

Introduction
The field of psychotherapy has undergone substantial transformation in recent decades, particularly concerning modes of delivery using technology (Edbacken and Vernmark, Reference Edbacken and Vernmark2021; Zale et al., Reference Zale, Lasecke, Baeza-Hernandez, Testerman, Aghakhani, Muñoz and Bunge2021). While face-to-face psychotherapy remains the dominant format, advances in digital technology, the COVID-19 pandemic, and rising demands for accessible mental health care have paved the way for digital formats such as internet-based treatment (Andersson et al., Reference Andersson, Titov, Dear, Rozental and Carlbring2019) and videoconferencing psychotherapy (VCP; Backhaus et al., Reference Backhaus, Agha, Maglione, Repp, Ross, Zuest, Rice-Thorp, Lohr and Thorp2012; Thomas et al., Reference Thomas, McDonald, Boer, Brand, Nedeljkovic and Seabrook2021).
Cognitive behavioural therapy (CBT) is the most empirically supported form of psychotherapy and has demonstrated effectiveness across a wide array of psychological conditions, including depression, anxiety, post-traumatic stress disorder (PTSD), somatic conditions and insomnia (Bhattacharya et al., Reference Bhattacharya, Goicoechea, Heshmati, Carpenter and Hofmann2023; Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012). CBT is typically structured, goal and action oriented, and focused on concrete activities such as identifying and modifying maladaptive thoughts and behaviours, making it particularly adaptable to various digital formats. Internet CBT (ICBT) has received significant empirical attention (Andersson, Reference Andersson2025) and is a well-established treatment modality in research and clinical settings in Sweden (Vernmark et al., Reference Vernmark, Buhrman, Carlbring, Hedman-Lagerlöf, Kaldo and Andersson2024). However, the interpersonal interaction in videoconferencing format more closely mirrors traditional CBT sessions.
VCP can be defined as a synchronous, real-time therapy delivered via video communication platforms and specific video applications, enabling interaction between therapist and client, regardless of geographic location (Backhaus et al., Reference Backhaus, Agha, Maglione, Repp, Ross, Zuest, Rice-Thorp, Lohr and Thorp2012; Tsai et al., Reference Tsai, Cheng and Shieh2020). Previous research has shown that VCP is generally well-received by both patients and therapists (Leuchtenberg et al., Reference Leuchtenberg, Gromer and Käthner2023). VCP has been found to be effective for various disorders, including anxiety, depression, and PTSD (Thomas et al., Reference Thomas, McDonald, Boer, Brand, Nedeljkovic and Seabrook2021), and the effects are comparable to face-to-face treatment in direct comparisons (Fernandez et al., Reference Fernandez, Woldgabreal, Day, Pham, Gleich and Aboujaoude2021). Despite these promising findings, the shift towards using VCP and other digital mental health interventions have raised concern among clinicians about the format and potential caveats in establishing a therapeutic alliance and providing effective care (Ibragimov et al., Reference Ibragimov, Palma, Keane, Ousley, Crowe, Carreño, Casas, Mills, Llosa, Group, Marques, Tijerino, Echeverri, Fredj, Sleit and Sultan2022). Even if the evidence suggests that therapeutic alliance can be successfully maintained in VCP treatment and other digital formats (Andersson et al., Reference Andersson, Paxling, Wiwe, Vernmark, Felix, Lundborg, Furmark, Cuijpers and Carlbring2012; Norwood et al., Reference Norwood, Moghaddam, Malins and Sabin-Farrell2018; Vernmark et al., Reference Vernmark, Hesser, Topooco, Berger, Riper, Luuk, Backlund, Carlbring and Andersson2019), patients and clinicians can perceive it more difficult to connect with each other on a personal level in online treatment formats, perceiving difficulties with using body language and interpreting emotions (Békés et al., Reference Békés, Doorn, Luo, Prout and Hoffman2021; Kessel, Reference Kessel2021; Song and Foster, Reference Song and Foster2022).
CBT is an umbrella term that contains several different methodologies and a plethora of techniques (Hofmann et al., Reference Hofmann, Asnaani, Vonk, Sawyer and Fang2012). One aspect of its provision through video is what components are suitable to be provided in the format. Videoconferencing CBT (VCBT) formats usually contains similar components as their face-to-face counterparts (Porter et al., Reference Porter, Galloghly and Burbach2022). However, as components differ in how they are delivered and to what degree they are verbal, experiential, highly emotional, dependent on subtle behavioural cues, or dependent on other aspects of the setting and requirements for their delivery, there should be differences in the perception of which components CBT clinicians consider more or less suitable for a videoconferencing format. Another aspect of VCBT provision is for what type of diagnoses and level of severity clinicians believe it can be used. Most studies so far have been on mild to moderate problems and for well-studied diagnostic groups, such as anxiety and depression (Thomas et al., Reference Thomas, McDonald, Boer, Brand, Nedeljkovic and Seabrook2021). Mild to moderate cases of these diagnoses are commonly treated in primary care settings, but more complex diagnoses and mental health problems usually seen in secondary (specialised care) settings are less well studied. An exception to this is the use of the videoconferencing format for post-traumatic stress in war veterans that has a long research history in the US (Kuhn and Owen, Reference Kuhn and Owen2020).
The National Board of Social Affairs and Health in Sweden and the national strategy Vision for eHealth 2025 has for almost a decade encouraged the integration of e-health technologies into clinical care (Socialdepartementet, 2016; Socialstyrelsen, 2016) and VCBT has been increasingly adopted by regional health authorities and private mental health services in the Swedish healthcare system. Changes in Swedish healthcare laws and regulations as early as 2015 consequently led to the dissemination of publicly funded psychologist video sessions through private caregivers and digital clinics with national reach starting to scale in 2018.
The COVID-19 pandemic further accelerated this development and created an unprecedented shift in service delivery, compelling many clinicians in Sweden and other parts of the world to adopt the videoconferencing format rapidly, often without prior training or established protocols (Gentry et al., Reference Gentry, Puspitasari, McKean, Williams, Breitinger, Geske, Clark, Moore, Frye and Hilty2020; Hall et al., Reference Hall, Bartley, Wenk, Connor, Dugger and Casazza2023). In Sweden, there was a 330% increase in the total number of digital psychologist visits (mainly VCBT) at private healthcare providers between the years 2019 and 2020 (Blix and Dahlstrand, Reference Blix and Dahlstrand2021). The number of video visits in the healthcare sector has continued to grow since then, and data from 2024 showed that almost one in five citizens in Sweden had attended a video meeting with a healthcare staff (SCB, n.d.), although specific numbers for the share of video sessions with psychologists or counsellors are not available. The standard time length of 45 minutes per session has been challenged by the provision of video sessions with psychologists through private providers in routine care, with sessions shortened to 25 minutes (Mindler, n.d.). This change of session duration is a consequence of several factors, including reimbursement models and the digital format itself, but it is not clear what session length CBT clinicians believe is necessary when delivering their interventions.
Despite the growing use of VCBT during the COVID-19 pandemic and it becoming an established format of delivery of mental health interventions in the healthcare sector, few studies have examined how CBT clinicians experience and evaluate how and for whom CBT can be delivered to through this modality. Given the importance of therapist perceptions for routine care implementation (Maack et al., Reference Maack, Karlsson, Gillberg, Wikström, Pikkemaat and Nymberg2024; Muir et al., Reference Muir, Boer, Thomas, Seabrook, Nedeljkovic and Meyer2020), and the perceived advantages and disadvantages of CBT therapists with the transition from face-to-face to digital alternatives (Dowling et al., Reference Dowling, Martland, King, Nguyen, Neely, Ball, Grant, Dom and McNulty2022; Weineland et al., Reference Weineland, Ribbegårdh, Kivi, Bygdell, Larsson, Vernmark and Lilja2020), there is a need to better understand how Swedish CBT practitioners view the appropriateness, feasibility, and clinical limitations of delivering VCBT in regular practice as well as the applicability of specific CBT-techniques commonly used in face-to-face settings. This understanding complements the already expressed need for increased knowledge and skills training among healthcare professionals in providing digital psychotherapy (Dobson et al., Reference Dobson, Variava, Douglas and Reynolds2022).
The current study aimed to explore the attitudes of Swedish CBT clinicians towards the use of the videoconferencing format during the COVID-19 pandemic. Specifically, it investigated how clinicians perceived the advantages and disadvantages of using the videoconferencing format, their opinions on various CBT techniques in this format, and which diagnostic categories they considered suitable for VCBT. By focusing on clinician perspectives, the study contributes to the growing literature on digital mental health and healthcare professional perspectives, a crucial aspect of the continued development and implementation of evidence-based digital formats.
Method
Study design
This study employed a cross-sectional survey design with the aim of exploring the attitudes of Swedish CBT clinicians towards the use of videoconferencing psychotherapy. The research was exploratory in nature, focusing on capturing a broad range of clinician perspectives regarding the feasibility, acceptability, and limitations of delivering VCBT. The study was conducted during the COVID-19 pandemic, a period that necessitated a rapid and widespread uptake of digital treatment formats across Swedish mental health services.
Participants and recruitment
Participants were recruited using a convenience sampling method during a period of 3 weeks in October 2020 (12 October to 30 October). The survey was distributed via email to members of two Swedish professional organisations for CBT practitioners: the Swedish Association for Cognitive and Behavioural Therapies (SFKBT) and the Behavioural Therapy Association (BTF). These associations include mainly psychologists and counsellors, but also other healthcare professionals trained in CBT. The survey was also shared in relevant professional Facebook groups, mailing lists within a Swedish healthcare region, and via professional networks to reach a broad range of clinicians working with CBT. As several healthcare professions can obtain a psychotherapist licence in Sweden, respondents of the survey could have two licences, e.g. being both psychologist and psychotherapist.
Survey development and design
The web-based survey included 58 closed and two open-ended questions, all in Swedish. The survey included background questions, preferred terminology for VCP, willingness to work via video, perceived suitability of various CBT techniques and interventions, perceived applicability of the videoconferencing format to different diagnostic groups, advantages and disadvantages with the format, suitable age groups, preferred length of video sessions, personal reflections on the impact of the COVID-19 pandemic on therapeutic work and other reflections about the use of videoconferencing. Questions were in the format of Likert-scale questions, multiple-choice items, and free-text open-ended questions.
CBT techniques listed in the survey were derived from well-established treatment manuals and CBT literature (Hofmann and Hayes, Reference Hofmann and Hayes2018; Linton and Flink, Reference Linton and Flink2021; Newman, Reference Newman2013). The final survey included 30 selected CBT techniques such as agenda-setting, exposure, behavioural activation, cognitive restructuring, and mindfulness. Clinicians were asked to rate the applicability of each technique when delivered via video. Similarly, 16 diagnostic categories were selected based on their suitability for CBT and their presence in the DSM-5-TR (American Psychiatric Association, 2022). Techniques and diagnostic categories commonly used and found in primary care settings were prioritised, it being the most common work setting for CBT clinicians in Sweden and the distribution of the survey would mainly reach respondents working at that level. Respondents rated the degree to which each diagnosis could be treated effectively using a videoconferencing format.
The survey was implemented using LimeSurvey (version 2.06+), a platform frequently employed in research settings, and distributed through the Iterapi platform (Vlaescu et al., Reference Vlaescu, Alasjö, Miloff, Carlbring and Andersson2016). Prior to distribution, the survey was pilot tested with four clinicians who provided feedback on clarity, usability, and relevance. Minor revisions were made accordingly based on their input.
Statistical procedures
Data were exported from the Iterapi platform and analysed using IBM SPSS Statistics 29.0. The analysis was primarily descriptive, including frequencies, percentages, and means to characterise respondents and summarise their views. Given the exploratory nature of the study and the use of a convenience sample, inferential statistical analyses were not applied. Free-text responses were used only as a contextual addition to the results from the descriptive analysis and were not analysed separately.
Results
A total of 488 individuals accessed the survey link. Of these, 348 did not start the survey or provided incomplete responses and were excluded from the final analysis. The final sample consisted of 140 participants who completed all items. Of these, 74% identified as female (n=103), 25% as male (n=35), and 1% (n=2) preferred not to disclose gender. The average age of respondents was 52.8 years (SD=10.3), with a range of 26–76 years.
Respondents represented a range of professional roles. As healthcare professionals in Sweden can have several professional titles and therapist educations, this was a multiple-choice question. The majority identified as psychotherapists (n=72, 51.4%), followed by psychologists (n=51, 36.4%), counsellors (n=44, 31.4%), behavioural health professionals (n=5, 3.6%), occupational therapists (n=3, 2.1%), and physicians (n=1, 0.7%).
In terms of academic training, the most common qualification was Bachelor of Science in Social Work (n=57, 40.7%), followed by Master of Science in Psychology (n=55, 39.3%), behavioural science degrees (n=12, 8.6%), Bachelor of Science in Nursing (n=9, 6.4%), and Master of Science in Medicine (n=1, 0.7%).
Eighty-three participants (59.3%) had received their CBT training as part of their formal psychotherapist training program, and nearly as many (n=80, 57.1%) had completed basic CBT training either during their master’s degree in psychology or through a comparable stand-alone course. CBT training was as a supervisor (n=28, 20%), single courses or workshops (n=6, 4.3%), or other training (n=10, 7.1%). The Other category included training in ICBT, acceptance and commitment therapy (ACT; Hayes and Strosahl, Reference Hayes and Strosahl2013), specialist courses in psychology, and dialectic behaviour therapy (DBT; Shearin and Linehan, Reference Shearin and Linehan1994).
Preferred CBT techniques
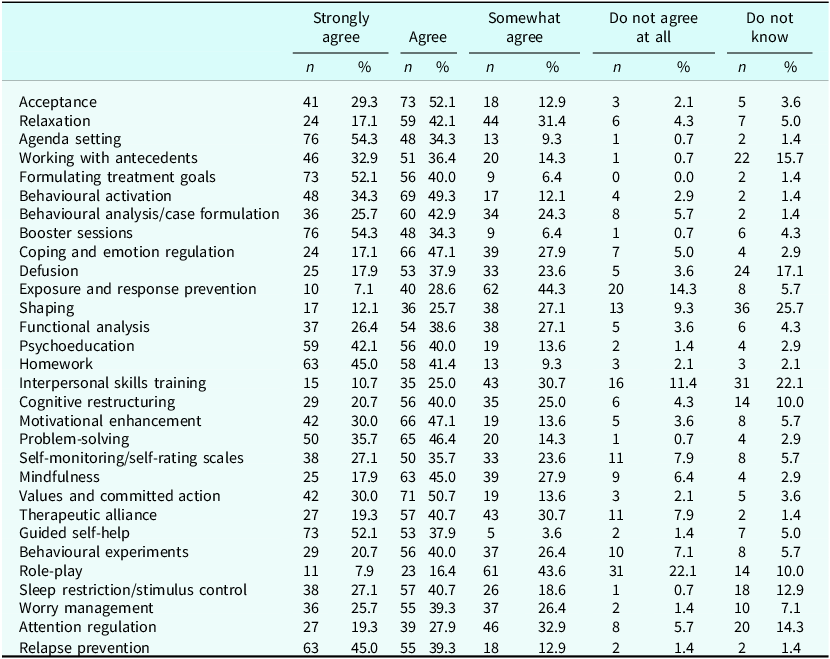
The five CBT techniques considered most suitable (agree and strongly agree responses combined) for delivery through video included formulation of treatment goals (92.1%), guided self-help sessions (90%), agenda-setting (88.6%), booster sessions (88.6%), and assigning and reviewing homework (86.4%).
Role-play was the technique that most respondents considered unsuitable (do not agree at all responses; n=31, 22.1%), followed by exposure and response prevention (n=20, 14.3%), and interpersonal skills training (n=16, 11.4%). Also, a large group of respondents picked the do not know answer for shaping (n=36, 25.7%), interpersonal skills training (n=31, 22.1%), and defusion techniques (n=24, 17.1%). The full list of techniques can be found in Table 1.
CBT techniques and their possible delivery through videoconferencing format
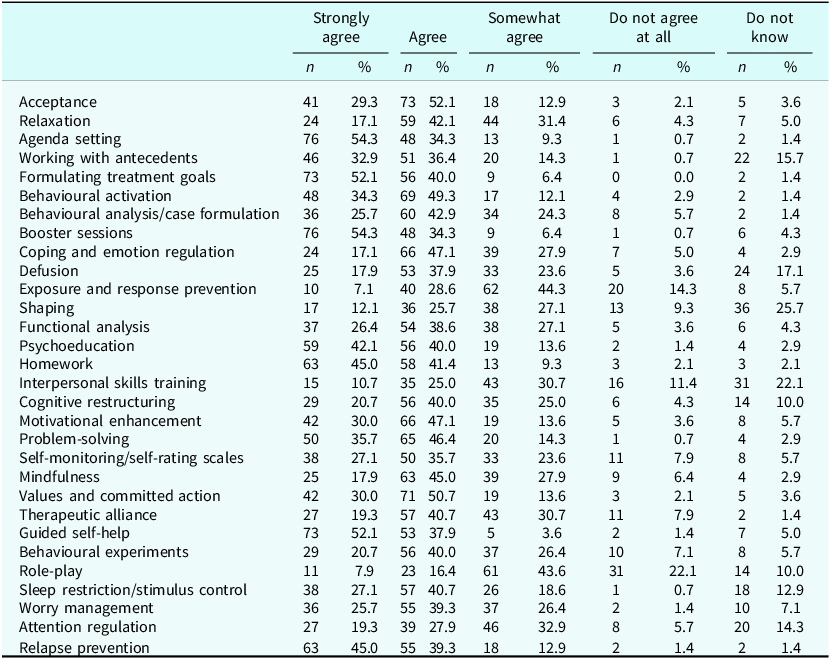
N = 140. Percentages may not total 100 due to rounding.
Suitability ratings
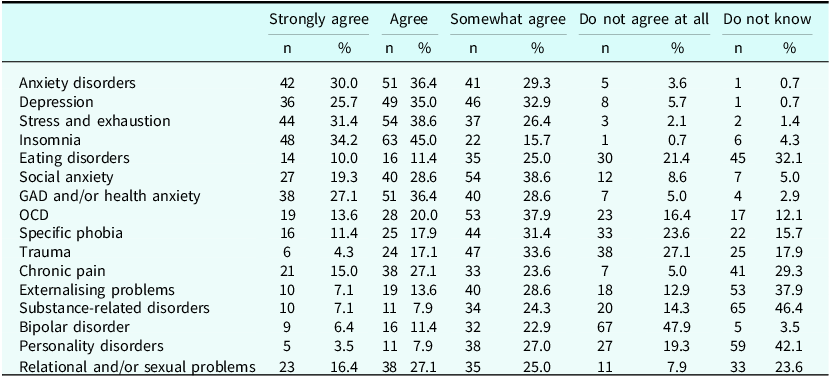
The highest suitability ratings (agree and strongly agree responses combined) were given for insomnia (79.2%), stress-related conditions (70.0%), anxiety disorders (66.4%), generalised anxiety/health anxiety (63.5%), and depression (60.7%). Diagnoses such as bipolar disorder (n=67, 47.9%), trauma (n=38, 27.1%), specific phobia (n=33, 23.6%), eating disorders (n=30, 21.4%), and personality disorders (n=27, 19.3%) were considered least suitable (do not agree at all responses). Substance related disorder was the diagnosis where most respondents chose to answer do not know (n=65, 46.4%), followed by personality disorders (n=59, 42.1%), and externalising problems (n=53, 37.9%). The full list can be found in Table 2.
Diagnoses and their perceived suitability for videoconferencing format
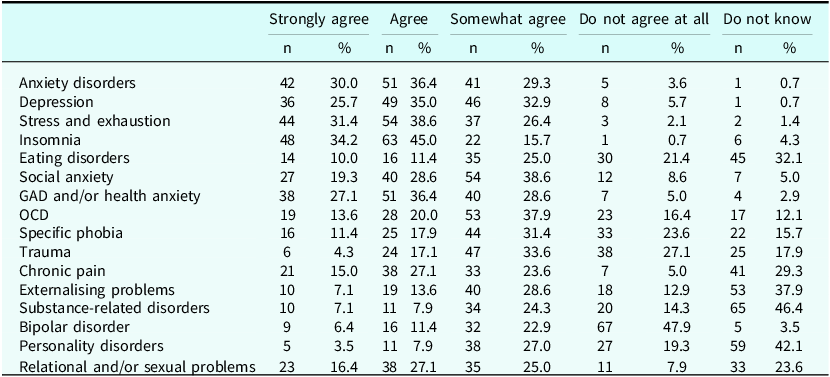
N = 140. Diagnoses are listed in the same order as they were presented in the survey. Percentages may not total 100 due to rounding.
Attitudes, advantages and disadvantages
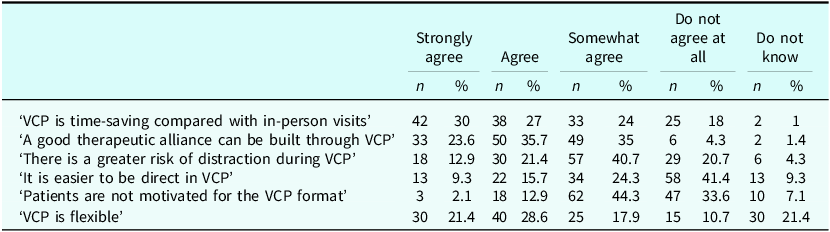
Twenty-nine respondents described their general attitude towards VCBT as very positive (20.7%), 69 as positive (49.3%), 34 as neutral (24.3%), seven as negative (5%), and one as very negative (0.7%). More than half of the respondents agreed or strongly agreed that VCBT saved time (n=80, 57%), and that a good therapeutic alliance could be maintained in the format (n=83, 59.3%). One in five (n=30, 21.4%) did not know if VCBT was a flexible format and many respondents did not believe it was easier to be more direct in VCBT (n=58, 41.4%). See Table 3 for the complete distribution of responses.
Perceived advantages and disadvantages with videoconferencing format
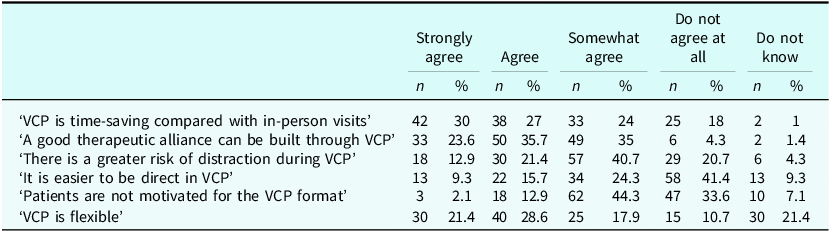
N = 140. Percentages may not total 100 due to rounding.
Age groups and length of sessions
A total of 58.6% (n=82) considered VCBT an alternative for those between 19 and 65 years of age, and 31.4% (n=44) for all ages. The same number of respondents considered VCBT to be an alternative for ages 13–18 years (n=44, 31.4%), and a few less for the older age group, 65+ years (n=42, 30%). Thirteen respondents considered the format suitable for 80+ years (9.3%) and only one (0.7%) for children (<13 years). A total of 16 (11.4%) respondents did not know which age groups could be treated with VCBT.
On the multiple-choice question on preferable length of a videoconferencing session, a majority reported that at least 30 minutes (n=72, 51.4%) was necessary. A session length of 45 minutes was considered preferable by 38 participants (27%). Thirty respondents (21.4%) considered 20 minutes enough time and 25 respondents (17.9%) considered 25 minutes to be necessary.
Discussion
The findings of this study provide valuable insights into how Swedish CBT clinicians, mainly psychotherapists, psychologists, and counsellors, perceive the videoconferencing format as a part of their clinical practice during the COVID-19 pandemic. Overall, the attitudes were predominantly positive, particularly for providing structured and less experiential and interpersonal CBT techniques for well-studied diagnoses such as stress, depression, insomnia and anxiety. This was further confirmed in the open-ended responses where only two respondents were explicitly negative towards the use of VCBT and the format was otherwise described as ‘useful’, ‘effective’, ‘the future’, or in similar terms. The results suggest that the videoconferencing format was already accepted among CBT clinicians seven months into the COVID-19 pandemic and seen as a credible alternative to face-to-face therapy, although its use for more complex mental health problems, the delivery of certain interpersonal and experiential techniques, and its use for other age groups than adults, needs to be further explored.
A common denominator of those techniques and components that clinicians rated as favourable for delivering VCBT, such as formulating treatment goals, agenda setting, and assigning and reviewing homework, is their highly structured and verbal nature. These components can be delivered in a conversational style with the help of structured digital support material used together by both therapist and patient. The COVID-19 pandemic called for a quick transition to digital formats and the ease of verbal provision of important treatment components in VCBT could have served as an advantage for its immediate use, both as a stand-alone option and as an adjunct to self-help material online (Ciuca et al., Reference Ciuca, Berger, Crişan and Miclea2018). Also, the digital medium could have contributed even further to the structured nature of CBT treatment, as using a digital format for mental health interventions has been shown to contribute to the perception among some therapists that the increased structure is a consequence of the digital format itself (Weineland et al., Reference Weineland, Ribbegårdh, Kivi, Bygdell, Larsson, Vernmark and Lilja2020).
Conversely, more complex, experiential or emotionally intense interventions, such as role-play, exposure techniques, and emotion regulation exercises, were considered less feasible in a digital format. These techniques tend to rely on subtle behavioural cues, shared physical environments, or in-the-moment affective engagement that may be perceived as difficult to replicate over video. The hesitancy to deliver these techniques in a video format can be a consequence of clinicians not having enough experience of their use. It could also be the belief that certain, but not all, parts of these techniques can be delivered in a digital format, as 44.3% of respondents somewhat agreed that exposure and response prevention can be delivered through video. While VCBT accommodates many core CBT components, certain interventions may require more elaborate adaptation for provision through video or are better suited to face-to-face formats. In an overview of the delivery of prolonged exposure during the COVID-19 pandemic, authors pointed to the necessity of adapting certain parts of the method in a videoconferencing format, such as relying more on verbal than non-verbal prompts (Wells et al., Reference Wells, Morland, Wilhite, Grubbs, Rauch, Acierno and McLean2020). The problem of transferring exposure techniques to a videoconferencing format and the lack of technological alternatives to face-to-face CBT therapist behaviours, such as the use of a whiteboard, have also been highlighted in comparative studies (Leuchtenberg et al., Reference Leuchtenberg, Gromer and Käthner2023). Ten respondents in our study described such pedagogical difficulties connected to the use of the video format, including difficulties with using digital whiteboards and sharing documents. However, clinicians tend to adapt their provision of VCP when faced with barriers or limitations with the digital format (Parisi et al., Reference Parisi, Dopp and Quetsch2021). These adaptations, together with the advancement of technological videoconferencing solutions, could facilitate and even advance the future delivery of VCBT (Cataldo et al., Reference Cataldo, Mendoza, Chang, Buchanan and Dam2023; Cataldo et al., Reference Cataldo, Chang, Mendoza, Buchanan and Dam2025).
One aspect of CBT is its heterogeneity in that it includes many different methodological variations, including third wave behaviour therapies such as ACT (Hayes and Strosahl, Reference Hayes and Strosahl2013). There was a high degree of uncertainty regarding the use of defusion techniques, a core component in ACT, through video. However, other techniques such as acceptance, mindfulness, values and committed action, were by most respondents considered highly possible to deliver in a video format. One explanation for this could be the lack of experience among the respondents of the technique itself, as defusion is less often used than cognitive techniques in standard CBT protocols. This could also partly explain the high degree of uncertainty among respondents regarding the use of shaping in VCBT, a technique more commonly used in strictly behavioural interventions (Cihon, Reference Cihon2022). Another possible explanation is that the experiential nature of defusion techniques and their design to facilitate a temporary disengagement from the dominance of language processes that contribute to psychological suffering, make them more difficult to deliver in a video format (Bramwell and Richardson, Reference Bramwell and Richardson2018).
The preferability of goal and agenda setting techniques, and less perceived suitability for relational components, is interesting from a therapeutic alliance perspective and the concept of a personal connection and relation between therapist and patient in therapy. In the open-ended responses, 21 respondents described difficulties in accessing and interpreting body language, non-verbal cues, nuances, and emotional expression in video sessions. Even so, only 4.3% of the respondents believed that a good alliance was unachievable in VCBT, and it is very likely the case that a therapeutic alliance can be created and maintained in the videoconferencing format (Simpson and Reid, Reference Simpson and Reid2014), including in real world settings where therapists have transitioned to a digital format during the COVID-19 pandemic (Doorn et al., Reference Doorn, Békés and Prout2020). As the pantheoretical concept of working alliance (Bordin, Reference Bordin1979) consists of both the emotional bond between therapist and patient, and the agreement on tasks and goals in therapy, it could be that the facilitated use of the latter components in VCP and other digital formats creates a foundation for a therapeutic alliance even though the bond is perceived as less emotional and personal than in face-to-face treatment (Békés et al., Reference Békés, Doorn, Luo, Prout and Hoffman2021; Weineland et al., Reference Weineland, Ribbegårdh, Kivi, Bygdell, Larsson, Vernmark and Lilja2020). Developing new scales for measuring alliance in digital interventions could be helpful for therapists, as they could incorporate and include the unique aspects of delivering interventions online (Ashur et al., Reference Ashur, Saar, Brandes and Baumel2024; Penedo et al., Reference Penedo, Berger, Holtforth, Krieger, Schröder, Hohagen, Meyer, Moritz and Klein2020), as well as new technological videoconferencing features post-COVID-19 helping therapists enhance control and positively affect the therapeutic alliance (Cataldo et al., Reference Cataldo, Chang, Mendoza, Buchanan and Dam2025).
Common mental health problems and disorders, such as anxiety, depression, stress-related conditions, and insomnia were perceived by most respondents as suitable for VCBT. These conditions are often treated with well-known CBT techniques and clinicians in this study are likely to have had experience of their provision themselves, which could have influenced the attitudes towards the use of digital interventions in a positive way. There is also research support for the use of digital formats, including VCBT, for several of these conditions (Batastini et al., Reference Batastini, Paprzycki, Jones and MacLean2021; Thomas et al., Reference Thomas, McDonald, Boer, Brand, Nedeljkovic and Seabrook2021). Clinicians were most sceptical about using VCBT with clients experiencing trauma, personality disorders, substance use issues, and bipolar disorder. These conditions often require a more comprehensive effort, and specific forms of CBT treatment (Shearin and Linehan, Reference Shearin and Linehan1994), as they are harder to treat. Together with the limited evidence for the use of digital treatment formats for severe mental health problems, it could have influenced the attitudes of clinicians toward the use of the videoconferencing format. An interesting finding is the perceived unsuitability among many respondents of VCBT for trauma, as it has been studied for many years in the US with promising results (Kuhn and Owen, Reference Kuhn and Owen2020). This could stem from a lack of local knowledge and current use of video sessions for PTSD treatment, making clinicians hesitant about its use for what is considered a more severe psychiatric diagnosis. Even though there is scarce evidence to support the use of video for complex cases, the use of videoconferencing in specialised settings in Sweden increased dramatically during the COVID-19 pandemic, more than doubling the number of distance contacts, with only a slight decrease post-pandemic (SKR, 2022; SKR, 2024), turning it into a well-established format of delivery in healthcare settings. As later studies have shown that therapists’ attitudes towards online therapy became more positive as its use increased during the COVID-19 pandemic, it is probable that conducting a new survey among healthcare professionals in Sweden would have resulted in more favourable attitudes towards the use for complex cases (Whitehead et al., Reference Whitehead, Alrashdi, Bin and Drini2025). However, the discrepancy between the actual use of VCBT for complex conditions in routine care and the lack of data on its effects and appropriateness in this setting is still a topic that needs to be addressed as it is a concern among healthcare staff such as psychotherapists and psychologists (Gullslett et al., Reference Gullslett, Kristiansen and Nilsen2021; Rutkowska et al., Reference Rutkowska, Furmańska, Marques, Martins, Lane and Meixner2025).
Most CBT clinicians preferred video sessions that were at least 30 minutes, and 27% preferred sessions that were 45 minutes or longer. This finding is interesting, as videoconferencing sessions through private providers in regular care now in 2025 often last no more than 25 minutes, which could highlight a gap between a preferred session length among clinicians and the actual session length in regular care. There is an ongoing discussion in Sweden if the length of sessions is guided by evidence and needs of patients, or by the laws and regulations that define reimbursement for videoconferencing sessions (Psykologtidningen, 2022). Our data indicate a preference among clinicians for maintaining a session duration comparable to traditional in-person therapy, while at the same time perceiving VCBT as a time-saving method compared with in-person visits. This only underscores the importance of including clinicians in the discussions regarding how digital formats need to be provided and that a more traditional view and perception of how psychotherapy should be delivered could clash with the use of new technology.
VCBT was considered most suitable for adults, which was expected as the research for this age group is well documented (Batastini et al., Reference Batastini, Paprzycki, Jones and MacLean2021; Thomas et al., Reference Thomas, McDonald, Boer, Brand, Nedeljkovic and Seabrook2021). However, only one respondent considered VCBT as an option for children. This aligns with the current weak evidence base for digital interventions in general, including VCBT, for children (Fischer-Grote et al., Reference Fischer-Grote, Fössing, Aigner, Fehrmann and Boeckle2024; Vigerland et al., Reference Vigerland, Lenhard, Bonnert, Lalouni, Hedman, Ahlen, Olén, Serlachius and Ljótsson2016) and studies showing that clinicians struggle with difficulties in delivering video-mediated psychotherapy to children, describing loss of therapeutic tools, ethical and technical challenges, and concerns about treatment effectiveness (Erlandsson et al., Reference Erlandsson, Forsström, Rozental and Werbart2022).
The current landscape of digital mental health interventions in Swedish healthcare is primarily characterised by the delivery of ICBT, VCBT, combinations of these formats, and blended approaches integrating in-person sessions with digital modes of delivery. Since the COVID-19 pandemic, Swedish healthcare regions have increasingly established their own publicly operated digital primary care clinics, predominantly offering VCBT alongside other digital formats. At the same time, changes in public reimbursement models have reduced the economic viability of nationally operating private providers delivering videoconferencing therapy. Instead, current financing structures favour regionally organised ‘digi-physical’ (hybrid) models, in which both public and private providers within each region offer a combination of in-person and digital mental health services to local populations.
Strengths and limitations
The methodology in this study aimed to facilitate accessibility and participation while gathering a diverse set of views from clinicians actively engaged in CBT. The timing of the survey, during a period of substantial digital transition due to the COVID-19 pandemic, offered a unique opportunity to capture real-time perspectives on the integration of technology into clinical practice, and the sample of 140 respondents is comparable to other surveys examining similar topics. However, the study has limitations. First, the use of a convenience sample means the findings may not be representative of all Swedish CBT clinicians. Even though the sample was representative with regard to gender and age in a mixed sample of psychologists, psychotherapists and counsellors (Socialstyrelsen, 2022), it is possible that those who chose to respond were more engaged with or interested in digital formats. On the other hand, the average age of respondents was 53 years, which could indicate the opposite, that a sample with younger clinicians could have been even more positive towards VCBT. Second, the cross-sectional nature of the data limits conclusions about changes in attitudes over time and causal relationships. As this survey was conducted during the COVID-19 pandemic, a transitional period for the use of digital formats in mental health delivery, a follow-up survey could provide insight into changes in attitudes and perceptions of digital delivery when experience of VCBT provision had increased among clinicians. Also, we did not ask respondents about their previous use and experience of VCBT, a variable that could have influenced attitudes and preferences towards the format in the survey. Furthermore, although qualitative responses provided valuable context, they were not subjected to formal thematic analysis in this study. Future research could employ mixed methods designs or in-depth interviews to further explore clinicians’ reasoning, theoretical considerations, and ethical reflections on using the videoconferencing format.
Conclusions
This study adds to the literature on how CBT clinicians, mainly psychologists, counsellors, and psychotherapists, in Sweden perceived and preferred to provide videoconferencing psychotherapy during the COVID-19 pandemic. It adds to the growing body of literature on digital CBT and therapist perspectives, including how experiences can be used to inform the post-pandemic dissemination of online psychotherapy (MacMullin et al., Reference MacMullin, Jerry and Cook2020). Swedish CBT clinicians were open to integrating and using videoconferencing in routine practice, particularly for common diagnoses in primary care for which there already was research support for the use of digital interventions, and with the use of specific CBT techniques that are more structured and verbal in their nature. Reservations remained for more complex cases, and emotionally and experientially intense CBT interventions. As mental health care systems and healthcare professionals increasingly use VCBT, other digital formats, and blended formats that combine in-person and remote sessions, in their everyday work, understanding clinician attitudes and their perception of providing CBT in these formats of delivery becomes essential. Their views can inform implementation strategies, training priorities, technological developments, and decisions about when and for whom the format is most appropriate.
Key practice points
-
(1) CBT therapists can confidently deliver treatment for common diagnostic groups via videoconferencing using familiar CBT techniques, without requiring extensive additional training.
-
(2) To expand beyond structured and verbally focused methods, therapists need training in how to adapt more experiential and interpersonal techniques for the video format.
-
(3) When selecting interventions, therapists should consider the limitations of videoconferencing for subtle interpersonal or experiential work and adapt these techniques accordingly.
-
(4) Because VCBT is increasingly used with severe cases despite limited evidence, therapists must carefully assess when videoconferencing is appropriate or inappropriate for a given patient.
-
(5) Therapists may consider shorter sessions (around 30 minutes) as a clinically acceptable and often preferred alternative to the traditional 45-minute CBT session.
Data availability statement
Data and other materials not included in the manuscript or as appendixes, including all relevant raw data, will be freely available to researchers for non-commercial purposes upon request.
Acknowledgements
We want to acknowledge the webmaster George Vlaescu for his support with the Iterapi platform. We also extend our thanks to all the respondents who participated in the survey. The authors declare that the artificial intelligence (AI) tools ChatGPT (OpenAI; versions GPT-4o and GPT-5, 2024–2025 releases) and DeepL Translator (DeepL SE, 2025 version) were used to assist in improving spelling, grammar, and increased readability of the manuscript. No AI tools were used for data analysis, interpretation of findings, or drawing scientific conclusions. The authors take full responsibility for the content of this article and that it adheres to the journal’s authorship policy.
Author contributions
Kristofer Vernmark: Conceptualization (supporting), Data curation (equal), Formal analysis (equal), Investigation (supporting), Methodology (equal), Project administration (supporting), Visualization (equal), Writing - original draft (lead), Writing - review & editing (lead); Mattias Norlin: Conceptualization (equal), Data curation (equal), Formal analysis (equal), Investigation (lead), Methodology (equal), Project administration (lead), Visualization (equal), Writing - original draft (supporting), Writing - review & editing (supporting); Gerhard Andersson: Conceptualization (equal), Data curation (equal), Formal analysis (equal), Funding acquisition (lead), Investigation (supporting), Methodology (equal), Project administration (supporting), Resources (lead), Supervision (lead), Writing - original draft (supporting), Writing - review & editing (supporting).
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standards
The survey was anonymous and did not collect personal identifiers or sensitive clinical data. Participation was voluntary, and respondents could skip any question and withdraw at any time. As the study did not involve patient data or clinical interventions, ethical review was not required under Swedish research legislation (SFS 2003:460). A brief ethics declaration was included in the survey introduction, assuring participants of anonymity, confidentiality, and the voluntary nature of participation. Informed consent was obtained from all participants. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.

 Open access
Open access
Comments
No Comments have been published for this article.