauma registry of a Level-1 trauma center within the city of St. Louis, which includes all adult trauma patients who presented to this center. The trauma registry is maintained and updated by the institution with a combination of automated and manual chart review, storing demographic, injury, intervention, and outcome data from all trauma patients for research and quality improvement purposes. This study was approved by the Saint Louis University IRB (St. Louis, Missouri USA) Protocol Number 32759. All patients between the ages of 18-99 who presented from January 2019 through January 2022 (three years) were screened for this study.
The study includes one of the two urban Level-1 trauma centers in St. Louis City. It serves as a major hub for the St. Louis metropolitan area and a large rural catchment area spanning eastern Missouri and southern Illinois. This setting provides a distinct contrast in transport dynamics: GEMS primarily handles high-volume, short-distance urban calls – often involving penetrating trauma – where transport times are frequently under 30 minutes. There are several EMS providers that serve the region, each with varying requirements and competencies. Conversely, HEMS assets in this region are typically utilized for long-distance transfers or scene responses in rural regions where ground transport to a definitive care center would take prohibitively long. These crews typically carry advanced paramedics or flight nurses, and often have access to medications and procedures not available on GEMS, such as blood products and tranexamic acid.
Information gathered included age, race, sex, location, time, and mechanism of injury, housing status, mode of transportation to hospital, trauma activation level, whether a patient had signs of life upon arrival, and discharge location (including morgue). All data used in this study were de-identified. Patients with missing necessary data were excluded for a full-case analysis; it was assumed that data were missing completely at random, and that this exclusion did not impact results or conclusions.
Due to the several confounding variables in the helicopter versus ambulance study, a propensity matching study was performed. Propensity matching attempts to minimize confounding variables between patient groups by statistically identifying similar patients. Here, as the ambulance group was significantly larger than the helicopter group, a 2:1 matching was performed to match patients by injury severity as determined by Injury Severity Score (ISS), Trauma and Injury Severity Score (TRISS), prehospital vitals, injury type, trauma level, and transport time. Matching was performed with the PsmPy Python package (Python Software Foundation; Wilmington, Delaware USA). Reference Kline and Luo37 Variable similarity before and after matching is determined by the standardized mean difference (SMD), where SMD > 0.3 is considered a large difference.
The primary outcome is survival to hospital presentation. Secondary outcomes are survival to hospital discharge, intensive care unit (ICU) length-of-stay, and hospital length-of-stay. The secondary outcomes are only calculated in the subgroup that survived to hospital presentation. Fisher’s exact test Reference Fisher’s Exact Test38 was performed to assess the significance of categorical outcomes; the independent two-sided t-test was used for continuous outcomes. The statistical analysis was pre-specified to account for multiple hypothesis testing. The single primary outcome was assessed with a significance level set at P < 0.05. To account for statistical multiplicity and minimize the chance of Type-1 error, P values of secondary outcomes are adjusted by the Benjamini-Hochberg procedure. Reference Benjamini and Hochberg39 A secondary finding was considered statistically significant if its adjusted P value was < 0.05. The widths of the 95% confidence intervals (CI) have not been adjusted for multiplicity, and these intervals should not be used in place of hypothesis testing. SciPy Reference Virtanen, Gommers and Oliphant40 (Python Software Foundation) and ROOT Reference Antcheva, Ballintijn and Bellenot41 (CERN; Geneva, Switzerland) are the statistical and graphical tools used.
Results
A total of 5,160 patients during this timeframe required a trauma team activation. Only patients transported from the scene of injury were considered; transfers from outside hospitals were excluded. Patients transferred from outside facilities were a large subgroup – a total of 2,403 (46.6%) patients – worth investigating. However, this paper solely examined prehospital care; care received at outside hospitals provided a confound beyond the scope of this manuscript.
After excluding transfers and patients with missing data, a total of 1,702 patients were included in the analysis. A full trauma team response (Level 1) was required for 854 (50.1%) patients, while the rest required a partial trauma team response (Level 2). Injury mechanisms were divided into blunt (eg, motor vehicle accidents and falls [898; 65.4%]) and penetrating (eg, gunshot and stab wounds [475; 34.6%]). Of the Level-1 patients, 99 (11.5%) presented dead on arrival to the trauma bay. No Level-2 patients were dead on arrival. Of all patients (Level 1 and Level 2) who presented with signs of life (1,603), 86 (5.4%) did not survive to hospital discharge.
Transportation Method
In the analysis of method of transportation, patients who were not transported by EMS and instead arrived by another method such as private vehicle or police were excluded, as they did not receive at least EMS-level prehospital care. Of the 1,373 patients included, 124 (9.0%) were transported by HEMS and 1,249 (91.0%) were brought in by GEMS.
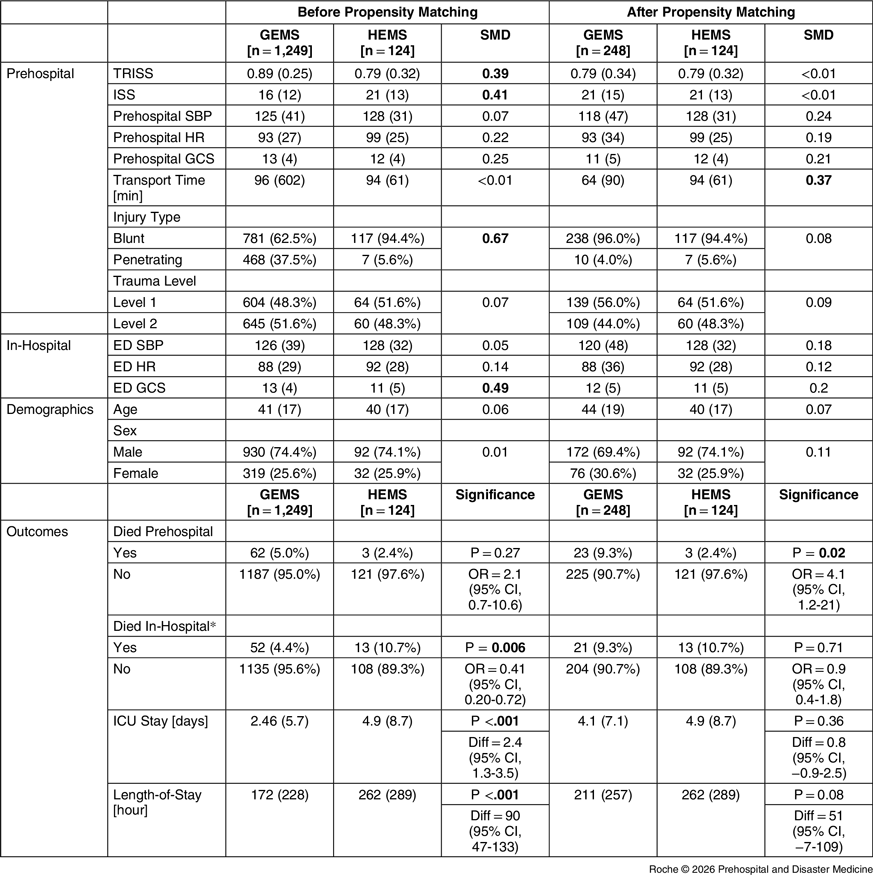
Table 1 reports the results for the two groups. Patients flown to the hospital via helicopter on average suffered worse injuries when compared to those transported by ambulance, noted by higher ISS (SMD = 0.41) and lower survival probability by TRISS (SMD = 0.39). Ambulances transported a higher proportion of patients with penetrating injury (SMD = 0.67), likely due to the trauma center’s location in the city, near most penetrating trauma. Differences in prehospital vital signs, transport times, and trauma activation level were small between the two groups.
Ambulance versus Helicopter Group, Before and After 2:1 Propensity Matching

Note: Significance of secondary outcomes are adjusted by the Benjamini-Hochberg method, as noted in the methods section. Confidence intervals of secondary outcomes are unadjusted and should not be used for hypothesis testing.
* Percentage calculated out of patients who survived to hospital presentation.
Abbreviations: HEMS, Helicopter Emergency Medical Services; GEMS, Ground Emergency Medical Services; SMD, standardized mean difference; TRISS, Trauma and Injury Severity Score; ISS, Injury Severity Score; SBP, systolic blood pressure; HR, heart rate; GCS, Glasgow Coma Scale; ED, emergency department; ICU, intensive care unit.
Despite including higher-acuity patients, patients transported by helicopter had similar rates of prehospital death as patients transported by ambulance. However, patients transported via helicopter had a significantly higher rate of in-hospital death (GEMS OR = 0.41; 95% CI, 0.20-0.72). Additionally, patients transported by helicopter on average spent longer in the ICU (by 2.4 days; 95% CI, 1.3-3.5) and hospital (by 90 hours; 95% CI, 47-133).
To account for the differences in injury severity and mechanism between groups, a 2:1 GEMS:HEMS propensity matching was performed. This yielded a total of 248 patients in the ambulance group and the original 124 in the helicopter group. Prehospital values reported in Table 1 were used for matching to account for the differences in injury type and severity. After propensity matching, there was no significant difference in TRISS and ISS. However, patients transported by GEMS had a markedly shorter transport time (SMD = 0.37). The propensity-matched ambulance cohort had a higher risk of prehospital death (OR = 4.1; 95% CI, 1.2-21) but similar risk of in-hospital death and comparable ICU and total hospital lengths-of-stay.
Transportation Time
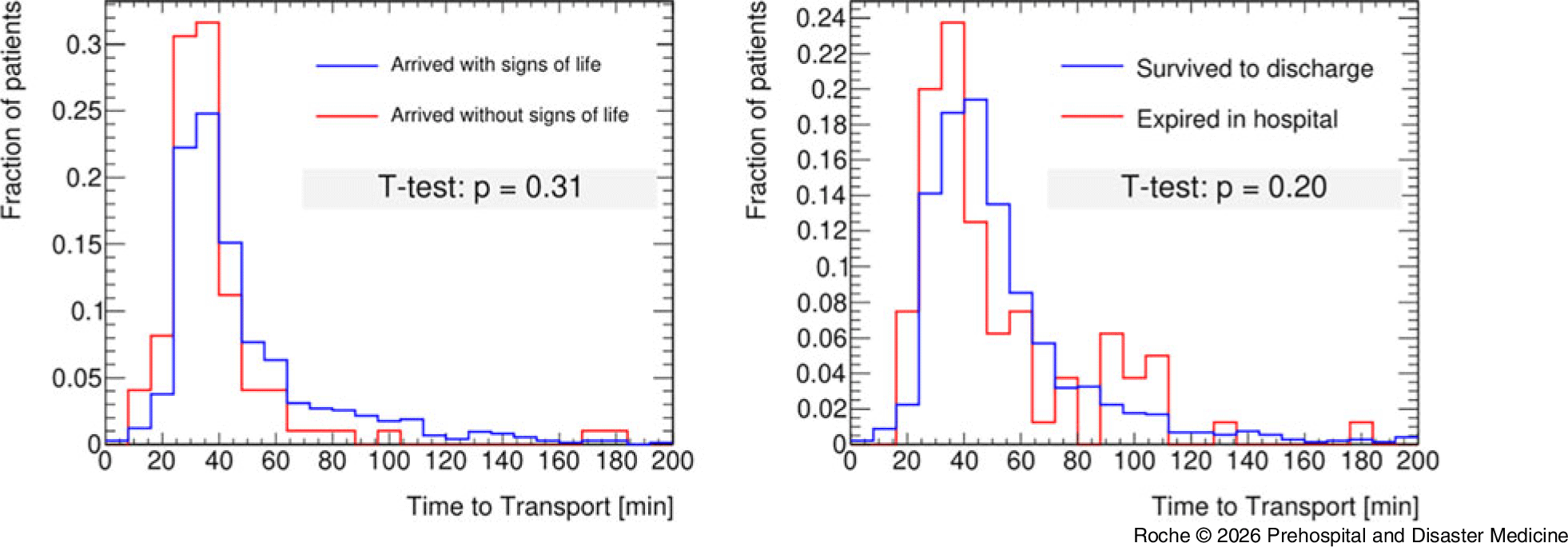
Patients with any transportation method were included in this analysis, including those from private vehicle. Figure 1 (left) compares the transport times of Level-1 patients who were declared dead on arrival (99; 11.5% [average minutes = 38 (24)]) to those who arrived with signs of life (755; 88.5% [average minutes = 49 (29)]). No significant difference in time between injury and arrival was found between these groups (P = 0.31). Figure 1 (right) compares the transport times of patients who survived to discharge (1,517; 94.6% [average minutes = 52 (28)]) to those who presented with signs of life but expired before discharge (86; 5.4% [average minutes = 50 (30)]). No significant difference in time between injury and arrival was found between these groups (P = 0.20).
Transport Times for Level 1 Patients Who Died Prehospital and Those Who Survived to Hospital Presentation (left).
Note: Of all patients (Level 1 and Level 2) who survived to hospital presentation, the prehospital transport times between those who survived to discharge are presented alongside those who did not (right).

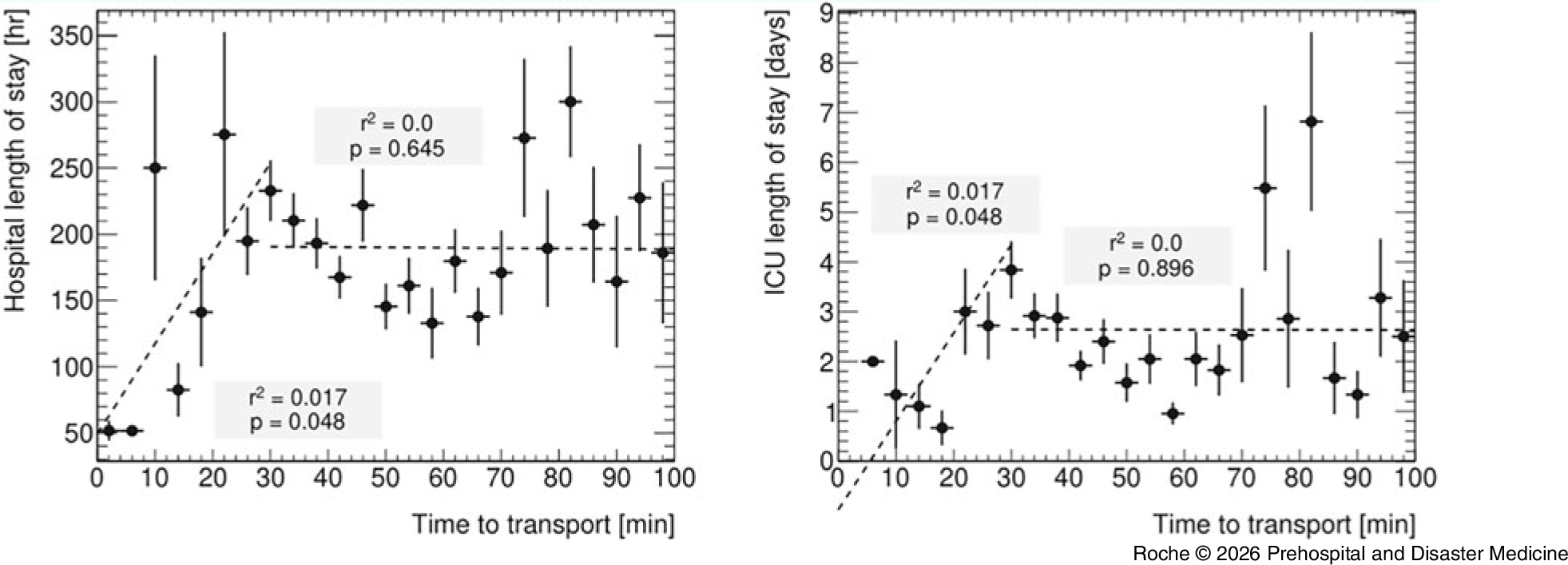
The effect of transport time on hospital stay time was examined. Figure 2 shows the hospital (left) and ICU (right) lengths-of-stay versus transport time. Two-part linear regression fits were performed for each: one for transport times between zero and 30 minutes, and one for >30 minutes. Both total hospital and ICU lengths-of-stay showed a positive correlation with transport times up to 30 minutes (P = 0.05; r2 = 0.02). For transport times >30 minutes, there was no significant correlation for either.
Time to Transport Plotted Against Hospital Length-of-Stay (left) and Total ICU Days (right) with a Two-Part Piecewise Linear Fit.
Note: Horizontal error bars represent bin width; vertical error bars represent standard deviation.

Discussion
Optimizing the survival of Level-1 trauma patients requires an effective transition from the field to the trauma center, where prehospital variables can play a role in patient outcomes. Here, the effects of transportation method and time are considered.
Transportation Method
Regarding transportation method, previous studies have demonstrated improved outcomes for some patient groups with HEMS, likely due to a combination of quicker transport time for far distances, more access to advanced resources not available in GEMS, and frequent exposure to critically ill patients. Reference Schneider, Ewing and Cull14–Reference Elkbuli, Dowd, Sanchez, Shaikh, Sutherland and McKenney27 In this analysis, patients transported to the trauma center via HEMS are on average more severely injured than those transported by GEMS, contributing to poorer in-hospital outcomes for that group before propensity-matching. After matching to account for the differences in injury severity, patients transported by helicopter were more likely to survive to presentation at the trauma center. However, with a small number of prehospital deaths in the HEMS group (3) and a wide odds ratio confidence interval (1.2-21), this should be interpreted cautiously. In addition, after presentation to the trauma center, outcomes between the two groups are similar. This may indicate that the decreased prehospital mortality in the HEMS group represents either a delayed mortality or earlier arrival rather than true improvement in long-term outcomes.
The implications of these results are open to interpretation and inspire further hypotheses. Choosing when to use helicopters for transport over ground ambulances is an imperfect science, highly dependent on the resources and needs of the system, along with the local patient population. Further complicating this is the fact that studies have shown variable benefit for HEMS in different subgroups. For instance, individual studies have indicated that more severely injured patients (measured by ISS) Reference Brown, Stassen, Bankey, Sangosanya, Cheng and Gestring42 may benefit more, while patients with traumatic brain injury Reference Di Bartolomeo, Sanson, Nardi, Scian, Michelutto and Lattuada43 may not. There also exist conflicting studies: in one, the young adult subgroup (18-54 years) experienced more benefit, Reference Sullivent, Faul and Wald26 whereas in another, the subgroup aged older than 55 years derived greater clinical gain. Reference Andruszkow, Schweigkofler and Lefering44
Therefore, targeted triage is essential to balance these limitations with the needs of patients, prompting the development of algorithms and scores. Reference Brown, Smith and Gestring32–Reference Brown, Forsythe, Stassen and Gestring36 Despite this, multiple trauma programs report inappropriate triage. Reference Brown, Smith and Gestring32,Reference Brown, Forsythe, Stassen and Gestring36,Reference Thomas and Biddinger45–Reference Horwood, Ricci, Sobol, Evans and Eiferman52 Inappropriate triage has not been specifically studied at this trauma center, and therefore, it is unclear how optimally helicopters are being utilized.
Transportation Time
In the second aspect of this analysis, shorter transport times do not correlate with increased survival, either to arrival or to hospital discharge. However, shorter transport times correlate with shorter ICU and hospital stays when less than 30 minutes. The clinical significance of this finding is tempered by the small effect size, with transport time explaining only approximately two percent (r2 = 0.02) of the variance in these outcomes. The high degree of unexplained variance suggests that patient physiology, injury mechanism, and in-hospital care remain the primary drivers of outcome, regardless of transport speed. For transport times greater than 30 minutes, there was no significant difference in outcomes as time increased. The 30-minute threshold was selected to distinguish direct urban scene-to-hospital transports from more prolonged intervals, as literature suggests prehospital intervention impact often shifts significantly beyond the 20-to-30-minute range. Reference Pusateri, Moore and Moore53 This bifurcation allowed to isolate transport efficiency within the window where the “Golden Hour” benefits are theorized to be most potent. The lack of correlation observed beyond 30 minutes may suggest a plateau effect where outcomes become primarily driven by initial injury severity and in-hospital management rather than marginal gains in transit speed. These results underscore that the relationship between transport duration and trauma recovery is non-linear and highly complex. It is likely that individual systems will need to assess their needs, rather than uniformly adhering to the increasingly controversial “Golden Hour.” Reference Lerner and Moscati54,Reference Rogers, Rittenhouse and Gross55
One major question is whether more time spent intervening in the prehospital setting improves outcomes. It appears that for patients near the trauma center, when transport times can be kept under 30 minutes, a shorter transport time may correlate with improved outcomes. This argues in favor of the “scoop-and-run” approach for this group, though further research will be necessary to truly elucidate optimal strategies. For patients requiring prolonged EMS activity, recent advances to prehospital care may further improve the bridge to care. For instance, prehospital blood transfusion has been shown in several studies to improve outcomes, and programs doing so have been successfully implemented. Reference Pusateri, Moore and Moore53,Reference Braverman, Smith and Ciaraglia56–Reference Crombie, Doughty and Bishop64 Similarly, prehospital tranexamic acid administration may yield benefits. Reference Ramirez, Spinella and Bochicchio65–Reference Guyette, Brown and Zenati68
Limitations
This study is isolated to a single urban trauma center, limiting generalizability of these results. Further studies with expanded regional or national datasets and randomized trials are necessary to determine exactly which policies are best. Furthermore, this dataset lacked granular data on geographic distance from the trauma center, rural versus urban origin of the call, and the specific composition of the transport crews (for instance, Basic Life Support versus Advanced Life Support). Similarly, different EMS organizations may have different scopes of practice or protocols that result in varying levels of care available. It was also not available in the dataset how much prehospital time was spent in the ambulance: a patient who spent 25 minutes awaiting ambulance arrival followed by a five-minute drive to the hospital would be recorded as having the same transportation time as a patient who spent five minutes awaiting an ambulance followed by a 25-minute drive to the hospital.
In addition, though propensity matching was employed to limit confounders, several inherent limitations of this retrospective registry analysis must be acknowledged. Notably, transport time remained imbalanced after matching, with the ambulance cohort experiencing significantly shorter durations. Because helicopter assets are selectively deployed for patients at greater distances or those perceived by scene providers to be more critically ill, confounding by indication cannot be entirely eliminated. Consequently, the associations observed between transport modality and survival to presentation should be interpreted as correlative rather than causal, as unmeasured variables such as specific prehospital interventions or environmental constraints may have influenced these outcomes.
Finally, these results cannot be extrapolated to include inter-facility transfers. Whether immediate transport to a distant tertiary trauma center is better than GEMS transportation to a local community hospital followed by transfer is an interesting question, though outside the purview of this paper. In addition, care should be taken when extrapolating these results to other regions. Different trauma centers have different criteria for helicopter transport, as well as different catchment regions and varying levels of EMS skill.
Conclusions
For severely injured patients, narrowing the time and intervention gap between injury and hospital-level care has the potential to save lives. In this retrospective analysis of a single urban Level-1 trauma center, helicopter transport was associated with improved survival to hospital arrival, though no significant difference was observed in in-hospital mortality. While transport times under 30 minutes showed a correlation with reduced hospital and ICU lengths-of-stay, no significant association was found between transport time and overall survival. These findings are limited by the study’s retrospective nature, single-center scope, and the lack of data on specific EMS protocols and environmental constraints. Consequently, these results should be viewed as a limited contribution to the growing body of research on this topic, further highlighting a need for multi-center, prospective research to further clarify the impact of transport modality and timing on trauma outcomes.
Authorship Contributions
STR: Data analysis, paper writing, and editing.
KD: Data acquisition, IRB approval, paper writing, and editing.
HW: Data acquisition, IRB approval, paper writing, and editing.
MT: Data acquisition, paper writing, and editing.
HI: Data analysis, paper writing, and editing.
VM: Study design, paper writing, and editing.
CB: Study design, paper writing, and editing.
Use of AI Technology
No AI tools were used in construction of this manuscript.
Conflicts of interest
None of the authors have any conflicts to disclose

 Open access
Open access