

Key messages
Chapter 3.3 examines informal payments. Informal payments are unsanctioned, unregulated payments made out-of-pocket (OOP) by patients directly to their health care provider for services that are covered by third-party purchasers. They are not recorded in routine administrative databases but can be captured in surveys, although they are usually underreported. Key learning includes that:
Informal payments reduce access to health care and financial protection. They can undermine population health and reduce trust in providers and governments in the long run.
Informal payments often stem from unmet desire for safe, timely or high-quality care and imply a mismatch between supply, demand and pricing in the formal health care payment system. When formal system payments are felt to be inadequate, informal payments may also be used to express gratitude to providers.
Settings with low physician density, and/or where the share of gross domestic product (GDP) spent on health care is low, tend to have higher levels of informal payments.
Informal payments are also associated with settings with high reliance on formal OOP payments (user charges).
Reducing or ending informal payments is difficult and requires a combination of specific, targeted measures and broad health systems reforms that address underlying causes.
The policy measures that may reduce informal payments include:
Introduction
Payments made directly by patients or users of the health system to their health care provider are known as OOP payments and comprise three types. Two are formal: (i) direct payments for services or goods that fall outside the remit of the official third-party payer such as government-funded health coverage programmes, private health insurance, or social health insurance (SHI); and (ii) cost-sharing, which refers to the contractual requirement by these third-party payers for individuals to pay a portion of the cost of goods and services that the third parties cover (Rechel, Maresso & van Ginneken, Reference Rechel, Maresso and van Ginneken2019). The third type of OOP payment is informal and outside the system – and it is these payments that form the focus of this chapter.
There is a lack of clarity about both the overall incidence of informal payments worldwide and the reasons for them. Informal payments are often not recorded in any accounting systems and may be illegal, depending on the type of exchange. These features make it difficult to measure their prevalence and frequency within a country, let alone make comparisons between countries. Also, informal payments can vary widely across key dimensions, such as: who initiates the payment (patient, provider); who pays (patients, families); who are the recipients (often physicians, but also other health care providers or administrative staff, or even hospitals or other health care organizations); what form they take (cash, in-kind medical supplies or equipment, or in-kind, unrelated to health care); and when they are made (before, during and/or after accessing health care) (Gaal et al., 2006). Additionally, whereas cost-sharing may be introduced into a health system to either raise revenue or to reduce/redirect health system utilization, the motivations or purposes of informal payments vary within and between countries. On the one hand, informal payments may be a form of gift-giving or expression of gratitude that is unrelated to the receipt of care or its quality. On the other hand, informal payments are commonly used to facilitate access or to secure higher quality health care.
The chapter presents our exploration of the phenomenon of informal payments as follows. We look briefly at how they are defined in the literature, the descriptions given of their motivation, and the detrimental effects they have on health system performance. We then discuss both the theoretical drivers of informal payments and empirical evidence that helps explain why they emerge. The next section then provides estimates of the global prevalence of informal payments before we zoom in on the Greek health system in a case study outlining their use there. The chapter concludes with suggestions of mechanisms to reduce/end informal payments and thus improve health system performance.
Informal payments in the literature: definitions and motivation
Three definitions of informal payments
A comprehensive review of the literature in 2013 identified 61 studies that defined informal payments in health care, and suggested that there were three distinct and original definitions (Cherecheş et al., Reference Cherecheş2013). The first was proposed by Lewis (Reference Lewis1999) who defined informal payments as:
payments to individual and institutional providers in-kind or cash that are outside the official payment channels, or are purchases that are meant to be covered by the health care system.
The second definition was introduced by Belli, Gotsadze and Shahriari (Reference Belli, Gotsadze and Shahriari2004) who explicitly positioned informal payments within the broader category of OOP payments. Specifically, they noted that informal payments are:
all payments that patients report to pay directly to their health care individual or institutional provider above the legally set co-payments for basic benefits package (BBP) services and above (or below) the regulated fee-for-service (FFS) fees for non-BBP services, plus all in-kind contributions and gifts. Thus, we consider informal payments as a subset of the OPPs (OOP payments). According to this definition, it is not really important whether or not transactions between patients and providers are registered for tax purposes, but whether such payments are or aren’t different from the legally set co-payments or regulated fees. We assume that all transactions where the patient reports he/she was not given any information about official co-payment rates or fees are to be considered as informal.
Finally, a now widely used definition of informal payments was developed by Gaal and colleagues (Reference Gaal2006) which captures the full spectrum of informal payments globally and underscores the importance of entitlements as the defining feature of informal payments that distinguishes them from other payments in the health sector. Thus, according to this definition, an informal payment is:
a direct contribution, which is made in addition to any contribution determined by the terms of entitlement, in cash or in-kind, by patients or others acting on their behalf, to health care providers for services that the patients are entitled to.
Therefore, in order to define and measure informal payments in the health sector, we need to understand the services that individuals are entitled to within the publicly funded, statutory health programmes.
Motivation: donation, FFS, tax avoidance
The question of motivation for the payment is an important consideration because, at one end of the spectrum, gift-giving that is common cultural practice may be a nuisance for some but may not in fact represent a policy problem in a jurisdiction. However, at the other end of the spectrum, an informal payment that is motivated by pressure on patients may have adverse impacts on intermediate and final health system objectives including efficiency, quality, equity in access, equity in finance, financial protection and health outcomes (see Box 3.3.1). Gaal and colleagues (Reference Gaal2006) delineate the two dominant motivations of informal payments as donation and FFS. The former is a “benign informal payment”, often called a “gratitude payment” because it is given voluntarily, is considered a form of appreciation, and is not given with the intention of directly impacting the services being provided. The latter is an “under-the-table” payment motivated by either an individual’s desire to receive safe, timely or good quality care, or to ensure or facilitate access to care, thereby potentially impacting health outcomes. Due to the lack of transparency, an under-the-table payment also limits the health system’s ability to protect individuals financially (e.g. by means of exemption mechanisms) and to ensure funds are reinvested into health systems in a way that is aligned with health system goals (Gaal et al., Reference Gaal2006).
1. Informal payments distort the allocation of resources for health care. In the presence of informal payments, resource allocation decisions do not incorporate elements related to clinical value and patient benefit, efficiency and cost–effectiveness. Instead, such decisions are largely based on market forces rather than evidence-based planning and public policy goals (Lewis, Reference Lewis and Mossialos2002). Resource allocation is thus driven by patients’ willingness to pay and providers’ coercion factors, with payments being independent of the value of care they provide or medical needs; the government has no role in setting these payments or prioritizing decisions and expenditure.
2. Informal payments impose substantial barriers to accessing health care and therefore undermine equity in access. Low-income patients might delay or forgo treatment or seek less specialized care due to limited affordability (Belli, Gotsadze & Shahriari, Reference Belli, Gotsadze and Shahriari2004; Habibov & Cheung, Reference Habibov and Cheung2017). This also has significant implications for patient outcomes and population health.
3. Informal payments undermine equity in financial protection. Given that informal payments are regressive, individuals often need to cut down expenses for other goods or services to finance their health care or even face the risk of financial catastrophe and poverty.
4. Informal payments tend to worsen quality of care, with patients often following suboptimal models of care due to lack of affordability or doctors recommending clinical processes driven by income generation rather than maximization of therapeutic value (Mæstad & Mwisongo, Reference Mæstad and Mwisongo2011; Vian et al., Reference Vian2006).
5. Informal payments lead to lower patient satisfaction with health services and undermine transparency, accountability, and trust in the health system and health workers (Kabia et al., Reference Kabia2021; Stepurko, Pavlova & Groot, Reference Stepurko, Pavlova and Groot2016).
Beyond these two major categories of motivation for informal payments – donation and FFS – there is a third which falls in between: a form of patient–doctor collusion with the primary aim of tax avoidance. All three of these exchanges have negative impacts on the health system, notwithstanding the benign intentions of straightforward gift-giving. For example, all can lead to reduced levels of trust in the doctor–patient relationship which may in turn lead to underutilization of health services. If patients anticipate additional fees for care that they are entitled to, they might be disincentivized to seek physician services. Also, there may be spillover effects on other parts of the health system (Currie, Lin & Meng, Reference Currie, Lin and Meng2013), such as incentivizing physicians to provide more care, including potentially unnecessary care, to patients who pay informally.
There is limited, and often contradictory, evidence to support one motivation or the other (Gaal et al., Reference Gaal2006). A systematic review of 31 studies (globally) found the same number of studies that reported the purpose of an informal payment as an expression of gratitude (10 studies) as those that reported the purpose as consistent with the FFS or fee-for-commodity hypothesis (10 studies) (Stepurko et al., Reference Stepurko2010). Others reported that the reasons for informal payments were to gain: better quality of care (10 studies); access to care (four studies); faster access (six studies); and psychological comfort (four studies). That same review found that nine studies reported the patients as initiating the payment (as an expression of thanks) and a further nine studies found the providers initiated it (as a required payment for service). Empirical literature on the motivation behind informal payments is sparse, and we look first at the theoretical drivers of informal payments.
Theoretical drivers of informal payments
The presence of rigidity in prices generates a mismatch between supply and demand for health care and can result in a lack of market equilibrium. Such an argument would suggest a need to increase the payments to providers (e.g. salaries, or formal OOP payments). Apart from the classical economic argument, health policy literature provides additional insights towards a better understanding of the drivers of informal payments, considering the motivation at individual level (cognitive behaviour theory), as well as from the broader institutional perspective (institutional theory).
Cognitive behaviour theory
Gaal and McKee (Reference Gaal and McKee2004) developed a theoretical framework drawing on cognitive behaviour theory to explains the causes of informal payments. They posit that informal payments are a “reaction by dissatisfied patients and physicians to shortage – a manifestation of deteriorating organization/system performance”. They extend Hirschman’s (Reference Hirschman1970) theory of “exit, voice and loyalty” as reactions to failures in organizations or states, by adding a new option/reaction which they call “inxit” (or a “informal/internal exit”) whereby dissatisfied patients and providers do not leave the system (exit), nor express their disappointment by complaining to bring about change in the system (voice), but rather they “seek to change its activities, not through open complaints, but using informal methods, such as payment or connections”.
The Gaal and McKee (Reference Gaal and McKee2004) cognitive behavioural model helps to explain why informal payments may arise under economic conditions of shortage. Specifically, when there is no option to leave the system (exit), as in Semashko systems with no private options, and there are no mechanisms for complaints to be heard (voice), then “inxit” as manifested by informal payments is the only possible reaction by patients to deteriorating health system performance. Thus, the policy solutions to address informal payments must simultaneously address the problem of shortage (e.g. by increasing investment in the system and health worker salaries) and expanding the formal options available to patients and providers to express their concerns with poor quality care; for example, through performance measurement and (enhanced) complaints procedures, or possibly with additional options to exit the public system (though this may exacerbate inequities).
Institutional theory
Additional explanations of the drivers of informal payments draw on institutional theory, considering both formal institutional shortcomings as well as informal institutions such as unwritten conventions and practices. Some of these institutional shortcomings include corruption in political systems and public programmes, lack of trust in government, and lack of government oversight over public programmes (Allin, Davaki & Mossialos, Reference Allin, Davaki and Mossialos2006; Pourtaleb et al., Reference Pourtaleb2020). Moreover, informal payments are expected to arise when “norms, practices and values of the informal institutions are not in symmetry with the formal rules of the game (i.e. laws and regulations)” (Williams & Horodnic, Reference Horodnic and Polese2017).
Recently, Binyaruka and colleagues (Reference Binyaruka2021) developed a supply-side theoretical framework which conceptualizes informal payments by placing the notion of concentrated power (which is similar to the issues arising from information asymmetry that affords more power to physicians than to both payers and patients) as a means to extract rent from various institutions and relationships. In Binyaruka et al.’s (Reference Binyaruka2021) model, individuals who have more power are more likely to obtain informal payments. Moreover, these individuals are more likely to bypass any transparency and anticorruption mechanisms because they have the power to game the system without consequences (Binyaruka et al., Reference Binyaruka2021). Thus, informal payments can arise in contexts where there is inadequate oversight in place to prevent abuse, suggesting a need for anticorruption measures and supervision along with awareness campaigns to address information asymmetry. The level of informal payments in a jurisdiction will relate to the health system and broader institutional context, including the extent of resource shortages and trust in government to address aspects of deteriorating health system performance, as well as the level of power held by medical professionals and health organizations.
Empirical evidence on the drivers of informal payments
A wide range of factors emerge in the empirical literature to help to explain the emergence and persistence of informal payments. Drawing in part on the theories above, these factors can be grouped into four broad categories: (i) economic; (ii) sociocultural; (iii) those related to governance and institutions; and (iv) those related to the health system. Existing evidence mainly reveals associations, and the findings should not be therefore interpreted as causal relationships.
Economic factors
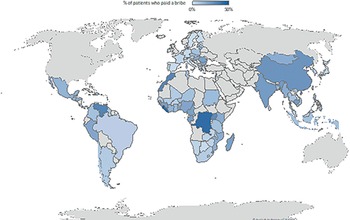
Economic factors broadly concern shortages, or a scarcity of resources in the publicly financed health system. Shortages – or a mismatch between the health care needs and expectations of the population and the supply and accessibility of care – are seen to be a necessary but not sufficient condition for informal payments to arise (Gaal & McKee, Reference Gaal and McKee2004). Data from Transparency International’s Global Corruption Barometer (Fig. 3.3.1) show that informal payments are present mostly in LMICs and that there is a correlation between health spending as a share of national income and prevalence of informal payments. (This correlation is also depicted in Fig. 3.3.4.)
Several studies have demonstrated the link between economic conditions and informal payments. For example, Tambor and colleagues (Reference Tambor2013) grouped 35 European countries into three categories drawing on a Health Consumer Powerhouse survey: no informal payments reported; some incidence of informal payments reported; and widespread informal payments reported. They found that countries with widespread informal payments had significantly lower public health expenditure as a share of total health spending.Footnote 1 Also, a cross-sectional analysis of Eurobarometer data from 28 European countries found a higher likelihood of patients reporting having made an informal payment in health care for countries with lower levels of health expenditure, either as a percentage of GDP or per capita (Williams & Horodnic, Reference Williams and Horodnic2018).
Sociocultural factors
Sociocultural reasons generally refer to a nationally embedded culture of tipping or custom of expressing gratitude through payments or gifts. Though there is probably a role played by cultural norms in explaining the origin and persistence of informal payments in many countries, and this appears as a theme in recent systematic reviews (Pourtaleb et al., Reference Pourtaleb2020), such explanations are insufficient to explain the majority of informal payments. For instance, the inability to identify a clear beginning and end to many clinical encounters, such as with chronic diseases management and primary care, make it difficult to separate gifts as an expression of gratitude from gifts/payments with a different motivation (e.g. to gain higher quality care/better access) (Gaal, Jakab & Shishkin, Reference Gaal, Jakab, Shishkin, Kutzin, Cashin and Jakab2010). Also, the fact that informal payments often take the form of in-kind contributions to the health care intervention itself, such as medical supplies or medicines, suggests that informal payments may not be a simple expression of gratitude in these contexts.
Factors related to governance and institutions
Institutional asymmetry
Williams and Horodnic (Reference Williams and Horodnic2018) tested the theory of “institutional asymmetry” as a driver of informal payments with a multi-level regression analysis of Eurobarometer data from 35 countries. They developed an index of institutional asymmetry based on answers to survey questions about the acceptability of three behaviours: to give money, to give a gift or to do a favour in order to get something from a public administration or public service. The index aims to capture the extent to which individuals believe that they should follow the legal and regulatory rules in society, though arguably it also reflects the country’s social norms and cultures, and therefore overlaps with the sociocultural explanation. The regression models revealed a strong association between higher levels of institutional asymmetry and the likelihood of making an informal payment in health care, even after adjusting statistically for individual level characteristics (e.g. demographics, rurality, socioeconomic status) and country-level economic and health system factors. The authors suggest that this finding supports their institutional theory-based explanation of informal payments. They further tested this theory during the COVID-19 pandemic and found significant associations between the prevalence of informal payments and both public acceptance of corruption and perceptions of the transparency of governments in their responses to the pandemic (Horodnic et al., Reference Horodnic2021). Also, a study in China found that informal payments were associated with lower levels of trust as well as poor communication with physicians (Li, Li & Yip, Reference Li and Yip2022).
Quality of governance
Some empirical support for the link between quality of governance and the incidence of informal payments can also be found in multi-country studies. For example, Tambor and colleagues (Reference Tambor2013) found that countries where informal payments are widespread also had the lowest perceived level of government effectiveness (average of 0.3 on a scale of −2.5 weak to 2.5 strong compared to 1.2 in countries with some informal payments, and 1.6 in countries with no informal payments). Also, Williams and Horodnic (Reference Williams and Horodnic2018) used the European Quality of Government Index (which combines perceptions with experiences of public sector services) and found strong evidence that informal payments are higher among countries with a lower quality of government (in their study of 27 European countries).
Role and size of the private sector
A further strand of the literature discusses how the role and size of the private sector relates to the incidence and intensity of informal health payments. In some settings, physicians have the option to exit the public system and provide care in the private sector either on a full- or part-time basis, thus allowing them to potentially earn higher income. The private sector also allows patients who are able to pay to opt out of the publicly financed system. The empirical support for a link between informal payments and the size of the private sector is mixed. Most studies rely on crude measures of the size and role of the private sector such as OOP payments as a share of total health expenditures. For example, Incaltarau and colleagues (Reference Incaltarau2021) used several years of pooled survey data across 117 countries and found higher shares of private finance (OOP and domestic private health expenditure) were correlated with a lower prevalence of informal payments. Also, Liu, Bau and He (Reference Liu, Bao and He2020) analysed panel data using the China Health and Retirement Longitudinal Survey and found that an increase in private health insurance coverage in China was associated with a reduction in informal payments. However, studies have also reported a positive association between the level of OOP payments and informal payments; for example, in some eastern European countries (Tambor et al., Reference Tambor2013) (Fig. 3.3.2). Further evidence is needed to uncover the actual impact of private sector development (in terms of financing and delivery of care) on the incidence and intensity of informal health payments.
Health system-specific factors
There are also numerous other health system reasons that help explain informal payments. Some of these relate to the broader economic context but are specific to health care; for example, low expenditures on health care, shortages of both human resources and medical supplies, low salaries for workers (Allin, Davaki & Mossialos, Reference Allin, Davaki and Mossialos2006; Gaal, Jakab & Shishkin, Reference Gaal, Jakab, Shishkin, Kutzin, Cashin and Jakab2010). Other health system factors relate to system governance and stewardship; for example: the lack of transparency and accountability in the health system; and inadequate public information and awareness about the benefits packages and what individuals’ entitlements and rights are in the publicly funded health systems (Pourtaleb et al., Reference Pourtaleb2020). Inefficiency in resource allocation and care delivery also appear as common explanations in the literature on informal payments, including the maldistribution of health workers and an overemphasis on curative over preventive care (Pourtaleb et al., Reference Pourtaleb2020; Williams & Horodnic, Reference Horodnic and Polese2017). Shortcomings in access to and quality of care are also frequently cited contributors to informal payments (Pourtaleb et al., Reference Pourtaleb2020). In some contexts, informal payments are a reaction to the problem of shortages and insufficient supply of health care, seeking to augment providers’ incomes, which may allow care to be provided, in particular in periods of economic difficulty.
How pervasive are informal payments?
The measurement of how pervasive informal health payments are is more challenging than with other mechanisms of health financing. Given the lack of data and records for pricing, utilization rates and transactions, estimates on the prevalence of informal payments are generally derived from surveys of patients or the public, which often use different sampling techniques and survey methods (Lewis, Reference Lewis2000).
View from the literature
A systematic review of 38 studies (globally) reported the variation in prevalence of informal payments (the percentage of patient encounters that had any type of informal payment) ranged from 2% to 80%, with higher prevalence in the inpatient sector than the outpatient (Khodamoradi et al., Reference Khodamoradi2018). Another systematic review of 33 studies (globally) also found informal payments were more common in inpatient services, surgery/delivery services (Amiri et al., Reference Amiri2019). A scoping review of the Western Balkans included 24 studies and found the highest prevalence of informal payments in the region was in Albania (19–91%), compared to 7–70% in KosovoFootnote 2, 7–23% in Serbia, and 5–22% in Bosnia and Herzegovina (Buch Mejsner & Eklund Karlsson, Reference Buch Mejsner and Eklund Karlsson2017). Another systematic review and meta-analysis of 15 studies in Iran estimated that the prevalence of informal payments was approximately 35%, with the main reasons provided as appreciating the staff, and in response to requests made by hospital staff (Mirabedini et al., Reference Mirabedini2017).
Measuring informal payments using cross-sectional survey data
As there is (most often) a lack of recording of informal payments in any state accounting or information system, national and international surveys are the main source of data on informal payments. Nevertheless, due to the often illicit nature of the practice and subsequent underreporting, these surveys might also underestimate the true prevalence. Another challenge of measurement relates to the methods followed, as different studies may adopt different definitions and approaches that make international comparisons challenging and not easily interpretable (Cohen, Reference Cohen2012).
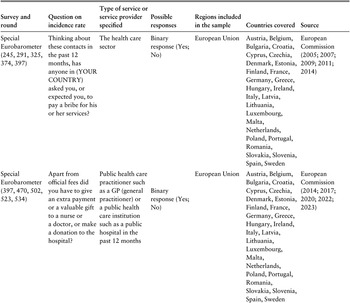
In response to this, we compiled a list of cross-sectional surveys that measure informal payments. The list in Table 3.3.1 describes how the question of experience concerning the practice has been approached by various organizations in different regional settings. Further, we draw on the Global Corruption Barometer by Transparency International in this section because it utilizes a uniform survey design to compare the prevalence of informal payments across regions. The surveys measure patients’ experience of paying physicians informally for care they are otherwise entitled to. This includes information on the public health sector in Latin America and the Caribbean, the Middle East and north Africa, Africa, Asia and the Pacific, and the EU. We used the most recent data available for each region, which meant that the time of collection varied across the global sample – EU (2021), Asia and the Pacific (2020), Latin America and the Caribbean (2019), Middle East and north Africa (2019), Africa (2019). Globally, 11% of patients made an informal payment in the 12 months prior to the survey. Fig. 3.3.1 illustrates the variation in prevalence of informal payments across regions.

Table 3.3.1a Long description
The table has 7 columns: Survey and round, Question on incidence rate, Type of service or service provider specified, Possible responses, Regions included in the sample, Countries covered, and Source. It reads as follows. Row 1: Special Eurobarometer (245, 291, 325, 374, 397). Question: Thinking about these contacts in the past 12 months, has anyone in (YOUR COUNTRY) asked you, or expected you, to pay a bribe for his or her services? Type of service: The health care sector. Possible responses: Binary response (Yes; No). Regions: European Union. Countries: Austria, Belgium, Bulgaria, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden Source: European Commission (2005; 2007; 2009; 2011; 2014).
Row 2: Special Eurobarometer (397, 470, 502, 523, 534). Question: Apart from official fees did you have to give an extra payment or a valuable gift to a nurse or a doctor, or make a donation to the hospital? Type of service: Public health care practitioner such as a G P (general practitioner) or a public health care institution such as a public hospital in the past 12 months. Possible responses: Binary response (Yes; No). Regions: European Union. Countries: Austria, Belgium, Bulgaria, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden. Source: European Commission (2014; 2017; 2020; 2022; 2023).

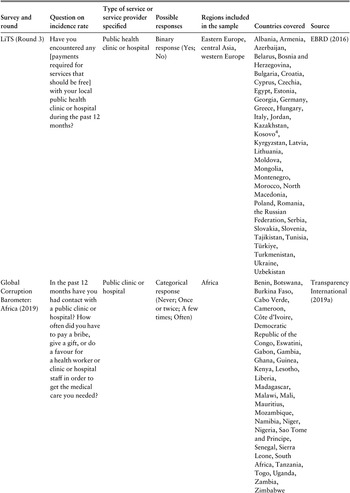
Table 3.3.1b Long description
The table has 7 columns: Survey and round, Question on incidence rate, Type of service or service provider specified, Possible responses, Regions included in the sample, Countries covered, and Source. It reads as follows. Row 3: Special Eurobarometer (470, 502, 523, 534). Question: Thinking about these contacts in the past 12 months has anyone in (YOUR COUNTRY) asked you or expected you to give a gift, favour or extra money for his or her services? Type of service: The health care sector. Possible responses: Binary response (Yes; No). Regions: European Union. Countries: Austria, Belgium, Bulgaria, Croatia, Cyprus, Czechia, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden. Source: European Commission (2017; 2020; 2022; 2023).
Row 4: Afrobarometer (Rounds 5, 6, 7, 8). Question: And how often, if ever, did you have to pay a bribe, give a gift, or do a favour for a health worker or clinic or hospital staff in order to get the medical care you needed? Type of service: Public clinic or hospital. Possible responses: Categorical response (Never; Once or twice; A few times; Often). Regions: Africa. Countries: Algeria, Benin, Botswana, Burkina Faso, Burundi, Cameroon, Cape Verde, Côte d’Ivoire, Egypt, Ethiopia, Gabon, Ghana, Guinea, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritius, Morocco, Mozambique, Namibia, Niger, Nigeria, Sao Tome and Principe, Senegal, Sierra Leone, South Africa, South Sudan, Sudan, Swaziland, Tanzania, Togo, Tunisia, Uganda, Zambia, Zimbabwe. Source: Afrobarometer (2015; 2016; 2019; 2022).

Table 3.3.1c Long description
The table has 7 columns: Survey and round, Question on incidence rate, Type of service or service provider specified, Possible responses, Regions included in the sample, Countries covered, and Source. It reads as follows. Row 5: L I T S (Round 1). Question: In your opinion, how often is it necessary for people like you to have to make unofficial payments or gifts in these situations? Type of service: Receive medical treatment in the public health system? Possible responses: 5-item Likert scale (Never; Always). Regions: Eastern Europe, central Asia. Countries: Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Czechia, Estonia, Georgia, Hungary, Kazakhstan, Kyrgyzstan, Latvia, Lithuania, Moldova, Mongolia, Montenegro, North Macedonia, Poland, Romania, the Russian Federation, Serbia, Slovak Republic, Slovenia, Tajikistan, Türkiye, Turkmenistan, Ukraine, Uzbekistan. Source: E B R D (2006).
Row 6: L I T S (Round 2 and 3). Question: Did you or any member of your household make an unofficial payment or gift when using these services over the past 12 months? Type of service: Medical treatment in the public health system. Possible responses: Binary response (Yes; No). Regions: Eastern Europe, central Asia. Countries: Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czechia, Egypt, Estonia, Georgia, Greece, Hungary, Jordan, Kazakhstan, Kosovo3, Kyrgyzstan, Latvia, Lithuania, Moldova, Mongolia, Montenegro, Morocco, North Macedonia, Poland, Romania, the Russian Federation, Serbia, Slovakia, Slovenia, Tajikistan, Tunisia, Türkiye Turkmenistan, Ukraine, Uzbekistan. Source: E B R D (2011; 2016).

Table 3.3.1d Long description
The table has 7 columns: Survey and round, Question on incidence rate, Type of service or service provider specified, Possible responses, Regions included in the sample, Countries covered, and Source. It reads as follows. Row 7: L I T S (Round 3). Question: Have you encountered any [payments required for services that should be free] with your local public health clinic or hospital during the past 12 months? Type of service: Public health clinic or hospital. Possible responses: Binary response (Yes; No) Regions: Eastern Europe, central Asia, western Europe. Countries: Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czechia, Egypt, Estonia, Georgia, Germany, Greece, Hungary, Italy, Jordan, Kazakhstan, Kosovo4, Kyrgyzstan, Latvia, Lithuania, Moldova, Mongolia, Montenegro, Morocco, North Macedonia, Poland, Romania, the Russian Federation, Serbia, Slovakia, Slovenia, Tajikistan, Tunisia, Türkiye, Turkmenistan, Ukraine, Uzbekistan. Source: E B R D (2016).
Row 8: Global Corruption Barometer: Africa (2019). Question: In the past 12 months have you had contact with a public clinic or hospital? How often did you have to pay a bribe, give a gift, or do a favour for a health worker, clinic or hospital staff in order to get the medical care you needed? Type of service: Public clinic or hospital. Possible responses: Categorical response (Never; Once or twice; A few times; Often). Regions: Africa. Countries: Benin, Botswana, Burkina Faso, Cabo Verde, Cameroon, Côte d’Ivoire, Democratic Republic of the Congo, Eswatini, Gabon, Gambia, Ghana, Guinea, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritius, Mozambique, Namibia, Niger, Nigeria, Sao Tome and Principe, Senegal, Sierra Leone, South Africa, Tanzania, Togo, Uganda, Zambia, Zimbabwe. Source: Transparency International (2019a).

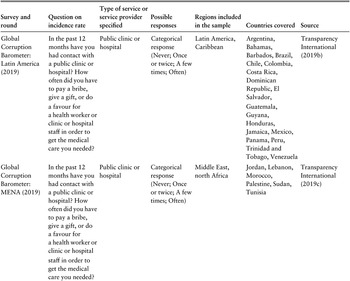
Table 3.3.1e Long description
The table has 7 columns: Survey and round, Question on incidence rate, Type of service or service provider specified, Possible responses, Regions included in the sample, Countries covered, and Source. It reads as follows. Row 9: Global Corruption Barometer: Latin America (2019). Type of service: In the past 12 months have you had contact with a public clinic or hospital? How often did you have to pay a bribe, give a gift, or do a favour for a health worker or clinic or hospital staff in order to get the medical care you needed? Type of service: Public clinic or hospital. Possible responses: Categorical response (Never; Once or twice; A few times; Often). Regions: Latin America, Caribbean. Countries: Argentina, Bahamas, Barbados, Brazil, Chile, Colombia, Costa Rica, Dominican Republic, El Salvador, Guatemala, Guyana, Honduras, Jamaica, Mexico, Panama, Peru, Trinidad and Tobago, Venezuela. Source: Transparency International (2019b).
Row 10: Global Corruption Barometer: MENA (2019). Question: In the past 12 months have you had contact with a public clinic or hospital? How often did you have to pay a bribe, give a gift, or do a favour for a health worker or clinic or hospital staff in order to get the medical care you needed? Type of service: Public clinic or hospital. Possible responses: Categorical response (Never; Once or twice; A few times; Often). Regions: Middle East, north Africa. Countries: Jordan, Lebanon, Morocco, Palestine, Sudan, Tunisia. Source: Transparency International (2019c).
Row 11: Global Corruption Barometer: MENA (2019). Question: In the past 12 months have you used wasta in order to get the medical care you needed? Type of service: Public clinic or hospital. Possible responses: Categorical response (Never; Once or twice; A few times; Often). Regions: Middle East, north Africa. Countries: Jordan, Lebanon, Palestine. Source: Transparency International (2019c).

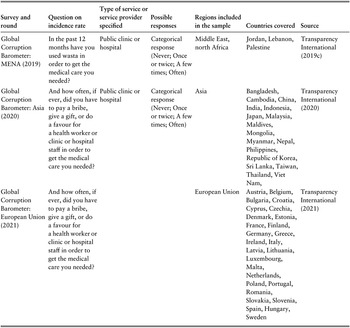
Table 3.3.1f Long description
The table has 7 columns: Survey and round, Question on incidence rate, Type of service or service provider specified, Possible responses, Regions included in the sample, Countries covered, and Source. It reads as follows. Row 12: Global Corruption Barometer: Asia (2020). Question: And how often, if ever, did you have to pay a bribe, give a gift, or do a favour for a health worker or clinic or hospital staff in order to get the medical care you needed? Type of service: Public clinic or hospital. Possible responses: Categorical response (Never; Once or twice; A few times; Often). Regions: Asia. Countries: Bangladesh, Cambodia, China, India, Indonesia, Japan, Malaysia, Maldives, Mongolia, Myanmar, Nepal, Philippines, Republic of Korea, Sri Lanka, Taiwan, Thailand, Vietnam. Source: Transparency International (2020).
Row 13: Global Corruption Barometer: European Union (2021). Question: And how often, if ever, did you have to pay a bribe, give a gift, or do a favour for a health worker or clinic or hospital staff in order to get the medical care you needed? Regions: European Union. Countries: Austria, Belgium, Bulgaria, Croatia, Cyprus, Czechia, Denmark, Estonia, France, Finland, Germany, Greece, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Hungary, Sweden. Source: Transparency International (2021).
Note: The datasets listed in the table above are all publicly available and were screened to identify the relevant questions.
Prevalence of informal payments in selected countries, 2019–2021

There is significant variation between regions globally. In the EU 6.9% of patients paid informally, compared to 10.9% in Latin America and the Caribbean, 11.6% in the Asia–Pacific region, 14.2% in sub-Saharan Africa and 16.6% in the Middle East and north Africa.
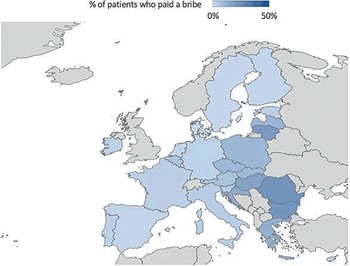
Importantly, informal payments also vary within regions. Fig. 3.3.2 illustrates the share of patients in the EU who paid in 2019. While the EU scores the lowest on this indicator across the globe, in parts of eastern Europe over 22% of patients have had to pay informally when using the publicly financed health care system (Table 3.3.2).
Prevalence of informal payments in the EU, 2021

| Country | Prevalence (%) |
|---|---|
| Romania | 22 |
| Bulgaria | 21 |
| Lithuania | 19 |
| Europe average | 7 |
| Luxembourg, Netherlands, Finland, Denmark | 1 |
| Sweden | 0 |
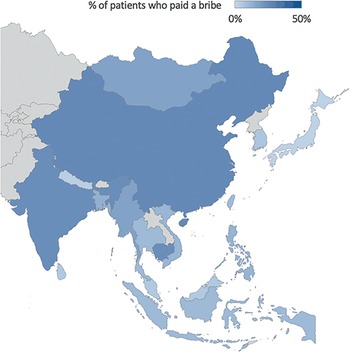
A similar trend is observed in other geographical contexts. For example, Fig. 3.3.3 shows that in the Asia–Pacific region, the prevalence varies between 1% of patients in the Maldives to 26% in China (Table 3.3.3).
Prevalence of informal payments in the Asia–Pacific region, 2020

| Country | Prevalence (%) |
|---|---|
| China | 26 |
| India, Cambodia | 24 |
| Asia–Pacific average | 11 |
| Nepal | 3 |
| Japan | 2 |
| Maldives | 1 |
Cross-sectional survey data: associations between informal payments and levels of health finance, OOP payments and physician density
Below, we explore the association between the share of patients who have made an informal health payment and health financing levels, OOP payments and physician density. These reflect the financial sustainability and resourcefulness of the health care institutions and allow us to compare settings which have different types of health system organization. Public spending on health care affects scarcity of resources in the system, potentially leading to increased competition between patients for access to treatments. On the supply side, low expenditures are associated with low physician pay which could increase the demand for informal payments as a subsidy.
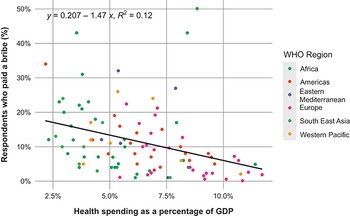
Fig. 3.3.4 visualizes a modest negative association between GDP spending on health and informal payments across the world. As countries spend a larger share of their GDP on health care, the prevalence of informal payments goes down. The relationships differ by region, with countries in the Latin America and Caribbean region and Europe displaying more statistically and economically negative associations when compared with other regions.
Share of GDP spent on health care versus percentage of patients who paid informally in the past 12 months, 2019–2021
Note: A simple linear regression between the share of GDP spent on health care and percentage of patients offering informal payments shows a negative relationship (y = −1.47x + 0.207) with an R-squared value of 0.12, suggesting minimal association between these two variables.

Figure 3.3.4 Long description
The y-axis represents Respondents who paid a bribe in percentage, from 0 to 50, while the x-axis represents Health spending as a percentage of G D P, from 2.5 percent to 10.0 percent. The plots are categorised into W H O regions: Africa, Americas, Eastern Mediterranean Europe, South East Asia, and Western Pacific. The best-fit line runs from about (2.0, 18) to (12, 3). The equation for the line is given as y equals 0.207 minus 1.47 times x, where R-squared equals 0.12.
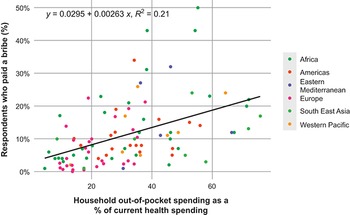
Next, we consider the relationship between formal OOP payments and informal payments. Unfortunately, it is not possible to distinguish between the two types of formal OOP payments – direct payments for costs incurred outside of the publicly financed or other third-party insurance coverage programme, and cost-sharing, or user charges to cover part of the costs of care within the public or private insurance coverage programme. There may be theoretical arguments for a negative association, for example if private options allow health care providers to supplement their income in formal, legitimate ways, and allow patients to express their dissatisfaction with the publicly financed health system by opting out and paying privately. However, Fig. 3.3.5, which illustrates this relationship between the two payment types on a global level, shows an overall positive association between the two: higher levels of OOP payments are associated with a higher prevalence of informal payments.
OOP payments as share of total health spending versus percentage of patients who have paid informally in the past 12 months, 2019–2021
Note: A simple linear regression between household OOP spending and percentage of patients offering informal payments shows a positive relationship (y = 0.00263x + 0.0295) with an R-squared value of 0.21, suggesting modest positive association between these two variables.

Figure 3.3.5 Long description
The y-axis represents Respondents who paid a bribe in percentage, from 0 to 50, while the x-axis represents Household out-of-pocket spending as a percentage of current health spending, from 0 to 60. The plots are categorised into W H O regions: Africa, Americas, Eastern Mediterranean Europe, South East Asia, and Western Pacific. The best-fit line runs from about (4, 5) to (75, 22). The equation for the line is given as y equals 0.0295 plus 0.00263 times x, where R-squared equals 0.21.
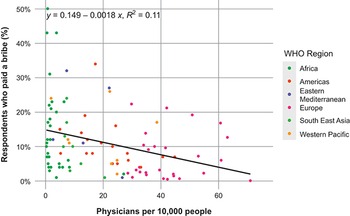
Absolute health system constraints or resource shortages may also contribute to informal payments. A commonly used measure of the extent of resource shortages in a health system is the density of physicians per 1000 people. Our measure here includes both primary and specialized physicians. The fitted regression line in Fig. 3.3.6 illustrates the negative association between physician density and prevalence of informal payments. In accordance with theories of market supply and demand, patients in systems with better availability of physicians would on average be less likely to experience informal payments. Where physician density is high, shortages of doctor appointments/visits are less likely, and so informal payments are not needed to bridge the gap between the current market price and equilibrium price. Greece, which we discuss in more detail in our case study, is one of the outliers. Although physician density in the country is relatively high at around 5.5 doctors per 1000 people, the corresponding prevalence of informal payments is around 13%.
Physician density versus percentage of patients who have paid informally in the past 12 months, 2014–2021
Note: A simple linear regression between physician density care and percentage of patients offering informal payments shows a negative relationship (y = −0.00182x + 0.15) with an R-squared value of 0.11, suggesting minimal association between these two variables.

Figure 3.3.6 Long description
The y-axis represents Respondents who paid a bribe in percentage, from 0 to 50, while the x-axis represents Physicians per 10,000 people, from 0 to 60. The plots are categorised into W H O regions: Africa, Americas, Eastern Mediterranean Europe, South East Asia, and Western Pacific. The best-fit line runs from about (0, 15) to (70, 2). The equation for the line is given as y equals 0.149 minus 0.0018 times x, where R-squared equals 0.11.
Prevalence of informal payments: summary
The global prevalence of informal payments is characterized by wide variation, notably in terms of both within-region and across-region variation. In addition, we explored three health systems indicators that have been shown to be significantly associated with informal payments: level of spend on health care, level of OOP payments and physician supply – and we provide some support for these associations on a global scale. Importantly, there are major data gaps in the comparable data on both the prevalence and frequency of informal payments but also the institutional and health system factors that may contribute to these payments. The continued use of comparable national surveys and reporting by organizations such as Transparency International is vital to support scholarly research and routine monitoring and tracking of the trends in informal payments over time.
A case study of informal payments in Greece
Financing arrangements in the Greek health system: a brief overview
Health financing in Greece is mixed, funded by both public and private expenditure. Public funding accounts for almost 60% of total health expenditure and consists of resources from taxation and social insurance, with each of them having almost equal contribution. Formal OOP payments make up more than a third of total health expenditure, a much higher share than the EU average of 22% (OECD & EU, 2020). In terms of funding, the Greek health system is historically considered as one of the most privatized among EU countries, with OOP payments being the main source of private funding and a major health financing mechanism (Abel-Smith et al., Reference Abel-Smith1994; Kyriopoulos, Nikolosi & Mossialos, Reference Kyriopoulos, Nikoloski and Mossialos2019; Mossialos, Allin & Davaki, Reference Mossialos, Allin and Davaki2005). At the same time, private health insurance is underdeveloped due to several economic, social, cultural and market-related aspects (Davaki & Mossialos, Reference Davaki and Mossialos2005; Economou, Reference Economou, Sagan and Thomson2016). Greece’s funding mix can be mainly attributed to the chronic weaknesses of the public sector, such as long waiting lists, low levels of satisfaction and responsiveness, weak primary care and undersupply of some types of services (Kanavos & Souliotis, Reference Kanavos, Souliotis and Meghir2017; Mossialos, Allin & Davaki, Reference Mossialos, Allin and Davaki2005).
The scale of informal payments in Greece
A significant proportion of household health expenditure arises from informal payments, which are traditionally regarded as one the main idiosyncrasies and policy challenges in Greece’s health financing system. Informal transactions are generally widespread in both hospital and outpatient care and across public and private services (Economou et al., Reference Economou2017). Using data from 2012 and some extrapolation assumptions, Souliotis and colleagues (Reference Souliotis2016) estimated that informal health payments amount to €1.5 billion, accounting for 28% of household health expenditure in Greece. Findings for inpatient services demonstrate that informal payments accounted for 20% of household payments for inpatient care in 2005 (Siskou et al., Reference Siskou2008), while a more recent survey revealed that the respective figure was 13% (Grigorakis et al., Reference Grigorakis2016).
Evidence from survey data reveals that informal payments were incurred in almost one third of admissions to public hospitals and in 36% of visits to private practitioners (Souliotis et al., Reference Souliotis2016). In addition, they were made in 13.5% of visits to private hospitals and 19% of appointments to private diagnostic centres. These findings are generally in line with those of an earlier study, which showed that 36% of patients admitted to public hospitals reported informal payments. In addition, patients who underwent a surgical procedure were more than twice as likely to incur informal payments (Liaropoulos et al., Reference Liaropoulos2008). Another study, of a sample of women who received obstetric care in public hospitals, revealed that more than seven out of 10 women faced informal payments (Kaitelidou et al., Reference Kaitelidou2013). Using data from a convenience sample, a more recent study showed that informal transactions were undertaken in 63% of health care incidents, the rate being greater for the utilization of oncology and surgical and emergency care (Giannouchos et al., Reference Giannouchos2020). Informal payments were reported in more than 43% of a sample of 217 admissions to private hospitals for surgical care (Grigorakis et al., Reference Grigorakis2016). Evidence from patients who visited contracted physicians also reveals that 47% of them made informal payments to get prescriptions (Kyriklidis et al., Reference Kyriklidis2016).
Explaining informal payments in Greece
Informal payments have traditionally served as a complement to inadequate public funding and can be largely attributed to the fragmented and patchy design of health coverage (Mossialos & Allin, Reference Mossialos and Allin2005) and the inefficient pricing and doctor reimbursement systems, while also reflecting the lack of effective control mechanisms (Economou et al., Reference Economou2017).
In a recent qualitative report, key informants identified both direct and indirect motives for the incidence of informal payments in Greece (WHO Regional Office for Europe, 2018). Doctors’ demand for additional payment, better access to high-quality care, provider choice, fear of getting inadequate care and adherence to the common practice were considered as the key reasons for the extensive informal transactions within the Greek health system. However, earlier studies report mixed findings. A strand of the evidence shows that patients tend to incur informal payments in order to skip the long waiting lists in Greek health system and facilitate access to care (Economou & Giorno, Reference Economou2009). This is also confirmed by quantitative evidence. According to survey data, more than 70% of patients who incurred informal payments did so to facilitate access and reduce waiting times. The corresponding figure was greater among respondents who visited public hospitals, private practitioners and private diagnostic centres, exceeding 80% (Souliotis et al., Reference Souliotis2016). The findings on the importance of access to health care as the key explanation for the incidence of informal payments contradict earlier evidence, which reveal that fear of receiving suboptimal care was the most common reason for paying informally in Greek public hospitals (Liaropoulos et al., Reference Liaropoulos2008). Almost nine out of 10 Greek patients who incurred under-the-table payments in public services did so following a doctor’s request, rather than offering them as a gratuity (Souliotis et al., Reference Souliotis2016). This is consistent with some earlier findings, showing that the primary reason for making such payments was doctor demands, with a smaller share of patients offering them as an expression of gratitude to health providers (Davaki & Mossialos, Reference Davaki and Mossialos2005; Kaitelidou et al., Reference Kaitelidou2013; Liaropoulos et al., Reference Liaropoulos2008).
Impact of informal payments on the Greek health system
Informal payments have detrimental effects on Greece’s health system performance, with their prevalence partly explaining the high rates of dissatisfaction with the public health services (Kyriopoulos & Mossialos, Reference Kyriopoulos, Mossialos and Immergut2021). Their high frequency does not merely reflect luxury preferences or cultural idiosyncrasies. Rather, informal transactions are an established practice and widespread behaviour, with a large share of doctors demanding such payments to facilitate access to care (Souliotis et al., Reference Souliotis2016). This practice directly compromises access to care, with those who cannot afford such payments facing additional barriers reflected in different quality of care or longer waiting lists (Mossialos, Allin & Davaki, Reference Mossialos, Allin and Davaki2005).
There is conflicting evidence on the link between financial status and the probability of informal payments in Greece. A strand of the literature has shown that socioeconomic characteristics are not associated with the incidence and intensity of informal payments (Horodnic et al., Reference Horodnic and Polese2017; Liaropoulos et al., Reference Liaropoulos2008), whereas a more recent study found that the better-off tend to make larger informal payments (Giannouchos et al., Reference Giannouchos2020). This discrepancy is potentially explained by the decreasing capacity to pay during the Greek economic crisis, especially among poorer households. But even if the worse-off pay less than their richer counterparts, their payments correspond to a higher share of their household income (Economou & Giorno, Reference Economou2009). In this context, informal payments further exacerbate the regressivity of an already regressive funding mix, disproportionately burden poorer households and compromise equity in financing and financial protection (Economou et al., Reference Economou2017; Kyriopoulos, Nikolosi & Mossialos, Reference Kyriopoulos, Nikoloski and Mossialos2021). For example, recent qualitative findings shows that Greek households may even cover their informal expenses for health care through credit (WHO Regional Office for Europe, 2018). Evidence from self-reported data demonstrates that informal payments had a large impact on living standards for 56% of people with poor financial status and for almost a third of their better-off counterparts (Souliotis et al., Reference Souliotis2016).
Patient pathways are currently guided by an informal referral process, given the lack of a well-functioning referral system and explicit official clinical guidelines. This system is largely driven and reinforced by informal payments, exacerbating inefficiency as a result of provider incentives for supplier-induced demand and suboptimal use of existing resources (WHO Regional Office for Europe, 2018).
Policy responses to informal payments
In Greece, there have been efforts to address the persistence of informal payments and minimize their adverse impacts. There have been multiple measures proposed for short-term implementation and impact: (i) focusing on the legal prohibition along with active enforcement of preventive regulations; (ii) increasing doctors’ salaries; (iii) providing information to raise awareness and increase transparency; (iv) introducing channels of voice and public opinion; and (v) formalizing informal payments. Apart from the short-term measures, there are several long-term policies for reducing fragmentation, inefficiencies and structural weaknesses in financing and delivery of care, which can help reduce the incidence and intensity of informal payments (Kyriopoulos & Mossialos, Reference Kyriopoulos, Mossialos and Immergut2021). For example, a list of such measures includes changes in provider payment and pay for performance schemes, reduced fragmentation of pooling, reform of primary care and the referral system, better care coordination, and expansion of the benefits package. To date these have had limited effects, due in part to the external environment: the financial crisis of 2008 and subsequent austerity measures, and the global COVID-19 pandemic have further challenged efforts to reform and strengthen the health system in Greece and to make a dent in informal payments. In addition, there are endemic and deep-rooted vested interests that often block the required reforms (Mossialos, Allin & Davaki, Reference Mossialos, Allin and Davaki2005; Kyriopoulos & Mossialos, Reference Kyriopoulos, Mossialos and Immergut2021). Some of the doctors’ associations are powerful interest groups with strong incentives to maintain the status quo, which allows them to secure higher income and autonomy. In addition, although politicians rhetorically emphasize the importance of addressing informal payments, they have not yet devised a comprehensive strategy for doing so. The reason for this possibly relates to the additional fiscal space needed for increasing public spending for health care and the political commitment required for the introduction of comprehensive auditing mechanisms.
Policy relevance and conclusions
Globally, informal payments play a role in financing health care in a diverse set of jurisdictions; they arise in the context of resource constraints, institutional deficiencies such as government corruption, and have multiple impacts on health and health systems. Within the literature on informal payments, there is strong evidence concerning the impacts on access to care and financial protection, as well as potentially on trust in providers and governments. Poorer patients may be forced to make significant sacrifices (e.g. borrowing money, selling produce, valuables or livestock), to pay for essential health services (Allin, Davaki & Mossialos, Reference Allin, Davaki and Mossialos2006). For example, studies have found both that vulnerable groups paid more often than other groups (Buch Mejsner & Eklund Karlsson, Reference Buch Mejsner and Eklund Karlsson2017) and that informal payments were more common for rich/wealthy individuals (Amiri et al., Reference Amiri2019).
The policy responses to reduce the prevalence of informal payments in a country will invariably depend on the national context, including the economic, social and political systems within which the health system is situated. Broadly the policy solutions will need to address the economic, institutional and health system factors that have been found to drive informal payments in the first place. Some theoretical drivers of informal payments may lend support to increasing private payments to both: (i) supplement provider salaries; and (ii) provide patients with an option to exit the public system and pay privately. However, the potential for new revenues and possible declines in informal payments need to be balanced against risks to equitable access and financial protection that come with increasing OOP payments. Where possible, collective or public financing could be used to increase wages, address workforce shortages and to reduce the need for informal payments. To address the lack of viable options for patients to express disappointment or concerns with quality of care in the publicly funded systems, potential policy responses include the establishment of formal options to address grievances, such as with a patient ombudsman, or patient complaints processes, while ensuring these are monitored and result in action. The institutional challenges such as government corruption, lack of oversight of the health system, informational asymmetry, and lack of trust among the population suggest a need to increase transparency and public communications about decision-making, including about the benefits package in the public system, and broader anticorruption measures could all help to address informal payments.
Overall, the policy actions should be informed by an understanding of the specific drivers of informal payments in a particular country, which may relate to some but not all of the factors described above. Moreover, since the existence of informal payments may not be the policy problem itself but rather a symptom or manifestation of broader health system and institutional challenges, the policy solutions may not directly target informal payments per se (e.g. tightening enforcement mechanisms) but they may require much broader health system reforms. Policy options that target the problem of informal payments include: formalizing informal payments to ensure that exemptions can be introduced to protect vulnerable populations and that revenues can be invested in health system improvement; and clarifying the definition of and communication about a benefits package that is reasonable given the economic context of the country. The broader system-level policy options that address broader challenges that are driving informal payments include: increasing spending on health systems; supporting better monitoring and enforcement of the rules and any penalties for informal payments; and maintaining and expanding the scope, breadth and depth of insurance coverage.
On a final note, we leveraged internationally comparable data from the Global Corruption Barometer in this chapter to describe the prevalence of informal payments and the association with a selection of institutional factors. Our analysis highlights that informal payments are reported in most world regions and there is considerable within-region variability, which relate in part to health system expenditures, the role of OOP payments, and physician supply. Though analyses such as these have a number of limitations, Transparency International conducts these surveys with representative samples. Due to data limitations, we were only able to focus on systemic factors rather than the relationship between individual level characteristics and likelihood of paying informally. Furthermore, due to potential underreporting of informal payments by patients, we can presume that our results are conservative estimates of the actual prevalence. As with other illicit or stigmatized behaviours, respondents might be unlikely to share their true experiences. This issue could be mitigated through a more diverse set of methodologies. In addition to standard surveys, which are the primary method of data collection on the topic, the academic and policy literature would benefit from alternative approaches to information elicitation.
Reducing informal payments in health systems requires targeted responses specific to informal payments, as well as broader health systems reforms to address their underlying drivers. Importantly, the policy solutions proposed to address the specific problem of informal payments have the potential to not only reduce the prevalence of informal payments but also to yield positive impacts on health system performance and health outcomes. The COVID-19 pandemic has further underscored the need to prioritize health workers and their adequate remuneration, and to ensure equitable access to essential services. However, the economic and health shocks of the pandemic, combined with high levels of distrust in governments in many jurisdictions, constitute a major obstacle both to prioritizing informal payments as a policy problem and implementing the needed health system reforms to address them.Footnote 5



 Open access
Open access