


Introduction
Antimicrobial resistance is a major public health problem, 1 and infections caused by antimicrobial-resistant organisms are associated with a longer hospital stay and higher mortality rate than those caused by antimicrobial-susceptible organisms. Appropriate antimicrobial use is vital to ensuring treatment efficacy and reducing unnecessary exposure, thereby decreasing adverse events and selective pressure on pathogens. Antimicrobial stewardship (AS) reduces antimicrobial use without increasing mortality and helps prevent the emergence of resistant organisms, including Clostridioides difficile. Reference Davey, Marwick and Scott2–Reference Tamma, Miller and Dullabh5
Guidelines recommend discontinuing antimicrobials after 72 hours absent clear evidence of infection requiring therapy. Reference Morgan, Croft and Deloney6 The Centers for Disease Control and Prevention (CDC) also encourage reassessing the need to continue antimicrobial therapy after the initial treatment period. Reference Pollack and Srinivasan7,8 However, this reassessment is often not performed even when additional diagnostic information becomes available. 8
Antimicrobial time-out is an AS intervention that prompts reassessment of several parameters—the appropriateness of the diagnosis, choice of drug, dosage, administration route, and treatment duration at a predefined time point (generally 48–72 h) after its start. The pharmacist-led variant—in which a pharmacist alerts the prescriber to trigger reassessment—has been endorsed by the Infectious Diseases Society of America and the CDC as highly feasible. 8,Reference Barlam, Cosgrove and Abbo9 However, previous studies of the time-out approach have produced inconsistent findings. Reference Thom, Tamma and Harris10–Reference Taylor, Coe, Stevenson, Wardlow, Boghdadly and Reed12 One study that implemented time-out by department found pharmacist-led time-out associated with reduced vancomycin use in the emergency and surgery departments but showed no significant change in other departments. Reference Hasegawa, Tagashira and Murakami13 This department-dependent response suggests that a time-out’s efficacy may vary by department and ward rather than producing uniform reductions across clinical areas.
Intravenous vancomycin, a glycopeptide antibiotic, is the main treatment for gram-positive infections, including those caused by methicillin-resistant Staphylococcus aureus (MRSA). The drug is also widely used as empirical therapy when a healthcare-associated infection (HAI), such as a catheter-related bloodstream infection or surgical site infection, is suspected; however, vancomycin choice or continuation has been deemed inappropriate in approximately 20%–70% of cases. Reference Junior, Correa, Marra, Camargo and Pereira14–Reference Snyder, Patel, Kallen, Strom, Tucker and D’Agata16 Therefore, optimizing vancomycin and other anti-MRSA agents is an important AS objective.
Although ASPs are the cornerstone of efforts to protect society against antimicrobial-resistant pathogens, they intensively require human resources and face many constraints on their implementation. In Japan, pharmacists often lack time to dedicate to ASP-related activities, Reference Maeda, Muraki and Kosaka17 and in Latin America, a shortage of clinical pharmacists and a similar lack of time have been identified as key barriers. Reference Fabre, Cosgrove and Secaira18,Reference Fabre, Secaira and Cosgrove19 Designing interventions for maximum efficacy under conditions of resource scarcity—for example, by identifying which departments and wards should be prioritized—is therefore equally important. We aimed to evaluate the impact of a pharmacist-led anti-MRSA time-out stratified by department and ward and to identify the groups most likely to benefit.
Methods
Study design and setting
This before–after study was conducted at the Institute of Science Tokyo Hospital (ISTH, formerly Tokyo Medical and Dental University Hospital), an 813-bed tertiary care hospital in Tokyo, Japan. The preintervention period was October 1, 2017, to September 30, 2022, and the postintervention period was October 1, 2022 to September 30, 2024. The study was approved by the institutional review board of ISTH (M2024-035). Because this was a minimal-risk quality improvement activity without direct patient intervention, the requirement for informed consent was waived.
The antimicrobial stewardship team (AST) is operated by stewardship pharmacists with a 0.9 full-time equivalent (FTE) and an infectious diseases specialist with a 0.1 FTE. The main ASP activities include: (1) postprescription audit and feedback for broad-spectrum antimicrobials (carbapenems and piperacillin/tazobactam) and intravenous antimicrobials administered ≥14 days; (2) prospective audit and feedback (PAF) for intravenous fluoroquinolones; (3) a preauthorization notification system for anti-MRSA agents and antimicrobials with anti-Pseudomonas activity; (4) a restriction policy requiring approval for daptomycin, linezolid, and non-formulary antimicrobials; (5) a multidisciplinary antimicrobial time-out covering all intravenous antibiotics has been operational within ICU rounds since June 2018, conducted by pharmacists and limited to ICU patients, and infectious diseases consultation has been provided since June 2021. Reference Mishima, Nawa and Asada20
Patients and intervention
Among all inpatients receiving an anti-MRSA agent (vancomycin, teicoplanin, linezolid, or daptomycin), those continuing therapy beyond 72 hours and meeting no exclusion criteria were included. The exclusion criteria were: 1) use of an anti-MRSA agent as first-line therapy (eg, MRSA bacteremia, methicillin-resistant coagulase-negative Staphylococcus bacteremia, or culture-negative cases judged appropriate for definitive therapy); 2) high epidemiologic risk (eg, known MRSA colonization, prior MRSA infection, or prolonged healthcare exposure). Anti-MRSA agents used solely as surgical prophylaxis were also excluded; this was completed within 72 hours unless a postoperative infection (eg, surgical site infection) was suspected and switched to treatment, continuing beyond 72 hours; 3) β-lactam allergy; and 4) the recommendations of an infectious diseases physician; 5) therapy completed before the 72-hour time-out. These criteria were defined based on prior research. Reference Hasegawa, Tagashira and Murakami13 When uncertain, pharmacists decided after discussion with infectious disease physicians.
For eligible cases, stewardship pharmacists contacted the prescriber by telephone at 72 hours to prompt reassessment of the continued need for anti-MRSA therapy; the time-out did not include specific recommendations to change therapy. If unreachable, pharmacists entered the same standardized EHR note based on available information. The standard operating procedure and example EHR notes are in Supplementary.
Outcome
The primary outcome was monthly days of therapy per 1,000 patient-days (DOT) for all anti-MRSA agents combined and for each anti-MRSA agent, stratified by ward type (critical-care vs general) and department (emergency medicine, surgery, internal medicine, hematology, and pediatrics), generating ten analytical groups. Secondary outcomes were: (1) hospitalwide monthly DOT for all anti-MRSA agents combined and per agent; (2) duration of anti-MRSA therapy per case; (3) acceptance rate, the proportion of cases in which anti-MRSA therapy ended within three days of the time-out; (4) monthly therapeutic drug monitoring (TDM) tests per 1,000 patient-days; and (5) average monthly length of stay and in-hospital mortality. Pediatric data were analyzed separately because these patients consisted primarily of those with primary immunodeficiency or undergoing hematopoietic stem cell transplantation.
Statistical analysis
Normality was assessed using the Shapiro–Wilk test. Welch’s t test was used for normally distributed continuous variables and the Mann–Whitney test for non-normally distributed variables; the χ2 test was used for categorical variables. To evaluate the intervention effect on monthly DOT, interrupted time-series analysis (ITSA) used 60 preintervention and 24 postintervention monthly time points to estimate level and slope changes. Stata version 18.0 (StataCorp, College Station, TX) was used for the ITSA analysis and R version 3.6.3 for other analyses.
Results
Antimicrobial time-out eligibility
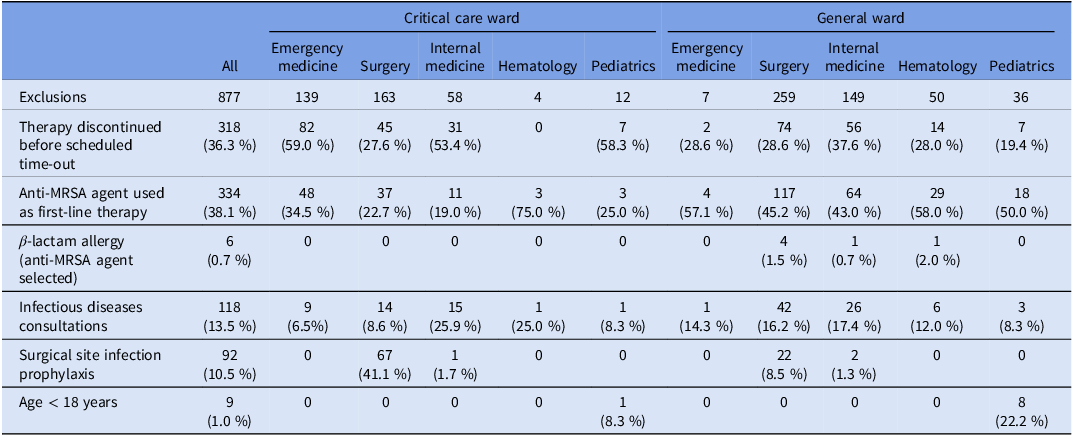
There were 3,937 inpatient anti-MRSA cases (2,906 preintervention; 1,031 postintervention). The patients’ median age (IQR) was 66 years (51–76) preintervention and 67 years (54–77) postintervention; 68% and 65% were male, respectively. Of the 1,031 postintervention cases, 877 (85%) met the exclusion criteria, and time-out was performed in 154 cases (15%) in Figure 1. Among the 154 eligible cases, the prescriber could not be contacted in 4 (2.6%), and in 15 (9.7%) the prescriber had proactively contacted the AST during other ASP activities. Reasons for exclusion by ward and department are in Table 1.
Number of cases excluded from the time-out and the reasons for exclusion stratified by ward and clinical department

Table 1. Long description
The table presents data on the number of cases excluded from the time-out and the reasons for exclusion, stratified by ward and clinical department. It has 10 rows and 11 columns. The columns are labeled as All, Critical care ward, and General ward, with sub-columns for Emergency medicine, Surgery, Internal medicine, Hematology, and Pediatrics. The rows are labeled as Exclusions, Therapy discontinued before scheduled time-out, Anti-MRSA agent used as first-line therapy, Beta-lactam allergy (anti-MRSA agent selected), Infectious diseases consultations, Surgical site infection prophylaxis, and Age under 18 years. Each cell contains numerical values representing the count of cases for each category. Notable trends include high exclusion rates in Emergency medicine and Surgery departments, and a significant number of therapy discontinuations in the Critical care ward.
Flowchart of the intervention.

Anti-MRSA agent use by ward and department
The trend in DOT by ward and department is shown in Figure 2. In the emergency department, DOT for all anti-MRSA agents combined declined significantly in both the critical-care ward (slope change −20.3; 95% CI −36.25 to −4.28; P = .01) and the general ward (slope change −31.6; 95% CI −61.4 to −1.79; P = .04); in the critical-care ward, vancomycin use decreased both immediately and significantly (level change −406.1; 95% CI −801.3 to −10.9; P = .04), with a continuing decrease (slope change −24.5; 95% CI −41.2 to −7.8; P < .001), while in the general ward only the trend indicated a significant decrease (slope change −34.4; 95% CI −62.9 to −5.87; P = .02). In the surgery department, overall anti-MRSA DOT showed no significant change, with a non-significant postintervention increase in both critical-care (slope change + 0.98; 95% CI −29.21 to 31.17; P = .95) and general wards (slope change + 1.52; 95% CI −1.46 to 4.49; P = .32); however, the duration of anti-MRSA therapy per case shortened significantly (−1.0 d; P < .05). In the internal medicine department, the critical-care ward showed an immediate and significant decrease in DOT (level change −793.3; 95% CI −1540.0 to −46.6; P = .04), with a non-significant trend, while the general ward showed a borderline decline (slope change −3.81; 95% CI −7.57 to −0.04; P = .05). In hematology, no statistically significant overall anti-MRSA DOT change was observed; in the general ward, vancomycin use decreased significantly (level change −14.9; 95% CI −24.53 to −5.18; P < .001) whereas teicoplanin use increased significantly (level change + 15.7; 95% CI 6.22 to 25.16; P < .001), suggesting agent substitution rather than overall reduction. In the pediatrics department, anti-MRSA DOT in the general ward showed an immediate significant decrease (level change −328.5; 95% CI −513.73 to −143.31; P < .001) followed by a significant rising trend (slope change + 21.6; 95% CI 11.06 to 32.19; P < .001), with vancomycin demonstrating an analogous pattern (level change −301.2; P < .001; slope change + 19.4; P < .001).
DOT trend for all anti-MRSA agents by ward and clinical department.

Hospital-wide use of anti-MRSA agents
Hospital-wide DOT showed a non-significant immediate decrease following the intervention (level change −19.23; 95% CI −59.17 to 20.72; P = .35) with no significant trend change (slope change + 0.82; 95% CI −1.18 to 2.82; P = .42) (Figure 3). Figure 4 shows the trend in DOT per agent.
DOT trend for all anti-MRSA agents at the study center.

DOT trend for each anti-MRSA agent at the study center.

Figure 4. Long description
Four scatter plots depict the DOT per 1,000 patient-days for Vancomycin, Teicoplanin, Daptomycin, and Linezolid over time. Panel A: The scatter plot for Vancomycin shows the y-axis labeled DOT per 1,000 patient-days ranging from 0 to 500 and the x-axis labeled with dates from October 2017 to October 2024. The data points show a general decreasing trend with a slight increase after the intervention line. Panel B: The scatter plot for Teicoplanin shows the y-axis labeled DOT per 1,000 patient-days ranging from 0 to 80 and the x-axis labeled with dates from October 2017 to October 2024. The data points show an increasing trend, especially after the intervention line. Panel C: The scatter plot for Daptomycin shows the y-axis labeled DOT per 1,000 patient-days ranging from 0 to 50 and the x-axis labeled with dates from October 2017 to October 2024. The data points show a slight increasing trend before the intervention line and a decreasing trend after. Panel D: The scatter plot for Linezolid shows the y-axis labeled DOT per 1,000 patient-days ranging from 0 to 60 and the x-axis labeled with dates from October 2017 to October 2024. The data points show a decreasing trend over time, with a notable drop after the intervention line.
Other outcomes
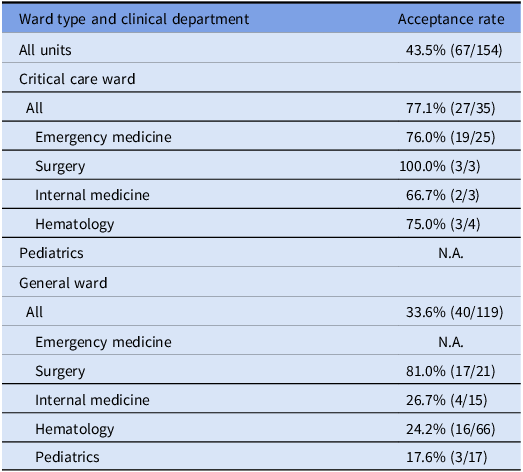
The overall acceptance rate was 43.5% (67/154). Acceptance was markedly higher in critical-care wards (77.1%, 27/35) than in general wards (33.6%, 40/119). Within critical-care wards, the rate by department was 76.0% (19/25) in emergency medicine, 100% (3/3) in surgery, and 66.7% (2/3) in internal medicine. Within general wards, acceptance was 81.0% (17/21) in surgery and 26.7% (4/15) in internal medicine; it was notably lower in hematology (24.2%, 16/66) and pediatrics (17.6%, 3/17). There were no eligible cases in the critical-care ward of the pediatric department or in the general ward of the emergency department (Table 2). Median anti-MRSA therapy duration per case by department before and after intervention is shown in Figure 5.
Comparison of the median duration of anti-MRSA therapy by clinical department before and after the intervention.

Acceptance rate of the time-out stratified by ward and clinical department

Monthly TDM tests per 1,000 patient-days decreased significantly from 8.47 ± 2.39 preintervention to 6.55 ± 1.18 postintervention (P < .001), driven primarily by vancomycin (8.30 ± 2.38 to 6.06 ± 1.17; P < .001). Teicoplanin TDM tests increased significantly (0.17 ± 0.22 to 0.50 ± 0.34; P < .001). Average monthly length of stay (11.06 vs 10.60 d) and in-hospital mortality (2.25% vs 2.17%) showed no significant deterioration between periods.
Discussion
In this study, a pharmacist-led anti-MRSA time-out produced few changes at the hospital-wide level; however, stratified analysis by department and ward demonstrated that it may have contributed to reducing the use of anti-MRSA agents in specific departments. In our data, the groups most likely to benefit were those with significant DOT reductions and high acceptance rates—most clearly the emergency department, where reductions were observed regardless of ward type. Prioritizing such departments and wards may therefore be useful when designing a more efficient ASP in settings lacking adequate human resources. At the same time, acceptance varied widely by department and ward, suggesting that where it was low, time-out alone may be insufficient and should be combined with other interventions, including PAF, department-specific consensus building, and systematic clinical support. Unlike PAF, in which the stewardship team evaluates the appropriateness of the prescription and provides culture-based feedback and specific recommendations to change therapy, the present time-out only prompted the attending physician to reassess the need for therapy; combining the two approaches may therefore be complementary.
Pharmacists play an important role in ASP by optimizing antimicrobial use, reducing medical costs, addressing antimicrobial resistance, and improving patient outcomes. Reference Wickens, Farrell, Ashiru-Oredope, Jacklin and Holmes21–Reference Sadyrbaeva-Dolgova, Aznarte-Padial, Jimenez-Morales, Expósito-Ruiz, Calleja-Hernández and Hidalgo-Tenorio27 Pharmacist-led interventions may shorten hospital stay and reduce broad-spectrum antimicrobial use. Reference Sawada, Inose, Goto, Nakatani, Kono and Muraki28–Reference Okada, Azuma and Tsujinaka30 One pharmacist-led intervention for uncomplicated gram-negative bacteremia shortened therapy duration. Reference Fukuda, Tanuma, Iio, Saito, Komura and Yamatani31 A study dividing departments into internal medicine and surgery found pharmacist-led time-out may have decreased vancomycin use in the surgery department. Reference Hasegawa, Tagashira and Murakami13 By subdividing into departments and stratifying by ward type, we found that anti-MRSA use in the emergency department decreased significantly regardless of ward type, with high acceptance rates, suggesting that pharmacists’ recommendations more readily translate into reassessment here.
In Japan, patients admitted under the emergency department remain under its care rather than being transferred or discharged early; consequently, many were still admitted under emergency medicine at 72 hours and thus eligible for the time-out. The emergency department frequently manages sepsis and septic shock, and guidelines recommend selecting broad-spectrum antimicrobials including anti-MRSA agents as initial empirical therapy. Reference Guarino, Perna and Cesaro32 Time-out at approximately 72 hours, when culture results and the clinical course become available, therefore provides a natural reassessment window to correct the initial empirical therapy. The high acceptance rate in emergency medicine is consistent with this interpretation: when the clinical rationale for discontinuation is clear and timely, physicians are more receptive to pharmacist recommendations. Notably, the absence of eligible cases in the general ward of the emergency department postintervention may reflect not only intervention-driven behavioral changes but also earlier discontinuation of anti-MRSA agents before the 72-hour threshold. Because our study did not capture cases discontinued before the time-out, future studies should examine the proportion of treatment courses discontinued within 72 hours.
In the surgery department, high acceptance rates coexisted with a non-significant increase in overall DOT and no reduction in DOT trend, yet the duration of therapy per case shortened significantly. Because cases with anti-MRSA agents as clear first-line therapy were excluded, it is likely that the duration of unnecessary cases was shortened, while the number of cases requiring anti-MRSA therapy increased during the same period. Interpreting DOT for surgery therefore requires concurrent tracking of microbiological background—including MRSA-related infection incidence, surgical site infection epidemiology, and blood culture positivity rates—which we did not capture.
In internal medicine, DOT showed a decreasing tendency, but the acceptance rate in general wards was low (26.7%), and the trend change was unclear. Acceptance heterogeneity across departments likely reflected differences in case-mix complexity, physician decision-making culture, and prior familiarity with stewardship recommendations. In areas with a low acceptance rate, more structured interventions beyond a telephone alert may be needed, such as feedback in departmental conferences, standardizing order sets and treatment templates, and collaborating more closely with infectious diseases specialists. Reference Mishima, Nawa and Asada20
In hematology, vancomycin use decreased, while teicoplanin use increased in the general ward, suggesting agent substitution rather than overall reduction. In immunocompromised and transplant populations, the threshold for continuing therapy may be higher due to disease severity and immunosuppressive status, and agent selection is more likely to reflect changes in renal function or pharmacokinetic considerations. Similarly, in the pediatrics department, unique factors in this population (centralized management of primary immunodeficiency and transplant cases) strongly influence prescribing patterns. Although some reports have demonstrated the efficacy of time-out in cancer centers, Reference Tverdek, Aitken and Mulanovich33 our findings suggest anti-MRSA use is less likely to decrease in hematology and pediatrics through standard time-out alone. Disease-specific, multidisciplinary strategies may be required in these settings.
The higher acceptance rate in critical-care wards across departments (77.1% vs 33.6% in general wards) may reflect a preexisting culture of daily antimicrobial reassessment, the influence of multidisciplinary rounds, Reference Mishima, Nawa and Asada20 and clearer clinical end points that facilitate de-escalation decisions. However, compared with the all-antibiotic time-out operated within ICU rounds, our time-out differed in two ways: (i) it focused on anti-MRSA agents and was delivered by pharmacists independently of rounds at 72 hours, and (ii) it was extended hospital-wide beyond the ICU. Critically, the emergency department—where the largest reductions were seen—was in a separate critical-care ward not covered by the ICU program, so the hospital-wide expansion explains the significant decreases in previously uncovered critical-care areas. Even where no clear change in overall anti-MRSA use is observed, a time-out may still reduce unnecessary antimicrobial exposure as one component of a multifaceted stewardship approach.
The significant reduction in TDM tests per 1,000 patient-days is a meaningful ancillary benefit. Although TDM helps reduce adverse events such as nephrotoxicity, Reference Schuts, Hulscher and Mouton34 unnecessarily prolonged anti-MRSA therapy generates avoidable TDM burden for pharmacists and laboratory staff.
Time-out has improved prescription appropriateness, shortened therapy, and reduced use of specific agents, but its effects on total antimicrobial consumption and patient outcomes are inconsistent. Reference Van Schooneveld, Rupp, Cavaleiri, Lyden and Rolek11,Reference Taylor, Coe, Stevenson, Wardlow, Boghdadly and Reed12,Reference Graber, Jones and Glassman35–Reference Salehi, Arabi and Khalili37 Some studies have found no significant reduction in antimicrobial use, Reference Thom, Tamma and Harris10 suggesting time-out is not universally effective alone but more effective within a multifaceted ASP. Reference Van Schooneveld, Rupp, Cavaleiri, Lyden and Rolek11 In our study, time-out covered only 15% of anti-MRSA cases, and overall DOT changes were modest; the effects of other ASP activities and behavioral changes such as increased early discontinuation should therefore also be considered. Accumulating evidence on which methods suit which populations may help conduct ASP more effectively within limited resources.
Several limitations must be acknowledged. First, this was a single-center study, limiting generalizability. Second, only 15% of cases met time-out criteria, and DOT changes may have been confounded by concurrent ASP activities or system changes. Third, the incidence of infections requiring anti-MRSA agents was not adequately accounted for. Fourth, safety outcomes such as nephrotoxicity, retreatment, readmission, and microbiological outcomes were not sufficiently assessed. Fifth, the pharmacist FTE dedicated to the time-out was not evaluated. Finally, all implementing pharmacists were female; physicians’ acceptance may be influenced by pharmacist gender, Reference Vaughn, Giesler and Mashrah38 though institutional culture, expertise, and relationships can exert similar influence. In addition, infectious diseases consultation became available in June 2021, before the intervention. Consultations were not provided for 118 of 1,031 cases (11.4%), and we could not fully disentangle their effect; ID consultation may have prompted some early discontinuation independently of the time-out. Future studies should examine the implementation process using qualitative or mixed-methods approaches to elucidate the contextual factors driving differential acceptance.
Conclusion
Pharmacist-led anti-MRSA time-out may contribute to reducing the use of anti-MRSA agents in specific departments—particularly emergency medicine—without worsening in-hospital outcomes. Implementation focusing on areas most likely to benefit, identified through stratified analysis by department and ward, may provide a feasible approach to curbing overuse even in settings with limited time and resources. In areas where acceptance is low or the patient population is clinically complex, time-out alone is likely insufficient; complementary strategies including PAF, department-specific education, and closer infectious diseases specialist involvement should be considered.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ash.2026.10778.
Data availability statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank James R. Valera for his assistance with editing this manuscript.
Author contributions
RY and YT designed the study protocol. RY, YE, MS, and YA collected the clinical data, and RY and DA analyzed the data and composed the figures. RY and YT drafted the first version of the manuscript. All the authors have contributed to the final version of the manuscript for submission.
Financial support
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing interests
The authors declare that they have no competing interests.
Ethical standard
This study was approved by the Ethics Committee of the Institute of Science Tokyo Hospital (Approval No. M2024-035). The requirement for informed consent was waived because the study was retrospective.
Consent for publication
Not applicable.








 Open access
Open access