


Introduction
The number of forcibly displaced people continues to rise, with 45 million refugees and asylum-seekers worldwide. These people experience prolonged human rights violations, exposure to multiple traumatic events, and persistent daily stressors, as documented across diverse contexts and over decades (Steel et al., Reference Steel, Chey, Silove, Marnane, Bryant and van Ommeren2009; Hou et al., Reference Hou, Liu, Liang, Ho, Kim, Seong, Bonanno, Hobfoll and Hall2020; Sisenop et al., Reference Sisenop, Chatarajupalli, Bain, Kaade and Lindert2025). Such experiences increase the risk of developing mental health problems (Blackmore et al., Reference Blackmore, Boyle, Fazel, Ranasinha, Gray, Fitzgerald, Misso and Gibson-Helm2020). Forced displacement also erodes the social fabric of societies and disrupts social networks, relationships and resources (Ager and Strang, Reference Ager and Strang2008; Silove, Reference Silove2013; Strang and Quinn, Reference Strang and Quinn2021). Despite the importance of these social sequela, research and practice among those forcibly displaced have largely focused on mental health outcomes, with limited attention to social functioning as a central component of well-being and psychosocial adaptation.
Several theoretical models have been developed to elucidate the link between stressors related to conflict and forced displacement, and the mental health of forcibly displaced populations. Among these, the ecological model of refugee distress developed by Miller and Rasmussen has gained increasing attention since its initial introduction in 2010 (Miller and Rasmussen, Reference Miller and Rasmussen2010) and subsequent iteration in 2017 (Miller and Rasmussen, Reference Miller and Rasmussen2017). This model posits that both conflict-related traumatic events and socio-environmental stressors following post-conflict and forced-displacement adversely impact mental health. As conflict and war often cause or exacerbate socio-environmental stressors encountered in daily life, these experiences exert their influence on mental health both directly and indirectly through these stressors. Given its simplicity and explanatory power, the ecological model has been the focus of considerable scientific inquiry over the past decade (Miller and Rasmussen, Reference Miller and Rasmussen2024) and has received substantial empirical support (e.g., Hou et al., Reference Hou, Liu, Liang, Ho, Kim, Seong, Bonanno, Hobfoll and Hall2020; Dangmann et al., Reference Dangmann, Solberg and Andersen2021; Goodkind et al., Reference Goodkind, Ferrera, Lardier, Hess and Greene2021; EL-Awad et al., Reference EL-Awad, Eves, Hachenberger, Bozorgmehr, Entringer, Hecker, Razum, Sauzet and Lemola2025). Studies consistently demonstrated that both conflict-related traumatic events and stressors in post-displacement settings, whether in resettlement contexts or during transit, significantly predict increased mental health problems, with post-displacement stressors showing overall stronger association than traumatic experiences (Hou et al., Reference Hou, Liu, Liang, Ho, Kim, Seong, Bonanno, Hobfoll and Hall2020). Although the later version of the model has been expanded to family functioning, such as parenting and parental mental health, it remained largely focused on understanding the predictors and consequences of poor mental health among conflict-affected populations. While this model has substantially advanced our understanding of conflict- and displacement-driven mental health problems, it represents only one aspect of psychosocial adaptation following such experiences.
Social functioning – the ability to form and maintain meaningful relationships and engage in social activities (Bosc, Reference Bosc2000; Hirschfeld et al., Reference Hirschfeld, Montgomery, Keller, Kasper, Schatzberg, Möller, Healy, Baldwin, Humble, Versiani, Montenegro and Bourgeois2000) is an important yet often underexplored dimension of adaptation and well-being in conflict-affected populations (Ager and Strang, Reference Ager and Strang2008; Lahiri et al., Reference Lahiri, van Ommeren and Roberts2017). Social functioning is closely related to mental health, as mental health difficulties are often accompanied by impairments in social functioning in both general (Scoglio et al., Reference Scoglio, Reilly, Girouard, Quigley, Carnes and Kelly2022) and conflict-affected populations (Kurt et al., Reference Kurt, Ekhtiari, Ventevogel, Ersahin, Ilkkursun, Akbiyik and Acarturk2023; Nickerson et al., Reference Nickerson, Kurt, Liddell, Keegan, Nandyatama, Yuanita, Argadianti Rachmah, Hoffman, Kashyap, Mastrogiovanni, Mai, Camilleri, Susanty, Tricesaria, Rostami, Im, Gurzeda, Khakbaz, Funnell, Pestalozzi and Specker2025). Yet, social functioning represents a distinct construct that extends beyond mental health symptoms, and difficulties in social functioning often persist even after mental health symptoms have subsided (Scoglio et al., Reference Scoglio, Reilly, Girouard, Quigley, Carnes and Kelly2022; Kupferberg and Hasler, Reference Kupferberg and Hasler2023). Improved social functioning, is often considered among the key recovery goals following adversities and mental health problems (Vera San Juan et al., Reference Vera San Juan, Gronholm, Heslin, Lawrence, Bain, Okuma and Evans-Lacko2021; Guerrero et al., Reference Guerrero, Barrios, Sampietro, Aza, Gómez-Benito and Guilera2024). For conflict-affected people, especially for refugees and asylum-seekers, social functioning is key to successful integration and psychosocial adaptation (Strang and Quinn, Reference Strang and Quinn2021). However, existing evidence on social functioning is scant, with most research relying on cross-sectional designs. A recent systematic review of 38 studies found that the majority of evidence supports the adverse impact of conflict-related traumatic events on social functioning, but some studies show that these experiences might also lead to increased social functioning outcomes, including greater participation in community and cultural groups and more frequent interaction with others (Perkins et al. Reference Perkins, Michalek, Dikomitis, Shergill and Mareschal2025). Further, other studies indicated that stressors encountered in forced displacement contexts likely impair social functioning (Wachter et al., Reference Wachter, Heffron, Snyder, Nsonwu and Busch-Armendariz2016; Steel et al., Reference Steel, Dunlavy, Harding and Theorell2017; Nguyen et al., Reference Nguyen, Al Asaad, Sena and Slewa-Younan2024). Despite evidence supporting the role of both conflict- and displacement-related factors for social functioning, no study to date has examined these factors together through the proposed direct and indirect pathways in Miller and Rasmussen’s model (Miller and Rasmussen, Reference Miller and Rasmussen2017), in relation to social functioning within the same model as mental health.
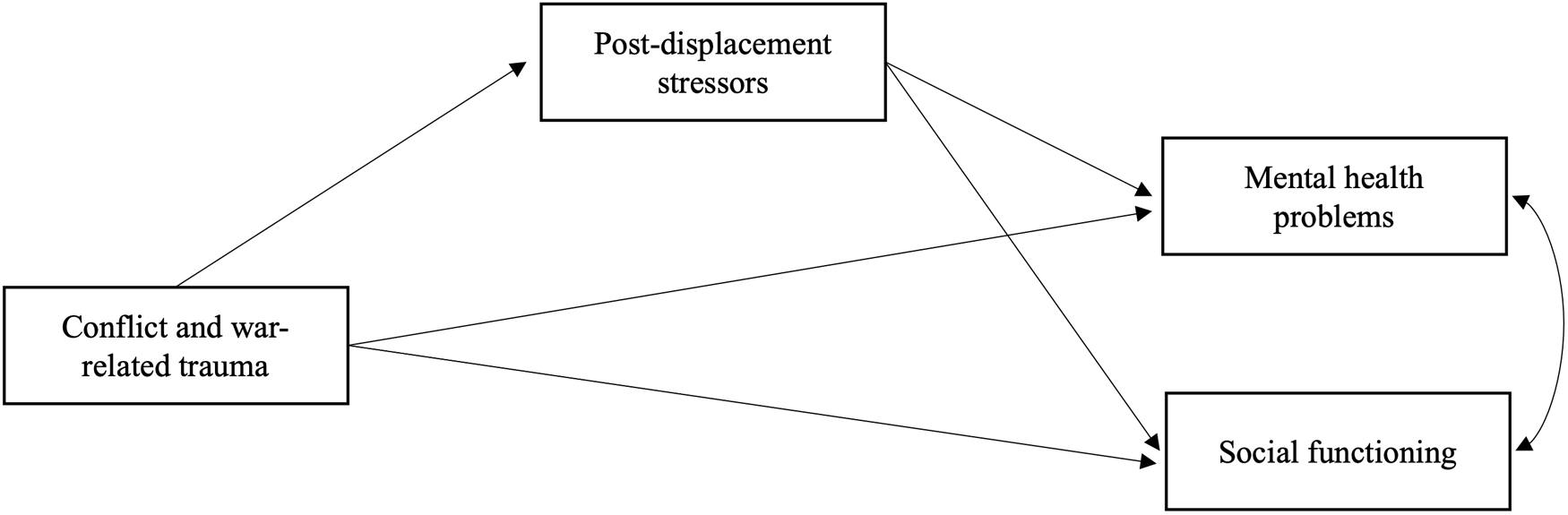
The present study aimed to longitudinally test the ecological model of distress in relation to social functioning among refugees and asylum seekers in Indonesia, to identify similarities and differences between the determinants of mental health and social functioning. Consistent with the ecological model, we hypothesized that there would be direct pathways from conflict-related traumatic events and post-displacement stressors to mental health outcomes as well as an indirect pathway from traumatic events to mental health via post-displacement stressors. Given emerging but still limited evidence on the potential dual role of conflict-related traumatic experiences for social functioning, we explored whether there would be a direct pathway from conflict-related traumatic events to social functioning without specifying the direction. Drawing from the established literature, we hypothesized that traumatic events would predict greater post-displacement stressors, which would in turn predict poorer social functioning. The extended ecological model for social functioning is depicted in Figure 1.
The extended ecological model of refugee distress to social functioning.

Methods
Participants and study design
This study used data from the first and third waves of a large-scale longitudinal study conducted with refugees and asylum-seekers in Indonesia between 2020 and 2022. The first wave (Time 1) was collected between February and October 2020, and the third wave (Time 3) was collected 12 months after the completion of Time 1. Participants were recruited through refugee services, community-based organizations in Jakarta and Bogor, Indonesia, and social media. Eligibility criteria were: (1) being a refugee or asylum seeker in Indonesia, (2) having arrived in Indonesia after January 2013, (3) being at least 18 years old and (4) being literate in one of the following languages representing the majority of refugees at the time of the study: Arabic, Farsi, Dari, Somali or English. Participants completed a self-administered online survey (approximately 1 hour) at each wave. The trained research assistants provided technical support when needed. Participants were compensated with an online grocery voucher of USD 7 (IDR 100,000) for their participation. Ethical approval was obtained from the UNSW Human Research Ethics Committee (HC190494) and Atma Jaya University, Jakarta (0792/III/LPPM-PM.10.05/07/2019).
Measures
All measures were translated and blind back-translated following a rigorous translation process by accredited translators. Refugee community members with varying levels of education pilot-tested the translated survey battery to assess comprehension and clarity.
Conflict-related traumatic events
Items from the Harvard Trauma Questionnaire (16 items; Mollica et al., Reference Mollica, Caspi-Yavin, Bollini, Truong, Tor and Lavelle1992) with additional three items (natural disaster, physical assault, and serious accident, fire or explosion) were used to assess potentially traumatic experiences related to war and conflict that participants had either directly experienced or witnessed in the past, using categorical response options (0 = No, 1 = Yes). A sum score indicating the number of distinct traumatic events (experienced and/or witnessed) endorsed was used to represent the diversity of conflict-related traumatic experiences in this study.
Post-displacement stressors
An adapted version of the Post-migration Living Difficulties Checklist (Steel et al., Reference Steel, Silove, Bird, McGorry and Mohan1999) was used to measure the stressors that participants experienced in their daily lives in Indonesia in the past 12 months. Forty-two items were presented to the participants to rate on a 5-point Likert Scale (1 = was not problem/did not happen, 5 = a very serious problem). The mean score of the overall items was used in the study. The Cronbach’s alpha was 0.96 in this study.
Mental health outcomes
Depression symptoms were measured using the Patient Health Questionnaire-8 items (PHQ-8; Kroenke et al., Reference Kroenke, Strine, Spitzer, Williams, Berry and Mokdad2009). Participants indicated how much they had been bothered by each item on a 4-point Likert scale (1 = not at all, 4 = nearly every day). The mean score across items was used in this study (α = 0.93). An adapted version of the Posttraumatic Diagnostic Scale for DSM-IV (Foa et al., Reference Foa, Cashman, Jaycox and Perry1997) was used to measure the symptoms of posttraumatic stress disorder. Four items reflecting the revised PTSD symptoms in DSW-5 were added to the original 16 items. Participants were asked to report how often each PTSD symptom bothered them over the past month on a 4-point Likert Scale (0 = not at all/only once, 3 = 5+ times a week/almost always). The mean score across 20 items was used in this study (α = 0.96). Anger symptoms were measured with the 5-item Dimensions of Anger Reactions Scale (Forbes et al., Reference Forbes, Alkemade, Mitchell, Elhai, McHugh, Bates, Novaco, Bryant and Lewis2014) rated on a 5-point Likert Scale (1 = none or almost none of the time, 5 = all or almost all of the time). The mean score of the items was used in this study (α = 0.92).
Social functioning
Social functioning was assessed using three items from the Short Social Capital Assessment Tool (De Silva et al., Reference De Silva, Harpham, Tuan, Bartolini, Penny and Huttly2006). These items covered different behavioural aspects of social functioning: Active group membership was indexed by the number of groups in which participants were active members over the past 12 months, out of seven group types (community groups, women’s groups, men’s groups, religious groups, sports groups, student groups, volunteer/charity groups). Support received from groups was indexed by the number of groups from which participants received emotional or economic assistance over the past 12 months, out of 12 groups (community groups, women’s groups, men’s groups, religious groups, sports groups, student groups, volunteer/charity groups, charitable organizations, refugee community groups and Indonesian community groups) Support received from individuals was indexed by the number of types of individuals from whom participants received emotional or economic assistance over the past 12 months, out of 14 categories (family, neighbours, friends, community leaders, politicians, religious leaders, government officials, charitable organizations, volunteers, refugees from one’s own community, refugees from other communities, members of the Indonesian community, non-refugees from other communities, and advocates).
Each item represents a count variable indicating the number of categories endorsed by the participants. A total social functioning score was calculated by summing these items. These items are shown as culturally meaningful and comparable behavioural indicators of social functioning across diverse settings (De Silva et al., Reference De Silva, Harpham, Tuan, Bartolini, Penny and Huttly2006, Reference De Silva, Huttly, Harpham and Kenward2007) and have been used in prior research with refugees (Nickerson et al., Reference Nickerson, Byrow, O’Donnell, Mau, McMahon, Pajak, Li, Hamilton, Minihan, Liu, Bryant, Berle and Liddell2019).
Demographic variables
Key demographic information, such as age, gender, language, time spent in Indonesia and separating from family (having no family member vs. all or some family member in Indonesia), was collected.
Data analysis
We used a longitudinal structural equation modelling in Mplus Version 8.2 (Muthen and Muthen, Reference Muthen and Muthen2023) to test the associations between diversity of conflict-related traumatic experiences, post-displacement stressors, and mental health and social functioning outcomes. Following a two-step approach, we first conducted Confirmatory Factor Analysis (CFA) using the mean scores of the symptoms of PTSD, depression, and anger at T3 to form a latent variable of mental health problems. Then, we tested our hypothesized mediation model using the diversity of conflict-related traumatic events before arrival in Indonesia measured at T1, post-displacement stressors in the past 12 months measured at T1, the latent variable of mental health problems at T3, and the observed variable of social functioning at T3. Social functioning was treated as an observed variable because it comprises behaviourally anchored indicators that reflect directly observable actions rather than an underlying latent construct. This analytical approach aligns with the conceptualization of social functioning as enacted behaviour (De Silva et al., Reference De Silva, Huttly, Harpham and Kenward2007; Baumgartner and Susser, Reference Baumgartner and Susser2013; Lahiri et al., Reference Lahiri, van Ommeren and Roberts2017).
We estimated direct paths from the diversity of conflict-related traumatic events and post-displacement stressors to mental health and social functioning, as well as indirect paths from traumatic experiences via post-displacement stressors to these outcomes. The significance of the indirect predictor role of diversity of conflict-related traumatic events on mental health and social functioning outcomes via post-displacement stressors was tested using the bootstrapping technique (1000 resampling) (MacKinnon et al., Reference MacKinnon, Fairchild and Fritz2007). Exploratory post hoc analyses were conducted examining group membership and support received from individuals and groups as separate social functioning outcome variables. The model controlled for age, gender, separation from family, time in Indonesia, and language groups (as a proxy for country of origin). Model fit was evaluated using the following indices: Comparative Fit Index (CFI) > 0.90, Root Mean Square Error of Approximation (RMSEA) < 0.08 with 90% CI and Standardized Root Mean Square Residual (SRMR) < 0.08 (MacCallum et al., Reference MacCallum, Browne and Sugawara1996; Brown, Reference Brown2015; Kline, Reference Kline2023). Full information maximum likelihood (FIML) estimation was used to account for missing data on endogenous variables, which represented the focal variables in the model, including missing outcome data at Time 3 due to attrition. This approach allows all available data to contribute to model estimation under the assumption that data are missing at random. The rate of missing data on exogenous variables was less than 5%; therefore, no imputation of these variables was conducted.
Results
Participants
A total of 1235 participants completed Time 1 with an average age of 30.53 (SD = 9.067). The majority of the sample was male (71.4%) and were from Farsi/Dari speaking backgrounds (39.4%) followed by Arabic (30.3%), English (17.5%) and Somali (12.9%). The average length of stay in Indonesia was 5.11 years (SD = 1.618). Half of the participants (53.5%) reported having no immediate family member in Indonesia. The average number of conflict-related traumatic experiences is 7.73 (SD = 5.03) with ill health without access to healthcare (59%), lack of food or water (58.7%), lack of shelter (52.8%) reported as the most common experiences. The mean of post-displacement stressors was 2.81 (SD = 0.86), with the most common issues being difficulties related to work and money, fear of being sent back to the home country, and worries about visa status. The full list of traumatic events and post-displacement stressors is given in Supplementary Material.
A total of 62.5% of the sample (N = 772) completed Time 3. There were no significant differences between participants who completed both Time 1 and Time 3 and those who completed only Time 1 in terms of gender (χ2(1) = 2.26, p = 0.133), age (t(1230) = 1.18, p = 0.240), diversity of conflict-related traumatic experiences (t(1010) = 0.51, p = 0.609), mean of post-displacement stressors reported (t(722) = 1.82, p = 0.069), initial level of social functioning (t(1120) = −0.53, p = 0.601), and symptoms of depression (t(1166) = 0.95, p = 0.341) and PTSD (t(1023) = −1.10, p = 0.271). On the other hand, those who completed both time points had been in Indonesia longer (t(1230) = 7.55, p < 0.001) and reported a lower level of anger symptoms (t(1162) = −2.25, p = 0.025) than those who completed only the Time 1 survey. Compared with participants who completed only the Time 1 survey, those who completed both time points were more likely to complete the surveys in Dari (χ2(1) = 6.35, p = 0.012) and Farsi (χ2(1) = 5.72, p = 0.017) and less likely in English (χ2(1) = 13.82, p < 0.001), than Arabic. After applying Bonferroni correction to account for multiple group comparisons, none of these observed differences remained significant.
Measurement model
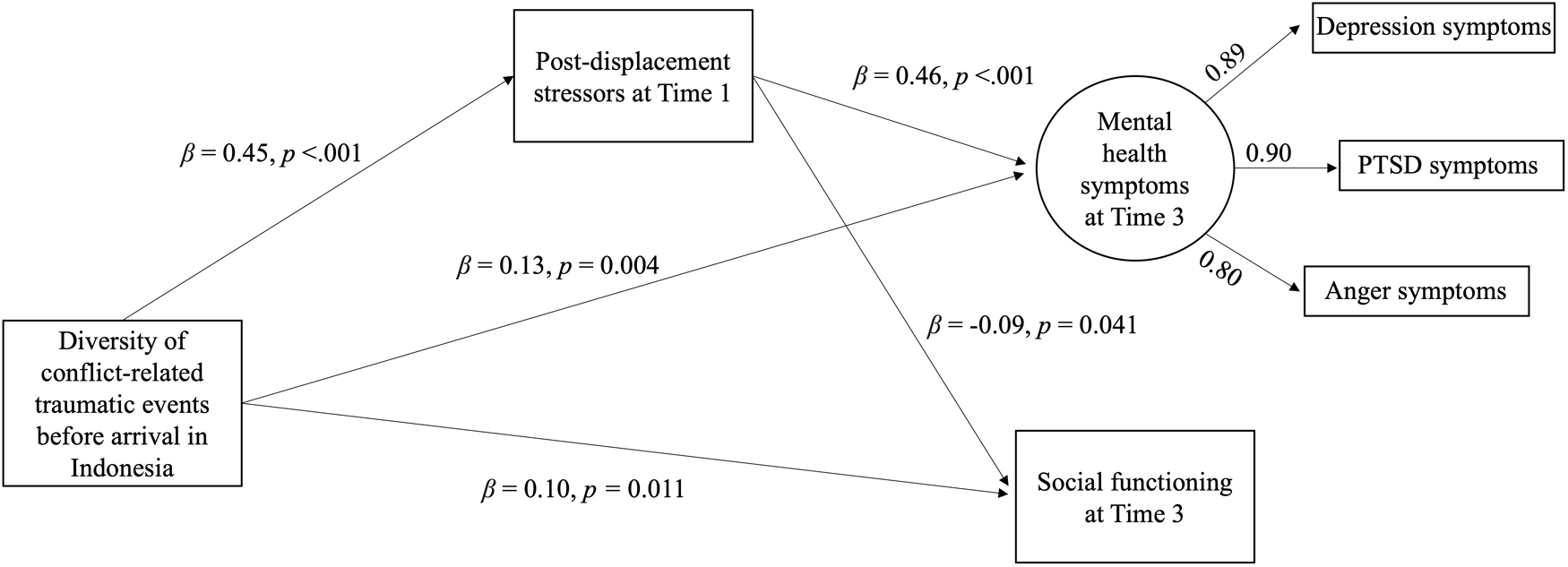
CFA yielded an overall good model fit for mental health as a latent variable (CFI = 1.00, RMSEA = 0.01, SRMR = 0.02) indexed by mean symptoms of PTSD, depression, and anger. The model was just identified with factor loadings of 0.89 for depression, 0.90 for PTSD, and 0.80 for anger, indicating acceptable loadings.
Structural equation model testing
Direct paths from diversity of conflict-related traumatic events and post-displacement stressors to mental health and social functioning
The model fit the data well, CFI = 0.98, TLI = 0.95, RMSEA = 0.04 (90% CI = 0.023–0.047), SRMR = 0.02. Figure 2 depicts significant standardized direct effects. Diversity of conflict-related traumatic events before arrival in Indonesia predicted greater post-displacement stressors at T1 (β = 0.45, SE = 0.03, p < 0.001). Diversity of conflict-related traumatic events and post-displacement stressors at T1 predicted greater mental health symptoms at T3 (β = 0.13, SE = 0.05, p = 0.004, β = 0.46, SE = 0.05, p < 0.001). Diversity of conflict-related traumatic events predicted better social functioning at T3 (β = 0.10, SE = 0.04, p = 0.011), while post-displacement stressors at T1 predicted worse social functioning at T3 (β = −0.09, SE = 0.04, p = 0.041).
The tested ecological model of refugee distress to social functioning.

Indirect path from the diversity of conflict-related traumatic events to the outcome variables via post-displacement stressors
The indirect associations of diversity of conflict-related traumatic events on mental health problems and social functioning via post-displacement stressors were significant (β = 0.21, 95% CI = 0.162 to 0.257, β = −0.04, 95% CI = −0.082 to −0.003). That is, diversity of conflict-related traumatic events predicted greater post-displacement stressors at T1, which, in turn, predicted greater mental health symptoms and worse social functioning at T3. Table 1 includes the full list of standardized coefficients for direct and indirect paths.
Standardized direct and indirect paths

a Confidence intervals of standardized results are report. LLCI: lower-level confidence interval; ULCI: upper-level confidence interval; CTE: conflict-related traumatic experiences; PDS: post-displacement stressors; MH: mental health symptoms; SocialF: social functioning.
Exploratory post hoc analyses examining active group membership and support received from individuals and groups as separate social functioning outcomes indicated similar patterns of association, with statistical significance observed only for active group membership (see Supplementary Material for details).
Discussion
In the present study, we longitudinally tested an extension of the ecological model of distress to social functioning in a sample of culturally and linguistically diverse refugees and asylum seekers in Indonesia. Our results accord with the established pathways from diversity of conflict-related traumatic experiences and post-displacement stressors to mental health, while highlighting both shared and unique associations for social functioning. The findings provide the first empirical evidence that social functioning is distinctly predicted by conflict- and displacement-related stressors.
Consistent with prior research (Steel et al., Reference Steel, Chey, Silove, Marnane, Bryant and van Ommeren2009) and our hypotheses, we found that greater diversity of conflict-related traumatic experiences predicted greater mental health problems via both direct and indirect pathways. These experiences were associated with greater post-displacement stressors in the past year, which, in turn, predicted higher levels of mental health problems 1 year later. The observed longitudinal pathways for mental health align with the accumulated evidence for the ecological model of distress and contribute to the relatively sparse longitudinal research in this area (Miller and Rasmussen, Reference Miller and Rasmussen2024). Further, the results revealed a dual pathway from conflict-related traumatic events to social functioning. That is, experiencing diverse conflict and war-related traumatic events before arrival in Indonesia (such as imprisonment, loss of loved ones, and deprivation of basic needs) was directly associated with greater social functioning, operationalized as greater engagement with and support from groups and individuals. In contrast, exposure to these traumatic events was also indirectly associated with worse social functioning over time via greater post-displacement stressors. These findings are particularly novel as they suggest that diversity of conflict-related traumatic experiences can have dual influences on social functioning, largely shaped by the post-displacement context.
The dual pathway from diversity of conflict-related traumatic events to social functioning might reflect distinct underlying processes. Regarding the pathway by which trauma exposure is associated with greater social functioning, experiencing traumatic events such as losing loved ones may motivate individuals to interact more with others and seek resources and support to restore connections disrupted by trauma (Posselt et al., Reference Posselt, Eaton, Ferguson, Keegan and Procter2019; Matos et al., Reference Matos, Costa, Park, Indart and Leal2021). To do so, they might engage in social activities, such as participating in social and community groups and seeking social support from other individuals and the groups that they are part of (Nickerson et al., Reference Nickerson, Byrow, O’Donnell, Mau, McMahon, Pajak, Li, Hamilton, Minihan, Liu, Bryant, Berle and Liddell2019; Frounfelker et al., Reference Frounfelker, Mishra, Dhesi, Gautam, Adhikari and Betancourt2020). Emerging evidence supports this notion, showing that experiences of diverse conflict-related events can be associated with increased participation in social groups, greater support from close others, and more engagement with the host culture (Perkins et al. Reference Perkins, Michalek, Dikomitis, Shergill and Mareschal2025). At the same time, the indirect pathway whereby the same conflict-related traumatic events predicted poorer social functioning through higher post-displacement stressors indicates the possibility of more than one behavioural route, shaped by the degree or type of contextual stress. One potential direct pathway may occur via increased motivation to approach others, while a second pathway may occur through the accumulation of post-displacement stressors that constrain behavioural engagement in social activities. This is consistent with the physiology of stress regulation, which describes the stress response as producing both mobilizing (approach) and hindering (avoidance) effects that operate non-linearly depending on the severity and duration of stress exposure to maintain equilibrium between stress exposure and one’s coping capacity (Gray, Reference Gray and Pawlik1984; Kasch et al., Reference Kasch, Rottenberg, Arnow and Gotlib2002; McEwen, Reference McEwen2007). Thus, in our case, exposure to diverse conflict-related trauma might activate behavioural approach systems to restore needs for connection and belonging, while greater chronic exposure to post-displacement stressors might engage inhibitory processes that reduce social engagement. These parallel processes can explain the dual pattern of associations with trauma observed in our study. This interpretation is further supported by exploratory analyses showing that these dual pathways were statistically more robust for active group membership than for support received from individuals and groups. The latter may be more directly influenced by the availability of support within social networks, whereas the former reflects behavioural engagement that individuals can initiate to seek support depending on the circumstances in their settings.
It is important to interpret the current findings within the broader structural context in which this study was conducted. In Indonesia, asylum-seeking claims are only processed by UNHCR as the country is not a signatory to the Refugee Convention and its protocol. This often means that individuals seeking asylum must wait for years without access to formal employment and limited access to health care and education (Amin, Reference Amin2022; Curby, N 20 October Curby, Reference Curby2020). Thus, systemic injustices, insecurity, and financial hardships pose significant structural barriers that preclude these individuals’ meaningful participation in social life (Ager and Strang, Reference Ager and Strang2008; Niemi et al., Reference Niemi, Manhica, Gunnarsson, Ståhle, Larsson and Saboonchi2019). In the absence of supportive legal and social structures, refugees and asylum seekers are presented with limited opportunities to engage in social activities (Niemi et al., Reference Niemi, Manhica, Gunnarsson, Ståhle, Larsson and Saboonchi2019). This situation portrays the structural barriers and systemic exclusion of refugees from participation common across transit, low-resource settings (Hynie, Reference Hynie2018). Addressing post-displacement stressors is therefore not only critical for mental health but also for fostering social functioning.
The study findings should be interpreted within certain limitations. Firstly, we focused on the behavioural dimension of social functioning, using a brief three-item measure, indexing the number of group memberships and support received from social networks. In the social psychology literature, these behavioural indicators have been linked to health and functioning benefits, especially after significant life transitions (Iyer et al., Reference Iyer, Jetten, Tsivrikos, Postmes and Haslam2009; Cruwys et al., Reference Cruwys, Dingle, Haslam, Haslam, Jetten and Morton2013; Haslam et al., Reference Haslam, Haslam, Jetten, Cruwys and Steffens2021; Stephen et al., Reference Stephen, Muldoon Orla and Bennett Kate2021). In particular, evidence from population-based studies indicates that being a member of multiple groups can enhance quality of life and physical well-being while reducing the risk of mortality (Steffens et al., Reference Steffens, Cruwys, Haslam, Jetten and Haslam2016; Stephen et al., Reference Stephen, Muldoon Orla and Bennett Kate2021). However, these benefits typically depend on the meaning and satisfaction derived from these groups (Haslam et al., Reference Haslam, Jetten, Cruwys, Dingle and Haslam2018), consistent with evidence showing that relationship quality is as strongly, or more strongly, associated with well-being than relationship quantity (Fiorillo and Sabatini, Reference Fiorillo and Sabatini2011; Pezirkianidis et al., Reference Pezirkianidis, Galanaki, Raftopoulou, Moraitou and Stalikas2023). Accordingly, a greater number of groups or sources of support does not necessarily mean better social functioning than having a smaller number of more meaningful social connections, as behavioural engagement in structurally constrained contexts such as Indonesia may reflect needs-driven social behaviours rather than the presence of supportive, high-quality relationships. Our measure implicitly assumes linearity, treating each additional group membership or support received as conferring equally incremental benefits for social functioning. This precludes assessing the point at which additional memberships or support meaningfully contribute to social functioning or whether benefits stabilize or diminish after certain levels. As this study relied on data from an existing cohort study, employing a brief, circumscribed measure was a practical choice, in line with common practice in public health research (e.g., Hughes et al., Reference Hughes, Waite, Hawkley and Cacioppo2004; Ahmad et al., Reference Ahmad, Jhajj, Stewart, Burghardt and Bierman2014), to provide an initial empirical examination of social functioning among refugees. Yet, this still represents a limitation in assessing the depth and breadth of social functioning. Future research should incorporate additional indicators that assess both the quantity and quality of social functioning, such as satisfaction with relationships and belonging and trust in people, community and institutions. Such approaches also allow modelling profiles of social functioning to uncover potentially non-linear patterns between quantity and quality dimensions of social functioning.
Another limitation is the online nature of data collection, which enabled us to access usually hard-to-reach communities in our study. However, this may have resulted in more participation from individuals with higher digital literacy. We also used non-random sampling, which might limit the generalizability of the findings to the broader refugee population in Indonesia and beyond. Nonetheless, the large sample size and the similarity of its demographic characteristics to those of the target population at the onset of the study (United Nations High Commissioner for Refugees, 2018) support the potential validity of our findings among refugees in Indonesia. We note that our measurement of conflict-related traumatic experiences reflects the diversity of traumatic events experienced or witnessed by participants, rather than the number of traumatic incidents experienced. This approach may have limited our ability to infer about the role of cumulative trauma exposure or repeated exposure to specific types of events. However, prior research suggests that the diversity and frequency of traumatic events are correlated (Weiss et al., Reference Weiss, Brunet, Best, Metzler, Liberman, Pole, Fagan and Marmar2010; Pinto et al., Reference Pinto, Henriques, Jongenelen, Carvalho and Maia2015), particularly in settings characterized by a high risk of trauma exposure, where diversity of traumatic experiences can be as strongly or even more strongly associated with psychological symptoms (Rasmussen et al., Reference Rasmussen, Romero, Leon, Verkuilen, Morales, Martinez-Maganalles and García-Sosa2020). Nevertheless, future research should examine whether similar patterns emerge when trauma exposure is operationalized as event frequency or severity.
Despite these limitations, this study has several implications for research, practice and policy to improve overall refugee well-being and psychosocial adaptation. First, our findings contribute to the burgeoning research highlighting the distinct nature of social functioning relative to mental health among refugees and asylum seekers (Kurt et al., Reference Kurt, Ekhtiari, Ventevogel, Ersahin, Ilkkursun, Akbiyik and Acarturk2023; Nickerson et al., Reference Nickerson, Kurt, Liddell, Keegan, Nandyatama, Yuanita, Argadianti Rachmah, Hoffman, Kashyap, Mastrogiovanni, Mai, Camilleri, Susanty, Tricesaria, Rostami, Im, Gurzeda, Khakbaz, Funnell, Pestalozzi and Specker2025). For the first time, this study provides empirical evidence supporting the extension of the commonly used ecological model of distress to social functioning and illustrates the distinct pathways linking established risk factors for mental health to social functioning. These findings lay the groundwork for future research to validate similar patterns of association with diverse refugee populations in both transit and resettlement contexts, while considering potential differences based on key individual and contextual determinants (e.g., age, gender, separation from family, and duration of time in the host setting). Given the differential associations of diversity of conflict-related traumatic experiences and post-displacement stressors, examining mechanisms underpinning these associations for mental health and social functioning is necessary. We also note that the conceptual extension and empirical testing of the ecological model in this study followed the predominant approach in the literature by considering conflict- and displacement-related stressors at an aggregate level, rather than disentangling these alongside protective factors operating at different socio-ecological levels, such as policy, community and interpersonal. Given the limited attention to social functioning in refugee mental health research, this study was guided by an initial examination of the model to provide impetus for future studies to build on and expand this line of inquiry. Further research is also warranted to investigate the granularity of social functioning by focusing on multiple domains of social life, as the measure used in the present study provided an overall view of social functioning. In this regard, it may be beneficial to draw on approaches previously used to understand cultural meaning and expressions of mental health (e.g., Keys et al., Reference Keys, Kaiser, Kohrt, Khoury and Brewster2012; Ventevogel et al., Reference Ventevogel, Jordans, Reis and de Jong2013; Ventevogel and Faiz, Reference Ventevogel and Faiz2018; Kirmayer, Reference Kirmayer2025). Similar to any other construct, social functioning is socially constructed – shaped by cultural and societal values, norms and expectations. These cultural and societal factors likely determine what it means to be socially functioning well. Understanding these influences and the cultural meaning of social functioning, then, becomes crucial for defining the construct accurately, measuring it appropriately, and designing effective strategies and interventions to promote it (Miller et al., Reference Miller, Omidian, Quraishy, Quraishy, Nasiry, Nasiry, Karyar and Yaqubi2006; Ubels et al., Reference Ubels, Kinsbergen, Tolsma and Koch2022; Greene et al., Reference Greene, Ventevogel, Likindikoki, Bonz, Turner, Rees, Misinzo, Njau, Mbwambo and Tol2023).
Considering the role of conflict-related traumatic experiences and post-displacement stressors in both mental health and social functioning, our findings contribute to the call for multilevel interventions that address trauma-related difficulties while simultaneously improving socio-environmental conditions to support overall well-being and psychosocial adaptation (Miller et al., Reference Miller, Jordans, Tol and Galappatti2021; Miller and Rasmussen, Reference Miller and Rasmussen2024). There is growing evidence base on the effectiveness and acceptability of multilevel mental health and psychosocial (MHPSS) interventions (Goodkind et al., Reference Goodkind, Ferrera, Lardier, Hess and Greene2021; Moyano et al., Reference Moyano, Vergara, Mirti, Bonz, Monar, Astudillo, Vaca, Cordova, Armijos, Barroso, Cherrez, Cottle, DuBois, Capriles, Grandes, Irarrazaval, Jaramillo, Kane, Martinez-Viciana, Mascayano, Rodríguez, Schojan, Sikkema, Susser, Ventevogel, Wessells, Zambrano López, Lovero and Greene2024). Although conflict-related traumatic events present a significant risk to mental health, our result on the positive association between diversity of conflict-related traumatic experiences and social functioning highlight the potential usefulness of strategies fostering constructive meaning-making process following trauma (Pop et al., Reference Pop, Williamson, Khan, Leightley, Fear and Dyball2025) to support social functioning. Further, given the distinct nature of social functioning as a construct from mental health, promoting and protecting social functioning might require interventions with explicit social components such as strengthening social support and enhancing social capital. However, the majority of evidence-based MHPSS interventions primarily target intrapersonal processes, with minimal or no explicit focus on the social dimensions of well-being (Barbui et al., Reference Barbui, Purgato, Abdulmalik, Acarturk, Eaton, Gastaldon, Gureje, Hanlon, Jordans, Lund, Nosè, Ostuzzi, Papola, Tedeschi, Tol, Turrini, Patel and Thornicroft2020; Schäfer et al., Reference Schäfer, Thomas, Lindner and Lieb2023). Moreover, even among those that include social components, limited number of studies evaluating their effectiveness typically rely on measures of psychological distress (Haroz et al., Reference Haroz, Nguyen, Lee, Tol, Fine and Bolton2020; Ubels et al., Reference Ubels, Kinsbergen, Tolsma and Koch2022). Thus, there remains a critical gap in our knowledge about the effectiveness of existing MHPSS interventions for social functioning. Building on the growing evidence of the importance of social functioning among forcibly displaced communities (Kurt et al., Reference Kurt, Almeamari, El-Dardery, Kardouh, Wong, McGrath, Klein, Beetar, Lekkeh, El-Vecih, Yasaki, Acarturk, Hadzi-Pavlovic, Steel, Rosenbaum and Wells2025; McGrath et al., Reference McGrath, Yasaki, Beetar, El-Vecih, Klein, Kurt, Lekkeh, Rosenbaum and Wells2025), our scholarly observations from working with refugee communities and humanitarian workers across several low-resource settings, and the findings from this study, we call for a deliberate effort to understand and support social functioning as a central component of MHPSS programming, as it was originally envisioned.
In summary, this study extends the ecological model of distress to social functioning among refugees and asylum-seekers. The findings lend credence to social functioning as a distinct construct with the differential pathways from conflict-related traumatic experiences and post-displacement stressors. Recognizing social functioning as an integral component of the ecological model provides a strong conceptual foundation for advancing research and practice in MHPSS programming for refugees and asylum-seekers.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796026100614.
Availability of data and materials
Anonymized data may be shared upon reasonable request to the corresponding author.
Acknowledgments
We would like to thank each participant who entrusted us with their experiences. We acknowledge the contributions of our study partners, HOST International, SUAKA and Universitas Gadjah Mada. Special thanks to Shraddha Kashyap, Mitra Khakbaz, Diah Tricesaria, Zico Pestalozzi, Yunizar Adiputera and Shaila Tieken for their invaluable contributions to the study.
Financial support
The current study was supported by an Australian Research Council Linkage Grant (LP170100852). P.S. was supported by an MQ: Transforming Mental Health Postdoctoral Scholarship (MPSIP\15). A.N. (2018104) was supported by an Australian National Health and Medical Research Council Investigator Leadership Grant.
Competing interests
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 200.




 Open access
Open access