


Introduction
Sustainable Development Goals (SDGs) address sustainability, health, well-being, social justice, environmental protection, economic development, and governance (Acharya et al. Reference Acharya, Lin and Dhingra2018; SDSN 2013). Within this framework, human health and well-being play a critical role as the main foundations of overall sustainable growth and development (Acharya et al. Reference Acharya, Lin and Dhingra2018; Stenberg et al. Reference Stenberg, Hanssen, Edejer, Bertram, Brindley, Meshreky and Rosen2017). Health and well-being are closely interrelated, and can be understood together as a state of complete good physical, mental, and social conditions leading to happiness and good quality of life (Fischer et al. Reference Fischer, Fung, Cave, Fischer-Bonde and González2022; Giles-Corti et al. Reference Giles-Corti, Lowe and Arundel2020; Sartorius Reference Sartorius2006; WHO 1946, 2014a, 2014b, 2020). In this context, health is used from here on for simplicity to refer to both health and well-being. Social, economic, and environmental factors influence and often determine both health and well-being outcomes (Anna Tarkington et al. Reference Tarkington, Denotti, Parker and Krylova2021; Barata et al. Reference Barata, Kinney, Dear, Ligeti, Ebi, Hess and Dickinson2018).
Global socio-economic disparities and environmental injustice have been associated with poorer health outcomes and vice versa (Kahn Reference Kahn2015; Greszczuk et al. Reference Greszczuk, Giles Alison, Graff Hannah, Modi, Jane and Greszczuk2019). Socio-economic determinants such as transportation, housing, and sanitation influence daily behaviors and exposure to pollutants/pathogens, impacting health outcomes (Ehrlich et al. Reference Ehrlich, Kemper, Pesaresi and Corbane2018; Fischer et al. Reference Fischer, Fung, Cave, Fischer-Bonde and González2022). Environmental determinants like air and water quality, noise, and access to green spaces have established health impacts (WHO and Government of South Australia 2018; Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019; Tan et al. Reference Tan, Chiu and Ren Ai2023). Additionally, human rights to access healthcare and, thereby, health outcomes are significantly influenced by economic security, education, social inclusion, and governance (Lowe et al. Reference Lowe, Adlakha, Sallis, Salvo, Cerin, Moudon and Higgs2022; Hogan et al. Reference Hogan, Stevens, Hosseinpoor and Boerma2018; Manderscheid et al. Reference Manderscheid, Ryff, Freeman, McKnight-Eily, Dhingra and Strine2010; Tan et al. Reference Tan, Chiu and Ren Ai2023; UNICEF et al. 2021). Poor health can reduce overall life satisfaction, limit opportunities, worsen inequality (Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019; Sartorius Reference Sartorius2006; WHO 2014c), and impact social cohesion and economic productivity (Giannakeas et al. Reference Giannakeas, Bhatia, Warkentin, Bogoch and Stall2020; UNICEF et al. 2021; Walker et al. Reference Walker, Whittaker, Watson, Baguelin, Winskill, Hamlet and Djafaara2020).
The above interrelations and interlinkages are captured explicitly in SDG 3, “good health and well-being,” and recognized in other SDGs (e.g., SDG 6 “clean water and sanitation,” SDG 10 “reduced inequalities,” SDG 11 “sustainable cities and communities,” or SDG 13 “climate action”). They demonstrate the need for integrated health policy and planning to support societal resilience, economic security, and environmental protection (Manderscheid et al. Reference Manderscheid, Ryff, Freeman, McKnight-Eily, Dhingra and Strine2010; Tan et al. Reference Tan, Chiu and Ren Ai2023; WHO 2023a). This is particularly pressing in urban areas, where 66% of the world’s population now resides and where the interrelations discussed above are magnified (Zinkernagel et al. Reference Zinkernagel, Evans and Neij2018). Urban agendas need to ensure health-inclusive planning across all sectors to support healthy livelihoods and equitable and resilient communities (Barata et al. Reference Barata, Kinney, Dear, Ligeti, Ebi, Hess and Dickinson2018; Global Taskforce of Local and Regional Governments 2016; WHO 2023b).
Achieving health goals, including those within the SDGs, depends highly on national, regional, and local governance in preparing legislative measures, policies, and strategies for implementation (Global Taskforce of Local and Regional Governments 2016; OECD 2023; Rozhenkova et al. Reference Rozhenkova, Allmang, Ly, Franken and Heymann2019). In the context of frameworks that foster human health and well-being, policy development and implementation are complex because they entail cross-sector and cross-party governance for effective environmental and social protection measures and infrastructure development (WHO 2014c). This implies coordinated policies that systematically and effectively integrate health considerations across sectors and a commitment to implementation (Glass and Newig Reference Glass and Newig2019; Local Government Association 2016; Rudolph et al. Reference Rudolph, Caplan, Ben-Moshe and Dillon2013).
In light of the above considerations, this paper applies a systematic, quantitative policy mapping method to explore the integration of health considerations over time in Indonesia from the country’s independence in 1945 to 2024. The main objective is to assess the extent to which the country’s governing efforts have supported health integration into national policy and sectoral development agendas. Policy mapping enables a comparative analysis of initiatives across time, domains, and contexts, and as such, findings may inform future policies and plans (Helms and Biggs Reference Helms and Biggs2007).
This paper also maps governance actors (e.g., government departments and development agencies) to enable the exploration of horizontal and vertical integration (Bainbridge et al. Reference Bainbridge, Potts and Gerard O’Higgins2011) and, thus, of relative coordination of efforts. The examination of the evolution of national policies’ consideration of health is situated within and interpreted through the broader socio-political contexts in Indonesia. This is done to explore and understand the underlying aspects that may have influenced policy development decisions and uncover any particular agendas (Rozhenkova et al. Reference Rozhenkova, Allmang, Ly, Franken and Heymann2019).
Indonesia is the largest economy in Southeast Asia and an important trade region (World Bank 1979, 1994, 2022). The country held the G20 presidency of the International Economic Cooperation Forum in 2022, where it agreed to more actively contribute to global economic recovery commitments through three interconnected pillars: global health architecture, sustainable energy transition, and digital transformation (Jütten Reference Jütten2022). The first of these pillars is central to enhancing human health in the country and supports Indonesia’s progress toward SDG achievement. Given its strategic location, economic growth, and agreed commitments, Indonesia presents an exemplary case study to explore policy patterns toward the global objective of good health and well-being (SDG 3). The following section describes the policy mapping approach, advanced in this research through the use of a quantitative method based on studies in other research areas (e.g., Allen et al. Reference Allen, Pilar, Walsh-Bailey, Hooley, Mazzucca, Lewis and Mettert2020; Walt et al. Reference Walt, Shiffman, Schneider, Murray, Brugha and Gilson2008). The results of the policy mapping are then discussed against the contextual socio-political background before drawing concluding remarks and recommendations.
Methodology
Policy mapping is a review technique that enables the establishment of an overview of policy evolution, integration, and coordination. It entails a systematic analysis of the content of legislation, administrative regulations, and formal policy statements at national, regional, local, and/or city levels (Bowen et al. Reference Bowen, Irish and Lightfoot2022; Van Kessel et al. Reference Van Kessel, Czabanowska and Roman-Urrestarazu2023; Scott et al. Reference Scott, Wagenaar, Swanson, Ibrahim, Wood and Mello2010). The approach adopted here is grounded in agenda-setting theory, which postulates that policy attention is reflected in the visibility and recurrence of issues within authoritative documents. Kingdon’s multiple-streams framework, which suggests that the sustained presence of issues in formal policy discourse signals their recognition as policy problems requiring governmental action, is noteworthy here. This is further reinforced by punctuated equilibrium theory, which demonstrates that longitudinal patterns in policy texts can capture shifts in institutional attention and priorities (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Baumgartner and Jones Reference Baumgartner and Jones1993). In this research, the frequency of policy documents and keyword references is used as a proxy for institutional salience, indicating the degree to which health is embedded within policy agendas over time. While keyword frequency does not directly measure policy implementation or effectiveness, it provides a transparent, replicable, and comparative indicator of agenda prominence and policy recognition. Prior policy mapping studies demonstrate that sustained and repeated references to concepts such as health reflect their institutionalization within governance systems and their relevance to evolving policy priorities (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Baumgartner and Jones Reference Baumgartner and Jones1993; Buijs et al. Reference Buijs, Gulsrud, Rodela, Diduck, van der Jagt and Raymond2024).
Data collection
The official date of Indonesia’s independence, August 17, 1945, when national policy development commenced, was chosen as the starting point for policy mapping. All policy documents were downloaded from the publicly accessible online database of Indonesia’s Directorate General of Legislation.Footnote 1 (Direktorat Jenderal Peraturan Perundang-undangan or DJPP). A total of 1,481 out of 1,525 national laws still effective as of May 5, 2024, were available for download and, therefore, included in this study. 44 policy documents could not be included due to their inaccessibility. In an attempt to address this and mitigate data gaps, missing policy documents were searched for in other potential sources (e.g., legislating organization websites), without success. While acknowledging this is a data gap that could potentially affect research outcomes, arguably, their small number (less than 3% of total documents) does not significantly affect the main objective of this study: establishing patterns of integration of health and well-being into Indonesia’s policy agendas.Footnote 2 All policy documents were in Bahasa, Indonesia’s official language.
Policy mapping indicators
The policy mapping was based on a systematic search of a set of predetermined keywords. Keyword selection was founded on the links between SDG health targets and key global health policy-making and sustainable urban development frameworks. Policy mapping assumes that repeated occurrence and prioritization of concepts in formal legislation reflect institutional salience and evolving governmental attention (Arnold et al. Reference Arnold, Beauchamp and Bowie2014). Frequency of documents and keyword references serves as a proxy for the degree to which health concerns are embedded within the policy agenda, providing a measurable link between policy discourse and political focus over time (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Baumgartner and Jones Reference Baumgartner and Jones1993). While frequency does not measure implementation directly, it offers a robust, replicable indicator of agenda prominence for what governments recognize as salient issues. High frequency of terms like “health” suggests institutional embedding and sustained policy attention (Baumgartner and Jones Reference Baumgartner and Jones1993).
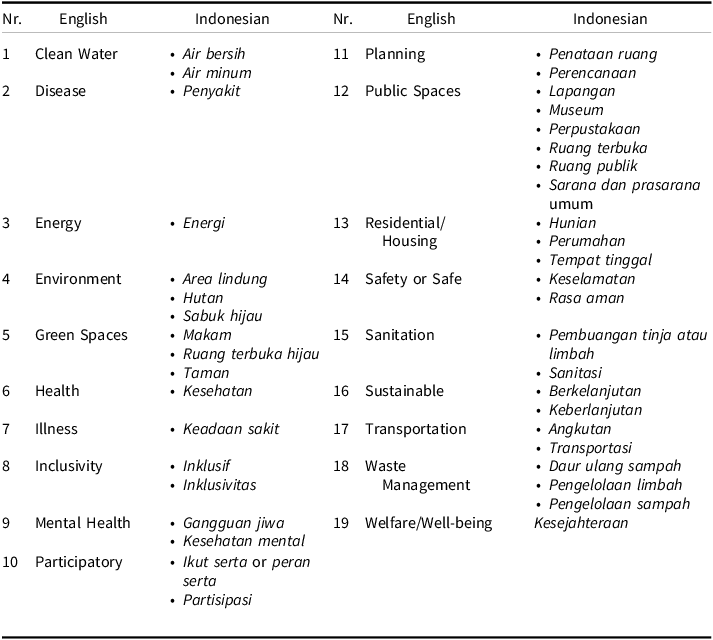
These key global frameworks included Health in All Policies (HiAP) (Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019), the New Urban Agenda (NUA) (Giles-Corti et al. Reference Giles-Corti, Lowe and Arundel2020; UN 2016), and the International Organization for Standardization (ISO 2018, 2019a, 2019b) compliance for sustainable, innovative, and resilient cities (Table 1). This comparative approach enabled the identification of common or closely related objectives across the global frameworks addressing health determinants and health outcomes pertaining to local (urban) implementation of health measures (Global Taskforce of Local and Regional Governments 2016; Leavesley et al. Reference Leavesley, Trundle and Oke2022). This was important as global goals require and rely on local action, as noted earlier. Subsequently, nineteen consistent common keywords were identified in this cross-comparison of SDG, HiAP, NUA, and ISO objectives, which reflect important health determinants and outcomes.
Selected keywords for the policy mapping (in alphabetical order)

Indicators translation to context
The quantitative policy mapping was based on keyword frequency counts in the available policy documents using NVIVO software, version 1.7.2. Every NVivo keyword finding was reviewed to cross-check its relevance; this was necessary to address linguistic complexities. The keyword analysis is not intended as a semantic or discourse analysis but as a structured agenda-mapping technique that combines quantitative frequency with qualitative relevance coding.
To ensure methodological robustness, the keyword-based policy mapping followed a structured validation process. First, keywords were not selected arbitrarily but derived through cross-mapping between SDG health targets and the established global frameworks, noted earlier: HiAP, the NUA, and ISO standards. This ensured conceptual validity and policy relevance. Second, synonyms and linguistic variations were systematically accounted for, including historically consistent Indonesian terms (e.g., “welfare” and “well-being,” both translated as kesejahteraan), as well as sector-specific expressions embedded within legislation. For example, kesehatan in Indonesian can mean different things other than health, like “resilient,” “transparent,” “stable,” and “soundness” in monetary systems or state-and regional-owned enterprises (e.g., sistem keuangan yang sehat, kesehatan bank, kesehatan keuangan). Third, contextual accuracy was ensured through a relevance classification process, whereby each keyword occurrence was manually coded as directly related, closely related, or distantly related (as further detailed below) to the policy’s substantive objectives. This step prevented the misinterpretation of incidental or symbolic mentions as policy priorities. Keyword frequency provides a transparent and replicable proxy for agenda salience and institutional attention, consistent with established agenda-setting theory and policy analysis literature.
The selected 19 English keywords are associated with 41 Indonesian Bahasa keywords and direct synonyms that encompass historical wording adjustments (Table 2). The old spelling and use of the selected keywords were identified, and any contemporary words with the same meaning were included as appropriate. This was done to optimize the analysis by minimizing global policy concept/term translation issues. Including all of the equivalent Indonesian keywords helped ensure maximum correlation and more robust policy mapping analysis in the specific context of Indonesia.
Selected keywords for the policy mapping in English and Indonesian
Analysis and classification of keyword frequencies
Keyword findings were analyzed across four dimensions: temporal patterns of policy attention, thematic framing, relative relevance, and institutional responsibility. Rather than treating socio-political context as an abstract construct, the study operationalizes it through measurable characteristics of policy production and discourse, consistent with agenda-setting and policy dynamics literature (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Baumgartner and Jones Reference Baumgartner and Jones1993). Keyword frequency was quantified through counts across time periods, relevance categories, themes, and governance actors. Policy documents were grouped into five-year intervals between 1945 and 2024 to align with Indonesia’s electoral cycles, a standard approach in longitudinal policy analysis for capturing shifts in political leadership and governance priorities.
While one full term of office in Indonesia is five years, this time grouping does not always reflect an exact period of power or regime. Governments have previously run for more than two terms (e.g., Soeharto, 1968–1998) or remained for less than a full term (e.g., Abdurrahman Wahid, 1999–2001). Nevertheless, this time grouping facilitated the identification and analysis of the historical socio-political contexts behind the formulation of policies and the consideration of health in those policies.
The keyword findings were also categorized based on their relative relevance or relatedness. This distinction reflects differences between symbolic recognition, operational commitment, and peripheral acknowledgment of health issues, a differentiation commonly used in policy content analysis to assess agenda salience beyond mere mention (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Bowen et al. Reference Bowen, Irish and Lightfoot2022) (see supplementary material for the full list), as follows:
-
• Directly related: The policy document’s title or a given policy or appendix therein specifically refers to one or several keywords (e.g., the title includes the word “health” and/or “disease management”).
-
• Closely related: The keyword(s) is mentioned in policy elements such as finance and budget allocations for health. This suggests that, while the issue may not be captured as a policy priority, it plays a significant part in policy implementation.
-
• Distantly related: The keyword(s) is mentioned in policy elements but is not relevant to the policy itself (e.g., keywords such as inclusivity or sustainability only being included in the law’s preamble, because it is a fundamental yet general part of the law).
Policy themes were identified using the classifications provided in Indonesia’s Directorate General of Legislation databaseFootnote 3, which reflect the government’s priority sectoral and development areas (e.g., health, economy, transportation, internal affairs). Structuring the policy mapping around these themes enabled a systematic assessment of how health is integrated across government agendas and sectors.
In addition to temporal and thematic grouping, the governance actors responsible for policy development were identified to assess institutional commitment and coordination in implementing international and national policy objectives. Shifts in health-related legislation and institutional responsibility were interpreted as indicators of changing governance capacity and political prioritization, consistent with prior studies linking institutional arrangements to policy effectiveness and agenda stability (Baumgartner and Jones Reference Baumgartner and Jones1993; Rudolph et al. Reference Rudolph, Caplan, Ben-Moshe and Dillon2013).
In this study, structured integration is defined as the explicit and recurring incorporation of health objectives across policy texts, sectors, and governance levels, as opposed to ad hoc or crisis-driven references. Together, the dimensions of time, thematic framing, relevance, and institutional responsibility provide a structured, replicable framework for examining how socio-political contexts shape the evolution of health within national policy systems. Agenda-setting theory posits that the frequency and prominence of policy concepts within official documents reflect governmental attention and prioritization over time (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Baumgartner and Jones Reference Baumgartner and Jones1993). From this perspective, repeated references to health-and well-being-related terms signal their salience within the policy agenda, while sudden increases correspond to agenda-refocusing events such as economic crises or public health emergencies. In parallel, multilevel governance theory provides the conceptual basis for examining how policy attention is distributed and coordinated across national, provincial, and local levels (Glass and Newig Reference Glass and Newig2019; Hooghe and Marks Reference Hooghe and Marks2003). In this study, the HiAP framework is adopted as an applied governance lens to assess the extent to which health considerations are systematically integrated across sectors and governance scales (WHO 2014a). These theoretical elements collectively justify quantitative policy mapping as an empirical approach to assessing policy attention, integration, and coherence over time.
Consideration of socio-political contexts
Indonesian government’s policy formulation is greatly influenced by political conditions, security considerations, global issues, and national interests (Russell Reference Russell2020; Sulistyo Reference Sulistyo2002; Ulum Reference Ulum2020). Therefore, analyzing Indonesia’s policy mapping results against national socio-political contexts, also taking into account global movements and challenges, enables an understanding of policy trajectories. More specifically, this approach provides insights on how historical events, governance structures, and/or national interests may have shaped policy decisions over time. In particular, the patterns and shifts of influencing factors shaping Indonesia’s policy-making can stem from a specific period’s political and governance landscape. For example, the centralization of governance through policies such as Law 5/1974 concerning the principles of regional government (Ministry of State Secretariat 1974) derived from security concerns (e.g., separatist movements in Aceh and Papua) and political control. The historical context, in this particular example, helps explain why many policies of Soeharto’s were authoritarian and Java-or urban-centric (Anwar Reference Anwar1999). The consideration of historical socio-political contexts also helps in understanding how past decisions impact current and future policies.
Together, these analytical steps establish a structured evaluation framework comprising four dimensions: (1) the volume and temporal distribution of health references; (2) the depth of their policy integration, assessed through keyword relatedness; (3) their sectoral embedding across government policy domains; and (4) the governance levels responsible for policy formulation. Each dimension is operationalized through specific quantitative indicators and reported systematically in the results section.
Results
Scope and temporal distribution of national policy documents on health and well-being
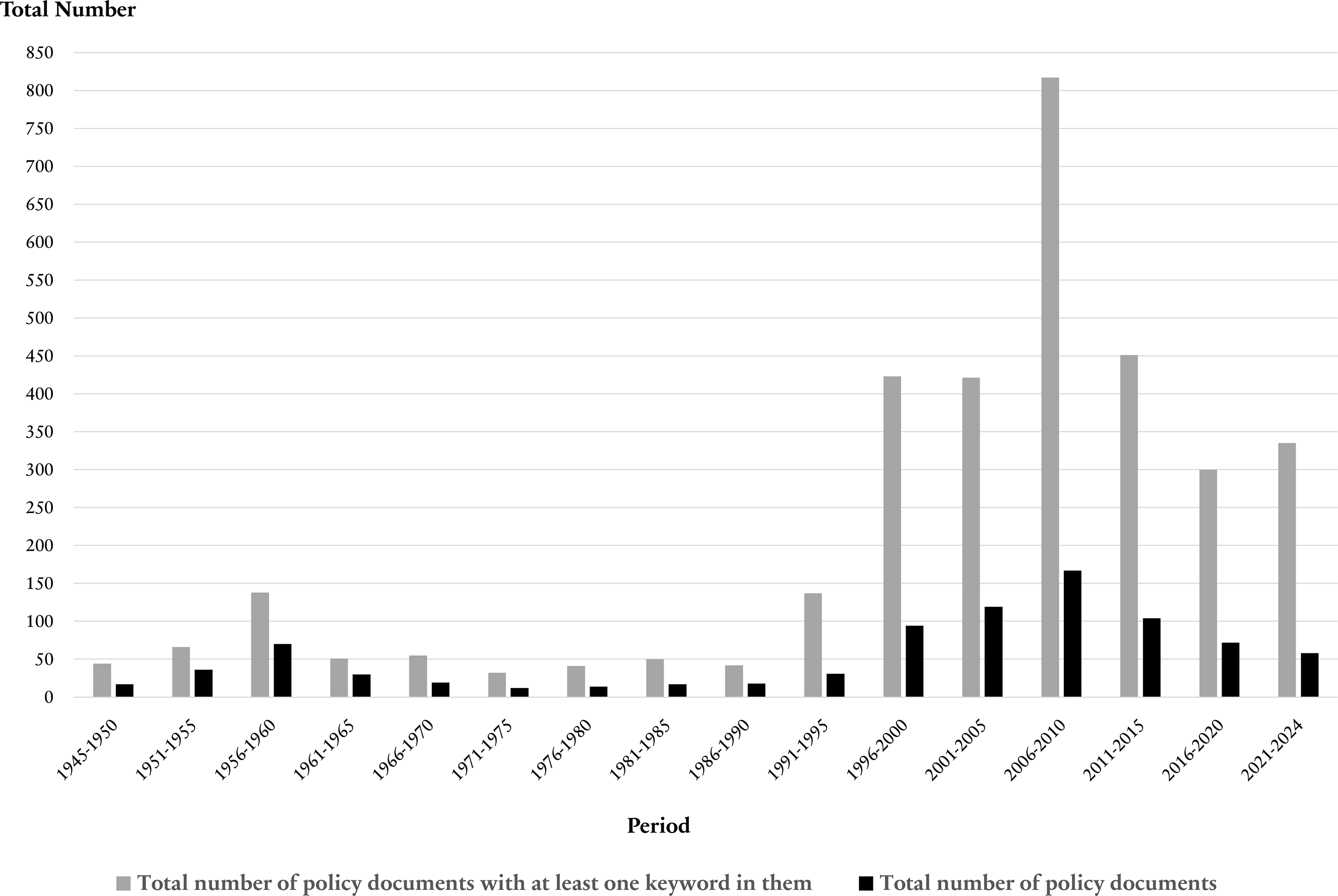
This section evaluates the volume and temporal distribution of health-and well-being-related legislation, capturing the extent to which these issues are present in national policy discourse over time. From the 1,481 policy documents reviewed, only 878 include one or more of the keywords searched (59%). This indicates that, interestingly, a significant proportion of the policy documents do not address health considerations (603 policies or 41%). Through the keyword search process, it was apparent that some policy documents are more health-centric, as they appear a significant number of times. For example, Law 17/2023 concerning health (Ministry of State Secretariat 2023b) contains the keywords “health,” “well-being,” “residential/housing,” “sanitation,” “sustainable,” “energy,” “waste management,” “clean water,” and others. As a result, the 878 relevant policy documents led to 3,402 repeated policies; that is, documents were duplicated for analytical purposes, according to the number of keywords found (Figure 1). The keyword search revealed a total of 26,054 keyword finds; this value is used as the total keyword frequency for the subsequent analysis.
Total policy documents analyzed.
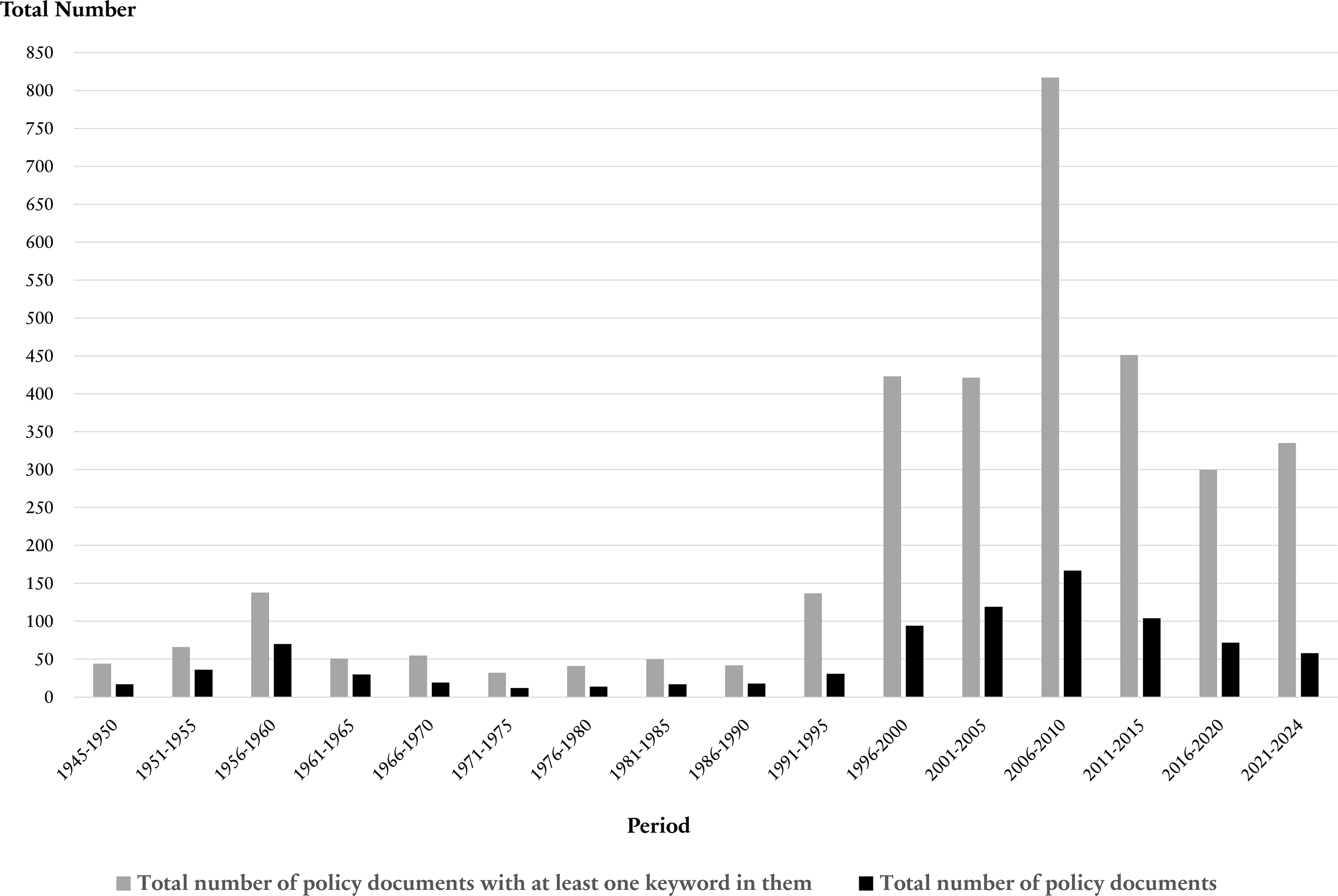
Figure 1 indicates that Indonesia’s government enacted a significant number of laws between the first five-year (1945–1950) and third (1956–1960) periods, which can reasonably be presumed to have been done in order to enforce laws and policies to govern the newly independent nation. Enacting of legislation then decreased between the fourth period (1961–1965) and the tenth (1991–1995). This decline was influenced by many factors, ranging from regime changes and political shifts to domestic and foreign turmoil and concerns over the stability of state security (Russell Reference Russell2020; Sulistyo Reference Sulistyo2002; World Bank 1975, 1979, 1994). The formation of legislation began to grow again from the period 1996–2000, influenced by the dramatic socio-political (e.g., political reform and the fall of Suharto) and economic (e.g., Asian financial crisis) upheaval that deeply affected national discourse (Knight Reference Knight2000; Russell Reference Russell2020; Ulum Reference Ulum2020). The crisis exposed systemic failures in social protection, leading to “welfare” and “well-being” (both are kesejahteraan in Indonesian) becoming more prominent in government discourse. This is apparent from the larger number of policy documents with more than one keyword in this period.
Interestingly, a decline in the number of policy documents published is observed when the SDGs were ratified in 2015. The SDGs were not adopted in national laws but integrated mainly through regulations such as the Presidential Regulation 59/2017 (Ministry of Law and Human Rights 2017) and the Decree of the Minister of National Development Planning 7/2018 (Ministry of Law and Human Rights 2018b). The latter was subsequently replaced by Regulation of the Minister of National Development Planning 1/2024 concerning coordination, planning, monitoring, evaluation, and reporting on the implementation of SDGs (Ministry of Law and Human Rights 2024a) and Presidential Regulation 6/2024 concerning innovative funding in the framework of achieving SDGs (Ministry of Law and Human Rights 2024b). Similarly, the policy mapping findings suggest that SDG targets are accommodated in other policy documents concerning forest plantations, animal husbandry and animal health, agricultural cultivation systems, and water resources.
Keyword frequencies and degrees of policy relatedness
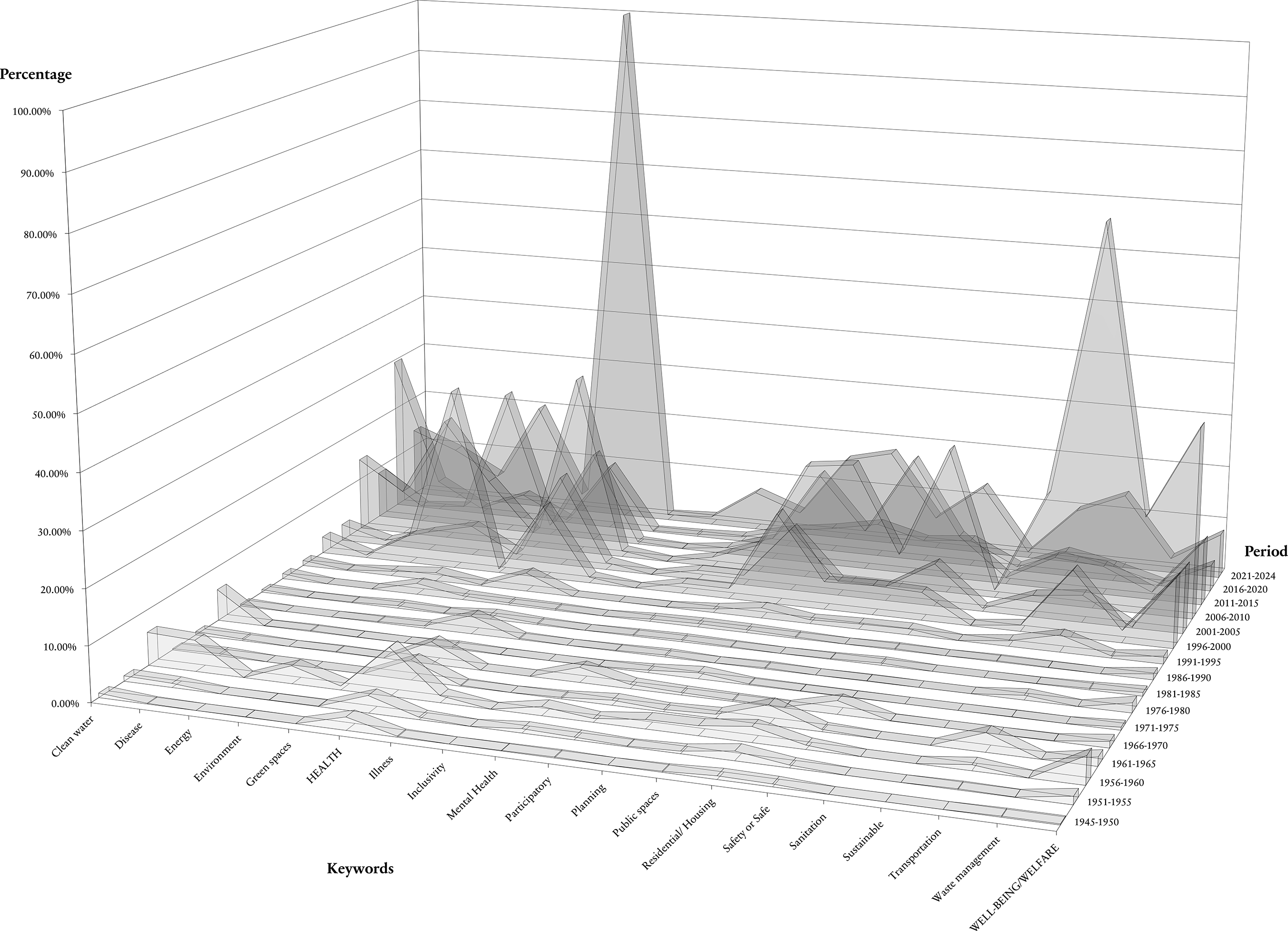
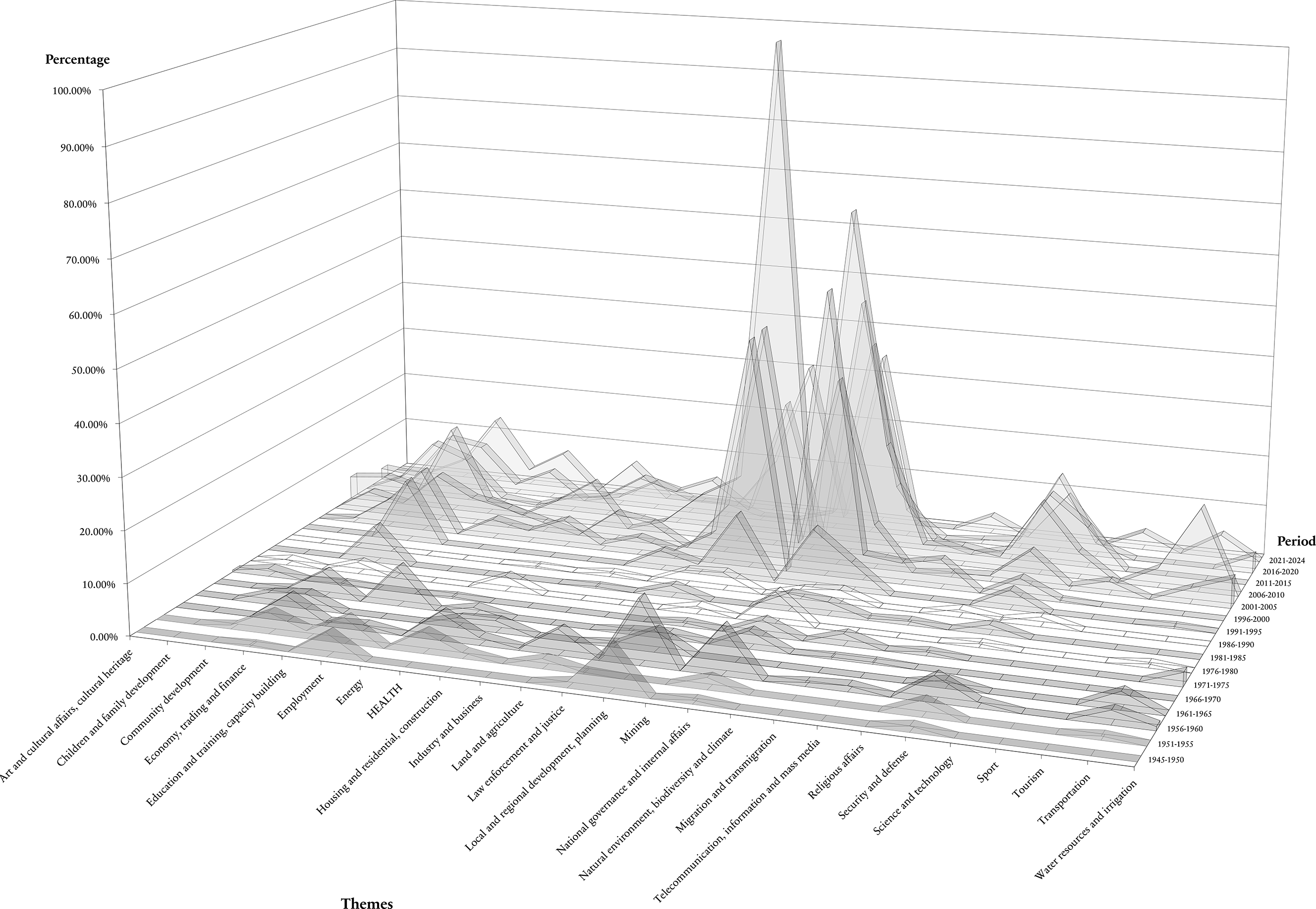
To assess the depth of policy integration, keyword occurrences were further classified according to their degree of relatedness to policy objectives. The top three keywords found in the policy documents are “health” (5,012 times), “transportation” (2,683 times), and “environment” (2,505 times); interestingly, “well-being” is the fourth most frequent keyword (2,265 times), while the two least found keywords are “sanitation” (117) and “inclusivity” (47) (Figure 2). The results suggest that the Government of Indonesia’s policies consistently address health and welfare/well-being from 1945 to 2024. Nevertheless, variations in the consideration of these aspects are also apparent, reflecting particular policy contexts and priorities over time, as discussed next. To maintain a clear and concise focus on the aim of this paper, the following description of results focuses mainly on the findings related to the “health” and “well-being” keywords, referring to other relevant keywords where appropriate.
Results of Indonesia’s policy mapping categorized by search keywords and periods.
“Health” has been a frequent word in Indonesia’s policy documents, with its first appearance in Law 2/1947 concerning the National Defense Council and Law 3/1948 on defense and armed forces related to the health division formation (Ministry of State Secretariat 1947a, Ministry of State Secretariat 1948a). It remained prominent in subsequent policy documents such as Law 12/1948 on labor for maintaining the health and safety of workers (Ministry of State Secretariat 1948b), Law 12/1950 concerning regency provincial government in East Java (Ministry of Law and Human Rights 1950a), Law 13/1950 concerning the formation of regency areas in Central Java Province (Ministry of Law and Human Rights 1950b), and related policy pertaining the supervision of health by the health department in provincial and regency/city levels.
Health-dedicated law was legalized in 1951 through Law 8/1951 concerning the suspension of granting licenses to doctors and dentists (Ministry of Law and Human Rights 1951a); Law 9/1951 concerning the rational distribution of doctors, dentists, and midwives (Ministry of Law and Human Rights 1951b); and Law 10/1951 concerning regulating private doctors in emergency situations (Ministry of Law and Human Rights 1951c). A significant fluctuation in the frequency of the “health” keyword is yet to be observed over time. For example, “health” appeared 275 times in 2016–2020 and 2,232 times in 2021–2024, the overall peak of this keyword. This was driven by the COVID-19 pandemic and aimed at transforming Indonesia’s health system across six domains: primary services, referral services, health resilience, funding, human resources, and health technology (Intania Reference Intania2023).
The growing emphasis on health in 2023 also influences the frequency of keywords “illness,” “disease,” and “mental health” with growing recognition in the 2021–2024 period. The keyword “illness” appears 23 times in this period, “disease” appears 222 times, and “mental health” appears 165 times. This can be explained by the enactment of Law 17/2023 (Ministry of State Secretariat 2023b) concerning health, which illustrates the government’s emphasis on prioritizing health goals.
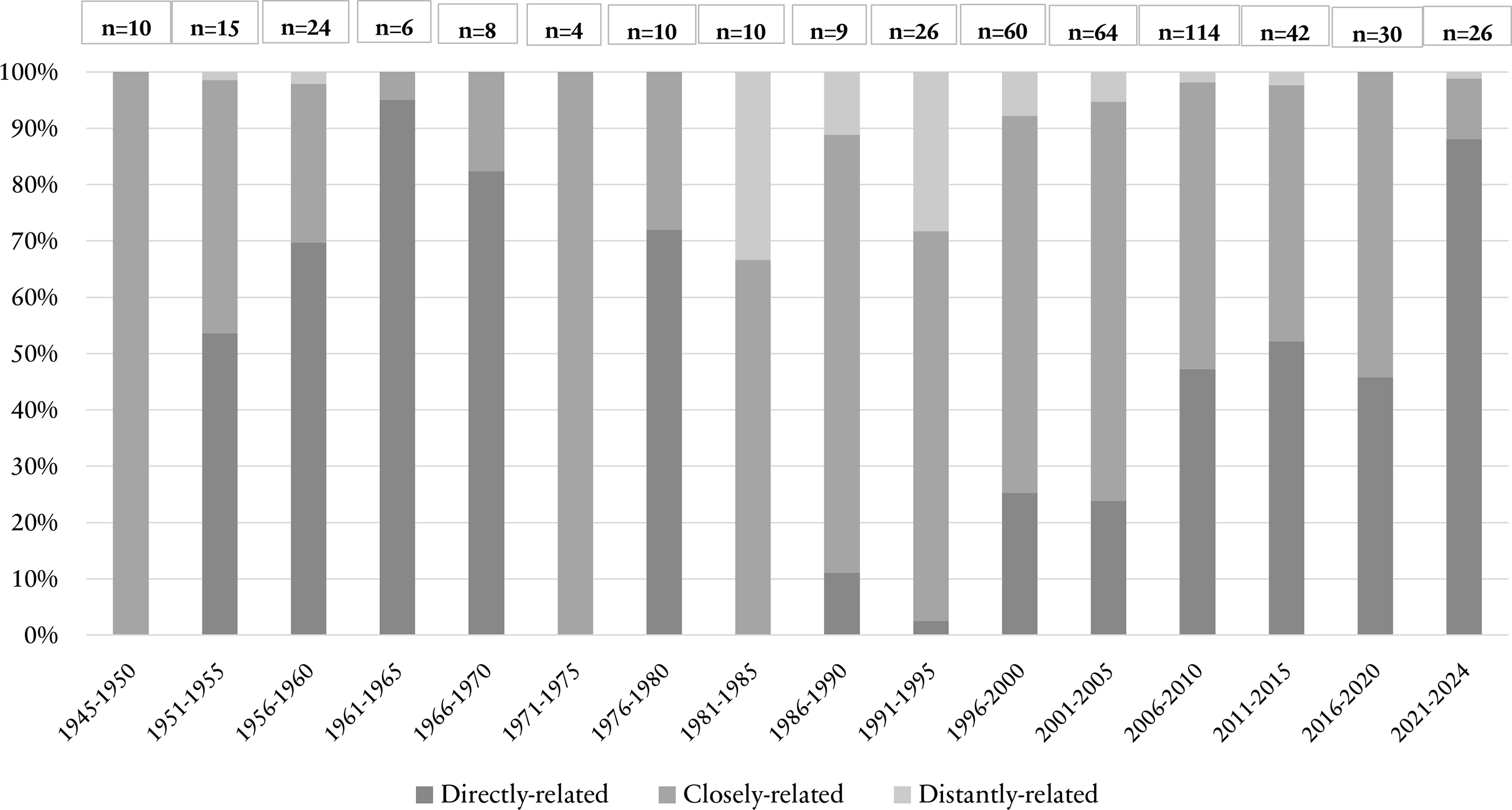
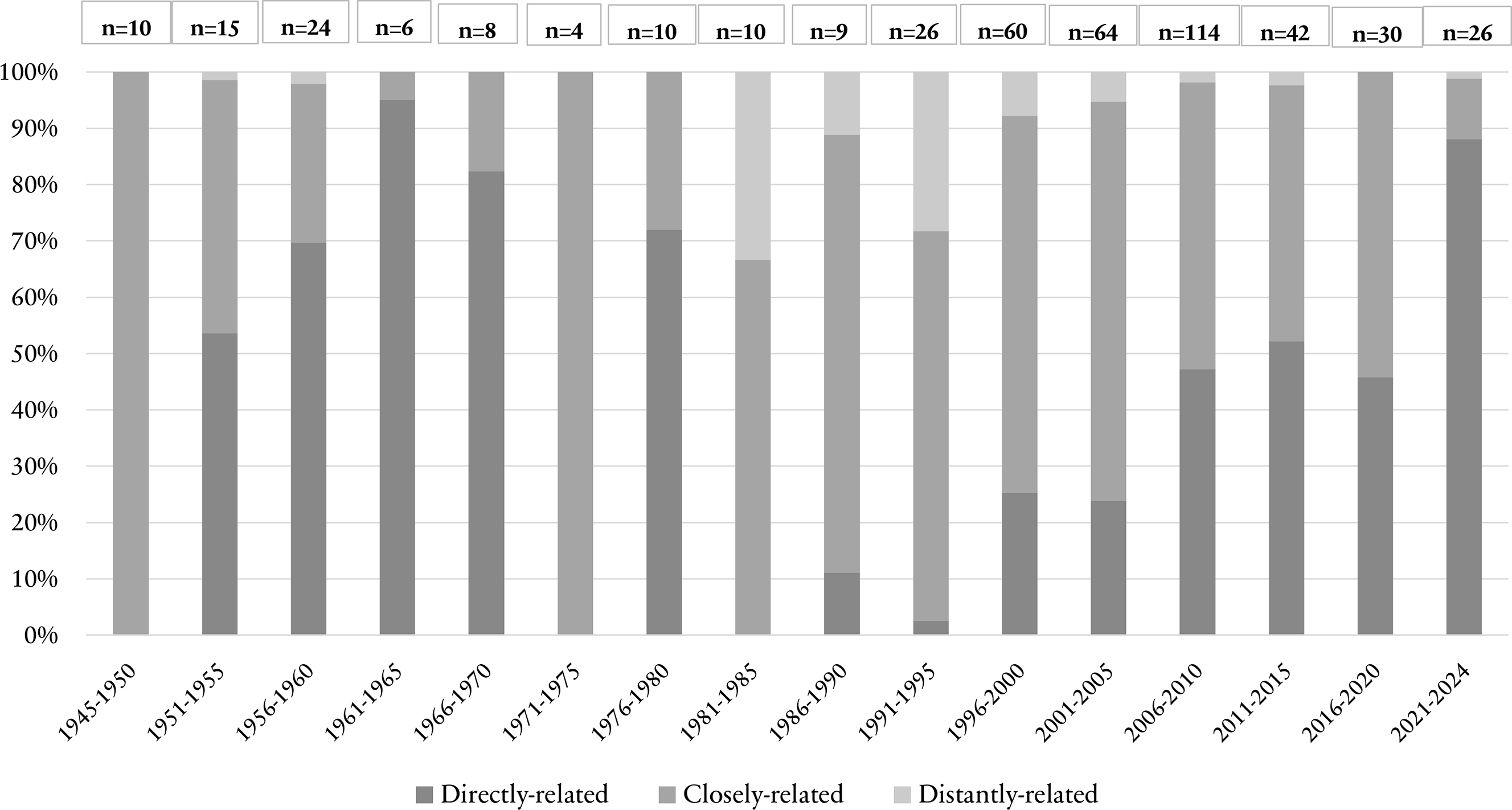
The relatedness of keywords reveals that “health” has been consistently addressed across all periods as “closely related” (Figure 3). The same pattern is observed for “clean water,” “participatory,” “mental health,” and “well-being” (see supplementary material for the full list). Nevertheless, “health” is “directly related” to specific policy objectives in only a small percentage of cases (3,242 keywords are directly related to the policy, which represents 12% of the 26,054 keyword finds). In this direct relation of keywords, “transportation” (1,901 or 7%), “environment” (1,649 or 6%), and “planning” (1,435 or 5%) also stand out. These results suggest an emphasis on urban health considerations in Indonesia, which are discussed further in Section 4.
“Health” keyword’s relatedness per period and number of policy documents.
Overall, the policy mapping reveals that health-related policy documents are more prevalent than well-being-related documents. In addition, welfare/well-being is not frequently incorporated across the sectoral themes. The term “well-being/welfare” began appearing frequently around 1948, three years after Indonesia’s independence and has since become the fourth most commonly occurring keyword. “Well-being” is translated as “kesejahteraan” in Indonesian, but it is also widely referred to as “welfare.” The increase in the frequency of this keyword’s usage, particularly in certain periods (e.g., 1996–2000 (290 times), 2006–2010 (276), 2006–2010 (801), and 2011–2015 (271)), can be attributed to several key legislations. These include Law 13/1998 concerning the welfare of the elderly (Ministry of State Secretariat 1998), Law 11/2009 concerning social welfare (Ministry of Law and Human Rights 2009b), and Law 6/2023 on job creation (Ministry of State Secretariat 2022). However, a frequency decline is observed in this keyword in the periods following the ratification of the SDGs with 110 times (2016–2020) and 186 times (2021–2024). Although economic recovery became a governmental priority in the post-COVID era, this focus has not been matched by a corresponding increase in policy emphasis on enhancing or equalizing welfare across cities/regencies (Ispriyarso and Wibawa Reference Ispriyarso and Wibawa2023; UNICEF et al. 2021).
The relatedness of the “welfare/well-being” keyword reveals that it has been consistently addressed across all periods as “closely related” (Figure 4). Although “welfare/well-being” is well integrated into themes and policy areas, it is not classified as “directly related” to the same extent as “health.” Specifically, only 647 keyword occurrences are “directly related” (representing just 2% of the total keyword finds). In the periods where “health” does not have direct policy relatedness (namely, 1945–1950, 1971–1975, and 1981–1985), “welfare/well-being” lacks the same. One possible explanation is that health directly affects well-being (Tan et al. Reference Tan, Chiu and Ren Ai2023; WHO 2021, 2023a, 2024).
“Welfare/well-being” keyword’s relatedness per period and number of policy documents.

Temporal patterns of keywords across socio-political contexts
This section further describes and discusses the socio-political contexts that have influenced the keyword frequencies identified. The first five years of the policy mapping review (1945–1950) marked the start of the Indonesian national revolution with the 1945 Constitution – used to this day with four amendments (Russell Reference Russell2020; Sulistyo Reference Sulistyo2002). The main policy focus during this era was on maintaining Indonesia’s unity and integrity as a nation, displayed by specific policies on health and socio-economic welfare/well-being (e.g., access to clean water and housing) resulting in notable “health” keyword finds (52 times), as well as “clean water” (18) and “residential/housing” (14) in that early policy period (Ministry of State Secretariat 1947b, 1947c, 1947d, 1948b).
The parliamentary system was set in 1950 with a temporary constitution, but the government cabinet experienced instability, and the parliament was rapidly dissolved. Thus, the original Indonesian constitution of 1945 was reimplemented in 1957 (Sulistyo Reference Sulistyo2002). The keywords for the periods between 1950 and 1970 reflect this instability as well as the poor conditions of Indonesian society (Sulistyo Reference Sulistyo2002; Ulum Reference Ulum2020), where the “health” (436 times), “well-being/welfare” (204), and “residential/housing” (181) keywords are dominant (Ministry of Law and Human Rights 1951a; Ministry of State Secretariat 1962a, 1962b, 1964, 1967, 1979).
The first national program of five-year development plans or REPELITA I (1969–1974) established Indonesia’s first centralized development planning framework, prioritizing infrastructure development and agricultural modernization to boost food production (Knight Reference Knight2000; Ministry of Finance of Indonesia 1969). Although health and education investment was limited, population pressures led to the introduction of the national family planning program (World Bank 1975; Booth Reference Booth1979). This shift is reflected in the policy mapping results, with increased references to “health” (98) and “welfare/well-being” (37) during the 1966–1975 period.
Subsequent REPELITA development plans (II–VI, from 1974 to 1998) progressively expanded state involvement in health-and well-being–related sectors, albeit largely through sector-specific interventions rather than integrated policy frameworks. Across these phases, national priorities consistently linked health to economic productivity, population management, and infrastructure development. Key investments in this period included the expansion of basic education through the Sekolah Dasar Inpres program, the scaling-up of community health centers, family planning, and immunization programs, and improvements in clean water and sanitation(A. E. Booth Reference Booth1979; Kementerian Kesehatan Republik Indonesia 2007; World Bank 1975, 1979, 1989a, 1989b).
The policy mapping results show that the dominant frequency of the keywords “environment” (864 times), “health” (495), and “planning” (467) derive from REPELITAs II to VI (1969–1998) and their focus on land-use planning (e.g., agriculture, forestry, urban), family planning, disease control and eradication, and infrastructure development. The enforcement of civil rights remained a significant issue in the REPELITA programs, especially with regard to equality in welfare, economy, education, and health (ILO 2021; Zein et al. Reference Zein, Yunanto, Nurhayati, Setiawan and Aziz Samudra2022; WHO 2014c). Importantly, the economic crisis that hit Asia in 1997–1998 marks a jump in the frequency of the keyword “well-being” (290 finds) in 1996–2000 (compared to 32 in 1991–1995). The recovery years following this crisis also show a prioritization of “well-being,” with 276 keyword finds between 2001 and 2005 and 801 between 2006 and 2010.
Indonesia’s entry into the 1998 reform period (Zein et al. Reference Zein, Yunanto, Nurhayati, Setiawan and Aziz Samudra2022; Russell Reference Russell2020; Ulum Reference Ulum2020) witnessed a new phase marked on democracy such as constitutional amendments, free elections, decentralization, and stronger civil liberties (Ministry of State Secretariat 1999; Zein et al. Reference Zein, Yunanto, Nurhayati, Setiawan and Aziz Samudra2022; Ulum Reference Ulum2020). These socio-political changes are reflected in the dominant keywords of the 1996–2000 period. The most frequently occurring keywords were “environment” (766 times), reflecting the focus on forestry policies and natural-resource-based economy or expenditures at the national and local level at that time, followed by “planning” (384) and “health” (308).
In 2001–2005, Indonesia underwent major socio-political restructuring under decentralization reforms (Soekarnoputri’s to Yudhoyono’s era) initiated by Law No. 22/1999 (Ministry of State Secretariat 1999), granting autonomy to regional governments in managing health services, environment, and urban planning. As expected, the dominant keywords were “health” (382 times), “welfare/well-being” (276), and “planning” (264). Several major health issues during this period contributed to this trend, including avian influenza in 2003 and filariasis in 2004 (Kementerian Kesehatan Republik Indonesia 2007). Although well-being and inclusivity concepts were not yet central in policy discourse, decentralization during this period laid the groundwork for more participatory and regionally responsive approaches.
From 2006 to 2015 (Yudhoyono’s to Widodo’s era), Indonesia experienced a marked shift in relation to health and well-being. The dominant keywords are “transportation” (1,719 times), “health” (1,140), and “well-being/welfare” (1,072). Transportation became dominant as a strategic priority in Indonesia’s national development agenda (Ministry of Law and Human Rights 2008, 2009a, 2009d). Similarly, the launch of the National Health Insurance Scheme in 2014 and investment in public health infrastructure strengthened the focus on health issues (Agustina et al. Reference Agustina, Dartanto, Sitompul, Susiloretni, Achadi, Taher and Wirawan2019).
2016–2024 (Widodo’s era) saw many strategic goals on health, welfare, and sustainability (e.g., expansion of National Health Insurance coverage, reduction of stunting, and mainstreaming of climate discourse). The dominant keywords are “health” (2,232 times), “environment” (453), and “public spaces” (401), with “well-being/welfare” also featuring significantly (186) (Ministry of Law and Human Rights 2024a, 2024b; Ministry of National Development Planning 2019).
Thematic distribution of health and well-being across policy sectors
This section examines the sectoral embedding of health and well-being, revealing the extent to which these issues are integrated across policy domains rather than being confined to the health sector. The dominant themes in the keywords finds were “national governance and internal affairs” (845 times or 25% of the total 3,402 repeated policies that include one or more keywords), “local and regional development, planning” (768 or 23%), “economy, trading and finance” (284 or 8%), “security and defense” (211 or 6%), and “natural environment, biodiversity and climate” (170 or 5%) (Figure 5). The dominance of “national governance and internal affairs” is because in the 1961–1965 period, Indonesia’s national revenue and expenditure budget became one single regulation for all ministerial and sectoral plans, published every fiscal year (Ministry of State Secretariat 1961); in previous years, each ministry had their own laws (e.g., the Ministry of Health had a national law on health budget allocations, the Ministry of Labor on budgets for employment and training). An implication of this is that since that early period, “health” and “well-being” have been consistently found in this “national governance and internal affairs” theme.
Results of Indonesia’s legislation policy mapping categorized by national themes over the keyword search examined periods.
There are a limited number of “health”-specific laws or policy documents in the search period of 1945–2024 (i.e., 24 of the 878 policy documents, just 3%), and the total number of policy documents that include the keyword “health” is 111 (or 3% of the 3,402 repeated documents). “Welfare/well-being” has no stand-alone theme or, indeed, policy documents in the government’s database. This keyword is accommodated in 564 (16%) of the policy documents. It is mostly related to the theme “children and family development” (46 repeated policies or 1%), “community development” (105 or 3%), “economy, trading and finance” (284 or 8%), “employment” (103 or 3%), and “education and training, capacity building” (43 or 1%).
Governance actors in health and well-being policies
To evaluate the governance structure underpinning health and well-being policies, policy documents were analyzed by the level of actor responsible for their formulation, grouped according to the categories established by Bainbridge et al. (Reference Bainbridge, Potts and Gerard O’Higgins2011): international, regional (in this case, all of Asia), national, provincial, and local (regency/city). This is done to understand the commitment and coordination in health policy development and implementation (Allen et al. Reference Allen, Pilar, Walsh-Bailey, Hooley, Mazzucca, Lewis and Mettert2020). Results (Figure 6) reveal that the national level had the highest number of repeated policy documents (2,427 of 3,402, or 71%), followed by the local level (534 or 16%) and the provincial level (199 or 6%). The adoption of international agreements corresponds to 168 policy documents (5%), principally in the periods 1996–2000 (32 policy documents), 2006–2010 (32), and 2016–2020 (27). Regional (Asia-based) agreements, by comparison, correspond to 74 policy documents (2%), which were primarily adopted within the 2011–2024 period (25 documents).
The distribution of governance actors per period of time.

When looking specifically at the theme of “health” at these different governance scales, the policy documents mostly (101 out of 111 that include the keyword “health” or 91%) relate to national laws, concerning aspects such as mental health, pharmaceuticals, animal husbandry and animal health, compulsory employment of para-medical personnel, and diseases/plague (Ministry of Law and Human Rights 2009c; Ministry of State Secretariat 1962a, 1966, 2023b). This is followed by international agreements (8 or 8%) including the ratification of the 1971 Convention on psychotropic substances (Ministry of State Secretariat 1996), the United Nations convention against illicit traffic in narcotic drugs and psychotropic substances (Ministry of State Secretariat 1997), and the Rotterdam convention on consent procedures for certain hazardous chemicals and pesticides in international trade (Ministry of Law and Human Rights 2013). The representation of “health” is weakest at the regional level (1%), linked to the treaty of mutual respect between the Republic of Indonesia and Papua New Guinea on development assistance, including health facilities (Ministry of State Secretariat 1987).
A growth in provincial actors is observed in the 2021–2024 period, with 79 policy documents (2% of 3,402). This can be explained by the creation of new provinces and additional authority given to provincial governments in managing their regions (Ministry of Law and Human Rights 2021). Meanwhile, the local level shows a significant jump in 1996–2000 (107 policy documents or 3%), 2001–2005 (102 or 3%), with a peak in 2006–2010 (234 or 7%). This growth in local policy-making suggests a significant change in the focus of the Indonesian Government, with a decentralization of tasks accompanied by dedicated community participation and empowerment efforts (e.g., Law 23 of 2014) concerning regional government (Ministry of State Secretariat 2014) and Law 3 of 2024 concerning the second amendment to law 6 of 2014 on villages (Ministry of State Secretariat 2024a). It acknowledges that with the addition of new provinces and local governments, services to address community needs (such as healthcare and community welfare facilities, housing, and clean water) could be maximized through more local socio-economic development supportive policy and regulatory approaches. This can be seen from the infrastructure development and expansion programs related to enhancing transport connectivity in the National Long-Term Development Plan 2005–2025 (Ministry of Law and Human Rights 2007) and investment in public health infrastructure through the National Health Coverage from 2014 that has improved healthcare access and equity (Ministry of National Development Planning 2019).
Discussion of key findings
Mixed integration of health and well-being into policy agendas
Interpreted through the lens of agenda-setting and multilevel governance theory, the policy mapping results reveal how health considerations have fluctuated in institutional salience over time and how governance fragmentation has, to an extent, affected their structured integration across policy sectors and levels. The consistent appearance of “health” and “well-being” as the keywords across policy periods suggests a long-standing recognition of their importance. However, the level of integration varies substantially. While “health” ranks highest in frequency (5,012 mentions), it is mostly categorized as “closely related” rather than “directly related” to legislative objectives. Only 12% of all “health” keyword mentions are directly related to specific policy aims, revealing a significant gap between acknowledgment and operational prioritization in national policies and programmes. Moreover, the sharp increase in health-related keywords (including “disease” and “illness”) frequency during 2021–2024, in response to the COVID-19 pandemic and the introduction of Law 17/2023, as well as other relevant peaks in 2003 and 2005 (in response to, e.g., severe acute respiratory syndrome and avian influenza outbreaks; or the establishment of HIV/AIDS monitoring and treatment programs), point to a reactive rather than proactive approach by the government when it comes to health policy formulation and implementation.
This trend aligns with global observations that health often gains legislative attention during crises (Giannakeas et al. Reference Giannakeas, Bhatia, Warkentin, Bogoch and Stall2020; Kruk et al. Reference Kruk, Gage, Arsenault, Jordan, Leslie, Roder-DeWan and Adeyi2018a; Kruk et al. Reference Kruk, Gage, Joseph, Danaei, García-Saisó and Salomon2018b). Nevertheless, long-term, evidence-based public health strategies (Halperin et al. Reference Halperin, Hearst, Hodgins, Bailey, Klausner, Jackson and Wamai2021) are also apparent at the heart of the country’s planning and development (e.g., REPELITA V and VI, which had a focus on healthcare infrastructure expansion – increasing the number of healthcare facilities, particularly in rural and underserved areas, disease prevention and control through immunization programs and controlling communicable diseases, maternal and child health, and family planning programs to control population growth and improve the quality of life for families) (Anwar Reference Anwar1999; A. Booth Reference Booth1989; Ministry of State Secretariat 1962a). The Government’s commitment to Universal Health Care (UHC) is also apparent by the recent implementation of the National Health Insurance Scheme in 2019, called Jaminan Kesehatan Nasional (JKN) (ILO 2021), through Presidential Regulation Number 82 of 2018 concerning Health Insurance (Ministry of Law and Human Rights 2018a). JKN provides comprehensive benefits such as promotive, preventive, curative, and rehabilitative health services (BPJS Reference BPJS2023), which support health.
Despite widespread commitment to the provision of health services and initiatives toward a healthy population through the national program, the limited number of health-specific policies (i.e., 24 documents) points to opportunities for improvement toward health-centered planning and governance. Adopting a HiAP to (urban) planning has been shown to yield both immediate and long-term benefits for physical, mental, and social well-being (Tan et al. Reference Tan, Chiu and Ren Ai2023).
The integration of “well-being” into national legislation is weaker, but the policy mapping results still exemplify the widely recognized linkages between health and well-being (Giles-Corti et al. Reference Giles-Corti, Vernez-Moudon, Reis, Turrell, Dannenberg, Badland and Foster2016; Giles-Corti et al. Reference Giles-Corti, Lowe and Arundel2020; Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019; Tan et al. Reference Tan, Chiu and Ren Ai2023; WHO 1946). The “welfare/well-being” keywords are found in many health-related measures in the reviewed policy documents associated with diverse sectors of employment (e.g., trading and finance, housing, and transportation) and areas (e.g., environment, climate, children, and family development) (Ministry of Law and Human Rights 2009e, 2009d; Ministry of State Secretariat 1979, 1994a, 2023a, 2024a). Thus, the frequency of “welfare/well-being” largely mirrors health’s keyword pattern in terms of rising and falling. However, there are two periods that deviate from this overall pattern: 1976–1980 and 1991–1995, where references to well-being appear more frequently than those to health. This shift reflects changing policy priorities. Children’s welfare and well-being, as part of child and family development, became a priority in the late 1970s (Ministry of State Secretariat 1979), while economic and financial well-being were a major national goal in the decade of the 1990s (Ministry of State Secretariat 1992, 1994a, 1994b, 1995). Nevertheless, the observed general lack of well-being-specific policies or, indeed, themes demonstrates the need for an integrated policy approach to health.
Health and well-being policy evolution
The integration of health and well-being into Indonesian legislation has also been deeply shaped by shifts in governance regimes and national development priorities. During the New Order era (1966–1998), development planning under the REPELITA framework was highly centralized, with health issues framed primarily through the lens of economic productivity and population control (Anwar Reference Anwar1999; A. Booth Reference Booth1989). Although infrastructure and basic health services were expanded during this period, health and well-being were often addressed in isolation from other determinants like housing, environment, or equity, limiting their integration into broader sustainable development strategies.
Following the democratic transition and decentralization reforms of the late 1990s and early 2000s, Indonesia entered a new governance phase characterized by increased local autonomy and political pluralism (Buehler Reference Buehler2005; Ministry of State Secretariat 1999; Ryaas Reference Ryaas2002; Ulum Reference Ulum2020). This enabled more context-specific and participatory approaches to health and urban planning at the city level. However, this also led to fragmented policy implementation, with disparities in capacity, budget allocation, and commitment across districts (Buehler Reference Buehler2005; Ryaas Reference Ryaas2002).
In the post-2015 SDG era and, especially, following the COVID-19 pandemic, Indonesia’s central government renewed its focus on a systemic health reform, culminating in the 2023 Health Law (Law 17/2023). This law represents a significant milestone in consolidating health as a national policy priority. However, stronger institutional mechanisms are still needed to translate national goals into equitable, cross-sectoral, and sustainable policies across all levels of governance.
Sectoral disconnect in health and well-being policy coherence
The dominance of “health” and “well-being” keywords in the “national governance and internal affairs” and “local and regional planning” themes, rather than in specific health or social policy sectors, reveals structural issues in policy coherence in Indonesia. Health considerations are often accommodated within broader governance or planning documents, potentially minimizing their strategic intent.
While integrated planning is a core component of the SDGs, HiAP, and NUA framework (Finnish Ministry of Social Affairs and Health 2006; WHO 2014a, 2014b, 2014c), the findings of this study suggest a fragmented approach. Notably, while the REPELITA phases provided a coherent development roadmap with health and infrastructure considerations (leading to multiple sectors’ involvement in improving health-related determinants), their sectoral focus rarely translated into cross-sectoral integration. For example, policies under REPELITA IV (1984–1989) promoted clean water, child nutrition, and health services (World Bank 1989b). Yet, these initiatives often came under separate ministries (e.g., Ministry of Health for immunization, Ministry of Public Works for clean water, and others), leading to sectoral implementation silos. The reviewed policy documents do not reveal any legal administrative mechanism to ensure that these efforts were planned together, shared data, or had shared targets at the time, so it appears that there was no integrated approach nor structured collaboration.
The common fragmented implementation of health considerations undermines Indonesia’s ability to meet the interconnected targets of SDG 3. For example, achieving the target of reducing deaths and illnesses caused by hazardous chemicals and pollution (including air, water, and soil pollution) requires coordinated planning across the environment, transport, and health sectors, among others. Thus, advancing SDG 3 necessitates an integrated, cross-sectoral legislative and planning framework that efficiently links public health determinants with public health outcomes. This underscores a missed opportunity for embedding global commitments into national law through structured legislative pathways.
Multilevel governance and vertical integration of health and well-being policies
Indonesia’s shift toward decentralization, which began in the late 1990s, triggered a diversification of policy actors, especially at provincial and local levels (Buehler Reference Buehler2005; Ulum Reference Ulum2020). As demonstrated in Section 3.5 (Figure 6), this decentralization has facilitated some localized improvements in addressing health determinants, particularly in urban planning, waste management, and public space development. However, rather than producing coherent multilevel integration of policy measures and/or instruments, decentralization has resulted in uneven vertical coordination and fragmented implementation across governance levels (Agustina et al. Reference Agustina, Dartanto, Sitompul, Susiloretni, Achadi, Taher and Wirawan2019; Buehler Reference Buehler2005; Ministry of State Secretariat 1999; World Bank 1994).
Despite the push toward decentralization, results show that policies remain formulated at the national level (71%), indicating limited vertical integration between national objectives and subnational implementation. Even though many health determinants (like sanitation, urban transport, and housing) need to be managed locally, only 16% of policy documents were local. Importantly, international agreements influence only 5% of keyword-containing policies (e.g., UHC, rights, the conventions on child labor and employment, psychotropic substances and narcotic drugs, the ratification of the Cartagena Protocol on biosafety, and others). This indicates weak integration of global frameworks into national policy and, ultimately, local action.
Despite Indonesia’s global commitments, such as those made during the 2022 G20 presidency (Jütten Reference Jütten2022), their translation into national policy, particularly through local actors, remains insufficient. The limited alignment of national legislation with international goals and the uneven capacity across provinces and cities/regencies have led to fragmented vertical implementation. Some attempts are worth highlighting though. For example, Indonesia tried to increase the availability of infrastructure and equipment in public health facilities, as well as the utilization of health services nationwide, through the World Bank Health Project in 2023 (World Bank 2023). Similarly, it attempted to strengthen primary healthcare and digital health integration across all planning tiers (World Bank 2024). Through these national programs, local community health centers (Puskesmas), auxiliary centers, and small clinics would be better equipped, and public health laboratories strengthened. This is expected to contribute to UHC and the country’s preparedness for future pandemics. While decentralization fosters local action, in the context of Indonesia’s weak vertical integration, it also challenges integrated urban health strategies (Bainbridge et al. Reference Bainbridge, Potts and Gerard O’Higgins2011; Glass and Newig Reference Glass and Newig2019) and thus defies uniform progress toward achieving SDG 3 targets. Overall, the findings indicate that decentralization has expanded the number of actors involved in health governance but without corresponding mechanisms for vertical policy integration, thus resulting in dispersed rather than coordinated multilevel action.
Weak consideration of health and well-being determinants
The analysis reveals that certain health determinants, such as sanitation (117 mentions) and inclusivity (47), are underrepresented. These figures are salient given their foundational role in achieving equitable health outcomes (Ehrlich et al. Reference Ehrlich, Kemper, Pesaresi and Corbane2018; Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019). The marginal presence of these keywords signals persistent thematic gaps within Indonesian policy-making, where urban infrastructure, economic growth, and defence dominate over social equity and public health. Similarly, the relatively low visibility of “mental health” (165 mentions in 2021–2024, but rarely earlier) suggests a belated policy awakening rather than sustained commitment. This belatedness is particularly concerning given the increasing global emphasis on mental health as a development issue (Manderscheid et al. Reference Manderscheid, Ryff, Freeman, McKnight-Eily, Dhingra and Strine2010; WHO 2021).
Despite the overlaps between sustainability and health (through determinants such as air quality, clean water, climate resilience, sanitation, and environmental justice), the policy mapping shows a disconnect. Health policies mainly focus on access to care or service coverage, while environmental policies address conservation, with no legal pathways that explicitly link sustainability to health outcomes. This lack of structured integration undermines the commitment to the SDGs (in particular, SDG 3, SDG 6, SDG 11, and SDG 13). This is surprising given the existence of SDG-centric legislation: Minister of National Development Planning Regulation 1/2024 concerning coordination, planning, monitoring, evaluation, and reporting on the implementation of SDGs (Ministry of Law and Human Rights 2024a) and Presidential Regulation 6/2024 concerning innovative funding in the framework of achieving SDGs (Ministry of Law and Human Rights 2024b). This lack of discrete policies addressing environment and health links and that are tiered through the country’s policy framework (i.e., from national to local) is particularly concerning given Indonesia’s vulnerability to urban pollution, climate change risks, and rising non-communicable diseases with high population growth (Giles-Corti et al. Reference Giles-Corti, Vernez-Moudon, Reis, Turrell, Dannenberg, Badland and Foster2016; Statistics of Indonesia 2024; UN 2023; WHO 2014c, 2023a).
The lack of integration is also apparent when looking at global frameworks such as One Health, HiAP, and the NUA, which emphasize sustainability as a cross-cutting pillar yet are sparsely reflected in Indonesian policy documents. For instance, no national policy documents reference “One Health,” despite its relevance for managing zoonotic diseases, environmental health, and pandemic prevention, and despite relevant national legislation in this regard (e.g., Law 17/2023 concerning health (Ministry of State Secretariat 2023b) and Law 18/2009 on animal husbandry and animal health (Ministry of Law and Human Rights 2009c). The findings of this policy review suggest that more efforts are needed toward strategic and effective health governance. This would require the adoption of integrated approaches on health, environment, and infrastructure planning at higher policy-making tiers (i.e., national) that are then vertically implemented across regional and local levels.
Toward a coherent health and well-being policy framework
The limitations identified in Indonesia’s policy documents point to a series of systemic issues, including limited dedicated health and no well-being policies, poor cross-sectoral coordination on the integration of health considerations, and inadequate assimilation of global goals and frameworks. In light of these limitations and in an attempt to inform the development of a coherent and responsive policy framework for health in Indonesia, the following is recommended:
-
• Develop dedicated policy documents for well-being, similar to those for health, and systematically include well-being considerations across environmental, urban, social, and economic policies (Barata et al. Reference Barata, Kinney, Dear, Ligeti, Ebi, Hess and Dickinson2018; Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019; WHO 2024).
-
• Mandate cross-sectoral coordination mechanisms, such as inter-ministry/agency SDG task forces, particularly linking health and well-being with environment, transport, housing, and urban planning sectors (Tan et al. Reference Tan, Chiu and Ren Ai2023; WHO 2023a).
-
• Embed international frameworks (e.g., HiAP, One Health, and NUA) directly into legal texts, with operational indicators and accountability systems (Giles-Corti et al. Reference Giles-Corti, Vernez-Moudon, Reis, Turrell, Dannenberg, Badland and Foster2016; Giles-Corti et al. Reference Giles-Corti, Lowe and Arundel2020; Lowe et al. Reference Lowe, Adlakha, Sallis, Salvo, Cerin, Moudon and Higgs2022; Ramirez-Rubio et al. Reference Ramirez-Rubio, Daher, Fanjul, Gascon, Mueller, Pajín and Plasencia2019; UN 2022).
-
• Strengthen vertical integration by embedding SDG 3 and other targets (e.g., SDGs 6, 11, and 15) into provincial and municipal development plans (Ministry of State Secretariat 2024b), medium-term national development plans (Ministry of State Secretariat 2025), and provincial long-term development plans (Secretary of DKI Jakarta Province 2024).
-
• Provide technical and financial capacity building to enable harmonizing and coordinating health programs and action plans across governance levels and sectors, as well as to enable consistent monitoring and evaluation from national through provincial to city/regency government levels.
Limitations and implications for interpretation
This study provides the first long-term quantitative mapping of health and well-being within Indonesia’s legislation, revealing persistent but uneven policy attention, reactive prioritization during crises, and limited structured integration across sectors and governance levels. Nevertheless, several research limitations merit consideration. First, keyword frequency and document count measure agenda prominence rather than policy quality, implementation, or health outcomes. High frequency therefore reflects institutional recognition, not effectiveness. Second, the five-year temporal aggregation, while aligned with electoral cycles, may obscure shorter-term policy trends. More importantly, the analysis does not seek to establish causal relationships between political events and policy outcomes. Nonetheless, discrete increases in keyword frequency during periods of political transition, institutional reform, and public health crisis provide quantitative support for interpreting these moments as shifts in policy attention. This interpretation aligns with agenda-setting and punctuated equilibrium theories, which posit that policy change often occurs through episodic bursts of attention rather than incremental adjustment (Arnold et al. Reference Arnold, Beauchamp and Bowie2014; Baumgartner and Jones Reference Baumgartner and Jones1993). Accordingly, keyword frequency is treated as a robust and replicable proxy for agenda salience within formal legislative discourse, rather than a measure of policy effectiveness.
Despite these constraints, the approach remains well suited to identifying long-term patterns, agenda shifts, and structural gaps in policy integration. The convergence of findings across multiple analytical dimensions, namely, frequency, relatedness, thematic embedding, and governance actors, strengthens confidence in the conclusions. These limitations do not undermine the study’s core contribution: demonstrating that health and well-being are widely embedded in Indonesia’s legislation yet remain insufficiently structured within an integrated policy framework.
Conclusion
Health appears as a stand-alone theme with 24 policy documents from 1945 to 2024. However, it is worth highlighting that it took eight years since the ratification of the SDGs for Indonesia’s government to introduce a dedicated Health Law 17/2023 and provide a legal basis for strengthening the health sector and providing UHC in the country. This slow development of health-centric legislation is even more poignant for well-being, which, to date, lacks dedicated legislation. The absence of legal or administrative mechanisms linking environmental, transport, and health policies indicates weak horizontal coherence between SDG 3 and SDGs 6, 11, and 13, despite their conceptual interdependence. Despite this, the terms are consistently integrated into national policy documents over time as closely related keywords, suggesting that the HiAP approach may be either deliberately or incidentally applied in Indonesia.
Overall, Indonesia’s policy frameworks show progressive awareness of health, even though their integration is inconsistent and thematically narrow. This suggests a policy development that is nominally inclusive of health, but not functionally structured around them. The distribution of health-related policy documents by theme shows that they are typically embedded within national governance and regional planning documents, rather than in health-specific policies. This indirect embedding dilutes the clarity and accountability of health-focused interventions and complicates implementation and monitoring.
The policy mapping findings show a positive trend in the consideration of health and well-being over time. However, the observed limited vertical integration calls for further examination of policy implementation and impact. Future studies should consider integrating urban spatial analysis with policy mapping to enable the exploration of the extent and effectiveness of policy implementation (e.g., national policy manifestation in an urban area). This would help gather the evidence base for any required adjustments to public health policy measures and action.
By systematically mapping legislative frequency, thematic embedding, and governance-level distribution for nearly eight decades, this study demonstrates how quantitative policy mapping can function as an evidence-based method to measure policy coherence toward the SDG targets. The approach allows policymakers to identify not only health policy gaps but also structural misalignments between national commitments and sectoral implementation. It offers a replicable framework for integrated sustainable urban health strategies in low-and middle-income countries.
This paper contributes to policy mapping scholarship by operationalizing a systematic quantitative longitudinal policy mapping methodology that enhances commonly applied qualitative methods. In doing so, it enables a more detailed identification of policy trends and gaps between governance periods, including their relatedness to health, main legal themes, and associated actors. Importantly, it provides an exemplary approach to incorporating linguistic variations in a country. This analytical framework is transferable to other countries and research areas, supporting more robust approaches to the examination of legislative intent.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S0143814X26101123.
Data availability statement
This data is publicly available. Our calculations can be reproduced and updated as new regulations become available. Replication materials are available in the Journal of Public Policy Dataverse: https://doi.org/10.7910/DVN/0ZVQFA.
Acknowledgments
The authors would like to thank the Directorate General of Legislation of the Republic of Indonesia for allowing access to all national and regional laws and regulations in Indonesia. Author 1 would also like to thank the Ministry of Finance of the Republic of Indonesia and related ministries for the Indonesia Endowment Fund for Education (Ph.D. scholarship) awarded to her to enable her to carry out her doctoral studies and research. Furthermore, the authors would like to thank University College Dublin for support with open-access publishing and for providing a supportive research environment during the writing process.
Funding statement
None.
Competing interests
The authors declare none.








 Open access
Open access