


Introduction
What is chemsex?
Sexualised drug use (SDU) involves the use of a wide range of psychoactive substances during sexual activities (Hibbert et al., Reference Hibbert, Hillis, Brett, Porcellato and Hope2021). Within this umbrella definition, chemsex is a distinct form of SDU, particularly common among men who have sex with men (MSM) (Bourne et al., Reference Bourne, Reid, Hickson, Torres-Rueda, Steinberg and Weatherburn2015; Stuart, Reference Stuart2019). This typically refers to gay and bisexual MSM (GBMSM), but may also include heterosexual MSM, a subpopulation who are less likely to access support services (Persson et al., Reference Persson, Newman, Manolas, Holt, Callander, Gordon and De Wit2019; Scheadler et al., Reference Scheadler, Rao, Shuper, Beer, Curtis, McInroy and Eaton2026). Definitions of chemsex can vary across the literature (Amundsen et al., Reference Amundsen, Muller, Reierth, Skogen and Berg2024), for example, also including trans women and non-binary people (European Chemsex Forum, 2018).
Chemsex typically involves the intentional use of specific drugs, or ‘chems’, before or during sexual encounters. Chems in the UK usually include crystal methamphetamine, gamma-hydroxybutyric acid/gamma-butyrolactone (GHB/GBL), synthetic cathinones such as mephedrone and 3-MMC, and, to a lesser degree, cocaine and ketamine (Bourne et al., Reference Bourne, Reid, Hickson, Torres Rueda and Weatherburn2014; McCall et al., Reference McCall, Adams, Mason and Willis2015). Other drugs that are not classically considered chems, but can facilitate chemsex, include alcohol, MDMA, cannabis, PDE-5 inhibitors such as sildenafil and tadalafil, and amyl nitrates (poppers). Table 1 provides an overview of chems. Although each drug carries a possible risk of adverse effects, combining drugs can lead to greater harm. For example, using sedative substances, like GHB/GBL, alongside other central nervous system depressants, such as alcohol or benzodiazepines, can increase the likelihood of life-threatening interaction effects (Schep et al., Reference Schep, Knudsen, Slaughter, Vale and Mégarbane2012).
Overview of typical drugs used within chemsex (Schifano et al., Reference Schifano, Bonaccorso, Arillotta, Guirguis, Corkery, Floresta, Papanti Pelletier, Scherbaum and Schifano2025)

Table 1. Long description
The table provides an overview of typical drugs used within chemsex, detailing their types, common names, administration methods, desired effects, and associated risks. The table includes three main drugs: GHB/GBL, synthetic cathinones, and methamphetamine. GHB/GBL is a sedative depressant with common names like G, Gina, and liquid ecstasy, administered orally or intravenously, and has desired effects such as euphoria, relaxation, and sexual arousal, but carries risks like overdose and withdrawal symptoms. Synthetic cathinones, such as mephedrone and 3-MMC, are stimulants and empathogens with common names like Meph and meow, administered through snorting, oral intake, smoking, intravenous injection, or rectal booty bump, and have desired effects like alertness, euphoria, increased energy, and sexual arousal, with risks including nausea, vomiting, headaches, hallucinations, vertigo, anxiety, and paranoia. Methamphetamine is a stimulant with common names like crystal meth, crystal, tina, glass, and ice, administered through snorting, smoking, intravenous injection, or rectal booty bump, and has desired effects such as exhilaration, sexual enhancement, sexual arousal, alertness, and disinhibition, with risks like paranoia, psychosis, cardiovascular toxicity, stroke, and aggression and agitation.
Chemsex is often characterised by sex with multiple concurrent or sequential partners, and is frequently organised via smartphone-based geolocation sexual networking apps for MSM, such as Grindr (Bourne et al., Reference Bourne, Reid, Hickson, Torres Rueda and Weatherburn2014). Chemsex may occur in a variety of settings, including private homes, cruising areas, gay saunas, clubs, and sex-on-premises venues (Santoro et al., Reference Santoro, Rodríguez, Morales, Morano and Morán2020).
The estimated prevalence of chemsex varies across continents and settings (Maxwell et al., Reference Maxwell, Shahmanesh and Gafos2019). Two large systematic reviews and meta-analyses from Europe and Asia reported a pooled prevalence of chemsex among MSM populations as 16% and 19%, respectively (Coronado-Muñoz et al., Reference Coronado-Muñoz, García-Cabrera, Quintero-Flórez, Román and Vilches-Arenas2024; Wang et al., Reference Wang, Jonas and Guadamuz2023), with a 2025 global meta-analysis reporting 22% (Georgiadis et al., Reference Georgiadis, Katsimpris, Vatmanidou, VASSILAKOU, Beloukas and Sergentanis2025). Prevalence may also be higher in large cities (Rosas Cancio-Suárez et al., Reference Rosas Cancio-Suárez, Ron, Díaz-Álvarez, Martínez-Sanz, Serrano-Villar, Moreno and Sánchez-Conde2023; Whitlock et al., Reference Whitlock, Protopapas, Bernardino, Imaz, Curran, Stingone, Shivasankar, Edwards, Herbert and Thomas2021), where there is also a greater prevalence of ‘slamming’ – injecting drug use in the chemsex context.
Motivations for chemsex participation
Reasons for chemsex participation are multi-faceted, encompassing sexual, social, and psychological motivators. Understanding these is key to working with chemsex participants in clinical practice.
For many, there is a belief or expectation that using chems will positively influence sexual activity (Maxwell et al., Reference Maxwell, Shahmanesh and Gafos2019). Chemsex participants may wish to increase sexual desire or libido, or enhance the quality of sex (e.g. increasing arousal, sexual intensity, or the experience of intimacy) (Weatherburn et al., Reference Weatherburn, Hickson, Reid, Torres-Rueda and Bourne2017). Using chems may also be associated with sexual disinhibition and increased sexual confidence (Hickson, Reference Hickson2018). This can allow participants to pursue or experience sex that would be more challenging when sober. This might include specific sexual acts (e.g. rough sex, anal fisting), or simply sex free of shame (Bourne et al., Reference Bourne, Reid, Hickson, Torres-Rueda, Steinberg and Weatherburn2015; Deimel et al., Reference Deimel, Stöver, Hößelbarth, Dichtl, Graf and Gebhardt2016; Hickson, Reference Hickson2018; Milhet et al., Reference Milhet, Shah, Madesclaire and Gaissad2019; Nimbi et al., Reference Nimbi, Rosati, Esposito, Stuart, Simonelli and Tambelli2021).
The specific drugs used during chemsex can enhance sexual sensation and pleasure (Bourne et al., Reference Bourne, Reid, Hickson, Torres Rueda and Weatherburn2014; Lafortune et al., Reference Lafortune, Blais, Miller, Dion, Lalonde and Dargis2021; Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025; Platteau et al., Reference Platteau, Schrooten, Herrijgers, den Daas, Ventura, Strong and de Wit2025). For people with a penis, they may subjectively improve erectile function and reduce the typical post-ejaculation refractory period, allowing longer and more intense sexual sessions (Schifano et al., Reference Schifano, Bonaccorso, Arillotta, Guirguis, Corkery, Floresta, Papanti Pelletier, Scherbaum and Schifano2025). Physical sexual performance may also be enhanced, with chemsex participants reporting increased stamina, energy, and libido, and reduced feelings of discomfort, pain, or exhaustion (Lafortune et al., Reference Lafortune, Blais, Miller, Dion, Lalonde and Dargis2021; Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025; Weatherburn et al., Reference Weatherburn, Hickson, Reid, Torres-Rueda and Bourne2017). However, some chemsex participants also report experiencing sexual problems, such as unreliable erections, inability to orgasm, or pain with anal sex (Bourne et al., Reference Bourne, Reid, Hickson, Torres Rueda and Weatherburn2014; Hirshfield et al., Reference Hirshfield, Chiasson, Wagmiller, Remien, Humberstone, Scheinmann and Grov2010; Pessina et al., Reference Pessina, Pavanello Decaro, Torri and Prunas2025), which can cause distress or sexual performance anxiety. This can drive further drug use, in an attempt to manage the sexual problem (Gertzen et al., Reference Gertzen, Karcher, Schwarz, Rosenberger, Strasburger, Rabenstein, Strasser, Palm and Rüther2024; Weatherburn et al., Reference Weatherburn, Hickson, Reid, Torres-Rueda and Bourne2017). Sometimes, continued use can lead to challenges with experiencing emotional intimacy and participating in sober sex (Kunelaki, Reference Kunelaki2019; Sánchez-Ocaña et al., Reference Sánchez-Ocaña, Fenollar-Cortés, Fernández-Artamendi and Esteban2025).
Social factors also motivate chemsex participation. Chemsex may be normalised within particular GBMSM social networks (Lafortune et al., Reference Lafortune, Blais, Miller, Dion, Lalonde and Dargis2021; Maxwell et al., Reference Maxwell, Shahmanesh and Gafos2019), and introduction to chemsex usually occurs through friends and sexual partners (Lafortune et al., Reference Lafortune, Blais, Miller, Dion, Lalonde and Dargis2021; Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025). Chemsex may be linked to positive LGBTQ+ identity formation, emerging in response to sexuality- or gender-related minority stress (Hakim, Reference Hakim2019; Jaspal, Reference Jaspal2022; López-Barrientos, Reference López-Barrientos2025). Participating in chemsex can also facilitate a sense of community belonging and connection (Hakim, Reference Hakim2019), known buffers of minority stress (Jaspal, Reference Jaspal2022; Meyer, Reference Meyer2003; Power et al., Reference Power, Mikołajczak, Bourne, Brown, Leonard, Lyons, Dowsett and Lucke2018; Stanton et al., Reference Stanton, Wirtz, Perlson and Batchelder2022). This is particularly important as LGBTQ+ people face significant discrimination, which can reinforce drug use as a coping strategy (Abrahão et al., Reference Abrahão, Kortas, Blaas, Koch Gimenes, Leopoldo, Malbergier, Torales, Ventriglio and Castaldelli-Maia2022; Connolly et al., Reference Connolly, Dewan and Holland2025b; Hillyard, Reference Hillyard2024). Chemsex can accelerate and enhance a sense of emotional closeness and intimacy between people, especially in the context of casual sex, where this might typically be harder to achieve (Weatherburn et al., Reference Weatherburn, Hickson, Reid, Torres-Rueda and Bourne2017). Chemsex can therefore help people overcome the perceived emotional barriers to forming connections, and reduce fears of social or sexual rejection (Lafortune et al., Reference Lafortune, Blais, Miller, Dion, Lalonde and Dargis2021; Pollard et al., Reference Pollard, Nadarzynski and Llewellyn2018). This may be particularly important to people living with HIV, who are more likely to participate in chemsex (Maxwell et al., Reference Maxwell, Shahmanesh and Gafos2019), although additional research is needed to understand the complex web of causality around HIV status and chemsex.
For some, engagement in chemsex is a means to ‘escape’ from psychological distress or difficulty, including loneliness, low mood, or anxiety (Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025). This can include worries about perceived attractiveness or sexual desirability, and experiencing negative judgements of their appearance while using apps. In people who report a negative impact of chemsex, one study found higher rates of internalised shame and negative appraisals of queer identity. Factors such as difficulty in ‘coming out’ were associated with increased chemsex engagement (Gertzen et al., Reference Gertzen, Karcher, Schwarz, Rosenberger, Strasburger, Rabenstein, Strasser, Palm and Rüther2024). Finally, chemsex may also help people cope with wider stressors such as racism, poverty, or the loss of physical LGBTQ+ spaces (Hakim, Reference Hakim2019; Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025).
Implications of chemsex
Although chemsex potentially confers considerable risks to participants, the actual experience of harm is non-uniformly distributed, with many participants reporting limited or no associated harm. Early public health approaches to chemsex sought to report chemsex harms, such as HIV transmission (Stuart, Reference Stuart2013). However, a purely risk-focused approach can be counterproductive when identifying effective interventions for chemsex participants (Bryant et al., Reference Bryant, Hopwood, Dowsett, Aggleton, Holt, Lea, Drysdale and Treloar2018). As understandings of chemsex have evolved, research has broadened beyond risk to explore chemsex across cultural, political, technological, psychological, and social lenses (Drysdale et al., Reference Drysdale, Bryant, Hopwood, Dowsett, Holt, Lea, Aggleton and Treloar2020; Møller and Hakim, Reference Møller and Hakim2023). This approach recognises the historical impact of pathologising sexual and gender minorities, and emphasises the need for culturally sensitive and affirming approaches (Rolt and Margetts, Reference Rolt and Margetts2023). As with any ‘edgework’, a voluntary activity which presents danger and that can be mitigated with a specialist set of skills, chemsex participants often become expert at navigating potential risks (Hickson, Reference Hickson2018).
Mental health implications
People who engage in chemsex multiple times per month are more likely to report the need for psychological support, and experience negative consequences of chemsex (Evers et al., Reference Evers, Hoebe, Dukers-Muijrers, Kampman, Kuizenga-Wessel, Shilue, Bakker, Schamp, Van Buel, Van Der Meijden and Van Liere2020). Chemsex has also been associated with psychological distress in the short-term, e.g. a drug ‘comedown’ or temporary drug-induced psychotic symptoms, and long-term mental health disorders, such as anxiety, depression, and enduring psychosis (Íncera-Fernández et al., Reference Íncera-Fernández, Gámez-Guadix and Moreno-Guillén2021; Moreno-Gamez et al., Reference Moreno-Gamez, Hernandez-Huerta and Lahera2022; Tomkins et al., Reference Tomkins, George and Kliner2019). Some research has observed that participants who engage in chemsex have a heightened risk of experiencing psychotic symptoms compared with the general population (Moreno-Gamez et al., Reference Moreno-Gamez, Hernandez-Huerta and Lahera2022). These risks are further exacerbated by the route of drug administration, with slamming methamphetamine posing greater risk (Dolengevich-Segal et al., Reference Dolengevich-Segal, Gonzalez-Baeza, Valencia, Valencia-Ortega, Cabello, Tellez-Molina, Perez-Elias, Serrano, Perez-Latorre, Martin-Carbonero, Arponen, Sanz-Moreno, De la Fuente, Bisbal, Santos, Casado, Troya, Cervero-Jimenez, Nistal and Ryan2019; Íncera-Fernández et al., Reference Íncera-Fernández, Gámez-Guadix and Moreno-Guillén2021; Moreno-Gamez et al., Reference Moreno-Gamez, Hernandez-Huerta and Lahera2022).
Sexual health implications
The disinhibiting effects of chems may mean people struggle with consistently using condoms or chemoprophylaxis (e.g. HIV pre- or post-exposure prophylaxis and/or prophylactic doxycycline) (Viamonte et al., Reference Viamonte, Ghanooni, Reynolds, Grov and Carrico2022). For people living with HIV, chemsex can affect their ability to take HIV treatments consistently (Hegazi et al., Reference Hegazi, Lee, Whittaker, Green, Simms, Cutts, Nagington, Nathan and Pakianathan2017; Ottaway et al., Reference Ottaway, Finnerty, Amlani, Pinto-Sander, Szanyi and Richardson2016). Practices that may be associated with chemsex, such as anal fisting, injecting drugs, and ‘bareback’ (condomless) sex, may also increase the risk of sexually transmitted infections (STIs) or blood-borne virus (BBV) transmission.
Substance use implications
‘Comedown’ is a colloquial term for the short-term after-effects of drug use. This can occur over two to three days and reduce over one to two weeks (McKetin et al., Reference McKetin, Copeland, Norberg, Bruno, Hides and Khawar2014). Typically, a comedown is characterised by a combination of symptoms, which include physical and mental fatigue, low mood, anxiety, paranoia, irritability, nausea, and disrupted sleep (Parrott, Reference Parrott2015). People report individualised symptoms that are dependent on the drug consumed (Nimbi et al., Reference Nimbi, Rosati, Esposito, Stuart, Simonelli and Tambelli2021). During a comedown, drug use can resume or increase to offset the symptoms, which typically prolongs or intensifies the negative effects (Spencer et al., Reference Spencer, Addison, Alderson, McGovern, McGovern, Kaner and O’Donnell2021).
With any addictive drug, increasing use can potentially lead to psychological and/or physiological dependence (Li et al., Reference Li, Ku, Huang, Chen, Wei, Strong and Bourne2021; McCall et al., Reference McCall, Adams, Mason and Willis2015). Drug dependence is an adaptive state which drives continued use of drugs to maintain functioning or prevent withdrawal (George and Koob, Reference George and Koob2010). Psychological dependence refers to altered motivational processes because of the rewarding nature of drug use (Feltenstein et al., Reference Feltenstein, See and Fuchs2021; Koob and Le Moal, Reference Koob and Le Moal2008), whereas physiological dependence refers to biological adaptations in response to continued drug use (O’Brien, Reference O’Brien2011).
For individuals experiencing dependence, withdrawal may occur when they attempt to reduce or cease drug-taking (WHO, 2009). Symptoms of withdrawal will vary between drugs and individuals. However, common symptoms include cravings, excessive sweating, aches and pains, tremors, nausea, anxiety, agitation, mood lability, suicidality, fatigue, and insomnia or hypersomnia (Dolengevich-Segal et al., Reference Dolengevich-Segal, Gonzalez-Baeza, Valencia, Valencia-Ortega, Cabello, Tellez-Molina, Perez-Elias, Serrano, Perez-Latorre, Martin-Carbonero, Arponen, Sanz-Moreno, De la Fuente, Bisbal, Santos, Casado, Troya, Cervero-Jimenez, Nistal and Ryan2019; Winstock et al., Reference Winstock, Mitcheson, Ramsey, Davies, Puchnarewicz and Marsden2011). Particularly in the case of GHB/GBL dependence, which has a physiological withdrawal syndrome similar to that seen with alcohol, cessation may rapidly precipitate psychotic symptoms, delirium, and potentially fatal seizures (Ghio et al., Reference Ghio, Cervetti, Respino, Belvederi Murri and Amore2014; Karila et al., Reference Karila, Angerville, Benyamina and Billieux2024). Withdrawal symptoms typically reduce after re-dosing.
Continued use of chems can lead to tolerance – a reduced and desensitised response to the effect of drugs. This change arises from neuroadaptations and requires increased use to attain the same desired effects (Turton and Lingford-Hughes, Reference Turton and Lingford-Hughes2016). Frequent polydrug use is common in chemsex, leading to higher tolerance in a short period of time (Poulios et al., Reference Poulios, Apostolidou, Triantafyllidou, Krasidis, Petrou, Kakota, Papadopetrakis, Kyprianou, Yiasemi, Georgiou, Nikolopoulos and Minas2024). Similar to withdrawal, tolerance for chems varies between service users.
Victimisation in the chemsex context
Sexual assault, rape, and non-consensual sexual image/video distribution have been reported in the chemsex context (Connolly et al., Reference Connolly, Coduri-Fulford, Macdonald, Gilchrist and Muschialli2025a; Drückler et al., Reference Drückler, Speulman, van Rooijen and De Vries2021; Wilkerson et al., Reference Wilkerson, Di Paola, Nieto, Schick, Latini, Braun-Harvey, Zoschke and McCurdy2021). There is also concern that chemsex participation may be linked to other forms of criminal victimisation, such as robbery, blackmail, physical assault, and even murder (Carthy et al., Reference Carthy, Hillier, Tracy, Pakianathan, Morris, Shell and Forrester2021). Drug intoxication (especially if leading to unconsciousness or semi-consciousness) may affect the capacity to consent to sex, or increase the potential for other forms of victimisation. Intoxication may not always be intentional, and there is a small body of literature reporting on drug-facilitated sexual assault in the chemsex context (Connolly et al., Reference Connolly, Coduri-Fulford, Macdonald, Gilchrist and Muschialli2025a). However, it is important to note that cultures of harm reduction, mutual support, and care exist within many chemsex communities (Hakim, Reference Hakim2019; Møller and Hakim, Reference Møller and Hakim2023).
Barriers to care
Barriers to accessing support for chemsex participants may stem from a variety of factors, such as inadequate service provision, fear of stigma, or previous negative healthcare experiences (Priester et al., Reference Priester, Browne, Iachini, Clone, DeHart and Seay2016). Negative attitudes towards people who use alcohol or other drugs are common among healthcare professionals (Cazalis et al., Reference Cazalis, Lambert and Auriacombe2023; van Boekel et al., Reference van Boekel, Brouwers, van Weeghel and Garretsen2013). A recent audit found NHS Talking Therapies (NHS TT) clinicians often over-exclude service users based on drug use (Shahriyarmolki et al., Reference Shahriyarmolki, Hemingway and Strang2025). Some reasons for exclusion included beliefs that drugs could limit the effectiveness of treatment, that taking certain drugs contraindicates therapy, and that therapy could exacerbate drug use. People with co-occurring mental health and alcohol or other drug problems are often instructed first to seek specific addiction treatment, or to be completely abstinent before starting psychological therapy (Dugmore, Reference Dugmore2013). This position can be disempowering, particularly for service users who understand their alcohol or drug use as helpful for coping with mental health challenges (Lee, Reference Lee2020). In reality, mental health and problematic alcohol/drug use often have a complex, bi-directional web of causality (Chorlton and Smith, Reference Chorlton and Smith2016; Cleary and Thomas, Reference Cleary and Thomas2017), and for some, use in moderation is neither a coping mechanism nor a precipitant of mental health difficulties.
Lesbian, gay, bisexual, transgender, and other sex, sexuality and gender minoritised (LGBTQ+) communities face additional challenges accessing care, and experience greater health inequities (Connolly et al., Reference Connolly, Meads, Wurm, Brown, Bayliss, Oakes-Monger and Berner2025c; Priester et al., Reference Priester, Browne, Iachini, Clone, DeHart and Seay2016; Zeeman et al., Reference Zeeman, Sherriff, Browne, McGlynn, Mirandola, Gios, Davis, Sanchez-Lambert, Aujean, Pinto, Farinella, Donisi, Niedźwiedzka-Stadnik, Rosińska, Pierson, Amaddeo and Network2018). LGBTQ+ people are more likely to report mental health difficulties and lower overall wellbeing than cisgender (cis) and heterosexual counterparts (Plöderl and Tremblay, Reference Plöderl and Tremblay2015; Semlyen et al., Reference Semlyen, King, Varney and Hagger-Johnson2016; Watkinson et al., Reference Watkinson, Linfield, Tielemans, Francetic and Munford2024). They also tend to report more hazardous patterns of alcohol and drug use compared with cis heterosexual peers (Connolly et al., Reference Connolly, Davies, Lynskey, Maier, Ferris, Barratt, Winstock and Gilchrist2022; Connolly et al., Reference Connolly, Ezquerra-Romano, O’Callaghan, Bayliss, Thayne, Holloway and Davies2024; Hughto et al., Reference Hughto, Quinn, Dunbar, Rose, Shireman and Jasuja2021; Pitman et al., Reference Pitman, Marston, Lewis, Semlyen, McManus and King2022). When accessing mental health services, LGBTQ+ people often encounter discrimination and clinicians who lack an adequate level of cultural competence (Rees et al., Reference Rees, Crowe and Harris2021). This discrimination and marginalisation of LGBTQ+ people within healthcare has been attributed to wider societal transphobia and homophobia (Alencar Albuquerque et al., Reference Alencar Albuquerque, de Lima Garcia, da Silva Quirino, Alves, Belém, dos Santos Figueiredo, da Silva Paiva, do Nascimento, da Silva Maciel, Valenti, de Abreu and Adami2016). Such experiences hinder an effective therapeutic relationship, leading to service user fears of disclosure, and healthcare professionals neglecting clinically relevant discussions (Morris et al., Reference Morris, Fernandes and Rimes2022). A recent evaluation of NHS TT highlighted the need for additional support for clinicians to better meet the needs of LGBTQ+ service users (Ho et al., Reference Ho, O’Rouke, Laville, Chellingsworth and Callaghan2023).
Chemsex participants have also expressed confusion about where to find support, and uncertainty about whether services can adequately address their needs (Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025). Moreover, chemsex participants frequently feel judged in healthcare contexts regarding their sexuality or drug use, and may need to explain what chemsex involves to professionals. Positively, some chemsex participants find support from alternative community-based organisations or LGBTQ+ peers (Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025). However, this can also evoke a feeling of over-reliance on peers and variability in the level of support received (Nagington and King, Reference Nagington and King2022). Fundamentally, to reduce barriers, care for chemsex participants should be integrated, holistic, and non-judgemental (Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025; Nagington and King, Reference Nagington and King2022; Tangerli et al., Reference Tangerli, Godynyuk, Gatica-Bahamonde, Neicun, Van Kessel and Roman-Urrestarazu2022).
Role of Talking Therapies
NHS TT are available nationwide in the UK, providing evidence-based psychological interventions for common mental health problems (NHSE, 2018). Services utilise a stepped care model to ensure that service users receive an appropriate intensity of intervention. The NHS TT manual outlines the scope of practice for services (NHSE, 2018). Alongside common mental health problems, NHS TT can also provide support for people with long-term health conditions and alcohol or other drug use. Although NHS TT does not provide specific, structured addiction interventions, TT treatment can be delivered alongside ongoing support from specialist drug and alcohol services. NHS TT and specialist drug and alcohol services are encouraged to develop locally shared pathways. Furthermore, positive practice guidelines have been developed for working with people who use alcohol and other drugs (NHSE, 2018). Positive practice guidelines outline that alcohol or drug use should not be automatic exclusion criteria. However, TT services or clinicians may hold such beliefs, preventing access for service users (Shahriyarmolki et al., Reference Shahriyarmolki, Hemingway and Strang2025). NHSE (2018) positive practice guidelines state:
-
• NHS TT therapists can appropriately offer brief advice on alcohol or drug reduction.
-
• NHS TT services need to offer a flexible approach, providing the example of tolerating some non-attended sessions.
-
• Service users should attend sessions sober and avoid using when engaging in relevant behavioural experiments (e.g. anxiety-related) between sessions. If someone is unable to do this, a referral to a specialist drug and alcohol service is recommended.
-
• If a service user is unable to attend without being under the influence of alcohol or drugs, the best approach for care is to agree a plan with local drug and alcohol services. This may involve an active referral, concurrent with NHS TT intervention.
-
• Lack of knowledge of drugs and alcohol should not interfere with psychological intervention nor be a barrier to care. Therapists should approach service users with curiosity to foster collaboration within the therapeutic relationship.
Alongside positive practice guidelines, the Royal College of Psychiatrists (RCP, 2025) recently published a report on co-occurring substance use and mental health disorders (CoSUM). Appropriate treatment services are advised based on the severity levels of both mental health and drug use across mild, moderate, and severe presentations. Accessing appropriate support is contingent upon a person’s primary concern, such as decreasing drug use or improving mental health. If mental health is identified as their primary concern and presents as mild/moderate severity, irrespective of the severity of drug use, the individual should be eligible to access NHS TT. In the context of severe drug use problems, a person should also be accessing drug and alcohol services alongside NHS TT treatment. These recommendations emphasise joint working between services to coordinate and manage care for CoSUM (RCP, 2025).
With regard to chemsex, NHS TT services are well-positioned to provide psychological therapies, which are limited within specialist drug and alcohol or sexual health services. Although NHS TT are not designed to deliver specific addiction interventions, many people do not need professional interventions to change their drug use (Sobell et al., Reference Sobell, Ellingstad and Sobell2000), or may not want to access specialist addiction services (Campbell et al., Reference Campbell, Gurreri, Margetts, Mundy and Rutter2024; PHE, 2017). It is likely that many service users accessing support from TT engage in drug use (Foster et al., Reference Foster, Robertson, Pallis and Segal2022), whether or not this is initially disclosed. Those who disclose chemsex participation should not be disqualified from accessing these therapies (NHS, 2012).
This paper aims to educate NHS TT therapists about how to work clinically with chemsex participants. We outline relevant models of care, reasonable adjustments for clinical practice, and provide components of intervention that can be translated for use with service users who participate in chemsex. NHS TT therapists are competently trained and supervised to offer evidence-based interventions for this service user group.
Guiding principles for care
Working effectively with chemsex requires drawing on various principles of care from different fields. Relevant areas include: chemsex-specific frameworks, drug use, trauma-informed care, and psychosexual principles. This paper consolidates these principles, especially given the lack of national guidance around effectively treating chemsex-related problems.
Chemsex-specific frameworks
In late 2023, the British Psychological Society published guidance for developing chemsex intervention services within the UK (Campbell et al., Reference Campbell, Gurreri, Margetts, Mundy and Rutter2024). Although these are guidelines for services, they outline and recommend important principles to be adopted when working with chemsex participants:
-
• An integrated, multi-disciplinary approach. Chemsex is an emerging and complex presentation requiring joined-up care from various professionals. Multi-agency working across services and sectors is key to providing effective care for people experiencing chemsex-related issues.
-
• Cultural competence and humility. Therapists should seek knowledge and understanding of the various experiences of GBMSM. Sexuality and gender knowledge is essential, alongside reasons for drug use. Some chemsex participants, such as those who are sex working, will require additional specialist knowledge and external expertise should be sought.
-
• Awareness of barriers to engagement. Specialist services have limited psychological provision and most referrals for chemsex problems are made to generic mental health services. Therapists should be aware of possible obstacles to accessing support, such as a lack of cultural competence.
-
• A holistic, biopsychosocial understanding of motivations, maintenance factors, and outcomes of chemsex participation. There should be a parity of focus between substance use models and focus on sex, with psychosexual elements remaining jointly focused.
-
• Sex-positive, non-judgemental, and community-based interventions. These include harm reduction, proactive engagement, and psychosocial support.
These guidelines, alongside government recommendations (PHE, 2017), encourage therapists to support service users who participate in chemsex, wherever they present, with culturally sensitive and psychologically informed care (Campbell et al., Reference Campbell, Gurreri, Margetts, Mundy and Rutter2024).
Substance use approaches
Five core elements underpin effective addiction treatment (Moos, Reference Moos2007). This psychosocial approach emphasises a strong therapeutic alliance, organised sessions with specific goals, a focus on alternative rewards and activities to drug use, engagement with recovery-oriented social networks, and the development of coping skills and self-efficacy (OHID, 2023). Many of these factors are common to both addiction treatment and standard cognitive behavioural therapy.
Trauma-informed practice
People who experience adverse childhood experiences (ACEs), or traumatic experiences as adults, have a greater risk of drug use (Konkolÿ Thege et al., Reference Konkolÿ Thege, Horwood, Slater, Tan, Hodgins and Wild2017; Zhu et al., Reference Zhu, Racine, Devereux, Hodgins and Madigan2023). Furthermore, research has shown that LGBTQ+ populations are at an increased risk of being exposed to traumatic events in comparison with heterosexual and cisgender peers (Chandrasekar et al., Reference Chandrasekar, Karamanos, Learoyd and Khanolkar2024; Marchi et al., Reference Marchi, Arcolin, Fiore, Travascio, Uberti, Amaddeo, Converti, Fiorillo, Mirandola, Pinna, Ventriglio and Galeazzi2022; Pitman et al., Reference Pitman, Marston, Lewis, Semlyen, McManus and King2022). This is important as some people who participate in chemsex report using chems to cope with traumatic experiences, which can precipitate and perpetuate use (Tan et al., Reference Tan, Phua, Tan, Gan, Ho, Ong and See2021).
Trauma-informed practice (TIP) recognises the profound effect of trauma on the development of individuals, groups, and communities (OHID, 2022). By integrating awareness and knowledge of trauma in healthcare services, systems can prevent re-traumatisation, reduce barriers to accessing care, and increase retention in care (Bartholow and Huffman, Reference Bartholow and Huffman2021; Sweeney et al., Reference Sweeney, Filson, Kennedy, Collinson and Gillard2018). The foundations of TIP include six key principles: safety, trust, choice, collaboration, empowerment, and cultural competence (Harris and Fallot, Reference Harris and Fallot2001; Hopper et al., Reference Hopper, Bassuk and Olivet2010).
Grounded in a strengths-based framework, TIP reframes the complexities of drug use as a function of survival (Comiskey, Reference Comiskey and Comiskey2024). Here, drug use as a means of coping with trauma can be seen as a normal response to abnormal experiences. The attitudes and beliefs of the therapist, and the language they use, can either contribute to or help to reduce stigma towards people who use drugs (Gray, Reference Gray2010). For example, instead of using words such as ‘addict’, ‘clean’, ‘abuse’ or ‘misuse’, preferred terms might be: ‘person who uses drugs’, ‘abstinent of’, or simply ‘use’. The Scottish Drug Forum has created a helpful glossary (see https://www.drugsandalcohol.ie/33136/1/Moving-Beyond-People-First-Language.pdf).
Furthermore, the term chemsex is not universal. Therapists should be mindful of cultural differences when assessing for chemsex. See Table 2 for alternative terms used in place of chemsex.
Example terms for chemsex and associated region

Table 2. Long description
A table with two columns and six rows. The first column lists various terms associated with chemsex, including Chemsex, High and horny, Chillouts, Party and play, and Hi-fun Chemfun. The second column specifies the associated regions for each term, such as Europe and Asia for Chemsex, Europe, North and South America, and Asia for High and horny, Europe for Chillouts, North and South America and Australia for Party and play, and Southeast Asia for Hi-fun Chemfun. The table highlights the regional variations in terminology used for chemsex activities.
Sex-positive and psychosexual principles
A sex-positive approach means therapists demonstrate respect for sexual practices and sexual diversity. It considers sexual wellbeing and pleasure, rather than merely the absence of disease, dysfunction, or sexual violence (Mitchell et al., Reference Mitchell, Lewis, O’Sullivan and Fortenberry2021). It aims to reduce shame, embarrassment, and stigma when talking about sex and sexuality. It involves therapists reflecting on their own discomfort and conscious/unconscious biases about the topic and affirming the rights of each individual’s sexual expression. It does not mean that therapists should never encourage service users to reflect on their sexual choices, and how aligned they are with a person’s overall goals and values. Using frameworks such as the Six Principles of Sexual Health (consent, non-exploitation, honesty, shared values, prevention of STIs/BBVs, and pleasure) may help encourage such reflection (Braun-Harvey and Vigorito, Reference Braun-Harvey and Vigorito2015).
Psychosexual principles
Sexual problems are prevalent in GBMSM (Cheng, Reference Cheng2022) and may present as antecedents or consequences of chemsex (Nimbi et al., Reference Nimbi, Rosati, Esposito, Stuart, Simonelli and Tambelli2021). Definitions of ‘normal’ sexual practices or sexual ‘dysfunctions’ are highly historically and culturally variable (Peterson, Reference Peterson2017). For example, the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) only removed ‘homosexuality’ as a diagnosable ‘mental disorder’ in 1973 (Spitzer, Reference Spitzer1981). In general, a psychosexually informed approach treats positive sexual experiences as an important part of overall psychological health (including the active decision to not engage in sex or romantic relationships). For service users who do desire sex, who want to improve it, or are troubled by sexual problems, therapists may want to consider the following psychosexual principles: accurate and thorough psychoeducation about sexuality, gender, and sexual functioning; combatting sex-negative, shaming, or repressive cultural messages about sex; and paying attention to the complex, multi-faceted, intersectional, and often political dimensions of sex and sexual pleasure (Peterson, Reference Peterson2017). It is helpful to formulate sexual problems using a biopsychosocial approach, and they are often responsive to cognitive behavioural interventions (Metz et al., Reference Metz, Epstein and Mccarthy2017). In the absence of specialist training, therapists should explore onwards or concurrent referrals to psychosexual services.
Harm reduction
Harm reduction approaches are essential when working with people who use drugs, and are well-evidenced to reduce morbidity and mortality (Pridgen et al., Reference Pridgen, Bontemps, Lloyd, Wagner, Kay, Eaton and Cropsey2025). Harm reduction should be presented in the context of the person’s capacity to make decisions within their social reality (Muschialli et al., Reference Muschialli, Yang, Engstrom, Puljevic, Beltazar, Beltazar, Siddique, Ferris and Connolly2024; Race, Reference Race2008). Simply put, people who engage in chemsex are often experts in drug use, individual tolerance, and harm reduction practices. Therapists have an obligation to explore drug use in an open and non-judgemental manner, offering choice in what psychoeducation or therapeutic treatment a service user may wish to receive, and acknowledging that there may be times when service users are more informed about drug use than their therapists. The evidence-based communication style, motivational interviewing (MI; Rollnick and Miller, Reference Rollnick and Miller1995), can facilitate discussions of drug use and change.
Harm reduction does not constitute official medical advice. Instead, it provides information to educate both service users and professionals about ways to reduce risk. In Table 3, we provide an overview of harm reduction information for people who engage in chemsex.
Basic harm reduction information for chemsex participants; adapted from GMHC (https://menrus.co.uk/drugs/about-drugs/)

Table 3. Long description
The table provides harm reduction strategies for chemsex participants, focusing on various aspects such as sexual health, general wellbeing, general drug use, safer injecting, GHB/GBL, synthetic cathinones, and methamphetamine. It includes recommendations for routine testing for sexually transmitted infections, the use of doxycycline post-exposure prophylaxis, HIV pre-exposure prophylaxis, and promoting HIV post-exposure prophylaxis. For general wellbeing, it emphasizes the importance of hydration, nutrition, sleep hygiene, and mental health. In terms of general drug use, it advises starting low and going slow, planning for recovery aids, and avoiding drug mixing. For safer injecting, it highlights the importance of washing hands, safely disposing of equipment, using new and clean equipment, and never sharing or borrowing injecting equipment. Specific guidelines are provided for GHB/GBL, including the difference between GHB and GBL, the importance of accurate measurement, avoiding direct contact with skin, and managing G sleep. Additionally, it offers advice on synthetic cathinones and methamphetamine use, including the importance of good dental hygiene and the risks associated with these substances.
Most chemsex harm reduction strategies involve discussing health risks, distributing supplies such as sterile needles and syringes, and encouraging safer sex practices, such as the use of condoms (Del Pozo-Herce et al., Reference Del Pozo-Herce, Baca-García, Martínez-Sabater, Pérez-Elvira, Gea-Caballero, Chover-Sierra, Satústegui-Dordá, Tovar-Reinoso, Rodríguez-Velasco, Sánchez-Barba, Pérez and Juárez-Vela2024). The Gay Men’s Health Collective (GMHC) provides a variety of culturally tailored, collaboratively developed information concerning all aspects of GBMSM health and chemsex. The Safer 2 pack, which can be accessed online, was created by gay men with lived experience and serves as a guide to safer chemsex practices (GMHC, 2025). Furthermore, Release (https://www.release.org.uk/) provide service users with free, confidential information on drugs and the law. People who participate in chemsex can also access support from the LGBT+ switchboard and Galop, the national helpline for LGBTQ+ victims and survivors of abuse and violence.
Adapting sessions for chemsex participants
When working with any service user who takes drugs, reasonable adaptations should be made to enhance attendance and retention (NHS, 2012). Unsurprisingly, greater retention and adherence are associated with positive treatment outcomes (Dacosta-Sánchez et al., Reference Dacosta-Sánchez, González-Ponce, Fernández-Calderón, Sánchez-García and Lozano2022). Some evidence-based, low-burden strategies available to therapists include: a pre-treatment overview of the intervention structure, contracting, text message/email reminders, and presenting information in an accessible format (Alderson et al., Reference Alderson, Spencer, Scott, Kaner, Reeves, Robson and Ling2021; Rubenis et al., Reference Rubenis, Nation, Katz and Arunogiri2023).
Therapists can benefit from scheduling the first session soon after the initial contact, capitalising on the motivation for change that prompted it (Lefforge et al., Reference Lefforge, Donohue and Strada2007). Consistent scheduling can also help establish structure throughout the week. Taking into account the service user’s pattern of drug use can prevent potential discontinuation due to comedown, withdrawal, or drug-related barriers. For example, scheduling a session at 9 am on a Monday, following a weekend of drug use, may not be ideal.
Accommodating drug-related barriers, such as the need for frequent re-dosing of GHB/GBL in people who are dependent, can be supported using virtual appointments, shortening sessions, or allowing breaks for service users to leave the premises to re-dose. As chemsex is typically facilitated by smartphones (Platteau et al., Reference Platteau, Herrijgers and de Wit2020; Zou and Fan, Reference Zou and Fan2017), many service users will have access to online sessions. Therapists should also consider reducing the length of sessions to enhance engagement and concentration. Finally, greater flexibility in did-not-attend policies, such as expanding the three-miss rule, is also preferable (NHS, 2012).
Sober mind contracting
Clear guidelines need to be agreed early on in treatment regarding the use of drugs before, during and after therapy sessions. A ‘sober mind policy’ should be discussed with service users and negotiated early on in therapy, prioritising stabilisation support, including stabilisation of drugs. This may involve contracting an agreement not to use chems before and after sessions to improve effectiveness. While chemsex should not prevent access to intervention, the presence of physical dependence warrants clinical prioritisation. In such cases, addressing dependence concurrently increases safety and often, service users are willing to reduce use to improve symptoms, for example in PTSD (Ehlers and Wild, Reference Ehlers and Wild2022).
Assessment
The initial task of assessment is to establish a collaborative, non-stigmatising, anti-shaming therapeutic alliance. Alongside standard assessment practices, sensitive questioning related to chemsex can help to improve care for participants. It offers an opportunity for the therapist to share psychoeducation, harm reduction advice (such as in Table 3), onward referrals (e.g. to local sexual health or specialist addiction services), and signposting to other relevant support (e.g. mutual aid groups such as Narcotics Anonymous/Crystal Meth Anonymous or SMART Recovery). Table 4 provides suggestions of questions to ask during assessments, derived from the authors’ collective clinical practice. However, it is also important to avoid an ‘inappropriate curiosity’ about chemsex or aspects of LGBTQ+ identity, which is a common experience for LGBTQ+ people in healthcare in general (Dean et al., Reference Dean, Victor and Guidry-Grimes2016; McNeill et al., Reference McNeill, McAteer and Jepson2023; Vermeir et al., Reference Vermeir, Jackson and Marshall2018).
Possible questions to ask about chemsex during an assessment

Table 4. Long description
The table presents a structured list of possible questions to ask about chemsex during an assessment, divided into several sections: Opening, Chemsex, Drug use, Sexual behaviours, Risks, Psychotic experiences, Sexual health, Physical health, and Goals. Each section contains specific questions related to the topic. The Opening section includes questions about personal identity and drug use before, during, or after sex. The Chemsex section asks about participation, feelings, and frequency of chemsex sessions. The Drug use section inquires about triggers, negative consequences, and sharing equipment. The Sexual behaviours section covers types of sex and number of partners. The Risks section addresses medical attention, unwanted sex, and crossing sexual boundaries. The Psychotic experiences section asks about paranoia and unusual experiences. The Sexual health section includes questions about HIV status, condom use, and vaccinations. The Physical health section covers physical changes and other medications. The Goals section asks about barriers to stopping chemsex and connections with the LGBTQ+ community.
Validated questionnaires designed to assess chemsex or capture chemsex-related harm have recently been developed (Del Pozo-Herce et al., Reference Del Pozo-Herce, Baca-García, Martínez-Sabater, Pérez-Elvira, Gea-Caballero, Chover-Sierra, Satústegui-Dordá, Tovar-Reinoso, Rodríguez-Velasco, Sánchez-Barba, Pérez and Juárez-Vela2024; Miwa et al., Reference Miwa, Lin, Ku, Li, Huang, Hsu, Bourne and Strong2025). In addition, there are many online resources. For example, the Chemsex Care Plan from 56 Dean St sexual health clinic (https://www.dean.st/chemsex-care-plan/) could be used to supplement existing questionnaires used in NHS TT.
The assessment stage is also a key period to implement Making Every Contact Count (MECC; PHE, 2016). MECC is an initiative that promotes behaviour change through ultra-brief (30 seconds) or brief (under 3 minutes) advice. There is evidence for its efficacy in reducing smoking and alcohol intake, and improving diet and physical activity (Parchment et al., Reference Parchment, Lawrence, Perry, Rahman, Townsend, Wainwright and Wainwright2023). This initiative could also be used with chemsex participants (ask-advise-act).
For example:
-
• Ask: ‘Are you injecting chems?’
-
• Advise: ‘Did you know our local pharmacy offers a needle exchange program?’
-
• If interested, act and refer or offer information to access local support options.
-
• If not interested, ‘the choice is yours, you can always find more information online (e.g. https://gaymenshealthcollective.co.uk/) if you change your mind’.
When is intervention warranted?
The point at which intervention in chemsex becomes necessary is often unclear and ambiguous. Therefore, it is best to adopt an individualised, service user-led approach to decision-making, which prioritises autonomy (Friedrichs et al., Reference Friedrichs, Spies, Härter and Buchholz2016; Marchand et al., Reference Marchand, Beaumont, Westfall, MacDonald, Harrison, Marsh, Schechter and Oviedo-Joekes2019). Whilst there are individuals whose chemsex participation causes low or no harm, there are also individuals who do experience harms, but feel that these are balanced against the perceived benefits of chemsex (Hickson, Reference Hickson2018; Mundy et al., Reference Mundy, Carter, Nadarzynski, Whiteley, de Visser and Llewellyn2025; Weatherburn et al., Reference Weatherburn, Hickson, Reid, Torres-Rueda and Bourne2017). Still others may experience chemsex-related harm and few or no benefits, but choose to prioritise other concerns over addressing chemsex (Lunchenkov et al., Reference Lunchenkov, Cherchenko, Altynbekov, Terlikbayeva, Primbetova, Gryazev, German, Batyrgaliev and Steinert2024).
Clinically, chemsex could be viewed as a spectrum ranging from recreational to harmful use (Malandain and Thibaut, Reference Malandain and Thibaut2023). Malandain and Thibaut (Reference Malandain and Thibaut2023) suggest the threshold for intervention is reached once sexual or drug use behaviour becomes ‘out of control’. This concept includes personal suffering and negative impacts on quality of life or health, such as mental illness or recurrent STIs. Instead of assuming chemsex is pathological, service users should be asked whether they experience harm from chemsex, what they perceive to be their individual balance of risks and benefits, and whether they want to or are ready to change. Addressing subjectively ‘out of control’ chemsex behaviour may be part of goal-oriented outcome planning. Therapeutic objectives might include decreasing distress, enhancing functioning, and supporting harm reduction. Some service users may choose to continue chemsex during TT treatment, which should be met with a non-judgemental approach.
Currently, there is no diagnostic entity that describes ‘problematic’ or ‘harmful’ chemsex. The International Classification of Diseases–11th edition (ICD-11) includes two disorders – compulsive sexual behaviour disorder (6C72) and drug use disorders (6C40-6C4H) – which share features with chemsex, yet neither fully captures its clinical presentation. Śniadach et al. (Reference Śniadach, Orlof, Sołowiej-Chmiel, Kicman, Szymkowiak and Waszkiewicz2025) have proposed provisional diagnostic criteria to inform the potential inclusion of Chemsex Use Disorder in ICD-12, to improve recognition and treatment. While this may enable more effective interventions, labelling these behaviours as an ‘addiction’ risks over-pathologisation (Billieux et al., Reference Billieux, Schimmenti, Khazaal, Maurage and Heeren2015). Viewing chemsex through a diagnostic lens also overlooks the broader psychological, social, and cultural factors which motivate chemsex participation (Bourne et al., Reference Bourne, Reid, Hickson, Torres-Rueda, Steinberg and Weatherburn2015; Bourne et al., Reference Bourne, Reid, Hickson, Torres Rueda and Weatherburn2014; Hakim, Reference Hakim2019; Weatherburn et al., Reference Weatherburn, Hickson, Reid, Torres-Rueda and Bourne2017).
Formulation
Formulation is a process by which existing theories, evidence, and ideas are integrated and linked to an individual’s presenting difficulty (Dallos and Johnstone, Reference Dallos and Johnstone2013). Although NHS TT are commissioned to treat conditions outlined in diagnostic criteria, the therapeutic approaches employed rely on formulation to treat the problem that has brought service users to seek help. Collaborative formulation is the ‘lynchpin’ of CBT (Butler, Reference Butler1998).
Therapists should aim for a holistic formulation encompassing mental health, alcohol/drug use, and psychosexual factors (Campbell et al., Reference Campbell, Gurreri, Margetts, Mundy and Rutter2024). It is the argument of this paper that NHS TT practitioners, if provided with adequate context, background theory and information, will be empowered to establish individualised formulations with their service users that include chemsex where this is relevant.
Principle-driven formulation with the ‘5 Ps’
The cognitive model (Beck, Reference Beck2020) underpins the practice of most of the evidence-based approaches delivered by NHS TT practitioners. The ‘5 Ps’ has become a popular framework to support therapists and service users in making the links between presenting issues, precipitating, perpetuating, pre-disposing, and protective factors (Macneil et al., Reference Macneil, Hasty, Conus and Berk2012). Table 5 presents possible areas for consideration when making formulations with service users who participate in chemsex and have co-occurring mental health difficulties.
Biopsychosocial formulation across the 5 Ps (presenting, pre-disposing, precipitating, perpetuating, and protective factors)

Table 5. Long description
A table with three columns labeled Biological, Psychological, and Social, and five rows labeled Presenting, Pre-disposing, Precipitating, Perpetuating, and Protective. The table lists various factors under each category relevant to individuals participating in chemsex with co-occurring mental health difficulties. For example, under Presenting, Biological factors include sleep disruption and weight changes, Psychological factors include psychosis and depression, and Social factors include loss of social and occupational functioning. The table provides a comprehensive framework for understanding the interplay of these factors.
* Sexual difficulties have been listed as a biological and psychological presentation as there can be a primarily physiological or psychological basis for these dependent on the individual case.
** Some or all of these may not be relevant for people who engage in chemsex.
Intervention
Chemsex is usually pleasure-driven, and individuals will not seek and do not need intervention; however, sometimes individuals may seek support. For those who do seek support, CBT represents a potential treatment modality. CBT is widely recognised as the ‘gold standard’ treatment for common mental health problems (Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012), and also has evidence of efficacy in drug use disorders (Hides et al., Reference Hides, Samet and Lubman2010; Magill et al., Reference Magill, Ray, Kiluk, Hoadley, Bernstein, Tonigan and Carroll2019), and compulsive sexual behaviour (Antons et al., Reference Antons, Engel, Briken, Krüger, Brand and Stark2022). Although there are evidence-based, culturally appropriate CBT models specifically for chemsex treatment (Del Pozo-Herce et al., Reference Del Pozo-Herce, Baca-García, Martínez-Sabater, Pérez-Elvira, Gea-Caballero, Chover-Sierra, Satústegui-Dordá, Tovar-Reinoso, Rodríguez-Velasco, Sánchez-Barba, Pérez and Juárez-Vela2024; Íncera-Fernández et al., Reference Íncera-Fernández, Gámez-Guadix and Moreno-Guillén2021; Reback et al., Reference Reback, Veniegas and Shoptaw2014; Śniadach et al., Reference Śniadach, Orlof, Sołowiej-Chmiel, Kicman, Szymkowiak and Waszkiewicz2025), interventions have not been sufficiently studied to enable the creation of formal best-practice chemsex treatment guidelines.
Cognitive models of substance use
Beck et al.’s (Reference Beck, Wright, Newman and Liese1993) cognitive model of drug use highlights the relevance of beliefs as a potential maintenance factor in drug use. The three over-arching sets of beliefs are: (a) core beliefs, mental schemas a person holds about themselves, others, and the world; (b) drug-related beliefs, usually anticipatory (positive expectations, e.g. ‘chems make sex so much better’) or relief-oriented (relief expectation of alleviation, e.g. ‘after chems, I won’t care about anything’); and (c) automatic thoughts, transient thoughts or images of use related to the present situation. Furthermore, these are supported by permissive beliefs (e.g. ‘I am having a good time, but chems would make things a lot better’). Permissive beliefs resolve the cognitive dissonance between existing drug-related beliefs and thoughts that could prevent use (e.g. ‘I don’t need chems to have a good time’). Activation of these different belief structures is dependent on situational factors, emotions, and physical states. By accounting for drug-related or permissive beliefs, further understanding of the function of chemsex can determine whether intervention is warranted or appropriate.
Complementary to Beck et al. (Reference Beck, Wright, Newman and Liese1993) is Marlatt and Gordon’s (Reference Marlatt and Gordon1985) model of relapse. In the model, relapse is considered a process that builds over time rather than being a singular event. Having made a decision to stop or reduce chemsex, individuals then face high-risk situations that may potentially trigger relapse. The likelihood of relapse can be decreased by adopting effective coping strategies and building self-efficacy. If an ineffective strategy is employed, subsequent cognitive processes can lead to dissonance (‘I can resist – I cannot resist’), rule violation effects (e.g. common thought distortions such as ‘I’ve started drugs again now, no point in stopping’), and a positive bias for chemsex (e.g. expecting a good outcome by using). Over time, chemsex participants build mastery of the practice itself and develop specialist skills, with high self-efficacy in their use (Hickson, Reference Hickson2018). Therefore, changing patterns seeks to develop new skills and an alternative position – to resist or stop use. Building confidence to resist use takes time and lots of practice to increase self-efficacy at the opposite pole.
Sustaining long-term change is reliant on ‘lifestyle balance’ (Marlatt and Gordon, Reference Marlatt and Gordon1985). Even with self-efficacy and effective coping strategies for high risk situations, lifestyle imbalance can lead to a build-up of stressors and evoke a series of cognitive processes. One process is the problem of immediate gratification. In the context of chemsex, a person may rationalise use despite negative consequences (e.g. ‘I haven’t used all week and I still don’t feel better, a little play won’t hurt’). This can be heightened by denial (e.g. ‘my chems use was bad last year, it is different this time’) or engaging in seemingly irrelevant decisions (e.g. ‘I can still meet a guy and if he gets high, I won’t’). These thinking patterns provide targets for treatment, teaching service users to prepare and rehearse effective coping skills like a ‘fire drill’ (Wanigaratne, Reference Wanigaratne1990).
Therapeutic techniques
The following section outlines therapeutic techniques that a cognitive behavioural therapist may wish to consider around problematic chemsex. In line with best practice, interventions would be linked to collaboratively established formulation and treatment goals. High-intensity therapists who are additionally competent in transdiagnostic strategies offered by mindfulness-based approaches, such as acceptance and commitment therapy (ACT) and dialectical behavioural therapy (DBT), or a process-based approach, such as compassion focused therapy (CFT), may find these useful in enhancing their intervention. Table 6 provides some examples of different chemsex presentations and ways of working with these in clinical practice.
Illustrative examples of functions of chemsex for which people might seek support

Table 6. Long description
The table presents a structured approach to addressing problematic chemsex through cognitive behavioural therapy. It is divided into four main functions of use: improve mood, performance and confidence, meet sexual and relational needs, and anxiety and distress regulation. Each function is broken down into key challenges, therapeutic techniques, cultural sensitivity tips, and case examples. The table includes four rows and five columns, with headers for each section. For improving mood, techniques like cognitive restructuring and distress tolerance are suggested, along with cultural sensitivity tips such as acknowledging internalized stigma. For performance and confidence, behavioural experiments and mindfulness-based CBT are recommended, with a focus on cultural pressures around masculinity. To meet sexual and relational needs, sensate focus and compassion-focused therapy are advised, along with psychoeducation about addiction models. For anxiety and distress regulation, psychoeducation and behavioural experiments are suggested, with an emphasis on LGBTQ+ affirming examples of social connections. The table provides specific case examples for each function, illustrating practical applications of the therapeutic techniques.
Behavioural activation
National Institute for Health and Care Excellence (2022) guidelines recommend behavioural activation as an intervention to help reduce avoidance and improve mood through engagement with valued activities. Behavioural activation seeks to increase daily rewarding experiences as an alternative to drug use (Martínez-Vispo et al., Reference Martínez-Vispo, Martínez, López-Durán, Fernández del Río and Becoña2018). In the context of chemsex, the use of drugs combined with sexual behaviours may provide pleasure, connection, and confidence. However, this may lead to reduced engagement in other life domains, diminishing a sense of mastery and potentially perpetuating a cycle of low mood. Identifying alternative, rewarding activities to chemsex could feasibly improve mood and increase mastery. Furthermore, setting short-term goals (e.g. taking a one-week break from chemsex) can create a foundation of achievement which can be built upon.
By drawing from an individualised, collaborative formulation that describes the function of chemsex, it may be possible to identify alternative valued activities. For example, the literature suggests that chemsex provides cultural connection as well as pleasure. Alternative activities which meet these needs (e.g. attending LGBTQ+ events or LGBTQ+ social groups) should be prioritised.
Cognitive skills training and restructuring
Cognitive skills training consists of identifying and challenging maladaptive beliefs, cognitive processing biases and increasing meta-cognitive awareness. Standard CBT techniques (e.g. Socratic questioning, advantages-disadvantages analysis, thought records) can be used by therapists across both drug use and depression (Beck et al., Reference Beck, Rush, Shaw, Emery, DeRubeis and Hollon2024; Beck et al., Reference Beck, Wright, Newman and Liese1993). Additional techniques, such as cognitive continuums and trigger diaries, are also applicable to facilitate cognitive change (Mitcheson et al., Reference Mitcheson, Maslin, Meynen, Morrison, Hill and Wanigaratne2010). Table 7 presents drug-related beliefs for therapists to be aware of, which are common among people who use drugs. Mitcheson et al. (Reference Mitcheson, Maslin, Meynen, Morrison, Hill and Wanigaratne2010) also provide guidance on how to work clinically with such drug-related beliefs.
Key drug-related beliefs with chemsex examples; drug-related beliefs taken from Mitcheson et al. (Reference Mitcheson, Maslin, Meynen, Morrison, Hill and Wanigaratne2010)

Table 7. Long description
A table with two columns and nine rows comparing drug-related beliefs with chemsex examples. The first column lists categories such as coping and self-efficacy, anticipatory, relief-oriented, craving and withdrawal, pharmacology and method of use, permissive, control, negative beliefs about the self and drug use, mental imagery, and cognitive biases. The second column provides specific chemsex examples for each belief category, such as ‘I can’t have sex without chems’ for coping and self-efficacy, and ‘Intrusive imagery triggered by a location’ for mental imagery. The table highlights various beliefs and their associated examples in chemsex contexts.
Alongside the drug-related beliefs, it is essential to consider the role of other belief structures related to sex, sexual identity, culture, and stigma. For example, LGBTQ+ youth report using ‘shame-avoidance strategies’, like drug use, to minimise the effects of stigma and homophobia (McDermott et al., Reference McDermott, Roen and Scourfield2008). Homophobic marginalisation contributes to harm for chemsex participants, which can perpetuate mental health difficulties (Miltz et al., Reference Miltz, Rodger, Sewell, Speakman, Phillips, Sherr, Gilson, Asboe, Nwokolo, Clarke, Gompels, Allan, Collins and Lampe2017; Pollard et al., Reference Pollard, Nadarzynski and Llewellyn2018).
Behavioural experiments
Behavioural experiments (BEs) are structured experiential activities integral to cognitive therapy, designed to test existing beliefs and construct new, helpful beliefs. They also help therapists gather information to support the ongoing cognitive formulation of the service user’s difficulties (Bennett-Levy et al., Reference Bennett-Levy, Westbrook, Fennell, Cooper, Rouf and Hackmann2004). BEs are a core aspect of cognitive therapy competencies (Roth and Pilling, Reference Roth and Pilling2008).
Incorporating BEs aligned with sex-positive principles would be beneficial for therapists working with service users experiencing distress or negative outcomes related to chemsex (Frank et al., Reference Frank, Noyon, Höfling and Heidenreich2010; Malandain and Thibaut, Reference Malandain and Thibaut2023). By asking specific open-ended questions about sex and responding in a non-judgemental, compassionate manner, therapists provide service users with an opportunity to identify specific situations and beliefs that may contribute to the service user’s presenting problems. Once beliefs are identified, therapists can utilise their core competency in planning BEs to help service users test or develop more helpful beliefs, linked to the function of chemsex within their individual formulation. Table 7 outlines examples of drug-related beliefs that therapists may identify in this process, and which may be amenable to testing and changing through the use of BEs. Table 6 provides brief illustrative examples that link behavioural experiments to possible functions of chemsex. Neither table provides a comprehensive list of possible beliefs or functions, but rather these tables demonstrate ways in which drug and sex-related difficulties may be incorporated into a planned cognitive behavioural intervention. By collaboratively designing experiments rooted in the service user’s individualised cross-sectional formulation of chemsex or sober sex situations, helpful beliefs and behaviours may be promoted, in line with the service user’s therapy goals.
Functional analysis
Functional analysis (FA) originates from behavioural science which assumes behaviour can be observed, measured, and predicted (Skinner, Reference Skinner1957). In drug use, FA can aid formulation and conceptualisation by identifying the function of drug use as a means of adaptation and/or survival (Reichert et al., Reference Reichert, Legal, Oliani, Zamignani, Oliani, Reichert and Banaco2021). This process helps to identify what precipitates, perpetuates, and determines behaviour through (a) antecedents (e.g. feeling isolated or lonely at the weekend), (b) responses (e.g. looking for a partner for the evening to use chems with), and (c) consequences (e.g. creating a sense of connectedness, disinhibition, relaxation). FA is helpful throughout treatment, to identify situations where difficulty persists. Therapists can explore this process using the five W’s: what happened, when, where, why, and who with (Reichert et al., Reference Reichert, Legal, Oliani, Zamignani, Oliani, Reichert and Banaco2021).
Transdiagnostic strategies
Emotion regulation
Regulating emotions is an active process which manages the intensity, response, and expression of emotions (Joormann and Stanton, Reference Joormann and Stanton2016). Difficulties in regulating emotions can lead to increased drug use (Weiss et al., Reference Weiss, Kiefer, Goncharenko, Raudales, Forkus, Schick and Contractor2022). Drug use acts as an effective method to cope with positive and negative emotions due to relatively immediate relief and low cognitive effort. Furthermore, homophobic and transphobic stigma can significantly impact cognitive resources to manage emotions effectively (Pachankis et al., Reference Pachankis, Rendina, Restar, Ventuneac, Grov and Parsons2015; Wang et al., Reference Wang, Burton and Pachankis2018). A possible mechanism by which stigma impacts cognitive resources is via the activation of minority stress processes, which increase cognitive and emotional load (Bridge et al., Reference Bridge, Langford, McMullen, Rai, Smith and Rimes2024). Experiences of stigma and discrimination can heighten vigilance and self-monitoring, as individuals anticipate or attempt to mitigate rejection. This hyper-awareness diverts cognitive resources away from other tasks, reducing capacity for problem-solving, concentration, and decision-making.
During periods of increased distress, regulating emotions using adaptive strategies can be difficult (Vujanovic et al., Reference Vujanovic, Meyer, Heads, Stotts, Villarreal and Schmitz2017). Therefore, CBT-based skills training to increase emotion regulation skills, such as breathing techniques and cognitive restructuring, are warranted. Service users who participate in chemsex report emotion regulation skills as one of the most helpful skills to develop (Arends et al., Reference Arends, Van den Heuvel, Foeken-Verwoert, Grintjes, Keizer, Schene, Van der Ven and Schellekens2020). Alongside building self-efficacy to manage emotions effectively, integrating third-wave approaches such as mindfulness, can help to develop self-awareness. Compassion-focused interventions targeting self-criticism and low self-esteem may also be acceptable and feasible in supporting with the impact of minority stress processes (Bridge et al., Reference Bridge, Langford, McMullen, Rai, Smith and Rimes2024).
Distress tolerance
Related to emotion regulation, distress tolerance is the ability to endure aversive emotional and physical states (Lass and Winer, Reference Lass and Winer2020). Such distress is common within both chemsex and mental health disorders (Vujanovic et al., Reference Vujanovic, Webber, McGrew, Green, Lane and Schmitz2022). Low tolerance for distressing states, such as cravings or comedowns, can increase the risk of further use to manage aversive symptoms (Spencer et al., Reference Spencer, Addison, Alderson, McGovern, McGovern, Kaner and O’Donnell2021). Integrating distress tolerance skills into therapy has the potential to alleviate aversive depression and distress from chemsex (Vujanovic et al., Reference Vujanovic, Meyer, Heads, Stotts, Villarreal and Schmitz2017). Third-wave CBT approaches, such as DBT or ACT, have feasible techniques to increase distress tolerance skills (Malandain and Thibaut, Reference Malandain and Thibaut2023). For example, DBT emphasises using the TIPP (Temperature, Intense exercise, Paced breathing, Paired muscle relaxation) skill to change body chemistry and reduce distress (Linehan, Reference Linehan2014). Furthermore, using behavioural experiments to predict the ability to cope when attempting distress tolerance skills can generate and consolidate learning experiences.
Motivational interviewing
MI is a person-centred therapeutic style that aims to guide the resolution of ambivalence and elicit behaviour change (Rollnick and Miller, Reference Rollnick and Miller1995). Miller and Rollnick (Reference Miller and Rollnick2013) outlined MI as a collaborative process that utilises four main skills: (a) open questioning, using structured evocative questions, such as elicit-provide-elicit; (b) affirmations of previous successes, personal strengths, and effort; (c) reflective listening to communicate understanding and acceptance towards the service user, facilitating empathy; and (d) summarising to reinforce key statements of change. See Miller and Rollnick (Reference Miller and Rollnick2013) for further information and guidance.
Over-arching ethical and clinical considerations
Cultural humility
‘Cultural humility’ in the chemsex context refers to the ability of therapists to communicate effectively and sensitively with service users, particularly when they do not have familiarity with LGBTQ+ and/or drug-using cultures. This encompasses theoretical knowledge (for example, an understanding of how homophobia or marginalisation may impact mental health), language (for example, understanding and reflecting a service user’s colloquial terms for drugs or sexual practices), and therapist reflexivity (actively challenging biases, learning about chemsex/LGBTQ+ culture, and developing self-awareness) (Cruciani et al., Reference Cruciani, Quintigliano, Mezzalira, Scandurra and Carone2024). Cultural competence improves service user satisfaction with healthcare and may also lead to improved outcomes (Beach et al., Reference Beach, Price, Gary, Robinson, Gozu, Palacio, Smarth, Jenckes, Feuerstein and Bass2005; Lie et al., Reference Lie, Lee-Rey, Gomez, Bereknyei and Braddock2011).
Non-judgemental approach
A non-judgemental approach is accepting a whole person for who they are, without bias or opinion. Adopting this attitude towards service users can foster acceptance, genuineness, and empathy within the therapy room to facilitate behavioural change (Rogers, Reference Rogers and Koch1959). This is an essential approach to working with service users who participate in chemsex, as some fear being misunderstood or judged for their actions (Evans, Reference Evans2019; Herrijgers et al., Reference Herrijgers, Poels, Vandebosch, Platteau, van Lankveld and Florence2020). Despite this, around one in four LGBT people and one in two trans people in British healthcare settings experience discrimination from healthcare staff (Bachmann and Gooch, Reference Bachmann and Gooch2018). Without a non-judgemental approach, therapists can exacerbate feelings of shame and create barriers to engagement (Jaspal, Reference Jaspal2020).
Inappropriate curiosity
By creating a safe space for disclosure, therapists can sensitively explore factors related to sex, drugs, and mental health leading to meaningful engagement from service users (Bourne et al., Reference Bourne, Ong and Pakianathan2018). This requires therapists to be open to service user’s experiences whilst being self-aware of their reactions to what is shared or expressed. For some therapists, stories or experiences unique to chemsex may be novel and generate a reaction (Jaspal, Reference Jaspal2020). This requires sensitive consideration of language, such as using accurate pronouns, and self-management of non-verbal communication, such as facial responses (Hegazi and Pakianathan, Reference Hegazi and Pakianathan2022; Jaspal, Reference Jaspal2020). Therapists should also be cautious to manage feelings of ‘inappropriate curiosity’ (Steinberg et al., Reference Steinberg, Alpert and Courtois2021). This may lead to invasive or potentially even distressing questioning of service users, for example seeking explicit descriptions of sexual practices, ‘coming out’, or traumatic experiences related to sexuality and gender, where heterosexual/cisgender service users would not be asked the same questions (Wall et al., Reference Wall, Patev and Benotsch2023). A curious, exploratory approach that aids clinical formulation is fundamental.
Conclusions
This paper has examined the need for inclusive, affirming, and psychologically informed approaches to working with chemsex and co-occurring mental health difficulties. By adopting a non-judgemental, trauma-informed, and sex-positive stance, therapists can support people who may be let down by existing mental health systems (Campbell et al., Reference Campbell, Gurreri, Margetts, Mundy and Rutter2024). Informed by established psychosocial approaches to working with addiction, this paper presents a range of cognitive behavioural strategies – including behavioural activation (Martínez-Vispo et al., Reference Martínez-Vispo, Martínez, López-Durán, Fernández del Río and Becoña2018), cognitive restructuring (Vujanovic et al., Reference Vujanovic, Meyer, Heads, Stotts, Villarreal and Schmitz2017), and behavioural experiments (Bennett-Levy et al., Reference Bennett-Levy, Westbrook, Fennell, Cooper, Rouf and Hackmann2004) – which can be adapted to support chemsex populations.
Rather than pathologising chemsex, we argue the need for contextual and functional understandings of drug use and sex, which account for intersectional factors such as minority stress, shame, trauma, and systemic discrimination (Abrahão et al., Reference Abrahão, Kortas, Blaas, Koch Gimenes, Leopoldo, Malbergier, Torales, Ventriglio and Castaldelli-Maia2022; Gertzen et al., Reference Gertzen, Karcher, Schwarz, Rosenberger, Strasburger, Rabenstein, Strasser, Palm and Rüther2024; Pitman et al., Reference Pitman, Marston, Lewis, Semlyen, McManus and King2022). To reduce barriers and improve outcomes, there is a critical need for culturally competent care – an approach that encompasses therapist reflexivity, appropriate language, and humility.
Alcohol and drug use should not be a barrier to accessing evidence-based treatment for mental health difficulties. NHS therapists are well-positioned to offer effective support, and this requires a shift in assumptions, training, and service delivery. Meeting the needs of chemsex participants is not a difficult task, as it encompasses, at its core, inclusive, responsive, and modern psychological practice.
Key practice points
-
(1) You do not need to be an expert in drugs and alcohol, or sex, to work with service users who participate in chemsex.
-
(2) Use a non-judgemental, sex-positive, trauma-informed, and culturally competent approach for effective engagement with chemsex participants.
-
(3) Cognitive behavioural techniques can be adapted to address common mechanisms underlying mental health difficulties and chemsex.
-
(4) Collaboration with multi-disciplinary teams, including sexual health, addiction, and psychosexual services, can improve care for service users who participate in chemsex.
Data availability statement
Not applicable.
Acknowledgements
None.
Author contributions
William Barber: Conceptualization (equal), Project administration (lead), Resources (equal), Writing - original draft (equal), Writing - review & editing (equal); Miriam Hillyard: Conceptualization (equal), Project administration (equal), Writing - original draft (equal), Writing - review & editing (equal); Dean Connolly: Conceptualization (equal), Project administration (equal), Writing - original draft (equal), Writing - review & editing (equal); Eve da Silva: Conceptualization (equal), Project administration (equal), Writing - original draft (equal), Writing - review & editing (equal); Gemma Scott: Conceptualization (equal), Project administration (equal), Writing - original draft (equal), Writing - review & editing (equal); Luke Mitcheson: Conceptualization (supporting), Writing - original draft (equal), Writing - review & editing (equal); Elizabeth Appiah-Kusi: Conceptualization (equal), Project administration (equal), Writing - original draft (equal), Writing - review & editing (equal).
Financial support
No specific funding was sought to undertake writing this article. Dr Miriam Hillyard is funded by an MRC Addiction Research Clinical (MARC) Fellowship. Dr Dean Connolly holds an NIHR Academic Clinical Fellowship in Public Health Medicine. Dr Luke Mitcheson within the last three years has received research grant funding from the NIHR for a realist evaluation of services for people with co-occurring mental health and substance use and a study of ketamine for AUD; from Indivior for the EXPO study of extended-release buprenorphine; and from Beckley PsyTech for a phase 2a trial of 5-MeO-DMT for AUD. The views in this paper do not necessarily reflect the views of the NIHR, MRC, NHS, OHID or DHSC.
Competing interests
William Barber – none to declare. Miriam Hillyard – none to declare. Dean Connolly co-chairs the UK Faculty of Public Health Drugs Special Interest Group and is a member of the Drug Science Enhanced Harm Reduction Working Group and UK Advisory Council on the Misuse of Drugs LGBTQ+ Working Group. Eve da Silva – none to declare. Gemma Scott – none to declare. Luke Mitcheson has a clinical psychology secondment at the Office for Health Improvement and Disparities, Department of Health and Social Care. He declares receipt of author royalties for a clinical textbook on CBT and addiction (published by Wiley). He has received consulting fees from the British Association of Counselling and Psychotherapy for work on counselling competencies. He is a member of the British Psychological Society’s Faculty of Addiction Committee. Elizabeth Appiah-Kusi – none to declare.
Ethical standards
The authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the British Association for Behavioural and Cognitive Psychotherapies (BABCP) and the British Psychological Society (BPS). This article is a empirically grounded clinical guidance paper and does not report original research involving human participants, the collection of new participant data, or the use of identifiable clinical material. As such, formal research ethics approval was not required. No individual service user case material is presented, and any clinical examples are illustrative.
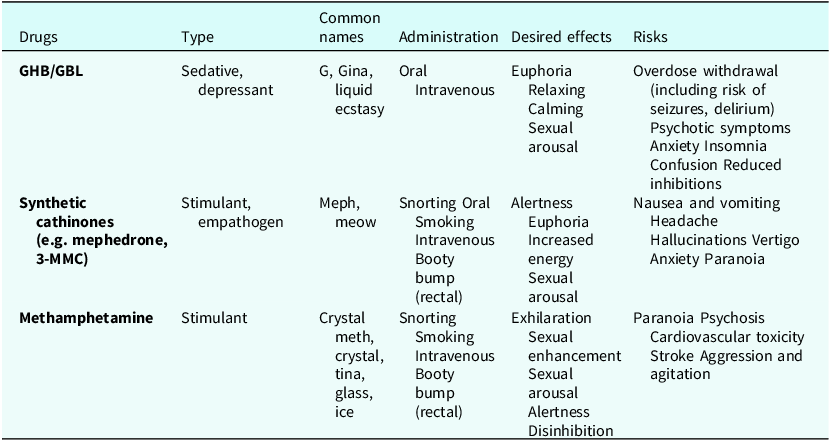

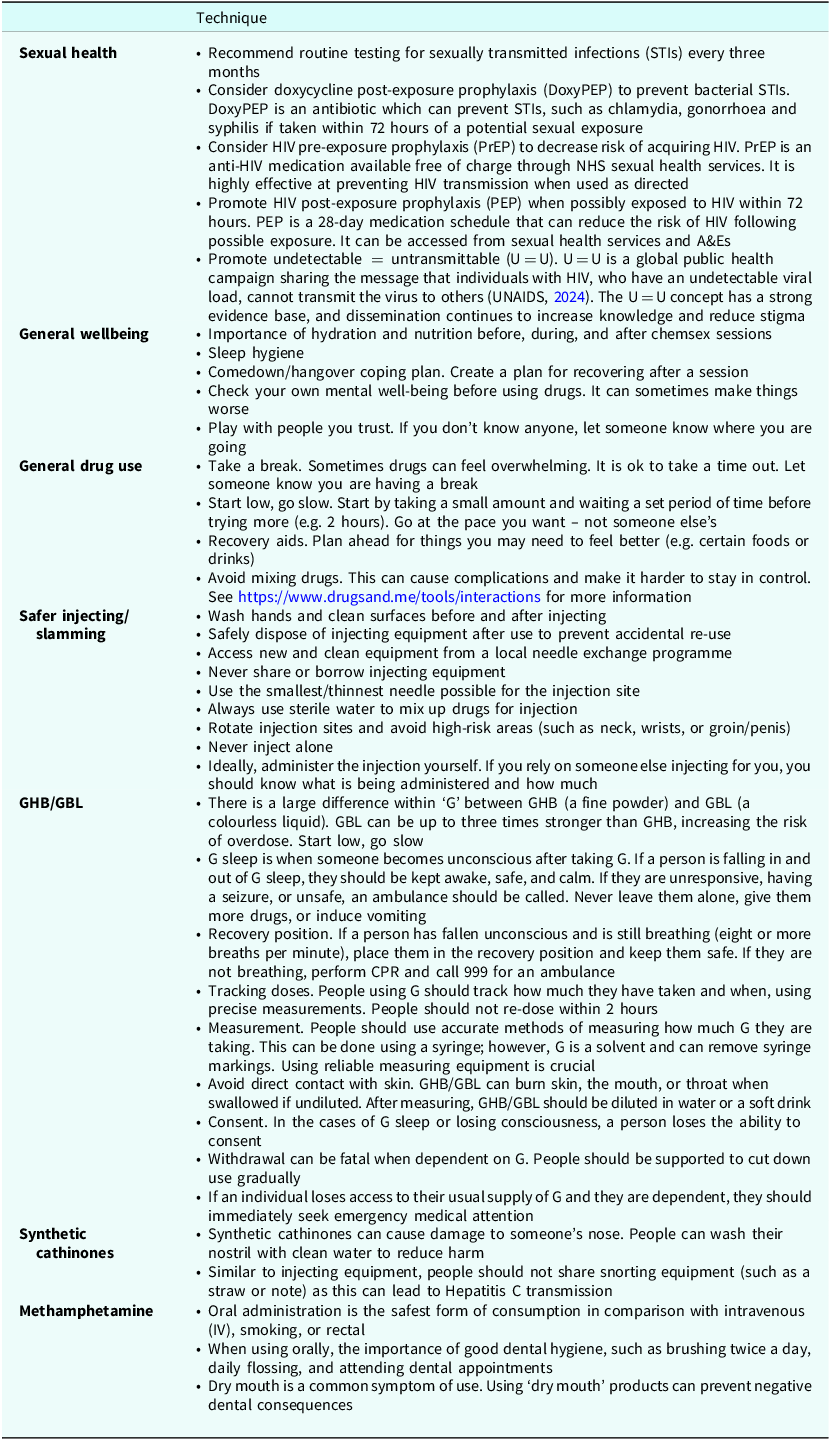
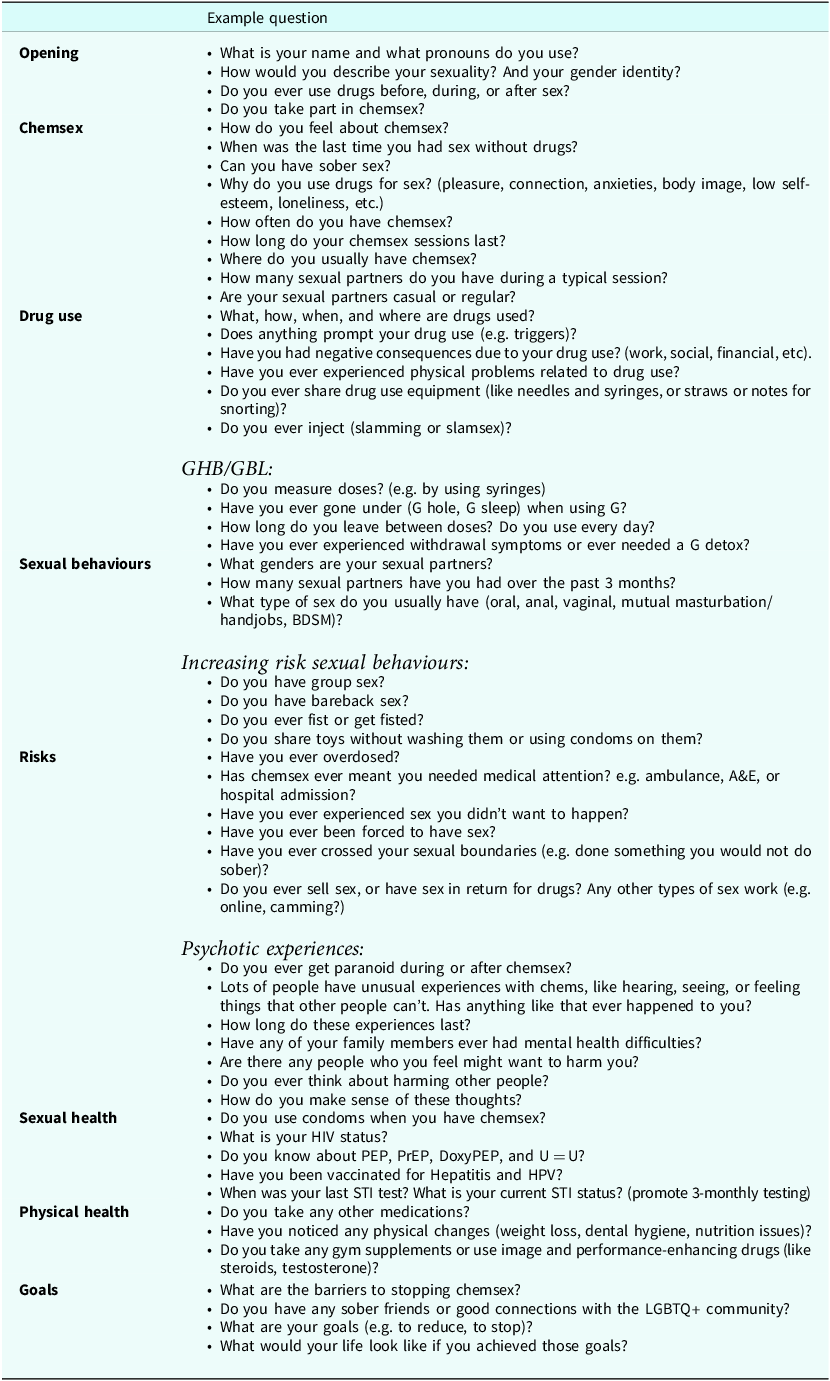
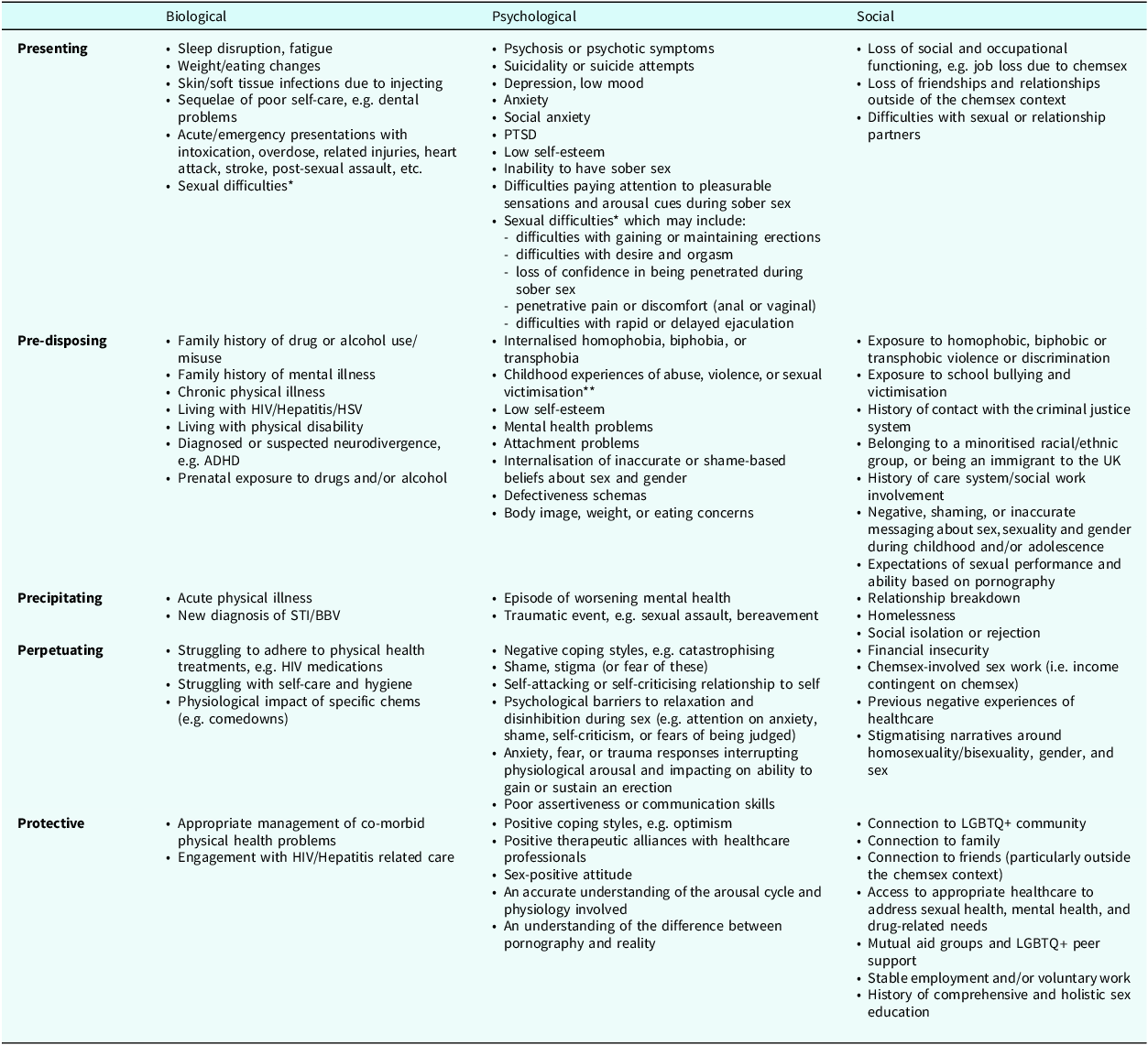
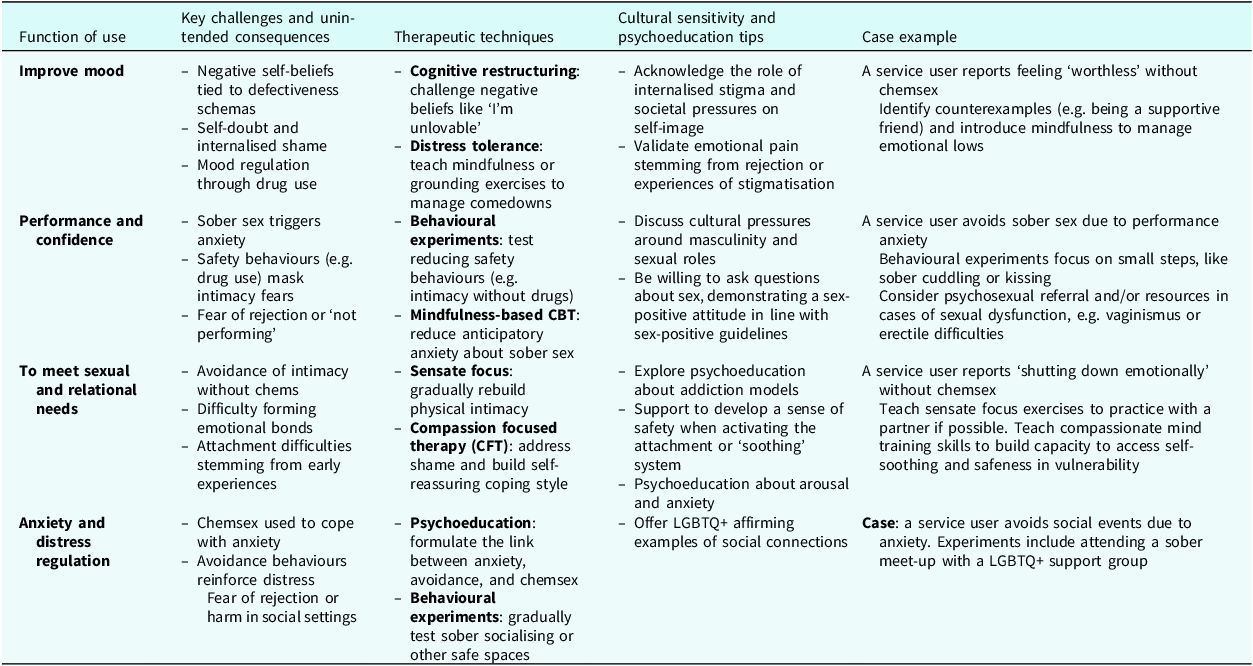
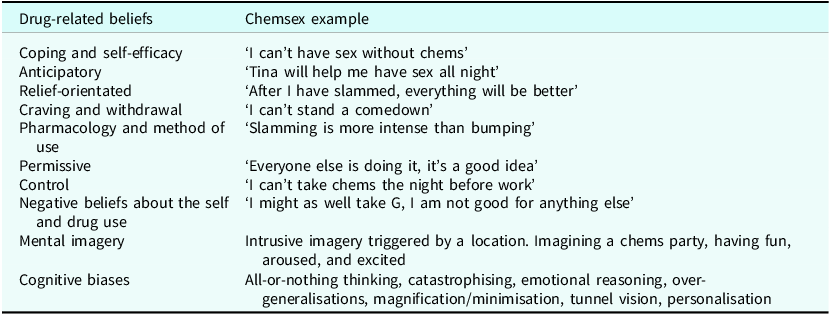

 Open access
Open access
Comments
No Comments have been published for this article.