


The causal relation between incidents of terrorism and mental illness has been the subject of a long running debate in psychiatric, sociological and criminological literature. Recent studies call for caution in establishing a linear relationship between mental disorders and terrorism, since prevalence studies and meta-analyses do not confirm this assertion. Reference Sarma, Carthy and Cox1,Reference Schulten, Doosje, Spaaij and Kamphuis2 Ho and colleagues discussed three highly relevant baseline principles. Reference Ho, Quek, Ho and Choo3 First, the majority of the terrorists are psychologically normal, and both group ideology and external factors might have even higher predictive value. Reference Ho, Quek, Ho and Choo3 Second, paranoid, antisocial and sadomasochistic personality traits have been associated with terrorist acts. In this regard, impulsive and emotionally unstable personality style was found in suicide bombers. Reference Ho, Quek, Ho and Choo3 Finally, lone actors are more likely to display mental illnesses (including schizophrenia, delusional disorder, antisocial personality disorder and autism spectrum disorder) than group actors. Reference Ho, Quek, Ho and Choo3 The possible association between mental disorders and acts of terrorism is of crucial importance for clinicians and society. Stakes are high and police, social and intelligence services count on mental health frameworks for risk assessment and prevention. Some assessment tools have been proposed. But they may still face some limitations. Reference Meloy and Gill4,Reference Bhui, Otis, Halvorsrud, Freestone and Jones5
In daily practice, the interaction between mental illnesses and the origins of extremist violence has not been fully elucidated, to the extent that practitioners are not always able to distinguish extremist behaviour due to psychopathology from that inspired by extremist ideology. Reference Schulten6 Therefore, one might wonder, for instance, whether a mentally ill person suffering from psychosis can be labelled ‘radicalised’ let alone ‘terrorist’. Reference Schulten6
The objective of this study is to identify and analyse all documented terrorist attacks in the Global Terrorism Database (GTD), containing incidents from 1970 to the first half of 2021, where the motive for terrorism is questioned due to suspected mental health issues.
Furthermore, this study aims to explore the potential link between mental health issues and acts of terrorism. By systematically reviewing those cases in which the classification as a terrorist act is uncertain, the study seeks to identify events that may be influenced by mental health concerns. Ultimately, the goal is to clarify the distinction between ideologically driven terrorism and acts of violence potentially rooted in mental health challenges, thereby informing future research and policy decisions.
Method
This study is based on a semi-quantitative, epidemiological analysis of all terrorism-related incidents from 1970 to 2020, as reported in the GTD. 7,8 Data collection was performed using a retrospective search through the GTD that was, until mid 2024, an open-source database containing over 200 000 worldwide terrorism incidents. The partial data from 2021 were never available online but were retrieved from the Microsoft Excel database (Microsoft Office LTCSC Professional Plus 2021, Microsoft Corporation, Redmond, Washington, USA; =https://learn.microsoft.com/en-us/microsoft-365/?view=o365-worldwide) that is made available on request for researchers.
The GTD is maintained by the National Consortium for the Study of Terrorism and Responses to Terrorism (START) at the University of Maryland, College Park, MD, USA. 7,8 In 2024, funding by the US government was terminated. As a consequence, data collection for 2021 will remain unfinished, only containing data from January till June. Furthermore, due to the loss of data, incidents from 1993 are not listed in the GTD.
The GTD defines terrorist attacks by non-state actors as follows: ‘the threatened or actual use of illegal force and violence by a nonstate actor to attain a political, economic, religious, or social goal through fear, coercion, or intimidation’. 7
An extensive description of the origin of the data and the methodology can be found in the GTD codebook, which is available on the GTD website. 8
In the context of the GTD, the label ‘doubt of terrorism’ refers to incidents with uncertainty or ambiguity about whether the attack meets the criteria to be classified as an act of terrorism. These doubts can arise due to factors such as: 8
-
‘(a) Lack of clear political, ideological, or religious motivation: for an event to be classified as terrorism, it must have an identifiable motivation related to these factors. If this is unclear or absent, the incident may be flagged as ‘doubtful.’
-
(b) Mental health concerns: when the attacker is found to have significant mental health issues, there may be uncertainty about whether his/her actions were driven by terrorist motives or personal, non-political factors.
-
(c) Criminal intent: if the primary goal of the attack seems to be criminal, such as financial gain or personal revenge, rather than advancing a political cause, there may be doubt about its classification as terrorism.
-
(d) Uncertain responsibility: in some cases, it may not be clear who carried out the attack or whether the group responsible for the attack can be classified as a terrorist organization.’
The full data-set of the GTD (1970–2020) was searched using the internal database functions and individual incident summaries. Ultimately, the included cases consist of terrorist attacks committed by mentally ill assailants or assailants under the influence of alcohol and/or drugs, of incidents attributed to (illicit-drug-induced) psychosis and of incidents in which authorities suspected the perpetrator to have a suicide-by-cop-motive. The same procedure was used to assess the partial data-set of 2021, made available for researchers as a downloadable EXCEL file.
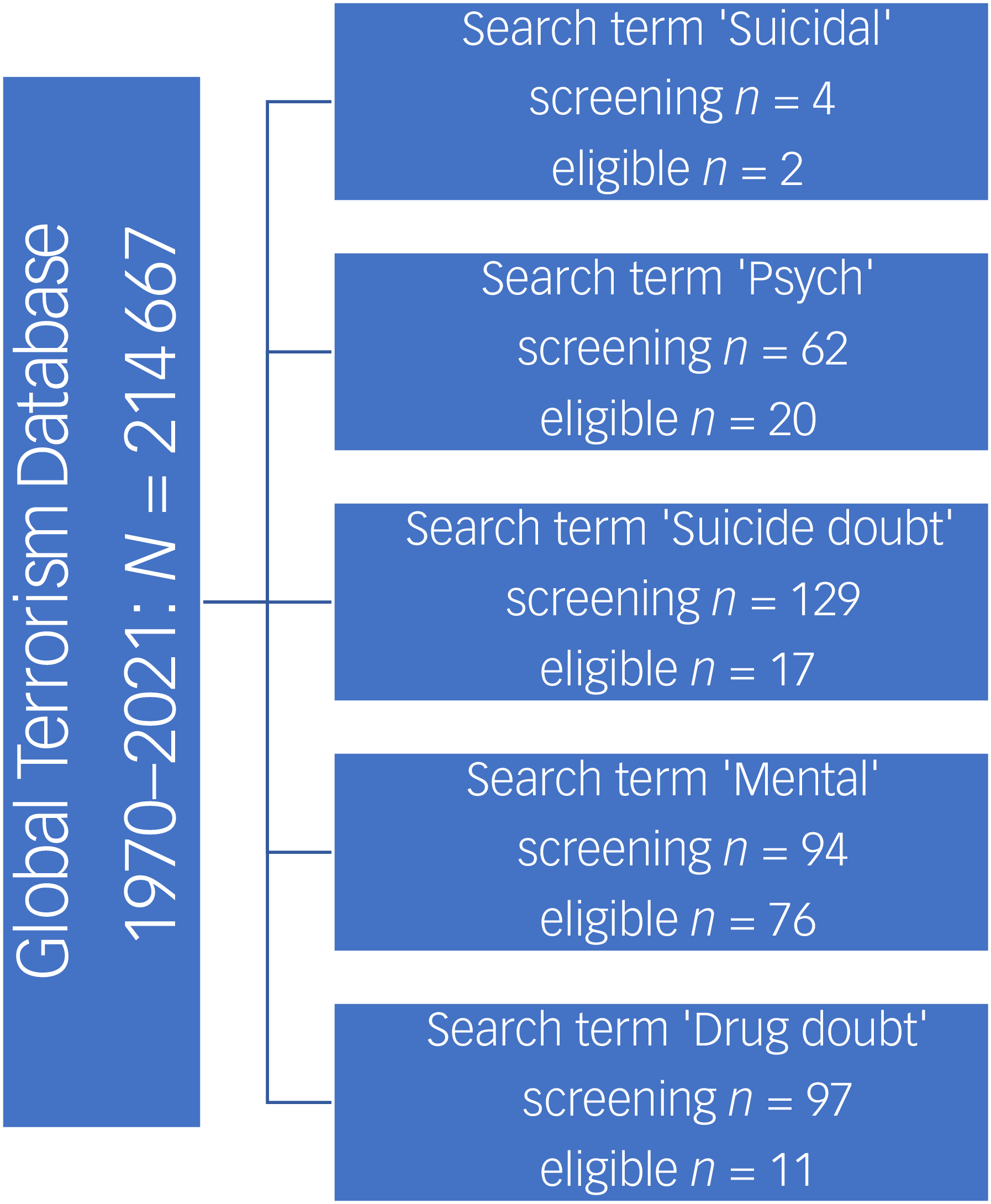
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram (Fig. 1) is provided for all subsets analysed. Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow9 The flow diagram depicts the flow of information through the different phases of the retrospective epidemiological analyses of the GTD: identification, screening and acceptance for eligibility. It contains the number of records identified, excluded and finally included, as well as the reasons for exclusions.
PRISMA flow diagram. Step 1: identification of all registered incidents in the GTD (1970–2021): N = 214 667. Step 2: screening for incidents with search terms ‘suicidal’, ‘psych’, ‘suicide doubt’, ‘mental’ and ‘drug doubt’: n = 386. Step 3: eligibility – incidents excluded because of insufficient data, not within the scope of this study (e.g. drug gang or drug traffic-related incidents, incidents against psychiatric hospitals): n = 126. Step 4: final exclusion of duplicates resulting in 107 incidents for further analysis.

Data collected per incident included temporal and spatial factors, type of target, type of weapon, perpetrator type and the number of casualties. To establish the perpetrator profile, additional information such as mental issues, conviction or internment and committal in psychiatric facilities was gathered by the GTD analysts in the additional information on the attack type or the incident summary.
Each entry was reviewed manually by H.D.C. for inclusion or exclusion based on the incident description. When in doubt about a case, a second author (F.S.) advised on the final decision. All collected data were exported into Excel spreadsheets and analysed descriptively.
Results
From 1970 to 2020, the GTD contains 102 incidents where mental illness, addiction or doubt of intent was mentioned in the incident summaries: ‘mental cases’. The database with semi-annual data from 2021 lists a total number of 4961 incidents, and contained five additional cases fulfilling the search criteria. Because the 2021 data are incomplete, the breakdown of incident characteristics will focus on the 1970–2020 data-set.
Temporal-spatial distribution
As the incident summaries of the first two decades contain far fewer variables and circumstantial information, the first two decades did not yield any hits. The majority of incidents (78%) were collected from the period 2011–2020, followed by 1991–2000 (n = 14; 13.7%) and 2001–2010 (n = 10; 9.8%). The additional database of 2021 contained five cases: two from North America (n = 59), two from the Middle East & North Africa (n = 1262) and one from Germany, Western Europe (n = 105).
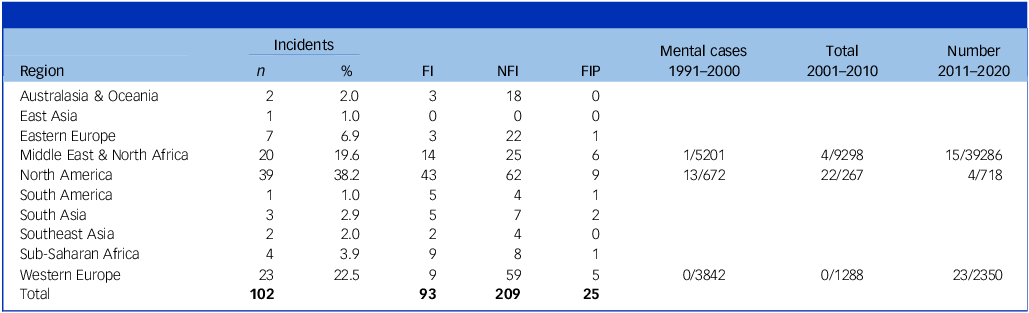
The incidents occurred globally. The majority of the attacks occurred in North America (38.2%), followed by the Middle East & North Africa and Western Europe, each accounting for almost 20% of the incidents (Table 1). In North America and Europe, there were relatively more cases in which an alleged association with mental illness and/or addiction was mentioned in the narrative. In North America, the incidence was as high as 8.2 and 3.4% of the number of terrorist attacks in this region in the periods 2001–2010 and 2021, respectively (Table 1).
Number of attacks per world region

FI, fatal injuries; NFI, non-fatal injuries; FIP, fatal injuries in perpetrators.
Impact of incidents
The 102 incidents from the first five decades resulted in a total of 93 fatal injuries and 209 non-fatal injuries (NFI). Twenty-five perpetrators died during the attacks.
Proportional to the number of incidents, the number of casualties was highest in the period 2011–2020, with 77 fatal injuries, 185 NFI and 22 fatal injuries in perpetrators (FIP), followed by 2001–2010 (7 fatal injuries, 18 NFI, 3 FIP) and 2001–2010 (9 fatal injuries, 6 NFI, 0 FIP).
The five cases from the first half of 2021 resulted in six fatal injuries, eight NFI and four FIP.
Aimed target types
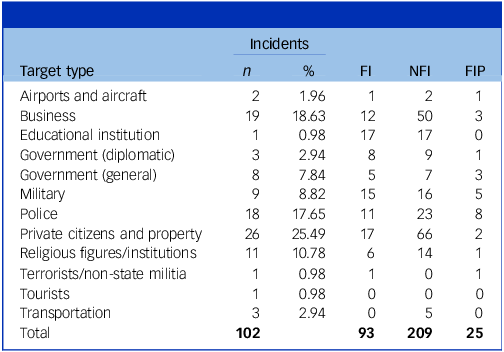
In this series, the most frequent targets were private citizens and property (n = 26; 25.5%), police forces (n = 18; 17.6%), business buildings (n = 19; 18.6%) and religious figures/institutions (n = 11; 10.8%) (Table 2). The highest perpetrator mortality rates were observed in attacks against the military (FIP n = 9; in 55.6% of the incidents the assailant was killed) and in bombings of ‘airports and aircraft’ (FIP n = 1; in 50% of airport attacks the perpetrator died). Of the 18 attacks directly targeting the police, 4 were labelled as possible attempts of ‘suicide by cop’ (deliberately threatening a police officer in order to provoke him to shoot), yet in only two alleged suicides by cops was the assailant was killed. In 8 attacks out of 18 (44.4%) targeting the police, the perpetrator died. One attack targeting educational institutions resulted in the highest number of fatalities (n = 17). Attacks on tourists and transportation constitute the other end of the pole by not leading to any fatalities.
Target types and related casualty numbers

FI, fatal injuries; NFI, non-fatal injuries; FIP, fatal injuries in perpetrators.
Attack types and perpetrator types
In the 1970–2020 period, attacks were predominantly carried out by lone actors (n = 98; 96.1%). ‘Armed assaults’ were the most frequent attack type (n = 68; 66.7%), followed by facility/infrastructure attacks (n = 10; 9.8%), hostage takings (n = 8; 7.8%), bombings/explosions (n = 7; 6.9%), unarmed assaults (n = 6; 5.9%) and hijackings (n = 3; 2.9%). While most lone actors only committed a single attack, eight (7.8%) incidents were committed by repeat offenders.
In 2021, the five assailants were all lone actors who were involved in only one incident each.
According to the incident summaries, terrorist motives were identified on the basis of the racist expressions assailants shouted immediately before the attack or on the basis of the terrorism-prone character of targets such as a church, a mosque, a rabbi, an imam, police and the military.
In this series, jihadist or Islamic extremism (shouting, e.g., ‘Allahu Akbar’, ‘They don’t read the Koran’, ‘Infidels’), anti-Semitism (targeting a rabbi or Israeli assets) and white-power beliefs (shouting neo-Nazi slogans, e.g. ‘Burn Arabs’, or targeting people of Arab, African or Asian descent) occurred frequently.
Events of doubted terrorism per reason of doubt
Underlying mental disorder and/or concomitant substance use disorder was suspected in cases of doubted terrorism. The individual incident summaries based on police reports, judicial outcomes, the defendant’s attorney’s opinion or the opinion of the GTD analysts contained several peripheral circumstances. Nevertheless, all the incidents were included in the GTD.
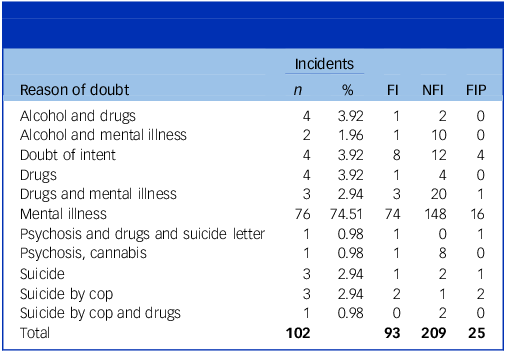
In 81 (79.4%) incident summaries a history of mental illness (e.g. schizophrenia (n = 1), bipolar disorder (n = 1), oligophrenia (n = 1), depression (n = 2), psychosis (n = 2) or mental illness or mental instability without further specification was mentioned (Table 3)). In two (1.9%) ‘psychosis’ was explicitly mentioned to be involved at the time of the incident. In seven incidents, suicidal ideation was noted (6.9%). Further, seven perpetrators had a history of being treated in a psychiatric hospital. Substance misuse was observed in 16 incidents (15.7%). In four cases (3.2%), there was a doubt of intent, without further specification of the nature of the suspected underlying mental illness. As can be derived from Table 3, different types of mental disorders can coexist.
Reasons of doubt of terrorist motives and related casualty numbers in the 1970–2020 database

FI, fatal injuries; NFI, non-fatal injuries; FIP, fatal injuries in perpetrators.
The extra five cases retrieved from the 2021 database were all doubtful: one suffered from a psychotic period ‘hearing voices that prompted him to commit this horrible crime’. Another perpetrator attempted suicide days before, and another was suicidal. The fourth case could have been a suicide-by-cop case. In the fifth case no further data were available
Judicial outcomes
According to the GTD, 25 perpetrators died on the scene, 18 were convicted (18 incidents) and 29 had unknown outcome. Nine perpetrators had not been sentenced, 5were committed to a psychiatric facility and data are lacking for the remaining 16.
In the cases from 2021, four died on the scene. The (judicial) outcome of the perpetrator with psychosis was not mentioned in the incident report.
Discussion
The relationship between mental illness and radicalisation is a subject of ongoing debate in the literature. In this study, the number of perpetrators with underlying psychopathology was low. While this suggests that mental disorders are not a mainstream common characteristic of perpetrators, it may be partly explained by the fact that the assailants’ possible psychopathological profile was not the main goal of data collection.
In fact, most other reviews fail to demonstrate a significant association between terrorism, radicalisation and mental illnesses, e.g. psychotic disorders. Reference Sarma, Carthy and Cox1–Reference Ho, Quek, Ho and Choo3,Reference Trimbur, Amad, Horn, Thomas and Fovet10–Reference Catapano, Cipolla, De Rosa, Milano, Vozza and Guadagno12 Furthermore, when comparing acts of terrorism and acts of homicide, no significant association with mental illness was found. Reference Theodorou, Sinclair, Ali, Sukhwal, Bassett and Hales13 Still, in some subsets of assailants and terrorist incident characteristics, mental illness issues could be involved. Reference Ho, Quek, Ho and Choo3,Reference Trimbur, Amad, Horn, Thomas and Fovet10–Reference Theodorou, Sinclair, Ali, Sukhwal, Bassett and Hales13
A recent comparative study by Theodorou and colleagues (2024) on family shooters, mass shooters and terrorists provided evidence of mental illness in only a minority of perpetrators, depression and psychosis being the most frequently reported underlying diagnoses. Reference Theodorou, Sinclair, Ali, Sukhwal, Bassett and Hales13 They concluded that no individual mental illness could be identified as the predominant risk factor in either of the subgroups. Hence, they underlined the importance of the interaction between mental disorders, socioeconomic factors, relationships and loss in determining individual risks.
Analysis of the Columbia (USA) mass murder database revealed that focusing on serious mental illness, e.g. psychotic symptoms, did not support preventive policies for mass murders. Reference Brucato, Appelbaum, Hesson, Shea, Dishy and Lee14
In our findings, lone actors prevail in terrorist attacks where psychopathology might be involved. Other studies provided similar evidence. Single issues and right-extremist lone actors have been studied most extensively. Reference Schulten, Doosje, Spaaij and Kamphuis2 Autism spectrum disorder, schizophrenia and delusional disorders were more frequent in lone actors than in the general population, but still only a minority of these perpetrators qualified for psychopathological characteristics. Reference Schulten, Doosje, Spaaij and Kamphuis2 Corner and Gill observed that lone actors were 14.3 times more likely to have a history of mental illness than group actors. Reference Corner and Gill15
A recent French study assessing 90 people in detention for jihadist terrorism confirmed the significant association between lone actors and psychiatric pathology, as 30% had an active psychiatric disease. The most frequent diagnosis was personality disorder, followed by schizophrenia, schizotypal disorders and delusional disorders, neurotic and stress-related disorders and somatoform disorders. Reference Monod, Ambar-Akkaoui, Levasseur and Pham-Scottez16
Additionally, socio-environmental (family dysfunction, friendships with radicalised individuals, an unstable geopolitical environment and societal polarisation) and neurobiological factors (structural and functional deficits in limbic and frontal brain areas) might be associated with terrorist behaviour. Reference Ho, Quek, Ho and Choo3,Reference Salib17
The 107 incidents listed in this series, resulted in a total of 99 fatal injuries and 217 NFI. Twenty-nine perpetrators died during the attack.
The possible relation between terrorism and mental illness or addiction is only addressed in the last three decades of the GTD. However, this series is likely an underestimation due to the lack of peripheral data on the incidents in the GTD before 1990, as established in previous GTD-based studies. Reference De Cauwer, Barten, Tin, Mortelmans, Lesaffre and Somville18–Reference De Cauwer, Granholm, Khorram-Manesh, Barten, Tin and Mortelmans20 Changing insight into this matter and a recent focus on the psychopathology of assailants might also be the reason for the growing number of assailants labelled as suffering from a mental disorder.
In this series, the typical attacker profile consisted of a lone actor with a(n assumed) mental illness committing an armed assault. This is in line with the above mentioned studies. Reference Schulten, Doosje, Spaaij and Kamphuis2,Reference Corner and Gill15,Reference Monod, Ambar-Akkaoui, Levasseur and Pham-Scottez16
Although 29 perpetrators were killed during the incidents, suicide by cop was reported in only five cases.
Suicide by cop is not similar to suicide bombings. In suicide bombings, suicide is merely instrumental, and not necessarily instilled by a psychopathological context. Suicide bombing is only one of many possible modes of attack and is rather driven by group-dynamic indoctrination and political motives. Reference Grimland, Apter and Kerkhof21
In these five analysed cases, psychopathological factors possibly played a role and were adjudged to take precedence over the perpetrator’s alleged narrative.
Armed assaults were the predominant attack type, followed by infrastructure attack, another difference with suicide bombings. Reference Tin, Galehan, Markovic and Ciottone22 The mean fatal injuries in this series was 0.91, far less than the mean fatal injuries in suicide bombings (9.66 per event). Reference Tin, Galehan, Markovic and Ciottone22
On the other hand, the most affected targets are similar in both groups: police, the military and private citizens and property, although in different order. Reference Tin, Galehan, Markovic and Ciottone22
In contrast with a previous study, none of the profiles of the five assailants suspected to have committed suicide by cop corresponded with the typical white male experiencing a romantic relationship conflict who has a significant mental health and criminal history and who is often intoxicated at the time of the offence. Reference Patton and Fremouw23
Bhui and colleagues found a similar profile in their assessment of sympathies for violent protest and terrorism: having major depression with dysthymia, anxiety, post-traumatic stress disorder, being young (<21 years), White and having previous criminal convictions were positively correlated with extremism. No associations were found with life events, social assets and political engagement. Reference Bhui, Otis, Silva, Halvorsrud, Freestone and Jones24
Similarly, in our study, none had previous convictions. One assailant did not match the age and race criteria (51-year-old male of Egyptian descent).
The others were definitely younger, but neither of them met the social or psychological profile. Due to the unavailability of forensic investigation results in the GTD, we are unable to thoroughly compare the perpetrator profiles.
Assessing the possible psychiatric background of perpetrators, the targets, the attack type, the motives, the outcome and the judicial aftermath can lead to a better understanding of the goals of such acts of terror. Eventually, this may refine initiatives to prevent terrorist attacks.
Law enforcement officers, social workers, public health authorities and (para)medical caregivers could play a role in preventing incidents, but they need tools to predict and assess imminent events. Treatment protocols have been established for assailants of terrorist attacks due to radicalisation.
Both risk assessment and therapeutic measures seem more efficient and valid in case of radicalisation than in mental illness-related terrorist incidents.
The TRAP-18 Terrorist Radicalisation Assessment Protocol, for instance, is a tool trying to assess the individual threat of targeted violence. Meloy and Gill’s study demonstrated four warning behaviours for successful attackers: leakage, pathway warning behaviour, fixation and identification. Reference Meloy and Gill4 Similarly, the Sympathies for Violent Protest and Terrorism (SVPT)-screening tool measures to what extent individuals sympathise/condemn seven specific actions (ranging from ‘committing a minor crime in political protest’ to ‘the use of suicide bombs to fight against injustices’). Reference Bhui, Otis, Halvorsrud, Freestone and Jones5
However, practitioners in mental health underline the challenges of risk-assessment procedures. From an ethical point of view, approaching ‘mentally ill’ or ‘radicalised’ people as potential terrorists is not only without scientific foundation but also diametrically opposed to the democratic values underlying our society. Reference Schumann, Brook and Heinze25–Reference Schuurman and Carthy27
It should be noted that radicalisation is not a mental disorder and that therapy for radicalisation is not always successful. On the other hand, the presence of the mental disorder could make someone more vulnerable to radical ideas or violent behaviour. Reference Schulten6
Once mentally ill perpetrators are convicted after a successful act of terror or committed in a psychiatric facility, Countering Violent Extremism programmes – added to regular mental health care – could be justified. Reference Schulten6
To conclude, despite the low prevalence among perpetrators, several attempts have been made in the literature to associate specific psychopathology, either personality traits or mental disorders, with terrorism. Whereas the personality traits ‘paranoid’, ‘antisocial’ and ‘sadomasochistic’ are associated with terrorists in general, ‘dependent’, ‘avoidant’ and ‘impulsive’ traits are more likely to occur in suicide bombers. Reference Ho, Quek, Ho and Choo3 When zooming in on lone actors, the mental disorders most frequently found are schizophrenia, delusions and autism spectrum disorder. Reference Schulten, Doosje, Spaaij and Kamphuis2 The study of Theodorou adds social role disjunction, motive, substance misuse and relevant risk or threat behaviours to the list. Reference Theodorou, Sinclair, Ali, Sukhwal, Bassett and Hales13
Importantly, the association is, however, not bidirectional: terrorist acts are not associated with mental illness, and radicalisation alone does not equal mental illness. Reference Schuurman and Carthy27 Although counterintuitive from the perspective of humanity, most terrorists are psychologically normal. Of those displaying mental difficulties or disorders, a majority had already developed these problems before they radicalised. Reference de Ridder, Fassaert and Grimbergen28 Instead of having predictive value, mental illnesses can be caused by involvement in terrorism or disable a person from engaging in larger goal-oriented activities. Reference de Ridder, Fassaert and Grimbergen28 Further, half of the perpetrators of mass shootings leaked their plans in advance, suggesting an opportunity for a mental health intervention. Reference Peterson, Erickson, Knapp and Densley29 Since radicalisation is not a static construct independent of individual, temporal and socio-environmental variables, the cause of radicalisation in terrorist violence should not be sought in individual experiences, vulnerability or even pathology; ‘it is the radicalisation process itself that forms the primary risk factor’. Reference Schuurman and Carthy27
In line with the commonly accepted biopsychosocial model in psychiatry, this paper confirms the importance of not only approaching mental health problems as a continuum, ranging from mental difficulties to strict DSM-5 diagnoses, but also of considering mental illnesses in perpetrators as the result of a dynamic process in which individual socio-environmental, neurobiological and cultural factors interact. Reference Sarma, Carthy and Cox1,Reference Ho, Quek, Ho and Choo3 Tools for risk assessment in potential terrorist perpetrators should be based on the widespread 4P model, which distinguishes between predisposing, precipitating, protective and perpetuating factors, which may vary over time. Reference Bolton30
Limitations
The GTD itself is subject to several limitations as discussed in earlier GTD-based research reports. Reference De Cauwer, Barten, Tin, Mortelmans, Lesaffre and Somville18–Reference De Cauwer, Granholm, Khorram-Manesh, Barten, Tin and Mortelmans20
The GTD includes only high-quality sources, creating a possible selection bias as not all acts of violence and possible terrorist attacks may be covered by news media. 7,8
The GTD’s standard practice is to report the lowest number of casualties when news articles provide conflicting information, and might thus underestimate the actual number of casualties. Reference Ellenberg, Taragin, Bar-On, Cohen and Ostfeld31
The GTD lists only immediate injuries and fatalities. It does not cover long-term disability or long-term medical sequelae, neither does it provide information on injury severities and outcomes. Reference De Cauwer, Barten, Granholm, Mortelmans, Cras and Somville32
As to the shortcomings of this study in particular, the psychiatric background of perpetrators is not registered in a specific tab in the database. This is only mentioned in the comments of the GTD analysts in the additional information on the perpetrator. As data are sparse in the earlier decades of the GTD registration, the total number of perpetrators with possible psychiatric disorder is certainly underestimated. We found no files from the period 1970–1990. The data information sheets of incidents that took place in the USA generally contain more peripheral details (e.g. perpetrators being sentenced or not, forensic psychiatric data) as more data sources were available to the analysts. This could partly explain the high incidence in North America.
Conversely, the GTD is less reliable on peripheral details for incidents outside the USA, which are not within the scope of the GTD.
Another important limitation is that these data are based on media-reported summaries rather than the medical reports of (forensic) psychiatrists. Furthermore, families and lawyers of assailants, could choose to plead temporary insanity for legal purposes.
Since the GTD contains data for only the first half of 2021, the full impact of the COVID-pandemic is not complete to assess these data. Nevertheless, the 2021 data suggest a higher incidence of cases that meet our case description.
Implications
Doubts about whether an incident qualifies as terrorism – due to factors such as underlying mental illness, substance use or ambiguous intent – have become more frequent in recent decades within the GTD, although earlier underreporting may partly account for this trend.
Another contributing factor may be the growing influence of legal strategies invoking insanity pleas to avoid trial; however, this study found that several perpetrators were still convicted, and only a minority were deemed unfit to stand trial.
The typical attacker in the sample was a lone actor with a presumed mental illness who carried out an armed assault. Although one in four perpetrators was killed during the incident, ‘suicide by cop’ was explicitly reported in only five cases, none of which matched the previously defined attacker profile.
This study hypothesises that a significant proportion of documented attacks in the GTD may be more closely linked to mental health concerns than to ideological motivations typically categorised as terrorism – although one should keep in mind that these data are based on media-reported summaries rather than clinically based (forensic psychiatric) diagnoses. Consequently, some incidents categorised as terrorism may instead reflect violent behaviours driven by mental health issues that do not align with conventional definitions of terrorism.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Author contributions
H.D.C., F.S. and K.V. conceived and designed the study. D.B., P.C. and G.C. contributed to the design of the project. K.V., A.K.-M., F.G. and H.D.C. drafted the manuscript. K.V., H.D.C., A.K.-M., D.B., D.T., F.G., F.S., P.C. and G.C. critically revised the manuscript, added to the discussion, worked on the adaptions suggested by the reviewers and approved the final version.
Funding
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.