


Depression, metabolic syndrome and COVID-19
Depression is a complex and debilitating mental health disorder that ranks among the leading causes of disability worldwide. Reference Piao, Huang, Han, Li, Xu and Liu1 Characterised by persistent low mood, loss of interest in activities, cognitive dysfunction and physical symptoms, depression significantly impairs quality of life and increases the risk of morbidity and mortality. Reference Moradi, Albatineh, Mahmoodi and Gheshlagh2 Beyond its psychological burden, depression is closely linked to physical health conditions, placing a significant strain on individuals and healthcare systems. Large-scale epidemiological studies have demonstrated an elevated prevalence of depression among individuals with metabolic conditions and a history of infectious diseases, further emphasising the importance of understanding these interconnections. Reference Al-Khatib, Akhtar, Kanawati, Mucheke, Mahfouz and Al-Nufoury3
One such condition is metabolic syndrome, a cluster of risk factors including central obesity, hypertension, dyslipidaemia and hyperglycaemia, which collectively increase the risk of cardiovascular disease and diabetes. Reference das Virgens Silva, Coutinho-Lima, Brandao, Dos Santos, Dias and Correa4 There is growing evidence of a bidirectional relationship between depression and metabolic syndrome, with shared underlying mechanisms such as chronic inflammation, oxidative stress and hypothalamic-pituitary-adrenal (HPA) axis dysregulation. Reference Moradi, Albatineh, Mahmoodi and Gheshlagh2,Reference Prakash, Sourabh, Rudra, Kumar and Abraham5 Individuals with metabolic syndrome are at a higher risk of developing depression, whereas depression itself contributes to metabolic dysfunction through reduced physical activity, poor dietary habits and increased systemic inflammation. Reference Berk, Köhler-Forsberg, Turner, Penninx, Wrobel and Firth6
The COVID-19 pandemic has further compounded the mental health crisis, not only by increasing psychological distress, but also by exacerbating the interplay between depression and metabolic syndrome. Reference Pećin and Reiner7 SARS-CoV-2 infection has been linked to depressive symptoms through biological mechanisms such as systemic inflammation, cytokine elevation, serotonin depletion and reductions in brain-derived neurotrophic factor, as well as dysregulation of the HPA axis and neurotransmitter imbalances. Reference Lorkiewicz and Waszkiewicz8–Reference Sherif, Deverapalli, Challa, Martirosyan, Whitesell and Pizuorno10 Additionally, individuals with metabolic syndrome and a history of COVID-19 may face an amplified risk for depression because of overlapping inflammatory pathways, heightened immune activation and neurobiological changes associated with both conditions. Reference das Virgens Silva, Coutinho-Lima, Brandao, Dos Santos, Dias and Correa4,Reference Shyam, Gómez-Martínez, Paz-Graniel, Gaforio, Martínez-González and Corella11 The psychosocial stressors of COVID-19, including social isolation, fear of contagion and stigma, further intensify mental health challenges, creating a compounded burden for those with pre-existing metabolic and psychiatric conditions. Reference Penninx, Benros, Klein and Vinkers12
Study rationale and aims
Despite increasing recognition of these interconnections, research has largely examined COVID-19, metabolic syndrome and depression as separate contributors to mental health outcomes, with limited exploration of their combined effects. Reference Berk, Köhler-Forsberg, Turner, Penninx, Wrobel and Firth6 This study aims to investigate the associations between depressive symptoms, metabolic syndrome and COVID-19 seropositivity in a representative population. By examining the interplay between these factors, we seek to provide insights into the mechanisms underlying their relationships and inform strategies for addressing the compounded burden of depression and chronic health conditions in the context of the COVID-19 pandemic.
Method
Study population
This cross-sectional study uses data from the 2021 and 2022 Encuesta Nacional de Salud y Nutrición (ENSANUT), a continuous health and nutrition survey conducted by the Instituto Nacional de Salud Pública (INSP) in Mexico. Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arredondo, Colchero and Gaona-Pineda13,Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arrendondo, Colchero and Gaona-Pineda14 ENSANUT provides representative data on Mexico’s non-institutionalised civilian population, covering urban and rural areas through stratified, multi-stage probabilistic sampling. Reference Contreras-Manzano, Mejía-Rodríguez, Villalpando, Rebollar and Flores-Aldana15 ENSANUT 2021 collected 12 060 complete household interviews, whereas ENSANUT 2022 gathered 10 160 interviews, including biological samples and anthropometric measurements. The survey combines face-to-face interviews, physical health assessments and laboratory analyses. Data are stratified by age and sociodemographic variables, covering chronic disease prevalence, SARS-CoV-2 seroprevalence, nutrition, mental health and COVID-19’s impact. This study includes adults aged ≥20 years with complete data on survey weights, the Center for Epidemiological Studies Depression Scale (CESD-7) questionnaire, metabolic syndrome variables and COVID-19 laboratory results.
ENSANUT ethical considerations
The protocols for ENSANUT were approved by the Ethics, Research, and Biosafety Committees of the INSP Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arredondo, Colchero and Gaona-Pineda13,Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arrendondo, Colchero and Gaona-Pineda14 Written informed consent was obtained from all participants, and assent was provided for minors as appropriate. All biological samples were handled under strict conditions, maintaining a temperature of <4°C during transport to certified laboratories for analysis. Reference Contreras-Manzano, Mejía-Rodríguez, Villalpando, Rebollar and Flores-Aldana15
ENSANUT data collection and methodology
The ENSANUT methodology involves a multi-stage process, starting with probabilistic, stratified sampling, where geographic areas serve as primary sampling units, localities and households as secondary units, and individual participants as tertiary units, utilising updated procedures from the 2020 national census. Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arredondo, Colchero and Gaona-Pineda13,Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arrendondo, Colchero and Gaona-Pineda14 Field teams conducted structured interviews to gather data on health, nutrition and social determinants, complemented by anthropometric and biological measurements, including blood samples, adhering to standardised protocols. ENSANUT 2021 focused on estimating SARS-CoV-2 seroprevalence, chronic disease prevalence (e.g. diabetes, hypertension) and the social impacts of the COVID-19 pandemic, whereas ENSANUT 2022 expanded themes to include micronutrient levels, physical activity, dietary intake and SARS-CoV-2 seroprevalence alongside chronic disease assessments. The surveys ensured regional and state-level representativeness, with oversampling in certain states like Nuevo León and Guanajuato for more granular insights. Fieldwork was systematically organised into health, nutrition and cartography components, with specialised teams conducting mapping, health surveys, and biological and anthropometric data collection.
Exposure variables
Metabolic syndrome was defined with the Adult Treatment Panel III criteria, requiring the presence of at least three of the following five factors: (a) elevated waist circumference (≥90 cm for males, ≥80 cm for females), (b) elevated triglycerides (≥150 mg/dL), (c) reduced high-density lipoprotein (HDL) cholesterol (<40 mg/dL for males, <50 mg/dL for females), (d) elevated blood pressure (systolic ≥130 mmHg and/or diastolic ≥85 mmHg) and (e) elevated fasting plasma glucose (≥100 mg/dL). Reference González-Rocha, Ortiz-Rodríguez, Salazar-Torres, Muñoz-Aguirre, Armenta-Girado and Campos-Nonato16
Venous blood samples
Venous blood was collected by trained personnel and preserved in cryotubes. Triglycerides, HDL cholesterol and fasting plasma glucose levels were analysed in certified laboratories, using enzymatic and colorimetric methods to ensure precision and standardisation. Blood samples were centrifuged at 3000 g for 20 min on-site and stored at controlled temperatures during transport. Reference González-Rocha, Ortiz-Rodríguez, Salazar-Torres, Muñoz-Aguirre, Armenta-Girado and Campos-Nonato16 Venous blood samples used for metabolic biomarkers were collected under fasting conditions according to the ENSANUT protocol; Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arredondo, Colchero and Gaona-Pineda13,Reference Romero-Martínez, Barrientos-Gutiérrez, Cuevas-Nasu, Bautista-Arrendondo, Colchero and Gaona-Pineda14 however, individual-level fasting duration was not available in the data-set.
Anthropometric measurements
Body weight was measured using a calibrated electronic scale, and participants were wearing minimal clothing and were barefoot. Height was measured using a stadiometer, and waist circumference was measured at the level of the iliac crest after a normal exhalation, ensuring accuracy to the nearest 0.1 cm. Reference González-Rocha, Ortiz-Rodríguez, Salazar-Torres, Muñoz-Aguirre, Armenta-Girado and Campos-Nonato16
Blood pressure readings
Blood pressure was measured twice using an automated device (Omron HEM-907 XL) after the participant rested for at least 5 min. A mean value was calculated for systolic and diastolic pressure from the two readings, ensuring reliability. Reference González-Rocha, Ortiz-Rodríguez, Salazar-Torres, Muñoz-Aguirre, Armenta-Girado and Campos-Nonato16
COVID-19 exposure was determined using SARS-CoV-2 seroprevalence data from ENSANUT 2021 and 2022. Seropositivity was assessed via the Roche Elecsys assay for IgG antibodies against the nucleocapsid protein, with samples considered positive if values were ≥1.0 U/mL.
Outcome variables
Depressive symptoms were assessed with the CESD-7, a validated instrument widely used in population studies, including ENSANUT. It measures the frequency of depressive symptoms over the past week, with response options from 0 (‘rarely or none of the time’) to 3 (‘most or all of the time’), yielding a total score of 0–21, where higher scores indicate greater symptom severity. Clinically meaningful depressive symptoms were defined as a CESD-7 score of ≥5 for adults aged ≥60 years and ≥9 for those aged <60 years. Reference Salinas-Rodríguez, Manrique-Espinoza, Acosta-Castillo, Téllez-Rojo, Franco-Núñez and Gutiérrez-Robledo17,Reference Salinas-Rodríguez, Manrique-Espinoza, Acosta-Castillo, Franco-Núñez, Rosas-Carrasco and Gutiérrez-Robledo18 As a screening instrument, the CESD-7 does not provide a clinical diagnosis of depressive disorders; therefore, the outcome reflects depressive symptom burden in the general population rather than specific psychiatric conditions such as major depressive disorder or bipolar disorder.
To further characterise symptom profiles, depressive symptoms were analysed across three domains: positive affect, negative affect and somatic symptoms. Positive affect included reverse-scored items on happiness and life enjoyment. Negative affect assessed sadness and loneliness, whereas somatic symptoms encompassed sleep disturbances, fatigue and psychomotor slowing. These domains were examined as continuous variables to examine their associations with COVID-19 exposure and metabolic syndrome, facilitating a more granular understanding of their interplay with physical health.
Covariates
Covariates included age (continuous), gender (female or male), body mass index (underweight <18.5 kg/m2, normal weight 18.5–24.9 kg/m2, overweight 25–29.9 kg/m2, obese ≥30 kg/m2), Reference Estrella and Gomez-de-Regil19 education level (high school or below, higher than high school), marital status (common-law/married, divorced, separated, single, widowed), smoking status (yes/no to ‘Currently, do you smoke tobacco: every day, some days, do not currently smoke, or no response?’), drinking status (yes/no to ‘In the past 12 months, how often have you had at least one drink of wine, beer, whiskey, or any other alcoholic beverage: daily, weekly, monthly, yearly, not in the past 12 months, never, or no response?’), Reference Zhou, Ma and Wang20 COVID-19 vaccine status (yes/no to ‘Have you been vaccinated for COVID-19?’), Reference Bello-Chavolla, Fermín-Martínez, Ramírez-García, Vargas-Vázquez, Fernández-Chirino and Basile-Alvarez21 and history of chronic health conditions, including heart stroke, angina and heart failure. Reference Guo, Weng, Chu, Xu, Wang and He22 The presence of these conditions was treated as a binary variable, with ‘yes’ indicating presence and ‘no’ indicating absence.
Statistical analysis
Statistical analyses were conducted using R version 4.4.0 for Windows (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/), incorporating the ‘survey’ package to account for survey weights with the svydesign function, which included the primary sampling unit, urban/rural stratum and weight. The same survey design object was used for all descriptive and regression analyses. Variance estimation was based on the survey package’s default linearised design-based estimator under the specified complex survey design, and standard errors and 95% confidence intervals were obtained accordingly; no additional external robust standard error correction was applied. In the table summarising demographic characteristics, unweighted frequencies were generated by using the CreateTableOne function, and weighted percentages were calculated with the svyCreateTableOne function. Categorical variables were presented as unweighted frequencies and weighted percentages, and continuous variables were reported as weighted means with standard deviations. Group differences in categorical variables by depressive symptom status were assessed with chi-squared tests, whereas t-tests were used for continuous variables (p ≤ 0.05).
Logistic regression models were employed to investigate the associations between COVID-19, metabolic syndrome and depressive symptoms (yes/no), using survey-weighted logistic regression with svyglm and a quasibinomial (link = ‘logit’) family. Linear regression models examined the relationships between COVID-19, metabolic syndrome, CESD-7 scores and symptom clusters by using survey-weighted linear regression with the Gaussian family. To improve clinical interpretability of the binary depressive symptoms outcome, absolute risk differences (ARDs) were also reported. Interaction models were specified by including a product term between COVID-19 laboratory results and metabolic syndrome within the same survey-weighted regression framework.
To account for multiple comparisons among the secondary symptom cluster outcomes, false discovery rate (FDR)-adjusted p-values were calculated separately within each model across the three CESD-7 clusters. Additional survey-weighted linear regression models were conducted to examine the associations between the five individual metabolic syndrome components and the negative affect and somatic symptom clusters. For these analyses, FDR adjustment was applied separately within each model across the five individual metabolic syndrome components, and the fully adjusted estimates were presented in forest plots. As a sensitivity analysis addressing potential misclassification owing to waning anti-nucleocapsid antibodies, the COVID-19 main-effect and interaction analyses were repeated among 2022 respondents only, using the same survey design specification.
Multicollinearity was assessed with variance inflation factors, with all values below four indicating no substantial multicollinearity concerns. Missingness was <2.5% for all covariates. To minimise bias, no imputation was performed for missing survey data; instead, listwise deletion was applied, excluding cases with missing values from the analysis.
Results
Descriptive statistics
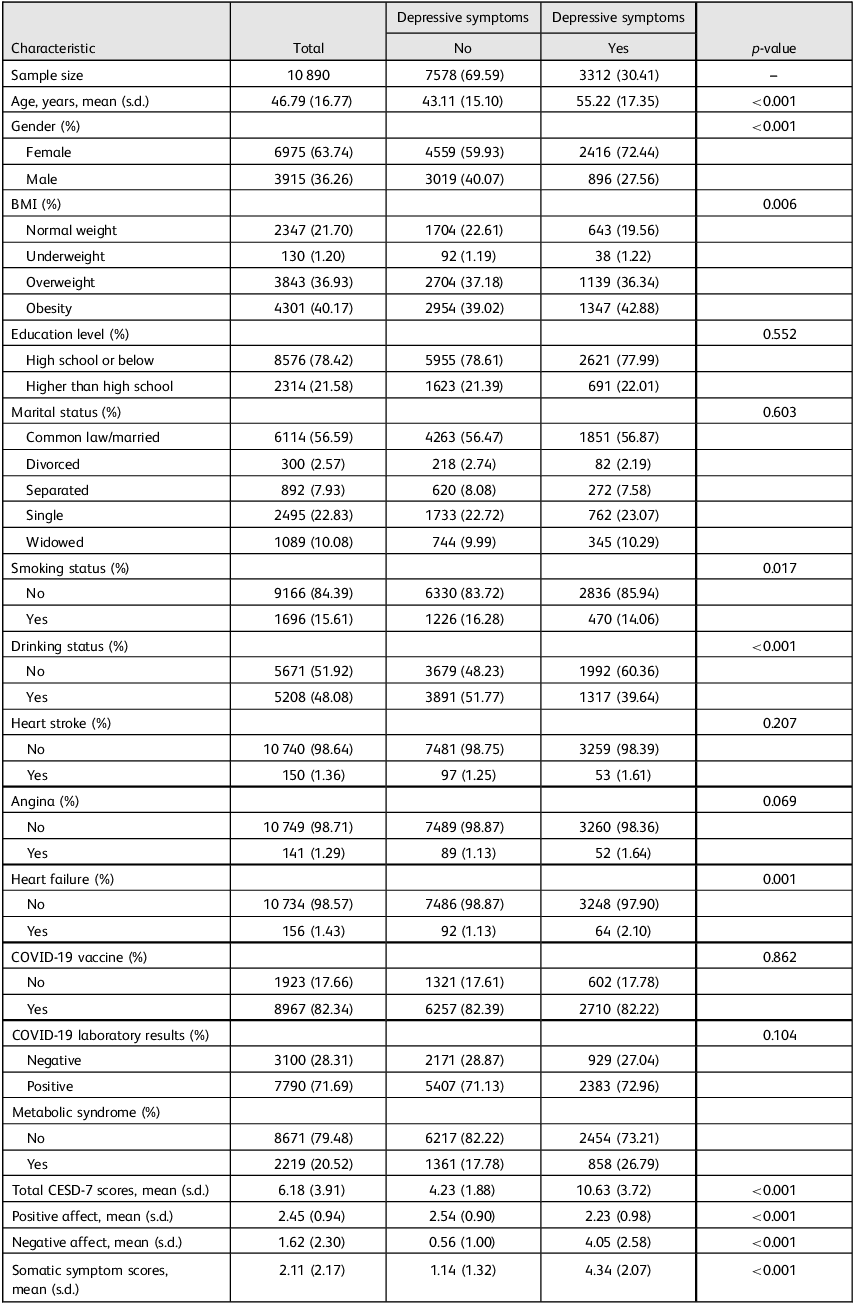
The study included 10 890 participants, of whom 6975 (63.74%) were female. Depressive symptoms were reported by 3312 participants (30.41%), 2219 (20.52%) participants met the criteria for metabolic syndrome and 7790 (71.69%) participants tested positive for COVID-19 (Table 1). Supplementary Fig. 1 presents the participant inclusion flowchart. Table 1 provides a detailed summary of the variables included in the main analysis, stratified by the presence of depressive symptoms.
Demographic characteristics, stratified by presence of depressive symptoms (n = 10 890)

Continuous characteristics reported as weighted mean and standard deviation. Categorical characteristics reported as unweighted frequency and weighted per cent. The first level of categorical variables is the reference level. p-values <0.05 denote significant differences between no depressive symptoms versus having depressive symptoms, and are reported as weighted p-values. BMI, body mass index; CESD-7, seven-item Center for Epidemiologic Studies Depression Scale.
COVID-19 laboratory results and depressive symptoms, including symptom clusters
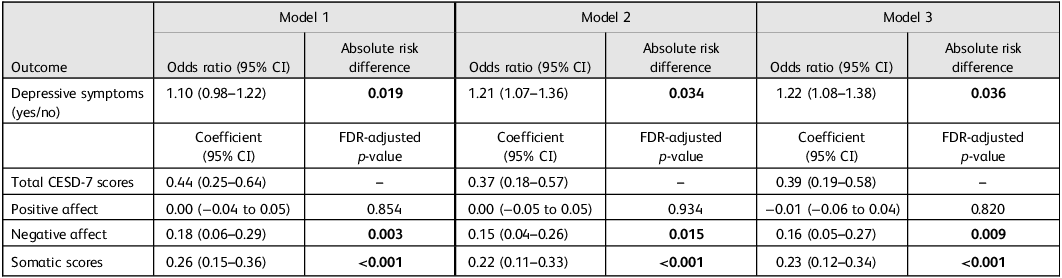
Table 2 summarises the associations between COVID-19 laboratory results and depressive symptoms, total CESD-7 scores and symptom clusters across unadjusted and adjusted models. In the association between COVID-19 laboratory results and depressive symptoms (yes/no), the odds of depressive symptoms were not statistically significant in the unadjusted model (model 1; odds ratio 1.10, 95% CI 0.98–1.22, ARD = 0.019). However, after adjusting for covariates (model 2), participants who tested positive for COVID-19 had 21% higher odds of reporting depressive symptoms compared with those who tested negative for COVID-19 (odds ratio 1.21, 95% CI 1.07–1.36, ARD = 0·034). This association remained significant in the fully adjusted model (model 3; odds ratio 1.22, 95% CI 1.08–1.38), with COVID-19 positivity associated with an absolute 3.6 percentage point higher prevalence of depressive symptoms (ARD = 0.036).
Main effects models for association between COVID-19 laboratory results and total CESD-7 scores, depressive symptoms (yes/no) and symptom clusters

Model 1: unadjusted model with only the exposure variable as the independent variable. Model 2: adjusted for age, gender, body mass index, education level and marital status. Model 3: adjusted for all covariates in model 2, plus COVID-19 vaccine status, smoking status, drinking status, history of heart stroke, angina, heart failure and metabolic syndrome. The exposure variable for all models is COVID-19-positive laboratory results (versus negative). For the CESD-7 cluster outcomes, FDR adjustment was applied separately within each model across the three cluster outcomes. Bold text denotes statistical significance, with p < 0.05. CESD-7, seven-item Center for Epidemiologic Studies Depression Scale; FDR, false discovery rate.
COVID-19 positivity was also associated with higher total CESD-7 scores across all models, with coefficients ranging from 0.37 to 0.44. Significant associations were observed among symptom clusters for negative affect and somatic symptom scores, whereas no significant relationship was found for positive affect scores. After FDR correction, the associations for negative affect and somatic symptom scores remained significant across all models, whereas positive affect remained non-significant.
Metabolic syndrome, depressive symptoms and symptom clusters
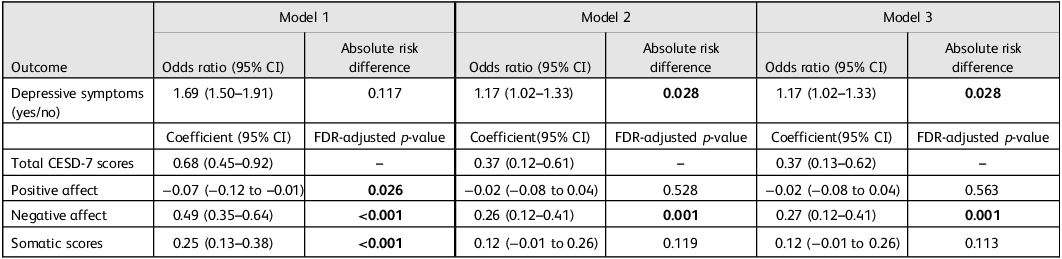
Table 3 summarises the associations between metabolic syndrome and depressive symptoms, total CESD-7 scores and symptom clusters. Metabolic syndrome was significantly associated with higher odds of depressive symptoms in the unadjusted model (model 1; odds ratio 1.69, 95% CI 1.50–1.91, ARD = 0.117), with the association remaining significant after full adjustment (model 3; odds ratio 1.17, 95% CI 1.02–1.33, ARD = 0.028), corresponding to an absolute 2.8 percentage point higher prevalence of depressive symptoms. Participants with metabolic syndrome also had significantly higher total CESD-7 scores in all models, with coefficients of 0.68 (95% CI 0.45–0.92) in model 1 and 0.37 (95% CI 0.13–0.62) in model 3. Significant positive associations were observed for negative affect among symptom clusters in all models. Positive affect and somatic scores were only significantly associated with metabolic syndrome in the unadjusted model (model 1; positive affect: coefficient −0.07, 95% CI −0.12 to −0.01, FDR-adjusted p = 0.026; somatic: coefficient 0.25, 95% CI 0.13–0.38, FDR-adjusted p < 0·001), but lost significance after adjustment.
Main effects models for the association between metabolic syndrome and total CESD-7 scores, depressive symptoms (yes/no) and symptom clusters

Model 1: unadjusted model with only the exposure variable as the independent variable. Model 2: adjusted for age, gender, body mass index, education level and marital status. Model 3: adjusted for all covariates in model 2, plus COVID-19 vaccine status, smoking status, drinking status, history of heart stroke, angina, heart failure and COVID-19 laboratory results. The exposure variable for all models is metabolic syndrome – yes (versus no). For the CESD-7 cluster outcomes, FDR adjustment was applied separately within each model across the three cluster outcomes. Bold text denotes statistical significance, with p < 0.05. CESD-7, seven-item Center for Epidemiologic Studies Depression Scale; FDR, false discovery rate.
In additional analyses of the five individual metabolic syndrome components, high blood pressure and high glucose remained positively associated with negative affect in the fully adjusted model, whereas no individual metabolic syndrome component remained significantly associated with somatic scores after full adjustment and FDR correction (Supplementary Tables 1 and 2; Supplementary Figs 2 and 3).
Interaction effects of COVID-19 laboratory results and metabolic syndrome on depressive symptoms and clusters
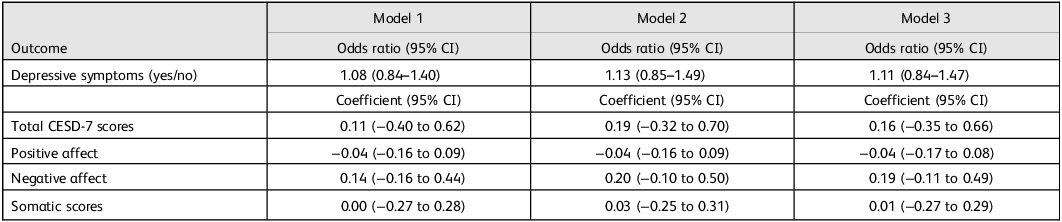
Table 4 presents the interaction effects of metabolic syndrome and COVID-19 laboratory results on depressive symptoms, total CESD-7 scores and symptom clusters. No statistically significant interaction effects were observed for depressive symptoms, total CESD-7 scores or any of the symptom clusters in any model.
Interaction models of metabolic syndrome and COVID-19 laboratory results on CESD-7 scores, depressive symptoms and symptom clusters

Model 1: unadjusted model with only the exposure variable as the independent variable. Model 2: adjusted for age, gender, body mass index, education level and marital status. Model 3: adjusted for all covariates in model 2, plus COVID-19 vaccine status, smoking status, drinking status, history of heart stroke, angina and heart failure. CESD-7, seven-item Center for Epidemiologic Studies Depression Scale.
Sensitivity analysis restricted to 2022 respondents
To address potential exposure misclassification related to waning anti-nucleocapsid antibodies, we repeated the COVID-19 main-effect and interaction analyses in respondents surveyed in 2022 only (n = 4892; Supplementary Tables 3 and 4). In this restricted analysis, the associations between COVID-19 seropositivity and depressive symptoms, total CESD-7 scores and symptom cluster scores were attenuated and no longer statistically significant in adjusted models. The interaction between COVID-19 seropositivity and metabolic syndrome also remained non-significant across all outcomes.
Discussion
In this study, we examined the relationship between depressive symptoms, symptom severity and symptom clusters with COVID-19 and metabolic syndrome, as well as the potential interaction between these factors. Participants who tested positive for COVID-19 had significantly higher odds of depressive symptoms, with the strongest associations observed for somatic and negative affect symptom clusters, as measured by the CESD-7. Similarly, metabolic syndrome was associated with increased odds of depressive symptoms and higher depressive symptom severity, particularly for negative affect. In contrast, its impact on somatic and positive affect symptom clusters diminished after adjusting for covariates. Interestingly, the interaction between COVID-19 positivity and metabolic syndrome did not yield significant results, suggesting independent rather than synergistic effects on depressive symptoms. These findings highlight the complex interplay between physical health conditions, infectious diseases and mental health. Although statistically significant, the magnitude of these associations was modest, corresponding to small absolute increases in the prevalence of depressive symptoms. Given the distinct symptom clusters, understanding how specific depressive dimensions interact with metabolic dysfunction is essential for refining targeted interventions.
The association between COVID-19 and depressive symptoms is supported by previous research demonstrating the psychological and physiological consequences of SARS-CoV-2 infection. Systematic reviews and meta-analyses have reported high prevalence rates of depression (21–45%) in COVID-19 survivors, regardless of disease severity. Reference Mazza, Palladini, Poletti and Benedetti9,Reference Deng, Zhou, Hou, Silver, Wong and Chang23 The increased risk of depressive symptoms among COVID-19-positive individuals likely results from a combination of direct viral effects on the central nervous system, systemic inflammation and psychological stressors related to illness and social isolation. Reference Mazza, Palladini, Poletti and Benedetti9,Reference Shyam, Gómez-Martínez, Paz-Graniel, Gaforio, Martínez-González and Corella11,Reference Piumatti, Amati, Richard, Baysson, Purgato and Guessous24 Moreover, COVID-19 positivity was associated with higher CES-D-7 scores and specific symptom clusters, particularly negative affect and somatic symptoms. Longitudinal studies have found that depressive symptoms can persist post-infection, with older adults exhibiting sustained increases in symptoms up to 12 weeks post-infection. Reference Penninx, Benros, Klein and Vinkers12,Reference Renaud-Charest, Lui, Eskander, Ceban, Ho and Di Vincenzo25 These outcomes likely stem from neuroinflammatory pathways and the exacerbation of pre-existing mental health vulnerabilities. Reference Mazza, Palladini, Poletti and Benedetti9,Reference Shanbehzadeh, Tavahomi, Zanjari, Ebrahimzadeh and Ashton26,Reference Kachaner, Lemogne, Dave, Ranque, de Broucker and Meppiel27 Additionally, post-COVID-19 fatigue, myalgia and other physical complaints appear closely intertwined with depressive states, contributing to a cyclical impact on patient well-being. Reference Penninx, Benros, Klein and Vinkers12,Reference Shanbehzadeh, Tavahomi, Zanjari, Ebrahimzadeh and Ashton26,Reference Ballering, van Zon, Olde Hartman and Rosmalen28 The presence of these symptoms underscores the need for integrated care approaches addressing both the biological and psychological sequelae of COVID-19.
Findings related to depressive symptom clusters and metabolic syndrome align with evidence that specific dimensions of depression differentially associate with metabolic dysfunction, with somatic-affective symptoms showing stronger links than cognitive-affective symptoms. Reference Wiltink, Michal, Jünger, Münzel, Wild and Lackner29 Adriaanse et al reported that negative well-being, including fatigue and emotional distress, is associated with metabolic dysfunctions like hyperglycaemia in individuals with type 2 diabetes. Reference Adriaanse, Dekker, Spijkerman, Twisk, Nijpels and van der Ploeg30 These patterns highlight the role of negative affect in amplifying metabolic risk factors such as obesity and hypertension, particularly in individuals with co-occurring metabolic and psychological conditions. Reference Al-Khatib, Akhtar, Kanawati, Mucheke, Mahfouz and Al-Nufoury3 The bidirectional relationship between metabolic syndrome and depressive symptoms is mediated by intertwined biological and behavioural mechanisms. Chronic low-grade inflammation, a hallmark of metabolic syndrome, contributes to depression, with elevated inflammatory markers (e.g. C-reactive protein, pro-inflammatory cytokines) linked to increased negative affect and depressive symptom severity. Reference Moradi, Albatineh, Mahmoodi and Gheshlagh2,Reference Al-Khatib, Akhtar, Kanawati, Mucheke, Mahfouz and Al-Nufoury3 Metabolic dysregulation may also disrupt HPA axis activity, worsening mood disturbances. Additionally, behavioural factors like reduced physical activity, poor diet and sleep disturbances reinforce this relationship. Reference Wiltink, Michal, Jünger, Münzel, Wild and Lackner29 By focusing on depressive symptom dimensions, this study provides a nuanced perspective on the interplay between specific depressive symptoms and metabolic syndrome. Unlike categorical depression diagnoses, which may obscure symptom-specific associations, these findings emphasise negative affect as a primary dimension linking metabolic and mental health. This aligns with evidence that negative affect, characterised by sadness, guilt and irritability, significantly contributes to poor health outcomes and increased mortality risk in individuals with metabolic syndrome. Reference Luppino, Van Reedt Dortland, Wardenaar, Bouvy, Giltay and Zitman31
The lack of significant interaction effects between COVID-19 and metabolic syndrome on depressive symptoms, symptom severity and symptom clusters suggests that their mental health impacts are largely additive rather than synergistic. This is consistent with prior research showing that both conditions independently contribute to depressive symptoms through distinct yet overlapping mechanisms. COVID-19’s psychological effects are largely driven by systemic inflammation, neuroinflammatory processes and social stressors such as isolation and fear of contagion. Reference Mazza, Palladini, Poletti and Benedetti9,Reference Shanbehzadeh, Tavahomi, Zanjari, Ebrahimzadeh and Ashton26 In contrast, metabolic syndrome is associated with chronic low-grade inflammation, insulin resistance and HPA axis dysregulation, all of which have been implicated in the pathophysiology of depression. Reference Adriaanse, Dekker, Spijkerman, Twisk, Nijpels and van der Ploeg30 Although these shared pathways contribute to depressive symptoms, their independent effects may reflect the multifactorial nature of mental health disturbances, with no single pathway sufficiently dominant to create an interaction effect. This aligns with evidence that metabolic syndrome components, such as obesity and hypertension, can exacerbate physical and emotional distress, but do not necessarily intensify the psychological impacts of COVID-19 in a measurable way. Reference Ballering, van Zon, Olde Hartman and Rosmalen28 Furthermore, the absence of interaction effects underscores the importance of addressing each condition separately in clinical and public health interventions. Routine depression screening for individuals with metabolic syndrome and COVID-19 survivors remains essential, but these results suggest that distinct treatment strategies may be required for each group.
Future research should focus on longitudinal studies to clarify the causal links between COVID-19 seropositivity, metabolic syndrome and depressive symptoms, and to better disentangle the relative contributions of infectious and metabolic pathways. Using representative data-sets like ENSANUT offers a valuable opportunity to examine these relationships across diverse populations. Particular attention should be given to how specific depressive symptom clusters, such as somatic symptoms and negative affect, interact with metabolic syndrome components like obesity, dyslipidaemia, and hypertension. Integrating biological markers like inflammatory cytokines and HPA axis activity could further elucidate shared pathophysiological pathways. Research should also assess how metabolic syndrome influences long-term mental health outcomes post-COVID-19, considering factors such as infection severity, vaccination and healthcare access. Finally, intervention studies targeting metabolic dysfunction or inflammation are needed to determine whether modifying these pathways can reduce depressive symptom burden and inform more targeted therapeutic strategies, as emerging evidence from randomised controlled trials and meta-analyses suggests that anti-inflammatory interventions may reduce depressive symptoms and support inflammation as a potential therapeutic target. Reference Köhler, Benros, Nordentoft, Farkouh, Iyengar and Mors32–Reference Du, Dou, Wang, Wang, Yan and Fan34
This study has several limitations. First, its cross-sectional design precludes establishing causality between COVID-19, metabolic syndrome and depressive symptoms, highlighting the need for longitudinal research. Second, depressive symptoms were assessed using the CESD-7, a validated screening instrument that does not provide a clinical diagnosis; therefore, the findings reflect depressive symptom burden in the general population rather than specific psychiatric disorders such as major depressive disorder or bipolar disorder. Third, COVID-19 status was based on laboratory results; however, infection severity, symptom duration and post-acute sequelae were not considered, which may have influenced the observed associations. Additionally, COVID-19 serostatus was determined using anti-nucleocapsid antibodies, which are known to wane over time; thus, seronegativity may not reliably exclude prior infection. This may have resulted in exposure misclassification, likely biasing associations toward the null. Sensitivity analyses restricted to 2022 respondents showed attenuated, non-significant adjusted associations, with a directionally different point estimate for the binary depressive symptoms outcome. Fourth, treating metabolic syndrome as a binary variable limited the ability to assess the contribution of individual components, such as obesity or dyslipidaemia. In addition, fasting status was not recorded at the individual level in ENSANUT, and non-fasting samples could not be identified, which may have introduced measurement variability in metabolic biomarkers. The study’s generalisability may also be restricted, particularly for populations disproportionately affected by COVID-19 or metabolic syndrome. Finally, the lack of significant interaction effects between COVID-19 and metabolic syndrome may reflect limited statistical power to detect subtle synergistic effects. Future studies should employ longitudinal designs, comprehensive mental health assessments and more detailed characterisation of COVID-19 severity and metabolic syndrome components, while also accounting for social and behavioural factors, to better elucidate the complex interplay between physical and mental health.
In conclusion, this study provides valuable insights into the independent associations of COVID-19 and metabolic syndrome with depressive symptoms and their severity, highlighting the significant roles of negative affect and somatic symptoms as key contributors. Although no interaction effects were observed between COVID-19 and metabolic syndrome, the findings underscore the additive mental health burden posed by these conditions. These results emphasise the need for integrated care models that address both physical and psychological health, with tailored interventions targeting specific symptom dimensions. Future longitudinal research should examine the causal relationships between COVID-19, metabolic syndrome and depression, investigate potential moderating factors such as gender and socioeconomic status, and evaluate targeted treatments to mitigate the complex challenges faced by these overlapping populations. By addressing these gaps, healthcare systems can better support individuals grappling with the dual burden of physical and mental health challenges in the wake of the COVID-19 pandemic.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1192/bji.2026.10116
Data availability
Materials used in this study, including survey instruments and methodological guidelines, are publicly available through the ENSANUT website (https://ensanut.insp.mx/). The code and data-set analysed for hypotheses will be made available upon reasonable request to the corresponding author, V.B.
Author contributions
R.J.-A. contributed to study conceptualisation, study design, data curation, data interpretation and writing the original draft of the manuscript. Q.L. contributed to data curation, formal analysis, statistical modelling and reviewing and editing the manuscript. S.M. and H.A.-S. contributed to methodology development, validation and reviewing and editing the manuscript. W.L. contributed to study supervision, formal analysis and statistical guidance. N.M.-D. contributed to visualisation and reviewing and editing the manuscript. V.B. contributed to study conceptualisation, methodology oversight, supervision, data verification and reviewing and editing the manuscript. More than one author directly accessed and verified the underlying data. This study was an academic collaboration with no commercial partnership.
Funding
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
R.J.-A., Q.L., S.M., H.A.-S., W.L. and N.M.-D. have no disclosures. V.B. is supported by an Academic Scholar Award from the University of Toronto Department of Psychiatry and has received research funding from the Canadian Institutes of Health Research, Brain & Behavior Foundation, Ontario Ministry of Health Innovation Funds, Royal College of Physicians and Surgeons of Canada, Department of National Defence (Government of Canada), New Frontiers in Research Fund, Associated Medical Services Inc. Healthcare, American Foundation for Suicide Prevention, Roche Canada, Novartis and Eisai.



 Open access
Open access
eLetters
No eLetters have been published for this article.