

International Medical Graduates: An Overview
The broadening of international professional and educational networks has seen both medical students and qualified professionals aspire to work and train overseas. Having attained their primary medical qualifications, international medical graduates (IMGs) migrate abroad, typically to high-income nations, generally seeking both personal fulfillment and professional development. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1) Correspondingly, many developed countries such as Australia require the recruitment and employment of IMGs to address current and projected clinician shortages (Reference Healey, Fakes and Nair2) as national populations continue to climb. It is estimated that one in three doctors currently working within Australia and the UK, and one in four American doctors are foreign-trained. (Reference Healey, Fakes and Nair2) Following re-accreditation within their country of emigration, IMGs tend to work in undersupplied or lower-paying specialities, and are increasingly over-represented in primary care and family medicine. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1; Reference Smith and Parkash3) They often find employment in densely populated, socio-economically disadvantaged areas or rural communities, which typically are less sought by domestically trained doctors. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1) While an increasingly demanding career, the difficulty of medical practice for IMGs is compounded by other factors with which domestic physicians may not have to contend – specifically racial discrimination, professional inequity and disadvantage, and sexism.
Challenges in acculturation shape the experiences of IMGs. Manageable hurdles such as language barriers are often complicated by cultural insensitivity, overt racism and institutional discrimination. (Reference Al‐Haddad, Jamieson and Germeni4) This may be instigated and perpetuated within the administration, as well as by colleagues and patients. (Reference Healey, Fakes and Nair2; Reference Filut, Alvarez and Carnes5) IMGs consistently cite differences in ethnicity and language as a basis for the discrimination they encounter. (Reference Szafran, Woloschuk, Torti and Palacios Mackay6) Contending with nuances of non-verbal communication, such as hand gestures or facial expressions, dialects, accents, (Reference Triscott, Szafran, Waugh, Torti and Barton7) and unfamiliarity with vernacular terms, in turn exacerbates the IMGs’ difficulty to achieve effective communication. This causes reluctance by some to contribute to discussions. They in turn feel apprehensive that their limited participation may be misconstrued for lack of medical knowledge or even incompetence. (Reference Al‐Haddad, Jamieson and Germeni4) Such communication issues heighten the isolation of IMGs within the professional environment by making it difficult to socialize, achieve a sense of inclusion, forge genuine friendships and ultimately successfully integrate into their collegial community. (Reference Al‐Haddad, Jamieson and Germeni4; Reference Al‐Haddad8)
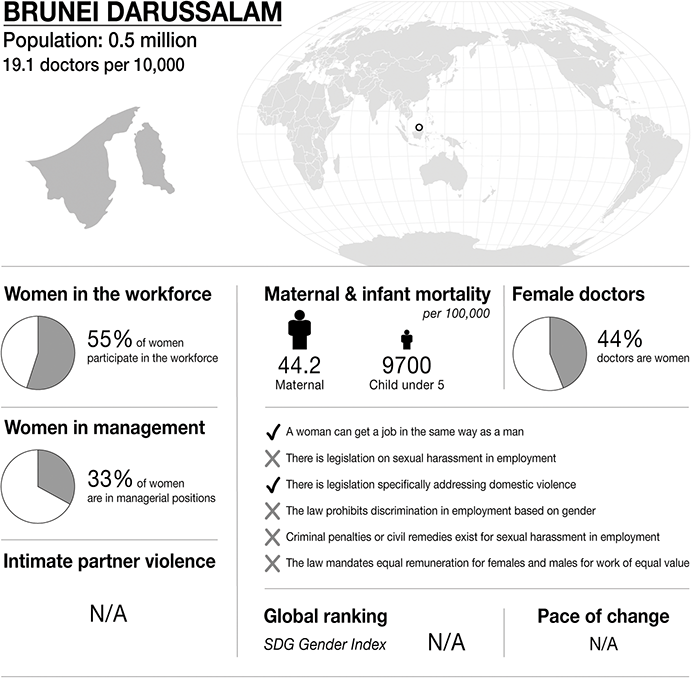
Infographic Brunei. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality
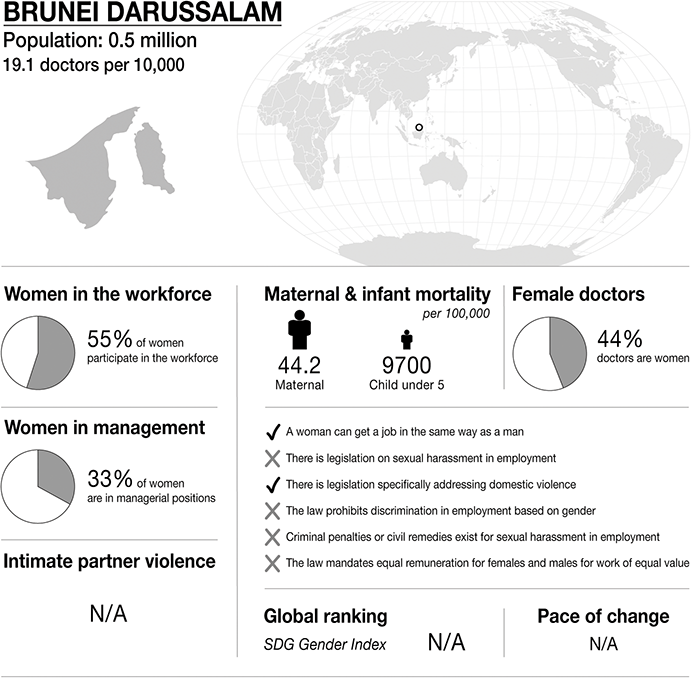
Figure 20.1 Long description
The infographic provides information about Brunei Darussalam, with a population of 0.5 million and 19.1 doctors per 10,000 people. It highlights several gender-related statistics. 55 per cent of women participate in the workforce. 33 per cent of women are in managerial positions. Maternal mortality is 44.2 per 100,000. Infant mortality under 5 is 9700 per 100,000. 44 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In (country):
– a woman can get a job in the same way as a man.
– there is legislation specifically addressing domestic violence.
– there is no law that prohibits discrimination in employment based on gender.
– there is no legislation on sexual harassment in employment.
– there are no criminal penalties or civil remedies for sexual harassment in employment.
– there is no law mandating equal remuneration for females and males for work of equal value.
There is no S D G Gender Index global ranking available.
Over and above the demands of the mandatory requirements of the IMG training environment, instances of intimidation and harassment serve to increase their distress, impact their morale and intensify workplace dissatisfaction, (Reference Crutcher, Szafran, Woloschuk, Chatur and Hansen9) ultimately contributing detrimentally to the IMGs psychological health. (Reference Schut10) The psychological repercussions of contending with such intimidation and harassment are significant, as doctors struggling with mental illness are at increased risk of making errors and impacting the potential quality of their patient care. (Reference Crutcher, Szafran, Woloschuk, Chatur and Hansen9) Furthermore, the presence of actual or perceived ‘medical inferiority’ bias can intensify the IMGs sense of alienation, with some IMGs’ stating that they felt ‘overly observed’ and critiqued compared to their domestic peers. (Reference Al‐Haddad, Jamieson and Germeni4) Subsequently, they felt greater pressures to perform. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1) Such examples of microaggression may subsequently translate to inequities of promotion opportunities as well as biased performance reviews. (Reference Filut, Alvarez and Carnes5) Managing such experiences may then be associated with increased distress and compounded workplace dissatisfaction, ultimately compromising their mental health and wellbeing. (Reference Filut, Alvarez and Carnes5)
The professional development and career progression of IMGs may also be disproportionately impacted. IMGs have been found (on average) to have poorer academic achievement (Reference Woolf, Viney, Rich, Jayaweera and Griffin11) and lower pass rates for postgraduate exams. (Reference Al‐Haddad, Jamieson and Germeni4; Reference Al-Haddad, Mulholland and Gardner12) As a result, they are less likely to achieve board certification (Reference Al‐Haddad, Jamieson and Germeni4) compared to the domestic medical graduates. Disparity also exists among IMGs who completed their education in developing countries compared to those who trained in developed nations, with the former more likely to experience marginalized career outcomes. (Reference Schut10) A number of factors explain the causation of this marginalisation; in general terms, this group’s experiences are compounded by a range of disadvantages including the less favourable conditions of skilled migration policies and the potential scepticism regarding the standard of their medical education. (Reference Schut10) The uninformed or biased perceptions of their cultural or linguistic dissimilarities to domestic physicians often work to make the IMGs appear less qualified. (Reference Schut10) This is in turn reflected in lower degrees of career satisfaction and perceived lack of collegial support as reported by IMG physicians. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1; Reference Smith and Parkash3; Reference Katakam, Frintner, Pelaez-Velez and Chakraborty13)
IMGs often experience limited autonomy in regards to their geographical area of practice, which may further impact on their opportunities for future training and research prospects. This may impede their career progression and financial security. It may also widen the inequities in career pathways and may generate uncertainty concerning their career sustainability. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1) Additionally, it may heighten their stress levels, exacerbate their social isolation and impact their self-esteem – all factors increasing the vulnerability of IMGs to experiencing burnout. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1) The influence of medical inferiority bias and cultural racism is also purported to limit the advancement of IMGs within academic medicine. The ‘incongruence of diversity between lower-level faculty and senior leadership’ creates a sense of disenfranchisement within the work environment. This potentially may lead to professional dissatisfaction and necessitate the recalibration of one’s ambition to pursue academic leadership roles. (Reference Smith and Parkash3) Acquiescing to this disadvantage in career progression is commonplace and is seen as the ‘cost of being an immigrant’. (Reference Smith and Parkash3)
The aforementioned challenges may be intensified for female IMGs, with gender proving an additional basis for discrimination. (Reference Smith and Parkash3; Reference Szafran, Woloschuk, Torti and Palacios Mackay6) This may especially occur in male-dominated specialities. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1) Female IMGs and their domestic counterparts are subject to sexist commentary and sexual harassment by clinicians, faculty and patients. This is further experienced with regards to pay inequality, general under-recognition, as well as gender-based stressors associated with role conflicts or biases. (Reference Bhugra, Smith, Ventriglio, Rao, Ng and Javed1; Reference Dellasega, Aruma and Andreae14) Female doctors often report a lack of respect for their authority. They highlight instances of being passively verbally dismissed by male colleagues, addressed by their first name as opposed to their male peers who are typically addressed by title, (Reference Dellasega, Aruma and Andreae14) or not having their position of authority as an educator respected by trainees and students. (Reference Triscott, Szafran, Waugh, Torti and Barton7) Additionally, their professional advancement has been impeded by incidences of differential or less affirming recommendations for faculty positions compared to male peers.
Female physicians may also encounter gendered stigma. They experience conflict in their life choices like pregnancy which may disrupt their training or influence their application for positions. Many are also concerned by the inadequacy of maternity leave options in relation to their career planning. (Reference Dellasega, Aruma and Andreae14) Exclusion from leadership roles is another major factor inhibiting their professional aspirations and further diminishes their potential for professional fulfillment. (Reference Dellasega, Aruma and Andreae14)
However, it is equally important to recognise that male IMGs may also experience gender-based challenges. This is commonly due to cross-cultural differences, in their communication styles, their professional expectations of themselves as doctors and the way they are treated by patients and colleagues. Similarly, IMGs who have not received education or training in the care of particular marginalised communities, including LGBTQIA+ patients may subsequently encounter professional difficulties, which in turn may affect their patient care. (Reference Triscott, Szafran, Waugh, Torti and Barton7)
It could be said that one’s choice to become a medical practitioner means that an individual is predestined to be challenged in many ways. Notwithstanding the intensity of the intellectual demands of this academic path and subsequent professional training, there also lies the complexity of functioning as a competent practitioner in the various professional settings. Navigating the professional and social networks of these environments is onerous at the best of times. However, for IMGs these challenges are compounded by a number of factors which combine to often negatively effect and indeed impede their professional journey with regards to their training and employment. Consequently, the nature of these challenges may bring with them potential negative impacts upon IMGs’ performance, their retention within the profession, and just as importantly, their overall wellbeing.
AN ANONYMOUS CASE STUDY FROM BRUNEI
Background
I come from Brunei, but ethnically I’m mostly Chinese. Brunei is a funny, little country. It’s so little that almost everyone knows everyone in one way or another, to the point where we recognize their car number plates. And people talk … a lot … about everyone. Probably because there’s not much to do. It is a Muslim country. Alcohol is not available for sale anywhere in the country, but you can bring your quota into the country for private consumption as long as you are not a Muslim. So there are no bars or clubs, and there is not much in the way of night life.
Brunei’s main resource is oil, so a lot of the expats in Brunei work in the oil and gas industry, just like my dad, though he’s not an expat. I hung out with a lot of my dad’s colleagues’ kids. Kids from England, Holland, France, USA, Australia, New Zealand, and the list goes on. There’s a little community of us, us families of the oil and gas industry, who are all members of a recreational club which has a few restaurants, pools, a gym, tennis courts, a golf course, basketball courts, badminton, squash, football fields, and a sailing club, and it’s on a beach. Spouses of the employees often ran particular social and enrichment groups such as aerobics, performing arts, silk painting, crochet, etc. Within this club, it seemed as if the rules that people normally follow in Brunei didn’t exist. I didn’t have to worry about wearing short shorts or a bikini because everyone else was dressed the same and no one looked at you twice. Outside though, that’s a different story. It is frowned upon for women to expose their decolletage, back, shoulders, midriff and thighs. Even if you cover up, people still stare at you because you might have a pretty face, nice hair or a desirable body shape. Interestingly though, most Bruneians are respectful and reserved.
You could say that I grew up in a mixed culture. I had ‘white’ friends who would greet you with a kiss on the cheek, and Asian friends who would greet you with a wave or a handshake. I adapted to both and changed my demeanor and accent depending on the company I was with. There is a certain behaviour that is expected of you as a child in the company of adults. You would always call an older person auntie or uncle, even if they are not related to you in any way. It’s just respectful. Back chatting, raising your voice or swearing is forbidden and will be met by physical punishment at home.
Now, why is this relevant? Because what you see on the outside is a far cry from what happens behind closed doors. I clearly recall many instances of domestic violence between my parents from the time I was about six years old. None of which I was allowed to speak of. I had to ‘save face’. But I was desperate. I needed my mum to get out of there. I honestly thought she was going to die at the hands of my dad. I came up with all sorts of ideas such as her moving back to Singapore and taking me and my brother with her, but she said she couldn’t financially support us and had to endure more of my dad’s abuse, just to give us the life she wanted us to have. I eventually told my paternal grandmother’s maid. I figured that she’s no relation to the family and therefore could find a way to help discreetly. She told my paternal grandmother and my dad’s sister who spoke with me about it. Unfortunately, my mum denied it and told me off about it saying I should never tell anyone anything.
Some time before I turned ten, my brother molested me. What I understood at the time was that he was ‘teaching me’. This included French kissing, what pubic hair looks like, finding my ‘hole’ (vagina), and how a penis gets hard. It felt wrong but I didn’t know it was wrong until a few years later. I didn’t know what it was called. I later learnt that it was really bad and I would get into a lot of trouble if anyone found out so I kept my mouth shut, out of embarrassment.
There aren’t any positive adjectives to describe my teenage years. I got into a lot of trouble with my parents as I rebelled. I was manipulated by my brother to think that he was the only person in the world who had my back so I took the blame for a number of things to protect him. I lied to my parents. My dad lost trust in me, but I never trusted him after seeing what he put my mum through. It was a terribly confusing time for me.
Medical Education
I knew from a young age exactly what I didn’t want in life. I had to leave Brunei. My parents were living a double life. A life that was perfect from the outside, but so, so horrible on the inside. We were playing pretend and I couldn’t be myself. I vowed to become financially independent from anything and anyone, so that I would never find myself in a situation similar to my mum’s. Doctor. That’s what I would be. Doctors are respected. It’s a prestigious profession. I would be untouchable. I had my first excuse to leave Brunei. I applied to London universities, the furthest away from Brunei my parents would let me go to, and I got in. I left Brunei alone with one overweight suitcase and one backpack. I brought my favourite pillow, a ridiculously large duvet because my mum was worried I would get cold, a tiny, one-cup rice cooker and slow cooker my mum bought me, and essential clothes and toiletries. I had only been to London once before to attend interviews for entry to medical schools, but I was confident that I would find my way to the halls of residence and uni with a map of London and the London Underground. I was on my way to be free from pretending. To be me.
Finding me, now that was one hell of a journey. What I discovered was that I yearned for acceptance by any means possible. I did what I thought would make people like me, from doing ridiculous dares to paying for meals or rounds or drinks. I had a father, but I didn’t have a father figure, someone I looked up to and could rely on, so I had boyfriends instead. Oh, and I clung on to them. I needed to be loved so badly. I met my most significant boyfriend at uni, and he is still a good friend of mine today. I have him and his family to thank for saving me when I was probably the most mentally unstable. He protected me when I was so vulnerable. We weren’t meant to be, but we still care deeply for each other.
I knew exactly what I didn’t want in a man. He had to be the exact opposite of my dad. He had to be non-Asian, a Christian or Catholic, open-minded and have a less prestigious profession to mine.
Sexual Harassment
Working as a junior doctor in London was character-shaping. A huge learning curve. On the first Wednesday in August every year, all the junior doctors move up a rank. For all med school leavers, this was the first day as an intern, and the previous interns to become a junior house officer, and so on. We were allowed to select our hospital preferences, but we were not guaranteed to get our first preference. I ended up in a hospital in northeast London. It was a beautiful, brand new hospital at the time and they put us interns up in lovely new apartments not far away. I didn’t know anyone. My external persona of confidence was built to hide my utter lack of it. I wanted to please people and to be liked. I was friendly with everyone and went to as many social gatherings as I could. All the interns and most junior doctors were lovely. The more senior doctors, on the other hand, they were, in general, scary people. I was certainly intimidated by them. There was a bullying culture because they had done the hard yards and felt they had the right to treat us the way they were treated.
On my surgical rotation, the specialist registrar on my team was doing some sort of study. It involved reviewing patients’ charts and collating data. He asked me to help, which I was more than happy to do. There was a little room full of patients’ charts and both of us went in. Everything happened so quickly. He locked the door behind us and pushed me down on the bench, started kissing me, licking my face and touching my body. I froze. Then rattling and a knock on the door. I pushed him off, jumped up and tried to open the door. You know how in movies, you see the poor victim trying to get away from the bad guy, and she can’t even put the key in the ignition of the car, and you’re screaming at the TV telling her to just slow down and the key would go in? That was exactly what it was like. I could not turn the lock and push the handle. I was fumbling. Panicking. I eventually got out after a few seconds, but it felt a lot longer than that. My friend was outside and I just ran in the opposite direction of that room and she followed me. Far enough away, I told her what happened. She immediately told me to report it, but I just wanted to go home. I tried to process what happened and work out what to do. I had to go back the next day and work with this guy. I wondered whether I would be taken seriously. I mean, this guy was a specialist registrar. He was basically the second in charge to the consultant. No one who needed to believe me would believe me. And even if they did, would they even class this as a reportable event? He didn’t rape me. He just kissed, licked and touched me. Was I being a sissy? Maybe it was my fault. Yes, that’s what it was. I was friendly with him and joked around, and maybe he got that vibe from me. It must be my fault. I will learn from this and try to be less friendly next time. So I didn’t report it. I acted like nothing happened and it was bloody awkward. He spoke to me the following day and apologized, saying that he didn’t know what came over him and to please not tell anyone. I shrugged it off and said, ‘Meh, no big deal. Forget about it’, but inside I just wanted to scream at him. I had to work under him for the next few months, which was really hard. Thankfully, I had the support of a colleague whom I had grown very close to as we worked on the same ward.
I moved to Brisbane in 2008 and worked at several different hospitals as part of the training process. I thought that there wouldn’t be much adapting to do as both countries speak English, cultures are pretty similar and medicine is medicine, right? Wrong! The culture shock moving from London to Brisbane was huge compared to the move from Brunei to London. Who would have thought? I struggled to understand Australian English because of the accent and the slang. Older Australians had a hard time understanding my British accent, so I forced myself to learn common Australian phrases, slang and eventually spoke with an Aussie accent. Medicine was hard too because guidelines, protocols, reference books, processes and procedures were different. Heck, even the use of brand names for medications was new to me. I looked like an idiot on a cardiology ward as an SHO asking what Cartia was. Oh, it’s just aspirin, but at 100 mg, not 75 mg? So I did what I felt I had to do and clinged to more senior doctors who would non-judgmentally guide me. Did they? Not really. Ridicule was commonplace. There were a handful who I thought were really helpful, but little did I know this was a recipe for assault.
There were many instances of inappropriate behaviour by more senior male doctors such as touching my inner thigh during grand rounds or meetings, sniffing my hair and neck, touching or squeezing my buttocks in the presence of a patient so I couldn’t do anything, undoing my bra clasps as a joke and many inappropriate text messages including one from a professor late at night asking to sleep next to me because his wife was on her period! After I refused, he treated me totally differently at work. He didn’t look at me and didn’t speak to me, instead of sharing jokes and laughing together which we used to do. I kind of felt guilty and almost sorry for him. It wasn’t long before he left the hospital suddenly and unexpectedly.
At one stage, I was working as Principal House Officer in an emergency department. I was seriously considering joining the training programme so I spent eighteen months working there and improving my skills and knowledge. My husband had been hobby home brewing for a number of years. One of the emergency consultants who had just resigned to return to his home country knew about this and asked if my husband could provide a keg for his son’s end of school party at their house and join in the fun, which he was more than happy to do. The emergency consultant’s wife and other kids were already overseas. We arranged to spend the night there with our three kids, knowing that we were going to be drinking. We had a ball. Our kids enjoyed swimming and playing games; then it was their bed time. We showered and put our kids to bed upstairs and we continued with the party. When the night was over, we headed to bed in our designated room. I fell asleep quickly with my husband next to me, but then I woke up to someone touching me. It was the consultant. He was kneeling on the floor beside me, stroking my buttocks and vulva and he put his fingers inside of me. I couldn’t move. I don’t know why. I felt sick. I know I said ‘Stop’ a number of times, but my voice was so weak. I heard him say, ‘Oh c’mon, you know you want this. You know I’ve always had a thing for you and I know you want me. Well, now you can.’ In my head I was thinking … Um, no! I thought we were just colleagues. You were my boss. I could hear him saying, ‘Mmmmm you are so fucking gorgeous and your pussy just gets me so fucking hard’, while he grabbed my hand and put it on his penis and with his other hand he continued molesting me. I elbowed my husband to try to wake him because my weak voice asking him to stop or asking for help didn’t get me anywhere. He just kept going. Again, I said, ‘Stop’, and elbowed my husband, told him to get out. It stopped. My husband fell back asleep. But my heart was pounding. Confused. Scared. Dirty. Disgusted. Angry. Asking myself what I did to make him think I felt that way towards him, or what I did to make him think he could do that to me.
Our kids came to our room in the morning and I had to act like normal Mummy. My husband had to transport his equipment back home. There wouldn’t have been enough space for all of us and his equipment in the car. He brought the equipment home and came back to get me. In the time he was gone, I was scared out of my mind. My kids desperately wanted to go for a swim again so I headed out of my room, down the stairs to watch them as they swam. I couldn’t believe it. The consultant acted like nothing happened. Nothing at all! I ignored him. It was so awkward. When I left with the kids, I was so relieved but yet I burst into tears almost as soon as I got in the car.
The consultant tried to keep in touch by sending me text messages and emails, but I never responded. Even his son tried to get in touch. I assume he didn’t know what happened and was confused as to why I didn’t want to have anything to do with them anymore.
This was a turning point for me. After this point, I stopped being friendly to any male doctor, I smiled less and I stopped attending social events organized by hospital colleagues.
I couldn’t stay in the hospital system any longer. In Australia, an International Medical Graduate is under a ten-year moratorium, where they have to work in a district of workforce shortage for ten years. This is scaled depending on how rural your placement is. The further away from the city you go, the less time you have under your moratorium. London to Brisbane was tough, but moving out to the country … man, that’s something else! Who would have thought that all you had to do to gain the trust of the local farmers as their doctor is to talk about the weather! So not only was I speaking differently and using words that don’t exist in the English dictionary, but the content of my conversations also had to change quick smart!
I specialized in general practice. I put everything I had into passing those exams: all my energy, time, and what felt like all the money I had. I turned all my anger and frustration into becoming a GP and I made it. I was my own boss. I took control.
I put everything behind me and moved on. I put on a hard, headstrong exterior so that I would never find myself in a similar situation again. I compartmentalized my past experiences and didn’t own them. Me writing this … this is me starting to own my experiences. It’s been such a difficult process. Until now, I didn’t recognize those events as assault. I recently asked my best friend from the London hospital I first worked in if he thought I came across as a slut. He was surprised and wondered why I would ask such a question. I told him about this book, which has made me reflect on my past. I did wonder why it kept happening to me because I was the common denominator. Surely there’s something in my persona or a big sign saying ‘slut’ on my forehead, I thought. My friend reassured me that I did nothing wrong, except maybe trust people too easily. I also learnt through the process of writing this that I’m really not alone, that this happens to so many people.
Brunei is a very safe country and the people are generally respectful. My trusting personality may have stemmed from this false sense of security, not truly understanding that there are real predators out there. My insecurity from growing up without a father figure, believing my brother that he was the only person who would look out for me and that we had a secret only he and I knew, and truly thinking I was ugly made me want to make up for these insecurities by being overly friendly and overly generous, which most likely led others to take advantage of this. As a foreign-trained doctor in Australia, I was further disadvantaged in a system I did not yet understand, and in a country where the culture and language were so unfamiliar.
Being a young, female, Asian GP, I filled my appointment book quickly. Managing mental illnesses in my patients is a big part of my day. For the most part, my past experiences helped me understand what my patients were going through, but there were times when I was guilty of thinking, ‘If only I could tell you that I get it because I’ve been there’, or ‘Oh, cry me a river! I’ve had to go through way worse’, or even a bit of jealousy that they are getting the help they need from their family and a doctor like myself, which I didn’t have access to. There were many, many other consultations that did bring up some painful memories and I had to act my way through it. Imagine trying to support someone when you haven’t had the support yourself. I have said goodbye to patients, shut the door, and just cried in my room, then get myself together before I run too late, and call my next patient in with a smile on my face. By the end of the day I’m pooped. I have nothing left to give to my family. I’ve become pretty good at leaving work at work so much so that when my husband asks how my day was, I will often reply with, ‘I can’t remember. Must have been okay.’
I had to do better. I learnt more about mental illness and available resources that may help my patients, which I used myself. Although my past experiences were traumatic, I don’t think I would be the doctor I am today otherwise. What strikes me as odd is the lack of support given to International Medical Graduates for their own mental health and wellbeing. As it is, we come into the country with nothing but a medical degree and we’re told to go forth and work in this health system, as long as it’s in a rural area where the availability of support, on-the-job training, and connections is limited and the spoken language and culture is different.
I wish for medical educators to encourage all doctors and medical students to read this book. Know that this happens. Don’t be a predator. Don’t let yourself fall victim to a doctor who thinks they have power over you and the ability to silence you. If you do, know that you’re not alone and it’s not your fault. It never was.

 Open access
Open access