

In the 1950s, Michael Balint wrote one of the signature texts for general practice: The doctor, his patient and the illness. (Reference Balint1) Balint was a psychoanalytic psychiatrist who pioneered a type of small group learning for GPs which came to be known as Balint groups. Balint groups encouraged doctors to reflect on the nature of therapeutic relationships, and to consider how these might be leveraged to improve care. Balint was an advocate of whole person care, and one of his core concepts was the ‘collusion of anonymity’, which described the situation where the patient is passed from one specialist to another with nobody taking responsibility for the whole person. The concept of collusion implied avoidance, the idea that each specialist chose to complete the relevant task at hand, but avoided engaging with the patient as a person.
I was reminded of Balint when considering the multiple options available to a survivor of sexual harassment in medicine. A survivor may have multiple options available to them if they choose to report, including law, medical regulatory bodies, workplace management processes, universities, and others. However, like the anonymous patients in Balint’s text, a survivor may well find themselves being moved from organisation to organisation, without anyone engaging with them as a person. The key feature of the collusion of anonymity is that none of the providers feel they have failed to manage the problem, and it is only the patient, or in this case the survivor, who experiences the demoralising impact of being shunted from place to place without having their issues resolved. Like Balint’s patients, the result is often the patient exiting from the process, unable to tolerate the demoralisation and exhaustion of trying to engage with a process causing them harm.
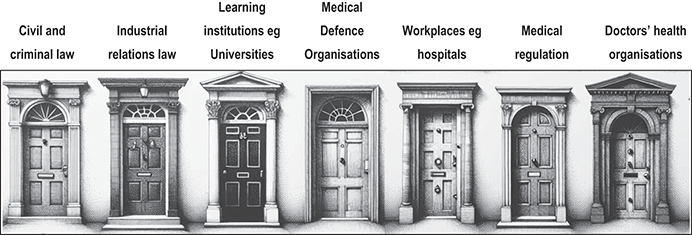
In 2023, there was a summit on sexual harassment in medicine in Australia, which aimed to address this exact problem. In a workshop, leaders from the various disciplines were asked to summarise what someone might expect should a survivor open their particular door and report sexual harassment to their organisation. Unsurprisingly, although there were clear policy frameworks available for each organisation, leaders were unable to find the answers to common questions asked by survivors (see figure 31.1). Without a clear understanding of what lies behind each ‘door’, reporting can be risky, bewildering, and feel profoundly unsafe.
The collusion of anonymity among organisations managing sexual harassment in medicine.
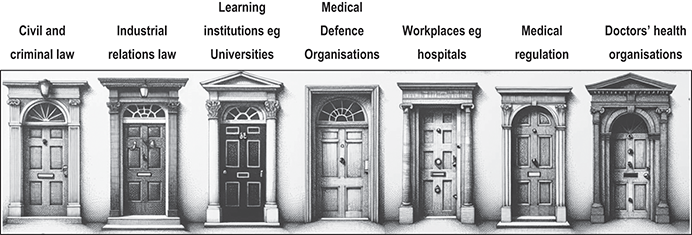
Figure 31.1 Long description
'The seven doors are each labelled with different sectors. The first door is labelled Civil and criminal law, the second door is labelled Industrial relations law, the third door is labelled Learning institutions like Universities, the fourth door is labelled Medical Defence Organisations, the fifth door is labelled Workplaces like hospitals, the sixth door is labelled Medical regulation, and the seventh door is labelled Doctors’ health organisations. Each door has a distinct architectural design.
| Civil and criminal law | Industrial relations law | Learning institutions eg Universities | Medical Defence Organisations | Workplaces eg hospitals | Medical regulation | Doctors’ health organisations |
|---|---|---|---|---|---|---|
| ||||||
In this, the final part of this book, we tackle the way forward for individual advocates and organisations so that survivors can have a better experience, and better outcomes. In doing so, we draw on examples of advocacy from a variety of perspectives. The point of advocacy is to lend one’s power to another, to facilitate change. We are aware that many will approach this book with a view to creating change, and so we wanted to conclude the book with some examples of people who have used their power in different ways to change the environment in which sexual harassment occurs.
In chapter 32, Elizabeth Teisberg and Deborah Cole consider the leadership challenge of being CEOs in organisations with poor culture. They describe how they, as managers, addressed this challenge to ensure a safer environment for their employees. In doing so, they discuss the personal and organisational strategies they use to achieve a lasting cultural shift.
In chapter 33, a number of authors reflect on their roles as advocates, using the lessons they have learned in their various contexts. Advocacy can occur on multiple levels, from one-on-one support to national or international campaigns. Using examples from their own work around sexual safety, they discuss the challenges of communicating effectively with a variety of audiences, and engaging people with different points of view.
Chapter 34 focuses on medical education. It is expected that strategies to change culture will differ according to the position advocates hold in an organisation. This chapter includes commentary by a medical student (Erlinger), doctors in training (Cox, Jewitt and Fleming) and medical educators for undergraduates and GPs in training (Stone and Moir). Together, these authors discuss the different ways change can be achieved, utilising the different forms of power and agency available to them at different stages of their careers.
Finally, in chapter 35, we focus on therapy, which is where this book began. The very first stage of recovery from sexual abuse is recognising the abuse, as it is frequently buried under natural defences like dissociation. The second stage involves breaking the silence to enable a survivor to tell their story. Sexual harassment can cause a significant psychological wound that needs expert treatment, and in this chapter, we consider what that treatment may entail, across the entire trajectory of trauma.
Together, the chapters in this part work to represent different ways of creating change. These efforts will always be more effective if the organisations around them provide transparent, consistent and trauma-informed policies that clearly align across the multiple actors in this complex policy environment. Collusions of anonymity that exhaust the survivor prevent effective management of abuse and, in doing so, maintain a culture that causes long-term harm.

 Open access
Open access