

1  Alprazolam
Alprazolam
Deprescribing
When and Why to Deprescribe (or Consider Deprescribing)
Alprazolam, a potent yet short-acting benzodiazepine, may have risks when used long term. Its potential for dependence, particularly due to its rapid onset and short duration, makes deprescribing an essential consideration in certain scenarios. Clinicians should consider:
When there’s evidence of dependence or abuse: Alprazolam’s short half-life can lead to dose escalation and dependence. Tolerance, withdrawal symptoms, and frequent dosing should prompt clinicians to consider tapering, as the risk of dependence may outweigh the benefits
When opioids are prescribed or needed concurrently: Combining alprazolam with opioids greatly increases the risk of sedation, respiratory depression, and overdose. If opioid therapy is needed, deprescribing alprazolam should be strongly considered to avoid potentially fatal interactions
When there’s evidence of cognitive impairment or falls: If patients present with cognitive decline or a history of falls, alprazolam should be reconsidered. Benzodiazepines can contribute to these issues, particularly in older adults, raising the risk of serious injury or worsening cognitive function
When there’s significant impulsivity: In individuals who have significant impulsivity, benzodiazepines, including alprazolam, may perpetuate disinhibition. These individuals should be re-evaluated for deprescribing
When there’s a co-occurring nonpsychiatric disorder: In some patients, benzodiazepines may worsen comorbid chronic medical conditions or perpetuate specific symptoms, such as in COPD
When the patient is pregnant, considering becoming pregnant, or breastfeeding: In general, benzodiazepines should be avoided in pregnancy and discussions related to minimizing unnecessary medication exposure should begin prior to conception. Also, benzodiazepines should be avoided in nursing women
When long-term efficacy is limited: Controlled studies do not support the long-term use of alprazolam beyond 12 weeks. In cases where patients have been on alprazolam for extended periods, especially beyond a year, reassessment of ongoing need is important, as benefits beyond short-term use are difficult to establish
Reassess at every visit: For patients on long-term alprazolam, ongoing reassessment at every visit is essential. Evaluating dependence, cognitive effects, and alternative treatments – such as SSRIs, SNRIs, or psychotherapy – can guide deprescribing efforts and may identify opportunities to deprescribe
Withdrawal
Before benzodiazepine use, excitatory glutamatergic signaling and inhibitory GABAergic signaling are balanced. Benzodiazepines, through increasing GABAA receptor activity, increase inhibitory effects. Importantly, with prolonged use, compensatory downregulation and desensitization of GABAA receptors occur. Then, upon benzodiazepine discontinuation, these adaptations transiently persist, resulting in reduced GABAergic signaling and unopposed glutamatergic activity. This excitatory–inhibitory imbalance (Figure 1.1) likely underlies withdrawal and rebound symptoms such as anxiety, agitation, insomnia, and, in severe cases, seizures. These synaptic changes highlight the neuropharmacological basis for careful tapering to mitigate withdrawal effects
Neurobiology of chronic alprazolam treatment and withdrawal. Following administration of alprazolam, GABAA receptors (purple and cream) are downregulated and glutamate receptors (brown and tan) are upregulated. The GABAA receptors later become less sensitive because of allosteric uncoupling between GABA and the benzodiazepine binding site. Chronic alprazolam use (central panel) also decreases GABAA subunit expression (padlock) and increases endocytosis (and subsequent degradation) of GABAA receptors (purple and cream receptor inside circle). In the right panel, these cellular changes, including persistent decreased GABAA receptor expression and hyperexcitability to glutamate, drive benzodiazepine withdrawal symptoms.

Figure 1.1 Long description
The three-panel diagram depicts changes in GABA and glutamate receptors at the synapse during pre-benzodiazepine, chronic benzodiazepine, and post-benzodiazepine phases. The left panel, labelled pre-benzodiazepine, features four GABA-A receptors and a glutamate receptors, several checkmarks, a glutamate, and GABA receptor. The middle panel, labelled chronic benzodiazepine, contains two GABA-A receptors, and three glutamate receptors, with glutamate and GABA, with a benzodiazepine molecule interacting with a locked receptor, and unchanged checkmarks. The right panel, labelled post-benzodiazepine, retains the same elements with two GABA-A and glutamate receptors each, the key and receptor are disconnected, and the checkmarks remain. A legend below the panels identifies receptor types and neurotransmitters. GABA-A receptor, glutamate receptor, GABA, glutamate, and benzodiazepine.
Withdrawal Symptoms
Withdrawal symptoms from benzodiazepines usually emerge within 2–3 days after stopping the medication and can persist for 10–14 days or even longer. However, the onset and duration can vary significantly depending on the specific benzodiazepine. For instance, withdrawal from benzodiazepines with short half-lives such as alprazolam generally begin within 24 hours and often as early as 6 hours after the last dose if a patient is taking regular or high doses (Figure 1.2)
Even brief use of benzodiazepines, as short as 2 weeks, can lead to withdrawal seizures upon abrupt discontinuation
Patients with mild withdrawal symptoms often recover without medical intervention. However, those experiencing severe withdrawal symptoms, such as delirium or seizures, may face life-threatening complications if not treated promptly
Seizures can occur as soon as 24 hours after stopping alprazolam, but they may also arise up to a week or more later
Specific withdrawal symptoms include:
The life-threatening complications of benzodiazepine withdrawal are varied and necessitate vigilant monitoring and intervention:
◦ Agitation: The most common symptom, occurring in the majority of cases
◦ Psychosis: 2–7% of cases; can manifest as hallucinations, delusions, or bizarre behavior
◦ Seizures: 1 in 25 patients, typically generalized tonic–clonic seizures that are isolated and self-limited. However, nonconvulsive status epilepticus can develop, particularly in older adults
If the hyperadrenergic state or seizures are prolonged or multiple, additional severe complications can arise, including:
◦ Volume depletion
◦ Respiratory dysfunction
◦ Hypoglycemia
◦ Rhabdomyolysis
◦ Acute kidney injury
◦ Cardiac dysfunction
◦ Cerebral edema
◦ Hepatic injury
As benzodiazepines are discontinued, clarify what symptoms may be related to medication withdrawal or worsening of the underlying disorder:
◦ Assess how current symptoms differ from the original disorder being treated
◦ Assess specific symptoms unique to withdrawal
◦ Assess the timing of symptoms – how quickly did they emerge after stopping or decreasing the dose of alprazolam?
◦ Assess whether the symptoms are like those experienced when the patient missed medication doses
Withdrawal of short and long half-life benzodiazepines. The typical withdrawal course for alprazolam (a short-acting benzodiazepine) is shown in green dotted line.
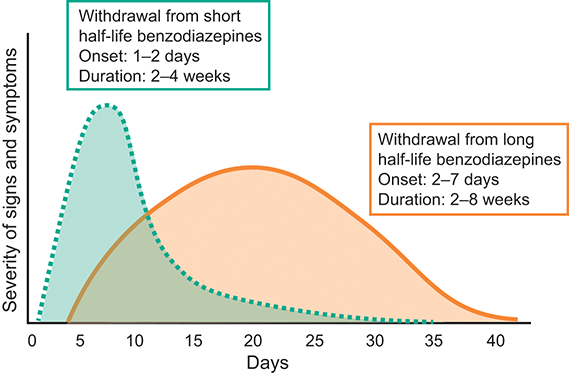
Figure 1.2 Long description
The x-axis of the graph is labelled in days from zero to forty and the y-axis indicating severity of withdrawal symptoms. A curve represents short half-life benzodiazepines, depicting onset at one to two days and duration of two to four weeks. Another curve represents long half-life benzodiazepines, with onset at two to seven days and duration of two to eight weeks. The first curve peaks earlier and higher, while the second curve rises gradually and lasts longer.
Withdrawal Type
Differentiating Withdrawal Symptoms from Relapse
Symptoms associated with relapse and withdrawal symptoms are given in Table 1.1

Table 1.1 Long description
The table has 2 columns: Relapse and Withdrawal symptoms. It reads as follows. Relapse: Anxiety, panic attacks; Depressed mood or irritability; Agitation, restlessness; Dizziness, lightheadedness; Palpitations. Withdrawal symptoms: Perceptual disturbances; Depersonalization; Hallucinations or formication; Sensory hypersensitivity; Muscle twitching, fasciculations; Tinnitus; Confusion, disorientation, delirium.
Discontinuation
Benzodiazepine withdrawal symptoms are common, particularly when scheduled alprazolam is stopped abruptly
The timing of withdrawal symptoms is influenced by the half-life and lipophilicity of the benzodiazepine and is particularly pronounced for alprazolam
According to the 2025 Joint Clinical Practice Guideline on Benzodiazepine Tapering, dose reductions should generally not exceed 25% every 2 weeks (American Society of Addiction Medicine, 2025). For patients with significant withdrawal symptoms, this guideline recommends even smaller, consistent reductions to enhance tolerability and reduce distress
While most benzodiazepine tapers can be managed in outpatient settings, inpatient care should be considered when: (1) there is imminent risk from continued use (e.g., overdose, drug interactions, falls, or suicidality); and (2) psychiatric or medical comorbidities may complicate the taper beyond what can be managed in an outpatient setting
The 2025 Joint Clinical Practice Guideline on Benzodiazepine Tapering also recommends inpatient or medically managed residential care for patients with severe or complex withdrawal. These settings allow for monitoring (e.g., vital signs, structured assessments) and seizure risk evaluation/intervention
The use of very long-acting agents such as phenobarbital for benzodiazepine withdrawal are recommend only in inpatient/medically monitored residential settings and only when managed by clinicians with specific expertise. This approach may be useful in highly refractory cases but carries inherent risks requiring close monitoring and experience
Acute Discontinuation
Acute discontinuation is NOT recommended, particularly from high doses
Acute discontinuation – especially from high doses – may lead to agitation, psychosis, delirium, and seizures, in addition to autonomic instability
Psychosis may occur with abrupt discontinuation at high doses and can manifest as hallucinations, delusions, or bizarre behavior
Slow Discontinuation
Slower discontinuation is preferred to avoid withdrawal effects and has been studied extensively. In fact, a meta-analysis of benzodiazepine discontinuation studies found that slow discontinuation increased the likelihood of successful discontinuation nearly six-fold (Parr et al., Reference Parr, Kavanagh, Cahill, Mitchell and Young2009)
When benzodiazepines are used for sleep, rebound insomnia is common, but the risk of rebound insomnia is decreased when benzodiazepines are tapered (Gillin et al., Reference Gillin, Spinweber and Johnson1989). Additionally, there is a higher risk for rebound insomnia associated with drugs with shorter half-lives (e.g., triazolam) versus those with longer half-lives (Soldatos et al., Reference Soldatos, Dikeos and Whitehead1999). As such, the likelihood of rebound insomnia increases when benzodiazepines are taken at higher versus lower doses (Watson et al., Reference Watson, Benca and Krystal2023)
A 25% per week taper has been preferred by many clinicians, although slower discontinuation rates (e.g., 10% per week) have been studied. In one prospective study of short versus long half-life benzodiazepines, a 25% reduction was initially attempted; however, if tapering was intolerable, patients could slow the rate. Ninety percent of patients experienced mild to moderate withdrawal, but 32% of those on long half-life and 42% on short half-life benzodiazepines could not taper (Schweizer et al, Reference Schweizer, Rickels, Case and Greenblatt1990). In this study, the most difficulty occurred in the last half of the taper
Despite the common recommendation to decrease by 10–25% every several weeks, many patients do not tolerate this, and discontinuation must be done much more slowly. In some patients, this process may take 6–12 months
Personality traits, particularly high neuroticism, female sex, and mild-to-moderate alcohol use, predict withdrawal severity (Schweizer et al., Reference Schweizer, Rickels, Case and Greenblatt1990), even with slow tapering
The approach to discontinuation may be informed by clinical factors (Table 1.2)
An example of discontinuation for alprazolam is shown in Table 1.3
In some situations, it may be necessary to convert alprazolam to a benzodiazepine with a longer duration of action to facilitate discontinuation. In this situation, chlordiazepoxide and diazepam both represent good options (Figure 1.3)

Table 1.2 Long description
The table has 2 columns: Current dose and Suggested tapering. It reads as follows. Row 1. Current dose: Low or moderate dose and no concerns for benzodiazepine use disorder. Suggested tapering: Taper total daily dose by 20 to 25 percent weekly based on response and tolerability. Row 2. Current dose: Extended or high-dose therapy, or suspected benzodiazepine use disorder. Suggested tapering: Taper daily dose by approximately 10 percent every 1 to 2 weeks based on response, tolerability, and individual patient factors. It may be possible to reduce the dose more rapidly initially and then, as the taper continues, to slow the rate of discontinuation.
| Step | WeeksFootnote * | Alprazolam dose (mg/day) |
|---|---|---|
| 0 | 0 | 4.0 |
| 1 | 1−2 | 3.5 |
| 2 | 2−4 | 3.0 |
| 3 | 4−6 | 2.5 |
| 4 | 6−8 | 2.0 |
| 5 | 8−10 | 1.5 |
| 6 | 10−12 | 1.0 |
| 7 | 12−14 | 0.5 |
| 8 | 14−16 | 0.25 |
* May be 2- or 2–4-week intervals depending on the clinical situation. In general, it is advisable to wait until withdrawal symptoms have resolved prior to moving to the next step in the tapering process.
Algorithm for benzodiazepine discontinuation, including a step involving transition from alprazolam to an alternative benzodiazepine.

Figure 1.3 Long description
The flowchart detailing a tapering strategy for benzodiazepine use, beginning with a decision point on whether the initial benzodiazepine is alprazolam. It includes steps to convert to a long-acting benzodiazepine at one hundred to one hundred twenty-five per cent of the current dose, followed by dose reductions of ten per cent weekly or biweekly. Multiple decision points assess response, with repeated conversion and tapering steps. If response is not maintained, adjunctive agents such as S G As, valproic acid, pregabalin, buspirone, trazodone, and C B T are suggested.
Rating Scales for Monitoring Discontinuation
Clinicians may consider several measures, including the Clinical Institute Withdrawal Assessment for Benzodiazepines (CIWA-B) (Busto et al., Reference Busto, Sykora and Sellers1989) and the Benzodiazepine Withdrawal Symptom Questionnaire (Tyrer et al., Reference Tyrer, Murphy and Riley1990)
The CIWA-B scale (see the Appendix for the full scoring system) is a critical tool in assessing and managing benzodiazepine withdrawal. Developed to provide a systematic and quantifiable approach, the CIWA-B scale helps clinicians accurately gauge the severity of withdrawal symptoms, ensuring timely and appropriate intervention
The CIWA-B scale was developed to address the need for a standardized method of assessing benzodiazepine withdrawal. Modeled after the CIWA scale used for alcohol withdrawal, it incorporates specific symptom categories relevant to benzodiazepine withdrawal
The CIWA-B scale covers several critical symptom domains that are commonly affected during benzodiazepine withdrawal, including anxiety, sensory disturbances, headaches, autonomic symptoms, and gastrointestinal distress. Symptoms are rated on a scale from 0 (none) to 4 (severe). The scale is designed to accurately capture the severity of each symptom, and the total score is the sum of the individual symptom scores, providing an overall measure of withdrawal severity. This approach allows for precise monitoring and comparison over time
The CIWA-B scale’s total score guides clinical interpretation and subsequent management strategies:
◦ Mild withdrawal (score 0–20): Typically managed with outpatient tapering and close monitoring. Patients in this category often experience mild anxiety, sensory disturbances, and mild autonomic symptoms that can be effectively managed with a gradual tapering schedule and supportive care
◦ Moderate withdrawal (score 21–40): May require more intensive monitoring, potentially in a structured outpatient or inpatient setting. Patients may exhibit more pronounced anxiety, significant sensory disturbances, and moderate autonomic hyperactivity. In these cases, adjunctive medications such as gabapentin or pregabalin can be employed to mitigate symptoms
◦ Severe withdrawal (score > 40): Usually necessitates inpatient management with close supervision and possibly adjunctive medications to manage severe symptoms and prevent complications such as seizures. Patients in this category are at high risk for severe autonomic dysregulation, pronounced anxiety, and potential seizures. Inpatient settings provide the necessary environment for intensive monitoring and rapid intervention
Risk Factors for Discontinuation Symptoms
Longer treatment: In some studies, patients who have been treated for longer than 12 months are at the highest risk for developing moderate withdrawal symptoms and, when attempting to stop diazepam, between 15% and 44% of patients will experience significant withdrawal symptoms (Hood et al., Reference Hood, Norman, Hince, Melichar and Hulse2014)
Higher dose (Rickels et al., Reference Rickels, Schweizer, Case and Greenblatt1990)
Concurrent use or cessation of other substances or medications
Abrupt discontinuation/rapid tapering
History of withdrawal symptoms when patients have missed doses
Expectation of negative events
Anxiety disorder
High awareness of bodily sensations (i.e., interoception)
Adjunctive Strategies during Discontinuation
For insomnia, consider cognitive behavioral therapy for insomnia (CBT-I) or adding melatonin, hydroxyzine, orexin receptor antagonists, or, in pediatric patients, clonidine. For patients experiencing rebound insomnia while discontinuing alprazolam, part of the struggle may not be purely pharmacological – it’s also behavioral. The act of taking something at bedtime can become a conditioned cue for sleep. Rather than abruptly eliminating this ritual, substituting a bridge intervention can make the transition smoother. One option is chamomile tea, which contains apigenin, a flavonoid that binds to benzodiazepine receptors and promotes sedation. This not only maintains the bedtime habit but also provides a mild natural sleep aid, reinforcing sleep onset without pharmacological hypnotics. The key is to preserve the sleep ritual while discontinuing alprazolam, allowing the brain to recalibrate both behaviorally and neurochemically
For anxiety, consider relaxation strategies, H1 antagonists, etc.
For nausea, consider ondansetron
For headaches, consider acetaminophen or NSAIDs and hydration
Several studies suggest that buspirone, pregabalin, trazodone, and divalproex can be used to facilitate successful discontinuation of benzodiazepines
Switching
How to Switch
Consider using the equivalent doses in Table 1.4 to convert from the alprazolam dose to the dose of the new benzodiazepine
In patients taking benzodiazepines for insomnia, a randomized, double-blind study (N = 24) found that switching them to zopiclone before discontinuation of hypnotics resulted in better sleep parameters as measured by polysomnography and actigraphy, as well as self-report (Pat-Horenczyk et al., Reference Pat-Horenczyk, Hacohen, Herer and Lavie1998)

Table 1.4 Long description
The table has 2 columns: Benzodiazepine and Approximate equivalent dosage (milligrams). It reads as follows. Alprazolam: 0.5. Chlordiazepoxide (Librium): 25. Clobazam (Onfi): 15. Clonazepam (Klonopin): 0.5. Diazepam (Valium): 10. Lorazepam (Ativan): 1. Chlorazepate (Tranxene): 15. Oxazepam (Serax): 20. Temazepam (Restoril): 20. Triazolam: 0.5.
Special Populations
Children and Adolescents
From a developmental perspective, benzodiazepines may have less anxiolytic efficacy and more tolerability concerns in pediatric patients (Dobson et al., Reference Dobson, Bloch and Strawn2019), although they generally appear effective for immediate use of anxiety in acute settings (Kuang et al., Reference Kuang, Johnson, Mulqueen and Bloch2017)
These differences in benzodiazepine efficacy and tolerability may be related to pharmacodynamic differences between pediatric populations and adults. GABA receptor expression and function do not reach “adult” levels until age 14–17½ years for subcortical regions and 18–22 years for cortical regions, although girls reach an adult expression of GABA receptors slightly earlier than boys (Chugani et al., Reference Chugani, Muzik and Juhász2001)
Currently, data from multiple randomized controlled trials in pediatric patients with anxiety disorders do not suggest efficacy, and in these pediatric trials, benzodiazepines are poorly tolerated, especially compared to other psychopharmacological interventions for children and adolescents with anxiety disorders (Dobson et al., Reference Dobson, Bloch and Strawn2019)
Regarding benzodiazepine discontinuation in youth, similar strategies as those used in adults are generally appropriate; however, it is important to consider pharmacokinetic differences in children and adolescents. Specifically, youth may have less fat, which decreases redistribution and may result in a shorter duration of action and more rapid clearance
Therapeutics
Brands
Xanax
Xanax XR
Generic? Yes
Class and Mechanism of Action
Neuroscience-based Nomenclature: GABA positive allosteric modulator (GABA-PAM)
Benzodiazepine (anxiolytic, anticonvulsant)
As positive allosteric modulators of GABAA receptors, benzodiazepines (in the presence of GABA) increase the frequency of opening of the inhibitory chloride channels (although they do not increase the conductance of chloride across the individual channels or the time that the channel is open), enhancing the inhibitory effects of GABA
Inhibits neuronal activity, presumably in amygdala-centered fear circuits, to provide therapeutic benefits in anxiety disorders
Inhibitory actions in the cerebral cortex may provide therapeutic benefits in seizure disorders
Pharmacokinetics and Metabolism
Metabolism
Alprazolam undergoes extensive hepatic metabolism primarily via CYP3A4 (major) and, to a lesser extent, CYP3A5 (Figure 1.4) and may be influenced by grapefruit and other CYP3A4 inhibitors
The major metabolites of alprazolam are 4-hydroxyalprazolam and alpha-hydroxyalprazolam. Of these, alpha-hydroxyalprazolam is the primary active metabolite (Figure 1.4)
Pharmacokinetics
Alprazolam is well absorbed after oral administration
The onset of action is relatively rapid, with the peak plasma concentration (Cmax) occurring within 1–2 hours. Factors such as the formulation of the medication and individual variations from patient to patient can affect the absorption
Alprazolam is highly lipophilic, which allows it to distribute widely throughout the body, including the CNS; however, this also means that it leaves the CNS quickly
Protein binding of alprazolam is about 80%
The half-life of alprazolam in adults is 12–15 hours; there are limited data on its kinetics in youth
Alprazolam metabolism. Alprazolam is primarily metabolized in the liver through CYP3A4 and, to a lesser extent, CYP3A5. Metabolism via these pathways results in the formation of hydroxylated metabolites that are eventually excreted in the urine. CYP3A4 inhibitors can increase alprazolam plasma levels by reducing its clearance.

Figure 1.4 Long description
The biochemical pathway diagram displaying alprazolam metabolized by enzymes C Y P 3 A 4 and C Y P 3 A 5 into 4-hydroxyalprazolam and alpha-hydroxyalprazolam. An accompanying grapefruit is depicted with a note indicating it inhibits these enzymes, though the inhibition is not consistently established.







