


Schizophrenia is a severe mental disorder characterised by persistent cognitive impairment, which substantially contributes to poor functional outcomes and long-term prognosis. Reference Galderisi, Rossi, Rocca, Bertolino, Mucci and Bucci1–Reference Guzman and Harvey3 Consequently, improving cognition and functional outcomes remains a major challenge in schizophrenia treatment. Reference Green, Horan and Lee2,Reference Maric, Jovicic, Mihaljevic and Miljevic4,Reference Marder and Cannon5
Psychosocial interventions, including occupational therapy, play an important role in addressing these functional impairments. There has been increasing interest in personalised or stratified interventions that adapt treatment strategies to individual patient characteristics. Previous research has suggested that baseline clinical characteristics, cognitive function and treatment engagement are important predictors of outcomes in schizophrenia. However, findings across studies remain inconsistent, and most prior research has focused on group-level effects rather than individual-level heterogeneity. Moreover, predictors of longer-term maintenance of gains after discharge have been less frequently examined.
We developed individualised occupational therapy (IOT), a goal-oriented, one-to-one intervention designed to facilitate proactive participation in treatment, enhance cognition and prompt adaptive behaviours in patients with schizophrenia. Reference Shimada, Nishi, Yoshida, Tanaka and Kobayashi6,Reference Shimada, Ohori, Inagaki, Shimooka, Sugimura and Ishihara7 We previously conducted a multi-centre randomised controlled trial demonstrating that adding IOT to group occupational therapy (GOT) during hospital stay led to greater improvements in several cognitive domains compared with GOT alone. Reference Shimada, Morimoto, Nagayama, Nakamura, Aisu and Kito8 A subsequent 2-year follow-up study showed that these improvements were partially maintained after discharge and were associated with reduced risk of readmission to hospital. Reference Shimada, Morimoto, Nagayama and Kobayashi9 Despite these positive group-level findings, substantial variability in individual changes in outcomes was observed, with some patients showing limited benefit or poor maintenance of gains.
Understanding which patients benefit most from IOT, and which components of IOT are associated with better outcomes, is essential for advancing more personalised rehabilitation strategies. However, to date, no study has systematically examined patient-level and treatment-component predictors of changes in outcomes and their maintenance specifically within IOT for schizophrenia. From a prognostic perspective, identifying factors associated with variability in changes in outcomes may help clinicians tailor intervention intensity and content, such as motivational interviews or self-monitoring strategies, to individual patients.
This study conducted a secondary analysis of data from our previous IOT trial and follow-up studies. Reference Shimada, Morimoto, Nagayama, Nakamura, Aisu and Kito8,Reference Shimada, Morimoto, Nagayama and Kobayashi9 The aim was to explore patient characteristics and IOT-related treatment factors associated with changes in cognition and functioning and their maintenance among patients with schizophrenia who received IOT during their hospital stay. By focusing on variability in changes in outcomes, this analysis seeks to provide clinically relevant information to support more personalised occupational therapy approaches in routine schizophrenia care. This study should be interpreted as an exploratory prognostic analysis nested within a randomised controlled trial, focusing on variability in changes in outcomes among participants receiving IOT, rather than on causal treatment effects.
Method
Study design and procedure
This study is a secondary analysis of data from a multi-centre randomised controlled trial and its 2-year follow-up. Reference Shimada, Morimoto, Nagayama, Nakamura, Aisu and Kito8,Reference Shimada, Morimoto, Nagayama and Kobayashi9 This analysis should be interpreted as a single-arm observational prognostic analysis restricted to participants allocated to the GOT plus IOT arm, focusing on predictors of changes in outcomes and their maintenance among those who received IOT. The original study was conducted between December 2021 and October 2024 at Medical Corporation Seitaikai, Mental Support Soyokaze Hospital, Nagano, Japan; Specified Medical Corporation, Hayashishita Hospital, Sapporo, Japan; Kinan Mental Medical Center, Wakayama, Japan; National Hospital Organization Sakakibara Hospital, Mie, Japan; Medical Corporation Okakai, Clinic Day-care Center, Kyoto, Japan; Medical Corporation Yuaikai, Tikumaso Mental Hospital, Nagano, Japan; Iwamizawa Municipal General Hospital, Iwamizawa, Japan; Kobe University Hospital, Hyogo, Japan; Nagoya University Hospital, Nagoya, Japan; Medical Corporation Kawasakikai, Mizuma Hospital, Osaka, Japan; Social Medical Corporation Mikamikai, Higashikouri Hospital, Osaka, Japan; Social Medical Corporation Mikamikai, Higashikouri Second Hospital, Osaka, Japan; Specified Medical Corporation Kyowakai, Kyowa Hospital, Aichi, Japan; and Okayama Psychiatric Medical Center, Okayama, Japan. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration. All procedures involving human participants were approved by the ethics committee of the Japanese Association of Occupational Therapists (approval number 2020001) and each trial site. Written informed consent was obtained from all participants. This study was registered in the University Hospital Medical Information Network Clinical Trials Registry (identifier UMIN000057527).
Following the baseline assessments, the participants were randomised to GOT plus IOT and GOT alone groups. Assessments were conducted at baseline before randomisation, at discharge or 3 months after hospital admission (if the hospital stay exceeded 3 months) and at 1 and 2 years after index discharge.
Participants
This study is a secondary analysis of data from a randomised controlled trial and its follow-up. In the original trial, participants were randomised to receive GOT plus IOT or GOT alone. For this analysis, we included participants who (a) were allocated to the GOT plus IOT arm; (b) received IOT during their hospital stay; and (c) had available outcome data at baseline, post-treatment and at least one follow-up assessment. Participants allocated to GOT alone were not included because they were not exposed to IOT. Accordingly, this analysis does not aim to estimate causal effects of IOT, but to explore factors associated with variability in outcomes among treated participants. A detailed flow of participants from the original trial to each analytic sample used in this study is shown in Fig. 1.
Study flow of participants from the original randomised controlled trial to the analytic samples included in this secondary analysis. Because the present study was a single-arm secondary analysis focused on predictors among participants allocated to the GOT plus IOT arm, only participants in the GOT plus IOT arm are shown. GOT, group occupational therapy; IOT, individualised occupational therapy.

Fig. 1 Long description
The flowchart illustrates the study flow of participants from the original randomised controlled trial to the analytic samples included in this secondary analysis. Initially, 315 participants were assessed for eligibility. Out of these, 247 were excluded due to not meeting inclusion criteria, declining to participate, or other reasons. This left 68 participants who were randomised. Of these, 34 participants were excluded as they were randomised to GOT alone. The remaining 34 participants were randomised to GOT plus IOT. All 34 participants received IOT. Baseline data was available for all 34 participants. Post-treatment data was also available for all 34 participants. At the 1-year follow-up, data was available for 32 participants, as 2 withdrew. At the 2-year follow-up, data was again available for 32 participants, with the same 2 participants having withdrawn.
Post-discharge treatment was not standardised and was provided according to routine clinical practice at each site. Therefore, follow-up outcomes may have been influenced by variations in post-discharge care and environmental factors.
Occupational therapy exposure
IOT consisted of multiple subprograms, including individualised interviews, self-monitoring, psychoeducation, discharge planning and activity-based interventions (e.g. craft activities), each targeting specific domains such as cognitive function, insight, daily functioning and preparation for community living.
IOT exposure was quantified using structured recording forms completed by treating occupational therapists. For each subprogramme, the number of sessions and total implementation time were recorded throughout the intervention period.
To ensure consistency across sites, a standardised intervention manual and common recording forms were developed and used in all participating facilities. Therapists were trained in the IOT protocol and documentation procedures before the study.
Although standardised procedures were implemented, exposure data were recorded by treating therapists, and some degree of measurement variability cannot be excluded.
Details of the occupational therapy interventions are described in our prior studies Reference Shimada, Nishi, Yoshida, Tanaka and Kobayashi6–Reference Shimada, Morimoto, Nagayama, Nakamura, Aisu and Kito8 and in Supplementary Material 1. All participants received usual GOT during their hospital stay. Participants in the GOT plus IOT arm additionally received IOT delivered individually by occupational therapists. After discharge, treatment was provided according to routine clinical practice at each site and was not standardised. This analysis therefore examines predictors of changes in outcomes and their maintenance within the context of naturalistic follow-up treatment.
Outcome measures
Outcome measures were assessed at baseline, post-treatment and at 1- and 2-year follow-up after index hospital discharge. Post-treatment assessments were conducted at different time points depending on the duration of hospital stay. For participants with hospital stays shorter than 3 months, post-treatment assessments were performed at discharge. For those with hospital stays of 3 months or longer, post-treatment assessments were conducted at 3 months after admission, in accordance with the study protocol. Outcome assessors were masked to treatment allocation throughout all assessment time points, including the 1-year and 2-year follow-up assessments. Cognitive functioning was assessed using the Brief Assessment of Cognition in Schizophrenia (BACS). Reference Keefe, Goldberg, Harvey, Gold, Poe and Coughenour10,Reference Kaneda, Sumiyoshi, Keefe, Ishimoto, Numata and Ohmori11 Functional outcome was assessed using the social functioning subscale of the modified Global Assessment of Functioning (mGAF-F). Reference Hall12,Reference Eguchi, Koike, Suga, Takizawa and Kasai13
Additional clinical and psychosocial measures included the Quality of Life Scale (QLS), Reference Heinrichs, Hanlon and Carpenter14–Reference Ryan and Deci16 the European Quality of Life 5 Dimensions 5 Level Version (EQ-5D-5L), Reference Herdman, Gudex, Lloyd, Janssen, Kind and Parkin17,Reference Shiroiwa, Fukuda, Ikeda, Igarashi, Noto and Saito18 the Life Assessment Scale for the Mentally Ill (LASMI) Reference Iwasaki, Miyauchi, Oshima, Murata, Nonaka and Kato19 and the Positive and Negative Syndrome Scale (PANSS). Reference Kay, Fiszbein and Opler20 Details of these measures are provided in Supplementary Material 2. Outcome assessments were conducted by trained assessors who were masked to treatment allocation.
For treatment exposure, the number of sessions and implementation time for each IOT subprogramme were recorded. Reference Shimada, Morimoto, Nagayama, Nakamura, Aisu and Kito8 Implementation time was calculated in 5-min units for each attended session and was rated by the occupational therapists providing the IOT through direct observation. Reference Shimada, Morimoto, Nagayama, Nakamura, Aisu and Kito8
Statistical analyses
Changes in cognitive and functional outcomes were analysed as continuous variables. Changes in BACS and mGAF-F were calculated from baseline to post-treatment (change) and from post-treatment to 1-year and 2-year follow-up (maintenance).
To examine associations between patient- and treatment-related variables and changes in outcomes, linear mixed-effects models were fitted. Random intercepts for study site were included to account for clustering of participants within sites and potential between-site variability in treatment delivery and clinical practice. Separate models were fitted for each outcome and time point (post-treatment change, 1-year maintenance and 2-year maintenance), rather than jointly modelling repeated measurements over time. Candidate predictors considered for inclusion in the models were selected based on clinical relevance rather than solely on statistical significance. Each model included (a) the baseline or post-treatment value of the outcome (BACS and mGAF-F scores), Reference van Dee, Schnack and Cahn21–Reference Silberstein and Harvey23 (b) the illness-related variable (total number of hospital stays, EQ-5D-5L score, physical comorbidities) Reference van Dee, Schnack and Cahn21,Reference DE Hert, Correll, Bobes, Cetkovich-Bakmas, Cohen and Asai24,Reference Dong, Lu, Zhang, Zhang, Ng and Ungvari25 and (c) the treatment-related variable (number of IOT interviews, number of self-monitoring). Additional clinical variables, including illness severity, medication and illness duration, were considered; however, these variables were not included in the final models because of data availability and sample size constraints.
Missing data were handled with a complete-case approach. Participants with available data at each relevant time point were included in the corresponding analyses. As a sensitivity analysis, post-treatment change models were repeated in a restricted sample including only participants with complete data at all assessment time points.
All statistical analyses were conducted using IBM SPSS Statistics version 28.0 for Windows (IBM Corporation, Armonk, New York, USA). All tests were two-sided, and p < 0.05 was considered statistically significant. Given the exploratory nature of this secondary analysis, findings should be interpreted cautiously.
Results
Participant flow
The detailed participant flow and the number of participants included in each analysis are shown in Fig. 1. Among the 68 participants randomised in the original trial, 34 were allocated to the GOT plus IOT arm and received IOT. Of these, 34 had baseline and post-treatment data available and were included in the post-treatment analyses. In addition, 32 participants had 1-year follow-up data and 32 had 2-year follow-up data and were included in the corresponding maintenance analyses.
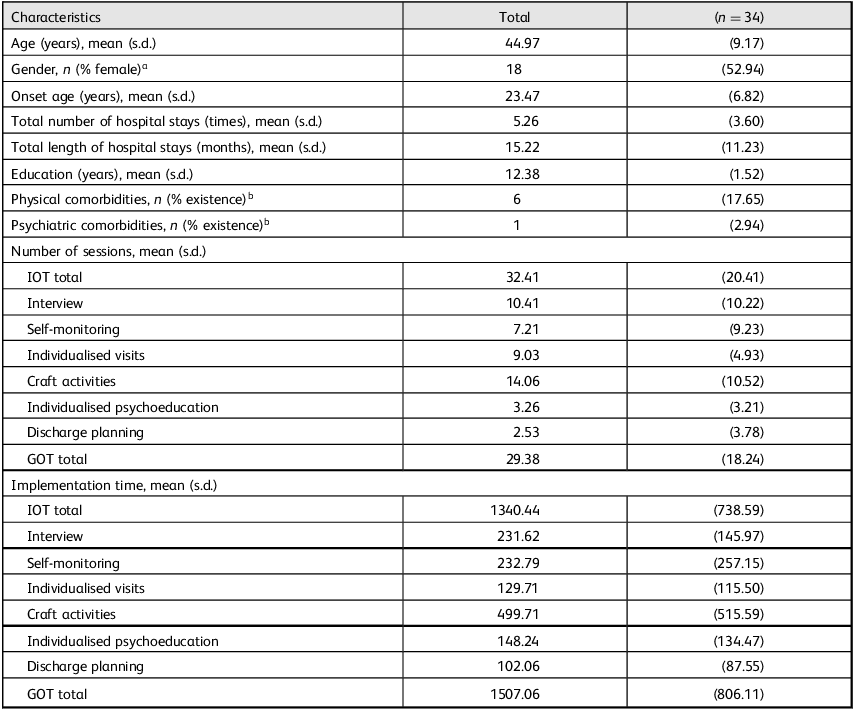
Patient characteristics are summarised in Table 1. The mean age of participants was 44.97 (s.d. = 9.17) years, 52.94% were female and total number of hospital stays was 5.26 (s.d. = 3.60) times. The mean baseline BACS composite and mGAF-F scores were −3.34 (s.d. = 1.40) and 42.06 (s.d. = 9.58), respectively.
Patient characteristics

Table 1 Long description
The table presents patient characteristics with 34 participants. The mean age is 44.97 years with a standard deviation of 9.17 years. 52.94 percentage are female. The mean onset age is 23.47 years with a standard deviation of 6.82 years. The total number of hospital stays is 5.26 times with a standard deviation of 3.60 times, and the total length of hospital stays is 15.22 months with a standard deviation of 11.23 months. The mean education level is 12.38 years with a standard deviation of 1.52 years. 17.65 percentage have physical comorbidities, and 2.94 percentage have psychiatric comorbidities. The table also details the number of sessions and implementation time for various activities such as interviews, self-monitoring, individualised visits, craft activities, individualised psychoeducation and discharge planning.
IOT, individualised occupational therapy; GOT, group occupational therapy.
a. Male versus female.
b. Existence versus no existence.
Changes in outcomes and their maintenance following IOT
Changes in outcomes and their maintenance following IOT are summarised in Supplementary Material 3. From baseline to post-treatment, BACS composite score (mean: 2.35, s.d. = 1.17; p < 0.001), QLS (mean: 4.71, s.d. = 2.68; p < 0.001), EQ-5D-5L index score (mean: 0.15, s.d. = 0.16; p < 0.001), LASMI daily living (mean: −0.72, s.d. = 0.58; p < 0.001), LASMI interpersonal relations (mean: –0.68, s.d. = 0.73; p < 0.001), LASMI work (mean: −1.04, s.d. = 1.60; p < 0.001), LASMI self-recognition (mean: −0.66, s.d. = 0.95; p < 0.001), PANSS total (mean: −24.65, s.d. = 17.93; p < 0.001) and mGAF-F (mean: 8.29, s.d. = 8.31; p < 0.001) showed significant improvement. From post-treatment to 12-month follow-up, LASMI endurance and stability (mean: −0.61, s.d. = 1.30; p = 0.011), LASMI self-recognition (mean: −0.37, s.d. = 0.66; p = 0.003) and mGAF-F (mean: 5.18, s.d. = 6.00; p < 0.001) showed significant improvement. Change from post-treatment to 24-month follow-up in LASMI interpersonal relations (mean: 0.18, s.d. = 0.45; p = 0.029), LASMI endurance and stability (mean: −0.44, s.d. = 1.22; p = 0.045) and mGAF-F (mean: 5.09, s.d. = 6.58; p < 0.001) showed significant improvement, whereas PANSS total increased significantly (mean: 6.46, s.d. = 7.60; p < 0.001), indicating a potential worsening of symptoms.
Predictors of changes in outcomes and their maintenance following IOT
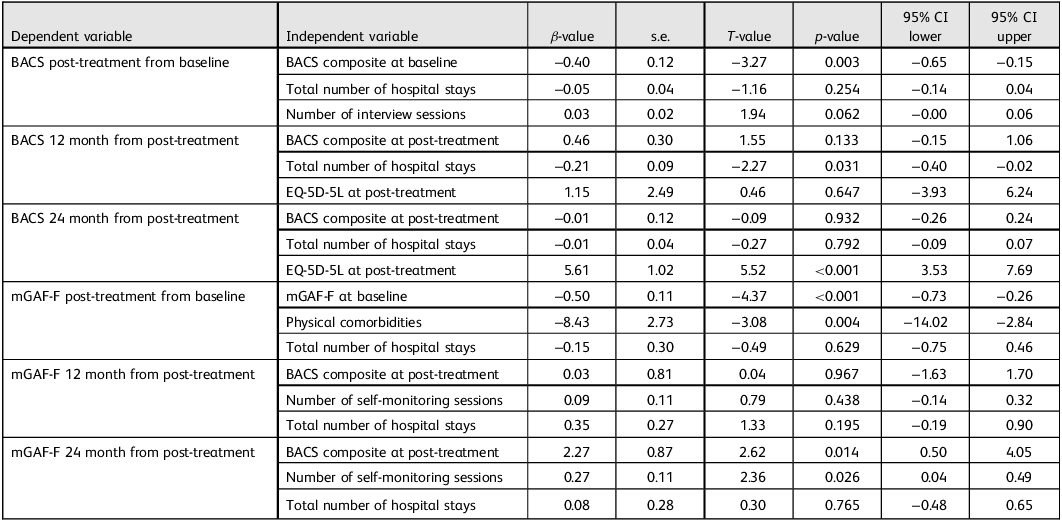
Associations between patient- and treatment-related variables and changes in outcomes are summarised in Table 2. Greater cognitive improvement from baseline to post-treatment was associated with BACS composite at baseline (β = −0.40, 95% CI −0.65 to −0.15, p = 0.003). Maintenance of cognitive improvement at 12 months was associated with total number of hospital stays (β = −0.21, 95% CI −0.40 to −0.02, p = 0.031). At 24 months, EQ-5D-5L at post-treatment was associated with maintenance of cognitive improvement (β = 5.61, 95% CI 3.53–7.69, p < 0.001). Greater functional improvement from baseline to post-treatment was associated with mGAF-F at baseline (β = −0.50, 95% CI −0.73 to −0.26, p < 0.001) and physical comorbidities (β = −8.43, 95% CI −14.02 to −2.84, p = 0.004). Maintenance of functional improvement at 24 months was associated with BACS composite at post-treatment (β = 2.27, 95% CI 0.50–4.05, p = 0.014) and number of self-monitoring sessions (β = 0.27, 95% CI 0.04–0.49, p = 0.026). In the multivariable models for 12-month functional maintenance, no predictors remained statistically significant.
Linear mixed-effects models of predictors of cognitive and functional changes

Table 2 Long description
A table with six rows and nine columns presents linear mixed-effects models of predictors of cognitive and functional changes. The columns include dependent variable, independent variable, beta-value, standard error, T-value, p-value, 95% CI lower and 95% CI upper. The table examines changes in BACS and mGAF-F scores from baseline to post-treatment and at 12 and 24 months post-treatment. Key predictors include BACS composite at baseline, total number of hospital stays, EQ-5D-5L at post-treatment, mGAF-F at baseline, physical comorbidities and number of self-monitoring sessions. Notable trends include significant associations between cognitive improvement and BACS composite at baseline, and functional improvement with mGAF-F at baseline and physical comorbidities.
BACS, Brief Assessment of Cognition in Schizophrenia; EQ-5D-5L, European Quality of Life 5 Dimensions 5 Level Version; mGAF-F, Modified Global Assessment of Functioning – social functioning subscale.
A sensitivity analysis restricted to participants with complete data at all assessment time points (n = 32) showed broadly similar patterns of associations, supporting the robustness of the findings (Supplementary Material 4).
Discussion
Main findings
This study examined patient characteristics and treatment-related factors associated with changes in cognitive and functional outcomes and their maintenance following IOT. To our knowledge, this is the first study to explore predictors of variability in changes in outcomes within IOT in schizophrenia.
Greater improvement in cognitive function was associated with lower baseline cognitive performance, suggesting that patients with more severe cognitive impairment may have greater capacity for improvement. This finding is consistent with previous studies in cognitive remediation indicating that individuals with lower baseline cognition may show larger gains. Reference Tan, Zhu, Fan, Tan, Yang and Wang26–Reference Saperstein, Choi, Jahshan, Lynch, Wall and Green28 In addition, greater engagement in individualised interviews was associated with greater cognitive improvement, which may reflect the role of therapeutic interaction and motivation in facilitating cognitive change. Reference Fervaha, Zakzanis, Foussias, Graff-Guerrero, Agid and Remington15,Reference Le, Ventura, Subotnik and Nuechterlein29
Maintenance of cognitive improvement at 12 months was associated with fewer prior hospital stays, suggesting that illness chronicity may influence the sustainability of treatment effects. At 24 months, better post-treatment quality of life was associated with maintenance of cognitive improvement, consistent with previous findings linking cognition and quality of life in schizophrenia. Reference Sigaudo, Crivelli, Castagna, Giugiario, Mingrone and Montemagni30,Reference Ehrminger, Roux, Urbach, André, Aouizerate and Berna31
Greater improvement in functional outcomes was associated with lower baseline functional level and absence of physical comorbidities. These findings suggest that both baseline functional severity and physical health status may influence functional gains. These results are consistent with previous findings that patients with more severe baseline impairment may demonstrate greater improvements following rehabilitation interventions. Reference Vita, Barlati, Ceraso, Nibbio, Ariu and Deste27,Reference Lejeune, Northrop and Kurtz32,Reference Sampedro, Peña, Sánchez, Ibarretxe-Bilbao, Iriarte-Yoller and Pavón33
Maintenance of functional improvement at 24 months was associated with better post-treatment cognitive performance and greater engagement in self-monitoring. These associations may reflect the importance of cognitive function and metacognitive processes in sustaining functional recovery over time, as supported by previous literature. Reference Galderisi, Rossi, Rocca, Bertolino, Mucci and Bucci1,Reference Green, Kern and Heaton34,Reference Mohamed, Rosenheck, Swartz, Stroup, Lieberman and Keefe35 The association between self-monitoring and maintenance of functional improvement may reflect the role of metacognitive and self-regulatory processes in long-term recovery. Reference Lysaker, Shea, Buck, Dimaggio, Nicolò and Procacci36,Reference Waters, Woodward, Allen, Aleman and Sommer37
Strengths and limitations
This study provides clinically relevant insights into factors associated with variability in changes in outcomes following IOT, which may inform more personalised rehabilitation strategies. Identifying patient and treatment characteristics associated with greater improvement may help tailor intervention intensity and content to individual needs. Personalised medicine is increasingly recognised as an important approach in schizophrenia care, and tailoring interventions based on patient characteristics may enhance treatment effectiveness. Reference Sampedro, Peña, Sánchez, Ibarretxe-Bilbao, Iriarte-Yoller and Pavón33,Reference Medalia, Saperstein, Hansen and Lee38 Adaptive trial designs, such as the Sequential Multiple Assignment Randomised Trial, may be useful for future studies aimed at optimising personalised intervention strategies. Reference Kidwell and Almirall39
Several limitations should be noted. First, this was a secondary analysis restricted to participants who received IOT and had available outcome data, which may limit generalisability. Second, this study was designed as an exploratory prognostic analysis, and findings should be interpreted as associations rather than causal effects. Third, post-discharge care was not standardised and may have varied across participants and sites, which could have influenced long-term outcomes. Fourth, the timing of post-treatment assessments varied across participants depending on the duration of hospital stay, which may have affected comparability. Fifth, intervention exposure was recorded by treating occupational therapists, which may have introduced measurement variability. Finally, the sample size was modest, and the findings require replication in larger studies.
In conclusion, both patient characteristics and engagement in specific IOT components were associated with variability in changes in outcomes and their maintenance. These findings may support more personalised occupational therapy strategies for schizophrenia, but require replication in larger samples.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1192/bji.2026.10109
Data availability
The data that support the findings of this study are available from the corresponding author, T.S., upon reasonable request.
Acknowledgements
The authors thank the following individuals: Naoko Nakamura, Kaori Aisu, Aki Kito, Ryo Kojima, Ayumi Yamanushi, Kojiro Kawano, Noriaki Hikita, Kayano Yotsumoto, Tomoe Ebisu, Masashi Kawamura, Takao Inoue, Junya Orui, Tatsumi Asakura, Masafumi Akazawa, Seika Sato, Machiko Irifune, Koji Kunita, Shoko Ito, Ami Koizumi, Aya Makabe, Sonoko Miyasaka, Fumiko Natsumi, Yumi Tanaka, Mihoko Nishitani, Emiko Kobayashi, Yurika Nishida, Saori Haga, Atsushi Kimura, Yuki Kurihara, Yuko Nishimura, Aiko Hoshino, Jun Nishino and Shuhei Fujita.
Author contributions
T.S. contributed to study conceptualisation, data curation, formal analysis, methodology, project administration, software, validation and visualisation. T.M. contributed to study conceptualisation, project administration and validation. H.N. contributed to study conceptualisation, formal analysis, project administration and validation. M.K. contributed to study conceptualisation, methodology, project administration, supervision, validation and visualisation. All authors wrote the original draft and reviewed and edited the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.