


Depression is the most common mental health disorder and poses a significant public health challenge, contributing to increased risk of chronic physical illness, reduced occupational productivity, suicide and elevated mortality. Reference Herrman, Patel, Kieling, Berk, Buchweitz and Cuijpers1 The overall health burden associated with depression is substantial. Reference Mathers, Loncar and Samet2,3 Although the pathophysiology of depression is multifactorial and complex, one of the most consistently identified risk factors for the onset of clinical depression is subthreshold depression. Reference Hao, Jia, Chen, Zou and Jiang4 Preventive interventions targeting individuals with subthreshold depression have therefore received considerable attention. Compared with pharmacological treatments, non-pharmacological approaches are generally safer and regarded as the most promising preventive strategies. Reference Hao, Jia, Chen, Zou and Jiang4 Among these, cognitive behavioural therapy (CBT) has repeatedly demonstrated efficacy. Reference Hao, Jia, Chen, Zou and Jiang4–Reference Cuijpers, Pineda, Quero, Karyotaki, Struijs and Figueroa7 Notably, CBT delivered via internet- or smartphone-based platforms offers advantages in terms of accessibility, portability, flexibility and scalability, and a growing body of evidence supports its utility. Reference Buntrock, Ebert, Lehr, Smit, Riper and Berking8,Reference Chen, Que, Chan, Shi, Li and Chan9 For instance, in a randomised controlled trial (RCT) involving individuals with subthreshold depression, Buntrock et al. reported that online CBT significantly reduced the incidence of major depressive disorder at 12-month follow-up. Reference Buntrock, Ebert, Lehr, Smit, Riper and Berking8
CBT comprises multiple psychological skill components. However, it remains unclear which specific elements or combinations are most effective for preventing the onset of clinical depression. We previously developed a smartphone-based intervention incorporating training in five core CBT skills (behavioural activation, cognitive restructuring, problem solving, assertion training and behavioural therapy for insomnia, and demonstrated its short-term effectiveness up to 6-months follow-up in adults with subthreshold depression. Additionally, we found that the included CBT skills and combinations had different effects. Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10 In the current study, we conducted a 50-week follow-up to investigate the long-term preventive effects of individual CBT skills and their combinations on the incidence of major depressive episodes. Additionally, we examined the cumulative burden of depressive symptoms over 50 weeks to evaluate the sustained impact of the intervention.
Method
The Resilience Enhancement with Smartphone in Living Environments (RESiLIENT) trial is a master protocol trial comprising four 2 × 2 factorial trials. Reference Furukawa, Tajika, Sakata, Luo, Toyomoto and Horikoshi11 The detailed study protocol of this trial has been previously published. Reference Furukawa, Tajika, Sakata, Luo, Toyomoto and Horikoshi11 The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects were approved by the Kyoto University Ethics Committee (C1556) on 3 March 2022. We preregistered the trial in the UMIN Clinical Trials Registry (UMIN000047124) on 1 August 2022. For the present analysis, we adopted a combined master protocol approach in which each intervention and control arm was analysed independently. This approach allowed us to efficiently summarise the specific effects of individual CBT skills, their combinations and potential interactions. The statistical analysis plan (SAP) for the long-term follow-up data was preregistered on medRxiv Reference Noma, Furukawa, Tajika, Toyomoto, Sakata and Luo12 prior to the final data lock and the commencement of the statistical analyses.
Participants
The details of the eligibility criteria have been reported previously. Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10,Reference Furukawa, Tajika, Sakata, Luo, Toyomoto and Horikoshi11 In brief, individuals aged 18 years or older who were not receiving treatment from mental health professionals at the time of screening were eligible if they had a total score on the Patient Health Questionnaire-9 (PHQ-9) of either (a) 5–9 (inclusive), or (b) 10–14 (inclusive), provided they did not score 2 or 3 on item 9 (suicidality). Participants were recruited from four sectors across Japan: health insurance societies, private companies and corporations, community and local government organisations and via direct-to-consumer online advertisements.
Procedures
Interested individuals were directed to the trial website and asked to complete a screening questionnaire. If individuals met the minimum eligibility criteria (age, PHQ-9 score and mental health treatment), they were invited to an online informed consent session. After providing written informed consent, participants completed baseline assessments, after which the app automatically randomised them to one of the intervention or control arms. The study was conducted entirely online, using a fully decentralised clinical trial design. Reference Bernard, Wilkins, Selker, Dwyer and Dean13 The recruitment started on 1 September 2022.
Interventions and control
The four 2 × 2 factorial trials consisted of nine intervention arms and the original trial had three types of control; in this analysis we used one control following the main analysis and SAP, as previously described in detail. Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10,Reference Furukawa, Tajika, Sakata, Luo, Toyomoto and Horikoshi11 All interventions were delivered through the Resilience Training App (version 2.1). Participants were randomly assigned in equal proportions to one of the nine intervention arms or the control arm.
The intervention arms included: behavioural activation, cognitive restructuring, problem solving, assertion training, behavioural therapy for insomnia and their combinations: behavioural activation + cognitive restructuring, behavioural activation + problem solving, behavioural activation + assertion training and behavioural activation + behavioural therapy for insomnia. Each component comprised seven to nine chapters, subdivided into two to four lessons per chapter, and included interactive worksheets to support skill practice. Participants were instructed to complete one chapter per week. Progression to the next chapter was permitted only after at least 1 week had passed and the corresponding worksheet had been completed.
In the present study, the control group engaged in weekly self-monitoring (self-check control group). Participants in this arm received weekly encouragement emails and completed the PHQ-9 weekly up to week 6, followed by monthly assessments up to week 50 (as in the intervention arms). This arm served as an attention control, designed to match the contact frequency of the intervention arms without delivering any active therapeutic content.
Concomitant interventions
Participants in both the intervention and control arms were free to access any mental health services of their choosing throughout the 50-week study period. At the 50-week follow-up, we collected self-reported data regarding receipt of professional mental health care, including pharmacotherapy and psychotherapy.
Baseline measurements
Demographic, psychosocial and clinical variables were measured at baseline as detailed elsewhere. Reference Furukawa, Tajika, Sakata, Luo, Toyomoto and Horikoshi11 All measurements were collected by the Resilience Training App.
Outcomes
The primary outcome is the time to incident of major depressive episode by week 50, as identified by the depression section of the computerised WHO Composite International Diagnostic Interview (CIDI), which has demonstrated good reliability Reference Shimoda, Inoue, Tsuno and Kawakami14,Reference Kawakami, Takeshima, Ono, Uda, Hata and Nakane15 administered at week 50. A smartphone-based version of the (CIDI) for major depression was administered, including assessment of onset.
Secondary outcome
-
(a) Total burden of depression (TBD); integral of PHQ-9 Reference Kroenke, Spitzer and Williams16,Reference Muramatsu, Miyaoka, Kamijima, Muramatsu, Yoshida and Otsubo17 scores through 50 weeks defined as the integral of the linear trajectory of PHQ-9 scores through 50 weeks.
-
(b) Changes in PHQ-9 from baseline to week 50.
Statistical methods
Primary efficacy analyses
To describe the survival time distributions, we used the Kaplan–Meier methods of the cumulative incidence of a major depressive episode. Additionally, we estimated the between-group relative hazards using the Cox proportional hazard model. Reference Cox18 We conducted the comparative analysis among all interventions (nine arms) and self-check control group. The Cox regression model included baseline PHQ-9 score, employment status, age and gender as adjustment factors. The number needed to treat (NNT) was estimated from the Kaplan–Meier estimates at week 50 using the Altman-Andersen method. Reference Altman and Andersen19
Secondary efficacy analyses
-
(a) TBD. We used analyses-of-covariance to conduct a between-groups comparative analysis of TBD adjusting for the baseline PHQ-9 score, employment status, age and gender; the comparison among all interventions (nine arms) and the self-check control group was conducted. Although the 50-week follow-up rate was 89.5%, a certain proportion of PHQ-9 scores was missing through the follow-up period. We adopted the multiple imputation to handle the missing data and defined the TBD score from the imputed trajectory data in the statistical analyses. Reference Little and Rubin20 The missing PHQ-9 was predicted by the predictive mean matching using employment status, age, gender and the nearest past measurement of PHQ-9 on the chained equation. Reference White, Royston and Wood21 We then integrated the PHQ-9 data through 50 weeks and defined the TBD. We performed 1000 imputations, and adopted Rubin’s rule Reference Little and Rubin22 in the synthesis.
-
(b) Changes in PHQ-9. We used the mixed-effects models for repeated-measures (MMRM) Reference Mallinckrodt and Lipkovich23 for the comparative analysis of the changes in PHQ-9 while adjusting for the missing data through 50 weeks. The regression model included treatments, baseline PHQ-9 score, employment status, age, gender, visit (as categorical) and treatment-by-visit interactions. The covariance matrix structure of outcome variables was set to unstructured. The s.e. estimates and d.f. were adjusted using the Kenward–Roger method. Reference Kenward and Roger24 We estimated least squares mean change scores for the PHQ-9 at weeks 6, 26, 30, 34, 38, 42, 46 and 50 using the estimated model of the MMRM analysis. Effect sizes were calculated using the observed baseline s.d. for within-group change scores and the observed week 50 s.d. for group differences.
We used R version 4.4.3 for Windows (R Foundation for Statistical Computing, Vienna, Austria) for all statistical analyses. All reported P-values are two-sided. We calculated 95% CIs to describe the precision of the estimates. The imputation analysis of TBD was updated from the pre-planned SAP through detailed analyses of TBD to treat the uncertainty of missing data appropriately.
Safety monitoring and analyses
Details of the safety monitoring procedures have been reported elsewhere. Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10 In brief, all serious adverse events were managed in accordance with a predefined standard operating procedure. If an increase in suicidality suggested by two consecutive instances of scores exceeding the threshold on the suicidality item of PHQ-9 score was detected, an email recommending consultation with a mental health professional was sent to the participant. Potential adverse reactions and serious adverse events during the 50-week study period were descriptively reported on the basis of participant self-reporting via the app.
Changes from the protocol or the SAP
As stated in the SAP (Supporting Information), we had initially planned to compare all intervention arms (nine arms) with both control arms (i.e. self-check and the health information arm). However, based on the findings of our previous main publication, a substantial difference was observed between the self-check control arm and the health information arm, despite both having originally been designated as inactive control conditions or as sham apps. In the health information arm, participants received the URLs of websites containing tips for a healthy life (physical activities, nutrition and oral health, none of which focused on mental health) for the initial 3 weeks and then were asked to answer quizzes to test comprehension. Participants were asked to complete self-reports at weeks 3 and 6 (without encouragement emails), and then follow-up evaluations thereafter up to week 50. With regard to the outcome, as illustrated in the Supplementary Figure (available at https://doi.org/10.1192/bjp.2026.10630), the health information arm consistently showed greater improvement than the self-check arm, suggesting that the health information arm may have functioned as an active control. Following discussions within the research team, we therefore decided to include only the self-check as the control group in the current analysis as it represents a more appropriate attention control.
Results
Participants
Figure 1 illustrates the participant flow. Of 34 123 individuals assessed for eligibility, 5364 were deemed eligible and provided informed consent, and a total of 3280 individuals were randomised to one of the nine intervention arms or the control arm. The follow-up rate at week 50 was 89% (2934/3280). Participants were predominantly in their 30s, 40s or 50s. Approximately half of the participants were male. Most participants were married and employed. The mean baseline PHQ-9 score was 8.1 (s.d. = 2.7); 29% had a history of mental health treatment and 33% reported physical comorbidities. The distribution of these baseline variables was well balanced across the intervention and control arms (Table S1). By week 50, 131 participants in the intervention arms and 19 in the control arm had sought professional mental health care (psychiatrist or psychologist). Additionally, 37 participants in the intervention arms and two participants in the control arm reported having received psychotropic medication. Overall, 5.9% of participants (189 of 3189) confirmed that they were seeking professional mental health care by follow-up week 50.
Consolidated Standards of Reporting Trials (CONSORT) diagram. PHQ-9, Patient Health Questionnaire-9; BA, behavioural activation; CR, cognitive restructuring; PS, problem solving; AT, assertion training; BI, behavioural therapy for insomnia; SC, self-check.

Adherence and follow-up completion
As reported previously, 66–92% of participants in the intervention arms completed all lessons by week 30. Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10 In the current extended follow-up, these rates slightly increased to 69–92% by week 50.
Primary outcome
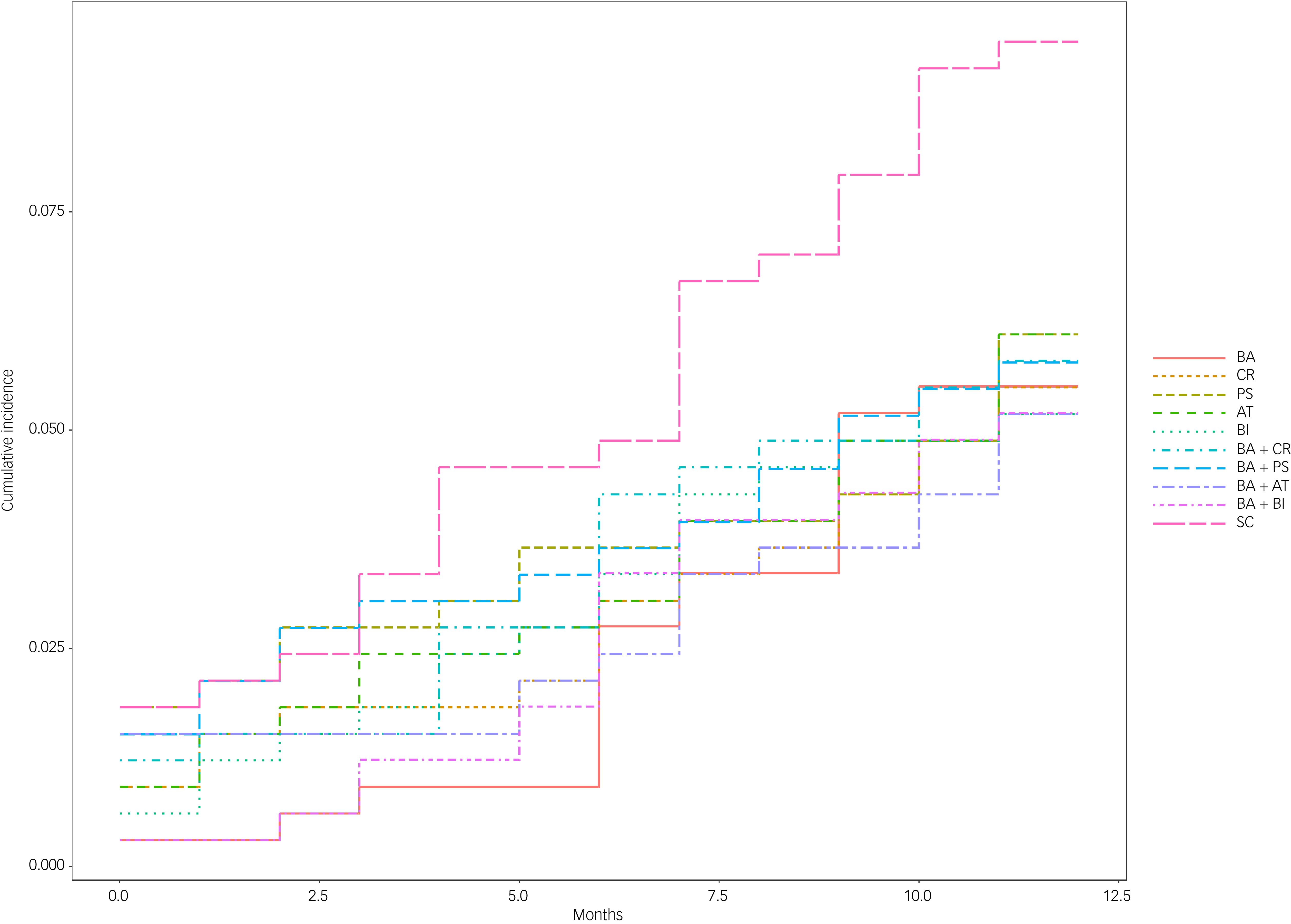
By week 50, the incidence of major depressive episodes for the 10 groups were 18 (behavioural activation), 18 (cognitive restructuring), 20 (problem solving), 20 (assertion training), 17 (behavioural therapy for insomnia), 19 (behavioural activation + cognitive restructuring), 19 (behavioural activation + problem solving), 17 (behavioural activation + assertion training), 17 (behavioural activation + behavioural therapy for insomnia) and 31 (self-check) and a total of 196 participants had developed a major depressive episode. Figure 2 illustrates the cumulative incidence of depression across all smartphone-delivered CBT interventions and the control group. The control group showed the highest cumulative incidence rate.
Cumulative incidence of major depression across all smartphone-delivered cognitive–behavioural therapy interventions and the control group up to week 50. BA, behavioural activation; CR, cognitive restructuring; PS, problem solving; AT, assertion training; BI, behavioural therapy for insomnia; SC, self-check.

Table 1 presents the results of a Cox proportional hazards model comparing the risk of developing major depression between the control group and nine smartphone-delivered CBT interventions. All nine interventions showed hazard ratios compared with the control group of less than or equal to 1, ranging from 0.52 (95% CI: 0.29–0.94) to 0.63 (95% CI: 0.36–1.1). The intervention behavioural activation + assertion training yielded the lowest hazard ratio, followed by behavioural therapy for insomnia, behavioural activation + behavioural therapy for insomnia and cognitive restructuring. There was strong evidence supporting the preventive effects of these four interventions (behavioural activation + assertion training, behavioural therapy for insomnia, behavioural activation + behavioural therapy for insomnia and cognitive restructuring), while there was suggestive evidence in support of the remaining five interventions. NNTs were 23.3 (12.2 to 250) for behavioural activation + assertion training, 23.3 (12.2 to 250) for behavioural therapy for insomnia, 23.3 (12.2 to 250) for behavioural activation + behavioural therapy for insomnia, 25.0 (12.7 to 1000) for cognitive restructuring, 25.6 (12.8 to ∞) for behavioural activation, 27.0 (12.8 to ∞, −∞ to −250) for behavioural activation + cognitive restructuring, 27.0 (12.8 to ∞, −∞ to −250) for behavioural activation + problem solving, 29.4 (13.3 to ∞, −∞ to −142.9) for problem solving and 29.4 (13.3 to ∞, −∞ to −142.9) for assertion training. When comparing all active intervention arms (nine arms) with the control group, the hazard ratio was 0.66 (95% CI: 0.49–0.90) and NNT was 25.6 (13.9 to 166.7).
Cox proportional hazards model comparing the risk of developing major depression between the control group and nine smartphone cognitive–behavioural therapy interventions

BA, behavioural activation; CR, cognitive restructuring; PS, problem solving; AT, assertion training; BI, behavioural therapy for insomnia.
Hazard ratios were adjusted for baseline Patient Health Questionnaire-9 scores, employment status, age and gender.
Secondary outcomes
TBD
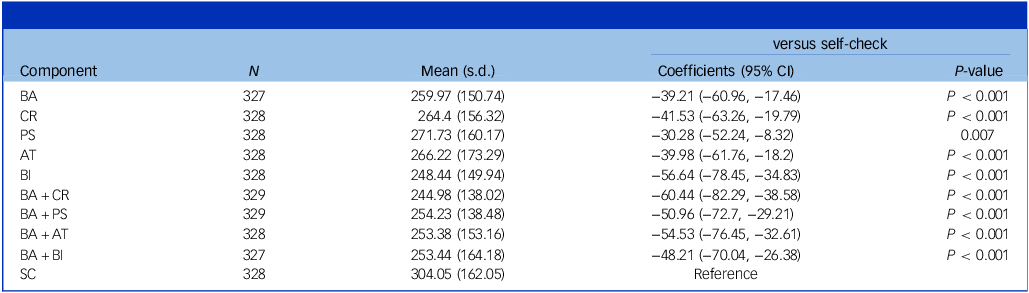
Table 2 shows the effect of the nine smartphone CBT interventions on TBD up to week 50. The TBD up to week 50 for the intervention or control arms ranged between 2.5 and 1168.2. All smartphone CBT interventions demonstrated important reductions in TBD in comparison with the self-check, ranging between −30.3 for problem solving and −60.4 for behavioural activation + cognitive restructuring. Behavioural activation + cognitive restructuring yielded the greatest reduction, followed by behavioural therapy for insomnia and behavioural activation + assertion training This suggests that, compared with the control, behavioural activation + cognitive restructuring was associated with a reduction of approximately 1.21 points in the average weekly PHQ-9 score.
The effect of the nine smartphone cognitive–behavioural therapy interventions on total burden of depression up to week 50

BA, behavioural activation; CR, cognitive restructuring; PS, problem solving; AT, assertion training; BI, behaviour therapy for insomnia; SC, self-check.
Changes in PHQ-9
Table 3 shows the combined analysis using the MMRM for PHQ-9 scores through 50 weeks. At week 50, the effect sizes of the smartphone-based CBT interventions compared with the control group ranged from −0.34 to −0.07. Behavioural activation + cognitive restructuring was the most effective intervention, showing the greatest improvement at week 50 in both the change score of PHQ-9 (−1.42) and the effect size (−0.34). This was followed by combinations such as behavioural activation + assertion training, behavioural therapy for insomnia and behavioural activation + problem solving. In contrast, problem solving alone yielded only a small change and effect size (−0.07, 95% CI: −0.22 to 0.08).
The combined analysis using the mixed-effects models for repeated-measures for Patient Health Questionnaire-9 scores up to week 50

BA, behavioural activation; CR, cognitive restructuring; PS, problem solving; AT, assertion training; BI, behaviour therapy for insomnia.
Safety monitoring and analyses
The total number of alerts triggered by two consecutive instances of scores exceeding the threshold on the suicidality item of the PHQ-9 score during the entire study period was 201, involving 141 participants (4.3% of 3280 participants). No serious adverse events were reported.
Discussion
In this study, we investigated adults with subthreshold depression and, for the first time, demonstrated that individual CBT skills have differential effects on the prevention of major depressive disorder over a 50-week period. All examined CBT skills and their combinations had important yet differential effects on the TBD in a 50-week follow-up period.
Although the effectiveness of specific skills varied depending on the depression-related outcome assessed, overall analyses indicated that the combination of behavioural activation and assertion training, behavioural activation and cognitive restructuring, as well as behavioural therapy for insomnia, were among the most effective strategies. While CBT is typically delivered as a multicomponent intervention – often including cognitive restructuring, behavioural activation and problem solving – our findings suggest that individual components may exert distinct and independent preventive effects. Notably, the combination of behavioural activation and assertion training, a pairing not commonly implemented in standard clinical practice, emerged as particularly effective, alongside more conventional cognitive–behavioural and sleep-focused behavioural interventions. On the other hand, the problem solving-only arm showed the smallest improvements in both TBD and PHQ-9 scores. The problem solving module taught a standard five-step strategy. When delivered as a standalone component, problem solving showed the lowest adherence among the nine interventions Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10 and the smallest effect size, suggesting that the skill may have been relatively difficult to acquire in this format. In contrast, when combined with behavioural activation, adherence to problem solving increased despite the greater overall task demand, Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10 and the behavioural activation + problem solving module produced a modest but clinically meaningful effect. These findings suggest that problem solving may be more effective when delivered in conjunction with behavioural activation, possibly because behavioural activation facilitates engagement with, and application of, more cognitively demanding skills. These results offer novel and clinically relevant insights into personalised and component-specific approaches to depression prevention.
Comparison with previous research
The magnitude of the preventive effects observed in the present study is broadly consistent with prior findings. For example, Buntrock et al. reported a hazard ratio value of 0.59 for the onset of major depressive disorder 1 year after a web-based CBT intervention, Reference Buntrock, Ebert, Lehr, Smit, Riper and Berking8 while Chen et al. found a similar effect size (hazard ratio 0.58) for behavioural interventions for insomnia. Reference Chen, Que, Chan, Shi, Li and Chan9 These results suggest that smartphone-delivered CBT – characterised by high accessibility and safety – can reduce the risk of developing major depression by approximately 40%.
The primary outcome for this study was time to a major depressive episode, in accordance with previous research. Reference Buntrock, Ebert, Lehr, Smit, Riper and Berking8 This measure may be more sensitive than severity to the importance perceived by patients, because the same depression severity at the long-term follow-up may represent an early relapse with continued symptoms or a very late relapse; for the patient, the latter is clearly preferable. However, early relapse with immediate recovery would constitute the same time to recovery as early relapse with continued symptoms; thus, the survival analysis would be insensitive to such differences. In contrast, the TBD, calculated as an integral of weekly depressive symptoms, may constitute a more sensitive and patient-important outcome.
We were able to measure the integral values using the repeated assessments on the smartphone, similar to the environmental momentary assessment. An average improvement of 1.21 points on the PHQ-9 may appear modest. However, if we equate being in euthymia with scoring less than 5 on the weekly PHQ-9 through the 50 weeks, hence 250 points, the euthymia rate of 37% among people receiving a self-check would have increased to 52% on behavioural activation + cognitive restructuring, resulting in an NNT of 6.9. Reference Furukawa, Cipriani, Barbui, Brambilla and Watanabe25 Thus, it would be necessary to provide behavioural activation + cognitive restructuring, instead of a self-check, for 6 weeks to 7 persons to lead to 1 more person being in euthymia through the subsequent year.
Interpretation of longitudinal patterns and intervention strategies
In our previous study, by week 6, high effectiveness was observed for behavioural activation + problem solving, behavioural activation + cognitive restructuring, behavioural activation alone and behavioural therapy for insomnia, indicating that even behavioural activation as a standalone intervention yielded favourable short-term outcomes. However, by week 26, combinations such as behavioural activation + cognitive restructuring, behavioural activation + problem solving and behavioural activation + assertion training demonstrated greater efficacy, suggesting that acquiring multiple CBT skills may be more beneficial for sustaining preventive effects over time. Consistent with these earlier findings, the present 50-week analysis revealed that behavioural activation + assertion training, behavioural activation + cognitive restructuring and behavioural activation + problem solving continued to show robust effectiveness. These results indicate that, for long-term prevention of depressive states, interventions enabling the acquisition of multiple CBT skills may be preferable. This finding is reasonable given that individuals are likely to encounter a range of life events over time, necessitating a broader repertoire of coping strategies.
Notably, behavioural therapy for insomnia demonstrated strong effects as a standalone intervention at both week 6 and week 50, highlighting its unique preventive profile. This finding is consistent with an RCT conducted in China, which showed that behavioural therapy for insomnia alone was effective in preventing depression in young people aged 15–25 with comorbid insomnia and subthreshold depressive symptoms. Reference Chen, Que, Chan, Shi, Li and Chan9
Our previous experience suggests that when three or more CBT skills are delivered simultaneously, adherence tends to decline markedly. Reference Akechi, Furukawa, Noma, Iwata, Toyama and Higaki26,Reference Sakata, Toyomoto, Yoshida, Luo, Nakagami and Uwatoko27 Therefore, delivering multiple components concurrently may not be optimal. On the basis of the present findings, a stepped-care approach may be more appropriate – initially introducing a core combination such as behavioural activation and assertion training, and subsequently adding behavioural therapy for insomnia, or in the reverse order if subthreshold depressive symptoms persist beyond 1 year. This staged delivery may represent a promising strategy for sustaining long-term preventive effects. Further investigation of this issue is warranted.
Clinical implications
The NNT for antidepressants in the acute treatment of major depression is typically estimated to be between 6 and 8, with adverse events being relatively common. Reference Ormel, Spinhoven, de Vries, Cramer, Siegle and Bockting28 In contrast, smartphone-based CBT is a safe, low-resource intervention, and preventive strategies generally yield smaller effect sizes (i.e. absolute risk differences) than treatment interventions. Therefore, the NNT observed in the present study, Reference Kenward and Roger24–Reference Sakata, Toyomoto, Yoshida, Luo, Nakagami and Uwatoko27 which is consistent with the meta-analytical findings regarding the preventive effects of psychotherapy (NNT 21), Reference Buntrock, Harrer, Sprenger, Illing, Sakata and Furukawa5 appears to be appropriate and represents a clinically meaningful effect size that may have important implications for clinical practice.
Although CBT in routine clinical settings often includes multiple components, our findings, including our previous experiences indicating efficiency of one or two components, Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10,Reference Akechi, Yamaguchi, Uchida, Imai, Momino and Katsuki29 suggest that implementing all elements may not be necessary and can sometimes be associated with compromised adherence. Reference Akechi, Furukawa, Noma, Iwata, Toyama and Higaki26,Reference Sakata, Toyomoto, Yoshida, Luo, Nakagami and Uwatoko27 Simplified combinations assuming the inclusion of behavioural activation as a component skill or even standalone interventions – such as behavioural therapy for insomnia – can be effective for preventing the onset of depression. Given the substantial public health burden posed by depression, the scalability, accessibility and demonstrated efficacy of smartphone-delivered CBT make it a promising strategy for population-level prevention.
However, the successful implementation of such interventions cannot be achieved by the medical and research communities alone. Reference Herrman, Patel, Kieling, Berk, Buchweitz and Cuijpers1 Strong policy-level support will be essential. Collaboration with public health authorities, healthcare systems and policymakers is critical for ensuring the integration of digital CBT interventions into national mental health strategies and preventive care infrastructures as repeatedly suggested. Reference Ormel and VonKorff30–Reference Holte32
Research implications
Although the present study demonstrated preventive effects against depression over a 50-week period, the durability of these effects beyond this time frame remains uncertain. As highlighted in previous meta-analyses, further longitudinal research is warranted to determine whether long-term prevention can be sustained and under what conditions it may be most effective.
This study also provided evidence for both short- and long-term preventive effects of behavioural therapy for insomnia, a relatively simple and low-burden intervention. Behavioural therapy for insomnia has previously been reported to exhibit efficacy for prevention of recurrence of depression, Reference Irwin, Carrillo, Sadeghi, Bjurstrom, Breen and Olmstead33 as well as anxiety disorders, alcohol use disorders, psychotic disorders and the prevention of lifestyle-related conditions such as diabetes, hypertension and cancer. Reference Itani, Jike, Watanabe and Kaneita34–Reference Hertenstein, Feige, Gmeiner, Kienzler, Spiegelhalder and Johann39 Thus, its potential utility may extend beyond mental health. Reference Itani, Jike, Watanabe and Kaneita34 Future research should investigate the broader health benefits of behavioural therapy for insomnia and its role in promoting psychological and physical well-being at the population level.
Limitations and strengths
The current study involved several limitations. As in our previous research, Reference Furukawa, Tajika, Toyomoto, Sakata, Luo and Horikoshi10 potential sources of bias – such as performance bias and assessment bias – may have also been present in the current trial. Furthermore, the generalisability of the findings to populations in different cultural or international settings remains uncertain. In addition, the long-term durability of the preventive effects beyond 50 weeks remains to be clarified. Reference Harrer, Sprenger, Illing, Adriaanse, Albert and Allart6
Despite these limitations, the RESiLIENT trial has several notable strengths. The large sample size ensured sufficient statistical power to detect differences in the incidence of major depressive episodes – a key advantage in preventive trials where event rates are typically low. The use of a smartphone app for intervention delivery enhanced scalability, portability, accessibility and feasibility for population-level implementation, increasing the translational relevance of the findings. Finally, the fully decentralised clinical trial model Reference Underhill, Freeman, Dixon, Buzza, Long and Burbury40 – conducted entirely online – facilitated recruitment, intervention and follow-up, reduced participant burden and achieved a high retention rate over the 50-week period. Repeated administration of the PHQ-9 on the digital platform enabled estimation of the TBD, arguably an index for treatment efficacy that is more sensitive to patient importance than time-to-an-episode let alone depression severity at the end of the follow-up period.
In conclusion, this study demonstrated that specific CBT skills – particularly the combination of behavioural activation and assertion training, as well as behavioural therapy for insomnia – had important preventive effects on the onset of major depressive episodes, reduction of the TBD and alleviation of depressive symptoms. Given the high prevalence and substantial societal impact of subthreshold depression, our findings suggest that smartphone-delivered CBT represents a promising strategy for population-level depression prevention.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10630
Data availability
De-identified individual participant data and the data dictionary will be made available 24 months after publication on UMIN-ICDR, an individual case data repository managed by the Japanese University Hospital Medical Information Network (UMIN) Center (https://www.umin.ac.jp/icdr/index.html). Proposals with specific aims and an analysis plan can be found in the Nature Medicine article (https://doi.org/10.1038/s41591-025-03639-1). Any queries in relation to that article should be directed to the corresponding author of that article, T.A.F. (furukawa@kuhp.kyoto-u.ac.jp). The R script for the primary analyses are provided in the Supplementary Material (Supplementary_Material_SAP_primary).
Author contributions
T.A., M.H. and T.A.F. conceived the study. H.N. and T.A.F. designed the study. Funding was obtained by T.A.F., M.H., T.A., N. Kawakami, T.N., N. Kondo, S.F. and H.N. T.A.F., M.H. and T.A. led the software development, with input from A.T., R.T., M.S. and Y.L. A.T., R.T., M.S. and Y.L. established the databases and managed the recruitment, data collection and processing, with help from N. Kawakami, T.N., N. Kondo and S.F. H.N. and T.A.F. undertook the statistical analyses, and had direct access to the full data. T.A. wrote the first draft, and all of the authors contributed to the interpretation and critical revision of the manuscript, and approved the final paper.
Funding
This study was supported by the Japan Agency for Medical Research and Development (grant number JP21de0107005), awarded to T.A.F. (principal investigator), A.T., R.T., M.S., Y.L., M.H., T.A., N. Kawakami, T.N., N. Kondo and S.F. The funder had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Declaration of interest
T.A. has received lecture fees from AstraZeneca, Chugai, Daiichi Sankyo, Eisai, Eli Lilly, Kowa, Kyowa Kirin, Lundbeck, Merck Sharp & Dohme, Meiji-Seika Pharma, Merck, Nipro, Otsuka, Pfizer, Shionogi, Sumitomo pharma, Takeda, Tsumura, UCB S.A. and Viatris, and a grant from Shionogi and royalties from Igaku-Shoin, outside the submitted work. T.A. serves as the representative director of the General Incorporated Association Nagoya City University Clinical Research Support System and receives compensation as an advisor to Snom Inc. T.A. has pending patents (2020-135195 and 2024-516288) (Institute) and patents (7313617) (Institute). A.T. reports personal fees from Eisai and Shionogi outside the submitted work. M.S. is employed in the Department of Neurodevelopmental Medicine, Nagoya City University Graduate School of Medical Sciences, which is an endowment department supported by the City of Nagoya, and has received a personal fee from SONY and Daiichi-Sankyo outside the submitted work. Y.L. is employed in the Department of Next-Generation Organ Transplantation, The University of Tokyo Hospital, which is an endowed department supported by the N28 General Incorporated Association, a non-profit organisation in Japan. M.H. has a patent (7448125) and has licensed intellectual properties for Kokoro-app to Mitsubishi Tanabe. N. Kawakami is employed by the Junpukai Foundation and the Department of Digital Mental Health, The University of Tokyo, an endowment department that is supported by an unrestricted grant from 15 enterprises (https://dmh.m.u-tokyo.ac.jp/en). T.N. reports grants or contracts with I&H, Cocokarafine, Konica Minolta and NTT DATA, consulting fees from Ohtsuka, Takeda, Johnson & Johnson, AstraZeneca and Nippon Zoki; payment or honoraria for lectures, manuscript writing or educational events from Pfizer, MSD, Chugai, Takeda, Janssen, Boehringer Ingelheim, Eli Lilly, Maruho, Mitsubishi Tanabe, Novartis, Allergan, Novo Nordisk, Toa Eiyo, AbbVie, Ono, GlaxoSmithKline, Alexion, Cannon Medical Systems, Kowa, Araya, Merck and Amicus; stock options in BonBon Inc.; and a donation from Cancerscan and JMDC, all outside the submitted work. S.F. received personal fees from Kyowa Kirin, Boehringer Ingelheim, Toray Medical, Health and Global Policy Institute, White Healthcare and Health Insurance for Start-up Companies, and research grants from the Japan Health Insurance Association, National Health Insurance Association for Civil Engineering and Construction, Osaka Prefecture and Cancerscan, outside this work. T.A.F. reports personal fees from Boehringer Ingelheim, Daiichi Sankyo, DT Axis, Micron, Shionogi, SONY and UpToDate, and a grant from DT Axis and Shionogi, outside the submitted work. In addition, T.A.F. has a patent (7448125) and a pending patent (2024-521973), and has licensed intellectual properties for Kokoro-app to DT Axis. The other authors declare no competing interests.
Relevance statement
Specific CBT skills – particularly behavioural activation + assertion training, behavioural activation + cognitive restructuring and behavioural therapy for insomnia – can effectively prevent the onset of major depression and reduce the total burden of depression at 50 weeks among individuals with subthreshold depression. Given its brevity, portability, accessibility and scalability, smartphone-based CBT is promising as a preventive intervention of major depression.
Transparency declaration
The lead author and manuscript guarantor affirm that the manuscript is an honest, accurate and transparent account of the research being reported; that no important aspects of the study have been omitted; and that any discrepancies from the original planned or (if applicable) registered study have been fully explained.






 Open access
Open access
eLetters
No eLetters have been published for this article.