


Impact statement
Forming a community-based, “safety net,” or a trusted and trained caregiving network, that includes family carers, religious leaders (at least for the Christians we interviewed) and biomedical providers working collaboratively through basic technology to provide coordinated care between hospitals and more rural areas, is important in low-resource settings. Voice-dialoguing approaches used in Europe to support people who hear distressing voices need to be a cultural mismatch in a region where hearing and speaking with one’s voices is stigmatized as signaling witchcraft-related activity. From our interviews with 43 patients in a low-resource setting in northern Tanzania who were hearing voices distressing enough to seek help at an outpatient nonprofit NGO, we identified participants’ ideas about how culture influenced the ways they identified their voices, experienced their voices, and sought treatment for those voices. Their approaches relied on local notions of health and well-being (e.g., mental wellness is related to moral wellness), explanatory models (e.g., hearing voices is a signal of witchcraft) and the limits of available supports (e.g., religious, biomedical and family support). Our findings reinforce the necessity for treatment pathways that foster collaboration between local and regional resources and mobilize and integrate multiple kinds of care providers while being sensitive to local culture.
Introduction
Hearing distressing auditory verbal hallucinations (AVHs) is a key symptom of psychosis (DeVylder et al., Reference DeVylder, Burnette and Yang2014; Ford et al., Reference Ford, Morris, Hoffman, Sommer, Waters, McCarthy-Jones, Thoma, Turner, Keedy, Badcock and Cuthbert2014; Waters and Fernyhough, Reference Waters and Fernyhough2017). Psychosis symptoms can occur in most major psychiatric disorders from psychotic disorder to posttraumatic stress disorder to autism (McCarthy-Jones, Reference McCarthy-Jones2012; Telles-Correia et al., Reference Telles-Correia, Ana Lúcia and Gonçalves2015; Köhler-Forsberg et al., Reference Köhler-Forsberg, Madsen, Behrendt-Møller and Nordentoft2021), and affects one to 4 % of the population globally, including in sub-Saharan Africa (Patel et al., Reference Patel, Simbine, Soares, Weiss and Wheeler2007; Kwobah et al., Reference Kwobah, Epstein, Mwangi, Litzelman and Atwoli2017; Green et al., Reference Greene, Yangchen, Lehner, Sullivan, Pato, McIntosh, Walters, Gouveia, Msefula, Fumo, Sheikh, Stockton, Wainberg and Weissman2021). According to the psychosis-continuum model, untreated psychotic symptoms that are disruptive to everyday life can be highly disabling, and – for vulnerable individuals experiencing stressful social contexts – can lead to the development of a psychotic disorder like schizophrenia (van Os et al., Reference van Os, Linscott, Myin-Germeys, Delespaul and Krabbendam2009; Butter et al., Reference Butter, Shevlin, McBride, Bentall, Hyland, Leavey and Murphy2023). In 2017, schizophrenia accounted for 12.7 million or .51% of all-cause Disability Adjusted Life Years (He et al., Reference He, Liu, Li, Guo, Gao, Bai, Bao and Lyu2020) and its effects are widely felt from the level of family to government.
Studies of urban youths experiencing psychotic symptoms in East Africa suggest that 9 % of Kenyan university students experience psychosis symptoms like AVHs (Jenkins et al., Reference Jenkins, Mbatia, Singleton and White2010, Reference Jenkins, Njenga, Okonji, Kigamwa, Baraza, Ayuyo, Singleton, McManus and Kiima2012; Ndetei et al., Reference Ndetei, Muriungi, Owoso, Mutiso, Mbwayo, Khasakhala, Barch and Mamah2012). Among Kenyan youths, women were more likely than men to report experiencing auditory hallucinations and had significantly higher severity scores regarding the sounds (Mamah et al., Reference Mamah, Mbwayo, Mutiso, Barch, Constantino, Nsofor, Khasakhala and Ndetei2012). Among Luo persons in Kenya and Tanzania, the rate of psychosis symptoms reported between 2004 and 2013 was significantly higher (6.9% in 2004 and 17.8% in 2013, p < .001) among women, but not men (Jenkins et al., Reference Jenkins, Othieno, Ongeri, Ogutu, Sifuna, Kingora, Kiima, Ongecha and Omollo2015). Maasai women in northern Tanzania (men were not interviewed) also reported higher rates of AVH compared to other sub-Saharan studies, with a prevalence of 39.4%, which were also correlated with high psychosocial stress and trauma exposure (Myers et al., Reference Myers, Mollel, Pauselli, Chacon and Compton2025). In South Sudan, psychotic-like experiences, which are instances of delusions or hallucinations, had a prevalence of 23.3%, but women had a lower rate compared to men and there was a correlation between traumatic events and psychotic-like experiences (Ayazi et al., Reference Ayazi, Swartz, Eide, Lien and Hauff2016).
However, even though we know that distressing AVHs are a commonly experienced symptom of multiple serious psychiatric conditions that can have long-term negative consequences if unchecked, there is limited research about how people manage them, especially in sub-Saharan Africa where there are limited biomedical professionals available (World Health Organization, 2017). For example, at last count in 2017, there were 41 psychiatrists and 236 psychiatric nurses to serve around 65 million Tanzanians (World Health Organization, 2017). In such a low-resource context, many people lack access to biomedical support.
In addition, barriers like accessibility and financial resources affect the kinds of treatment patients seek (James et al., Reference James, Wardle, Steel and Adams2018). Research suggests that in Nigeria, people in need of mental health care seek help from traditional and religious healers first (Abiodun, Reference Abiodun1995; Gureje et al., Reference Gureje, Acha and Odejide1995; Adeosun et al., Reference Adeosun, Adegbohun, Adewumi and Jeje2013). In Kenya and Uganda, a mix of traditional and allopathic treatment for psychosis is common (Beckerleg, Reference Beckerleg1994; Teuton et al., Reference Teuton, Dowrick and Bentall2007). There is little evidence indicating that religious healers are effective in treating serious mental health disorders, but some suggest that there is potential for traditional medicine, in conjunction with biomedicine, to be used in LMICs to fill the care gap (Gureje et al., Reference Gureje, Nortje, Makanjuola, Oladeji, Seedat and Jenkins2015; Nortje et al., Reference Nortje, Oladeji, Gureje and Seedat2016). However, some research also characterizes religious healers as a barrier to receiving formal mental health care (Burns and Tomita, Reference Burns and Tomita2014).
This article focuses on a clinical population of persons who reported hearing distressing voices that had accessed biomedical care at a tertiary clinic attached to a semiurban hospital in northern Tanzania. Families sometimes traveled hours to seek care, and no inpatient facilities were available. In 2015, when this study was conducted, 431 patients visited this clinic. Patients received free mental health consultations with nurses, who then prescribed them medications based on their needs. There was one social worker there who could provide therapy, but patients rarely had the opportunity to participate due to financial and transportation issues. Beyond an initial handout from the government pharmacy, which was never enough because what was in stock was very limited, patients had to pay out-of-pocket for the medicines prescribed at a local pharmacy, which could be costly. Helping persons manage distressing voices with very limited access to medication, and almost no social workers, nor any other “safety net” interventions like public housing or food vouchers, presented a challenge.
In Europe, community-based approaches for voice-hearing emerged initially from research with voice-hearers who were not receiving clinical care and discussions of the strategies they used to manage those voices (Romme and Escher, Reference Romme and Escher1989, Reference Romme and Escher1993, Reference Romme and Escher2000; Branitsky, Reference Branitsky2017). The result was the formation of “hearing voices groups,” which encouraged participants to explore their voice-hearing experiences with their peers. Over time, these groups set themselves apart from other groups run within the mental health system because attendance was not required and they encouraged the building of authentic relationships (Hornstein et al., Reference Hornstein, Robinson Putnam and Branitsky2020; Hornstein et al., Reference Hornstein, Branitsky and Robinson Putnam2021; Hornstein et al., Reference Hornstein, Branitsky and Robinson Putnam2024). The effects of belonging to such “hearing voices” mutual support groups helped participants feel more hopeful, have fewer hospital visits, and find professional success.
Also in Europe, clinical researchers have developed psychotherapeutic interventions to help people manage distressing voices when medications were not desired or available (Birchwood and Trower, Reference Birchwood and Trower2006; Craig et al., Reference Craig, Rus-Calafell, Ward, Leff, Huckvale, Howarth, Emsley and Garety2018; Heriot-Maitland et al., Reference Heriot-Maitland, Gumley, Wykes, Longden, Irons, Gilbert and Peters2023; Longden et al., Reference Longden, Branitsky, Jones and Peters2023). Cognitive behavioral therapy for psychosis (CBTp), the gold standard approach, aims to reform the patient’s cognition of and behavioral responses to voices to reduce the distress caused by persecutory voices, emotional comorbidities and stress, which can all contribute to persistent voice-hearing (Birchwood and Trower, Reference Birchwood and Trower2006). CBTp specifically aims to reduce the perceived power of the voices (Kråkvik et al., Reference Kråkvik, Gråwe, Hagen and Stiles2013). Originally, it was developed as an individual treatment and later became a group-based intervention (Guaiana et al., Reference Guaiana, Abbatecola, Aali, Tarantino, Ebuenyi, Lucarini, Li, Zhang and Pinto2022). Typically, the therapy is administered by a trained professional, ranging from therapists to social workers.
Building on CBTp and the Hearing Voices approaches, “Talking With Voices” was developed by a person with lived experience of voice-hearing, Eleanor Longden, and involves a therapist and patient dialoguing with the patient’s voice or voices during 26 structured sessions. In the sessions, the patient and their therapists build positive relationships with the voice, eventually allowing the therapist to guide the patient in gaining control over them. A recent Randomized Clinical Trial (RCT) found “signals” of efficacy in reducing dissociation, voice-hearing, and perceptions of recovery for this intervention (Longden et al., Reference Longden, Branitsky, Jones and Peters2023). A multi-site RCT is currently underway.
Similarly, AVATAR approaches are an individual therapy that involves digitally crafted visual and auditory representations of patients’ voices, which are then controlled by a trained therapist from another room while the patient interacts with them (Leff et al., Reference Leff, Williams, Huckvale, Arbuthnot and Leff2014). The therapist has the avatar representation of one’s voices become gradually less hostile and eventually the avatar gives up its power over the voice-hearer. Learning to assert oneself over the voices may be helpful to decrease severity and frequency (Craig et al., Reference Craig, Rus-Calafell, Ward, Leff, Huckvale, Howarth, Emsley and Garety2018; Garety et al., Reference Garety, Edwards, Jafari, Emsley, Huckvale, Rus-Calafell, Fornells-Ambrojo, Gumley, Haddock, Bucci, McLeod, McDonnell, Clancy, Fitzsimmons, Ball, Montague, Xanidis, Hardy, Craig and Ward2024).
Another approach is compassion-focused therapy for psychosis (CFTp), which involves the voice hearer approaching their self-critical thoughts (not the negative voices) with curiosity and compassion to counteract adversities commonly experienced by people with psychosis. CFTp can achieve positive social mechanisms like reducing self-criticism to decrease malevolent voices, as well as delusions and depression (Heriot-Maitland et al., Reference Heriot-Maitland, Gumley, Wykes, Longden, Irons, Gilbert and Peters2023). This therapy can be implemented as individual or group therapy (Braehler et al., Reference Braehler, Gumley, Harper, Wallace, Norrie and Gilbert2013) and is traditionally delivered by clinicians.
The research presented here sought to explore the first-person experiences of distressing voice-hearers in low-resource settings to consider what might be feasible and acceptable to them as an intervention as compared to these peer and therapist-led voice-dialoguing approaches for those living in high-income countries. This addresses an important gap in the literature because most interventions developed to manage voices have been developed and tested in the Global North. The research team interviewed people seeking nonspecialized treatment who reported hearing distressing voices to better understand how people in this social context thought about health and mental health, how they thought of their voice-hearing experience, the explanatory models they used for voice-hearing, and the local strategies they used to find support and take care of themselves.
Overall, we found that mental health was often defined in terms of relational wellness – being socially oriented, performing well for others (in school, at work) and not engaging in antisocial activities (e.g., socially undesirable behaviors). Experiences of voice-hearing were typically negative and were seen as a signal of social unwellness that was often distressing. The presence of malevolent voices signaled that people were perceived as vulnerable to witchcraft and demonic attack and may have been involved in witchcraft themselves. In addition, people appreciated biomedical care the most but approached religious healers first. Such a contrast in the ways people thought of their symptoms culturally calls for more nuanced efforts to implement voice-hearing approaches in the Global South.
Methods
In 2015, the lead author (who has conducted 6 months of ethnographic fieldwork in the region across 3 years) worked in partnership with the psychiatric nursing Director of the Arusha Mental Health Trust, the local nursing staff and two native Tanzanian research assistants who were also fluent in Kiswahili (the main language in Tanzania) on this collaborative interview study. All patients who were visiting the clinic for outpatient appointments during June and July 2015 were invited to take part in the study by their local Tanzanian mental health nurse during admissions if they reported hearing distressing voices either currently or in the past as one of their symptoms. Inclusion criteria for participants included being over the age of 18 and reporting hearing voices currently or in the past. Exclusion criteria were an inability to respond to the study screening questions. While this may have biased the sample if someone experienced distressing voices but could not share basic answers correctly, self-report is required in all hearing voices studies.
Once referred, the patients went through a consent process for a same-day interview with one of the two native Kiswahili-speaking research assistants who had received training in research methods, ethics, and the interview protocols. Many were willing to engage in an interview because wait times to see clinical staff could last for hours, and also likely because we were offering a $5 gift, about the equivalent of a half day of salary. If they expressed interest, they were verbally consented per human subjects regulations.
Once they had provided informed consent, they were then engaged in an audio-recorded qualitative interview about their experiences with mental health and hearing voices. First, the same two trained native Tanzanian research staff fluent in the local form of Kiswahili offered them adaptations of three English-based interview protocols (two reported here) in Kiswahili, the national language of Tanzania. The Kiswahili interviews included the Kessler-10 Swahili version (Kessler et al., Reference Kessler, Andrews, Colpe, Hiripi, Mroczek, Normand, Walters and Zaslavsky2002) that assessed past 30-day psychological distress in ten questions with a Likert scale and the Hearing Voices Protocol Interview used in published studies about voice-hearing across cultures (Luhrman et al. Luhrmann et al., Reference Luhrmann, Padmavati, Tharoor and Osei2015). We also added some questions about defining mental health and happiness in the local context, how people defined mental health and mental illness, and where they sought out help for mental illness.
All interviews were audio-recorded and then professionally transcribed into English over the next year by another Tanzanian native research assistant fluent in Kiswahili and English. Transcriptions were then uploaded into the qualitative data analysis software, Dedoose, where the second and third authors (both trained in qualitative methods) generated open codes related to the data. Codes were then tested, refined and narrowed by consensus to generate a codebook, then applied by the same authors. Codes were then grouped into themes of interest, which included: how mental health was defined in the interviews; how people experienced and explained their own voice-hearing; and, how they defined mental health recovery, all of which are relevant to planning interventions that address voice-hearing in locally feasible and acceptable ways.
Results
Demographics
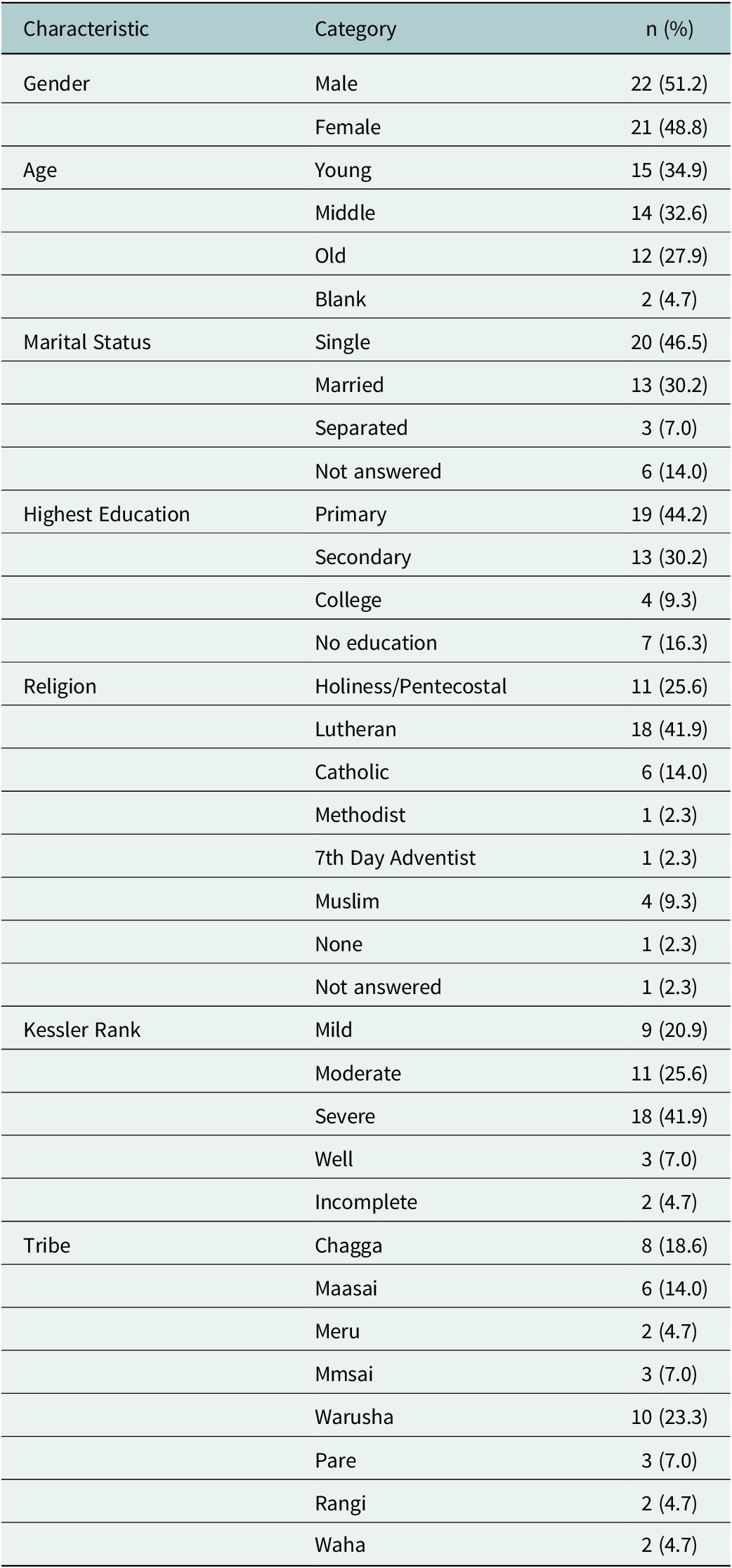
Forty-three individuals qualified as persons who heard distressing voices when they sought out clinical mental health support (see demographics, Table 1). The sample was balanced by gender. Age groups were well distributed across young (18–34 years old), middle (35–55 years old), and older adults (55+ years old). Two patients’ ages were not recorded. Self-reported religious orientations were primarily Christian; four participants identified as Muslim. Participants reported belonging to eight different ethnic groups (which they all “tribes), with the most prevalent being Warusha, Chagga, and Massai. Over half had achieved their highest education level (if any) in primary school (under age 14).Footnote 1 Another one-third had attended at least some secondary school. Almost half were single and another one-third were divorced.
Participant demographics (N = 43)

Notes:
- Percentages are rounded to one decimal place.
- The “Blank” category under “Age” refers to participants who did not provide an age.
- The “Incomplete” category under Kessler Rank indicates participants who did not complete the assessment.
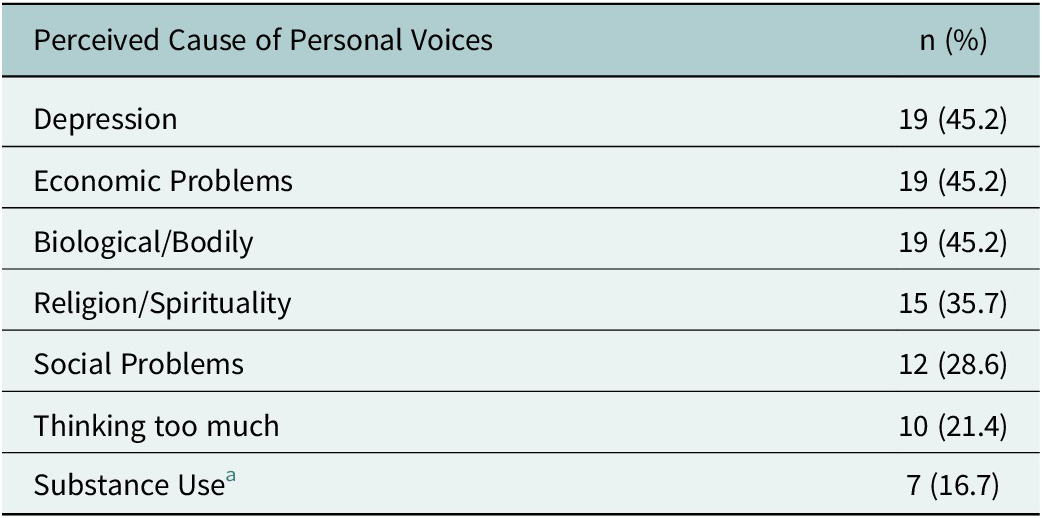
Perceived causes of personal voice-hearing among participants (N = 42)
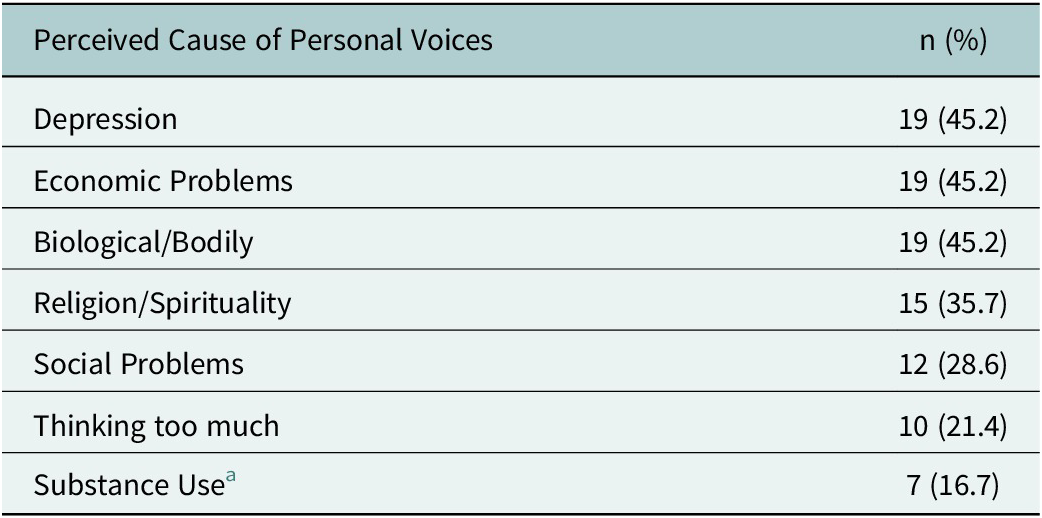
a Substance use was frequently mentioned by participants as a cause of mental illness generally but less commonly identified as a personal cause.
Most (88%) also met criteria for some form of psychopathology based on past 30-day stress, according to the Kessler-10, with nine (21%) showing mild psychopathology, eleven (26%) moderate, and eighteen (42%) severe.
Thematic findings
Overall, there were several findings relevant to the planning of future interventions, including information about help-seeking, what shapes access to biomedical care, what people expect from a mentally healthy life, what they think caused their AVHs, what their primary explanatory models were for their voices, and their perspectives on help-seeking options like psychopharmaceuticals, hospitals, traditional healing, religious healers, supportive relationships, and self-help. Please see Table 4 for frequencies and exemplary quotes.
Where do people go for help with their voices? (n = 43)

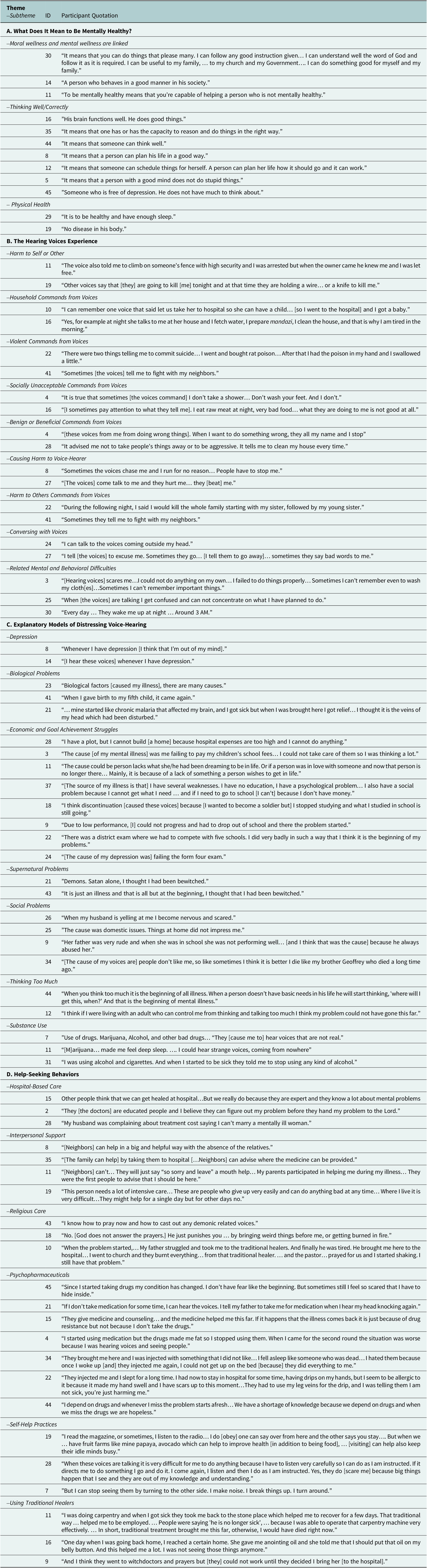
Sample quotations by theme/subtheme
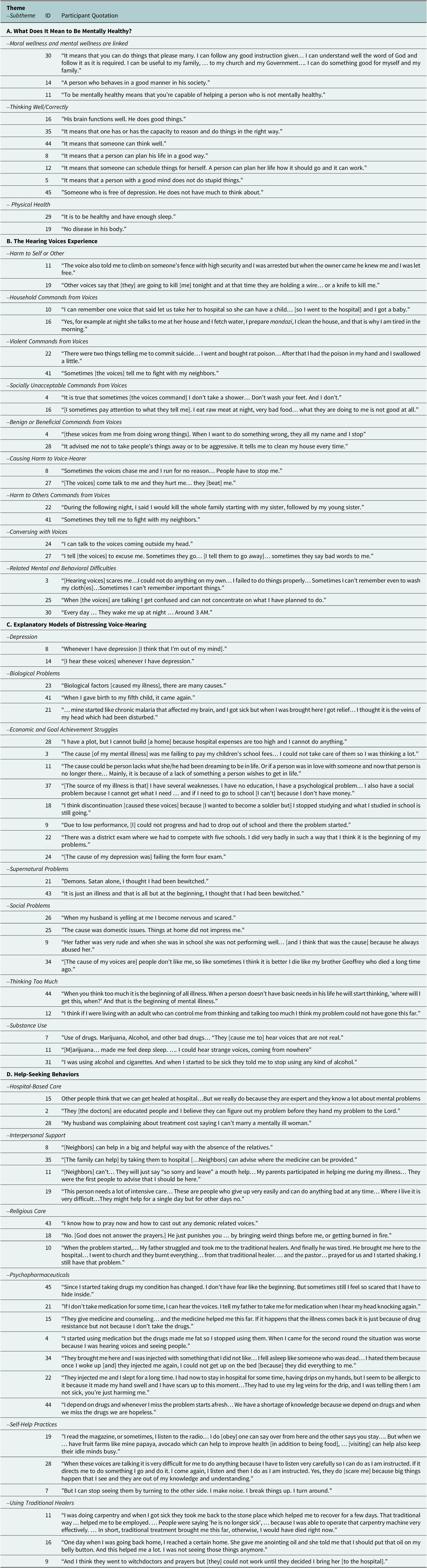
Kuwa na afya ina maana gani kwako wewe? (what does it mean to be healthy?)
Several participants defined being healthy in terms of moral wellness, such as being or doing good things. For example, a healthy person could distinguish between local definitions of “good” and “bad” while also making the right choices and engaging in positive ways with family, church, government, and God. A few also described being mentally healthy as helping and advising others and being socially oriented, which were moral values in this region. For several interviewees, the definition of being mentally healthy also included how well one’s brain or mind seemed to be performing, the ability to plan and organize one’s life, and not engaging in activities thought to be irrational or foolish. A few also noted it was important to be free of depression and “thinking too much.” A few more described physical health as part of mental health, such as eating or sleeping well or the absence of diseases like malaria in their body.
Experiences of voice-hearing
About four-fifths of the interviewees offered in-depth details about their experiences of hearing voices, of which the majority (88%) reported negative experiences. Three-fourths reported hearing “command” voices, which for about one-fourth of patients included instructions to engage in dangerous behaviors that put them at risk or were harmful to others. Of those, about half heard household-related commands (e.g., recommending they do chores), and one-fourth heard violent commands (e.g., poison your family) or commands to act in socially unacceptable ways (e.g., not bathing). Over two-thirds reported that their voices attempted to harm or actively harmed them (the voice-hearer), with examples including: physically pushing them, raping them, causing them to run incessantly, causing them to hide from the voices and others, or causing self-harm. Around one-fourth reported being told to harm others. When asked about conversing with voices, only 21 responded, with 11 not answering. Of those asked, only one-third reported speaking to their voices. Several reported difficulties performing basic tasks, as well as fear, confusion, forgetfulness, and disrupted sleep, which they attributed to the voices. Almost one-third also experienced benign or even beneficial voices.
Explanatory models of distressing voice-hearing
Most people offered more than one explanation for their voices (see Table 2). About half of individuals told us that their personal voices were caused by depression, biological causes, or economic problems. Another one-third attributed them to supernatural causes and social problems. For one-fifth, thinking too much and substance use were also mentioned.
Some attributed their distressing voices to mental characteristics like depression. Biological factors like giving birth and malaria were also mentioned. Patients described economic problems related to their income, like not being able to pay their medical bills, take care of their children, and marry because of financial struggle. Failing to achieve one’s goals was a challenge. Economic struggles made it difficult to pursue further education, which left patients feeling as thought they could not keep progressing forward in life. Around one-third of the patients also talked about stress from school directly contributing to their voice-hearing. Specifically, taking school exams, which must be passed to continue one’s education in Tanzania, was linked with auditory hallucinations.
Some blamed supernatural forces like demonic activities or being the target of witchcraft. Also, patients thought social problems like childhood trauma, violence and domestic disputes could cause distressing voices. Sometimes, an overactive mental process, termed “thinking too much” was thought to explain their auditory hallucinations. A few also thought using alcohol, cannabis and cigarettes were causal factors.
Help-seeking and pathways to care for mental health concerns
Over half of the persons interviewed talked about seeking relief from their symptoms in hopes of achieving mental health again (see Table 3).
Hospital-based Care
Nearly everyone claimed that hospitals were the best place for treatment. Many expressed trust and respect for doctors. The financial burden of using hospital-based care was also mentioned.
Interpersonal Support
For nearly everyone, interpersonal relationships played a significant role in descriptions of healing and recovery. People reported receiving aid from neighbors, family, and friends, especially in accessing treatment. Additionally, close friends and family supported them in properly taking their medication. Relatives also helped care directly for the patient’s family (e.g., their children) and finances. A few people thought only relatives could aid them in mental health recovery. One felt his illness had placed a burdensome toll on those who helped him.
Religious Care
About three-fourths also mentioned using a religious healer and prayer as a resource for recovery. When distressed by the voices, many prayed or went to services to manage their voices and stop them from occurring. However, some also thought religion inspired fear rather than encouragement. A few also described how church treatment conflicted with other means of recovery.
Psychopharmaceuticals
Around three-fourths of participants shared thoughts about taking medications, although they had mixed views on whether medications helped with their symptoms. Most said that prescribed medications and injections helped them and were things they wanted to access more. Around one-fourth of the patients also talked about experiencing a mental illness relapse, typically when they stopped taking medication, although the reasons were not always clear. Some also claimed to relapse even with biomedical treatment, but they still sought it out. Several also described the adverse effects of medications, such as gaining weight, feeling sleepy, having a dry throat, and losing one’s appetite and how that led to their inconsistent medication use. A few also discussed an adverse feeling towards injections of sedatives. Some thought that taking medications might shorten their life. Others described how drug shortages led to hopelessness and fears of relapse.
Self-Help
Almost two-thirds of patients described trying to manage their “voices” with self-help practices. Distraction was an important tool, including reading, listening to or making music, listening to the radio, talking to other people, and talking to themselves. People reported that sometimes they obeyed the voices’ commands to quiet the voices by appeasing them. Some also talked about physically turning their backs to their voice or smashing or breaking objects to frighten them away.
Traditional Healers
Of the one-third who mentioned traditional healers at all, only one-third of those said they had used one themselves, and they reported mixed results. A few of the participants who used traditional healers reported that this type of treatment was helpful to recover. However, some also described traditional treatments as not working well.
Discussion
Peer support between people who have also experienced psychosis or at least serious mental distress is an important intervention in Europe and the US (e.g., Myers, Reference Myers2015), but interventions involving family and other community-based relationships may be key in this context given the cultural sensitivity around how voices were interpreted culturally. Sixty percent of the people we interviewed recognized the voices as a living person – a relative, neighbor, enemy, or stranger. In Tanzania and much of Africa, witchcraft attacks by envious neighbors or relatives are a well-recognized source of misfortune and illness, including mental distress (e.g., Green, Reference Green2005; Marsland, Reference Marsland, Harper and Adams2015; Taylor et al., Reference Taylor, Bradbury-Jones and Lund2019). In a social context where good social relationships are key for health and well-being, being the subject of witchcraft attempts signals the distressing news that one is socially unwell or has been socially deviant. Creating a group of people in the name of “peer support” who may be locally interpreted as being attacked by witchcraft or practicing witchcraft and acting as sorcerers against others could make them a target of further magical attack or of social stigma.
Additionally, two-thirds of our participants said they did not try to interact intentionally with their voices, which they typically described as malicious agents, suggesting that Euroamerican approaches that involve getting to know, having compassion for, asserting oneself over, or dialoguing with voices may not be culturally acceptable in this setting. Even therapist-led approaches like CBTp involved interacting with voices, which may not fit in this context. Moreover, in such a low-resource setting, it is unlikely that approaches like CBTp that require time and training can be delivered feasibly.
One target for future early interventions may be Tanzanian schools. School exams were described as a major stressor by participants that affected their experience of voices and related mental health symptoms. School-based mental health counselors or training for teachers in free online training programs like Mental Health First Aid (https://www.mentalhealthfirstaid.org/) may help improve support for young people during these challenging times.
In addition, interpersonal relationships were a strong source of well-being and care for our participants, who claimed that relatives helped with medications, social support, and morale, as well as transportation, housing and financial support. These data point to the burden this imposed on the family, which patients acknowledged openly, and the first author observed. This has also been noted elsewhere, including in sub-Saharan Africa (e.g., Addo et al., Reference Addo, Agyemang, Tozan and Nonvignon2018; Mbedzi et al., Reference Mbedzi, van der Wath and Moagi2024). However, in Tanzania, there were no family support groups at the time. Implementing family mutual support groups could help fill a much-needed gap in preventing carer burnout, as families are the social safety net in this setting.
Far fewer participants than we anticipated (around one-third) described going to a traditional healer for mental health support. Those who did added (unbidden) that it was a waste of time and money. This is surprising because much of the global mental health literature suggests traditional healers are perceived to be an effective source of mental health care in sub-Saharan Africa and are the first stop for care for around 80 % of the population (World Health Organization, 2002, 2019; Abbo, Reference Abbo2011). Given that many global mental health initiatives focus on partnering with traditional healers (Okello and Musisi, Reference Okello, Musisi, Akyeampong, Hill and Kleinman2015), it might be worth considering what local people think of those healers specifically for mental health concerns.
Instead, without being directly asked, three-fourths of the people interviewed also mentioned going to a religious healer for help with their mental health concerns and most went there first. Only one person directly said they did not use religious healers. Religious healers offered advice and prayers. This suggests faith-based approaches might be one way to supplement biomedical support for persons hearing voices in Tanzania who identify as Christian, perhaps especially because “health” in this social context seems linked to moral wellness and churches discourage people from visiting traditional healers. While Lee et al. (Reference Lee, Coleman, Nakaziba, Terfloth, Coley, Epparla, Corbitt, Kazungu, Basiimwa, Lafferty, Cole, Agwang, Kathawala, Nkolo, Wogali, Richard, Rosenheck and Tsai2025) claim that traditional and faith healers have not thus far “change[d]” the course of severe mental illness regionally, there is likely more work to be done in this area as some positive, cost-effective outcomes have been identified in Nigeria and Ghana (Gureje et al., Reference Gureje, Appiah-Poku, Bello, Kola, Araya, Chisholm, Esan, Harris, Makanjuola, Othieno, Price and Seedat2020).
The range of explanations for what caused the voices were similar to those identified recently in Uganda (Lee et al., Reference Lee, Coleman, Nakaziba, Terfloth, Coley, Epparla, Corbitt, Kazungu, Basiimwa, Lafferty, Cole, Agwang, Kathawala, Nkolo, Wogali, Richard, Rosenheck and Tsai2025) and demonstrated a keen awareness of structural challenges to maintaining mental health, including economic (e.g., unemployment, lack of money to eat or go to school) and social (e.g., family arguments, divorce) challenges. Many people also recognized a biological cause that they labeled as depression – and at times malaria or childbirth–which may have been linked to the treatment they received at the hospital where such explanations were likely offered (and clearly also accepted).
This array of explanatory models for people hearing distressing voices suggests that pathways to care in this region range from being easily accessible and affordable (such as going to church for prayer and advice) to more expensive and less accessible (such as hospital-based interventions and pharmaceutical treatment). While a voice-focused form of peer support could invite witchcraft-related stigma, perhaps mutual support groups for depression or medication management or to learn social skills or have family therapy could be appealing and keep people safe from additional stigma.
It is important to acknowledge the limitations of our study. Limitations included that Tanzania is a diverse country ethnically and so the sample lacked representation across Tanzania’s 130+ ethnic groups. In addition, only 10 % of the study population identified as Muslim, while the Muslim Tanzanian population, in general, is around 34% (Hackett et al., Reference Hackett, Stonawski, Tong, Kramer, Shi and Zanetti2025). One influencing factor may be that the data were collected in a clinic originally started (but not currently run) by Catholic missionaries. The Muslim population may have access to alternative carers, which could include private clinics or hospitals, or other kinds of religious or traditional healers. There were also fewer married people in the sample than in the general population. In addition, our exclusion criteria were the inability to respond to the initial study screening questions. This could have led to a sample bias where those who were extremely impaired were potentially underrepresented, even though the Kessler scores indicated that people experiencing severe psychopathology were represented well. Finally, the interview data we analyzed for the qualitative process were translated from Kishwali to English, and it is possible some cultural phrases did not translate well. To mitigate this, we were able to consult the translator on points of confusion directly.
While nearly everyone who went to the outpatient clinic seemed to prefer biomedical care over all others, basic biomedical care for mental health in Tanzania was not possible for most (Patterson, Reference Patterson2023). Even so, our participants described trusting the doctors and the medications. It is possible that the patients were afraid to express anything but delight in their care; however, we were not asking anything specific to the hospital, and they were interviewed confidentially by persons who were not employed by the hospital, all of which was made clear in the consent process. We also assured them their recordings would be kept confidential. Another possibility is that outpatient, hospital-based care in a mental health specialty clinic in a country where there were extremely few resources was highly desirable and satisfying. A similar finding was recently reported in Uganda (Lee et al., Reference Lee, Coleman, Nakaziba, Terfloth, Coley, Epparla, Corbitt, Kazungu, Basiimwa, Lafferty, Cole, Agwang, Kathawala, Nkolo, Wogali, Richard, Rosenheck and Tsai2025), but more research would be needed to understand further. Despite people expressing a positive impression of biomedical care, our Kessler-10 scores indicated that in the past 30 days, most people were experiencing symptoms or psychopathology. People need more community-based support that is sustainable, accessible, and effective.
Conclusion
Adapting Euroamerican approaches derived from CBTp and using voice-dialog approaches are likely a cultural mismatch for this setting. Tanzanians do not have reliable access to trained therapists and technology. Therapeutic approaches that offer training and support to people who interact with persons hearing distressing voices on the frontline, like school personnel, family members and religious healers, could be more effective. They can work to support people earlier on in their symptom course than expensive and inaccessible hospital care, as well as in between hospital visits if a crisis does occur.
In this region, patients rely on and trust family, religious leaders, and biomedical treatment for support with their mental health needs. Networking the three together to offer regular, basic interventions for psychosocial support with persons who are experiencing psychotic symptoms could create a sustainable resource for long-term therapeutic follow-up and mutual support (e.g., families helping families). Religious healers may be especially appropriate carers, as they can be helpful when people are afraid to dialog or interact with voices thought to be caused by witchcraft or demonic forces. Widely available technology (like SMS messaging) could be used to connect biomedical, hospital-based providers, the patient, and family and religious carers across long distances for advice and coordination of care. Such a “carer network,” ideally trained in psychosocial supports for voice-hearers, could also relieve the burden on any one provider by creating a coordinated role for all three that is low cost, matches local resources, and is neither dependent on any one form of care – biomedical, religious, or relational – nor on any one person to provide “task-shifted” care (Kakuma et al., Reference Kakuma, Minas, van Ginneken, Dal Poz, Desiraju, Morris, Saxena and Scheffler2011; Healy et al., Reference Healy, Kaiser and Puffer2018; Galvin and Byansi, Reference Galvin and Byansi2020). Using this social approach, a “low-resource” setting may turn out to be one that is rich in resources after all.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10142.
Data availability statement
The authors have not made the data publicly available; please contact the corresponding author for more information.
Acknowledgements
Neely Myers would like to acknowledge Lydiah Achieng and Eunice Ezekiel for their research assistance in northern Tanzania. Emmanuel Bujululu was critical for securing permissions related to the research on the ground and mobilizing research support at the Arusha Mental Health Trust. In addition, Timothy Andrews and Moses Pulei made critical introductions while Pamoja Ministries offered logistical support.
Author contribution
The first author designed the project, collected the data, designed the data analysis, helped with coding, supervised data analysis and interpretation, and wrote most of the Introduction, Methods, Discussion and Conclusion and edited the Results section and tables. The second author assisted with data analysis and interpretation, conducted literature searches, created a research poster on this topic for an international conference, and co-authored the tables, Abstract, Impact Statement, Introduction, Results and Discussion with the first author. The third author assisted with data analysis and interpretation, co-authored the tables and Results sections. All authors approved the final manuscript.
Financial support
Thanks to The George Washington University Elliott School of International Affairs SOAR Award for initial seed funding, the Southern Methodist University’s University Research Council for follow-on funding for data collection, and the Sam Taylor Foundation for translation-related funding that made the full project possible.
Competing interests
The authors have no conflicts of interest to report.
Ethics statement
This research was approved by the Southern Methodist University IRB, the Tanzanian Commission on Science and Technology (COSTECH), the Regional Medical Officer, and the District Medical Officer to meet local requirements.


 Open access
Open access
Comments
No accompanying comment.