


Introduction
The primary treatment for low-risk early-stage breast cancer typically involves surgery followed by adjuvant radiotherapy (RT). Advancements in RT have significantly improved survival rates. Reference Ellison and Saint-Jacques1 However, many breast cancer patients report arm dysfunction in the months to years following treatment, Reference Johansen, Fossa, Nesvold and Fossä2,Reference Ng (Muffet), Kilburn and Kirby3 negatively affecting their quality of life. Given that survival rates are at an all-time high, 4 it is critical to ensure a high quality of life in those living beyond cancer.
A critical aspect of RT treatment planning is ensuring the maximum radiation dose is delivered to the tumour site while minimising exposure to the organs at risk (OARs), such as the heart and lungs. During RT treatment planning, OARs are outlined on a computer tomography (CT) scan to ensure radiation doses remain below the organ tolerance thresholds. RT technique and patient positioning have been shown to affect the amount of radiation delivered to the OARs. For example, radiation to the OARs is reduced when using the hybrid-intensity-modulated RT (hybrid IMRT). Reference Bi, Zhu and Dai5 Additionally, positioning the patient in the prone compared to the supine position significantly reduces radiation to the lung, thyroid and oesophagus. Reference Deseyne, Speleers and De Neve6
Unlike the OARs, the skeletal muscles are not avoided during RT treatment planning, leaving them vulnerable to varying degrees of radiation exposure. The skeletal muscles surrounding the shoulder have different functions that enable arm movement and stabilise the four shoulder joints to perform various activities. Skeletal muscles are generally considered to have a high radiation tolerance (60–80 Gy). Reference Hall and Giaccia7 In contrast, one study reported that arm dysfunction, including pain, stiffness and swelling, occurs when a much lower RT dose is delivered to the shoulder (15 Gy). Reference Johansen, Fossa, Nesvold and Fossä2 Moreover, radiation delivery to the shoulder muscles was found to reduce pectoralis major thickness and increase stiffness, Reference Wolfram, Takayesu and Pierce8 alter muscle stretch reflexes, Reference Lulic-Kuryllo, Leonardis, Momoh and Lipps9 decrease range of motion and strength Reference Herrera and Dickerson10 and increase self-reported impairments in arm function. Reference Bazan, DiCostanzo and Hock11
The amount of radiation delivered to the shoulder muscles is dependent on the RT technique used. Previous research has shown that using 3- or 4-field techniques results in a greater mean dose delivered to the shoulder muscles compared to 2-field techniques. Reference Lipps, Sachdev and Streuss12 More recent work has also shown that using IMRT reduces the radiation dose to the shoulder compared to 3D conformal RT (3DCRT) Reference Bazan, DiCostanzo and Hock11 and that intensity-modulated proton therapy (IMPT) results in less radiation exposure to the shoulder compared to using volumetric-modulated arc therapy (VMAT). Reference Burlile, Shiraishi and Gunn13 Lastly, 3DCRT can result in up to 75% of the shoulder volume receiving a dose of V20 Gy. Reference Fadavi, Arefpour and Beigi14
Previous work evaluating the effects of RT on the shoulder did not compare common RT techniques used in clinical practice, such as hybrid IMRT, wedged fields, VMAT and hybrid VMAT. Reference Bradley and Mendenhall15 Furthermore, no studies have assessed shoulder muscle exposure when RT is delivered in the prone position. Therefore, this study aims to: 1) compare the dose delivered to the shoulder muscles between common RT techniques and 2) investigate the influence of patient position on the mean dose delivered to the shoulder muscles. Our main hypotheses are that: 1) hybrid IMRT would deliver a lower mean dose and expose less muscle volume to V15/V30 Gy compared to wedged field, VMAT and hybrid VMAT; 2) 3-field supraclavicular RT technique would increase muscle volume exposure, affecting the posterior shoulder muscles; and 3) delivering RT in the prone position would result in less mean dose delivered to the shoulder muscles compared to the supine position.
Materials and Methods
The treatment plans of 54 patients with unilateral breast cancer treated with various RT techniques in either prone or supine positions were evaluated. The patients were separated into specific cohorts based on the type of treatment they would typically receive. Twenty-four patients were included in the analyses comparing hybrid IMRT, wedged field, VMAT and hybrid VMAT. Twenty-three patients were included in the 3-field supraclavicular RT analyses. Lastly, seven patients treated in the supine position and seven patients treated in the prone position were included in the analyses investigating the effect of patient positioning. The treatment was delivered to the right or the left breast, and both intact breast and post-mastectomy chest wall patients were included. The retrospectively accessed CT scans were previously acquired for clinical care. Eligible patients included those treated with RT in the last 5 years. This study was approved by the Waterloo-Wellington Research Ethics Board (WWREB #2023-0762).
Muscle contouring
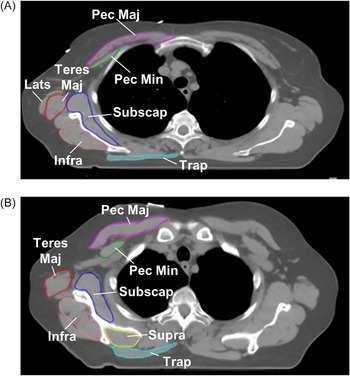
The boundaries of the eight shoulder muscles were contoured on the patient’s CT scan for each axial slice as described. Reference Lipps, Sachdev and Streuss12 The contoured muscles included the pectoralis major, pectoralis minor, infraspinatus, latissimus dorsi, subscapularis, supraspinatus, teres major and trapezius (Figure 1A and 1B). The radiodensity window was adjusted to distinguish between the muscles and other structures, such as bone or breast/subcutaneous tissue.
Eight muscles were contoured on each axial slice, abbreviated in A and B. Pec Maj: pectoralis major; Pec Min: pectoralis minor; Teres Maj: teres major; Supra: supraspinatus; Infra: infraspinatus; Subscap: subscapularis; Lats: latissimus dorsi; Trap: trapezius.

RT techniques
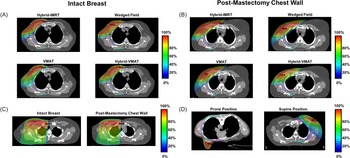
Treatment plans for each patient were prepared by an experienced radiation therapist in collaboration with the medical physics team. Representative CT scans are shown in Figure 2, along with individual muscle segmentations and dose colour wash. Four different commonly used RT treatment techniques were evaluated, including hybrid IMRT, wedged field, VMAT and hybrid VMAT. A total of 24 patients were included. Treatment plans were prepared in the Eclipse Treatment Planning System version 18 (Varian Medical System, Palo Alto, USA). The details of the four RT techniques are described below.
Representative image depicting different RT techniques and how they affect anterior and posterior shoulder muscles. (A)–(B) Hybrid IMRT, wedged field, VMAT and hybrid VMAT for intact breast (A) and post-mastectomy chest wall (B). (C) A 3-field supraclavicular technique intact breast and post-mastectomy chest wall. (D) The effect of radiation when the patient is positioned in the prone versus the supine position.

Hybrid IMRT
The hybrid IMRT uses a medial and lateral tangential open-field arrangement and another medial and lateral optimised field arrangement (Figure 2A and 2B). The open fields are weighted 70% of the prescription (i.e., 70% of the prescription is delivered by the open fields), while the remaining 30% is delivered by IMRT fields. Details on the specifics of hybrid IMRT delivery at our cancer centre have been published previously. Reference Osei, Darko and Fleck16
Wedged field
The wedged field plans utilised a standard medial and lateral tangential beam arrangement with dynamic wedges applied to improve dose homogeneity across the target volume (Figure 2A and 2B). Similar to the hybrid IMRT technique, a portion of the prescription dose was delivered using static open tangential fields without beam modifiers, thereby preserving the contribution of unmodulated beams to the overall plan.
VMAT
The VMAT plans are generated using two complementary arcs about a common isocenter (Figure 2A and 2B). The first arc initiates at the medial tangential beam orientation (analogous to the medial tangential field in the hybrid IMRT technique) and rotates clockwise through the ipsilateral anterior quadrant to approximately 180° posterior. The second arc is delivered in the counterclockwise direction, extending from the posterior (≈180°) position back to the medial tangential orientation, thereby providing continuous dose modulation across the ipsilateral breast or chest wall.
Hybrid VMAT
The hybrid VMAT technique employed the same overall field geometry as the hybrid IMRT approach (Figure 2A and 2B). In contrast to the hybrid IMRT, in which tangential optimised static fields are used, the hybrid VMAT plan replaced the static IMRT fields with two complementary VMAT arcs. The first arc was delivered clockwise from the medial tangential orientation to the lateral tangential orientation (like the hybrid IMRT), and the second arc was delivered counterclockwise from the lateral tangential orientation back to the medial tangential orientation.
3-field supraclavicular technique
An additional cohort of 23 patients with nodal involvement were treated using a 3-field supraclavicular technique designed to encompass the supraclavicular region. The 3-field arrangement consisted of a mono-isocentric two tangential fields, configured analogously to those used in the hybrid IMRT plans, supplemented by a single anterior field directed at the supraclavicular nodal region (Figure 2C). Details on the exact planning procedures were previously described. Reference Osei, Dang and Darko17
Patient positioning
Supine position
Patients who were treated in the supine position (47 out of 54 patients) lay on their back with both arms raised above their head. Reference Osei, Dang and Darko17 The patient’s head was turned slightly contralateral. For some patients, the arm position had to be adjusted because they could not be scanned through the CT simulator bore diameter due to arm positioning. In these cases, the positioning was slightly modified so that the ipsilateral arm is raised above the head, and the contralateral arm is placed by the patient’s side.
Prone position
A subset of patients received treatment while in the prone position (N = 7). These patients were compared to seven age-matched patients who received treatment in the supine position. In the prone position, the patient lay on their stomach with their arms above their head on the Q-Fix Prone Breast Board with the ipsilateral treatment breast falling anteriorly into the board opening (Figure 2D).
Data and statistical analyses
All treatment plans were prescribed at 40 Gy in 15 fractions. Muscle radiation exposure was quantified by mean, maximum and minimum dose, along with the percentage muscle volume receiving 5 Gy (V5) to 40 Gy (V40) in 5 Gy increments. Statistical tests focused on two specific dose metrics: V15 Gy, which was previously shown to be associated with arm dysfunction Reference Johansen, Fossa, Nesvold and Fossä2 and V30 Gy, which was evaluated in previous studies. Reference Bazan, DiCostanzo and Hock11–Reference Fadavi, Arefpour and Beigi14 The Wilcoxon signed-rank test was used to compare mean dose, V15 Gy and V30 Gy for each muscle between hybrid IMRT and wedged field, VMAT, and hybrid VMAT. Considering the number of comparisons performed, the significance was Bonferroni-corrected and set to p < 0.0006. The Mann–Whitney U test was used to compare the mean radiation dose between the prone and supine patient positions. To account for multiple comparisons, the significance was Bonferroni-corrected and set to p < 0.006.
Results
The impact of the RT technique on dose and muscle volume affected
Mean dose
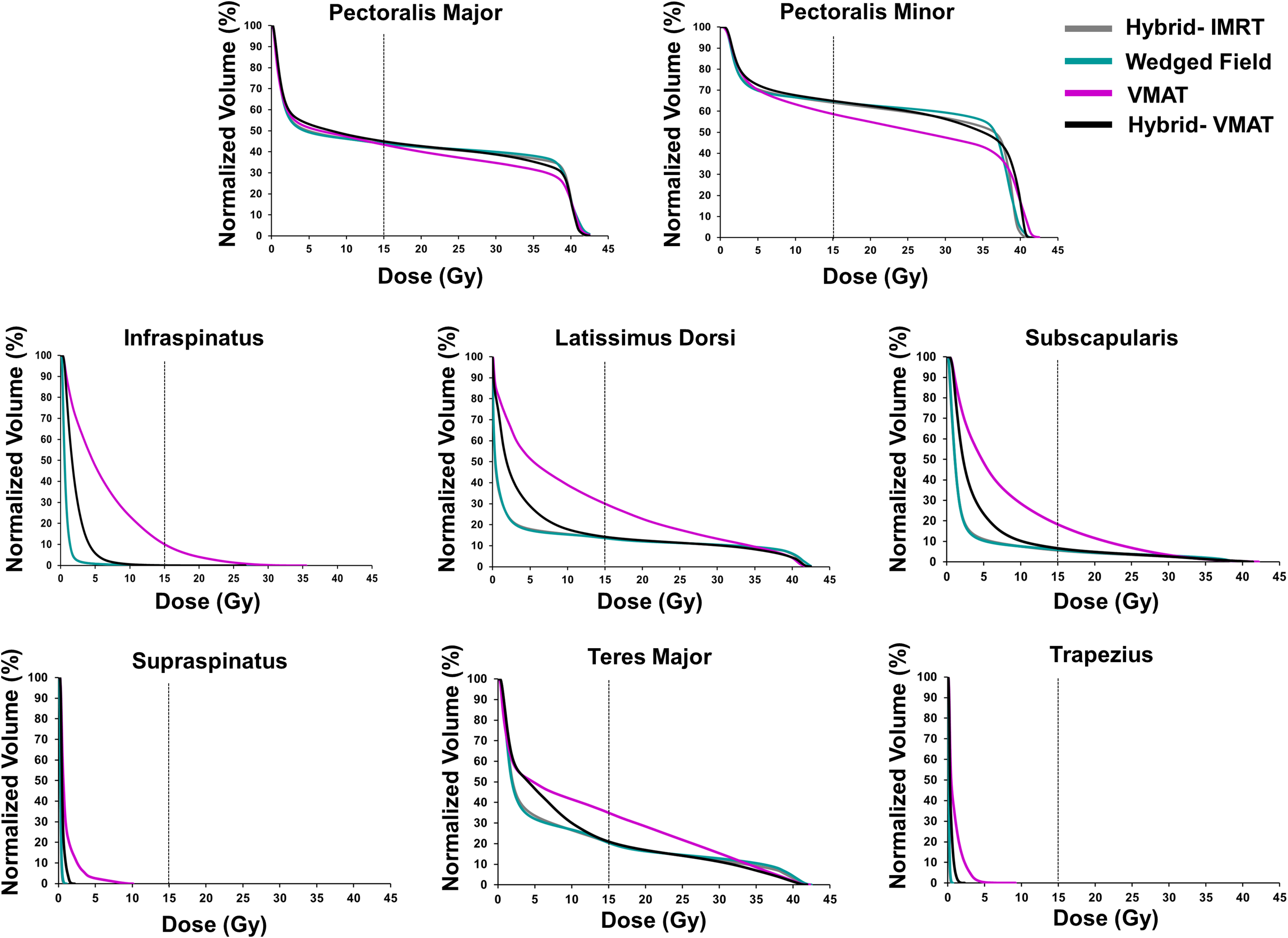
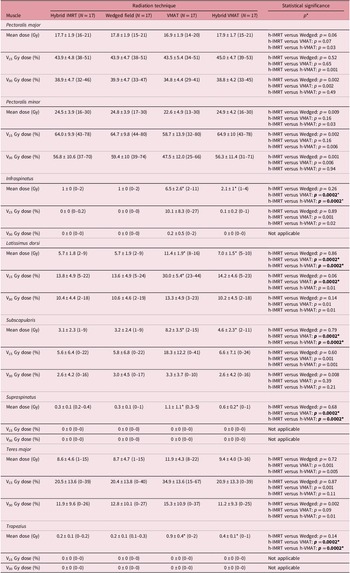
The amount of radiation delivered to the pectoralis major and the pectoralis minor was similar between four RT techniques (all p > 0.0006; Table 1). VMAT and hybrid VMAT compared to hybrid IMRT delivered greater mean dose to the infraspinatus, latissimus dorsi, subscapularis, supraspinatus and trapezius in intact breast patients (Table 1). There were no differences between RT techniques in the mean dose delivered for post-mastectomy chest wall patients for any of the muscles (all p > 0.0006; Supplementary Table 1).
The mean dose (Gy) and the percentage volume (%) of each shoulder muscle that received V15 and V30 Gy of radiation when hybrid IMRT, wedged field, VMAT and hybrid VMAT were used for the intact breast. Values in brackets indicate range. An asterisk (*) in the table indicates significant differences (p < 0.0006) compared to hybrid IMRT. Not applicable in the statistical significance column indicates that the statistical tests were not performed because the mean dose, V15 Gy dose or V30 Gy dose for one or more techniques were equal to 0. h-IMRT: hybrid IMRT; h-VMAT: hybrid VMAT

Muscle volume
The volume of the pectoralis major (∼43–45% at V15 Gy and ∼35–40% at V30 Gy) and pectoralis minor (∼59–65% at V15 Gy and ∼50–60% at V30 Gy) exposed to V15 Gy and V30 Gy radiation did not significantly differ between RT techniques (all p > 0.0006; Figure 3). Notably, the pectoralis minor remained substantially affected by moderate to high radiation doses (up to 55% at V35 Gy and 17% at V40 Gy; Supplementary Table 2). For other muscles, only the latissimus dorsi was significantly more exposed to V15 Gy when VMAT was used compared to the hybrid IMRT (Z = −3.62, p = 0.0002; Figure 2), but not to V30 Gy. Additionally, there were no significant differences between RT techniques in the muscle volume exposed to V15 Gy and V30 Gy for the remaining posterior muscles (all p > 0.0006; Table 1). Data for the percentage muscle volume receiving 5 Gy to 40 Gy can be found in Supplementary Table 2.
Mean dose–volume histograms for eight shoulder muscles across four different RT techniques in intact breast patients. Each histogram depicts four mean dose–volume lines illustrating the radiation dose distribution for a specific muscle by RT technique. A line at 15 Gy signifies a dose that was previously linked with arm dysfunction.
The impact of the 3-field supraclavicular technique
Mean dose
When a 3-field supraclavicular technique was used to treat the lymph nodes, all muscles received more radiation dose (Supplementary Table 3). The pectoralis major, the pectoralis minor and the supraspinatus received the highest mean dose.
Muscle volume
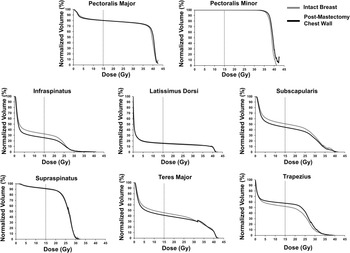
Approximately 76–80% of the pectoralis major and ∼100% of the pectoralis minor were exposed to V15 Gy and V30 Gy with the 3-field supraclavicular technique (Figure 4). Muscles which were substantially exposed to V15 Gy also included the subscapularis (∼45–51%), supraspinatus (∼92%) and trapezius (∼52–58%) (Supplementary Table 3). Regarding V30 Gy, about 26% of the subscapularis, 32% of the teres major and ∼10% of the trapezius received this dose. About 67 to 91% of the supraspinatus muscle volume was exposed to moderate doses of radiation (V15 to V25) (Figure 4).
Mean dose–volume histograms for eight shoulder muscles for a 3-field supraclavicular technique for intact breast and post-mastectomy chest wall patients. Each histogram depicts two mean dose–volume lines illustrating the radiation dose distribution for a specific muscle. A line at 15 Gy signifies a dose that was previously linked with arm dysfunction. Note the DVH for the pectoralis minor and the supraspinatus.

The impact of patient positioning
Mean dose
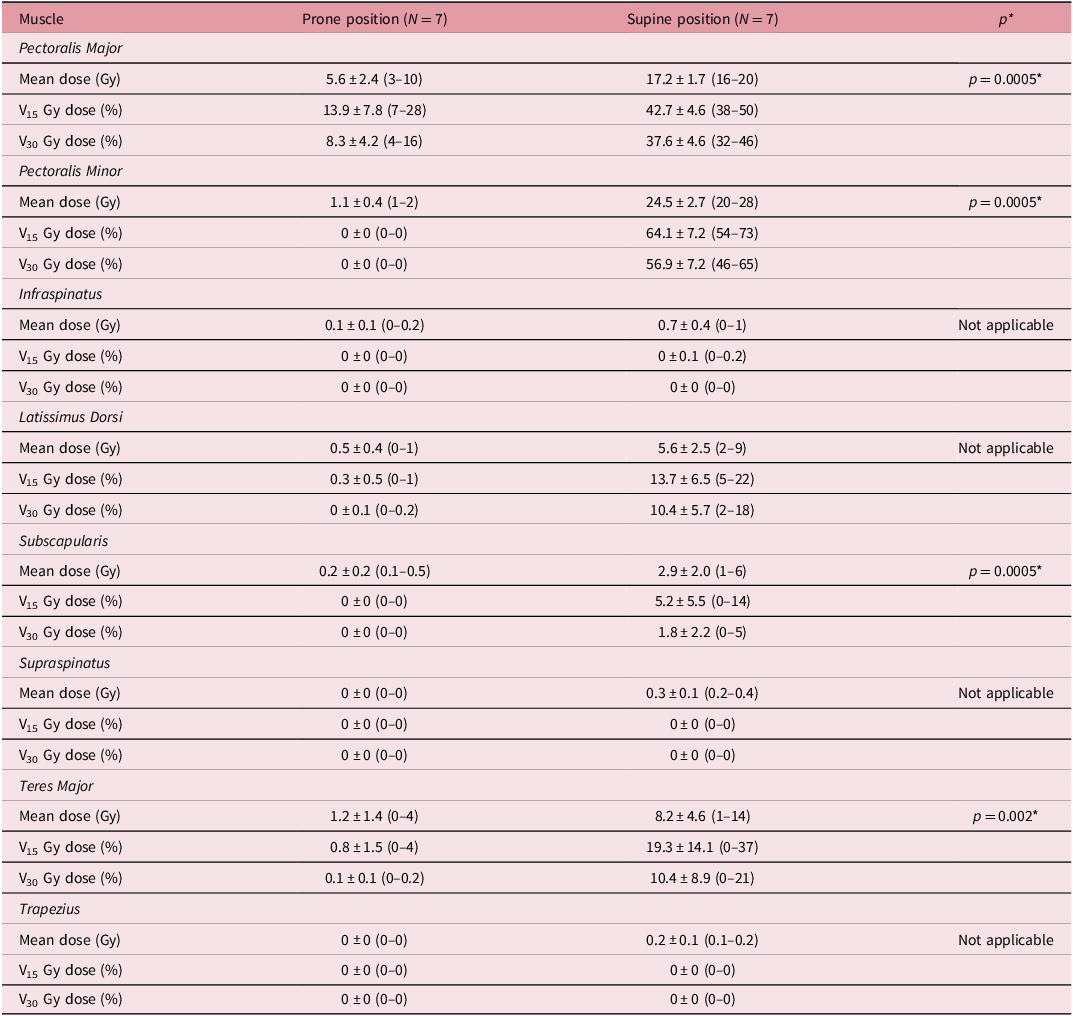
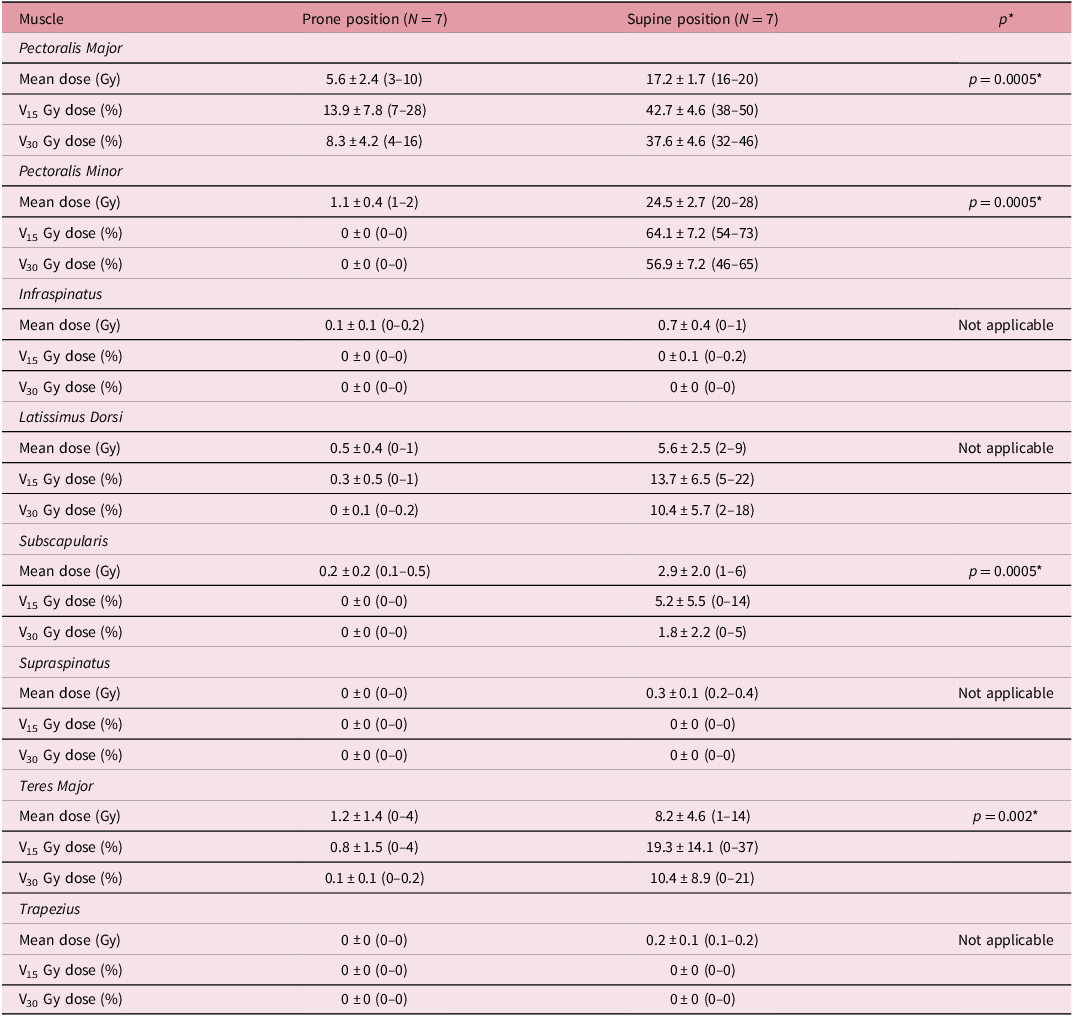
The mean dose delivered to all shoulder muscles was significantly less when RT was delivered in the prone compared to the supine position (Table 2).
The mean dose (Gy) and the percentage volume (%) of each shoulder muscle that received V15 and V30 Gy of radiation when patients are treated in the prone versus the supine position. Values in brackets represent a range. An asterisk (*) in the table indicates significant differences (p < 0.006) between the prone and the supine position. Not applicable in the statistical significance column indicates that the statistical tests were not performed because the mean dose was equal to 0 Gy for one of the positions
Muscle volume
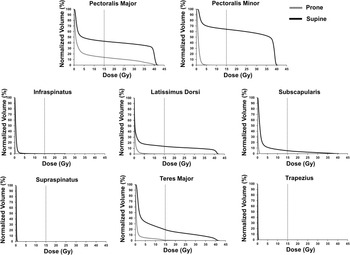
When RT was delivered in the prone position, the muscle volume exposed to V15 Gy and V30 Gy was smaller for the pectoralis major, pectoralis minor, latissimus dorsi, subscapularis and teres major (Figure 5). Data for the percentage muscle volume receiving 5 Gy to 40 Gy can be found in Supplementary Table 4.
Mean dose–volume histograms for eight shoulder muscles, comparing RT treatment delivered in the prone versus the supine position. Each histogram depicts two mean dose–volume lines illustrating how patient position affects a specific muscle. A line at 15 Gy signifies a dose that was previously linked with arm dysfunction.

Discussion
RT is a highly effective breast cancer treatment. As survival rates increase, it becomes increasingly important to address the cumulative effects of RT on healthy tissues, Reference Leonardis, Lulic-Kuryllo and Lipps18 which can be impacted by treatment field design. Reference Lipps, Sachdev and Streuss12 To our knowledge, our study is the first to compare the amount of radiation delivered to the shoulder muscles with common, clinically used RT techniques. We show that hybrid VMAT and VMAT deliver more radiation to the posterior shoulder muscles compared to hybrid IMRT, though overall exposure is generally low for these muscles. Furthermore, the 3-field supraclavicular RT results in greater muscle volume exposure to V15 Gy specifically for the pectoralis major, pectoralis minor and supraspinatus. Lastly, the amount of radiation delivered to the shoulder muscles in the prone position is significantly lower compared to the supine position. These findings provide critical new insights into the extent of shoulder muscle exposure to radiation when common RT techniques are used, informing treatment planning decisions to mitigate shoulder morbidity.
Our primary hypothesis that hybrid IMRT would result in less shoulder muscle radiation exposure compared to the wedged field, VMAT and hybrid VMAT techniques was not supported for the anterior muscles. We found that the pectoralis major and pectoralis minor are exposed to moderate doses of radiation irrespective of the RT technique used. This finding is clinically significant because moderate radiation doses to the pectoralis major are associated with increased muscle stiffness, decreased muscle thickness Reference Wolfram, Takayesu and Pierce8 and significant arm impairments. Reference Bazan, DiCostanzo and Hock11 In situ research indicates that irradiation elicits long-term muscle damage, including aberrant gene expression, increased apoptosis and immune cell infiltration. Reference Wallner, Drysch and Hahn19 As the three distinct regions of pectoralis major are vital for arm function, Reference Lulic-Kuryllo, Negro, Jiang and Dickerson20,Reference Leonardis, Desmet and Lipps21 exposure may result in strength and range of motion limitations impacting arm adduction, internal rotation, flexion or extension. Reference Johansen, Fossa, Nesvold and Fossä2,Reference Bazan, DiCostanzo and Hock11,Reference Fadavi, Arefpour and Beigi14,Reference Maciukiewicz, Hussein and Mourtzakis22
While previous work primarily focused on the effects of radiation on pectoralis major function, Reference Wolfram, Takayesu and Pierce8,Reference Lulic-Kuryllo, Leonardis, Momoh and Lipps9,Reference Wallner, Drysch and Hahn19,Reference Lipps, Leonardis and Dess23–Reference Seo, Hwang and Lee25 our data show that the pectoralis minor is also consistently exposed. Approximately half to three-quarters of this muscle, which is critical in scapular stabilisation and inspiration, received moderate to high doses of radiation with every technique. Although the pectoralis minor is known to atrophy post-treatment, Reference Shamley, Stinanaganathan and Weatherall24 a direct link between radiation exposure and subsequent scapular dysfunction Reference Acet, Guzel and Keser26,Reference Shamley, Srinaganathan and Oskrochi27 remains unclear.
The exposed volume for the posterior shoulder muscles did not differ between the four RT techniques, with the exception of the latissimus dorsi. Specifically, latissimus dorsi exposure during VMAT was more than double that of hybrid IMRT. Since the latissimus dorsi and the pectoralis major have overlapping lines of action, this dual exposure (pectoralis major ∼44% and latissimus dorsi ∼30%) could potentially lead to limitations in internal rotation and adduction previously reported. Reference Fadavi, Arefpour and Beigi14
Finally, in partial support of our hypothesis, hybrid IMRT delivered less radiation to the posterior shoulder muscles compared to hybrid VMAT and VMAT (except for the teres major). However, the mean dose delivered with hybrid VMAT and VMAT to all posterior shoulder muscles remained below 15 Gy. Therefore, this finding is likely not clinically significant, as delivery of 15 Gy or more is currently considered a threshold for development of shoulder morbidity. Reference Johansen, Fossa, Nesvold and Fossä2
Our second hypothesis that using the 3-field supraclavicular technique would increase shoulder muscle exposure to radiation was supported. Using the 3-field supraclavicular technique resulted in a greater mean dose and muscle volume receiving moderate-to-high doses of radiation. Reference Bazan, DiCostanzo and Hock11,Reference Lipps, Sachdev and Streuss12 Moreover, using the 3-field supraclavicular technique resulted in 100% of the pectoralis minor and about 80% of the pectoralis major exposed to moderate-to-high doses of radiation. These findings underscore that the anterior shoulder muscles are substantially more exposed to radiation when a 3-field supraclavicular technique is used.
Posterior shoulder muscles also received a greater radiation dose when the 3-field supraclavicular RT was used. The subscapularis, supraspinatus, teres major and trapezius all received 15 Gy or more, increasing the potential for greater dysfunction. Notably, 60% to 96% of the supraspinatus muscle was consistently exposed to low-to-moderate doses. The supraspinatus is a critical rotator cuff muscle for initiating arm abduction and stabilising the glenohumeral joint. Since rotator cuff pathology often originates in the supraspinatus tendon, Reference Kim, Nirvikar and Teefey28 this finding suggests that 3-field supraclavicular RT may compromise its function, potentially leading to subacromial impingement and rotator cuff dysfunction following treatment. Reference Gala-Alarcon, Prieto-Gomez and Bailon-Cerezo29,Reference Wolfram, Herriman and Lipps30 Collectively, these findings suggest that patients treated with the 3-field supraclavicular technique may require more frequent monitoring for shoulder morbidity, though longitudinal studies are needed to confirm the long-term clinical consequences.
Lastly, delivery of RT in the prone position significantly lowered the mean dose to the shoulder muscles, with most muscles receiving almost no radiation. Exposure to the pectoralis major was minimal, with the mean dose well below 15 Gy and only about 14% of the muscle volume was at risk of receiving V15 Gy. Since the prone position also reduces doses to OARs Reference Lai, Zhong and Deng31 and decreases acute toxic effects, Reference Vesperini, Davidson and Bosnic32 this patient position should be used whenever clinically appropriate to spare musculoskeletal structures.
This study has several limitations. First, we did not perform a longitudinal study to investigate functional and patient-reported outcomes associated with radiation dose or exposed muscle volume. Future studies are needed to determine threshold dose that impairs muscle function. Second, our analysis of the prone position was limited to a small sample size, because delivery of radiation in the prone position is not commonly used at our cancer centre. However, the amount of radiation delivered to the shoulder muscles in the prone position was highly consistent among the included patients.
Conclusion
This study reports shoulder muscle-specific data for the most commonly used RT techniques in clinical practice and lays the foundation for a better understanding of radiation exposure to healthy musculoskeletal structures during breast RT. Our findings highlight that using a 3-field supraclavicular technique substantially increases the dose to both anterior (pectoralis major and minor) and posterior shoulder muscles. The association between the dose delivered by these techniques and long-term shoulder morbidity should be explored in future investigations. Conversely, the use of novel techniques such as hybrid VMAT and VMAT may expose the posterior shoulder muscles to more radiation. However, the amount delivered and percentage of muscle volume exposed may not be clinically meaningful. Lastly, delivering RT in the prone position can spare the shoulder muscles. Therefore, the benefits of delivering RT in the prone position to spare the musculoskeletal structures should be further explored.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1460396925100332.
Competing interests
The authors have no financial or personal relationships with other people or organisations that could inappropriately influence the submitted manuscript.
Ethical consideration
This study has been reviewed and approved by the Waterloo Wellington Research Ethics Board (WWREB #2023-0762) and was conducted in accordance with the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective analysis of anonymised clinical data.




 Open access
Open access