


Introduction
Hypoplastic left heart syndrome is one of the more common and most severe forms of single-ventricle CHD and accounts for approximately 20% of all CHD deaths in infants. Reference Chang, Chen and Klitzner1–Reference Gordon, Rodriguez, Lee and Chang4 This form of CHD is characterised by varying degrees of aortic and mitral valve obstruction with associated hypoplasia of the aortic arch and left ventricle. An intact or highly restrictive atrial septum occurs in ∼ 10% of patients with hypoplastic left heart syndrome and is associated with mortality ≥50%. Reference McHugh, Hillman, Gurka and Gutgesell5–Reference Hoque, Richmond, Vincent, Bacha and Torres7
In fetuses with hypoplastic left heart syndrome, oxygenated blood returning from the pulmonary veins must cross the atrial septum left to right to maintain cardiac output and adequate systemic oxygenation. Restriction to flow across the atrial septum impairs the ability of the pulmonary veins to drain from the lungs. Reference Szwast, Tian, McCann, Donaghue and Rychik8 The occurrence of a restrictive atrial septum in utero may result in pulmonary vascular and lymphatic abnormalities, as well as elevated left atrial pressure, which makes these patients difficult to stabilise postnatally Reference Glatz, Tabbutt and Gaynor9,Reference Rychik, Rome, Collins, DeCampli and Spray10 and at higher risk for mortality during necessary future palliative surgeries that depend on passive pulmonary blood flow. Reference Graziano, Heidelberger, Ensing, Gomez and Ludomirsky11
Detection of a restrictive atrial septum using fetal echocardiography includes both direct assessment of the appearance of the atrial septum and pulmonary veins, as well as evaluation of indirect markers of restricted left atrial egress: the presence of a decompressing vein and/or abnormal pulmonary vein Doppler patterns. Two-dimensional assessment of the atrial septum can be difficult given the limitations of fetal echocardiography, and studies have described using pulmonary vein Doppler patterns as the more reliable predictor of need for urgent postnatal intervention. Reference Taketazu, Barrea, Smallhorn, Wilson and Hornberger12
Fetuses with hypoplastic left heart syndrome and a restrictive atrial septum often require balloon atrial septostomy or stenting of the interatrial septum to provide adequate intracardiac mixing and left atrial decompression. In addition to postnatal interventions, there have been several intrauterine procedures in which technical success has been described, including catheter-based balloon atrial septostomy and/or atrial stent placement, as well as EXIT procedures with atrial stenting. The benefits of these procedures have not been clearly established. A recent retrospective study showed an association with improvement of fetal lung disease for those who underwent fetal atrial septal intervention. Reference Yilmaz Furtun, Trivedi and Day13 On the other hand, while a recent metanalysis of fetal atrial septal intervention showed that fetuses with prenatal intervention were less likely to have a restrictive atrial septum postnatally, there was no difference in survival to birth, neonatal survival, or survival to hospital discharge when compared to fetuses who were managed expectantly. Reference Mustafa, Aghajani, Jawwad, Shah, Abuhamad and Khalil14 The benefits of these procedures are an important topic of continued research.
The aim of our study was to compare postnatal outcomes and survival among patients without atrial restriction and those meeting diagnostic criteria for a restrictive atrial septum before (Early) or after (Late) 30 weeks’ gestational age. Understanding the association between the timing of atrial restriction in patients in utero and postnatal outcomes has potential implications for prenatal counselling, delivery planning, and postnatal management, as well as in utero cardiac interventions.
Methods
Study population
We performed a single-centre, retrospective review of patients evaluated at Vanderbilt University Medical Center between December 2008 and August 2022. The study was approved by the Vanderbilt University Medical Center Institutional Review Board. Patients were included based on the following criteria: 1) prenatal diagnosis of hypoplastic left heart syndrome (mitral atresia/aortic atresia, mitral stenosis/aortic atresia or mitral stenosis/aortic stenosis); 2) at least 1 reviewable fetal echocardiogram prior to delivery; 3) first fetal echocardiogram performed at or before 30 weeks’ gestation; and 4) diagnosis/anatomy confirmed postnatally by transthoracic echocardiogram. Exclusion criteria included intrauterine fetal demise, incomplete postnatal records, or diagnosis of hypoplastic left ventricle in the setting of other complex CHD (including, but not limited to, double outlet right ventricle, unbalanced atrioventricular septal defect, and heterotaxy syndrome). Fetal restrictive atrial septum was diagnosed by the presence of at least one of the following fetal echocardiographic criteria: an intact atrial septum, the presence of a decompressing vein, or an antegrade:retrograde pulmonary vein Doppler velocity time integral ratio <3, which has been reported to be highly predictive of the need for emergent postnatal atrial septostomy. Reference Gellis, Drogosz and Lu15–Reference Michelfelder, Gomez, Border, Gottliebson and Franklin18
A restrictive atrial septum diagnosed before 30 weeks’ gestation was considered “Early,” and atrial restriction at or after 30 weeks’ gestation was defined as “Late.” A cutoff of 30 weeks’ gestation was a priori chosen to define our restriction groups because pulmonary blood flow increases in the late second and early third trimester as pulmonary vascular resistance increases and because the American Academy of Pediatrics uses a gestational age <30 weeks to define significant lung immaturity. Reference Polin and Carlo19,Reference Verder, Albertsen and Ebbesen20 Individual medical records were then reviewed by the research team. Study data were collected and managed using REDCap (Research Electronic Data Capture), an electronic data capture tool hosted at Vanderbilt University Medical Center. Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde21
Clinical data and outcomes
The electronic medical record was reviewed to collect demographic, clinical, echocardiographic, and haemodynamic data. Fetal echocardiographic data included gestational age at echocardiogram, presence of an intact atrial septum, presence of a decompressing vein, antegrade:retrograde pulmonary vein Doppler velocity time integral ratio, degree of tricuspid valve regurgitation, and presence of right ventricular dysfunction. Postnatal data included race, sex, gestational age at birth, birth weight, Apgar scores, cardiac diagnosis, genetic diagnoses, and receipt of emergent postnatal intervention within 24 hours of life (defined as catheter-based intervention on the atrial septum or emergent cardiac surgery).
For patients who met criteria for fetal atrial restriction and for patients who underwent cardiac intervention within 24 hours of birth, pulmonary vein Doppler velocity time integral measurements were manually re-measured by a single reviewer (ACV) who was blinded to the primary outcome. All measurements were performed over at least two cardiac cycles and averaged. The first postnatal echocardiogram was reviewed to ensure accuracy of fetal diagnosis and to assess right ventricular function, degree of tricuspid regurgitation, and presence of coronary artery fistulae.
The type of stage I palliation was determined and classified as (1) Norwood with Blalock-Thomas-Taussig shunt, (2) Norwood with Sano (right ventricular to pulmonary artery) shunt, or (3) hybrid palliation, which included pulmonary artery banding with either continuation of prostaglandin infusion or stent placement in the ductus arteriosus. Because pulmonary hypertension is usually considered to be a contraindication to successful stage II palliation and is thought to contribute to poor outcomes in patients with hypoplastic left heart syndrome and atrial restriction, interstage haemodynamic data were obtained by reviewing the first cardiac catheterisation following stage I palliation. Haemodynamic data collected included age at catheterisation, right ventricular end-diastolic pressure, mean pulmonary artery pressure, mean left atrial pressure, transpulmonary gradient (calculated as mean pulmonary artery pressure—mean left atrial pressure), indexed pulmonary vascular resistance, ratio of pulmonary to systemic blood flow (Qp:Qs), and presence of aorticopulmonary and/or venovenous collaterals. Outcome data included 30-day mortality following stage I palliation, overall survival, and transplant-free survival at last follow-up in April 2023.
Statistical analysis
Continuous data are reported as medians with interquartile ranges. Categorical data are reported as frequencies with percentages (n/N, %). Patient characteristics and outcomes data were compared across the three groups using Pearson’s chi-squared for categorical variables and Kruskal–Wallis for continuous variables. For variables with significant p-values (<0.05), pairwise comparisons were performed between each pair of groups using Pearson’s chi-squared for categorical variables and the Mann–Whitney U test for continuous variables. Comparative survival and transplant-free survival analyses were performed using the Kaplan–Meier method and the log-rank test for statistical significance. A commercially available statistical software package was used for data analysis (STATA Version 17.0, College Station, Texas).
Results
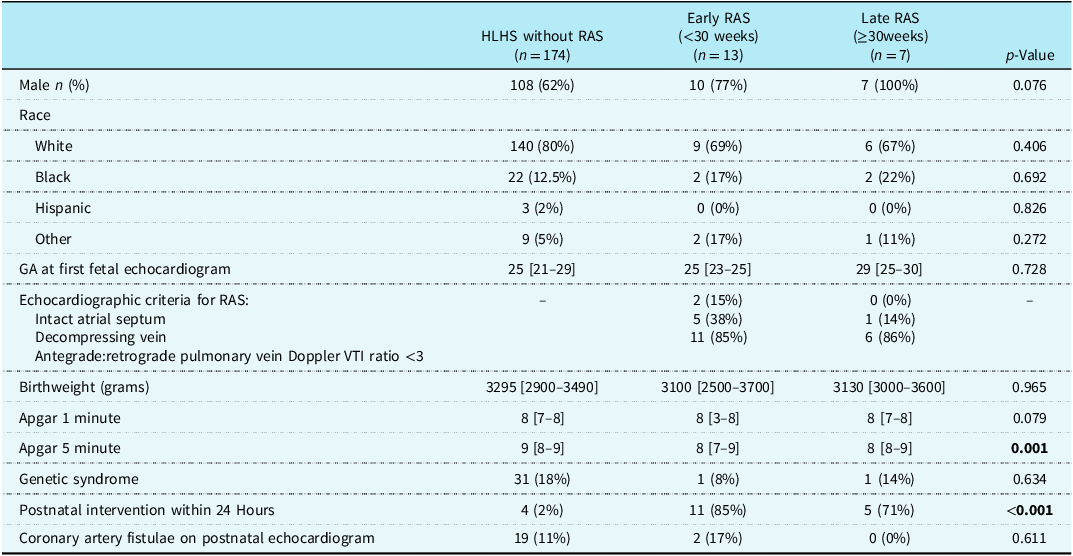
A total of 196 patients with hypoplastic left heart syndrome were reviewed; 22 patients met criteria for fetal atrial restriction (11%), and 20 had a reviewable fetal echocardiogram prior to 30 weeks’ gestation. Of these, 13 met criteria for Early restriction and 7 for Late restriction. Other than the 5-minute Apgar score, there were no significant differences in postnatal demographics (Table 1). There was no significant difference in gestational age at first fetal echocardiogram or restrictive atrial septum diagnostic criteria, with most patients meeting criteria based on pulmonary vein Doppler ratios (Table 1). None of the patients met the inclusion criteria for atrial restriction based on the presence of a decompressing vein alone. There were no significant differences in the presence of coronary artery fistulae, right ventricular dysfunction, or significant tricuspid regurgitation on the first postnatal echocardiogram among the groups, with most patients in all groups having no or mild ventricular dysfunction and no significant tricuspid regurgitation (defined as mild or less). Both the Early and Late restriction groups had significantly higher rates of emergent postnatal intervention (11/13, 85% for Early restriction, and 5/7, 71% for Late restriction) compared to the group without atrial restriction (4/174, 2%) (p ≤ 0.001). Pairwise comparisons of significant differences among the three groups are shown in Supplemental Table 1.
Pre- and post-natal demographics

HLHS = hypoplastic left heart syndrome; GA = gestational age; RAS = restrictive atrial septum; VTI = velocity time integral.
*p-values are from the Kruskal–Wallis test for continuous variables and from the Pearson’s chi-squared test for categorical variables by comparing the three groups. Continuous data are presented with medians and [IQRs] (interquartile ranges).
**No difference in right ventricular function or tricuspid regurgitation among groups.
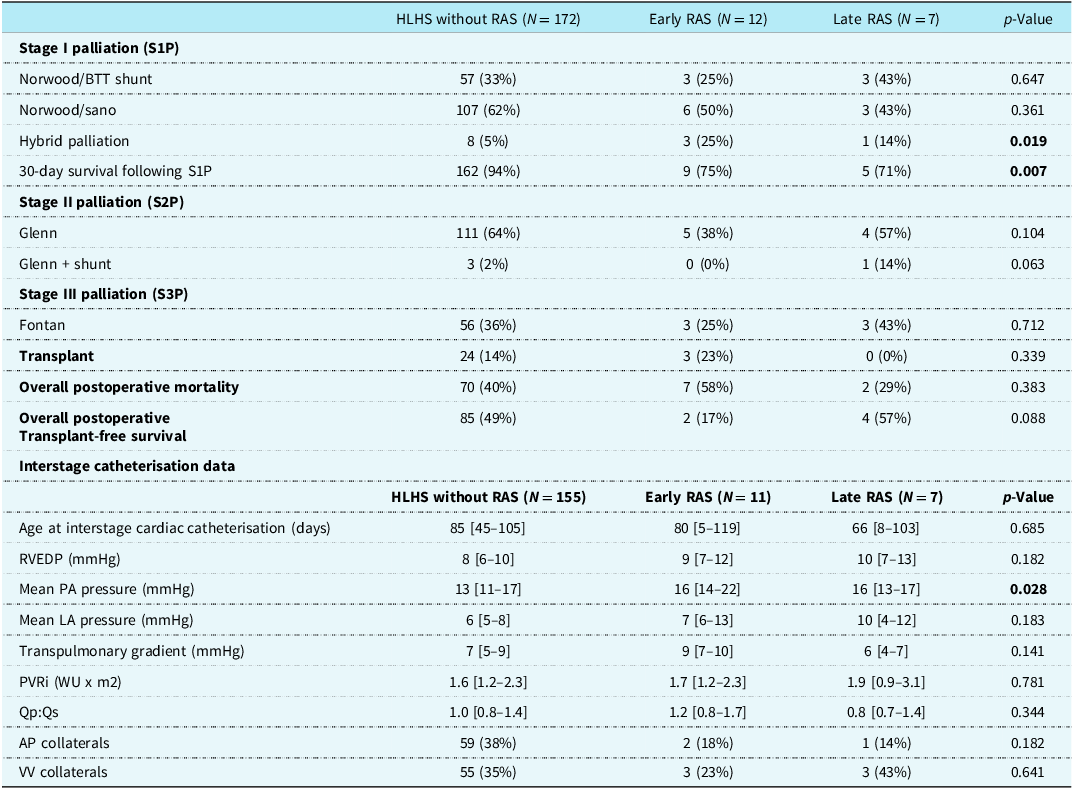
Surgical outcomes and cardiac catheterisation data are shown in Table 2. Patients who died prior to stage I palliation (2 in the group without restriction, 1 in the Early restriction group) or did not undergo cardiac catheterisation (19 in the group without restriction, 2 in the Early restriction group) were not included. Patients in both Early and Late restriction groups had a significantly higher likelihood of undergoing a hybrid approach for stage I palliation (3/12, 25% Early, 1/7, 14% Late) compared to patients without atrial restriction (8/172, 5%) (p = 0.019). The indications for hybrid palliation in these patients included instability on extracorporeal membrane oxygenation, cerebral infarct, severe lung parenchymal disease, significant end-organ injury, and instability after failed balloon atrial septostomy.
Surgical pathways and outcomes

HLHS = hypoplastic left heart syndrome; RAS = restrictive atrial septum; S1P = stage I palliation; S2P = stage II palliation; S3P = stage III palliation; RVEDP = right ventricular end diastolic pressure; PA = pulmonary artery; LA = left atrium; PVRi = indexed pulmonary vascular resistance; WU = wood’s units; Qp = pulmonary flow; Qs = systemic flow; AP = aortopulmonary; VV = venovenous.
Additionally, patients in both Early and Late restriction groups had significantly higher 30-day surgical mortality following stage I palliation (3/12, 25% Early, 2/7, 29% Late) compared to patients without atrial restriction (10/172, 6%) (p = 0.007), with no significant difference between the Early and Late groups. There was no significant difference among the three groups in the proportion of patients who underwent stage II palliation, including Glenn and Glenn plus shunt, or stage III palliation (Fontan). Patients in the Early group had higher overall post-operative mortality (7/12, 58%) compared to the Late group (2/7, 29%) and the group without restriction (70/172, 40%), though this did not reach statistical significance (p = 0.383). Similarly, rates of heart transplantation were higher in the Early group (3/12, 23%) compared to the Late group (0/7, 0%) and the group without restriction (24/172, 14%, p = 0.339). Overall transplant-free survival was lower in the Early group (2/12, 17%) compared to the Late group (4/7, 57%) and the group without restriction (85/172, 49%, p = 0.088). Individual pulmonary vein velocity time integral measurements and markers of atrial restriction, as well as postnatal interventions and outcomes, are summarised in Supplemental Table 2.
Except for mean pulmonary artery pressure, there was no significant difference among the groups in haemodynamic data among on interstage cardiac catheterisation between stage I and stage II palliations. The mean pulmonary artery pressure was significantly higher in both Early and Late groups (median 16 mmHg for both) compared to the group without restriction (median 13 mmHg). Not all patients in each group had interstage cardiac catheterisation data available for review.
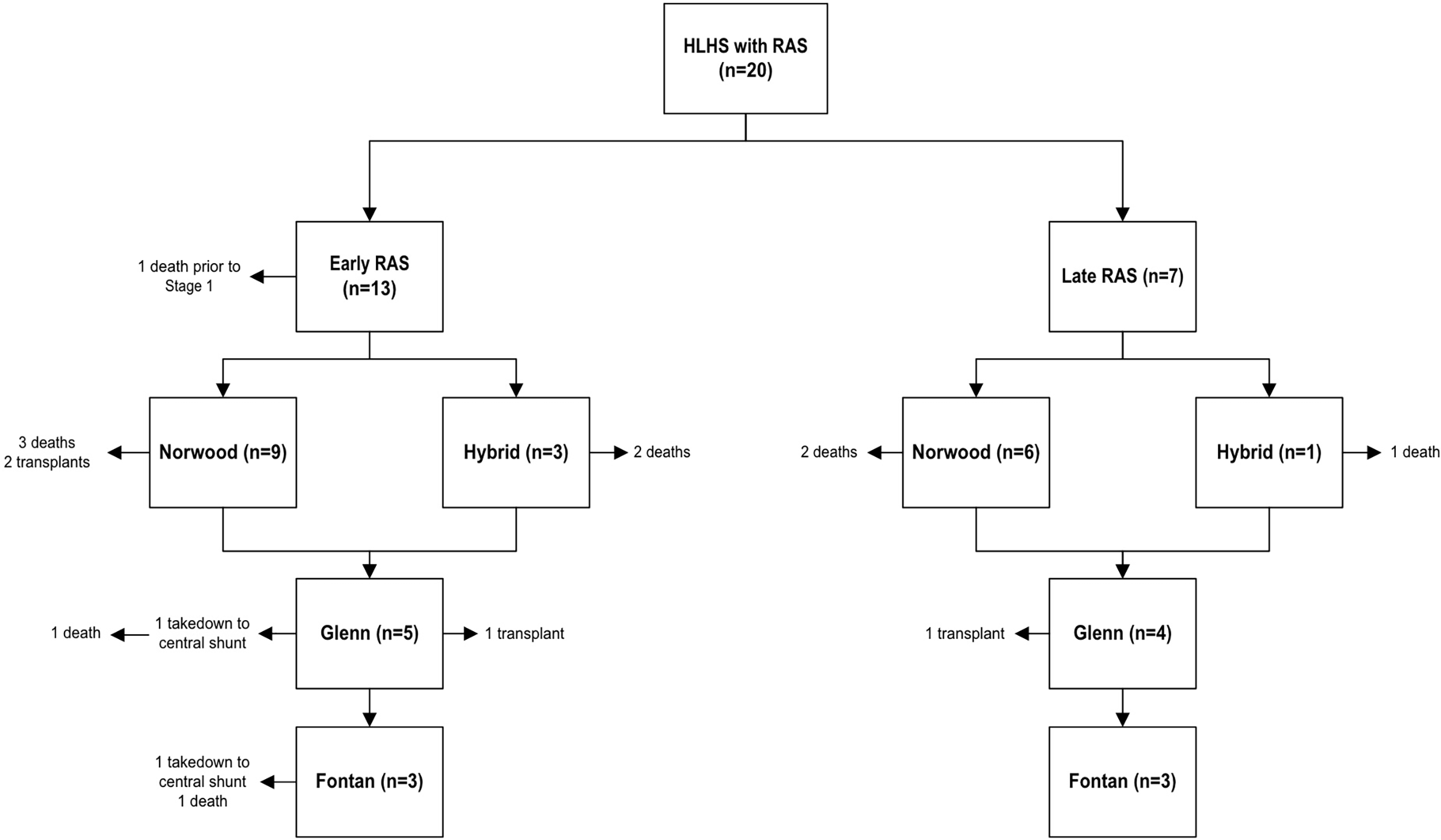
Survival for the Early group trended worse than for the Late group and the group without restriction (Figure 1). Overall long-term outcomes demonstrated increased rates of heart transplantation and overall mortality in the Early group (25% transplant, 62% mortality) compared to the Late group (0% transplant, 29% mortality) and the group without restriction (15% transplant, 40% mortality) but did not reach statistical significance (p = 0.339 for transplant, p = 0.255 for mortality). The Late group appeared to have similar clinical outcomes to the group without restriction in all comparisons, although there was no significant difference in overall survival or transplant-free survival among the 3 groups. The surgical and long-term outcomes of all patients with a restrictive atrial septum are shown in Figure 2.
Log-rank values for each graph: (a) 0.367 (b) 0.076 (c) 0.308 (d) 0.098. HLHS = Hypoplastic Left Heart Syndrome; RAS = Restrictive Atrial Septum.

In the Early group, 2 of the 3 patients who underwent hybrid palliation died; of the remaining patients, 3 progressed to Fontan and only one remains alive with Fontan. In the Late group, one patient underwent hybrid palliation and died; of the remaining, 3 progressed to Fontan and remain alive with Fontan. Abbreviations: HLHS = Hypoplastic Left Heart Syndrome; RAS = Restrictive Atrial Septum.

Discussion
Hypoplastic left heart syndrome with prenatal evidence of a restrictive atrial septum has been shown to confer worse overall outcomes compared to those without atrial restriction. Reference Connor, Arons, Figueroa and Gebbie2 Reference Glatz, Tabbutt and Gaynor9,Reference Rychik, Rome, Collins, DeCampli and Spray10 To our knowledge, ours is the largest study group to include medium- and long-term outcomes and invasive haemodynamic data in this population. Similar to previous reports, there was significantly higher 30-day mortality following stage I palliation in patients with restrictive atrial septum (26%) compared to patients without atrial restriction (6%). The timing of fetal atrial restriction diagnosis and whether this has implications for postnatal outcomes has not been previously investigated. While our data demonstrated higher rates of heart transplantation and mortality in the Early group, this difference did not reach statistical significance. Additionally, proportionally fewer patients in the Early group reached stage II and III palliation (38% and 25%, respectively) compared to the Late group (56% and 33%, respectively) and the group without restriction (66% and 36%, respectively). We hypothesise that although clinical outcomes were worse in the Early group, these values did not reach statistical significance due to small sample size.
Of the three patients with Early restriction who survived to Fontan, only one (33%) was still alive with Fontan physiology at the time of last follow-up (one died, and one required Fontan takedown). In comparison, all three patients (100%) with Late restriction who survived to Fontan were still alive with Fontan physiology at the time of last follow-up. In patients without atrial restriction, 56 survived to Fontan, of whom 49 (88%) were still alive with Fontan physiology at the time of last follow-up. These findings suggest that for patients with a restrictive atrial septum who survive beyond stage I palliation, those with Early restriction may be less successful candidates for continued staged palliation compared to those with Late restriction, which could have important implications for surgical decision-making in this unique patient population.
It is known that lung disease adversely impacts the passive pulmonary blood flow upon which stages II and III palliations rely and can even be prohibitive for these operations. Additionally, patients with atrial restriction in utero can have evidence of pulmonary lymphangiectasia on MRI, an appearance known as “nutmeg lung,” Reference Barrera, Johnson and Rychik22,Reference Saul, Degenhardt and Iyoob23 which has been shown to be an independent marker of mortality. We theorise that patients who have experienced longer periods of intra-uterine atrial level restriction and elevated left atrial pressures (i.e., Early group) experience worse outcomes following surgical transition to passive pulmonary blood flow because of this sustained in utero lung damage. Due to the time period of our study and the evolving use of fetal MRI, MRI data were not included in our study.
Prior studies evaluating fetal atrial level restriction have defined restrictive atrial septum in various ways, with some studies making a distinction between mild, moderate, and severe restriction based on pulmonary vein Doppler patterns. Reference Taketazu, Barrea, Smallhorn, Wilson and Hornberger12,Reference Gellis, Drogosz and Lu15,Reference Divanovic, Hor, Cnota, Hirsch, Kinsel-Ziter and Michelfelder17,Reference Michelfelder, Gomez, Border, Gottliebson and Franklin18,Reference Better, Apfel, Zidere and Allan24–Reference Lowenthal, Kipps, Brook, Meadows, Azakie and Moon-Grady26 We defined fetal atrial restriction as having at least one of the following findings: intact atrial septum, decompressing vein, and/or antegrade:retrograde pulmonary vein velocity time integral ratio <3, which has been reported to be highly predictive of severe neonatal instability and need for emergent postnatal intervention in this population. Reference Gellis, Drogosz and Lu15–Reference Michelfelder, Gomez, Border, Gottliebson and Franklin18 Other studies have highlighted the challenges in diagnosing atrial restriction, with velocity-time integral ratios perhaps remaining the most sensitive. Reference Marshall, Levine and Morash27 Similar to our study, the study by Jadczak et al. reported an association between earlier onset and longer duration of atrial restriction and increased neonatal mortality; Reference Marshall, Levine and Morash27 however, atrial restriction was defined by different criteria, including foramen ovale size, flow velocity across the foraman ovale, and flow reversal in the pulmonary veins. In our cohort, pulmonary vein velocity time integral ratios varied at different gestational ages for each patient, with some patients having echocardiograms that did not meet criteria for restriction following earlier echocardiograms that did meet criteria. Differences in operator technique likely played a role in this variability, though it is possible that the haemodynamic state of the fetus fluctuated throughout gestation. Regardless, our findings suggest that serial monitoring of the pulmonary vein velocity time integral ratio is likely superior to a singular value.
A growing body of literature over the past decade and a half has evaluated the role of maternal hyperoxygenation in determining the need for urgent postnatal balloon atrial septostomy in patients with a restrictive atrial septum. Reference Szwast, Tian, McCann, Donaghue and Rychik8,Reference Jadczak, Respondek-Liberska and Sokołowski28–Reference Madan, Donofrio, Szwast, Moon-Grady and Patel30 Our centre has not yet performed acute hyperoxygenation testing in fetuses with hypoplastic left heart syndrome and atrial restriction. While we agree that this can be a helpful adjunct test to help prepare for urgent neonatal intervention, there are no data correlating the long-term outcomes for these patients at the Glenn and Fontan stages, where alterations in pulmonary vascular reactivity are potentially most impactful.
Interstage haemodynamics, as determined by cardiac catheterisation, were assessed in our cohort to look for surrogate markers of lung disease and pulmonary hypertension that are typically considered contraindications to the passive pulmonary blood flow of stage II and III palliations. We found that the mean pulmonary artery pressure was significantly higher in both Early and Late groups (median 16 mmHg for both) compared to the group without restriction (median 13 mmHg). Additionally, the highest mean pulmonary artery pressures (up to 35 mmHg) were seen in the group with Early restriction. This may reflect subtle lung differences in patients with restriction, though the median values for all groups did not meet criteria for pulmonary hypertension per the revised 2023 American Heart Association guidelines. Reference Maron31 Additionally, the difference in mean pulmonary artery pressure did not reflect a difference in indexed pulmonary vascular resistance among the groups.
The identification of a restrictive atrial septum in utero for patients with hypoplastic left heart syndrome affects fetal counselling and provider/family expectations. It may also affect postnatal surgical management and influence the type of stage I palliation; more patients with atrial restriction have undergone initial hybrid palliation at our centre. Currently at our centre, patients with atrial restriction in utero are counselled similarly, with no distinction on the gestational age at which restriction is identified. Despite not meeting statistical significance, our data suggest that diagnosis of a restrictive atrial septum later in gestation may be associated with more favourable long-term, transplant-free outcomes, as the outcomes data for these patients were more similar to patients without restriction compared to those with Early restriction. This may be helpful in counselling families about expected short- and long-term prognosis depending on the timing of onset of atrial restriction.
Additionally, there is an increasing number of centres performing in-utero atrial septoplasty for fetuses with atrial restriction with variable results. Reference Taketazu, Barrea, Smallhorn, Wilson and Hornberger12,Reference Jantzen, Moon-Grady and Morris32 Given the worse long-term outcomes in patients with Early restriction, these patients may be better candidates for fetal atrial intervention, Reference Chang, Chen and Klitzner1,Reference Gillum3 although long-term outcomes of these interventions are also not well understood. Understanding the impact of the timing of in utero development of atrial restriction may be an important factor in future risk stratification for in utero intervention. Although multicenter evaluations to date have not found a significant survival benefit among those undergoing fetal intervention, Reference Moon-Grady, Morris and Belfort33 identifying subgroups of patients at higher risk for worse outcomes, such as those with Early atrial restriction, may have important clinical utility.
Limitations
This was a retrospective, single-centre study with a relatively small sample size, which limits statistical power and creates selection bias. The timing of initial fetal diagnosis was variable, and there was no standardised interval for follow-up fetal echocardiograms, which makes it difficult to determine precisely when some fetuses in our cohort developed atrial restriction. Other centres have used fetal MRI to assess for significant lung pathology (“nutmeg lung”), which may be an important independent risk factor. Because we did not routinely perform fetal MRI for this indication at our medical centre during the period of the study, this data could not be included in our analysis.
In conclusion, it is well known that hypoplastic left heart syndrome with evidence of fetal atrial restriction portends worse outcomes; however, the impact of the gestational age at which atrial restriction develops is not well studied or understood. While our small, single-centre study did not show a statistically significant difference in overall survival or transplant-free survival between patients with Early compared to Late gestation diagnosis of restrictive atrial septum, the data suggest that patients who develop atrial restriction later in gestation may have better long-term outcomes (similar to those without restriction) than patients who develop restriction earlier in gestation. Future multi-centre studies should prospectively investigate the impact of timing of onset of fetal atrial restriction with standardised fetal echocardiographic protocols and fetal lung MRI to help guide optimal management strategies for this unique population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S104795112611316X.
Acknowledgements
None.
Competing interests
None.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Ethical Standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines.
Ethical review and approval were waived for this study, as only deidentified compliant data were used in the analysis. Patient consent was waived due to the retrospective nature of the study. All the information being collected was part of routine care.




 Open access
Open access