


‘Childless’ or ‘Childfree’, the distinction between the two is fundamental to this study’s examination of decision-making in the choice of contraceptives. The term childless describes those who are without children due to infecundity, implying that having children is a desirable aspect of life which they lack. Conversely, those who are fecund and have chosen not to have children are termed childfree, as they deliberately opt for freedom from parenthood (Blackstone, Reference Blackstone2014). The desire to remain childfree for a heterosexual couple is invariably tied to the use of any mode of contraception. The study examines three questions: Which contraceptives are most preferred by childfree couples in India and Canada? Do preferences vary between couples who decided to be childfree via different decision-making pathways (early articulators and postponers)? And how do the unique cultural and structural contexts of India and Canada influence the choice of contraceptives?
Through much of history, people have sought ways to control their fertility. Yet it was not until the 20th century that an acute need to invest in the systematic scientific development of contraceptives emerged, driven by the sudden and unprecedented population explosion (Anderson and Johnston, Reference Anderson and Johnston2023). Initially intended to control population growth, the contraceptive revolution of the 1960s began to be acknowledged as a source of social revolution that enabled individuals to decide if, when, and how many children they want (Benagiano et al., Reference Benagiano, Bastianelli and Farris2007). The contraceptive revolution not only allowed heterosexual couples to manage the timing and number of pregnancies but also enabled other individuals and couples who do not intend to have children to fulfil their decision without the concern of unwanted pregnancies. With the advent of modern contraceptives, researchers acknowledged that a couple may not necessarily be childless due to their inability to conceive. Instead, they may have consciously chosen to remain childfree. Pioneering studies in the 1970s and 80s on the decision not to have children highlight this important distinction between being childless and being childfree (Veevers, Reference Veevers1973, Reference Veevers1980; Baum, Reference Baum1982, Reference Baum1983). Before modern contraception became widely accessible, it was challenging for heterosexual couples to remain childfree without completely abstaining from sexual intimacy. In short, contraception is essential to maintaining the commitment of heterosexual couples to be childfree. This study examines the contraceptives that self-reported childfree couples prefer and use, highlighting how these methods are essential to their decision to remain childfree.
The present study on decision-making in contraceptive use is part of a larger study that found that for many individuals and couples, the inclination and resolve to forego parenthood evolve over time, influenced by life transitions in areas such as relationships, education, and work (Bhambhani and Inbanathan, Reference Bhambhani and Inbanathan2020). The two main pathways to remaining childfree identified in the larger study were early articulation and postponement, each with two sub-pathways. The early articulation pathway involves individuals or couples who choose to forego parenthood early in their relationship, often even before marriage or entering a common-law union. When an individual is an early articulator in a relationship, the decision-making is called independent early articulation; and when both partners make this decision early on before marriage, it is called mutual early articulation. The postponement pathway, on the other hand, involves individuals or couples who initially delay parenthood but later decide to remain childfree, either individually (unilateral postponement) or together (shared postponement), after years of marriage or a common-law relationship. Given these different pathways to the decision to remain childfree, the first question that this study examines is whether these pathways influenced decision-making on the use of specific contraceptives.
Another question that this study explores arose from reviewing the increasing body of literature on contraception among childfree individuals in the Global North, particularly focusing on women (Veevers, Reference Veevers1980; Richie, Reference Richie2013; Shreffler et al., Reference Shreffler, Tiemeyer, McQuillan and Greil2020; Mui and Costescu, Reference Mui and Costescu2021; Parker et al., Reference Parker, Morse and Bryant2025). These studies mainly concentrated on sterilisation, suggesting that it is a preferred method of contraception for those who have chosen to stay childfree. This may apply to early articulators or individuals who, at a young age, decide not to have children even before they find a potential partner or spouse. However, for the postponers or those who delay the decision to have children or remain childfree, sterilisation might not necessarily be the preferred contraceptive method until they are fully committed to remaining childfree. The study, thus, examines whether sterilisation is more frequently preferred among early articulators. If not, it considers whether the lack of preference for sterilisation, even among couples who are resolute in their decision to forego parenthood from the start, could suggest that they may reconsider parenthood in the future.
Furthermore, as this study is situated in the distinct cultural contexts of India and Canada, it examines the role of cultural and structural factors in informing and shaping the childfree couples’ decision to use specific contraceptive methods. The rationale for conducting this study in India and Canada is threefold. First, existing knowledge on the decision to remain childfree primarily stems from the Global North, likely because of sustained low fertility rates over several decades. Countries such as India have achieved replacement-level fertility rates over the last decade (IIPS & ICF, 2017), and recent estimates indicate that the national average of 1.9 has now fallen below the replacement level (United Nations Population Fund [UNFPA], 2025). However, there is still a significant gap in research focusing on individuals and couples in these countries who choose to remain childfree. This was also indicated by the broader study on the decision-making processes of childfree couples from which this paper originates (Bhambhani and Inbanathan, Reference Bhambhani and Inbanathan2020). Secondly, the study explored how diverse cultural contexts influence the same choice: the decision to remain childfree. Thirdly, this research provided an opportunity for a scholar from a Global South country to investigate the experiences of people in the Global North. This is a rare occurrence, as a growing body of documentation and theory shows that the Global South is often seen as a ‘Field Forever’ (Kanagasabai, Reference Kanagasabai2023). The disparities in material conditions typically make it easier for scholars from Global North institutions, including migrant scholars from the Global South, to conduct fieldwork in the Global South.
Background
To contextualise the questions this study explores, a review of the existing research in India and Canada was conducted. Studies in Canada, the U.S., and other Global North countries indicated some noteworthy findings, particularly the challenges encountered by childfree individuals and couples in obtaining sterilisation. In contrast, the relatively fewer studies on the subject in India led us to examine the overall prevalence of contraceptives, factors influencing contraceptive use, and the challenges to their adoption.
Contraceptive use among childfree in Canada
The total fertility rate of Canada dropping to a historic low of 1.25 children per woman in 2024, along with the rise in women aged 20–49 years without children who ‘definitely’ or ‘probably’ plan never to have children to 31.1% (Statistics Canada, Reference Canada2026), suggests that more women in heterosexual relationships might be using contraception to prevent pregnancy. In one of the earliest studies on the decision to stay childfree, Jean E. Veevers (Reference Veevers1980) emphasised the importance of modern contraception in expanding the choice to remain childfree. Veevers interviewed more than 150 voluntarily childless individuals in Southern Ontario, Canada, and explored various aspects of the childfree experience. She observed that physicians were reluctant to provide sterilisation to nulliparous women, even if they had been married for years and had explicitly requested it. Veevers interpreted this as a manifestation of the pressure to conform to pronatalist norms. An illustrative excerpt captures this pressure to be a conformist:
‘. . . the first year he [physician] gave her [a participant in Veevers’s study] a physical examination and prescribed the pill . . . the second year he asked her why she was not having a baby, but seemed satisfied that she and her husband were still adjusting to one another . . . the third year he delivered a long lecture . . . she would have a baby now before it’s too late (Veevers, Reference Veevers1980: p. 146)’.
Veevers reviewed other studies on contraceptive use during the time of her study (1970s) and noted that they indicated unpleasant side effects of long-term oral contraceptive use and the higher rates of expulsion experienced by nulliparous women using intrauterine devices (IUDs). However, instead of mentioning these risks as the basis to deny extending prescriptions for oral pills or providing IUDs, physicians urged women to become parents before it was ‘too late’. Veevers also emphasised that the physicians’ refusal to perform sterilisation on unmarried and nulliparous women occurred despite laws and policies in the US and Canada allowing it for any adult.
Frances Baum’s (Reference Baum1982; 83; Baum & Cope, Reference Baum and Cope1980) qualitative study on married childfree couples in England studied 38 childfree husbands and wives. Similar to Veevers’s findings, couples in Baum’s study reported that their requests for sterilisation were often dismissed or trivialised by doctors. She also observed that many participants were often apprehensive about undergoing surgical procedures, making them opt for alternative contraceptives instead of sterilisation. Carlisle (Reference Carlisle1982) in Scotland and Callan (Reference Callan and Que Hee1984) in Australia revealed similar concerns among physicians when voluntarily childless individuals or couples requested sterilisation. These studies also compared the use of contraceptives among those who were firm on their intention to be childless even before they were married (early articulators), with those who postponed parenthood and later decided to remain childfree (postponers). A higher rate of sterilisation was found among the former, affirming their determination to remain childfree.
Studies in the 2010s and later have continued to indicate physicians’ reluctance and frequent refusal to sterilise childless women. In her investigation, Richie (Reference Richie2013) tried to discern the motivations of childfree women seeking sterilisation, and the reasons for refusing sterilisation, from both the women’s and physicians’ perspectives. Potential biological and psychological risks to themselves and any child born to them, if they were to have an unwanted pregnancy, were factors that persuaded women to pursue sterilisation. Physicians declined to carry out sterilisation because the women were deemed too young to make such a life-altering decision, due to concerns about potential future regrets or a desire for children. A recent study of childfree women in Canada (Mui and Costescu, Reference Mui and Costescu2021) who had sought or undergone sterilisation also emphasised the challenges encountered by women in obtaining sterilisation. Participants described their consultations with doctors as akin to ‘walking into battle’, which required them to ‘arm [themselves] with as much information’ (ibid.: p. 662).
Sterilisation is an irreversible procedure, and two recent studies (Shreffler et al., Reference Shreffler, Tiemeyer, McQuillan and Greil2020; Parker et al., Reference Parker, Morse and Bryant2025) explored the possibility for women to regret this decision later in life. Shreffler et al. (Reference Shreffler, Tiemeyer, McQuillan and Greil2020) studied sterilised nulliparous women who underwent tubal ligation, hysterectomy, and other surgeries that could make conception difficult or impossible for both medical and contraceptive reasons. They analysed the nationally representative National Survey of Fertility Barriers conducted in the U.S. between 2004 and 2006, and a total of 105 nulliparous women who chose sterilisation for contraceptive and health reasons were identified. The findings revealed that none of the nulliparous women who chose sterilisation as a contraceptive method reported any regrets about the procedure. In Parker et al. (Reference Parker, Morse and Bryant2025), a team of obstetricians and gynaecologists surveyed 400 childfree women from various online communities (including Reddit, Facebook, and TikTok) to examine the barriers to sterilisation that they encountered and whether they regretted the procedure afterwards. Of the 151 women who had undergone sterilisation, 70% had to approach more than one doctor to undergo sterilisation, and 97% of respondents affirmed that sterilisation was an appropriate contraceptive choice for them. The study highlighted several hurdles, including the refusal of many physicians to perform the procedure due to the women’s younger age or nulliparous status. Across these studies, the emphasis on sterilisation of nulliparous individuals, particularly women, suggests it as a favoured contraceptive choice among those without children.
Birth control in Canada
In addition to examining contraceptive use among childfree individuals in Canada, it is important to contextualise the decision-making of childfree couples in the use of contraceptives within Canada’s broader culture of contraceptive use. The history of the birth control movement in Canada illustrates a shift in legal perspectives, moving from criminalisation to recognising access to contraception as a vital aspect of sexual and reproductive rights (SRHR) (Backhouse, Reference Backhouse1983; Dodd, Reference Dodd1983). A historical review of birth control in Canada shows that abortion and contraceptive use were seen as private matters until the 19th century. During that time, different provinces began to pass legislation that gradually criminalised abortion and the advertisement and sale of contraceptives, except when they served a public good, such as preventing overpopulation and the expansion of poverty, particularly in low-income areas (ibid.). Before abortion was decriminalised in Canada in 1969, women’s procedures such as abortions and salpingectomies were carried out by doctors disguised as performing other medical interventions (Shropshire, Reference Shropshire2014; Hulme et al., Reference Hulme, Dunn, Guilbert, Soon and Norman2015). Canada currently ranks among the four countries in the world with no regulations and restrictions, such as gestation limits, on accessing abortion. However, there are still challenges in obtaining contraception and abortion services, such as high costs in several provinces, especially for vulnerable groups, including northern and indigenous communities, undocumented immigrants, women dependent on parental or spousal insurance coverage, certain refugees, and visitors to Canada. Besides, people often lack knowledge of service providers because Canadian health services are not advertised to the public. Rural–urban disparities in healthcare further hinder equitable access to contraception across Canada (Shaw and Norman, Reference Shaw and Norman2020).
The legalisation of contraception in Canada happened alongside the launch of the birth control pill in 1960. Before legalisation, the pill was only prescribed for non-contraceptive purposes such as managing menstrual irregularities and cycle control. Initial concerns and reports of side effects, along with issues of informed consent during trials, limited its acceptability (Seaman, Reference Seaman2011). However, with the development of improved formulas and dosages in the 1980s, the use of the pill increased significantly. Contraceptive pills were identified as the second most common method of contraception among sexually active women in Canada, after condom use by their partners, with a usage rate of 22.3%, according to the Canadian Community Health Survey (CCHS 2019–20). The use of IUDs is also significant, with a prevalence rate of 13.5%. The CCHS (2019–2020) also indicated that oral contraceptive pills and male condoms were commonly used by young couples aged 15 to 24 years, and a shift towards long-acting contraception and sterilisation was noted among older women and couples aged 25 to 49 years. This trend towards long-acting contraceptives among older women may be attributed to the perception that they have reached their desired family size and do not wish to have more children (Statistics Canada, Reference Canada2025). Besides female contraceptives, Canada shows a higher rate of vasectomies compared to tubectomies. However, there are differences across income groups, with higher vasectomy rates in high-income areas and more tubectomies in low-income regions. This indicates variations in male–female relationship dynamics among different income levels (Fransoo et al., Reference Fransoo, Bucklaschuk, Prior, Burland, Chateau, Martens and Team2013). The growing preference for vasectomy in Canada, particularly among younger couples who have completed their desired family size (usually after having two children), also reflects a shift towards more egalitarian attitudes among men, who are increasingly sharing responsibility in decision-making for contraceptive use and practices (Shropshire, Reference Shropshire2014).
Birth control in India
To the best of the authors’ knowledge, there is a noticeable lack of research on voluntary childlessness and birth control in India. This is despite the evidently rising proportion of childlessness, with 7.89% of women above 40 years identified as childless based on 2011 data (Baudin and Sarkar, Reference Baudin and Sarkar2018), a significant increase from 6.2% of ever-married women being childless in 2001 (Ram, Reference Ram2005). Due to difficulties in distinguishing between childlessness and being childfree in these figures, the exact proportion of voluntary childlessness remains hard to determine. In the absence of clear statistics and studies focusing on contraceptive use among childless women, this review examines extensive literature on contraceptive use, the factors influencing it, and the barriers to its adoption.
The acceptance, prevalence, and use of modern birth control methods in India have been influenced by a variety of factors, including demographic concerns, the evolving policy and programme environment, and the growing involvement of diverse stakeholders, particularly the private sector and non-governmental organisations (Santhya, Reference Santhya2003). Significant advancements in contraceptives, such as the increased availability of short-term reversible methods (including contraceptive implants, emergency pills, and contraceptive patches), have also played a crucial role, especially for women (McNay et al., Reference McNay, Arokiasamy and Cassen2003; Ross and Stover, Reference Ross and Stover2013). Moreover, exposure to the mass media (Ghosh et al., Reference Ghosh, Mozumdar, Chattopadhyay and Acharya2021) and a heightened emphasis on men’s involvement in contraception (Hardee et al., Reference Hardee, Croce-Galis and Gay2016) have further influenced birth control usage.
The launch of the world’s first nationwide family planning program in 1952 marked a notable post-Independence (after 1947) focus on population control in India. Although being a pioneer in implementing this program might imply widespread use of a variety of modern contraceptives in India, the review revealed a complex and often contradictory landscape. According to the UNDESA’s World Family Planning report (2022), female sterilisation accounts for the highest share of global contraception, with India contributing 48% of the global total. The National Family Health Survey (NFHS), a critical population-based data source on various dimensions of health and well-being, including contraception, since its launch in 1992, has consistently reported that female sterilisation is the most widely used contraceptive method in India. It has significantly increased from 26.9% in 1992–93 to 37.9% in 2019–21 (Jayakumar, Reference Jayakumar2024).
An analysis of the NFHS 4 (2015‒16) by Ewerling et al. (Reference Ewerling, McDougal, Raj, Ferreira, Blumenberg, Parmar and Barros2021) examined the demand for family planning satisfied, an indicator that pertains to women of reproductive age (15–49) who either do not want to have another child or wish to delay conception and are currently using modern contraception. The study categorised its results based on women’s demographic traits, including age, education, household wealth quintiles, and empowerment levels, as assessed by the SWPER global index. The Survey-based Women’s Empowerment Index (SWPER) measures women’s empowerment across three domains: Attitudes to Domestic Violence, Social Independence, and Decision-Making, using individual indicators cross-culturally. Among the 339,540 partnered women surveyed, aged 15–49 years, 71.8% were using contraceptive methods, and a significant portion of them relied on female sterilisation (76.1%), while 20.7% used short-acting reversible contraception (SARC), such as condoms and pills, and only 3.2% used long-acting reversible contraception (LARC), specifically intrauterine devices (IUDs). Hormonal implants and patches were not reported, and only 0.6% of male partners had undergone a vasectomy. Wealthier and better-educated women had higher usage of SARC and LARC methods, while reliance on permanent sterilisation was more common among less educated women, particularly those with children. The study also revealed that women with higher empowerment scores on SWPER, particularly in attitudes towards violence and social independence, were less likely to rely on permanent sterilisation and more likely to use SARC and LARC. Conversely, women with low empowerment scores on SWPER tended to rely more on sterilisation. Many factors contribute to this trend, including inadequate information on long-term reversible contraceptives, poor access, and less autonomy. In contrast, women with higher education levels and those from wealthier households tend to prefer temporary contraceptive methods over sterilisation due to greater awareness, better access, and relatively more autonomy than women from disadvantaged sections (Singh et al., Reference Singh, Singh and Singh2021; Bansal et al., Reference Bansal, Dwivedi and Ali2022; Jana and Shekhar, Reference Jana and Shekhar2023).
A further examination of female sterilisation reveals significant variations in sterilisation rates that cannot be explained entirely by factors such as socio-economic status or education (Mishra, Reference Mishra and Guilmoto2023). The study reports an unexpected trend that poorer regions, such as the North-Eastern states of India, have lower sterilisation rates, while wealthier states, such as Punjab, do not show higher rates, despite their better economic conditions. In contrast, southern states, with better socio-economic indicators, have high rates of sterilisation. These findings suggest that local cultural norms around acceptable forms of contraception played a key role in influencing the likelihood of women opting for sterilisation. However, the influence of local cultural norms on contraceptive use, particularly female sterilisation, appears to diminish when husbands are educated. Studies on spousal education highlight the significant role a husband’s education plays in influencing contraceptive choices, especially for male-based methods like condoms and male sterilisation. Educated husbands tend to have better knowledge of contraception and are more open to adopting temporary methods, even if these methods challenge traditional cultural beliefs, such as the idea that contraception is women’s responsibility (Gubhaju, Reference Gubhaju2009). Moreover, an educated husband’s typically higher income further reinforces contraceptive use, as his financial stability enables overcoming barriers to accessing various contraceptive methods (Adebowale et al., Reference Adebowale, Adedini, Ibisomi and Palamuleni2014).
In addition to the husbands’ education, their gender attitude has also been found to be associated with contraceptive use. Vishwakarma & Shekhar (Reference Vishwakarma and Shekhar2022) explore covert contraception use (CCU) among married women in India, using data from the NFHS 2005–06 and 2015–16 to examine the influence of men’s attitudes on contraceptive choices. The study defines CCU as the use of modern female contraceptives for spacing, reported by women but not by their husbands. The key independent variable is the husband’s egalitarian gender attitude, measured through responses to questions regarding gender roles and domestic situations in NFHS (2015–16). These questions covered topics such as the justification of violence in various situations, the wife’s right to refuse sex, and whether husbands believe they have the right to use force or seek sex outside the marriage if their wife refuses. The findings of the study indicate a significant rise in CCU from 14.6% in 2005–06 to 26.6% in 2015–16, with pills being the most preferred method due to their ease of use and secrecy, followed by IUDs and injectables. Women, whose husbands held moderate to low egalitarian attitudes, were more likely to use contraception covertly. Conversely, women with higher education and married to men with high egalitarian attitudes had more open communication and greater reproductive autonomy. The study, thus, emphasised the role of men’s gender attitudes and women’s education in influencing contraceptive use and reproductive rights.
Besides the studies based on NFHS data, numerous qualitative studies from across India brought out the significant unmet need for modern contraception stemming from various constraints and concerns. A review of qualitative studies on family planning across 14 states from 2000 to 2019 by Parsekar et al. (Reference Parsekar, Hoogar, Dhyani and Yadav2021) reveals that women’s limited autonomy in family planning decisions, often due to fears of abuse, violence, or desertion, remains a major hurdle. Additionally, a lack of trust in reversible contraceptives, such as IUDs and oral contraceptive pills, due to past side effects or second-hand accounts has led many women to prefer sterilisation despite its irreversible nature. A panel data analysis of Indian Human Development Survey waves 1 and 2 data indicated that sterilisation is indeed a vital stage in the life course of women in India after they have had the desired number of children (Reed, Reference Reed2021). While sterilisation addresses the issue of permanent family planning, it does not provide an option for spacing births. The NFHS-4 (2015–16) indicates that approximately 13% of women have an unmet need for family planning, with 6% specifically needing spacing methods (Muttreja and Singh, Reference Muttreja and Singh2018). This unmet need often leads women to resort to induced abortions, sometimes in unsafe conditions, further compromising their health and well-being (Cleland, Reference Cleland2020).
Data and methods
This paper draws on a larger study that examined how heterosexual childfree couples reflect on their decision-making processes and narrate some events as critical in their journeys (see Bhambhani and Inbanathan, Reference Bhambhani and Inbanathan2020). To understand the meanings and interpretations that couples assigned to their experiences, an interpretive paradigm was utilised. The participants in the study were primarily identified and contacted through social media groups of childfree members (primarily on Facebook), and some who were not part of these communities were referred by their friends and acquaintances, resulting in snowball or referral sampling. The participants were purposively selected for interviews based on the inclusion criteria: self-reported heterosexual childfree couples living in India and Canada, married (or in a common-law relationship in Canada), for at least four years in India and five years in Canada, and without known physiological issues that could prevent conception. The variation in the length of marital or common-law unions in India and Canada, as reflected in the inclusion criteria, was based on a first-birth interval of 1.5–2.5 years in India (Pratap et al., Reference Pratap, Kumar and Yadava2011). In Canada, since the pioneering study on voluntary childlessness in the 1970s (Veevers, Reference Veevers1980), the criterion of five or more years of marriage or common-law union has been used in research to capture the experience of pressure to reproduce from family and the community, which tends to increase after several years of marriage. Selected participants were first requested to complete a structured questionnaire on their personal and family background. This was followed by joint interviews of couples using a semi-structured interview guide to understand couples’ decision-making journeys to forego parenthood that covered various dimensions of their lives, including the use of contraception at different stages of their lives. After the interview, individual participants were sent a reflective journal to record any thoughts or responses that they could not share in their spouse’s presence or any reflections that occurred to them afterwards. None of the participants’ reflective journals mentioned details or experiences linked to their contraceptive use, so their analysis is not included in this paper. In all, thirty-six couples were jointly interviewed, eighteen each from Canada and India. The interviews were transcribed and analysed using ATLAS.ti, with open codes generated and then thematically analysed. The process of identifying and defining themes was iterative and reflective. Themes, sub-themes, and their connections were continually revisited to systematically organise the data into recognisable patterns of experience. These patterns were interpreted using a narrative enquiry approach, in which, at each stage of analysis, the interactions between participants’ personal narratives and their socio-cultural contexts were examined to explore what Connelly and Clandinin (Reference Connelly and Clandinin1990) called the personal and human dimensions of experience. To maintain participants’ anonymity, pseudonyms have been used, and despite using various details to contextualise their experiences against their biography, their individual identification remains extremely unlikely.
Study participants
The profiles of study participants across the two countries showed heterogeneity in education, occupation, ethnicity, and religiosity. Table 1 presents the demographic characteristics of male and female participants in Canada. The Canadian couples participating in the study had different relationship types, with six in common-law unions. Five of the married couples had been in common-law unions for one to four years before their marriage. The average length of couples’ relationships was 11.9 years, and they had been married or in a common-law union for 9.2 years. Three women and a man were in their second marriages or common-law unions. Only eight individual participants mentioned their religious affiliation: one who was a Buddhist, and the others were Christians. A majority of the participants had been residing in Canada for generations and, therefore, did not identify with a distinct ethnic identity. But among five couples, one or both spouses mentioned distinct ethnic identities, recalling experiences of immigrating to Canada or having parents who were first-generation immigrants. A couple was from West Asia, another from East Asia, and the remaining three were in interethnic marriages involving an East Asian-American couple, a German-American couple, and an Asian couple with spouses from different regions of Asia (i.e., South Korea and the Philippines). All the participants lived in a two-person household, with the majority having one or more pets (see Supplementary Information, Section B (2)).
Profile of individual participants in Canada

Source: Authors’ analysis of the data collected between 2017–18 (see Supplementary Information, Section B (1)).
The demographic profile of Indian participants, consisting of age, education, and occupation, is shown in Table 2. All the study participants in India were in their first marriage, and they courted their prospective spouses for an average of 2.7 years before getting married. The average duration of marriage was 7.8 years, within a range of 4 to 19 years. It is noteworthy that all but two couples made their own decisions about marriage and entered intergroup marriages with spouses from different regions, linguistic backgrounds, or religious affiliations. Marriages arranged by families remain common in India, and autonomy in marriage decisions remains quite limited, with self-chosen marriages reported to be as low as just 5% (Banerji and Deshpande, Reference Banerji and Deshpande2021; Reed, Reference Reed2025). The two couples involved their parents and extended families in the initial selection of potential spouses. The participants’ choice of spouses demonstrated their autonomy in marriage, which also influenced their decision to remain childfree, something that could have been harder if their families had arranged their marriages. More than half of the individual participants reported no religious affiliation. Among those who mentioned their faith, almost all were Hindus, except for one who was a Jain and one who was a Muslim. All except for one couple lived in two-person households, and ten of them had one or more pets. The one exceptional couple lived in a patrilocal joint household.
Profile of individual participants in India

Source: Authors’ analysis of the data collected between 2018–19 (see Supplementary Information, Section B (3)).
Though this study has a small sample size, it indicates a clear pattern across different cultures and countries in the characteristics of those who choose to remain childfree. Higher educational qualifications, engagement in professional and managerial roles, and a low level of religiosity characterised participants in India and Canada. Studies conducted in Canada and other countries of the Global North that have examined the rising trend of childlessness have analysed demographic factors that determine the likelihood of remaining childless, such as education, occupation, income, and religion. However, none of these demographic factors has a unidirectional effect on the likelihood of being childless. Instead, it is primarily a cumulative effect of several factors, each playing a different role to varying degrees (Veevers, Reference Veevers1980; Park, Reference Park2005; Mynarska et al., Reference Mynarska, Matysiak, Rybińska, Tocchioni and Vignoli2015).
Results
Choices of contraceptive use among childfree couples
To trace the participants’ decision-making regarding contraceptive use, details of the birth-prevention measures utilised and the discussions on contraception that they had during the course of being in a stable heterosexual union with their partners or spouses were sought. Distinctive strategies to prevent conception emerged in the accounts of couples from Canada and India, bringing to the fore differential preferences for various birth control measures. Among Canadian participants, the utilisation of a range of contraceptives at different stages of their relationship was observed. The majority of the Indian participant couples preferred and relied on the male barrier method. In addition to examining variations in birth control strategies across the two countries, we also explored whether there was a relation between the decision-making pathways involved in choosing to forego parenthood and the contraceptives utilised.
Decision-making pathways and choices in the methods of contraception
Building on the authors’ study of childfree couples’ decision-making journeys and the distinct pathways of early articulation and postponement of parenthood (see Bhambhani and Inbanathan, Reference Bhambhani and Inbanathan2020), a descriptive analysis examined whether these pathways affected the choice of specific contraceptive methods.
Table 3 presents the analysis of the methods of contraception among Canadian participants, revealing a diverse range of approaches adopted by couples over time. Many began with female-centric oral contraceptives, later transitioning to IUDs, and in two cases, opting for tubectomy. Similarly, three men who had previously relied on barrier methods or their partners’ use of oral contraceptives for several years later opted for vasectomy. This distribution of contraceptive choices across various decision-making pathways makes it difficult to establish a clear association between early articulation, or postponement in the decision to forego parenthood, and the contraceptive methods utilised.
Representation of decision-making pathways and contraceptive strategies of Canadian participant couples

Source: Author’s analysis of the data collected.
Analysis of the practices of contraception of the Indian participants, as represented in Table 4, revealed a predominant reliance on condoms across various decision-making pathways. Four wives initially used oral contraceptives, but later transitioned to the use of condoms as their husbands took on the responsibility of birth control. Notably, four couples occasionally used emergency contraception pills to mitigate pregnancy risks when condoms were not utilised. Only two wives switched to intrauterine devices (IUDs) after several years of marriage, and one husband opted for a vasectomy. These patterns suggest a consistent preference for barrier methods, regardless of the decision-making pathway, indicating no clear correlation between decision-making pathways and choices of contraceptives.
Representation of decision-making pathways and methods of contraception of Indian participant couples

Source: Author’s analysis of the data collected.
Given the absence of a definite relationship between decision-making pathways of early articulation and postponement and contraceptive methods among both Indian and Canadian couples, a thematic analysis was conducted. This analysis delved into the narratives of how couples negotiated their use of specific methods of contraception and responsibilities, shedding light on their journeys toward choosing and maintaining a childfree lifestyle.
Dynamics of contraceptive use over time among Canadian couples
In the early stages of their intimate relationships, the majority of male participants from Canada used a barrier method, while their female partners often used oral contraceptives at the same time. These dual methods of contraception were utilised to prevent sexually transmitted infections as well as unwanted conception. Arizona (age 40 years, married for seven years after being in a common-law union for two years, a teacher in Toronto) recounted, ‘I was always on pills. I took birth control pills since I was sixteen, including when I met him’. To this, her husband Mark (age 37, a graphic designer) added, ‘We also used condoms initially’. A similar pattern of using dual contraceptive methods was noted among all but two couples in the initial stage of their sexual intimacy.
In the case of two couples, it was the women participants who were solely responsible for the contraception and had been using oral contraceptives. Both these women participants, Jia (aged 37 years, married for eight years, a civil engineer, Toronto, Canada) and Anne (aged 36 years, married for ten years, a job seeker at the time of interview, Toronto), were immigrants from different Southeast Asian societies and were married to men from similar cultural backgrounds. In many societies across Southeast Asia and South Asia, the responsibility of contraception is often heavier on women. The low prevalence of condom use among married men in Southeast Asia and South Asia has been explained in terms of the cultural norms and practices that place women in a subordinate position and make it challenging for them to negotiate decision-making in sexual matters and contraceptive use (Wellings et al., Reference Wellings, Collumbien, Slaymaker, Singh, Hodges, Patel and Bajos2006). This is evident in the narratives of Jia and Anne, who were solely responsible for contraception without their husbands’ involvement in the decision-making, as reflected in the responses of Jia and Minsoo (aged 44 years, a stock trader):
‘Jia: No, we have never discussed’
‘Minsoo: On that side of things, she has always taken care. We have never sat down and said that this would be the best method. I have never asked her. Whatever she thinks is right for her, she does’.
Jia and Minsoo are shared postponers, as they arrived at the decision to forego parenthood by delaying parenthood for some years, and in the course of postponement, together they realised their disinclination to become parents. Despite mutually deciding to forego parenthood, the responsibility to prevent conception was borne by Jia alone. A similar account was shared by Anne, who, too, had arrived at the decision through shared postponement with her husband Li Jun (aged 43 years, an engineer), and yet she alone bore the responsibility of contraception. Moreover, Minsoo’s remark, ‘Whatever she thinks is right for her, she does’, manifests the traditional notion of women being responsible for birth control since they are the child bearers.
Unlike Jia and Anne, who solely assumed the responsibility for birth control, mutual early articulators, Marilyn (aged 37 years, married for seven years after being in common-law for four years, a graphic designer, Toronto), who has Southeast Asian roots and is married to George (aged 38 years, working in the entertainment industry) of European ancestry, narrated their discussion on their family planning steps:
‘George: Condom was a preferred method in the beginning. Then she just started birth control pills, and after a while, she told me that she was getting this five-year thing, and it can obviously be taken out if needed. I was like, “Fine, go for it” ’
‘Marilyn: The reason I switched to an IUD is that I didn’t want to take the pill every day, and it had a higher success rate. So that’s what it was. And I didn’t have to worry about human error a.k.a. my own error [chuckled]. IUD gives you 100 percent protection, so that was an important reason’.
The two noticeable attributes of Marilyn and George’s birth prevention decision, which varied from Jia and Anne’s accounts, were their inter-ethnic marriage and both partners had an equal disinclination towards parenthood from an early stage of their relationship (categorised as mutual early articulation). The utilisation of the barrier method by George in the initial stage of their relationship indicates his share of responsibility for the birth control. Besides, Marilyn’s openness to discuss her preference for a particular contraceptive with George demonstrates a sense of confidence in switching contraception practices together. However, Marilyn had to take charge of the change of contraception from oral pills to an IUD.
Most Canadian couples in the study had discussions when transitioning from a temporary contraception, such as condoms, to a long-term contraceptive, such as an IUD, regardless of whether the decision was made early in the relationship or reached through the postponement of parenthood. The IUD was the preferred contraception for many women participants, who viewed it as a convenient and long-acting way to avoid unintended conception. This was also due to the limited choices of contraceptives available to men, one being the barrier method and the other being sterilisation. In contrast, women have several options for contraception, including temporary and long-term methods. The dearth of male-dependent reversible contraceptives made it challenging for a majority of the Canadian male participants to initiate, participate equally in, and share the responsibility of birth control. However, the couples’ narratives indicated the active participation of men in the discussions on their female partners’ shift to long-term contraception.
Sterilisation: the decision and experiences of Canadian couples
As noted above, the primary reason for the majority of male participants’ inability to equally share the responsibility of contraception was the limited options available to men. Yet, three male participants from Canada waited until they reached an age when doctors were willing to perform the necessary surgical procedure, ultimately opting for sterilisation.
A mutual postponer couple, Eva and Arthur (ages 43 and 50, respectively, married for twenty-three years; Eva is an accountant, and Arthur is a professor, Lethbridge, Canada), narrated their journey of employing different birth control methods at different stages of their relationship and decision-making:
‘Arthur: Eva was using pills for, I think, the first decade, and then about 12 or 13 years ago, I had a vasectomy. She thought it [pill] was the best idea to start with because it was affordable, and we still hadn’t made the decision not to have kids. Once we did make that decision not to have kids, vasectomy made the most sense . . . Actually, before the procedure, they counselled me in ways like, it’s an irreversible method, and I could try other temporary methods. They, in fact, made me bring Eva in so that they could talk to both of us and ascertain that we were very dedicated and serious about the decision that we were making’.
‘Eva: I think age has also got to do with it because Arthur went three years earlier, and they declined, saying that he was too young’.
‘Arthur: Right’
‘Eva: but once you hit a certain age, it is less of an issue’.
The experience of transitioning from non-permanent to permanent contraception was similar for two other couples, where the male partners were early articulators and chose to undergo vasectomy after reaching a certain age and stage in their relationship. These selected accounts highlight an egalitarian division of responsibility for contraception, which was negotiated and shared at various stages in the process of initiating and sustaining a heteronormative childfree family.
Some women participants who were early articulators or unilateral postponers also considered permanent sterilisation. For instance, in the case of Alex (aged 44 years, entrepreneur) and Christy (aged 40 years, marketing professional, married for 12 years, Waterloo, Canada), after postponing parenthood for several years, it was Christy who conveyed her decision to remain childfree to Alex. When Christy was in her late 30s, her physician agreed to her request for sterilisation. However, in other cases, doctors refused to perform the procedure due to the women’s relatively young age and nulliparous status, prompting them to opt for long-acting contraception instead of their preferred sterilisation. In these instances, the women indicated that they had asked their partners to undergo a vasectomy but were unable to persuade them. For example, Nancy (aged 42 years, in a common-law relationship for 17 years, librarian, Quebec City), who had an IUD inserted after years of using oral contraceptives, narrated:
‘I asked [my partner] Roy why he doesn’t get a vasectomy, because we were obviously not going to have children, so having something permanent was an option. But he was afraid to tamper with his ‘manhood’, so he didn’t do it, and I was left to be in charge of our birth control’.
‘[Roy chuckled without saying a word]’
This comment reflects a prevalent misconception about the reduction in sexual potency, which often causes men to hesitate in contemplating an option that is considered to be simple, safe, and a practical contraceptive choice. Research has demonstrated that these methods have no negative impact on sexual potency (Engl et al., Reference Engl, Hallmen, Beecken, Rubenwolf, Gerharz and Vallo2017; Drobner et al., Reference Drobner, Fu, Kaldany and Velez-Leitner2023; Guo et al., Reference Guo, Lamberts and Eisenberg2015). A few other women participants had explicitly urged their partners to undergo sterilisation, but their partners either did not agree or said that they would consider it in the future if necessary. While these experiences align with the widespread reluctance to undergo vasectomy, clearly articulated by men, they diverge from trends in Canada, where vasectomy rates are notably higher than the global average and even surpass tubectomy rates (Jacobstein et al., Reference Jacobstein, Radloff, Khan, Mimno, Pal, Snell and Tripathi2023).
Diverging from the relatively high prevalence of vasectomy in Canada, the decision-making on the use of contraceptives, in this study, revealed that although male partners were involved in discussions about birth control, the responsibility for implementing the plan and maintaining a childfree lifestyle largely fell on the women. Fifteen out of eighteen women participants shouldered this responsibility, while only three men chose to undergo sterilisation.
Decision-making on the use of contraceptives among Indian childfree couples
Birth control measures and responsibility for contraception were significantly different between Indian participants and Canadian participants and reflected the underlying cultural and structural factors causing such disparity. The majority of the Indian participants employed the male barrier method as the preferred form of birth control from the beginning of their relationships. For instance, Mouni and Sachin (ages 40 and 41 years, respectively, married for eleven years, a medical doctor, and a teacher, respectively, Mumbai) described their discussions on the preference and concerns around the available birth control measures:
‘Mouni: Actually, because I work in the medical field, I am aware that no family planning method gives 100 percent protection . . . We looked for vasectomy and similar options, but unfortunately, we could not get one. We asked a couple of doctors, and they were laughing and were not ready to do it. They were like, “You are so young, why do you want to get it done? We cannot perform it on you”. So, we had to go for a more conservative form of contraception. Hormonal pills are a strict no for me because I know the side effects from them. So, we have just been relying on the barrier method. We, in fact, had this discussion before marriage itself’
‘Sachin: Frankly speaking, we discussed most of the things before marriage to avoid any issues later’
Mouni was an independent early articulator in their relationship and took charge of initiating discussions on various aspects of leading a childfree life, including contraception. She and her husband’s contemplation of permanent contraception for him, and the doctors’ reluctance to sterilise, resonated with a few other early articulators’ experiences. These couples considered sterilisation but could not obtain it because the doctors refused to perform the procedure, citing their ages and nulliparous status.
Indian women’s reservations against oral and long-acting reversible contraceptives
A majority of the women participants in India expressed some concern about the side effects of oral contraceptives, thereby reducing the options from which the participants could choose a suitable method. In fact, four women participants who had tried oral contraception for a short duration reported the inconvenience of regularly taking it and, after experiencing health problems, stopped oral contraception. Just two women participants had an IUD implanted, as their gynaecologists suggested that it would ease their menstrual health issues (see Supplementary Information, Section A (1)). The utilisation of IUD was, therefore, not a deliberate contraceptive choice that they made, yet it acted as an effective birth control apart from alleviating the menstrual health issues of the two women participants.
A majority of women participants from India argued that there was no need to consider a long-acting contraceptive. Even for relatively younger participants such as Priya (age 26, married for five years, a nutritionist, Chennai), getting a semi-permanent contraception was not usually contemplated, as she remarked,
‘I have never really felt the need to think about it. The condom has been serving our needs perfectly. Why would I unnecessarily meddle with my body? That is also one of the reasons why I don’t want to reproduce. I dread that it will alter my entire body’
Priya and other women participants who voiced their concerns about getting a long-acting contraceptive as ‘meddling with their body’ articulate accounts that are similar to those of women participants who cited concerns of side effects from consuming oral contraceptives. Several studies have indicated this as a larger systemic-level issue by describing how a lack of confidence in the various modern contraceptives available to women, particularly IUDs, plays a crucial role in the low prevalence of long-acting contraception in India (Mishra et al., Reference Mishra, Panda, Pyne, Srinivas, Pati and Pati2017; Gehani et al., Reference Gehani, Pal, Arya and Singh2019). Thus, Canadian participants saw an opportunity in the availability of greater contraception choices for females, and preferred to shift to a longer-acting method. Inadequate trust in the same methods formed the basis for Indian women participants’ continued support for their husbands’ use of the barrier method. In addition, the fear of conception persuaded the husbands to acquiesce to their wives’ preference, as evident in Lakhan’s remark (aged 31 years, a sales executive, married for five years, Chennai), ‘I am scared of accidents. So, we never have unprotected sex. But a couple of times when I have missed using it [a condom], I make sure that she takes an [anti-]pregnancy pill’. The use of emergency contraception by female participants who were otherwise relying on the male barrier method was another recurring aspect in the childfree lives of Indian participant couples. It further reflected their reliance on the transient methods of preventing births instead of opting for a long-acting method of contraception.
For couples who have gone beyond what might be considered the optimum age for having children, their ages added another justification for continuing with the male barrier method, as Apeksha (she is aged 45 years, married for fourteen years, an entrepreneur, residing in Bhimtal, India) pointed out,
‘We decided mutually. There is nothing long-term that we have done. Condoms sometimes, sometimes withdrawal and then of course, calendar days. But I think my age also plays in. I am 45, and so that fertile age for me has already passed’.
Throughout their marriage, Apeksha and her husband, Jitendra (aged 44 years, a marketing consultant), have consistently relied on condoms. This unwavering mutual preference and discussion by Indian participant couples on the male-driven barrier method contrasts with the evolving contraceptive choices over time made by Canadian participants. In Canada, couples initially relied on male condoms and female oral pills but later shifted to long-acting reversible IUDs, or, in five cases, sterilisation (three men and two women).
A few independent and mutual early-articulator Indian couples discussed sterilisation as a choice of contraceptive. However, as observed in the case of Mouni and Sachin in the preceding section, the doctors’ reluctance to perform it on young childless couples made them refrain from further consideration of a permanent method of contraception, at least for some years. The only Indian participant couple who relentlessly pursued a permanent method of birth control was Harsh and Parul (aged 34 and 31 years, respectively, married for four years, Harsh is a financial risk manager, and Parul is a holistic nutritionist, Pune, India). They recounted their experience of discussing and undergoing a vasectomy:
‘Harsh: At first, we both were thinking of getting it done’
‘Parul: Yeah, at first, we were thinking if we both should get it done, or if I should get it done, or if he should get it done. So, we were looking for what’s better. With that intention, we had gone to many gynaecs [gynaecologists] as well as urologists and general surgeons . . . So, we did a lot of research on the medical aspect of it. Like, will there be a problem for him during sex, or will he have pain while peeing, or will it [getting a tubectomy] affect my periods? So, all those things we wanted to clarify, because the childfree thing was already decided’.
‘Parul: Some docs told him, if you undergo a vasectomy and she wants a child later, what would you do then? So, I said, for any reason if you [referring to Harsh] feel insecure or anything, I am ready to get it [tubectomy] done. Because both of us are equally responsible for our decision to be childfree’.
Harsh was an independent early articulator in their decision-making, and even though he underwent sterilisation, Parul was equally involved in the decision-making as well as the responsibility to obtain the permanent contraception. Their narrative coincides with the accounts of the five Canadian participant couples who faced a similar reluctance from some doctors to perform sterilisation in the absence of any biological children. Although Canadian participants waited until a certain age, when doctors would be willing to carry out the vasectomy, Harsh and Parul did not stop trying until they found a doctor willing to perform the procedure, even when they were relatively young. Even before he underwent a vasectomy, Harsh was responsible for using the barrier method of contraception, as were all the other Indian male participants. This suggests that in the contraceptive decision-making of childfree couples in India, wives mainly initiated the choice of which method to use, while the actual responsibility for using the chosen method of birth control fell on the husbands.
Discussion
Having examined the decision-making in the choice of contraceptives of childfree couples, it is important to discuss the factors that lead individuals and couples to prefer or avoid specific contraceptives in two settings: India and Canada.
Beginning with the sterilisation method, the discussion covers whether the reluctance of couples to undergo sterilisation, among those who are otherwise committed to remaining childfree, suggests the possibility of reconsidering parenthood in the future. The hesitance to undergo sterilisation by the participants reflected a reluctance at two distinct levels in India and Canada. One was at the individual level, for instance, the reluctance of men to undergo sterilisation even when explicitly asked by their partners/spouses. And secondly, at the level of physicians, to provide sterilisation even when explicitly requested by childfree couples. Whether to undergo sterilisation or not, and whether to provide sterilisation or not, could be viewed as individual decisions concerning one’s body and the norms of medical practice. However, just as the participants’ decision to forego parenthood was a reflection and outcome of the pronatalist habitus they inhabit (Bhambhani and Inbanathan, Reference Bhambhani and Inbanathan2020), likewise, their decision to avoid sterilisation, or the doctor’s denial of the sterilisation when sought, could be embedded in the habitat of cultural and structural prerogatives and constraints.
Across the two cultural contexts, the men’s refusal to undergo sterilisation was situated in an apprehension of “tamper(ing) with his (their) ‘manhood’” (a phrase used by Nancy to describe her partner Roy’s denial of vasectomy). This apprehension has persisted in studies examining the relatively low number of vasectomies performed across cultures (Guo et al., Reference Guo, Lamberts and Eisenberg2015; Engl et al., Reference Engl, Hallmen, Beecken, Rubenwolf, Gerharz and Vallo2017; Drobner et al., Reference Drobner, Fu, Kaldany and Velez-Leitner2023). It is often posited that this stems from how masculinity is constructed and its link to coital reproduction as a symbol of virility. Notably, studies on vasectomised men mainly focused on those who had the procedure after having children. For these men, to some extent, having children could have served as a visible affirmation of their virility and, by extension, their masculinity. In contrast, the participants who did not have children lacked this tangible marker of masculinity. This absence, albeit voluntary, may have heightened their fear of losing a sense of masculinity, reinforcing the apprehension that undergoing sterilisation could be perceived as ‘tampering with their manhood.’
Besides men’s apprehension to undergo a vasectomy, women participants too were not found to be inclined towards sterilisation. Out of the eighteen women participants in Canada, only two underwent a tubectomy. In comparison, none of the women participants from India had undergone sterilisation. This is noteworthy because female sterilisation globally represents the largest share of contraception (UNDESA, 2022), and in India, it is the most commonly used method of contraception among married women and has increased in prevalence over the years (Jayakumar, Reference Jayakumar2024). Qualitative and ethnographic studies emphasising the experiences of women undergoing sterilisation reveal that many women seek this procedure due to a compelling need to prevent further pregnancies (Van Hollen, Reference Van Hollen1998, Reference Van Hollen2003; Luksaite, Reference Luksaite2016). This is often exacerbated by a lack of male partners taking responsibility for contraception, inadequate information on the other long-term contraceptive options and the perceived risks associated with them, and instances where sterilisations are performed on postpartum women without their consent or are persuaded to undergo sterilisation through incentivisation (Singh et al., Reference Singh, Singh and Singh2021; Jana and Shekhar, Reference Jana and Shekhar2023). These findings suggest that the high prevalence of female sterilisation in India cannot always be interpreted as a deliberate, informed choice by women. In many instances, it reflects a pressing need to prevent further pregnancies. In the present context, the lack of urgency to prevent births among the participants, who were nulliparous, makes sterilisation less of an immediate contraceptive need. The hesitance of childfree women in India to consider sterilisation as a contraceptive option emphasises the necessity to explore the contraceptive choices of childfree individuals and couples more broadly. This is noteworthy, especially since many studies in the Global North, including those conducted in Canada among childfree individuals and couples (Veevers, Reference Veevers1980; Richie, Reference Richie2013; Shreffler et al., Reference Shreffler, Tiemeyer, McQuillan and Greil2020; Parker et al., Reference Parker, Morse and Bryant2025), have primarily focused on sterilisation.
Other than sterilisation, the Indian women participants also displayed significant apprehension towards oral contraceptives, IUDs, and hormonal implants, and among the eighteen participant couples, seventeen primarily relied on male condoms. The exception was one male participant who had undergone a vasectomy, along with two women who later opted for an IUD after several years of managing with male condoms that their husbands used. The two women participants who later opted for an IUD did so not as a contraceptive measure but upon their gynaecologists’ recommendation to alleviate their menstrual health issues. Indian women participants explicitly affirmed their reluctance to oral and long-acting contraceptives, as conveyed in the excerpt, ‘Why would I unnecessarily meddle with my body?’ (Priya, aged 26 years, married for five years, a nutritionist, Chennai). This expression, ‘unnecessary meddling’ with their bodies, resonates with male participants’ apprehension of ‘tampering with their manhood’ if they undergo a vasectomy. Oral contraception usage was reported by only 4.3% of married women (15–49 years) in India, while IUD usage was reported by 2.7% in the NFHS 5 (2019–21) (IIPS & ICF, 2021). It is also noteworthy that although all the participants were highly educated (holding bachelor’s degrees or higher) and were working professionals – factors typically linked to a greater use of modern contraceptives and not sterilisation (Ewerling et al., Reference Ewerling, McDougal, Raj, Ferreira, Blumenberg, Parmar and Barros2021; Singh et al., Reference Singh, Singh and Singh2021; Bansal et al., Reference Bansal, Dwivedi and Ali2022) – their reluctance suggests that building institutional trust is crucial for encouraging the use of modern contraceptives. In other words, in the decision-making related to the use of contraceptives, individual factors such as education, occupation, and income interact with the institutional enablers and constraints to determine the preferred form of contraception.
An examination by feminist scholars of decision-making in the use of contraceptives (Nandagiri, Reference Nandagiri2021; Morison et al., Reference Morison, Macleod and Ndabula2025) suggested that the family planning programs, both international and national, have increasingly emphasised the person-centric, voluntary approach, with a vision to empower women and girls through improving accessibility and availability of contraception. However, they often fail to acknowledge the institutional and structural barriers that an individual faces when making a ‘voluntary’ decision. These institutional and structural barriers involve the absence of trained doctors and staff, inadequate medical supplies, counselling services for individuals who need to be sensitised on diverse options of contraceptives, and the provider bias of the high-risk populations (often along the intersectional lines of class, race/ethnicity, ability, education, age, marital status, parity, and other socio-economic attributes) (Manzer et al., Reference Manzer, Ouellette, Tingey, Carrillo-Perez, Hogan, Atkins and Blum2024; Morison et al., Reference Morison, Macleod and Ndabula2025). The discussion now turns to the Indian women participants’ avoidance of oral contraceptive pills or an IUD implant, as these were perceived as ‘meddling with their bodies’, leading them to prefer male condoms as the main form of contraception. The absence of a shared awareness of positive experiences with oral contraceptives or IUDs, coupled with the widespread presence of misconceptions, could have further reinforced the participants’ perception of using these methods as ‘meddling with their bodies’. In a recent systematic review of studies on misconceptions about long-acting reversible contraceptives (LARC), the widespread belief that they cause infertility and that they are unsuitable for young, nulliparous women was noted. These misconceptions prevailed not only among the public but also among physicians. Consequently, many physicians often discourage their use among young, nulliparous women (Kirubarajan et al., Reference Kirubarajan, Li, Yau, Yu, Got, Li and Sobel2022).
The interaction between individual characteristics and institutional factors is corroborated by the high use of long-acting contraceptives among Canadian women participants. In contrast to the Indian women participants, all but one of the Canadian women participants had used oral contraception for several years before transitioning to other methods, including IUDs (6 participants), tubectomies (2 participants), and vasectomies (3 participants). This approach to contraceptive use is notably different from that of the Indian women participants, who expressed a strong aversion to oral and long-acting contraceptives. As discussed in the background on birth control in Canada, oral contraceptives are among the most commonly used methods (CCHS 2019–20). A notable shift towards IUDs and sterilisation is also observed, particularly among women over 50 and couples aged 25 to 49 years (Statistics Canada, Reference Canada2025). When women in a community use a variety of birth-control methods, the participants’ exposure to these methods and trust in them cannot be inferred as solely based on their individual characteristics, such as education, occupation, and income. Instead, it is shaped by a collective contraceptive culture, where individuals are influenced by shared experiences and observations regarding the usage and prevalence of different methods of contraception. Such a collective contraceptive culture is, in turn, situated in the institutional emphasis on sex education as a fundamental human right to promote sexual health and well-being (SIECCAN, 2019). This contrasts with India, where sex education largely revolves around and is primarily directed at married couples (Tripathi and Shekhar, Reference Tripathi and Sekher2013). The Canadian women participants’ active use of oral contraceptives and later IUDs is, thus, situated in their early exposure to a variety of contraceptives through comprehensive sex education; a shared culture of women using oral contraceptives and IUDs; and the availability, accessibility, and affordability of these options.
The discussion revisits sterilisation, one of the most effective and permanent forms of contraception for those who have had their desired number of children or do not wish to have any children. Yet, just one participant in India and five participants in Canada (two tubectomies and three vasectomies) reported undergoing the procedure. The sole Indian participant (aged 34 years, married for four years, a financial risk manager, Pune, India) to undergo a vasectomy, an independent early articulator, had explicitly stated his desire to remain childfree to Parul (aged 31 years, a nutritionist) before they were married. Like him, and based on the studies that indicate sterilisation as a preferred contraceptive choice among childfree individuals (Richie, Reference Richie2013; Mui and Costescu, Reference Mui and Costescu2021; Parker et al., Reference Parker, Morse and Bryant2025), early articulating participants were assumed to have undergone sterilisation or planned to do so in the future. This was based on the consideration that early articulators had decided to forego parenthood even before they married or entered a common-law union. However, among the five Canadian participants who underwent sterilisation, two were postponers, i.e., couples who postponed parenthood for several years and eventually decided to remain childfree. This observation, along with the study’s qualitative approach and small, non-representative sample size, cannot conclusively establish an association between decision-making pathways (i.e., early articulation and postponement) and the decision to undergo sterilisation. However, a noteworthy convergence of experiences in the decision to undergo sterilisation emerged in the two countries. First, in the initial years of their marriage or common-law union (Canada), the participants relied on temporary contraceptive methods such as oral pills, condoms, and IUDs in a few instances and later decided to undergo sterilisation. For postponers, it was an obvious decision, as in the early years of their marriage or common-law union, they were unsure whether to have children. For early articulators, this reliance on temporary and reversible contraceptives, however, was primarily situated in the challenges encountered in finding a physician willing to perform the sterilisation. Similar challenges were also narrated by postponer couples who later decided to remain childfree and transition to sterilisation. These challenges entailed visiting numerous physicians and not finding a doctor who agreed to provide sterilization on the first visit. The cautionary remarks from the physicians narrated by the participants, ‘you are too young’ (Arthur, aged 50 years, Lethbridge, Canada) and ‘[what if] she wants children later’ (Harsh, aged 34 years, Pune, India), underscore the challenges they experienced. It is crucial to consider if such cautionary remarks and denials emanate from the medico-legal guidelines that the physicians are expected to abide by or if the personal beliefs of the physicians influenced their decision to deny sterilisation. Both Canada and India are among the nations with laws explicitly permitting sterilisation for contraceptive purposes (Scott and Glasier, Reference Scott and Glasier2003). Yet there are differences in the criteria for contraception seekers who can avail of sterilisation. In Canada, the sterilisation could be provided to any adult who does not desire a future pregnancy, who has also been informed about alternate methods of contraception, understands the permanence of the procedure, and has given informed consent (Black et al., Reference Black, Guilbert, Costescu, Dunn, Fisher, Kives, Mirosh, Norman, Pymar, Reid, Roy, Varto, Waddington, Wagner, Whelan, Ferguson, Fortin, Kielly, Mansouri and Todd2015). The Canadian Contraception Consensus, in fact, explicitly states ‘age and parity should not be a barrier to permanent contraception’ (p. 1035). In India, the eligibility criteria for male and female sterilisation include the following conditions: seekers must be married; females must be over 22 years of age, and males must be under 60 years of age; the couple should have at least one child who is over one year old, unless there are medical reasons for sterilization; and the spouse should not have undergone sterilisation in the past (MoHFW, 2006). Age, marital status, and parity constitute criteria for seeking sterilisation in India, which are distinct from the Canadian requirements.
In India, the doctors could have cited the government guidelines to refuse sterilisation. Yet they used cautionary remarks about the participants’ age and nulliparous status, similar to the Canadian participants’ experiences. The personal influence of doctors on an adult’s health-related decisions has been conceptualised as ‘medical paternalism’ (see Supplementary Information, Section A (2)) and is often manifested as provider bias. Age and marital status have been found to be the most common reasons for provider bias in provider-dependent contraceptives such as IUDs, implants, and sterilisation (Solo and Festin, Reference Solo and Festin2019) and are violative of the SRHR approach adopted in the International Conference on Population and Development (United Nations, 1995) (see Supplementary Information, Section A (3)).
This study does not capture physicians’ perceptions and lacks a representative sample. However, these accounts, even if considered anecdotal, emphasise the importance of examining healthcare providers’ perceptions and reasons for not offering sterilisation to nulliparous individuals and couples. Moreover, since the study is based on a non-representative sample of 36 participant couples from India and Canada, the findings do not claim to reflect the contraceptive decision-making of all heterosexual couples who choose to remain childfree. Nevertheless, its focus on exploring an underexamined group in contraceptive research could be vital for future studies with a representative sample on the contraceptive needs of childfree individuals and couples. Finally, while the study utilised a joint interview approach and attempted to capture each spouse’s reflections through email-requested journals after the interviews, none of the participants mentioned contraceptives in their journals. Future research could consider conducting individual interviews as well as joint couple interviews to more effectively examine each spouse’s perspective on decision-making related to contraceptive use.
Conclusion
The study participants’ decision-making processes regarding the use of contraceptives, much like their decision to remain childfree, show that what might seem like a straightforward decision between having or not having children, or between temporary or permanent contraception, is actually a complex process. Just as the participants’ realisation of their desire to forego parenthood involved a prolonged and challenging process of unlearning deeply ingrained pronatalist norms that view procreation as the normative expectation in heterosexual unions (see Bhambhani and Inbanathan, Reference Bhambhani and Inbanathan2020), their decisions on contraceptive use required continuous reflection, deliberation, and negotiation. They carefully considered which contraceptives aligned with their conviction to remain childfree, evaluated the available options, and navigated the willingness or reluctance of partners to share equally in the responsibility of contraception. This process of reflection, deliberation, and negotiation may seem an interpersonal matter between a couple. However, this study emphasises that it is situated in the context of cultural and institutional influences and limitations. The cross-cultural perception of vasectomy’s association with the perceived loss of masculinity made the male participants reluctant to undergo the procedure. Furthermore, the institutional limitation of only condoms and vasectomies as male-centric contraceptives restricted men’s involvement in contraceptive decision-making. Similarly, the reluctance of Indian women to use oral contraception and IUDs was situated in the collective concern of their side effects and inadequate institutional efforts to address them. On the other hand, Canadian women participants’ active use of oral and long-term contraceptives was situated in their early exposure to these contraceptives, as well as their widespread availability and prevalence in Canada. Moreover, the challenges encountered by childfree couples seeking sterilisation in both societies highlight a cultural bias in providing this option to nulliparous couples, based on the assumption that they may later regret the decision. This is despite the institutional guidelines, at least in Canada, explicitly stating that age and parity should not be barriers to obtaining sterilisation. This study suggests the importance of examining decision-making in the use of contraceptives by considering the interplay between individual characteristics, such as education, occupation, and income, and cultural and institutional influences. This approach could uncover the underlying factors behind using or avoiding contraception, whether for childfree individuals and couples or those who have children.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0021932026100649.
Acknowledgements
The authors wish to acknowledge the International Union for the Scientific Study of Population for offering a platform at the International Population Conference 2025, where an earlier version of this paper was presented and received constructive feedback. The authors also express deepest gratitude to the Institute for Social and Economic Change in Bengaluru, India, and the Centre for Feminist Research at York University in Toronto, Canada, for their mentorship, supportive environment, and infrastructure that enabled this study.
Funding statement
The research for this article was financially supported by the Shastri Indo-Canadian Institute and Jawaharlal Nehru Memorial Fund, New Delhi.
Competing interests
The authors have no conflicts of interest to declare.
Ethical standard
The study was conducted in compliance with the ethical guidelines set by the Office of Research Ethics at York University in Toronto and the Institute for Social and Economic Change in Bengaluru.
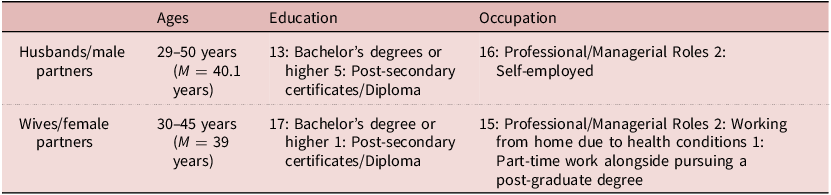

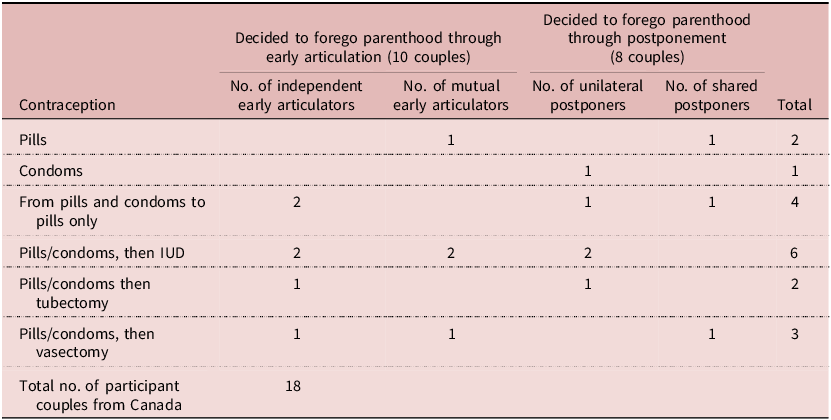
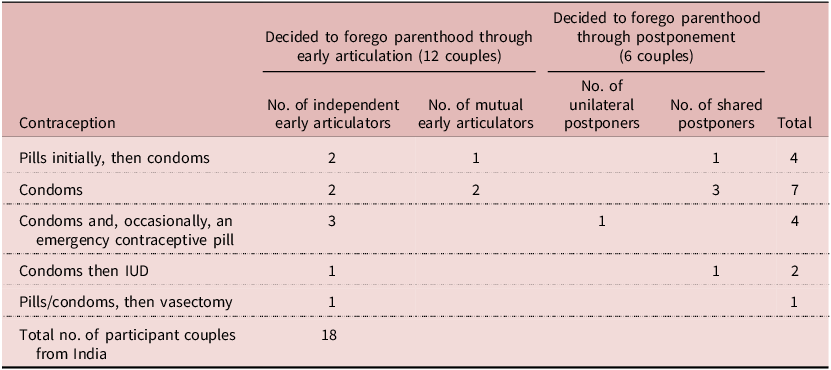



 Open access
Open access