


Introduction
Self-harm in adolescents is a major public health concern and a key predictor of suicide (Hawton et al. Reference Hawton, Saunders and O’Connor2012, O’Connor et al. Reference O’Connor, Rasmussen, Miles and Hawton2009). Both the economic and social costs of self-harm are considerable, and thus public health approaches to self-harm, and indeed interventions for the psychosocial problems associated with self-harm, must be considered (Moran et al. Reference Moran, Chandler, Dudgeon, Kirtley, Knipe, Pirkis, Sinyor, Allister, Ansloos, Ball, Chan, Darwin, Derry, Hawton, Heney, Hetrick, Li, Machado, McAllister, McDaid, Mehra, Niederkrotenthaler, Nock, OKeefe, Oquendo, Osafo, Patel, Pathare, Peltier, Roberts, Robinson, Shand, Stirling, Stoor, Swingler, Turecki, Venkatesh, Waitoki, Wright, Yip, Spoelma, Kapur, O’Connor and Christensen2024). The school environment is one of the principal settings that influences the health behaviours, well-being and emotional health of adolescents (Kidger et al. Reference Kidger, Heron, Leon, Tilling, Lewis and Gunnell2015; Pisinger et al. Reference Pisinger, Hawton and Tolstrup2019). Moreover, self-harm presentations at emergency departments have been found to be lower during school holidays in adolescents (McEvoy et al. Reference McEvoy, Joyce, Mongan, Clarke and Codd2024). Furthermore, many of the psychosocial problems associated with self-harm involve, or may occur in, the school setting – such as bullying, being unpopular with peers, school truancy or dropout, conduct or behavioural issues, and engaging in violence (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023). Given the extensive time spent in school by adolescents, it is both an obvious and convenient setting for implementing universal interventions for self-harm and the psychosocial problems to which self-harm is associated.
Self-harm is defined as intentional self-poisoning or self-injury irrespective of the apparent purpose of the act (National Institute for Health and Care Excellence (NICE) 2022). It typically begins in young people in early adolescence, about the same time adolescents enter secondary or high school (Hawton et al. Reference Hawton, Saunders and O’Connor2012; Sawyer et al. Reference Sawyer, Azzopardi, Wickremarathne and Patton2018).
School-based interventions for suicide prevention have been found to be effective in reducing suicidal self-harm (Bailey et al. Reference Bailey, Spittal, Pirkis, Gould and Robinson2017; Moran et al. Reference Moran, Chandler, Dudgeon, Kirtley, Knipe, Pirkis, Sinyor, Allister, Ansloos, Ball, Chan, Darwin, Derry, Hawton, Heney, Hetrick, Li, Machado, McAllister, McDaid, Mehra, Niederkrotenthaler, Nock, OKeefe, Oquendo, Osafo, Patel, Pathare, Peltier, Roberts, Robinson, Shand, Stirling, Stoor, Swingler, Turecki, Venkatesh, Waitoki, Wright, Yip, Spoelma, Kapur, O’Connor and Christensen2024; Wasserman et al. Reference Wasserman, Hoven, Wasserman, Wall, Eisenberg, Hadlaczky, Kelleher, Sarchiapone, Apter, Balazs, Bobes, Brunner, Corcoran, Cosman, Guillemin, Haring, Iosue, Kaess, Kahn, Keeley, Musa, Nemes, Postuvan, Saiz, Reiter-Theil, Varnik, Varnik and Carli2015). In addition, school-based interventions that address common psychosocial problems associated with self-harm, such as anti-bullying programmes, school-based violence prevention programmes, and emotional learning programmes have been proven to be successful in improving the mental health of young people, more generally (Dowling and Barry Reference Dowling and Barry2020; Fraguas et al. Reference Fraguas, Díaz-Caneja, Ayora, Durán-Cutilla, Abregú-Crespo, Ezquiaga-Bravo, Martín-Babarro and Arango2021; Stänicke Reference Stänicke2021). Implementing such programmes in schools, like effective anti-bullying measures, could simultaneously improve mental health for young people in school (Fraguas et al. Reference Fraguas, Díaz-Caneja, Ayora, Durán-Cutilla, Abregú-Crespo, Ezquiaga-Bravo, Martín-Babarro and Arango2021) and possibly reduce self-harm. Hence, school-based interventions targeting psychosocial problems associated with self-harm, as well as interventions for self-harm itself, could help to reduce self-harm in adolescents.
Understanding the extent to which the rates of self-harm and its risk factors (psychosocial problems) vary across different types of schools is important so that, in cases of limited resources, departments or ministries of education could assess which schools have the most pressing need for such public health interventions. Furthermore, identifying which types of schools demonstrated higher levels of self-harm, or psychosocial problems associated with self-harm, could aid in the identification of sub-groups of adolescents at an elevated risk.
School demography, ethos, and policies vary widely and could have an influence on the propensity of students to experience distress and engage in self-harming behaviours. Schools can vary with respect to being coeducational or single-sex, having a religious ethos or being non-denominational, being socio-economically disadvantaged, or being a private fee-paying versus a non-fee-paying school. It is currently unknown to what extent these factors influence the levels of self-harm and the psychosocial problems to which self-harm is associated.
Most of the research concerning self-harm, or the psychosocial problems to which it is associated, has typically been conducted at the individual level rather than the school level (Kim and Chun Reference Kim and Chun2020). Studies that have examined school-level differences for self-harm are rare. One example of such a study by Young et al., found that while holding Catholic religious beliefs were protective for students against suicidal behaviours, paradoxically attending a Catholic school was a risk factor (Young et al. Reference Young, Sweeting and Ellaway2011). There were also studies that examined psychosocial problems associated with self-harm across different types of schools. For example, emotional and behavioural health, measured by the Strengths and Difficulties Questionnaire (SDQ), is a key risk factor for self-harm (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023; McEvoy et al. Reference McEvoy, Joyce, Mongan, Clarke and Codd2024) and was found to vary across different primary schools (Lewer et al. Reference Lewer, Gilbody, Lewis, Pryce, Santorelli, Wadman, Watmuff and Wright2024). Furthermore, bullying has been found to vary across different schools in low- and middle-income countries (Kim and Chun Reference Kim and Chun2020).
This study used a nationally representative longitudinal cohort study in Ireland to explore how self-harm, and well-established psychosocial problems associated with self-harm, varied across different types of schools. Psychosocial problems, such as internalising problems or bullying, have been well established as risk factors for self-harm by an umbrella review of systematic reviews (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023). These risk factors are referred to as psychosocial problems in this study since they are also important outcomes in their own right. Types of schools was determined by sex composition, socio-economic status, and religious ethos.
The primary aim of this study was to explore which types of schools had higher proportions of young people with lifetime reported self-harm in adolescents at age 17. The secondary aim of the study was to examine which types of schools had higher proportions of young people exhibiting psychosocial problems (risk factors) associated with self-harm at age 13. The tertiary aim of this study was to examine and separate the school-level and individual-level effects on self-harm and the psychosocial problems to which it is was associated, using multilevel regression models.
Methods
Study population
Growing Up in Ireland (GUI) is a nationally representative longitudinal cohort study in Ireland (Murphy et al. Reference Murphy, Williams, Murray and Smyth2019). This study used data from Cohort ’98, which recruited n = 8,568 nine-year-olds born in 1998 (or the year before or after) and followed them up at ages 13, 17, and 20 years (Murphy et al. Reference Murphy, Williams, Murray and Smyth2019). Data collected involved outcomes covering the participants’ physical health and development, social and emotional well-being, and educational achievement. This study used data from two waves from the GUI Cohort ’98: n = 7,525 participants at age 13 and n = 6,216 participants followed up at age 17. There were 84 participants that were removed at age 13 for analysis since they were still in primary school, were in a special school or did not provide information on the type of school that they attended. Hence, n = 7,441 participants at age 13, clustered within 622 secondary schools, were analysed for this study.
Exposure variables
All of the exposure variables were from the age 13 wave of the data. Typically, adolescents transition from primary school to secondary school in Ireland about the age of 12 and adolescents who self-harm usually first exhibit this behaviour approximately from ages 12 to 14 (Cipriano et al. Reference Cipriano, Cella and Cotrufo2017; Department of Education and Science 2004). At age 13, a number of school-level variables were derived in the GUI dataset using a database of schools from the Department of Education in the Republic of Ireland. The school-level derived variables included whether the school type was coeducational or single-sex; a non-fee-paying school or a fee-paying school; or whether the school was a disadvantaged school. A disadvantaged status of a school was determined if the school was subsidised by the Delivering Equality of Opportunity in Schools (DEIS) programme during the time that data for the age 13 wave of GUI was collected. The DEIS programme was designed to give tailored support to schools that have a high concentration of disadvantage (Department of Education and Skills 2017). Data pertaining to religious ethos of schools were also included. A summary of the exposure and outcome variables is presented in Figure 1.
Exposure and outcome variables used in this study.

In order to differentiate between the sex composition at the school-level and individual-level differences with respect to sex, this study used two variables at each level: parent-reported sex of the young person and the sex composition of the school – coeducation, single-sex girls, and single-sex boys, with coeducation school being the reference category.
Two variables were also included to differentiate between school-level disadvantage and individual-level disadvantage. This study also used another derived variable from the GUI dataset – namely, household social class of the young person. This variable was derived using the reported occupations of the primary and secondary care givers, with the following categories in descending order of social status: professional workers, managerial and technical, non-manual, skilled manual, semi-skilled, unskilled, and all others gainfully occupied and unknown occupational status. This six-category ordered variable was collapsed into a three-category ordered variable into ‘professional or managerial’, ‘non-manual or skilled’, and ‘semi-skilled or unskilled’, with the first of these being the reference category. The associated school-level variable was the three-outcome school type: disadvantaged school, fee-paying school, and standard school, which was a school that was in neither of the former categories and was the reference group for this variable.
Finally, two variables were also used to differentiate between individual-level religion and the religious ethos of the school. Each school had a religious denomination from the following list: Catholic, inter-denominational, Church of Ireland, multi-denominational, Methodist, and Quaker. This was recoded into three categories: Catholic, multi-/inter-denominational, and Protestant (combining Church of Ireland, Methodist, and Quaker, due to small numbers in each). There was no explicit variable for the young person’s religion at age 13 years; rather, the variable that both parents had a religion was used as a proxy variable. This variable was coded as missing if only one parent or neither parent provided a response.
Outcome variables
All of the outcomes for this study were binary. The outcomes were self-harm by age 17 and psychosocial problems (risk factors) associated with self-harm at age 13: internalising problems (depression or anxiety); externalising problems (behavioural or conduct issues); bullying; substance use; school truancy or excessive absence from school; low popularity with peers; being involved in violence; and not getting on with parents.
Lifetime self-harm
Lifetime self-harm data were recorded at age 17. The participants were asked if they had ever hurt themselves on purpose in any way.
Psychosocial outcomes at age 13
Psychosocial risk factors were measured at age 13 to ensure clear temporal ordering between school-type exposure, early psychosocial functioning, and later self-harm. Although we observed cross-sectional associations between school type and psychosocial problems at age 13, it is unlikely that psychosocial difficulties determine the type of school attended, which is usually established earlier and remains stable. Thus, the more plausible direction is that school environment influences psychosocial problems. Using age 13 measures also avoids reverse causation, providing a valid baseline of psychosocial problems before self-harm by age 17.
The selection of these psychosocial problems was informed by two studies conducted prior to this study (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023, McEvoy et al. Reference McEvoy, Brannigan, Walsh, Arensman and Clarke2024). Using an umbrella review examining risk factors for self-harm in young people (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023), a list of psychosocial factors was compiled from the risk factors that had a pooled odds ratio from meta-analyses of at least two and/or were identified as a risk factor in at least four systematic reviews. This list of well-established risk factors for self-harm was then reduced to psychosocial factors for which data was available from the GUI dataset. Then using a latent class analysis of psychosocial factors for self-harm at age 13 using the GUI dataset (McEvoy et al. Reference McEvoy, Brannigan, Walsh, Arensman and Clarke2024), it was determined which risk factors from this list should be included in this study (i.e. factors that did not have a low prevalence) – namely, the nine psychosocial factors listed in previously mentioned and listed in Figure 1. Note that being female (a risk factor for self-harm) was included instead as an exposure variable and not an outcome variable.
Internalising problems was measured using the SDQ, which is the emotional problems sub-score added to the peer problems sub-score (Goodman and Goodman Reference Goodman and Goodman2009). An internalising problems score of 8 or more is considered to be clinically significant and was used as a ‘yes’ for this variable (Goodman and Goodman Reference Goodman and Goodman2009).
Externalising problems was also measured using the SDQ, which is the conduct problems sub-score added to the hyperactivity problems sub-score (Goodman and Goodman Reference Goodman and Goodman2009). An externalising problems score of 11 or more is considered significant and was used as a ‘yes’ for this variable (Goodman and Goodman Reference Goodman and Goodman2009). A second measure of school-specific conduct issues (i.e., school misbehaviour) was also used as an outcome. For ‘school misbehaviour reported by the young person at age 13’, the young person had to report either ‘often’ or ‘all the time’ to not following the school rules, unruly behaviour in class, getting detention, being suspended, or receiving other punishments for misbehaviour.
Bullying was defined as a report by the primary care giver that the young person had been bullied in the last three months.
For school truancy or excessive absence from school, this variable was recorded as ‘yes’ if either the young person was absent from school for more than 20 days in the past school year or answered that they occasionally, quite often or always skipped classes. Irish schools are mandated to inform social services if a child has missed 20 days or more in the school year (TUSLA: Education Welfare Service 2025).
For substance use, the young person had to answer ‘yes’ to at least one of: smoked cigarettes at least once a week; consumed alcohol at least once a month; or ever tried using cannabis, sniffing glues or illicit drugs.
Low popularity with peers was determined by a score of ≤39 on the Piers–Harris Children’s Self-Concept popularity sub-scale Community-University Partnership for the Study of Children Youth and Families 2011).
Violence or peer conflict was a report by the young person that they had been involved in a serious physical fight where someone got badly hurt or needed to see a doctor. ‘Does not get on with a parent’ was a report by the young person that they did not get on with their mother, father or both.
Statistical analysis
Cross table proportions were calculated for all of the school factors with lifetime self-harm at age 17 and the psychosocial problems to which self-harm is associated. Sample weights were applied to these proportions to make them representative of the population of the Republic of Ireland. Chi-square tests then were used to determine if there were significant relationships between each of the 3 school variables and the 10 outcome variables.
The Benjamini–Hochberg procedure was used to control the false discovery rate of the m = 30 hypothesis tests and is an appropriate method for this type of exploratory analysis (James et al. Reference James, Witten, Hastie and Tibshirani2013). This procedure ranks the p-values and compares them to adjusted thresholds, allowing for the identification of statistically significant results while limiting false positives (James et al. Reference James, Witten, Hastie and Tibshirani2013).
Next, categories of schools were created using both school sex (girls, boys, or coeducation) and school type (standard, fee-paying, and DEIS) to examine the interactions between these two school variables. Using sample weights, the proportions of lifetime self-harm reported at age 17 was calculated for participants within each of these categories of schools. These proportions were then ranked to determine which categories of schools had the highest proportions of self-harm. For statistical disclosure control reasons, school religion was not included in these interactions due to small numbers in coeducation denominational schools. Proportions for single-sex DEIS schools were also excluded from these analyses due to small raw numbers in these categories. All data wrangling and statistical analyses described thus far were conducted in R.
To disentangle school-level from individual-level effects, multilevel regression models were used with students nested within schools. For each of the ten dependent variables (self-harm and the nine psychosocial problems), a multilevel logistic regression was used, which included both school-level variables and their matching individual-level control variables (see Figure 1). Multilevel logistic regression was conducted using the ‘meqrlogit’ function using STATA (version 18). We did not apply sample weights to these models since including them inflated the school-level variance to implausible levels. Within each multilevel regression model, the variance partition coefficient (VPC) or intra-class coefficient (ICC) was used to determine the variation between schools for each outcome variable. Again, we applied the Benjamini–Hochberg procedure to all m = 100 p-values to control the false discovery rate. A sensitivity analysis was also conducted by alternately including and excluding school- and individual-level variables for sex, socio-economic status, and religion.
Results
School characteristics and participant distribution
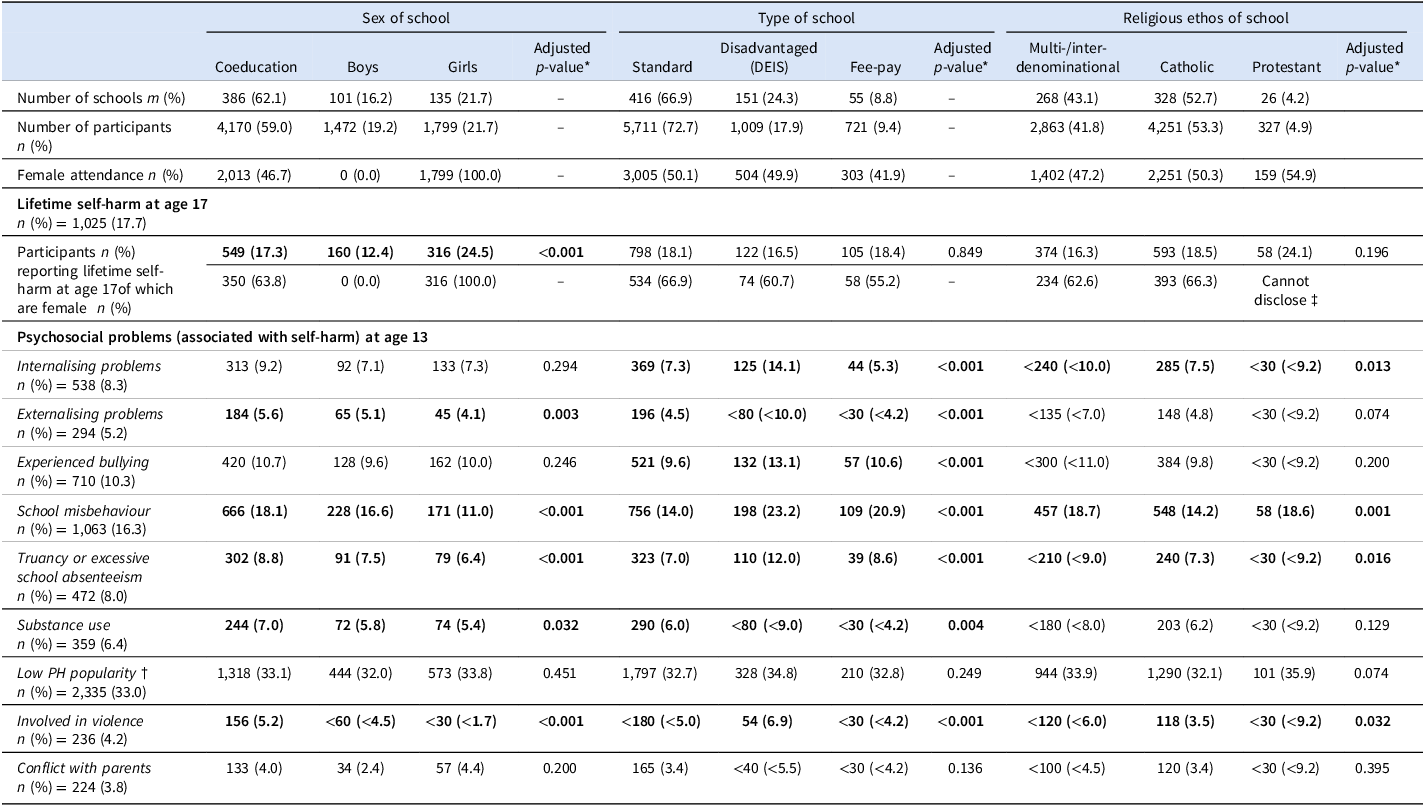
Variation for self-harm and the psychosocial problems across the different school characteristics (unadjusted for individual-level factors) are presented in Table 1. The majority of participants (59%) attended 386 coeducational schools; 21.7% of participants attended 135 single-sex girls’ schools; and 19.2% of the participants attended 101 single-sex boys’ schools. The majority (72.7%) of participants also attended schools that were neither fee-paying nor DEIS schools (416 ‘standard’ schools); 17.9% of individuals attended 151 DEIS schools; and 9.4% of individuals attended 55 fee-paying schools. With respect to religious ethos of schools, 53.3% of participants attended schools with a Catholic ethos; 41.8% attended multi- or inter-denominational schools; and a small proportion of participants (4.9%) attended schools with a Protestant ethos.
School-level characteristics (unadjusted for individual-level factors) and the proportion of self-harm and its associated psychosocial problems within each stratum

Notes: Proportions have been adjusted using sample weights; * chi square test and adjusted p-values were computed using the Benjamini–Hochberg False Discovery rate procedure; † Low Piers Harris sub-score for popularity with peers at age 13; ‡ Figure not disclosed since it would be possible to identify other figures less than n = 30.
The majority (78.0%) of students attending a Protestant school also attended a fee-paying school, whereas a minority (10.3%) of those attending a Catholic school also attended a fee-paying school. Virtually all multidenominational schools were non-fee-paying. See the supplementary material for further details.
Self-harm variation across different types of schools
A lifetime report of self-harm was reported by 17.7% of all young people. The sex of the school was the only category that had a statistically significant difference in the proportions of young people that reported having ever self-harmed by age 17 (not adjusting for individual-level factors). The highest proportion of young people who reported lifetime self-harm was in girls’ schools (24.5%), followed by coeducation schools (17.3%), and then boys’ schools (12.4%). There were no statistically significant differences in the proportions of self-harm across type of schools (standard, DEIS, or fee-pay) or across schools of different religious ethos.
We can also see the trend of higher proportions of lifetime self-harm in those who attended girls’ schools in Figure 2. Within girls’ schools, those who attended fee-paying schools reported lower proportions (albeit non-statistically significant) of lifetime self-harm at age 17 compared to those in standard schools. Conversely, in boys’ schools, those in fee-paying schools had higher proportions of lifetime self-harm by age 17 compared to those in standard schools (again non-statistically significant).
Interactions between sex of school and school type (adjusted using sample weights).

School variation of psychosocial problems associated with self-harm at age 13
While single-sex girls’ schools had statistically significant higher proportions of lifetime self-harm at age 17, paradoxically, single-sex girls’ schools had statistically significant lower proportions in five out of the nine risk factors for self-harm: namely, externalising problems, school misbehaviour, truancy or excessive school absenteeism, substance use, and being involved in violence.
Disadvantaged schools did not have a statistically significant different proportion for lifetime self-harm at age 17 but the participants who attended DEIS schools had statistically higher proportions in seven out of the nine risk factors for self-harm compared to those who attended standard or fee-paying schools (namely, internalising and externalising problems, bullying, school misbehaviour, truancy or excess absenteeism, substance use, and being involved in violence).
Participants attending Catholic schools exhibited a statistically significant lower percentages of school misbehaviour and being involved with violence at age 13.
School-level versus individual-level effects for self-harm
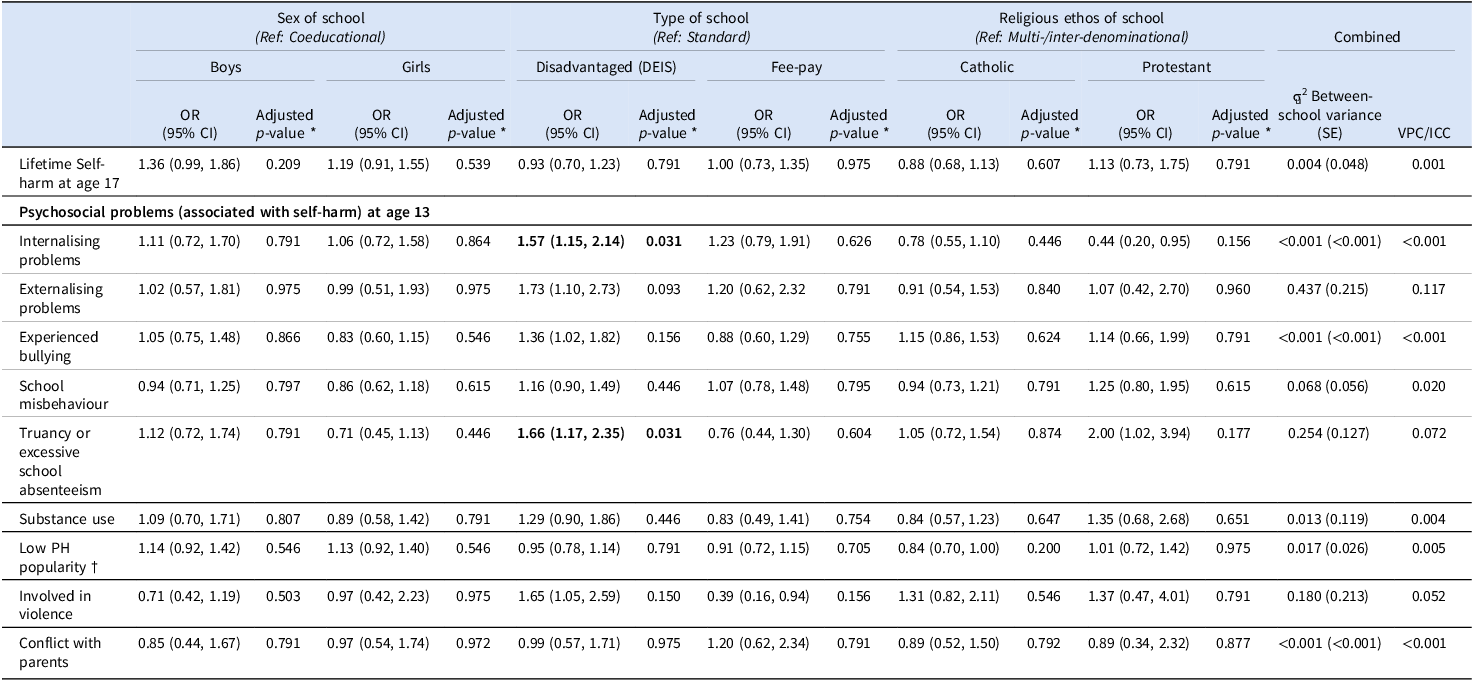
School-level and individual-level effects, separated using multilevel models, are presented in Tables 2 and 3, respectively. In Table 2 (school-level effects), boys in single-sex school were compared to boys in coeducational schools (the reference category). Similarly, girls in single-sex school were compared to girls in coeducational schools. In Table 3 (individual-level effects), boys were compared to girls, regardless of what type of school they attended.
Odds ratios and school-level effects (adjusted for individual-level factors)

Notes: * p-values were computed using the Benjamini–Hochberg False Discovery rate procedure; † Low Piers Harris sub-score for popularity with peers at age 13.
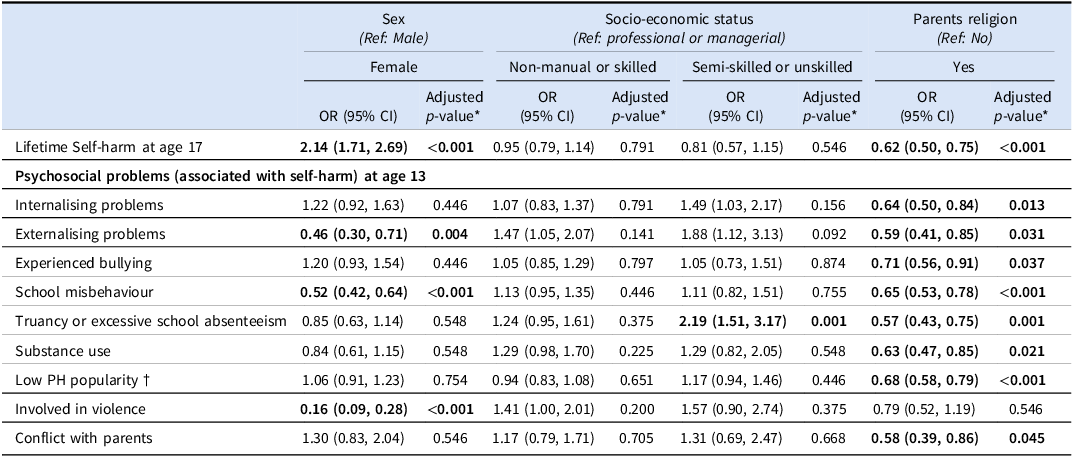
Odds ratios and individual-level effects (adjusted for school-level factors)

Notes: *p-values were computed using the Benjamini–Hochberg False Discovery rate procedure; † Low Piers Harris sub-score for popularity with peers at age 13.
School-level effects (self-harm)
School-level characteristics (adjusted for individual-level effects) for self-harm and the associated psychosocial problems are presented in Table 2. None of the school-level independent variables were significantly associated with self-harm. Specifically, there were no statistically significant associations between the sex, type, or religious ethos of the school and self-harm in young people, when controlling for individual-level associations. Moreover, the majority of the variation for self-harm was between individuals rather than between schools. The ICC for the self-harm model was 0.1% meaning that only 0.1% of the total variance in lifetime reported self-harm in young people was due to differences between schools – that is, virtually all of the variance was at the individual level.
Individual-level effects (self-harm)
Individual-level characteristics (adjusted for school-level effects) for self-harm and the associated psychosocial problems are presented in Table 3. Being female was found to be significantly associated with higher lifetime reported self-harm at age 17: the odds ratio (OR) for females self-harming was 2.14 (95% CI 1.71–2.69) compared to males. Given the significant individual-level effect of being female, the non-significant effect of school sex (coeducational v. single-sex), and the fact that virtually all variance in self-harm lies at the individual level, the higher proportions of self-harm in single-sex girls’ schools compared to coeducational schools (and in coeducational relative to single-sex boys’ schools) are explained by the larger proportion of girls attending those schools.
Both parents having a religion was associated with lower lifetime reported self-harm in the young person (OR = 0.62, 95% CI 0.50–0.75) compared to young people where one or both of the parents did not have a religion.
A statistically significant association between being in a lower social class and lifetime self-harm was not found.
School-level versus individual-level effects for psychosocial problems associated with self-harm
School-level effects (psychosocial problems)
Like in the self-harm outcome model, the ICC was also less than 1% in the models with internalising problems, bullying, substance use, low popularity, and conflict with parents as dependent variables. The highest ICC values were in the models with externalising problems (11.7%) and truancy/excessive absence (7.2%) as dependent variables.
Being in a disadvantaged (DEIS) school was only associated with two psychosocial problems associated with self-harm: internalising problems (OR = 1.57, 95% CI 1.15–2.14) and truancy or excessive absence from school (OR = 1.66, 95% CI 95% 1.17–2.35). A sensitivity analysis found that if ‘both parents having a religion’ was excluded, then being in a disadvantaged school was also associated with externalising problems, bullying, and school misbehaviour, suggesting that these relationships were confounded by family background characteristics correlated with parental religiosity.
Individual-level effects (psychosocial problems)
Even though being female had over twice the odds of lifetime self-harm at age 17 compared to males, being female was associated with lower odds of externalising problems, school misbehaviour, and being involved in violence (0.46 (95% CI 0.30–0.71), 0.52 (95% CI 0.42–0.64), and 0.16 (95% CI 0.09–0.28), respectively).
As well as being protective against a lifetime report of self-harm by age 17, having both parents report having a religion was found to be protective in eight out of the nine risk factors for self-harm – only not statistically significant for being involved in violence. The ORs ranged from 0.57 (95% CI 0.43–0.75) for engaging in truancy or having excessive absence from school at age 13 to 0.71 (95% CI 0.56–0.91) for being a bullying victim at age 13.
The odds for engaging in truancy or having excessive absence from school at age 13 was 2.19 (95% CI 1.51–3.17) in those from a semi-skilled or unskilled social class compared to those from a professional or managerial social class.
Discussion
While girls’ schools showed higher crude proportions of self-harm, this was fully explained by the larger number of girls in those schools. Once individual sex was accounted for, school sex type was no longer associated with self-harm, indicating that the differences seen reflected the sex makeup of the student body rather than school-level factors. Girls report self-harm at roughly twice the rate of boys – as seen in this study (OR = 2.14, 95% CI 1.71–2.69) and in other Irish studies (Doyle et al. Reference Doyle, Treacy and Sheridan2015; Griffin et al. Reference Griffin, McMahon, McNicholas, Corcoran, Perry and Arensman2018; McMahon et al. Reference McMahon, Keeley, Cannon, Arensman, Perry, Clarke, Chambers and Corcoran2014) – so schools with more girls will naturally have higher crude proportions. Virtually all variance in self-harm was at the individual level.
Higher levels of self-harm in adolescent girls compared to boys are not unique to the Irish context; internationally, the girl-to-boy ratio can be as high as five or six to one in early adolescence, narrowing in later years when self-harm increases among boys (Hawton et al. Reference Hawton, Saunders and O’Connor2012; Trafford et al. Reference Trafford, Carr, Ashcroft, Chew-Graham, Cockcroft, Cybulski, Garavini, Garg, Kabir, Kapur, Temple, Webb and Mok2023). Suggested explanations for this imbalance include girls experiencing higher levels of internalising problems and influences associated with the timing of menarche (Keyes and Platt Reference Keyes and Platt2023; Roberts et al. Reference Roberts, Fraser, Gunnell, Joinson and Mars2020). There is also some evidence to suggest that girls are more susceptible the social contagion effect of self-harm than boys – that is, being exposed to peers engaging in self-harm may predispose them to engage in this behaviour themselves (Prinstein et al. Reference Prinstein, Heilbron, Guerry, Franklin, Rancourt, Simon and Spirito2010).
Girls had significantly lower odds of externalising problems, school misbehaviour, and violence. Yet, paradoxically, girls’ schools had higher crude proportions of self-harm despite showing significantly lower levels of five of the nine key risk factors – externalising problems, school misbehaviour, truancy or excessive absence, substance use, and involvement in violence. Paradoxes of this kind are not uncommon in the self-harm and suicide literature: for example, girls consistently report higher levels of self-harm than boys (Doyle et al. Reference Doyle, Treacy and Sheridan2015; Griffin et al. Reference Griffin, McMahon, McNicholas, Corcoran, Perry and Arensman2018; Hawton et al. Reference Hawton, Saunders and O’Connor2012; McMahon et al. Reference McMahon, Keeley, Cannon, Arensman, Perry, Clarke, Chambers and Corcoran2014; Trafford et al. Reference Trafford, Carr, Ashcroft, Chew-Graham, Cockcroft, Cybulski, Garavini, Garg, Kabir, Kapur, Temple, Webb and Mok2023), whereas boys tend to have higher suicide rates (McMahon et al. Reference McMahon, Keeley, Cannon, Arensman, Perry, Clarke, Chambers and Corcoran2014) even though self-harm is one of the strongest predictors of suicide (Hawton et al. Reference Hawton, Saunders and O’Connor2012; O‘Connor et al. Reference O’Connor, Rasmussen, Miles and Hawton2009).
Self-harm is often described as a strategy for affect regulation, helping to reduce overwhelming emotions or regain a sense of control, and is commonly used by adolescent girls (Stänicke Reference Stänicke2021). The higher prevalence of self-harm among girls, contrasted with higher physical aggression among boys, may reflect social and cultural norms around emotional expression (Paulo et al. Reference Paulo, Vagos, Ribeiro Da Silva and Rijo2020). Society may be more accepting of aggressive behaviour in boys and anxious or depressive behaviours in girls, shaping how distress is expressed even when underlying emotions are similar (Paulo et al. Reference Paulo, Vagos, Ribeiro Da Silva and Rijo2020). Although school sex type was not significantly associated with self-harm after adjusting for individual sex, the higher crude proportions in girls’ schools indicate a clustering of higher-risk individuals (i.e. girls). These schools may therefore be appropriate settings for targeted preventive interventions for girls.
Self-harm proportions in disadvantaged (DEIS) schools were not significantly different from those in fee-paying or standard schools. In another paradox, however, DEIS schools showed significantly higher proportions for seven of the nine risk factors for self-harm, including both internalising and externalising problems, which were more than twice as common as in non-DEIS schools. Although earlier research identified low socio-economic status as a risk factor for self-harm (Aggarwal et al. Reference Aggarwal, Patton, Reavley, Sreenivasan and Berk2017; Bozzini et al. Reference Bozzini, Bauer, Maruyama, Simões and Matijasevich2021; Carballo et al., Reference Carballo, Llorente, Kehrmann, Flamarique, Zuddas, Purper-Ouakil, Hoekstra, Coghill, Schulze, Dittmann, Buitelaar, Castro-Fornieles, Lievesley, Santosh, Arango, Curran, Selema, Flanagan, Craig, Parnell, Yeboah, Sala, Singh, Fiori, Pupier, Vinkenvleugel, Glennon, Bakker, Drent, Bloem, Steenhuis, Berg, Häge, Dau, Mechler, Rauscher, Aslan, Schlanser, Keller, Schneider, Plener, Fegert, Paton, Macey, Iessa, Alfred, Helen, Nick, Baillon, Peyre, Cohen, Bonnot, Brunelle, Franc, Raysse, Humbertclaude, Rodriguez-Quiroga, Díaz-Caneja, Espliego, Merchán, Tapia, Baeza, Romero, La Fuente, Ortiz, Pintor, Ligas, Cera, Frongia, Falissard, Schwalber, Dittrich, Wohner, Zimmermann, Schwalber and Aitchison2020), recent evidence suggests this pattern may be changing, with rising self-harm among girls in less deprived communities (Trafford et al. Reference Trafford, Carr, Ashcroft, Chew-Graham, Cockcroft, Cybulski, Garavini, Garg, Kabir, Kapur, Temple, Webb and Mok2023).
It is unclear why higher proportions of young people with risk factors for self-harm in disadvantaged schools did not translate into higher self-harm rates. One conjecture (Kim and Chun Reference Kim and Chun2020), is that the psychological impact of stressors like bullying may be reduced in these settings because such behaviours are more common. Another possibility is that other behaviours – such as externalising problems, substance use, violence, truancy or absenteeism – may substitute for self-harm as responses to distress. Because health risk behaviours tend to co-occur and predict one another (Bozzini et al. Reference Bozzini, Bauer, Maruyama, Simões and Matijasevich2021), elevated levels of these behaviours may diffuse the risk of self-harm. Additional potential explanations include stronger pastoral supports, greater stigma surrounding self-harm, or increased resilience arising from repeated exposure to adversity in disadvantaged schools.
While most self-harm risk factors were more prevalent in disadvantaged schools, only internalising problems and truancy/absenteeism remained significantly associated with school disadvantage in the fully adjusted multilevel model. After adding the variable ‘both parents having a religion’, three previously significant associations – externalising problems, bullying, and school misbehaviour – were substantially attenuated, suggesting that these relationships were confounded by family background characteristics correlated with parental religiosity. Prior research indicates that parental religiosity often serves as a proxy for aspects of the family environment known to influence behavioural risk, including greater parental involvement and monitoring (Bornstein et al. Reference Bornstein, Putnick, Lansford, Al-Hassan, Bacchini, Bombi, Chang, Deater-Deckard, Di Giunta, Dodge, Malone, Oburu, Pastorelli, Skinner, Sorbring, Steinberg, Tapanya, Tirado, Zelli and Alampay2017; Kim-Spoon et al. Reference Kim-Spoon, Farley, Holmes, Longo and McCullough2014), and higher levels of family cohesion and stability (Spilman et al. Reference Spilman, Neppl, Donnellan, Schofield and Conger2013). These family-level processes likely account for the higher prevalence of these behaviours in disadvantaged schools observed in the unadjusted analyses.
Overall, although attending a DEIS school was not directly associated with self-harm, the concentration of risk factors suggests these schools may contain clusters of vulnerable students who could benefit from targeted support. Given that internalising problems and truancy/absenteeism disproportionately affect disadvantaged schools, evidence-based well-being programmes should be introduced in accordance with Ireland’s mental health policy (Department of Health 2020–2030), and the School Completion Programme (providing targeted supports for young people at risk of early school leaving) should be continued (TUSLA: Child and Family Service 2025).
Unlike the Young et al., study, which found that attending a Catholic school was a risk factor (Young et al. Reference Young, Sweeting and Ellaway2011), the current study found no statistically significant differences in self-harm prevalence across schools with different religious ethos. However, consistent with Young et al., who reported that Catholic religious beliefs were protective against suicidal behaviours, the current study found that both parents having a religious affiliation – used as a proxy for the young person’s own religion – was associated with a 38% lower odds of lifetime self-harm (OR = 0.62, 95% CI 0.50–0.75), compared with young people whose parents did not both identify with a religion.
Parents reporting a religious affiliation may signify aspects of a more positive or cohesive family environment (Bornstein et al. Reference Bornstein, Putnick, Lansford, Al-Hassan, Bacchini, Bombi, Chang, Deater-Deckard, Di Giunta, Dodge, Malone, Oburu, Pastorelli, Skinner, Sorbring, Steinberg, Tapanya, Tirado, Zelli and Alampay2017; Kim-Spoon et al. Reference Kim-Spoon, Farley, Holmes, Longo and McCullough2014; Spilman et al. Reference Spilman, Neppl, Donnellan, Schofield and Conger2013), and in an increasingly secular society, it may also reflect cultural belonging or heritage rather than adherence to doctrine (Central Statistics Office 2023; Inglis Reference Inglis2007). Thwarted belongingness is a well-established predictor of suicidal behaviour (O’Connor and Kirtley Reference O’Connor and Kirtley2018; Young et al. Reference Young, Sweeting and Ellaway2011), suggesting that the protective effect observed from ‘both parents having a religion’ may be explained by greater social connectedness or community identification. Additionally, having a sense of meaning in life is known to protect against mental health problems and suicidal behaviours (Disabato et al. Reference Disabato, Kashdan, Short and Jarden2017; Lew et al. Reference Lew, Chistopolskaya, Osman, Huen, Abu Talib and Leung2020). Altogether, although parental religious affiliation appeared strongly protective against both risk factors for self-harm and self-harm itself, there was no evidence that the religious ethos of the school influenced these outcomes.
Overall, almost all of the variance for self-harm, and most of the variance for the risk factors for self-harm, was at the individual level. While schools remain important sites for interventions, the data from this study suggests that interventions should be primarily targeted at individuals in high-risk groups.
Public health implications and further research
Girls may need to be prioritised in both single-sex and coeducation schools for specific interventions for the prevention of self-harm. On the other hand, while there have been well-evaluated school-based programmes for equipping young people to seek help when experiencing mental health difficulties, well-evaluated programmes specific to self-harm are rare (Moran et al. Reference Moran, Chandler, Dudgeon, Kirtley, Knipe, Pirkis, Sinyor, Allister, Ansloos, Ball, Chan, Darwin, Derry, Hawton, Heney, Hetrick, Li, Machado, McAllister, McDaid, Mehra, Niederkrotenthaler, Nock, OKeefe, Oquendo, Osafo, Patel, Pathare, Peltier, Roberts, Robinson, Shand, Stirling, Stoor, Swingler, Turecki, Venkatesh, Waitoki, Wright, Yip, Spoelma, Kapur, O’Connor and Christensen2024). Whilst the positives of implementing youth self-harm or suicide prevention strategies in schools generally outweigh the negatives, such programmes have had some unanticipated adverse consequences like increasing maladaptive attitudes related to suicide or help-seeking; increasing the endorsement that suicide was a reasonable solution; or increasing maladaptive coping styles like self-harm or suicidal behaviour – sometimes even leading to hospitalisations (Kuiper et al. Reference Kuiper, Goldston, Godoy Garraza, Walrath, Gould and McKeon2019). More randomised control trials of school-based interventions to reduce self-harm are therefore needed.
With this in mind, this study could inform the implementation of other public health measures, not specific to self-harm, but addressing the psychosocial problems associated with self-harm. This could result in the reduction of self-harm in adolescents and thereby possibly reduce later deaths by suicide, for which self-harm is a key risk predictor (O‘Connor et al. Reference O’Connor, Rasmussen, Miles and Hawton2009). While this study did not find a significant OR for being in a disadvantaged (DEIS) school with self-harm, there were higher proportions in seven out of the nine risk factors examined for self-harm in disadvantaged schools. Therefore, these schools should be prioritised for interventions addressing the psychosocial problems highlighted in this study. Implementing effective anti-bullying measures or interventions aimed at reducing substance use in disadvantaged schools could simultaneously improve the mental health of its students (Fraguas et al. Reference Fraguas, Díaz-Caneja, Ayora, Durán-Cutilla, Abregú-Crespo, Ezquiaga-Bravo, Martín-Babarro and Arango2021; Van Ryzin et al. Reference Van Ryzin, Cil and Roseth2023). Well-designed evidence-based social and emotional learning programmes, which have been shown to have effective positive outcomes for students (Dowling and Barry Reference Dowling and Barry2020), could be implemented in disadvantaged schools to address the higher levels of internalising and externalising problems, or school misbehaviour in their pupils.
Proportions of poor school behaviour, truancy, and violence were highest in disadvantaged schools. School and social policies in response to negative classroom behaviours, such as reduced timetables, suspensions, expulsions, can be ineffective and even counterproductive (Downes et al. Reference Downes, Pike and Murphy2020; Robison et al. Reference Robison, Jaggers, Rhodes, Blackmon and Church2017). Indeed, exclusion from school is higher among those from a lower socio-economic status and is associated with higher psychopathology (Ford et al. Reference Ford, Parker, Salim, Goodman, Logan and Henley2018) – a key risk factor for self-harm (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023). Multidisciplinary teams of counsellors/therapists, speech and language therapists, occupational therapists in schools (particularly disadvantaged schools), and other professionals should have a role in schools to support students with poor classroom behaviours, externalising problems, poor school attendance, mental health problems or students who are bullying victims or perpetrators (Downes et al. Reference Downes, Pike and Murphy2020; Sourander et al. Reference Sourander, Jensen, Rönning, Elonheimo, Niemelä, Helenius, Kumpulainen, Piha, Tamminen, Moilanen and Almqvist2007). Ultimately, designing and implementing interventions around the risk factors (psychosocial problems) for self-harm may result in the reduction of self-harm itself among adolescents, especially among those in disadvantaged schools.
Much of the literature on risk and protective factors for self-harm has been focused on risk factors (McEvoy et al. Reference McEvoy, Brannigan, Cooke, Butler, Walsh, Arensman and Clarke2023). Future studies could explore protective factors at ages 9 and 13 of the GUI ’98 Cohort for self-harm at ages 17 and 20.
Limitations
Sample weights in the multilevel regression models were removed. Ignoring sample weights in multilevel models may introduce some bias into the models (Cai Reference Cai2013), and it also results in lower external validity of the results of the model. In addition, there was also a small number of participants from disadvantaged and protestant schools, and this may have contributed to a lack of statistical power.
It is also possible that the number of participants in the study who self-harmed was underreported for two reasons. Firstly, any participants that reported “prefer not to say” were counted as missing, though it is possible they did self-harm but did not wish to disclose it due to the stigma surrounding self-harm (Moran et al. Reference Moran, Chandler, Dudgeon, Kirtley, Knipe, Pirkis, Sinyor, Allister, Ansloos, Ball, Chan, Darwin, Derry, Hawton, Heney, Hetrick, Li, Machado, McAllister, McDaid, Mehra, Niederkrotenthaler, Nock, OKeefe, Oquendo, Osafo, Patel, Pathare, Peltier, Roberts, Robinson, Shand, Stirling, Stoor, Swingler, Turecki, Venkatesh, Waitoki, Wright, Yip, Spoelma, Kapur, O’Connor and Christensen2024). Secondly, it is also possible at age 17, some participants may not wish to disclose if they engaged in self-harm in their lifetime, given the stigma of self-harm. Boys, in particular, are less likely to disclose if they had engaged in self-harm (Victor et al. Reference Victor, Muehlenkamp, Hayes, Lengel, Styer and Washburn2018).
Finally, this study controlled for the false discovery rate rather than the family-wise error rate. While this limits the number of type 1 errors, it does not fully eliminate the possibility of these occurring (James et al. Reference James, Witten, Hastie and Tibshirani2013). On balance, limiting the number of type 1 errors rather than eliminating them totally was more appropriate since the analyses were exploratory (James et al. Reference James, Witten, Hastie and Tibshirani2013).
Conclusion
Virtually all of the variance in self-harm and most of the variance in associated psychosocial problems occur at the individual level. Therefore, interventions should primarily target high-risk individuals rather than school types. Nevertheless, the school context remains important when designing public health strategies to address mental health among young people. Consistent with existing evidence, this study found that the prevalence of self-harm among adolescent girls is more than twice that of boys. Accordingly, girls’ schools and coeducational schools should be prioritised for self-harm–specific interventions, although further research is needed to assess the feasibility and effectiveness of such approaches. While the higher prevalence of psychosocial problems associated with self-harm in disadvantaged schools can largely be explained by adolescents’ family circumstances, the greater concentration of affected individuals in these schools suggests they should be prioritised for the implementation of well-being programmes and the continued delivery of interventions aimed at improving school attendance.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ipm.2026.10192.
Data availability statement
The GUI datasets are available upon application to the ISSDA in Ireland.
Acknowledgements
We wish to thank the Central Statistics Office (CSO) in Ireland for providing access to the data. Results are based on analysis of strictly controlled Research Microdata Files provided by the CSO. The CSO does not take any responsibility for the views expressed or the outputs generated from this research. We also wish to thank all of the participants from the Growing Up in Ireland (GUI) study. We wish to thank Professor Emer Smyth from the Economic and Social Research Institute (ESRI) and Dr Eve Griffin from the National Suicide Research Foundation for their advice and expertise during this project. We also wish to thank Professor George Leckie from the Centre for Multilevel Modelling in the University of Bristol. We also wish to thank Dr Fiona Boland from the Data Science Centre, RCSI.
Funding statement
This was funded by the Health Research Board (HRB) Ireland as part of the SPHeRE Programme (Structured Population and Health-services Research Education): https://www.sphereprogramme.ie.
Competing interests
None to declare.
Ethical standards
Ethical approval for GUI was granted by the research ethics committee of the Health Research Board in Ireland. The secondary analysis of this dataset was approved by the Research Ethics Committee for the Royal College of Surgeons in Ireland (Record ID: 212,613,109). The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008.
Consent for publication
Not applicable.
Patient and public involvement
School teachers were consulted prior to the study being conducted on the direction of the study.





 Open access
Open access