


Introduction
Adverse childhood experiences are related to long-term psychological, social, and physical health difficulties (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards and Koss1998). Among these experiences, child maltreatment is commonly categorized as emotional, physical, and sexual abuse, and emotional and physical neglect (Norman et al., Reference Norman, Byambaa, De, Butchart, Scott and Vos2012; Wang, Chen, Zhou, & Zhang, Reference Wang, Chen, Zhou and Zhang2023). Depression is among the most frequently examined outcomes of maltreatment, given its prevalence and global disease burden (Murray et al., Reference Murray, Vos, Lozano, Naghavi, Flaxman, Michaud and Ezzati2012; World Health Organization, 2017).
Historically, research has emphasized sexual abuse, reflecting assumptions about its comparatively severe psychological consequences (Gardner, Thomas, & Erskine, Reference Gardner, Thomas and Erskine2019; Infurna et al., Reference Infurna, Reichl, Parzer, Schimmenti, Bifulco and Kaess2016). Accordingly, early meta-analyses focused largely or exclusively on sexual abuse (e.g. Jumper, Reference Jumper1995; Neumann, Houskamp, Pollock, & Briere, Reference Neumann, Houskamp, Pollock and Briere1996). As research expanded, meta-analyses began addressing additional maltreatment forms, and more recent reviews have included multiple forms within the same analytic framework to allow cross-form comparisons (e.g. Li, D’Arcy, & Meng, Reference Li, D’Arcy and Meng2016; Norman et al., Reference Norman, Byambaa, De, Butchart, Scott and Vos2012).
In the past decade, a series of meta-analyses has synthesized associations between depression and emotional, physical, and sexual abuse, and – less consistently – emotional and physical neglect (e.g. Gardner et al., Reference Gardner, Thomas and Erskine2019; Humphreys et al., Reference Humphreys, LeMoult, Wear, Piersiak, Lee and Gotlib2020; Mandelli, Petrelli, & Serretti, Reference Mandelli, Petrelli and Serretti2015). These reviews have advanced comparative understanding, and their key characteristics are summarized in Table 1.
Previous meta-analyses of child maltreatment (assessing emotional, physical, and sexual abuse at the minimum) versus depression, from 2015 to 2024

Note: CM, child maltreatment; EA, emotional abuse; EN, emotional neglect; PA, physical abuse; PN, physical neglect; SA, sexual abuse; N, neglect (both EN and PN); OR, odds ratio; d, Cohen’s d; g, Hedge’s g; r, standardized correlation coefficient; zr, Fisher’s z transformation from r.
a In Kuzminskaite et al. (Reference Kuzminskaite, Gathier, Cuijpers, Penninx, Ammerman, Brakemeier and Bruijniks2022) and Souama et al. (Reference Souama, Lamers, Milaneschi, Vinkers, Defina, Garvert and Stein2023), individual-study effect sizes for CM forms were not provided in the publications or online, so data from them were not included in the present meta-analyses.
b A quarter to a half the r-effect sizes in Lai et al. (Reference Lai, Fan, Man and Huang2023) and Li et al. (Reference Li, Gao, Su, Zhang, Yang, D’Arcy and Meng2023) were point-biserial and were converted to ORs for analysis; the remaining were Pearson’s correlations, entered into the severity analyses.
c Some of the ORs in Yu et al. (Reference Yu, Cao, Shang and Li2024) were identified as based on Pearson’s correlations; these were entered into the severity analyses instead.
Key limitations of previous meta-analyses
Most prior meta-analyses of maltreatment versus symptoms have used single-level models and treated effect sizes from different maltreatment forms as independent – the case for almost all the reviews in Table 1 (exceptions were Lai et al., Reference Lai, Fan, Man and Huang2023, who employed multilevel models, and Nelson et al., Reference Nelson, Klumparendt, Doebler and Ehring2017, who used single-level models but employed robust variance estimation to address dependencies). However, primary studies have frequently reported multiple effect sizes for several maltreatment forms, making those estimates statistically dependent. Ignoring this dependence can bias pooled estimates and invalidate cross-form comparisons (Assink & Wibbelink, Reference Assink and Wibbelink2016; Cheung, Reference Cheung2014; van den Noortgate, López-López, Marín-Martínez, & Sánchez-Meca, Reference van den Noortgate, López-López, Marín-Martínez and Sánchez-Meca2013).
A second limitation concerns between-samples confounds. Many prior reviews included large numbers of studies that assessed only one or two maltreatment forms. If samples contributing effect sizes for different maltreatment forms differ systematically – for example, if researchers studying sexual abuse versus physical abuse disproportionately recruit different populations – then comparisons of pooled effects may conflate true differences with sample composition. More comparable estimates arise from ‘complete-form’ studies assessing most or all maltreatment forms, because sample characteristics are held constant across those forms.
Emerging pattern
Despite these limitations, an overall pattern emerges across existing meta-analyses: emotional abuse and emotional neglect often show the strongest associations with depression, whereas sexual abuse tends to yield comparatively smaller effects (e.g. Humphreys et al., Reference Humphreys, LeMoult, Wear, Piersiak, Lee and Gotlib2020; Infurna et al., Reference Infurna, Reichl, Parzer, Schimmenti, Bifulco and Kaess2016; Nelson, Klumparendt, Doebler, & Ehring, Reference Nelson, Klumparendt, Doebler and Ehring2017; Yu, Cao, Shang, & Li, Reference Yu, Cao, Shang and Li2024). These findings suggest a central role for emotional maltreatment, though the methodological issues noted earlier temper the strength of this inference.
The present study
We employed effect size data provided by the source meta-analyses (Table 1), eliminating duplicates. First, we compared all five child maltreatment forms (emotional, physical, and sexual abuse; emotional and physical neglect) in relation to depression. To account for statistical dependence within samples, we employed multilevel random-effects meta-analyses, with Level 1 representing sampling variance among effect sizes and Level 2 modeling the clustering of multiple effect sizes within studies (Cheung, Reference Cheung2014; Konstantopoulos, Reference Konstantopoulos2011). We performed two types of meta-analyses: risk (i.e. depression as a binary outcome, based on diagnoses—e.g. Mandelli et al., Reference Mandelli, Petrelli and Serretti2015—or dichotomized symptom scores—e.g. Gardner et al., Reference Gardner, Thomas and Erskine2019) and severity (i.e. depression and maltreatment as continuums). Second, focusing just on abuse, we meta-analyzed effect sizes (risk and severity) from ‘complete-abuse’ samples (assessing all three forms of abuse) and then ‘incomplete-abuse’ samples (assessing only one or two abuse forms) to address the issue of between-samples confounds.
Using these approaches, we obtained (a) pooled associations between each maltreatment form and depression; (b) direct pairwise comparisons among the forms; and (c) estimates of heterogeneity (Q, I 2) within the multilevel framework. This design along with the huge set of samples and effect sizes offered a methodologically more rigorous comparison of how different maltreatment experiences relate to depression than previous meta-analytic reviews.
Based on the pattern emerging from prior reviews (Table 1), we hypothesized that emotional abuse would exhibit the strongest association with depression, whereas sexual abuse would show substantially weaker associations. We further expected that this hierarchical pattern among abuse forms would emerge most clearly in analyses restricted to complete-abuse samples. In contrast, we anticipated greater inconsistency in analyses based on incomplete-abuse samples, which assessed only one or two abuse forms and therefore confounded comparisons with between-samples differences. Across all analyses, our overarching goal was to obtain valid comparative estimates and establish a credible ranking of maltreatment forms in their associations with depression, based on wide-ranging samples geographically (e.g. from the U.S. to China) and compositionally (e.g. from clinical to representative).
Method
Search and inclusion criteria
We conducted a systematic search for published meta-analyses examining associations between child maltreatment and depression. Eligibility was restricted to reviews that reported separate effect size estimates for at least three forms of maltreatment – emotional, physical, and sexual abuse. This criterion ensured provision of comparative estimates of key maltreatment forms and increased the likelihood that source studies included multiple maltreatment forms.
Searches were conducted on January 30, 2025, using Google Scholar and SciSpace. For Google Scholar, the following terms were entered: meta-analysis, child maltreatment, and depression. For SciSpace, the following query was entered: ‘Give a list of meta-analyses of child maltreatment and depression’. Two researchers with meta-analytic experience (the first author and an independent coder) independently screened the outputs. Because Google Scholar ranks results by relevance rather than enforcing strict term matching, screening on that platform was limited to the first 100 results, after which retrieved records were largely irrelevant to the research question. Reviews were retained for further consideration if their titles included the terms meta-analysis and either depression or depressive, along with child maltreatment or a related term indicating exposure to adverse experiences in childhood (e.g. abuse, adverse childhood experiences, trauma).
Abstracts of selected reviews were then examined. Following discussion and consensus, full texts were obtained for reviews, in which provision of separate effect size estimates for emotional, physical, and sexual abuse in relation to depression was considered possible. No restriction was placed on publication year.
Full texts were independently evaluated to determine whether they reported separate meta-analytic effect size estimates for at least emotional, physical, and sexual abuse. Intercoder agreement was complete. Reviews meeting this criterion were retained for analysis. Reference lists of included reviews were also examined to identify additional eligible meta-analyses.
Ten reviews, published between 2015 and 2023 and comprising 12 meta-analyses, met the inclusion criteria. As a recheck and final verification step, the search was repeated on January 20, 2026, using identical search terms, to determine whether additional eligible reviews had become listed or were originally missed. Two were found and added (Lai, Fan, Man, & Huang, Reference Lai, Fan, Man and Huang2023; Yu et al., Reference Yu, Cao, Shang and Li2024), yielding a final sample of 12 reviews encompassing 14 meta-analyses, which were used to extract effect size data for the present meta-analyses (Table 1). Two additional reviews deemed eligible (Kuzminskaite et al., Reference Kuzminskaite, Gathier, Cuijpers, Penninx, Ammerman, Brakemeier and Bruijniks2022; Souama et al., Reference Souama, Lamers, Milaneschi, Vinkers, Defina, Garvert and Stein2023) did not provide effect size data in their publication or online; hence, their data did not enter the present meta-analyses (for completeness, their results are also included in Table 1). A flowchart summarizing this updated search and selection process is provided in Figure 1.
Flowchart of included reviews.

Although this study is not a primary-level systematic review and therefore did not implement a full PRISMA protocol, the meta-analytic reviews from which effect sizes were drawn almost uniformly reported PRISMA-compliant searches, screenings, and reporting procedures, sometimes with preregistered protocols. In addition, several of these reviews formally evaluated the quality or risk of bias of original studies using established tools (e.g. the Newcastle–Ottawa Scale, NIH Quality Assessment Tool, or structured quality checklists), generally finding that most included studies met moderate to good quality thresholds (e.g. LeMoult et al., Reference LeMoult, Humphreys, Tracy, Hoffmeister, Ip and Gotlib2020; Li et al., Reference Li, Gao, Su, Zhang, Yang, D’Arcy and Meng2023; Mandelli et al., Reference Mandelli, Petrelli and Serretti2015; Tan & Mao, Reference Tan and Mao2023; Wang et al., Reference Wang, Chen, Zhou and Zhang2023; Yu et al., Reference Yu, Cao, Shang and Li2024). Where examined, study quality did not significantly moderate effect size estimates, and sensitivity analyses excluding lower quality studies yielded comparable results (e.g. LeMoult et al., Reference LeMoult, Humphreys, Tracy, Hoffmeister, Ip and Gotlib2020; Mandelli et al., Reference Mandelli, Petrelli and Serretti2015). Other reviews suggested that publication bias, when present, had only modest influence on pooled estimates (e.g. Humphreys et al., Reference Humphreys, LeMoult, Wear, Piersiak, Lee and Gotlib2020; Nelson et al., Reference Nelson, Klumparendt, Doebler and Ehring2017). Thus, while this review did not independently assess study quality, it drew on an evidence base that was systematically evaluated for methodological rigor and potential sources of bias, providing relevant context for interpreting the findings summarized here.
Definitions of child maltreatment
This research examined emotional, physical, and sexual abuse, plus, if assessed in the reviewed research, emotional and physical neglect. Definitions of the child maltreatment forms here reflect their definitions in the included studies, which were based on measures such as the Childhood Trauma Questionnaire (Bernstein & Fink, Reference Bernstein and Fink1998), the Adverse Childhood Experiences Questionnaire (Felitti et al., Reference Felitti, Anda, Nordenberg, Williamson, Spitz, Edwards and Koss1998), and the Maltreatment and Abuse Chronology of Exposure Scale (Teicher & Parigger, Reference Teicher and Parigger2015). Definitions varied across measures and studies, but their conceptual cores can be outlined as follows.
Emotional abuse referred to repeated acts of verbal hostility, rejection, humiliation, or threats by caregivers or adults, which undermine a child’s emotional development and self-worth (Teicher, Samson, Polcari, & McGreenery, Reference Teicher, Samson, Polcari and McGreenery2006). Examples include name-calling, belittling, and making the child feel unwanted.
Emotional neglect involved persistent failure to meet a child’s basic needs for affection, support, and belonging (Glaser, Reference Glaser2002). Examples include a lack of warmth shown to the minor or a lack of comfort provided during distress.
Physical abuse denoted intentional use of physical force that results in, or potentially results in, injury (Gilbert et al., Reference Gilbert, Widom, Browne, Fergusson, Webb and Janson2009). Examples are hitting, kicking, slapping, or burning.
Physical neglect referred to chronic failure to provide for a child’s basic physical needs, including failure to provide food, clothing, hygiene, medical care, and protection (Dubowitz, Pitts, & Black, Reference Dubowitz, Pitts and Black2004).
Definitions for sexual abuse were more varied than those for other maltreatment forms (e.g. in types of acts, ages involved). In general, they focused on unwanted, negative sexual experiences before age 18 with other minors or adults (Bernstein & Fink, Reference Bernstein and Fink1998; World Health Organization, 2020). Less often, they were based solely on age-discrepancies, for instance, sexual experiences before age 18 with someone at least 5 years older, including willing encounters (Wyatt, Reference Wyatt1985).
Data extraction
Effect size extraction was performed by the first author. Effect sizes were obtained directly from the included meta-analytic reviews (Table 1), taken from tables or figures in the publications or online, when provided (as noted previously, two reviews did not provide these data). When information in a review was unclear or missing, effect sizes were extracted from the source studies.
For the risk analyses, odds ratios, Cohen’s ds, and Hedges’ gs (with 95% confidence intervals) were converted to log odds with corresponding standard errors (Cooper, Hedges, & Valentine, Reference Cooper, Hedges and Valentine2019). Point–biserial correlations (in Lai et al., Reference Lai, Fan, Man and Huang2023 and Li et al., Reference Li, Gao, Su, Zhang, Yang, D’Arcy and Meng2023) were likewise converted to log odds with standard errors. For the severity analyses, in which both maltreatment and depression were assessed using continuous scales, Pearson’s correlations (with 95% confidence intervals) were converted to Fisher’s zs with standard errors, and reported Fisher’s zs (in Humphreys et al., Reference Humphreys, LeMoult, Wear, Piersiak, Lee and Gotlib2020) were entered directly, with confidence intervals converted to standard errors.
Duplicates of source studies across reviewed meta-analyses were removed (if their reported effect sizes differed, effect sizes were extracted from the source studies). When a source study reported multiple effect sizes for the same maltreatment form (e.g. different age groups), effect sizes were aggregated following standard procedures (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2009) to avoid violating independence. However, effect sizes were kept separate by sex, consistent with practices in the reviewed meta-analyses.
Finally, information on moderating variables was extracted by both coders from information provided in the reviews, or from each source study when necessary, including publication year, maltreatment measure, sample type (case–control, representative, clinical, convenience), sample size, percentage of female participants, country or region, and language of assessment.
Statistical analyses
Two-level random-effects multilevel meta-analyses were conducted in JASP (JASP Team, 2025). Level 1 represented the sampling variance of effect sizes, whereas Level 2 modeled the clustering of multiple effect sizes within studies, thereby accounting for their statistical dependence (Cheung, Reference Cheung2014; Konstantopoulos, Reference Konstantopoulos2011). When dependencies are addressed directly through an appropriate multilevel structure, additional corrections such as robust variance estimation are generally unnecessary and may yield overly conservative standard errors (Borenstein, Hedges, Higgins, & Rothstein, Reference Borenstein, Hedges, Higgins and Rothstein2021; Cheung, Reference Cheung2014; Hedges, Tipton, & Johnson, Reference Hedges, Tipton and Johnson2010).
Restricted maximum likelihood (REML) estimation was used. Residual heterogeneity was evaluated using the Q statistic, which tests whether the observed variability in effect sizes exceeds what would be expected from sampling error alone after accounting for the predictors in the model. The I 2 statistic quantified the proportion of total observed variance attributable to true heterogeneity rather than sampling error. Moderator analyses were conducted using metaregression within the multilevel framework.
Pairwise comparisons among maltreatment forms were conducted using iterative reference-category coding. With five maltreatment forms (three abuse, two neglect), this produced 10 planned pairwise contrasts, requiring a Bonferroni-adjusted familywise significance level of α = .005. A separate set of contrasts examined only the three abuse forms, yielding three pairwise comparisons and a Bonferroni-adjusted α = .017. As noted earlier, risk (binary outcome; analyzed using log odds) and severity (continuous outcome; analyzed using Fisher z) were examined in parallel models. For interpretability, log-odds estimates were converted to odds ratios, and Fisher’s z values were converted to Pearson’s rs.
Results
Effect size dependencies
We first examined the extent to which effect sizes for different maltreatment forms were statistically dependent within samples. Because complete-abuse studies (i.e. those assessing all three abuse forms) provided the fullest information for pairwise comparisons, we restricted this analysis to those samples. Log-odds ratios (risk) and Fisher’s z (severity) correlations were examined separately.
Effect sizes were strongly correlated across maltreatment forms (Table S1 in the Supplementary Material). For risk, all pairwise correlations were significant, with a median r = .46. For severity, all but one were significant, with a median r = .48. These substantial cross-form correlations confirm that effect sizes were not independent within studies, supporting our use of multilevel modeling to account for statistical dependence.
Multilevel meta-analyses: all samples and maltreatment forms
Our initial multilevel meta-analyses drew on all effect sizes extracted from the 12 eligible meta-analytic reviews. Although all reviews assessed at least the three abuse forms, individual primary studies varied: some assessed all five maltreatment forms, whereas many assessed only one or two.
Depression risk
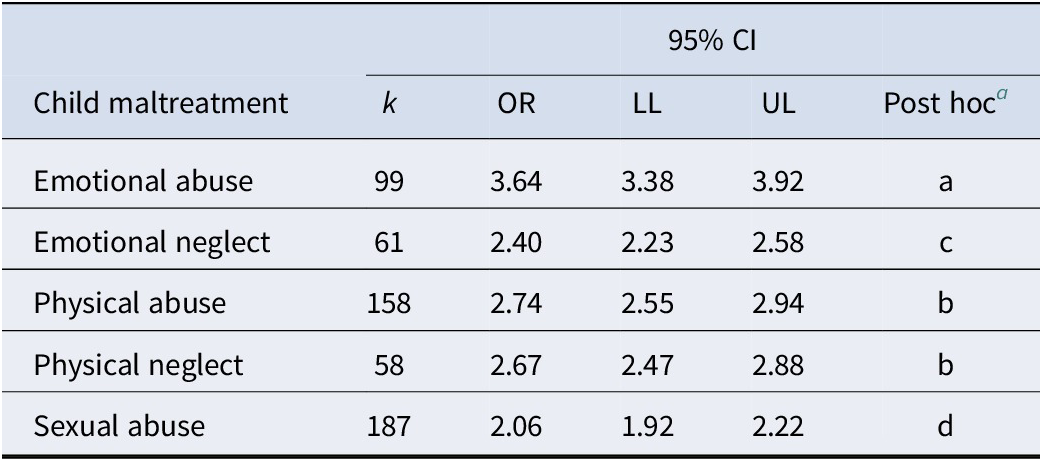
Table 2 summarizes results for depression risk (225 samples, 217 studies; 563 effect sizes; N = 379,383). Emotional abuse showed the strongest association with depression (OR = 3.64, 95% CI [3.38, 3.92]). Sexual abuse showed the weakest association (OR = 2.06, 95% CI [1.92, 2.22]). Physical abuse and physical neglect (ORs = 2.74 and 2.67, respectively) exceeded sexual abuse, whereas emotional neglect was intermediate (OR = 2.40). Substantial residual heterogeneity was observed, Q(558) = 6844.18, p < .001, I 2 = 91.8%.
Meta-analysis (multilevel, random-effects, all samples) of risk of depression in relation to five forms of child maltreatment, employing samples used in meta-analyses from 2015 to 2024
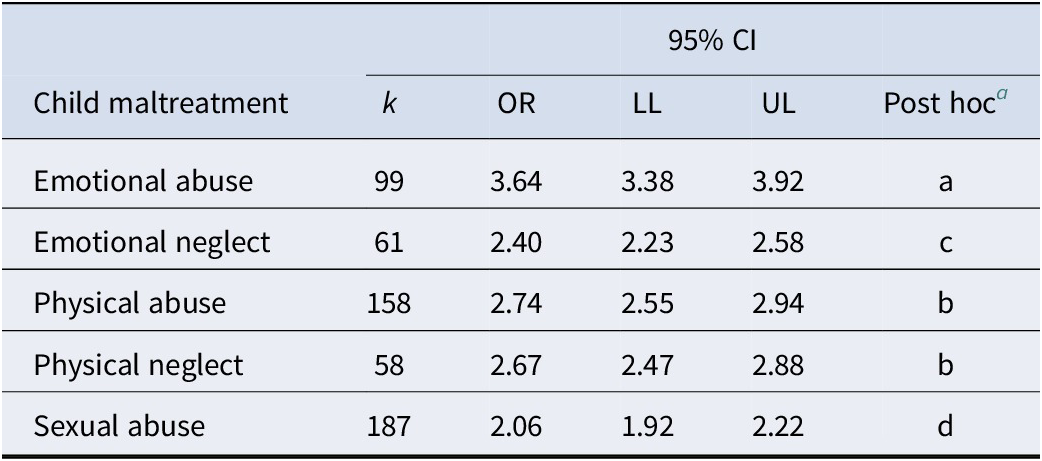
k, number of samples for a given maltreatment; OR, odds ratio risk of depression; Q(558) = 6844.18, p < .001; I2 = 91.8%.
a Maltreatments without common letters (in last column) were significantly different at Bonferroni-adjusted alpha level of .005.
Depression severity
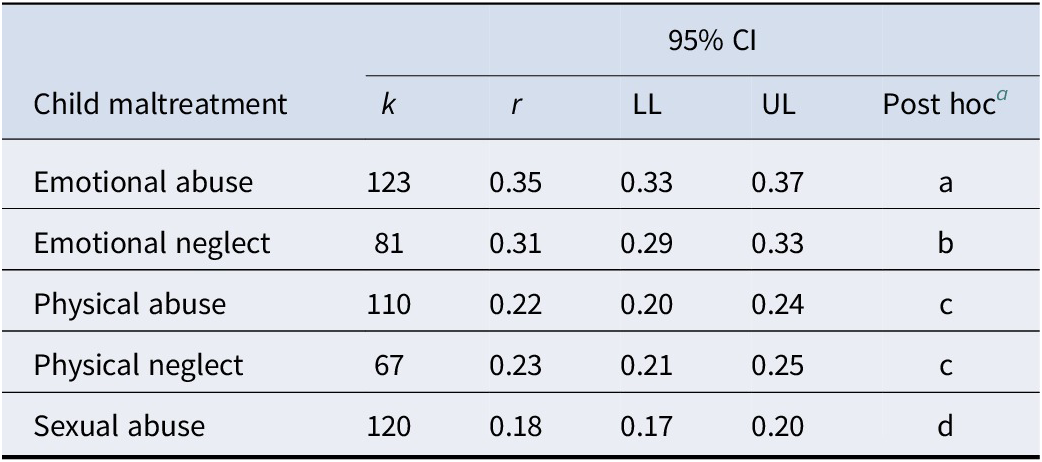
Results for severity (162 samples, 157 studies; 501 effect sizes; N = 87,659) appear in Table 3. Emotional abuse again showed the strongest association (r = .35, 95% CI [.33, .37]), followed by emotional neglect (r = .31, 95% CI [.29, .33]). Sexual abuse was least associated (r = .18, 95% CI [.17, .20]). Physical abuse and physical neglect were intermediate. Heterogeneity remained high, Q(496) = 4068.66, p < .001, I 2 = 87.8%.
Meta-analysis (multilevel, random-effects, all samples) of severity of child maltreatment versus severity of depression, employing samples used in meta-analyses from 2015 to 2024
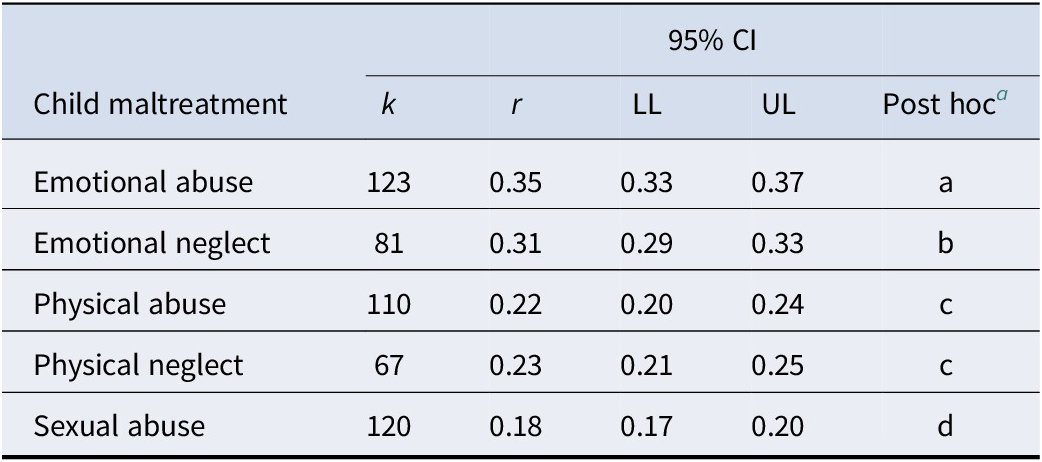
k, number of samples for a given maltreatment; r, Pearson’s correlation representing magnitude of association between severity of maltreatment and severity of depression; Q (496) = 4068.66, p < .001; I2 = 87.8%.
a Maltreatments without common letters (in last column) were significantly different at Bonferroni-adjusted alpha level of .005.
Complete-abuse versus incomplete-abuse samples
We next examined whether the pattern of associations depended on whether studies assessed all three abuse forms (complete-abuse samples) or only one or two (incomplete-abuse samples). Neglect forms were excluded from this comparison because incomplete studies too infrequently assessed them, making parallel comparisons infeasible.
Depression risk
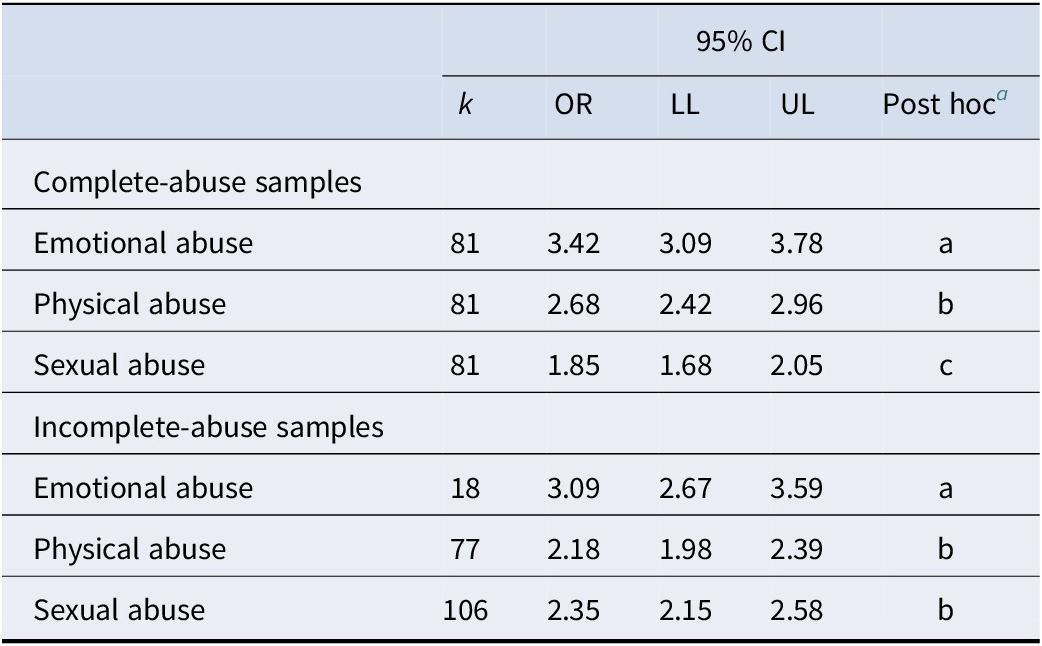
Results for complete-abuse samples (k = 81; effect sizes = 356; N = 71,054) appear in Table 4 (upper panel). A clear hierarchy emerged: emotional abuse produced the largest increase in risk (OR = 3.42, 95% CI [3.09, 3.78]), sexual abuse the smallest (OR = 1.85, 95% CI [1.68, 2.05]), with physical abuse intermediate (OR = 2.68, 95% CI [2.42, 2.96]). Heterogeneity was high, Q(240) = 2446.21, p < .001, I 2 = 90.2%.
Meta-analysis (multilevel, random-effects) of risk of depression in relation to the three abuse forms of child maltreatment, conducted separately for complete- and incomplete-abuse samples, employing samples used in meta-analyses from 2015 to 2024
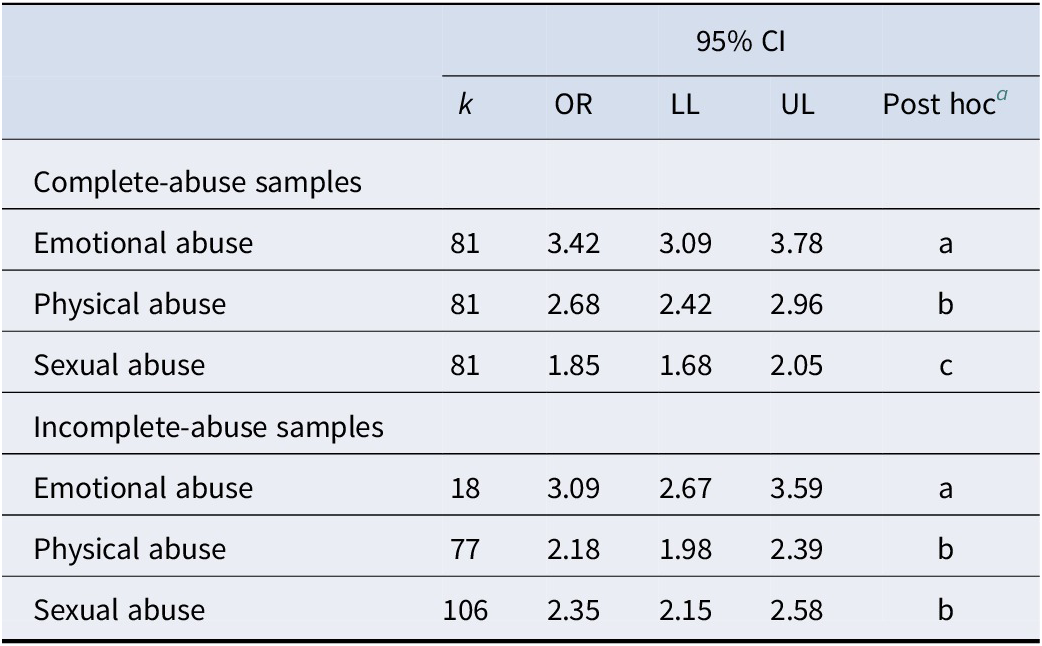
Complete-abuse samples assessed all 3 abuses (emotional, physical, sexual); incomplete-abuse samples did not. k, number of samples for a given maltreatment; OR, odds-ratio risk of depression. Complete-abuse: Q(240) = 2446.21, p < .001; I 2 = 90.2%. Incomplete-abuse: Q(198) = 1166.14, p < .001; I 2 = 83.0%.
a Maltreatments without common letters (in last column) were significantly different at Bonferroni-adjusted alpha level of .0167.
For incomplete-abuse samples (k = 144; effect sizes = 207; N = 308,329), the pattern was attenuated (Table 4, lower panel). Emotional abuse reduced somewhat but retained the highest association (OR = 3.09), while sexual abuse increased (OR = 2.35), nominally exceeding physical abuse (OR = 2.18). Heterogeneity remained substantial, Q(198) = 1166.14, p < .001, I 2 = 83.0%.
Depression severity
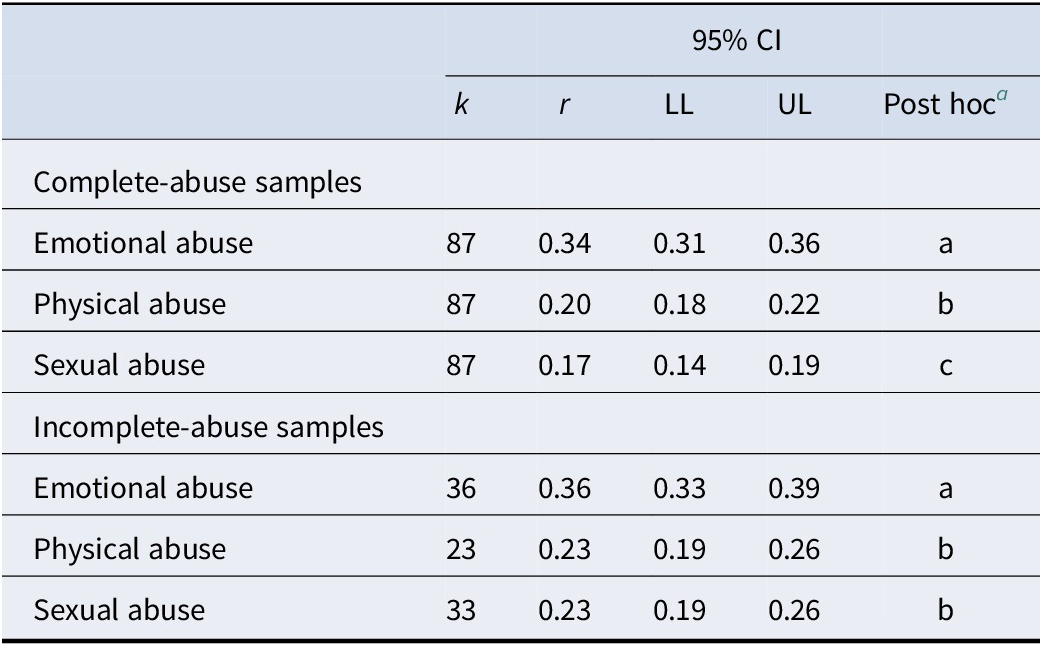
Severity analyses for complete-abuse samples (k = 87; effect sizes = 386; N = 51,747) again produced a clear hierarchy (Table 5, upper panel): emotional abuse (r = .34) > physical abuse (r = .20) > sexual abuse (r = .17). Heterogeneity was high, Q(258) = 2021.76, p < .001, I 2 = 87.2%.
Meta-analysis (multilevel, random-effects) of severity of depression in relation to severity of the three abuse forms of child maltreatment, conducted separately for complete- and incomplete-abuse samples, employing samples used in meta-analyses from 2015 to 2024

Complete-abuse samples assessed all 3 abuses (emotional, physical, sexual); incomplete-abuse samples did not. k, number of samples for a given maltreatment; r, Pearson correlation representing magnitude of association between severity of maltreatment and severity of depression. Complete-abuse: Q(258) = 2021.76, p < .001; I 2 = 87.2%. Incomplete-abuse: Q(89) = 526.11, p < .001; I 2 = 83.1%.
a Maltreatments without common letters (in last column) were significantly different at Bonferroni-adjusted alpha level of .0167.
Among incomplete-abuse samples (k = 75; effect sizes = 115; N = 35,912), emotional abuse remained significantly strongest (r = .36), but sexual abuse increased notably relative to the complete-abuse analysis (r = .23 vs .17), becoming equal to physical abuse (r = .23). Heterogeneity was substantial, Q(89) = 526.11, p < .001, I 2 = 83.1%.
All maltreatment forms in complete-abuse studies
Complete-abuse studies (unlike incomplete-abuse studies) provided enough neglect data to allow a full five-form comparison. For risk, emotional abuse showed the strongest association (k = 81, OR = 3.79, 95% CI [3.39, 4.24]). Physical abuse (k = 81, OR = 2.98, 95% CI [2.66, 3.33]) was equivalent to physical neglect (k = 55, OR = 2.80, 95% CI [2.50, 3.14]). Emotional neglect (k = 58, OR = 2.49, 95% CI [2.23, 2.79]) was moderately lower. Sexual abuse (k = 81, OR = 2.06, 95% CI [1.84, 2.30]) was significantly lowest. Heterogeneity was very high, Q(351) = 5019.20, p < .001, I 2 = 93.0%.
For severity, emotional abuse (k = 87, r = .33; 95% CI, [.31, .35]) was significantly more correlated with depression than emotional neglect (k = 64, r = .30; 95% CI [.28, .32]), which was greater than physical neglect (k = 61, r = .22; 95% CI [.20, .25]), which was greater than physical abuse (k = 87, r = .20; 95% CI [.17, .22]). Sexual abuse was significantly least associated (k = 87, r = .17; 95% CI [.14, .19]). Heterogeneity remained high, Q(381) = 3087.26, p < .001, I 2 = 87.7%.
Moderator analyses
Bivariate multilevel metaregressions were conducted for publication year, maltreatment measure, sample type, sample size, percentage of female participants, country, and language of assessment. Moderators satisfying p < .10 were entered into a multivariate model, when two or more moderators satisfied this criterion, with the following results.
For risk, the multivariate model was significant, F(5, 524) = 5.40, p < .001. Sample type, F(3, 524) = 5.14, p < .01, and sample size, F(1, 524) = 5.05, p = .025, were significant moderators, while percentage female, F(1, 524) = 2.78, p = .096, was a marginally significant moderator. Jointly, these moderators reduced unexplained heterogeneity by 23.5%. Case–control samples yielded larger effects than clinical samples. Smaller sample sizes yielded larger effect sizes, but only modestly (the spread from one standard deviation below to one above the mean was narrow; Table S2 in the Supplementary Material). Thus, there was minor evidence for small sample bias. Higher proportions of female participants were marginally significantly associated with larger effects.
For severity, multivariate metaregression was not performed because only one moderator met the criterion of p < .10. Sample type was significant, F(3, 496) = 4.06, p < .01, reducing residual heterogeneity modestly (R 2 change = 6.8%). Representative samples showed smaller effects than convenience samples (Table S3 in the Supplementary Material).
Discussion
This study synthesized data from 12 meta-analytic reviews to provide the most methodologically comparable examination to date of how five forms of child maltreatment relate to depression. By restricting certain analyses to source studies that assessed most maltreatment forms – thereby reducing between-samples confounds – and by modeling statistical dependence via multilevel meta-analysis, we were able to evaluate cross-form differences with greater validity than prior reviews. Across analytic layers, emotional abuse consistently emerged as the form most strongly associated with depression, whereas sexual abuse yielded the weakest associations. Emotional neglect approached emotional abuse in magnitude in the severity analysis. Physical abuse and physical neglect showed intermediate associations. These findings refine the emerging conclusion that emotional maltreatment – particularly emotional abuse – has a strong link to depressive outcomes.
A key contribution of the present work is demonstrating how analytic design shapes cross-form comparisons. Complete-abuse studies, which assessed all three abuse forms within the same sample, provided the most internally valid test because they held sample characteristics constant across forms. In these studies, a consistent hierarchy emerged: emotional abuse > physical abuse > sexual abuse. This pattern appeared for both depression risk and severity and was replicated across effect size metrics. In contrast, analyses of incomplete-abuse studies – paralleling the structure of most prior reviews – showed much weaker differentiation. In these analyses, sexual abuse estimates increased to equal or nominally surpass those for physical abuse. Our results indicate that this inflation does not reflect true stronger effects but rather systematic differences in the populations and research designs used for certain maltreatment forms. This methodological artifact clarifies inconsistencies across the literature and underscores the necessity of complete-form samples for valid cross-form comparisons.
The multilevel analyses also confirmed that effect sizes for different maltreatment forms were statistically dependent within studies: correlations among forms were substantial (median rs ≈ .46–.48). This dependence is expected, given shared developmental pathways, environmental contexts, and measurement approaches across maltreatment types. If unmodeled, such dependence can distort pooled estimates and inflate Type I errors in pairwise contrasts. By modeling these dependencies directly through a multilevel structure, the present analyses yielded more accurate standard errors and effect size estimates than single-level models typically used in earlier reviews.
Prominence of emotional maltreatment in depressive outcomes
Although emotional abuse consistently produced the largest associations with depression, emotional neglect was also relatively strongly associated – exceeding physical abuse and physical neglect in the severity analysis. This pattern aligns with theoretical perspectives emphasizing the importance of emotional communication, validation, and caregiver attunement for the development of depressive cognitions and emotion-regulation capacities (e.g. Rose & Abramson, Reference Rose, Abramson, Cicchetti and Toth1992). Emotional maltreatment directly shapes interpersonal schemas and self-evaluative processes central to depression (Bowlby, Reference Bowlby1982), and its theoretical coherence and biological plausibility (Bradford Hill, Reference Bradford Hill1965) in relation to depression are supported by cross-cultural evidence (e.g. Khaleque & Rohner, Reference Khaleque and Rohner2002) and nonhuman primate models (e.g. Suomi, Reference Suomi1991, Reference Suomi1997, Reference Suomi2011).
In contrast, although sexual abuse has historically been regarded as uniquely harmful (Gardner et al., Reference Gardner, Thomas and Erskine2019; Infurna et al., Reference Infurna, Reichl, Parzer, Schimmenti, Bifulco and Kaess2016; Mandelli et al., Reference Mandelli, Petrelli and Serretti2015), its association with depression in the present analyses was notably smaller than that of emotional abuse. While emotional abuse produced medium-to-large effects (per Cohen, Reference Cohen1988; Salgado, Reference Salgado2018), sexual abuse yielded small-to-medium effects. This difference is clinically meaningful, particularly because emotional abuse is roughly three times more prevalent than sexual abuse, combining rates for boys and girls (World Health Organization, 2014). These findings support recent calls for greater prioritization of emotional abuse in global prevention initiatives (World Health Organization, 2014).
Limitations
Several limitations should be noted. First, most source studies relied on retrospective self-reports, which may inflate associations of maltreatment with maladjustment relative to prospective research (Baldwin, Coleman, Francis, & Danese, Reference Baldwin, Coleman, Francis and Danese2024). Second, although multilevel modeling accounted for within-study dependencies, substantial residual heterogeneity remained, suggesting the influence of additional moderators – such as genetic factors, cultural norms, maltreatment chronicity, and co-occurring adversities (Baldwin et al., Reference Baldwin, Sallis, Schoeler, Taylor, Kwong, Tielbeek and Barkhuizen2023a, Reference Baldwin, Wang, Karwatowska, Schoeler, Tsaligopoulou, Munafò Marcus and Pingault2023b; Khan et al., Reference Khan, McCormack, Bolger, McGreenery, Vitaliano, Polcari and Teicher2015). Third, because this study was a review of reviews, certain relevant original studies may have been missed, especially more recent ones.
Finally, caution is needed in assuming causal effects in the present findings, given potential confounds. Forms of child maltreatment frequently co-occur, and observed associations with depression may therefore be only partially causal. Or they may reflect preexisting vulnerabilities that both increase the likelihood of maltreatment exposure and contribute to later maladjustment (Baldwin et al., Reference Baldwin, Sallis, Schoeler, Taylor, Kwong, Tielbeek and Barkhuizen2023a, Reference Baldwin, Wang, Karwatowska, Schoeler, Tsaligopoulou, Munafò Marcus and Pingault2023b, Reference Baldwin, Coleman, Francis and Danese2024; Humphreys et al., Reference Humphreys, LeMoult, Wear, Piersiak, Lee and Gotlib2020; Infurna et al., Reference Infurna, Reichl, Parzer, Schimmenti, Bifulco and Kaess2016). Genetically informed meta-analytic evidence indicates that genetic liability accounts for a substantial proportion of the risk of exposure to child maltreatment (approximately 40%; Dahoun et al., Reference Dahoun, Peel, Baldwin, Coleman, Lewis, Wertz, Rijsdijk and Danese2025). Further, associations between maltreatment and mental health outcomes are markedly attenuated (by approximately 45%) when adjusting for nonmaltreatment factors, including genetic influences (Baldwin et al., Reference Baldwin, Sallis, Schoeler, Taylor, Kwong, Tielbeek and Barkhuizen2023a). Accordingly, estimates of the relative strength of associations across maltreatment forms in this study should be interpreted as descriptive patterns rather than direct indicators of causal impact.
Conclusion
Despite these limitations, the present findings provide a strengthened empirical foundation for theory, prevention, and intervention. The consistent prominence of emotional abuse – and, to a lesser degree, emotional neglect – suggests that emotional maltreatment warrants increased attention in clinical assessment and public-health prevention efforts, which have historically emphasized physical and sexual abuse. Future work should further refine models of emotional maltreatment, examine developmental timing and subtype distinctions, and prioritize designs that assess multiple maltreatment forms within the same sample to permit valid comparative inferences.
Overall, this study offers a methodologically rigorous synthesis showing that emotional abuse has the strongest association with depression, whereas sexual abuse has the weakest. By reducing between-samples confounds and explicitly modeling statistical dependence, the present analyses resolved several longstanding inconsistencies and reinforced the fundamental link between emotional maltreatment and depressive outcomes.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S003329172610381X.
Acknowledgements
AI (ChatGPT) was occasionally used to sharpen phrasings in the text.
Competing interests
The authors declare none.





 Open access
Open access