


Duration of untreated illness (DUI) in anxiety disorders represents one of the most overlooked yet clinically crucial dimensions in contemporary psychiatry. DUI, defined as the time between symptom onset and adequate treatment, is a strong predictor of prognosis across disorders: prolonged delays are consistently linked to poorer outcomes, reduced treatment response, higher recurrence rates and persistent functional impairment. Reference Altamura and Camuri1
In anxiety disorders, DUI conceptualisation is more complex: the variability of onset (insidious versus acute), the multiplicity of subthreshold symptoms and avoidance and the role of non-pharmacological interventions complicate its measurement. Some studies define DUI as time to first pharmacological treatment (e.g. antidepressants, benzodiazepines, pregabalin), whereas others include psychotherapy. In addition, ‘onset’ may be defined as either first symptoms, first distressing symptoms, first full-syndromal onset or first help-seeking.
Anxiety disorders affect nearly 300 million people worldwide, representing the most prevalent group of psychiatric conditions and impacting approximately 1 in 3 individuals during their lifetime. Nevertheless, the average delay between symptom onset and adequate treatment initiation ranges from 1 to 10 years and, in some conditions, may extend to 15 years.Reference Altamura and Camuri1
Each additional untreated year significantly worsens prognosis – raising the risk of major depression by 15–20%, increasing vulnerability to substance misuse and reinforcing chronic disability. Despite these consequences, DUI is rarely assessed in routine practice and no health system systematically monitors or targets it, representing a major missed opportunity for early intervention and secondary prevention.Reference Surace and Baldessarini2
Despite its clinical importance, DUI remains largely absent from psychiatric guidelines and service models. This editorial outlines its relevance in anxiety disorders, reviews available evidence, highlights disorder-specific barriers to timely care and proposes pragmatic strategies to shorten treatment delay. We argue that DUI should be established as an actionable quality indicator in psychiatry, with a role comparable to early-intervention frameworks in psychosis.
The current evidence on DUI in anxiety disorders
Although the concept of DUI is well established in psychosis research, systematic studies in anxiety disorders are more limited. Epidemiological investigation nevertheless reveals consistent patterns: anxiety disorders frequently follow a chronic course when untreated, and delayed treatment initiation can significantly reduce the probability of full remission and functional recovery.
Population-level data suggest a median episode length of 7.5 months and a mean duration of 15.2 months, yet nearly 40% of patients remain symptomatic at 12 months and 30% continue to experience significant symptoms at 36 months.Reference Altamura and Camuri1 These findings challenge the misconception that anxiety disorders are self-limiting or benign; instead, delays in treatment can entail a trajectory of chronicity and relapse, ultimately increasing disability over time.
Treatment delay, however, is not uniform across disorders. Social anxiety disorder (SAD) consistently shows the longest untreated duration, with patients often waiting over a decade before receiving any form of evidence-based care.Reference Altamura and Camuri1 Panic disorder often shows shorter delays to first clinical contact yet treatment pathways remain suboptimal, with benzodiazepines still commonly prescribed earlier and for a longer period of time than guideline-recommended interventions (e.g. selective serotonin reuptake inhibitors (SSRIs) and serotonin–noradrenaline reuptake inhibitors (SNRIs)Reference Grancini and De Caro3). In generalised anxiety disorder (GAD) the gradual onset, blurring the line between personality traits and psychopathology, can complicate the recognition and measurement of DUI.Reference Bandelow and Michaelis4 Specific phobias, despite their circumscribed focus and favourable prognosis with exposure therapy, may remain untreated for years due to avoidance strategies.
Finally, agoraphobia often progresses insidiously to severe restriction of functioning, particularly when emerging secondary to panic disorder.Reference Bandelow and Michaelis4
Disorder-specific DUI patterns
Duration of untreated illness varies significantly across anxiety disorders, reflecting disorder-specific barriers to recognition, help-seeking and access to evidence-based care. Understanding these heterogeneities is crucial to designing tailored early intervention strategies.
SAD: the longest delays
Treatment delay in SAD is typically 10–15 years, representing one of the most protracted latencies to treatment in psychiatry.Reference Bandelow and Michaelis4 SAD often emerges during adolescence, a critical developmental window when social skills, academic performance and career trajectories are shaped. Symptoms are frequently misattributed to personality traits (e.g. ‘shyness’), leading to normalisation rather than clinical recognition and delaying appropriate therapeutic intervention. Each year of untreated SAD can increase the risk of major depression, substance misuse and relational difficulties. Consequences reverberate across education, employment and interpersonal domains, creating cascading disadvantages that compound over time. These delays are compounded by self-stigma and fear of negative judgement, which paradoxically hinder help-seeking.
Panic disorder: suboptimal treatment pathways
Naturalistic studies report an average delay of 5.4 years before patients with panic disorder receive guideline-recommended treatment (e.g. SSRIs and SNRIs), whereas benzodiazepines are typically prescribed earlier, within 2.9 years.Reference Grancini and De Caro3 This gap highlights prescribing attitudes favouring rapid symptomatic relief at the expense of long-term stability. Prolonged reliance on benzodiazepines, however, may entail tolerance, misuse and dependence, delaying recovery and compounding morbidity.
GAD: the problem of insidious onset
GAD exemplifies the difficulties of defining and assessing DUI in gradually developing conditions. Patients frequently describe themselves as lifelong ‘worriers’, normalising pathological anxiety as personality style or life stress. This adaptation masks impairment, fosters resignation and delays help-seeking. By the time GAD is diagnosed, years of functional impairment may accumulate and chronic worry patterns become more resistant to treatment.Reference Piccoli, Bergamaschini, Molteni, Vanzetto, Varinelli and Viganò5
Specific phobias and agoraphobia: avoidance, progression and delayed treatment
Avoidance-based disorders such as specific phobias and agoraphobia often remain undetected for years, allowing maladaptive patterns to solidify. In phobias, avoidance can create a false sense of adaptation, masking impairment and delaying help-seeking, despite the high effectiveness of brief exposure-based treatments – making prolonged DUI a preventable source of disability.
Agoraphobia, especially when linked to panic disorder, typically progresses towards increasing functional restriction, at times leading to home confinement. Across anxiety and obsessive–compulsive spectrum disorders, untreated periods often exceed 2 years, correlating with greater chronicity, comorbidity and poorer treatment response.Reference Altamura and Camuri1
Assessment challenges
Unlike psychotic disorders, where DUI can be measured through standardised instruments, anxiety disorders lack validated tools in this respect. Retrospective interviews, such as the Composite International Diagnostic Interview, combined with Life Chart methods, provide some structure but remain vulnerable to recall bias.Reference Altamura and Camuri1
Disorder-specific features further complicate assessment. In SAD, the gradual developmental trajectory blurs the threshold between personality traits and psychopathology. In panic disorder, panic attacks are discrete markers, but distinguishing isolated, situational attack from full disorder requires nuanced assessment. In GAD the pervasive, fluctuating nature of worry defies episodic framing. In phobias, impairment may be limited to specific contexts, leaving other life domains apparently intact.
Recognition challenges in children and adolescents: for disorders with childhood or adolescent onset – particularly SAD and GAD – accurate determination of illness onset is further complicated by developmental and familial factors. Children with anxiety disorders often have a parent with an anxiety disorder who may have accommodated and normalised their symptoms, delaying recognition and help-seeking. This intergenerational pattern of normalisation can obscure the distinction between temperament and emerging psychopathology. Additionally, anxiety symptoms in children are frequently misattributed by medical and psychological practitioners as personality style (e.g. ‘shy’, ‘cautious’) rather than the onset of a diagnosable disorder, contributing to underdetection and prolonged DUI.
Moreover, systemic factors in primary care – brief consultations, coding practices prioritising symptoms over diagnosis, lack of continuity – reinforce diagnostic delays. Without standardised tools and system-level prioritisation, DUI remains under-assessed and underestimated.
Clinical and public health implications
The implications of prolonged DUI may be profound. From a clinical perspective, a longer DUI is associated with poorer treatment response, with data showing that GAD patients with a shorter versus longer DUI to first antidepressant treatment (≤12 months) experienced better clinical improvement.Reference Piccoli, Bergamaschini, Molteni, Vanzetto, Varinelli and Viganò5 Moreover, although well studied in psychosis, there is emerging evidence suggesting that prolonged DUI (and duration of illness) may be associated with brain abnormalities, including the reduced left putaminal grey matter volume observed in patients with panic disorder. Longer untreated illness allows time for secondary complications to develop, such as comorbid depression and substance misuse, as well as social and occupational dysfunction. In fact, extended delays predict not only worse psychiatric outcomes but also broader social costs,6 including unemployment, reduced educational attainment, impaired relationships and increased healthcare utilisation. From a public health perspective, therefore, reducing DUI could represent a cost-effective strategy to alleviate the burden of anxiety disorders.
Nevertheless, DUI is not merely a temporal marker. It reflects broader systemic failures: failure to recognise early symptoms, to provide timely access and to prioritise preventive intervention. In this sense, DUI reduction represents a cultural shift in psychiatry, moving from crisis-driven responses toward proactive, early and integrated care.
Intervention strategies
Reducing DUI requires multi-level, coordinated strategies spanning universal prevention, early detection and disorder-specific interventions.
Universal approaches
-
(a) Primary care integration: screening tools for anxiety should be embedded in routine consultations, with systematic follow-up and referral protocols. Reference Dell’Osso and Oldani7 However, it is important to acknowledge that many individuals lack access to primary care altogether, which remains the initial gateway to mental health resources. Expanding primary care access – through training of nurses, nurse practitioners, social workers and physician assistants in the early identification of anxiety symptoms – is essential to reducing DUI at the population level.
-
(b) Pharmacological stewardship: in line with current treatment guidelines, clinicians should favour evidence-based, first-line interventions (e.g. SSRIs and SNRIs), using benzodiazepines only in the short term. Reference Grancini and De Caro3
-
(c) Continuity of care: building systems that track patients across healthcare touch-points can prevent long periods of unnoticed impairment. Nonetheless, the feasibility of continuity models depends on adequate access to both primary and specialist care, which is not universally available.
Disorder-specific approaches
-
(a) SAD: school-based screening, psychoeducational programmes targeting adolescents, teachers and parents, and low-threshold youth services are priority interventions. Particular attention should be given to children of adults with anxiety disorders, who represent a high-risk group. These families would benefit from psychoeducation about the importance of early recognition and the potential harms of prolonged DUI, as well as from efforts to reduce stigma and normalise early mental health intervention. Engaging these parents as allies in reducing DUI may be one of the most impactful strategies. Additionally, training teachers in the early identification of impairing anxiety is essential, because they are well positioned to recognise children who are outliers in their classes and may benefit from early support. Reference Bandelow and Michaelis4
-
(b) Panic disorder: emergency departments should implement panic screening protocols and structured referral to psychiatric care.
-
(c) GAD: chronic disease management models should integrate GAD screening, leveraging primary care to detect insidious onset, because patients often present at first to non-psychiatric specialists – such as general practitioners, cardiologists or gastroenterologists – due to somatic symptoms or stress-related complaints. As noted earlier, recognition in childhood and adolescence is particularly challenging because GAD symptoms may be dismissed as personality traits rather than emerging psychopathology, especially in families where parental anxiety has normalised such presentations. Reference Bandelow and Michaelis4
-
(d) Phobias: opportunistic screening in healthcare contexts (needle phobia, dental phobia) can enable early-exposure interventions. Reference Bandelow and Michaelis4
-
(e) Agoraphobia: telehealth- and home-based services are essential for patients unable to access clinics. Reference Bandelow and Michaelis4
Research gaps
Despite advances, major gaps remain. Prospective, population-based studies are scarce and most data derive from treatment-seeking samples. Operational definitions of DUI are inconsistent across anxiety disorders, complicating cross-study comparisons. Disorder-specific priorities include the following:
-
(a) SAD: longitudinal studies on transition from personality traits (e.g. shyness) to disorder;
-
(b) panic disorder: research on sequencing pharmacological and psychological treatments;
-
(c) GAD: improved methods for onset identification;
-
(d) phobias: predictors of progression from mild fears to disabling phobia;
-
(e) agoraphobia: prevention of progression from panic disorder remains unexplored.
Perhaps most importantly, intervention trials targeting DUI reduction are almost entirely absent. Although observational data support the benefits of early treatment, randomised studies testing system-level strategies are urgently required. Reference Cipriani and Saunders8
Proposed framework for implementation
Based on current evidence, DUI reduction in anxiety disorders should be recognised as a public health priority requiring action at multiple levels:
-
(a) individual level: systematic DUI assessment in patients with anxiety disorders;
-
(b) provider level: structured screening in primary care, schools and workplaces; prescriber education to optimise treatment pathways;
-
(c) system level: integrated service models ensuring rapid access, tailored to disorder-specific barriers.
Priority stratification may guide policy: highest priority: SAD (given major delays); high priority: panic disorder (given prescribing biases); moderate priority: GAD and agoraphobia; targeted priority: phobias.
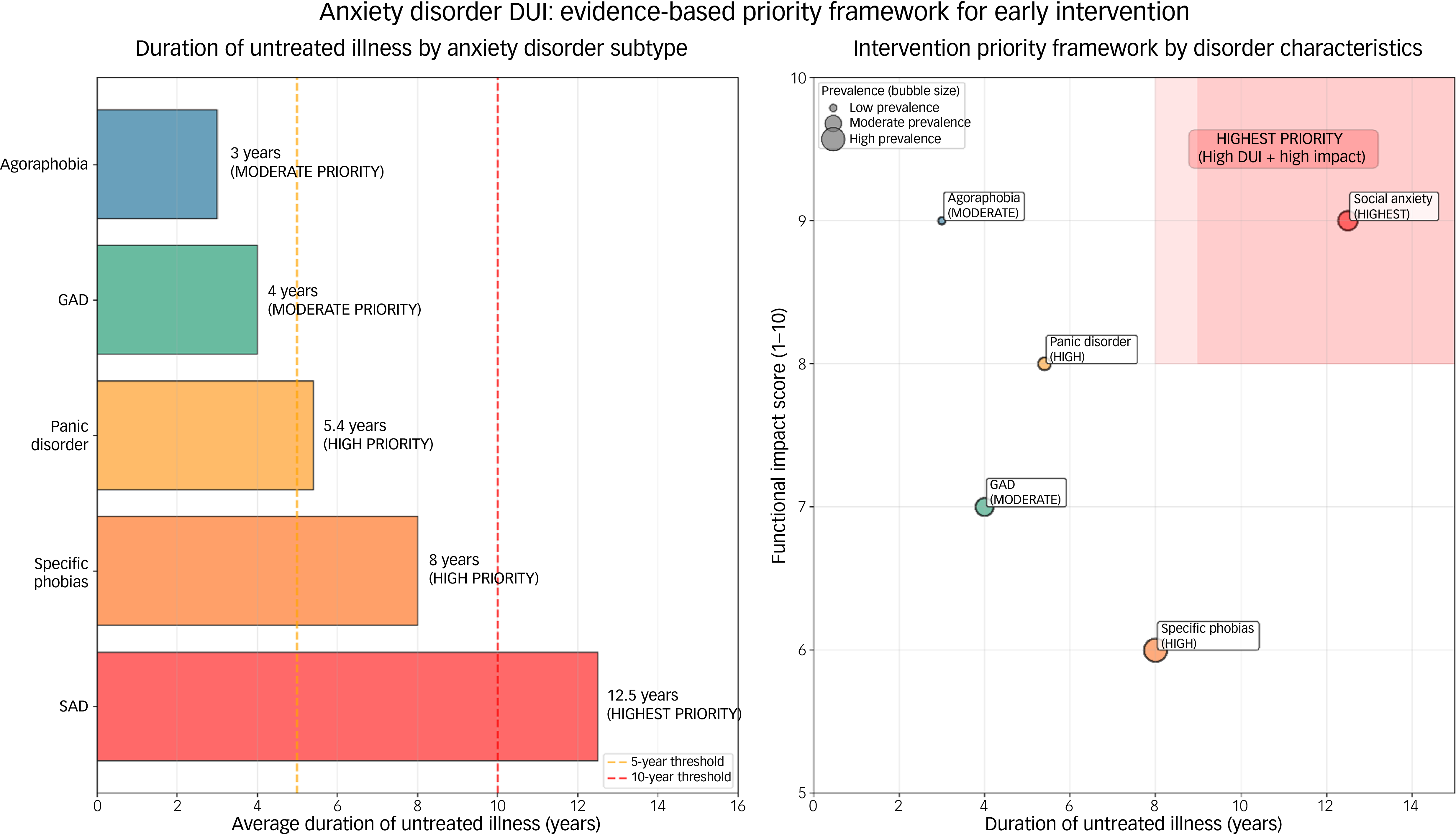
Figure 1 illustrates the prioritisation framework described in this section.
Evidence-based priority framework for reducing duration of untreated illness (DUI) in anxiety disorders. Left panel: average duration of untreated illness across anxiety disorder subtypes. Social anxiety disorder (SAD) shows the longest delays (approximately 10–15 years), followed by specific phobias, panic disorder, generalised anxiety disorder (GAD) and agoraphobia. Dashed vertical lines indicate reference thresholds at 5 and 10 years. Right panel: intervention priority framework based on disorder characteristics. The x-axis represents duration of untreated illness and the y-axis represents functional impact. Bubble size reflects population prevalence. SAD emerges as the highest priority target for early intervention due to the combination of long untreated duration and high functional impairment.

Adoption of DUI as a formal quality indicator would require consensus on operational definitions, acknowledgment of measurement challenges (including recall bias and variability across healthcare systems) and pragmatic implementation strategies tailored to local contexts. Healthcare systems should consider adopting DUI metrics as quality indicators alongside remission and relapse rates. This would create accountability for early recognition and timely intervention.
Duration of untreated illness in anxiety disorders is both a marker of systemic failure and a modifiable determinant of outcome. Delays of 5–15 years worsen prognosis, increase comorbidity and generate substantial social and economic burden for both patients and their families. In line with early-intervention paradigms in psychosis, psychiatry must now adopt DUI reduction in anxiety disorders as a core objective through systematic assessment, disorder-specific early interventions and integrated service models. The marked variability of DUI – from about 5.4 years in panic disorder to over a decade in SAD – demands targeted strategies to prevent chronicity and relapse. DUI reduction should be treated as a clinical and public health imperative with routine assessment, accessible care pathways and early-detection models to limit long-term disability.Reference Altamura and Camuri1 DUI should be incorporated into international quality indicators for mental health services (e.g. World Health Organization, Organisation for Economic Co-operation and Development).Reference Dell’Osso and Oldani7 Future research should refine and test tailored interventions, with health systems embedding DUI monitoring and reduction into everyday practice. As psychiatry moves towards precision medicine, addressing DUI is both feasible and potentially transformative, with major implications for the nearly 300 million individuals living with anxiety disorders. Making DUI visible, measurable and actionable is a necessary step towards a more effective, preventive and ethically responsible model of care.
Author contributions
M.O.: writing – review and editing, writing – original draft, conceptualisation. M.M.: writing – review and editing, writing – original draft. B.D.: writing – review and editing, writing – original draft, supervision, conceptualisation.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors declare the following financial interests/personal relationships that may be considered as potential competing interests. In the past 3 years, B.D. has received lecture honoraria and grants from Angelini, Lundbeck, Janssen, Pfizer, Otzuka, Neuraxpharm and Livanova. M.O. and M.M. declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.

eLetters
No eLetters have been published for this article.