


Impact statement
This systematic review addresses a critical blind spot in global mental health: the wellbeing of the family caregivers who provide most of the care for people with severe mental health conditions in low- and middle-income countries (LMICs). Drawing on evidence from 76 qualitative studies, it brings caregivers’ voices to the forefront and highlights the immense emotional, social and economic pressures they endure within largely unsupported home environments. The review traces caregivers’ journeys from early confusion and fear to hard-won resilience grounded in faith, peer connections and efforts to maintain the person’s place within family life. It also shows how systemic neglect shifts responsibility for care almost entirely onto families, disproportionately onto women. Importantly, it documents what caregivers say they urgently need: accessible information, involvement in treatment decisions, practical skills, peer support networks and financial relief. By amplifying the voices of caregivers, this review challenges global mental health approaches that rely on family care without investing in structures that sustain it. While existing efforts focus on treating the person with severe mental health conditions, this research demonstrates that the home environment is the primary setting for recovery in many LMICs. The findings make a compelling case for shifting from individual-focused clinical models toward family centered interventions that improve recovery environments at home while reducing caregiver burnout and isolation. They call for approaches that recognize family caregiving as both gendered and economically consequential. Supporting the family unit can be a cost-effective strategy to close the mental health treatment gap in LMICs and advance broader goals of health equity, gender justice and social inclusion.
Introduction
Severe mental health conditions (SMHCs), such as schizophrenia and bipolar disorder, are often chronic and result in significant impairment in one or more areas of functioning (Vigo et al., Reference Vigo, Thornicroft and Atun2016; Asher et al., Reference Asher, Abebaw, Solomon, Md, Soumitra and Hanlon2017; Forthal et al., Reference Forthal, Fekadu, Medhin, Selamu, Thornicroft and Hanlon2019; Smartt et al., Reference Smartt, Ketema, Frissa, Tekola, Birhane, Eshetu, Selamu, Prince, Fekadu and Hanlon2021). Without adequate treatment and support, these impairments are often exacerbated (Fekadu et al., Reference Fekadu, Medhin, Lund, DeSilva, Selamu, Alem, Asher, Birhane, Patel, Hailemariam, Shibre, Thornicroft, Prince and Hanlon2019). Contemporary treatment approaches reflect the biopsychosocial understanding of mental illness, incorporating both biological and psychosocial interventions (Gaebel and Zielasek, Reference Gaebel and Zielasek2015). However, these interventions are not universally accessible. Globally, the mental health treatment gap is substantial, but it is particularly acute in low- and middle-income countries (LMICs), where up to 90% of individuals may lack effective treatment (WHO Team: Mental Health BH, and Substance Use, 2024).
Research from high-income countries (HICs) has extensively documented the emotional, social and economic burdens faced by caregivers of people with SMHCs and demonstrated the effectiveness of family interventions in reducing burden and improving outcomes (Hayes et al., Reference Hayes, Hawthorne, Farhall, O’Hanlon and Harvey2015; Bighelli et al., Reference Bighelli, Rodolico, García-Mieres, Pitschel-Walz, Hansen, Schneider-Thoma, Siafis, Wu, Wang, Salanti, Furukawa, Barbui and Leucht2021; Sin et al., Reference Sin, Elkes, Batchelor, Henderson, Gillard, Woodham, Chen, Aden and Cornelius2021; Rodolico et al., Reference Rodolico, Bighelli, Avanzato, Concerto, Cutrufelli, Mineo, Schneider-Thoma, Siafis, Signorelli, Wu, Wang, Furukawa, Pitschel-Walz, Aguglia and Leucht2022). These findings have informed clinical guidelines in HIC settings (NICE, 2014; Ventriglio et al., Reference Ventriglio, Ricci, Magnifico, Chumakov, Torales, Watson, Castaldelli-Maia, Petito and Bellomo2020). However, evidence from HICs cannot illustrate the scale or nature of family caregiving experience in LMICs. In LMIC, contexts with limited social security systems and scarce biomedical mental health services, families provide almost all ongoing care, becoming the de facto primary support (Tirfessa et al. Reference Tirfessa, Lund, Medhin, Hailemichael, Fekadu and Hanlon2019). Cultural norms, family structures, health system constraints and greater reliance on traditional and religious healing practices further shape distinct caregiver experiences (Mendenhall et al., Reference Mendenhall, De Silva, Hanlon, Petersen, Shidhaye, Jordans, Luitel, Ssebunnya, Fekadu, Patel, Tomlinson and Lund2014; Brandon and Kohrt, Reference Brandon and Kohrt2015; Patterson et al., Reference Patterson, Edwards, Vakili, Abu-Hassan, Wampler, Rastogi and Singh2020).
Although research on caregiver experiences in LMICs is growing, existing reviews have important limitations. Quantitative syntheses offer data on the magnitude of burden but fail to capture nuanced lived experiences and support needs (Andualem et al., Reference Andualem, Melkam, Tadesse, Nakie, Tinsae, Fentahun, Rtbey, Medfu and Gm2024). Existing qualitative reviews, meanwhile, are highly restricted in scope. Geographically, these syntheses are largely confined to single regions, such as the Middle East (Alyafei et al., Reference Alyafei, Alqunaibet, Mansour, Ali and Billings2021) or sub-Saharan Africa (Ntsayagae et al., Reference Ntsayagae, Poggenpoel and Myburgh2019). Thematically, other reviews narrowly focused on singular dimensions of caregiving, such as economic burden (Addo et al., Reference Addo, Agyemang, Tozan and Nonvignon2018; Kisangala et al., Reference Kisangala, Mbivnjo, Webb, Barrett, Rukundo, Namisango and Heslin2024), or stigma (Yin et al., Reference Yin, Li and Zhou2020), missing the holistic caregiving experience.
Therefore, a critical knowledge gap remains: to our knowledge, no global systematic review has synthesized qualitative evidence on the multifaceted experiences, needs and priorities of caregivers across the diverse cultural and health-system contexts of LMICs worldwide. This qualitative systematic review addresses this gap by synthesizing available qualitative evidence on the lived experiences of family caregivers of people with SMHCs in LMICs. By generating a deeper, cross-contextual understanding, this synthesis aims to provide a foundational evidence base to inform the development of feasible, culturally appropriate and effective family interventions tailored to local LMIC realities.
Methods
We followed the ENhancing Transparency in REporting the synthesis of Qualitative research statement to enhance transparency in reporting the synthesis of qualitative research (Tong et al., Reference Tong, Flemming, McInnes, Oliver and Craig2012). The protocol was prospectively registered with PROSPERO (CRD420250654264).
Condition or domain being studied
The domains of interest were: (1) the lived experiences of families caring for a family member with SMHC and (2) families’ perceived needs and priorities for intervention. Family caregivers can be parents, spouses, siblings, adult children or extended family members who provide unpaid, informal care to a relative diagnosed with an SMHC. Studies focusing on nonfamily informal caregivers (such as neighbors, community members or traditional healers) or formal, paid caregivers were excluded. The search terms used to capture the condition of interest, family and the study setting are listed in Supplementary File S1.
We searched the following databases from 2013 up to February 7, 2025: CINAHL, Embase, ERIC (Ebsco), Global Health, Global Index Medicus, PsycINFO, PubMed, Scopus and Web of Science. We included studies published from 2013 onward to align with the adoption of the first WHO Comprehensive Mental Health Action Plan (2013–2030) (WHO Team: Mental Health BH, and Substance Use (MSD), 2021). This timeframe allowed us to capture recent evidence that was not included in previous reviews. The search strategy combined controlled vocabularies and keywords related to severe MHCs (e.g., “severe mental illness,” schizophrenia); family caregivers (e.g., parent, spouse, caregiver), qualitative research (e.g., qualitative study, opinions, meanings) and standard terminology for LMICs, as defined by the World Bank (2024). There were no search restrictions by language. The full search strings used are provided in Supplementary File S1.
Eligibility criteria
We included primary qualitative studies (i.e. ethnography, phenomenology, grounded theory) that utilized established qualitative methods for data collection and analysis (such as thematic, phenomenological or content analysis). Participants included family caregivers of individuals diagnosed with SMHCs, regardless of the duration of the illness. For this review, SMHCs were operationally defined to include affective and nonaffective psychoses (schizophrenia and bipolar disorder), as well as broad classifications of ‘severe mental illness’ as defined by the authors of the primary studies. Eligible studies focused on caregiving experiences, coping mechanisms, challenges and support needs within LMICs. We excluded book chapters, reviews, editorials and conference abstracts.
Data extraction and study quality assessment
All retrieved citations were imported into Rayyan software (Ouzzani et al., Reference Ouzzani, Hammady, Fedorowicz and Elmagarmid2016), where duplicates were removed. Title and abstract screening was conducted as a single-rating process, with the total yield of citations divided among five independent reviewers. To ensure high consistency and mitigate the limitations of single screening, the team held extensive calibration meetings before screening to align on the eligibility criteria. Reviewers adopted a conservative, inclusive approach during this phase; any citation deemed ambiguous or unclear was automatically retained for full-text assessment. Full-text articles of potentially relevant studies were subsequently retrieved and assessed for final eligibility. Uncertainties or disagreements were resolved through team discussion and consultation with a senior reviewer. Reasons for exclusion at the full-text stage were documented in Rayyan and reported in the PRISMA flow diagram.
To further ensure methodological rigor and verify that the eligibility criteria were applied consistently across the team, we conducted a collaborative pilot of the data extraction process. All five reviewers independently extracted data from the first 20% of the included studies using a collaboratively developed, standardized extraction sheet. The team then held a consensus meeting where reviewers presented their extractions, discussed their experiences and resolved any challenges. This exercise not only refined the usability of the extraction tool but also served as a rigorous check of our shared understanding of the inclusion criteria. After finalizing the extraction sheet, individual reviewers extracted data from their assigned remaining studies. The prepiloted form captured key study characteristics, including author, year of publication, country, aim, population, phenomenon of interest, context, methods and main findings.
The methodological quality of the included studies was independently assessed by the reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Qualitative Research (Lockwood et al., Reference Lockwood, Munn and Porritt2015). This assessment evaluated the alignment between research methods and questions, the representation of participants’ voices and the rigor of data analysis. While this appraisal informed our overall interpretation of the findings, no studies were excluded based on quality scores alone. The detailed rating for each item on the quality appraisal checklist is presented in Supplementary File S2.
Strategy for data synthesis
All included full-text articles were uploaded to NVivo (version 14) for data management and analysis. To clarify the scope of our data extraction, we specifically coded the “Findings/results” sections of the included articles. This encompassed both first-order constructs (direct quotations from family caregivers) and second-order constructs (the primary authors’ analytical interpretations and summaries).
We conducted a thematic synthesis following the established approach described by Thomas and Harden (Reference Thomas and Harden2008). Our interpretation was guided by a phenomenological
theoretical framework to ensure the synthesis remained grounded in the nuanced, lived experiences of the participants. The synthesis involved three distinct stages:
-
1. Line-by-line coding: The primary reviewer applied inductive codes to the extracted text.
-
2. Development of descriptive themes: These initial codes were grouped into broader, descriptive categories based on similarities and shared meanings.
-
3. Generation of analytical themes: We synthesized the descriptive categories to generate new interpretative findings that directly addressed our research question.
To ensure analytical rigor and depth, two reviewers shared the coding responsibilities. Initially, these two reviewers independently coded a subset of 10 articles and subsequently held a consensus meeting to compare their codes and processes. This collaborative exercise was designed to enrich the coding process. By combining their complementary perspectives, the reviewers were able to capture a more comprehensive and nuanced range of codes during the initial phase.
This exercise informed the development of a robust initial codebook. The two reviewers then utilized this codebook to code the remaining articles, holding frequent discussions with the wider research team to refine codes and resolve any discrepancies. Finally, a lived-experience expert, who is a member of the review team, reviewed the categories and analytical themes, contributing their insights to the final interpretation of the findings.
Authors’ reflexivity
Throughout the review process, the research team engaged in continuous reflexive practice to acknowledge and mitigate how our respective biases and positionalities influenced data interpretation. While our funder provided feedback on methodological milestones through weekly and biweekly meetings, they had no role in data analysis, theme generation or the interpretation of findings, ensuring the team’s analytical independence.
Our core team comprised individuals with diverse backgrounds in psychology, psychiatry, mental health systems research and lived experience of psychosis. We explicitly recognized that our clinical backgrounds (psychology and psychiatry) inherently predisposed us to view caregiver burden through a biomedical lens, potentially leading us to overemphasize symptom management and clinical deficits. To counter this, team consensus meetings were used to actively challenge these clinical biases. These deliberations helped us ensure that the sociocultural, economic and structural realities of caregiving in LMICs were elevated in the coding process. The mental health systems researchers on our team helped contextualize these burdens within the broader landscape of LMIC health system constraints.
Findings
Characteristics of included studies
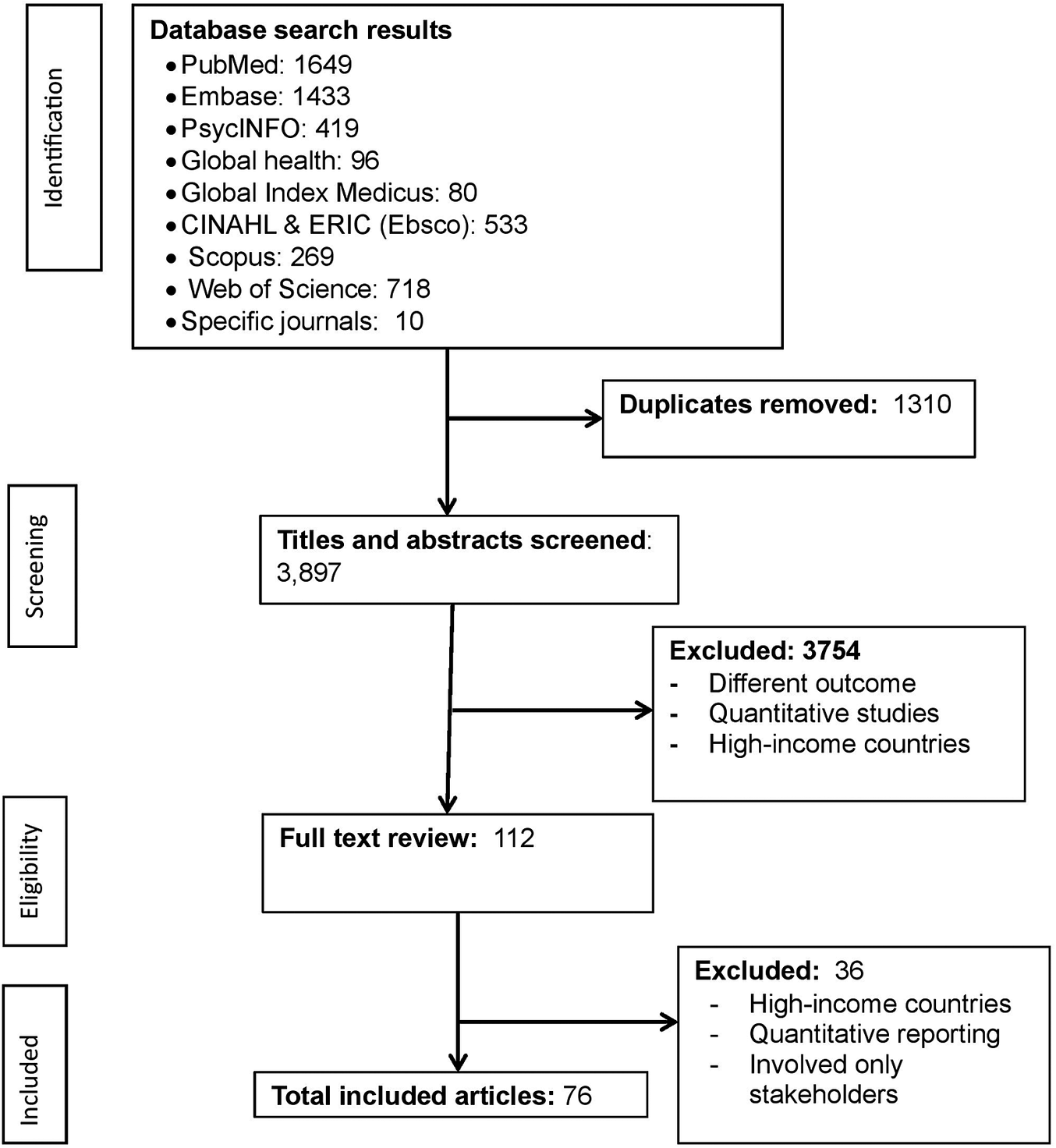
A total of 76 (n = 76) articles met the inclusion criteria (Figure 1). Descriptions of all included studies are presented in Supplementary File S2. The included studies covered a range of geographical and cultural settings, originating from all six WHO regions (Table 1). The largest number of studies came from the South-East Asia Region (20 studies), followed by the Eastern Mediterranean Region (17 studies), the African Region (14 studies), the Western Pacific Region (11 studies), the European Region (8 studies) and the Region of the Americas (6 studies).
PRISMA flow diagram.

Figure 1. Long description
At the top, a box lists database search results: PubMed 1649, Embase 1433, PsycINFO 419, Global health 96, Global Index Medicus 80, C I N A H L and E R I C (Ebsco) 533, Scopus 269, Web of Science 718, Specific journals 10. An arrow points right to a box: Duplicates removed 1310. A downward arrow leads to Titles and abstracts screened 3897. To the right, a box: Excluded 3754, with reasons: Different outcome, Quantitative studies, High-income countries. Downward arrow to Full text review 112. To the right, a box: Excluded 36, with reasons: High-income countries, Quantitative reporting, Involved only stakeholders. Downward arrow to Total included articles 76. The left margin labels each stage: Identification, Screening, Eligibility, Included.
Number of articles included in the review from the WHO regions

Table 1. Long description
From the top row, South-East Asia Region includes India and Indonesia with 20 studies. Next, Eastern Mediterranean Region covers Iran, Oman, and Pakistan with 17 studies. African Region lists Ethiopia, Ghana, Nigeria, South Africa, Tanzania, Uganda, and Zimbabwe with 14 studies. Western Pacific Region includes China, Malaysia, and Thailand with 11 studies. European Region contains Turkey with 8 studies. Region of the Americas includes Brazil, Colombia, and Mexico with 6 studies. The table shows a descending trend in study count from South-East Asia Region to Region of the Americas.
Among the 76 included studies, eight focused on a single-family caregiver group such as mothers (n = 2), spouses (n = 1), siblings (n = 3) or children (n = 2). The rest of the studies included a mix of two or more family member types, such as a mix of parents, spouses and siblings, some extending to children or other relatives. The majority of the included articles (72.2%, n = 55) focused on participants diagnosed with schizophrenia. Smaller proportions of the studies included individuals with bipolar disorder (13.9%, n = 10) or participants broadly categorized as having a severe mental illness (13.9%, n = 11). The included articles were conducted across a variety of settings. One-third of the articles (33.3%) reported data collected in outpatient psychiatric services, 30.2% in community settings, 22.2% were in inpatient psychiatric facilities and 14.3% of studies on mixed settings that combined both community and clinical environments (Supplementary File S2).
Sixty-one articles (80%) used in-depth interviews as the primary data collection method, while seven studies used focus group discussions. A small number of studies employed combined methods (n = 7), and only one study utilized observation as a data collection approach. Across the included studies, thematic analysis was the most frequently used analytical approach (30 studies), followed by content analysis (18 studies). A smaller number of studies applied Interpretative Phenomenological Analysis (7 studies), Framework analysis (4 studies) and Grounded Theory (4 studies). The remaining studies (n = 13) used other or unspecified qualitative analysis methods.
Quality appraisal using the JBI Critical Appraisal Checklist for Qualitative Research indicated that most included studies (85%, n = 65) were rated “YES” on items assessing coherence between the stated philosophical perspective, research methodology, research questions, data collection, analysis and interpretation of findings (Supplementary File S2). In contrast, aspects of researcher reflexivity were consistently underreported. Only 30% (n = 23) of studies explicitly described the researcher’s cultural or theoretical positioning, and fewer than one-third (25%, n = 19) addressed the potential influence of the researcher on the research process and participants (Supplementary File S2).
Overview of themes
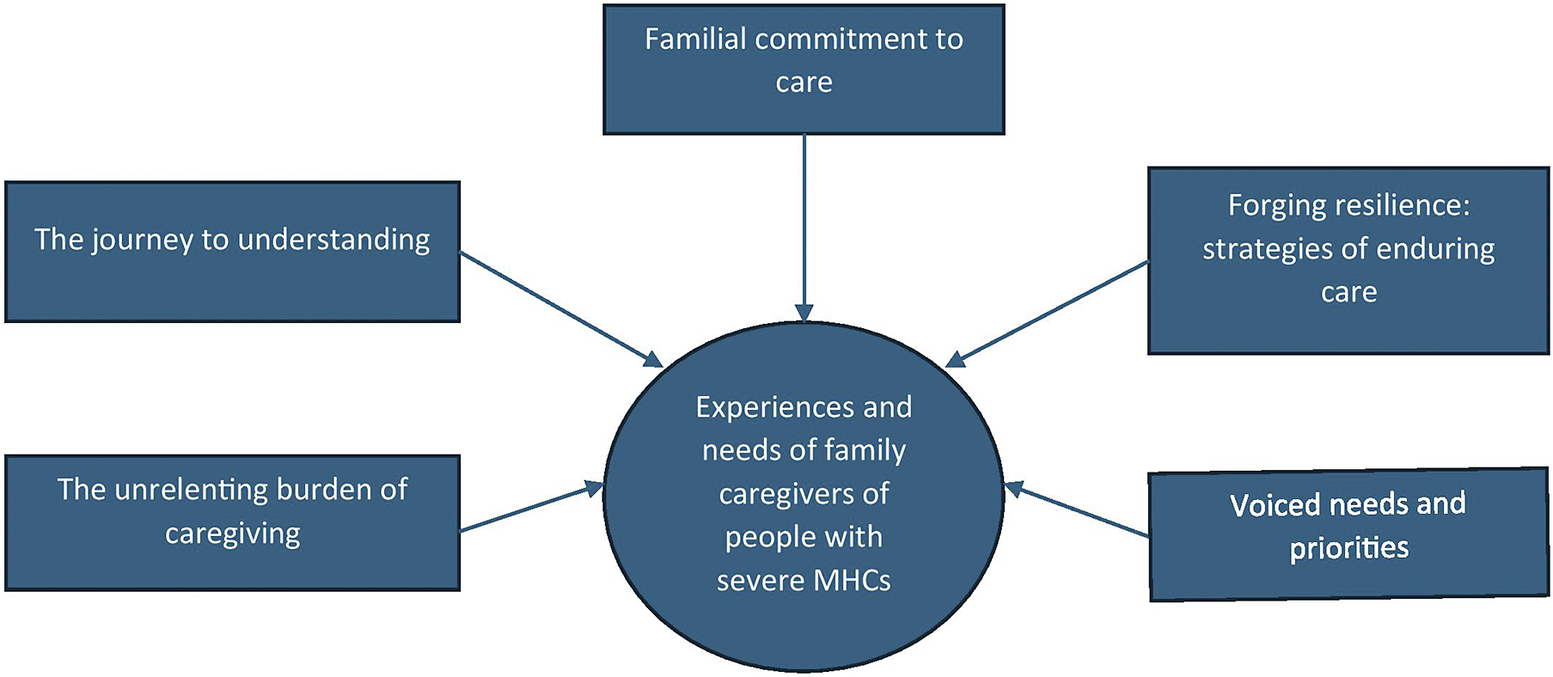
Family caregivers described a multifaceted caregiving journey shaped by their evolving understanding of the illness, daily caregiving demands and the social and structural environments in which care took place. Thematic synthesis yielded five interconnected themes (Figure 2): (1) the journey to understanding the illness, (2) family commitment to care, (3) the unrelenting burden of caregiving, (4) strategies to forge resilience and (5) voiced needs and priorities. Initially, family caregivers embarked on a complex journey to make sense of the condition, which subsequently shaped their deep commitment to providing care. However, assuming the lion’s share of this responsibility exacted a significant emotional, social and economic toll on these families. Despite these profound challenges, family caregivers developed coping mechanisms and resilience to sustain both themselves and their relatives with SMHCs. Finally, emerging from these complex lived experiences are the clearly defined support needs and priorities of the family caregivers. The following sections provide a detailed narrative account of each theme.
Conceptual map of the themes describing the experience of family caregivers of people with severe mental health conditions in LMICs.

Journey to understanding the illness
This theme describes the dynamic and laborious process families undergo to make sense of the illness, moving from deep confusion to hard-won, experiential expertise. The caregiving journey typically begins with uncertainty, as families struggle to name and interpret bewildering symptoms, often turning to spiritual or traditional explanations (Olwit et al., Reference Olwit, Musisi, Leshabari and Sanyu2015; Khadem et al., Reference Khadem, Shahidi, Zarani and Panaghi2022; Dijkxhoorn et al., Reference Dijkxhoorn, Padmakar, Bunders and Regeer2023). As one mother recalled, “People said he was bewitched… I was in a state of confusion” (Olwit et al., Reference Olwit, Musisi, Leshabari and Sanyu2015). Early signs are commonly misinterpreted as personal failings, and this disorientation is intensified by the systemic failure of the formal (biomedical) health system to provide clear information or nonjargon explanations, leaving families isolated and unprepared (Bellini et al., Reference Bellini, Soares Cunha, Fernandes Cardoso da Silva and Ciccone Giacon2016; Pan et al., Reference Pan, Li, Jin and Lu2024). As one caregiver lamented, “No, he [the doctor] never clarified it to me… Neither there, nor here, nor anyone [explained]” (Bellini et al., Reference Bellini, Soares Cunha, Fernandes Cardoso da Silva and Ciccone Giacon2016).
Faced with this informational void, families embarked on a desperate search for help. They navigated a fragmented landscape that spans biomedical facilities, traditional healers and religious institutions (Nuraini et al., Reference Nuraini, Tumanggor, Hungerford, Lees and Cleary2021; Verity et al., Reference Verity, Turiho, Mutamba and Cappo2021). The hospital often serves as a last resort. This search itself is costly and tiring, forcing caregivers into a role they are unprepared for: “I had to take on the role of family caregiver without being ready” (Pan et al., Reference Pan, Li, Jin and Lu2024). Over time, this self-directed effort fosters a pragmatic, experiential expertise in daily management, characterized by active problem-solving. Families start to adjust routines, define roles and responsibilities and involve the person with the illness (Akgül Gök and Duyan, Reference Akgül Gök and Duyan2020; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025): “Once he takes his medicine … his brothers take him to his job” (Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025).
Receiving a diagnosis often brings devastating news, unleashing grief, anxiety and despair that can even push caregivers to contemplate self-harm (Bai et al., Reference Bai, Luo, Wang, Guan, Zhong, Sun and Tang2020; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025). This sorrow is primarily centered on mourning the loss of the future envisioned for their family member, such as missed educational milestones, career prospects and opportunities to build their own family (Liu and Zhang, Reference Liu and Zhang2020; Fekadu et al., Reference Fekadu, Craig, Hanlon, Mayston and Fekadu2024; Pan et al., Reference Pan, Li, Jin and Lu2024). A father mourned, “She was a very good student… I would have grandchildren by now” (Fekadu et al., Reference Fekadu, Craig, Hanlon, Mayston and Fekadu2024 ). For primary caregivers who are spouses of the person, the change in roles fundamentally transforms relationships, often replacing romantic love with a sense of compassionate duty or pity: (Rahmani et al., Reference Rahmani, Ebrahimi, Seyedfatemi, Namdar Areshtanab, Ranjbar and Whitehead2018; Hasanpour et al., Reference Hasanpour, Poortaghi, Zare, Yahyavi and Shahsavari2024) “My love… turned to this feeling of pity… for the sake of God” (Rahmani et al., Reference Rahmani, Ebrahimi, Seyedfatemi, Namdar Areshtanab, Ranjbar and Whitehead2018).
Familial commitment to care
This theme focuses on the profound motivation that sustains caregiving. At the core of caregiving lies a strong moral imperative, kinship and communal duty to sustain efforts amid sacrifices and absent reciprocity. Caregiving is not framed as a choice but as an inherent, defining moral duty attached to the caregiver’s identity as a parent, sibling or spouse (Liu et al., Reference Liu, Hsiao, Chen, Shiau and Hsieh2022). It transcends personal wellness: “How could I give up? He is my son. I have a duty” (Liu et al., Reference Liu, Hsiao, Chen, Shiau and Hsieh2022). External social pressure reinforces this perceived duty, as failing to provide care can lead to harsh community judgment and social condemnation (Read and Nyame, Reference Read and Nyame2019). One caregiver explained: “……People will be talking against you… you are not trying your best” (Read and Nyame, Reference Read and Nyame2019).
Commitment to care often manifests in exhausting labor; endless vigilance over meals, hygiene, medications and ensuring protection from harm. One participant described the scope of their duties: “I have to do everything for my son… supervise everything from eating to taking medicine” (Tamizi et al., Reference Tamizi, Fallahi-Khoshknab, Dalvandi, Mohammadi-Shahboulaghi, Mohammadi and Bakhshi2020). The continuous supervision severely limits caregivers’ mobility, autonomy and capacity to earn an income, resulting in lost livelihoods and consumption of personal time (Gloria et al., Reference Gloria, Osafo, Goldmann, Parikh, Nonvignon and Kretchy2018; Demissie et al., Reference Demissie, Hanlon, Ng, Fekadu and Mayston2021). The cost of caregiving often has a ripple effect, leading to neglect of other healthy family members (Karaca et al., Reference Karaca, Şener and Kundakçi2024). One study noted the children of caregivers often “received little care or interest from the healthy parent who undertakes the care of their spouse and therefore is tired and fails to care for their children” (Karaca et al., Reference Karaca, Şener and Kundakçi2024).
To endure these pressures, families actively negotiate responsibility. Support gathered manifests as role sharing, shared emotional burden and long-distance practical aid from extended relatives (Amaresha et al., Reference Amaresha, Venkatasubramanian and Muralidhar2019; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025; Sari and Duman, Reference Sari and Duman2025). A caregiver shared, “Whenever I fall into despair, my elder sister… gets me into shape” (Sari and Duman, Reference Sari and Duman2025). However, this negotiation is highly gendered, with the primary, day-to-day emotional and practical work falling almost exclusively to women, particularly mothers (Attepe Özden and Tuncay, Reference Attepe Özden and Tuncay2018). One mother stated, “All in all, the father works. He goes in the morning and returns in the evening. In addition, our child is female. It’s me [who] cares more” (Attepe Özden and Tuncay, Reference Attepe Özden and Tuncay2018). This structural dynamic often results in mothers bearing the brunt of day-to-day care, transforming the “family” unit into the “mother” alone (Read and Nyame, Reference Read and Nyame2019; Kanungpiarn et al., Reference Kanungpiarn, Tungpunkom, Kantaruksa and Chaloumsuk2021). Lack of support can also be fraught with conflict, where pleas for help are met with criticism rather than assistance: “My husband… blames me, saying I’m not doing a good enough job” (Pan et al., Reference Pan, Li, Jin and Lu2024). Another mother felt her only remaining support was divine: “I have no man except God” (Read and Nyame, Reference Read and Nyame2019).
The unrelenting burden of caregiving
The caregiving role can exact a substantial and multidimensional toll that threatens the caregiver’s emotional stability, financial security and social life. For many, the emotional landscape is characterized by a relentless cycle of worry, sadness, frustration and guilt (Jack-Ide et al., Reference Jack-Ide, Uys and Middleton2013; Marimbe et al., Reference Marimbe, Cowan, Kajawu, Muchirahondo and Lund2016). A caregiver shared their experience, “I have sleepless nights… worsened my high blood pressure” (Jack-Ide et al., Reference Jack-Ide, Uys and Middleton2013). The daily grind of repetitive, often unappreciated tasks fuelled a sense of helplessness and led to a feeling of being trapped in the caregiving cycle (Bedoya Hernandez and Builes Correa, Reference Bedoya Hernandez and Builes Correa2013; Wulandari et al., Reference Wulandari, Keliat and Susanti2024). Erosion of identity and a paradoxical mix of deep love and resentment were reported as a result of the constant pressure of caregiving. Families expressed anger and guilt that are directed both inward and outward (Saville Young and Flannigan, Reference Saville Young and Flannigan2021; Kalayci et al., Reference Kalayci, Uzunaslan and Uzunaslan2023). Chronic strain shatters the peace of the home, leading some to regret their relational choices or contemplate divorce (Asher et al., Reference Asher, Abebaw, Solomon, Md, Soumitra and Hanlon2017; Kargar et al., Reference Kargar, Faghihi and Nazari2021). For some, the exhaustion and hopelessness reach a point where they express desperate wishes for the death of their loved one, or contemplate ending their own lives, compounded by deep anxiety over the future of their family member with psychosis (Peng et al., Reference Peng, Ma and Ran2022; Lohrasbi et al. Reference Lohrasbi, Maghsoudi, Alavi and Akbar2024; Soni and Kumar, Reference Soni and Kumar2024).
Caregivers described a sense of alienation from their relative. A spouse reported feeling as though she was “dealing with a stranger” (Al-Sawafi et al., Reference Al-Sawafi, Lovell, Renwick and Husain2021). Intimacy was transformed into functional exchanges: “I can’t communicate…[I] just give him the medicine” (Rahmani et al., Reference Rahmani, Ebrahimi, Seyedfatemi, Namdar Areshtanab, Ranjbar and Whitehead2018). In some families, communication breakdowns fuelled irritability that further strained family interactions. One participant acknowledged this cycle: “I get easily irritated …‥and that affects my interactions with people” (Mbadugha et al., Reference Mbadugha, Ogbonnaya, Iheanacho, Omotola, Ogbonna and Anetekhai2023). Paradoxically, crises are reported to also deepen bonds: “After I became sick, I… bared my heart to my mother… Now, we had a good relationship” (Attepe Özden and Tuncay, Reference Attepe Özden and Tuncay2018).
The caregiving burden indicates not only personal strain but also the absence of support, often driving families into financial collapse. The simultaneous difficulties faced by the person in work and the caregiver’s need to provide constant supervision can force the caregiver to abandon their livelihoods, plunging families into debt and precarity: “Now I don’t work. All my time is used up” (Soni and Kumar, Reference Soni and Kumar2024). Economic devastation accompanied a loss of social connection. For some families, the all-consuming nature of caregiving led to total confinement and isolation, trapping caregivers and forcing younger family members to abandon their own aspirations to support the household (Tamizi et al., Reference Tamizi, Fallahi-Khoshknab, Dalvandi, Mohammadi-Shahboulaghi, Mohammadi and Bakhshi2020; Saville Young and Flannigan, Reference Saville Young and Flannigan2021; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025). One sibling lamented, “when my mom got sick, I became their mother” (Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025). For some, the erosion of oneself felt like being “a butterfly who has been trapped in a spider’s web” (Rahmani et al., Reference Rahmani, Ebrahimi, Seyedfatemi, Namdar Areshtanab, Ranjbar and Whitehead2018).
The unpredictability of the illness in some individuals necessitated a state of constant hypervigilance, transforming the home into a site of potential danger (Gloria et al., Reference Gloria, Osafo, Goldmann, Parikh, Nonvignon and Kretchy2018; Kanungpiarn et al., Reference Kanungpiarn, Tungpunkom, Kantaruksa and Chaloumsuk2021; Hasanpour et al., Reference Hasanpour, Poortaghi, Zare, Yahyavi and Shahsavari2024). Caregivers reported living with the constant, often realized, threat of physical violence, verbal abuse and property destruction (Demissie et al., Reference Demissie, Hanlon, Ng, Fekadu and Mayston2021; Neha et al., Reference Neha, Gandhi, Manjula and Padmavathi2021; Nuraini et al., Reference Nuraini, Tumanggor, Hungerford, Lees and Cleary2021; Putri et al., Reference Putri, Afrizal, Hamidi and Effendy2022). Managing high-risk behaviors defined the caregiving experience for many. In the absence of external support, families often resort to desperate and coercive measures like physical restraint to prevent harm (Verity et al., Reference Verity, Turiho, Mutamba and Cappo2021; Ilmy et al., Reference Ilmy, Windarwati, Noorhamdani and Wijaya2022).
Stigma is another pervasive burden that imposes social isolation and exclusion. Caregivers may internalize society’s negative attitudes, leading to deep feelings of shame and embarrassment (Read and Nyame, Reference Read and Nyame2019; Akgül Gök and Duyan, Reference Akgül Gök and Duyan2020; Sawab et al., Reference Sawab, Fitryasari, Pujiastuti and Putra2023). Families protect themselves from ridicule and social condemnation by employing a conscious strategy of concealment (Al-Sawafi et al., Reference Al-Sawafi, Lovell, Renwick and Husain2021; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025). Disclosure often leads to social rejection and isolation, where family and friends withdraw support (Chen et al., Reference Chen, Zhao, Tang, Jin, Liu, Zhao, Chen and Lu2019; Karaca et al., Reference Karaca, Şener and Kundakçi2024). Most consequentially, stigma creates a deep fear for the future, tainting the reputation of the entire family and actively hindering the marital and professional prospects of healthy siblings (Kargar et al., Reference Kargar, Faghihi and Nazari2021; Latifian et al., Reference Latifian, Raheb, Uddin, Abdi and Alikhani2022; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025). While families often stood as a united front against public stigma, the home was not always a safe space for people with severe MHCs. Exclusion within the home is often manifested as a lack of genuine intimacy and connection with the person (Rahmani et al., Reference Rahmani, Ebrahimi, Seyedfatemi, Namdar Areshtanab, Ranjbar and Whitehead2018), active distancing by relatives who are not primary caregivers (Kalayci et al., Reference Kalayci, Uzunaslan and Uzunaslan2023) and avoidance of the person in social events (Latifian et al., Reference Latifian, Raheb, Uddin, Abdi and Alikhani2022).
Forging resilience: strategies of enduring care
Family caregivers actively forged diverse coping pathways characterized by psychological adjustment, resource mobilization within the family and tenacious commitment. A foundational strategy involved a cognitive shift toward pragmatic acceptance of the enduring nature of the illness, which is framed as a necessary step to reduce anger and denial (Hailegabriel and Berhanu, Reference Hailegabriel and Berhanu2023; Pan et al., Reference Pan, Li, Jin and Lu2024). Active problem-solving and the search for knowledge were born out of this acceptance (Akgül Gök and Duyan, Reference Akgül Gök and Duyan2020). For many, acceptance is deeply intertwined with religious faith, which provides a framework for understanding suffering, offers emotional solace through prayer and allows caregivers to view their role as a divine test (Iseselo et al., Reference Iseselo, Kajula and Yahya-Malima2016; Gumilang, Reference Gumilang2023). The process often involves lowering expectations for a complete cure, providing a measure of peace (Kanungpiarn et al., Reference Kanungpiarn, Tungpunkom, Kantaruksa and Chaloumsuk2021; Pan et al., Reference Pan, Li, Jin and Lu2024). For example, in Thailand, this was framed as tamjai (reconciliation to a situation), a conscious adjustment of one’s mindset to the reality of lifelong caregiving, guided by the philosophy that “Whatever happens, happens” (Kanungpiarn et al., Reference Kanungpiarn, Tungpunkom, Kantaruksa and Chaloumsuk2021).
Resilience is actively fortified through relational resources, especially connecting with peers who share the lived experience (Bademli and Lök, Reference Bademli and Lök2020; Liu and Zhang, Reference Liu and Zhang2020). As one young caregiver explained: “…There is no one who understands me, there are attendants [family caregivers] in the hospital, it makes me feel good to talk to them. Because we understand each other …” (Bademli and Lök, Reference Bademli and Lök2020). Furthermore, families actively seek to involve the person in daily routines and adapted work. This strategy served both as a therapeutic endeavor to counter idleness and relapse and as a powerful means of cultivating a renewed sense of purpose (Budiarto and Mustikasari, Reference Budiarto and Mustikasari2024; Fitryasari et al., Reference Fitryasari, Nurlela, Syadiyah, Yusuf, Maliah, Ambarwati, Mulud, Diba and Sari2024). Involving the person in tailored tasks is reported to affirm the individual’s value as a contributor to the family (Yunita et al., Reference Yunita, Yusuf, Nihayati and Hilfida2020; Fitryasari et al., Reference Fitryasari, Nurlela, Syadiyah, Yusuf, Maliah, Ambarwati, Mulud, Diba and Sari2024; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025; Sari and Duman, Reference Sari and Duman2025).
Despite the challenges, the shared struggle is reported as a catalyst for personal growth, deepened relational bonds and empathetic transformation (Bellini et al., Reference Bellini, Soares Cunha, Fernandes Cardoso da Silva and Ciccone Giacon2016; Saville Young and Flannigan, Reference Saville Young and Flannigan2021; Mbadugha et al., Reference Mbadugha, Ogbonnaya, Iheanacho, Omotola, Ogbonna and Anetekhai2023). A sibling shared his experience: “… I would say his illness brought me close to him.” (Saville Young and Flannigan, Reference Saville Young and Flannigan2021) Caregivers reported gaining a deeper insight into mental illness and developing an appreciation for small, incremental progress, finding gratitude and companionship where others might only see burden (Wulandari et al., Reference Wulandari, Keliat and Susanti2024). A mother said: “….She[her daughter] didn’t want to take a shower or get out of bed, but all praise to God, now….she can wipe her own pants” (Wulandari et al., Reference Wulandari, Keliat and Susanti2024).
While families demonstrate remarkable resilience, some coping mechanisms born of desperation can become maladaptive. Two prominent maladaptive pathways that emerged from the data were the inequitable and unsustainable burden of gendered care and the use of coercive, overcontrolling measures to manage risk. Leaving the brunt of care to women risks burnout of the primary caregiver and can create fractured, blaming family dynamics (Read and Nyame, Reference Read and Nyame2019; Pan et al., Reference Pan, Li, Jin and Lu2024). The desperate use of coercive and overcontrolling measures such as constant scrutiny, forced medical compliance or physical restraint was reported as counterproductive. It often resulted in renewed conflict, shattered trust and inflicted further trauma (Soni and Kumar, Reference Soni and Kumar2024; Heydarikhayat et al., Reference Heydarikhayat, Darban and Farokhzadian2025).
Voiced needs and priorities
Family caregivers expressed a strong need for broad and consistent support in several key areas. They prioritized getting clear and practical information about the illness: what it is, what causes it, how it might progress over time and how it can be treated (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015; Kumar et al., Reference Kumar, Sood, Verma, Mahapatra and Chadda2019). A caregiver shared… “Don’t know how long he has to take tablets” (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015). Caregivers need specific training on practical management skills, including effective communication strategies to de-escalate difficult situations and tips for recognizing early warning signs (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015; Özgönül and Bademli, Reference Özgönül and Bademli2022). A brother asked, “I know he has a problem, but I cannot control myself… I need some tips in talking with my brother patiently” (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015). Their informational needs also include guidance to counter misinformation within the family and address concerns such as whether the illness may be hereditary (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015).
Beyond simply receiving information, families called for their active and respectful participation in the care and treatment process (Asgari et al., Reference Asgari, Adib, Nayeri and Rezayat2023). They expressed their frustration with a healthcare system that sidelines their expertise and excludes them from critical decision-making (Akgül Gök and Duyan, Reference Akgül Gök and Duyan2020). They demanded a collaborative relationship where their unique insights are valued, and they are not instrumentalized or deceived by professionals (Zarei et al., Reference Zarei, Zeighami and Javadi2021). A participant described being directed by a physician to deceive their mother: “Do not use a child as a tool to take a mother to a physician. The physician should not use the child and ask him/her to tell lies” (Zarei et al., Reference Zarei, Zeighami and Javadi2021).
Family caregivers also articulated the need for psychosocial support to combat the deep sense of isolation stemming from community and extended family withdrawal (Fauziah et al., Reference Fauziah, Balqis, Obar, Suryadin and Chairunisa2024). One caregiver shared their plea for solidarity from their kin: “Well, we want our relatives to be able to provide support, don’t just ignore it, besides being ignorant, avoid it too” (Fauziah et al., Reference Fauziah, Balqis, Obar, Suryadin and Chairunisa2024). The absence of solidarity in some families not only increased the workload of primary carers but also added emotional strain. A powerful, recurring need was for peer support groups, which were seen as essential for mutual understanding, reducing alienation and building solidarity (Vargas-Huicochea et al., Reference Vargas-Huicochea, Berenzon, Rascon and Ramos2018). Systemic needs include calls for professional counseling, legal support and broader interventions to fight societal stigma (Oz et al., Reference Oz, Duran and Incedere2022; Hailegabriel and Berhanu, Reference Hailegabriel and Berhanu2023).
Another need expressed was robust financial assistance to mitigate the crippling economic burden (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015; Zarei et al., Reference Zarei, Zeighami and Javadi2021; Hailegabriel and Berhanu, Reference Hailegabriel and Berhanu2023). The financial strain arises from the simultaneous loss of income and the high cost of effective treatment, often forcing families to choose between basic necessities and medication (Amaresha et al., Reference Amaresha, Joseph, Agarwal, Narayanaswamy, Venkatasubramanian, Muralidhar and Subbakrishna2015; Hailegabriel and Berhanu, Reference Hailegabriel and Berhanu2023). Caregivers called for financial solutions from governmental or nongovernmental bodies, advocating specifically for support that enables access to affordable and better medications with fewer side effects (Chen et al., Reference Chen, Zhao, Tang, Jin, Liu, Zhao, Chen and Lu2019; Lohrasbi et al. Reference Lohrasbi, Maghsoudi, Alavi and Akbar2024).
Discussion
This systematic review synthesized evidence from 76 qualitative studies, offering an understanding of the family caregiving experience for people with severe MHCs in diverse LMIC contexts. Our review consolidates evidence that outlines a complex caregiving journey, most often characterized by moral commitment, with substantial personal burden, systemic resource scarcity, and, for some, emerging resilience. We also highlight the differential impact of caregiving on family members and pinpoint key needs to guide global mental health efforts.
Our findings illustrated a wide range of experiences associated with the caregiving role. Caregivers’ efforts to understand the illness, which involved moving from initial uncertainty to learning through lived experience, align with existing literature (Kuipers et al., Reference Kuipers, Kuipers, Leff and Lam2002). In many of the studies included in this review, families shouldered most of the care responsibilities in the absence of adequate formal support. This heavy reliance on family care often led to competing demands between caregiving and livelihood, contributing to financial strain, job loss and emotional exhaustion. The cumulative social and economic pressures experienced by families in these settings were often more severe than those described in high-income contexts (Attepe Özden and Tuncay, Reference Attepe Özden and Tuncay2018; Pedersen et al., Reference Pedersen, Smallegange, Coetzee, Hartog, Turner, Jordans and Brown2019; Abayon et al., Reference Abayon, Raymonds, Brahmbhatt, Samnani and Hanna2024; Oluwole and Obadeji, Reference Oluwole and Obadeji2025). Across many LMIC settings, strong family ties and a deep sense of moral and relational duty were central in sustaining care for people with severe MHCs. However, the nature and intensity of this commitment can vary across cultural, social and economic contexts (Brandon and Kohrt, Reference Brandon and Kohrt2015). The findings showed how the context of caregiving transforms an otherwise universal family value into a potentially overwhelming obligation.
Our review also highlighted the heavily gendered nature of caregiving. Mothers and other female relatives were routinely expected to shoulder most responsibilities, while men were typically portrayed as less involved in daily care tasks. A recent review from Ethiopia also reported similar findings (Tesfaye and Demelash, Reference Tesfaye and Demelash2025). This imbalance can lead to caregiver burnout and, in some cases, strain family relationships or stability (Sharma et al., Reference Sharma, Chakrabarti and Grover2016; Attepe Özden and Tuncay, Reference Attepe Özden and Tuncay2018). However, there are reports where caregiver gender is not always a significant predictor of negative caregiving outcomes (Sharma et al., Reference Sharma, Chakrabarti and Grover2016). Nevertheless, the accounts of family caregivers in this qualitative review are overwhelmingly from female caregivers. Social expectations, cultural norms and limited formal support could place disproportionate responsibility on women. Interventions that fail to account for these gendered dynamics risk overlooking a key source of fragility in the family based care in many LMIC settings. Future initiatives should therefore aim to better support women caregivers and promote more equitable sharing of caregiving responsibilities.
Across the studies, stigma emerged as a deeply embedded and multidimensional force, yet its mechanisms showed specific variations compared to HIC literature. While stigma by association is well-documented in HICs (Corrigan and Miller, Reference Corrigan and Miller2004), our review highlighted how stigma in LMIC settings often threatens the social capital of the entire family unit. Its effect ranges from internalized shame, community rejection, to institutional barriers that constrained education, employment and marriage opportunities for the entire family (Schomerus and Angermeyer, Reference Schomerus and Angermeyer2008). In many contexts, families described living under the weight of social judgment, where fear of being identified with a mental illness fostered secrecy and delayed help-seeking. Although the expression and consequences of stigma can vary across cultural and economic settings, its effects are consistently detrimental. Addressing stigma, therefore, requires locally grounded strategies that engage with community leaders and recognize the intersection of social exclusion and economic poverty.
Despite the challenges in caregiving, families often demonstrated remarkable resilience. Caregivers drew on faith, peer connections and structured daily routines to find meaning, sustain hope and strengthen family bonds. Such adaptive strategies countered the dominant language of “burden” with stories of growth and purpose within adversity (Saville Young and Flannigan, Reference Saville Young and Flannigan2021). However, this resilience coexists with distressing reports of coercion, restraint and concealment. These responses were often signals of desperation in the face of overwhelming circumstances and limited alternatives. Coercive measures underscore the urgent need for accessible, humane and adequately resourced care options that enable families to protect both their relatives’ dignity and their own wellbeing (Onwumere et al., Reference Onwumere, Zhou and Kuipers2018).
The lived experiences described above reinforce the need for supportive, family focused interventions. Our synthesis identified several intervention targets grounded in caregivers’ realities. A primary gap is basic, comprehensible information about the illness: its nature, causes, likely course and treatment options. Participants in the included studies expressed a need for collaborative, respectful care with jargon-free education about the illness. This needs to focus on practical skills, like symptom management, relapse prevention and conflict resolution (Sin et al., Reference Sin, Gillard, Spain, Cornelius, Chen and Henderson2017). Health care providers must also address maladaptive coping, such as physical restraint or concealment. Alongside access to mental health care, families could be equipped with alternatives to coercion, such as de-escalation techniques (Onwumere et al., Reference Onwumere, Zhou and Kuipers2018). Families emphasized the importance of being treated as partners whose lived knowledge is valued. Involving them meaningfully in treatment planning and discharge decisions has been shown to improve medication adherence and reduce relapse rates (Chatterjee et al., Reference Chatterjee, Naik, John, Dabholkar, Balaji, Koschorke, Varghese, Thara, Weiss, Williams, McCrone, Patel and Thornicroft2014).
Caregivers also highlighted the value of strengthening relational resilience and the benefits of family to-family networks and support groups. These can alleviate isolation, promote shared learning and provide emotional uplift (Bademli and Duman, Reference Bademli and Duman2014). Equally critical are access to available opportunities with no barriers and providing financial support. The economic devastation from caregiving demands more than education. Policymakers need to recognize that reliance on family for all caregiving drives poverty. Solutions like disability grants could cover income gaps and medication costs (Parker-Grewe, Reference Parker-Grewe2017). A recent comprehensive review commissioned by UNICEF reported that cash transfer programs for families in Africa increased hopefulness, decreased feelings of shame and greater autonomy (Novignon et al., Reference Novignon, Palerm, Prencipe, Neijhoft and Rogers2025). Integrating support with income-generating programs or vocational training, especially for women, might reduce dependency on the care recipient’s finances. Finally, legal protections are essential. These should safeguard the assets and rights of both the person with psychosis and their caregivers, particularly in marital or property disputes.
Strengths and limitations
Strength of this review is the inclusion of 76 studies exclusively from LMICs, providing the necessary depth and contextual focus to inform global policy. The use of thematic synthesis allowed us to move beyond descriptive summaries to generate high-level, analytical themes of commitment, burden and resilience. Furthermore, the inclusion of a multidisciplinary research team ensured that our interpretations remained deeply grounded in the realities of caregiving rather than relying solely on clinical or systemic lenses.
However, several limitations must be acknowledged. First, grouping vastly diverse nations under the broad economic designation of “LMICs” inherently masks significant intra- and inter-regional differences in culture, religion, family structures and health system infrastructures. While our synthesis identified common, cross-cutting themes, local adaptation and cultural tailoring remain essential before applying these findings to specific intervention designs. Second, as noted in our quality appraisal, many of the primary studies lacked explicit researcher reflexivity. The failure of primary authors to interrogate their own theoretical or cultural positioning may have influenced the depth and framing of the original data we extracted. Third, the dominant qualitative narrative in the primary literature is heavily deficit-focused. Because research questions frequently center on “burden” and “challenges,” the positive dimensions of caregiving are likely underrepresented in this synthesis. Finally, the literature search for this review concluded in February 2025. While this represents a comprehensive synthesis of the qualitative literature up to that point, studies published in the subsequent months are not reflected in this analysis; however, given the large volume of included studies (n = 76), thematic saturation was robustly achieved.
Conclusion
Evidence from diverse LMIC settings finds common themes of caregiving as a tenacious moral commitment sustained despite systemic neglect and pervasive stigma. While social and economic assistance remains important, family caregivers also emphasized that access to quality mental healthcare would make their situations manageable. In particular, family focused interventions and consistent clinical guidance were seen as essential yet often unavailable. Without these supports, the financial pressures, social isolation and caregiver exhaustion can become even more severe. A more effective response requires strengthening routine mental health services, providing targeted support to families and addressing the wider social and economic conditions that shape the caregiving experience.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10224.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10224.
Data availability statement
The data that support the findings of this study are available from the corresponding author, DK, upon reasonable request.
Acknowledgments
Charlotte Hanlon (CH) was funded by an NIHR global health research group on homelessness and mental health in Africa (HOPE; NIHR134325). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care, England. CH, DS and EF were funded by the Wellcome Trust through grants 222154/Z20/Z (SCOPE). CH was additionally supported by Wellcome grant 223615/Z/21/Z (PROMISE). For the purposes of open access, the author has applied a Creative Commons Attribution (CC BY) licenselicence to any Accepted accepted aAuthor mManuscript version arising from this submission.
Author contribution
All authors contributed to the conceptualization of the study. DK designed the methodology and research protocol, conducted the literature search and data extraction, oversaw all stages of the review process and led manuscript writing and submission. WF managed communication with WHO staff, contributed to the literature search and data extraction and supported the synthesis of findings and discussion and manuscript review. AM ensured methodological rigor, managed articles from each database and contributed to study design and adherence to review procedures. AS contributed to writing the discussion, particularly policy implications, managed articles from each database and reviewed the manuscript. SX contributed to the literature search and data extraction, provided specific support for publications in Chinese languages and reviewed the manuscript. YT contributed as a person with lived experience reviewer and assessed the sensitivity and interpretation of findings from draft to final manuscript. CH oversaw overall study activities, reviewed the protocol and report drafts and provided critical input to the final manuscript. AA, LD, AMG, AMa and AF reviewed the study protocol, report drafts and the final manuscript.
Financial support
This work was commissioned by the WHO through funding from Wellcome Trust (grant number 77448).
Competing interests
None.


 Open access
Open access