


Introduction
The prolonged COVID-19 pandemic has resulted in high death rates and health-care system strain, highlighting the importance of early advance care planning (ACP) to guide care and protect patient choice, but COVID-19 created additional ACP barriers (Curtis et al. Reference Curtis, Kross and Stapleton2020). ACP is an iterative behavior change process that consists of individual and family preparation for decisional incapacity (Fried et al. Reference Fried, Bullock and Iannone2009; Sudore et al. Reference Sudore, Lum and You2017). Ideally ongoing discussions and documentation occur over time to update the plan of care with the patient’s most current preferences and values (Fried et al. Reference Fried, Bullock and Iannone2009; Sudore et al. Reference Sudore, Lum and You2017). Health-care system barriers to all forms of ACP during COVID-19 included insufficient palliative care coordination among health-care entities and community-based ACP barriers (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021). Recommendations to improve the ACP infrastructure consisted of simplified ACP documentation procedures, technological support to improve the health-care–community connection, and proactive, community-based ACP (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021). However, such improvements may be challenging without knowledge of how COVD-19 exacerbated existing disparities in the everyday lived experiences among low socioeconomic status (SES), older adults.
Unfortunately, prior to COVID-19, ACP rates among low SES, older adults were already low and little is known regarding the effects of COVID-19 on everyday experiences, which may challenge community-based efforts to improve ACP participation. Prior to COVID-19, only 1 in 3 adults in the United States had completed an Advance Directive (Yadav et al. Reference Yadav, Gabler and Cooney2017). Furthermore, compared with the highest, the lowest SES, older adults were approximately 33% less likely to participate in ACP (Barwise et al. Reference Barwise, Juhn and Wi2018; Inoue Reference Inoue2016).
These low rates of participation are disappointing considering the health challenges experienced by low SES, older adults. Low SES, older adults are susceptible to multi-comorbidities and advanced physiological aging, which partially stem from systemic factors such as inconsistent health-care access and the social determinants of health (e.g., housing, education) (House et al. Reference House, Lantz and Herd2005; Kawachi et al. Reference Kawachi, Daniels and Robinson2005). The COVID-19 pandemic has exacerbated pre-existing health system challenges and health disparities, and reduced capacity to deliver add-on services such as ACP, but it is unknown whether COVID-19 has had an immediate impact on low SES, community-dwelling, older adult’s ACP views outside of the hospital setting. We aimed to explore limited income, older adults’ perceptions of the effect of COVID-19 on living in the community and on ACP views. In this study, SES was operationalized as personal income below US$20,000/year.
Methods
Design
A qualitative descriptive design was selected to investigate the unique lived experiences of low-income, older adults recruited from Nashville, Tennessee (Sandelowski Reference Sandelowski2000). Qualitative procedures and reports were aligned with the standardized qualitative reporting guidelines (Consolidated Criteria for Reporting Qualitative Studies) (Booth et al. Reference Booth, Hannes, Harden, Moher, Altman, Schulz, Simera and Wager2014). All research protocols were approved by the Vanderbilt University Institutional Review Board (IRB#210905).
Theoretical framework
The Social Ecological Model informed the interview guide and interpretation of the results. This behavioral theory situates individual behavior within the multilevel context of overlapping social relationships and systems (Bronfenbrenner Reference Bronfenbrenner1974). This theory informed the interview guide and served as a descriptive framework for assessing a population susceptible to COVID-19, health-care, and planning inequities.
Research team
Six team members included 1 man and 5 women. The primary investigator (PI) (CK) was a PhD nursing research student who studied ACP inequities and had no interactions with the participants beyond study operations. The senior (CAM), second (JL), third (DS), and fourth (MD) authors were research faculty with extensive methodological, content, and publication expertise. The fifth author (ACR) was a doctoral-prepared nurse practitioner.
Sample and recruitment
We purposively and snowball sampled participants from 6 community-based locations (e.g., free food pantry, affordable housing, community resource center, etc.) If not in-person, then we screened potential participants by phone.
Participants were eligible for inclusion if they self-reported (1) an age of 50 years or older; (2) an individual, yearly income of less than US$20,000; and (3) independence without 24-hour caregiver support. Participants were excluded if they self-reported any severe hearing, visual, or language barriers to participation. Participants were also screened to meet stratification goals for sufficient representation for race (i.e., 70% of the sample self-identified as Black or African American), gender (i.e., 60% women), and age (i.e., 30% 50–59, 40% 60–69, 30% 70+ years). Finally, the PI purposively sampled participants to participate in an 1-hour, in-person qualitative interview to ensure rich and varied perspectives. Among 21 participants invited to complete a qualitative interview, 20 agreed. Interviews were scheduled according to each participant’s preference and were performed between November 11, 2021 and June 9, 2022. Each participant received a US$25 gift card incentive after qualitative interview completion.
Data collection
All participants completed in-person, electronic informed consent. The PI finalized the study procedures in quiet, private areas in participant homes or at recruitment sites per each participant’s preference to limit distractions and preserve privacy.
Demographic information included sociodemographic variables such as age. Semi-structured, individual, in-person interviews were audio-recorded using a pilot-tested, expert and theory-informed interview guide. Themes were based on responses to 2 interview guide questions: “The novel coronavirus (COVID-19) caused a lot of areas to shut down in March of 2020. Please tell me how COVID has affected your life in your community” and “How has COVID-19 affected your views about end of life and end-of-life planning?” Verbatim transcriptions were generated from the recordings by Rev.com.
Data analysis
Descriptive statistics for the qualitative sample were calculated with IBM SPSS Statistics (Version 28). Frequency distributions were used to describe nominal and ordinal categorical variables. Age as the only normally distributed, continuous variable was described with mean, standard deviation, and minimum and maximum values.
Using thematic analysis, 2 coders (CK and ACR) performed multiple, iterative cycles that consisted of transcript review (N = 20) to develop a hierarchical coding system (Maguire and Delahunt Reference Maguire and Delahunt2017; Nowell et al. Reference Nowell, Norris and White2017). This analytic method provided a flexible approach to identify patterns that emerged from the data, allowed for an improved understanding of the meaning of key themes, and helped to maintain a close relationship between the results and supporting data.
The coding system was inductively informed by the specific responses to the 2 COVID-19 interview questions. The coders initially coded transcripts with a recursive process for major categories, which were divided into subcategories to reflect further conceptual detail. The coding system consisted of 2 major categories that reflected the interview questions: (1) COVID’s impact on everyday life in the community and (2) COVID’s effect on end-of-life or planning for end-of-life. Each speaking term in the interview was analyzed as a quotation and each quote received a maximum of 5 codes. Major themes emerged inductively from review of prominent codes (i.e., most frequent) and less frequent codes, then were deductively informed by the Social Ecological theoretical framework.
The trained coders independently coded each transcript and then reconciled any differences in the codes together by reaching consensus. Coded transcripts were combined into a single file and then sorted by coding category. During this analytic stage, the PI reviewed quote clusters by each code category to interpret the similarities and differences among the results, which contributed to how the formation of higher-level themes and relationships between the themes were identified. All authors agreed on the final themes and conceptual framework. Data analysis was augmented using IBM SPSS Statistic (Version 28) and Microsoft Excel 2022.
Results
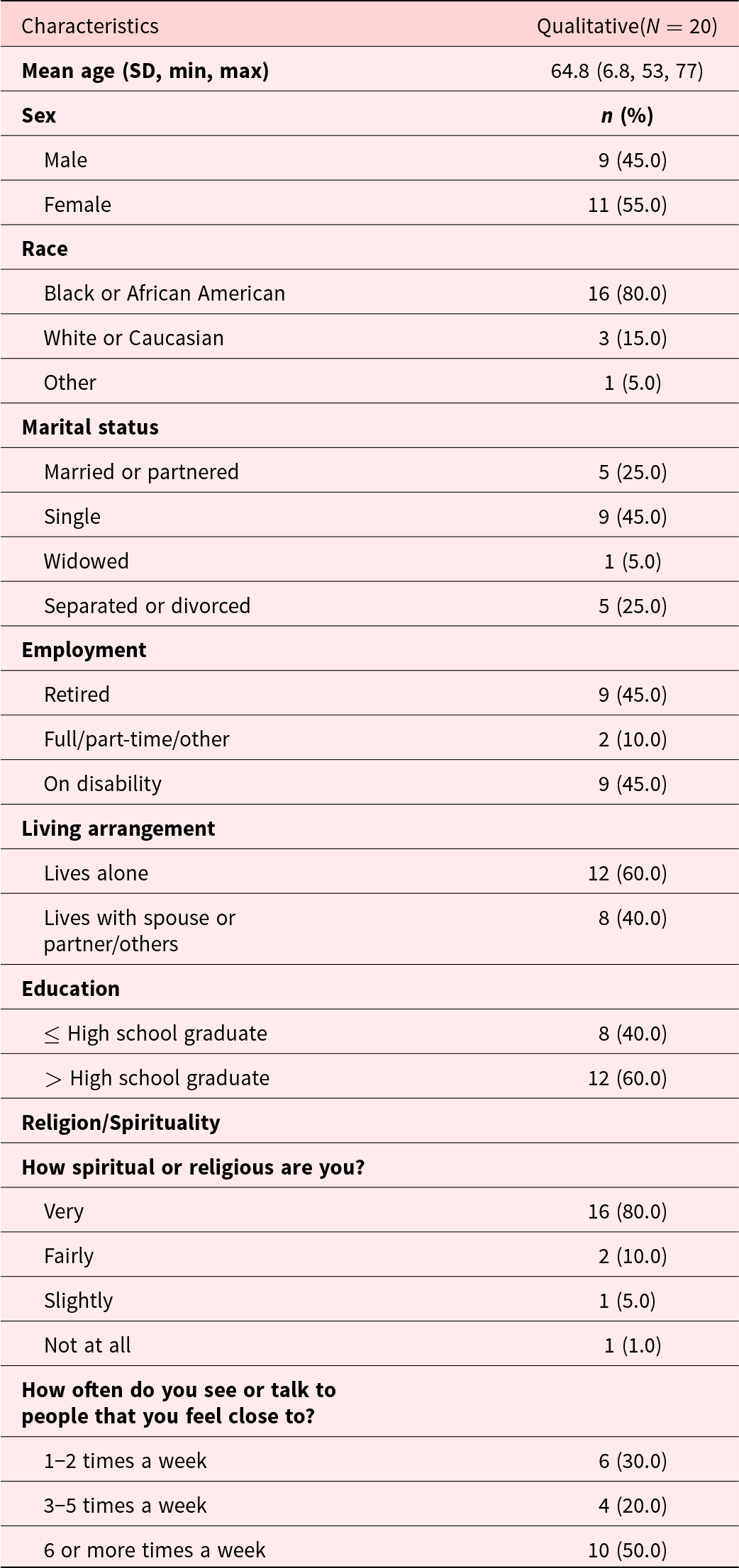
Descriptive statistics are provided (Table 1). Twenty participants completed qualitative interviews. One participant completed the interview with his wife (also consented), but her data were not included in the analysis or report. The sample consisted of participants aged from 53 to 77 years, including 11 women (55%), and 16 (80%) identified as Black or African American. Median interview length was 47.5 minutes and ranged from 21 to 82.5 minutes.
Sample characteristics for qualitative interviews (N = 20)

Thematic analysis of interviews
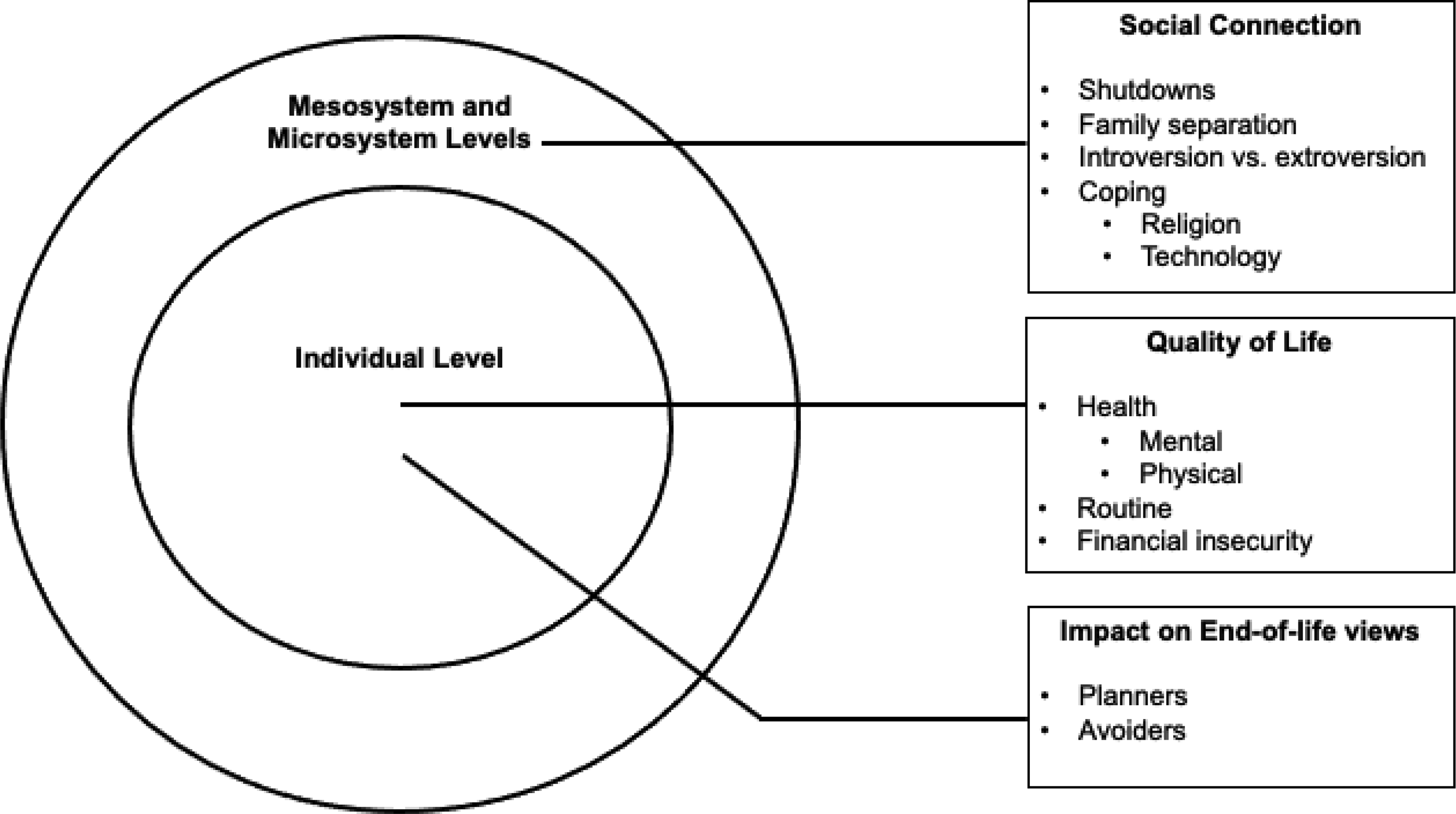
Three themes emerged that represented the everyday COVID-19 experiences and the effect on end-of-life planning views among limited income, older adults: (1) social connection, (2) quality of life, and (3) impact on end-of-life views. Themes and subthemes are supported by quotes and depicted in Fig. 1.
Social connection
Social connection referred to the feeling of fitting in with and being cared for by one’s social relationships (Kasar and Karaman Reference Kasar and Karaman2021). Subthemes included shutdowns, family separation, introversion vs. extroversion, and coping (e.g., religion, technology). A participant missed visiting the gym, “Going to the Y, being able to talk to my friends and we all exercise together..All that’s now just totally different…” (P-46). Another participant missed social activities, “I couldn’t go to church…couldn’t go shopping because some people wouldn’t have a face mask on and you are afraid…” (P-60).
Participants discussed separation from family. One participant avoided family get-togethers because of his high health risk, “…if you said, ‘…you want to go to the barbecue?’ I’m going to tell you no, because that’s a situation I shouldn’t be in…” (P-66). Participants described family separation, “My nephew…said, ‘…You have to say bye for at least 40 days or a reasonable time to the grandchildren..’ …is this real?” (P-73). Another participant described the general state of connection:
The social connections are no more. If you got a religious faith, that’s basically no more. Family connection, unless you got a telephone, that’s no more. Family reunions, holidays, traveling…at a standstill… (P-93)
Participant experiences differed depending on their socializing preferences. One participant described being an introvert and was unbothered by social distancing, “I was already socially like that…ready for mentally…” (P-12). Another more extroverted participant described the pain of being isolated from people, “COVID made me very lonely because I’m an outgoing type of person…I love to talk…God did not make man to be isolated…” (P-82).
Themes and subthemes adapted to the Social Ecological Model.

Participants described coping with social distancing including technology and religious faith. One participant met his wife on social media during the pandemic, “…she accepted the [Facebook] friend request, we talked…been two peas in the pod since…” (P-68). Another participant used Zoom to supplement in-person gatherings, “My friends come in here, we eat dinner, all of them here…and it just shut it down…we started doing things on the Zoom.” Another participant relied on her relationship with God to overcome feeling lonely, “…COVID really had a negative effect on me. It allowed me to my relationship with God to grow stronger…” (P-82).
Quality of life
Quality of life referred to the belief of how good or bad life is related to the multidimensional areas of health, routine, and socioeconomic stability (Kasar and Karaman Reference Kasar and Karaman2021). Subthemes included health effects, routine, and financial insecurity. Participants reported a range of mental and emotional experiences such as fear, depression, and the hope that life would end. One participant developed a fear mindset during COVID, “…plays on the mind. Everything is COVID, COVID, COVID…‘Well, I just don’t want to hear COVID no more,’ but you got fear of COVID because you got to…” (P-04). One participant had additional psychological challenges during COVID-19 while being restricted to a small apartment by the cold weather as well as infection precautions, “…when you grow up in a place [where you can go outside all year], you are adjusted to everything that place offers. But if not, you don’t know how to deal…” (P-73). Another participant felt constricted when she couldn’t go outside, “I was in a four-cornered wall and it was like they were closing in…scared to this and scared to that…I didn’t have a balcony to sit on…” (P-30). This participant hoped her time would come early, but not from a suicide, “I have what any average person…. Lord God, come on then take me away…” (P-30).
Participants described the challenges around COVID-19’s physical health effects based on personal or family experiences. One participant was still recovering from COVID-19 hospitalization, “I just thank God that it didn’t shut none of my organs down…I had it pretty bad because it seemed like I’m climbing a ladder…I’m still struggling” (P-74). Another participant worried about her adult child with long-term COVID effects, “…my daughter had pneumonia and COVID…. Right now…she can’t hardly walk. Air makes it hard for her to breathe…” (P-60). Lastly, a participant described living in a state of fear while her son seemed to be sick with COVID, “I had never seen my son with a fever like that…For me, he had COVID…it’s [living in fear]. It is like not having life…” (P-73).
Participants described adjusting or sustaining their routines during the pandemic. One participant would only leave the house early in the day to avoid the heat, “…the mask kind of a little bit makes it kind of a little bit uncomfortable…when you start sweating and you need to breathe…” (P-46). Another participant described new cleaning rituals directed by her children, “you’re afraid for your own people to come visit. Like, my son…He’s like, ‘…anybody come in, make sure they clean their hand…’” (P-60). Another participant reported not noticing much of a lifestyle change because of the pandemic, “No more than wearing a mask everywhere you go. Kind of disturbed about how many people’s passed during this epidemic, other than that it hasn’t bothered me at all…” (P-22).
A few participants conveyed the effects of the pandemic on financial and material security. A participant summed up the main effect of COVID, “…kind of screwed everything up…Basically financial…” (P-62). Another participant described his wife not being able to work in her hospitality job, “Going down from a two-salary household down to one…We had to…go to the food banks…” (P-67). Another participant had to find a new place to work, “…the place that I was working at, they shut out…so I worked at…this thrift store …It didn’t pay that much…I’m one of them type people I’ve got to be doing something” (P-78). Another participant continued to work as an essential, transportation industry worker, “…I was flagging traffic…I worked the whole time…My company was even nice enough to give us hazard pay…” (P-68). Another participant talked about the challenges with getting disability income during COVID-19 closures, which he needed to afford housing, “When you call [Social Security case manager], you’ll never talk to them because it’s closed, because of the pandemic…. Everything’s on the phone” (P-66).
Impact on end-of-life views
The impact on end-of-life views referred to the degree to which individuals experienced changes to their end-of-life or end-of-life planning views because of COVID-19 (Kim-Knauss et al. Reference Kim-Knauss, Lang and Rupprecht2022). Subthemes include planners and avoiders, which exhibited two types of planning readiness, whose status remained unchanged by COVID-19. Another participant with ACP already in place remarked that COVID had no effect on her end-of-life care plans, “Everything’s just still the same with me. If I contract it and have to go in and put me on ventilators and all that? Uh-uh (negative)…” (P-78). A participant reinforced the idea that COVID had no impact on planning because she already had her plans established, “It never did because if you already have planned. You have got a process that way…” (P-29). Another participant with high risk for health complications had enhanced her commitment to preventing illness from COVID, “…even now, the doctors tell me I still have to try to protect myself…” (P-04)
One participant without any ACP aside from verbally naming his health-care proxy, “No, it didn’t. It made no difference, because everybody you live to die…we’re all going to die…” (P-22). Another participant with no ACP stated expressed his views about the impotency of planning on death: “Well, no. It hadn’t any influence on that…and it is not going to change that situation…If the doctor can’t change it, somebody not a doctor sure can’t change it” (P-93).
Discussion
Three themes encapsulated the COVID-19 perceptions of low-income, older adults: (1) social connection, (2) quality of life, and (3) the impact on end-of-life views. Despite the relevance of COVID-19 to ACP, participants denied any changes in their ACP views or behaviors. While clinicians and advocates have called for increased ACP during the pandemic as COVID continues to be a leading cause of death (McAfee et al. Reference McAfee, Jordan and Cegelka2022), participants commented decisively on the everyday experience of COVID-19 rather than a sense of urgency to plan for care. This finding may reflect the need for a segment of this low-income population to prioritize daily survival and practical matters over planning ahead, particularly in the context of lifelong financial insecurity (Mayo et al. Reference Mayo, Pham and Patallo2022). Additionally, the data indicated that participants experienced loneliness and mental health struggles that may have precluded the social and learning activity necessary for robust ACP. This study has contributed to the literature in the following ways, using the Social Ecological Model as a framework for discussion.
First, we learned that the breakdown of social systems was experienced differently depending on pre-pandemic social preferences and practices and these breakdowns may have limited the change to ACP views. The microsystem of one’s direct social influences (i.e., family) experienced a shift from in-person activity to social distancing. Additionally, several microsystems (i.e., church, extended family) were disrupted because of building closures. At the mesosystem level, COVID-19-mandated closures disrupted interactions with extended family and friends that occurred during gatherings such as reunions and church attendance (Bronfenbrenner Reference Bronfenbrenner1974). These disruptions were experienced differently based on individual characteristics (e.g., introversion), group membership (e.g., church, gym), and coping strategies (e.g., technology, prayer).
While we did not investigate the underlying reasons for unchanged ACP views, these system breakdowns may have reduced in-person ACP opportunities that foster communication quality within marginalized communities (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021). For instance, family trust and communication is more important than that of the clinician–client relationship among African American families (Sanders et al. Reference Sanders, Robinson and Block2016); however, low-income, older adults may have had limited in-person or phone interactions, which prevented ACP conversation quality and depth with family. As reported in previous literature, participants experienced social isolation and loneliness during shutdown periods (Kasar and Karaman Reference Kasar and Karaman2021) and social isolation reduces ACP participation (Cudjoe et al. Reference Cudjoe, Boyd and Wolff2020). Future research should investigate the impact of social system breakdowns on ACP during and after the pandemic.
Additionally, while we did not investigate the COVID-19 health-care interactions, current literature supports that many routine health-care visits were delayed, shortened, or shifted to telehealth during the pandemic (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021). Health-care systems were forced to prioritize the influx of COVID-19 cases amid staffing attrition and resource limitations over lower priority activities (i.e., ACP) (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021). Coupled with reduced face-to-face social interactions and limited time, clinicians often must focus on the multi-faceted health and social needs among low-income, older adult patients rather than engage in lengthy ACP conversations (Ashana et al. Reference Ashana, D’Arcangelo and Gazarian2021). Future studies should explore the impact of COVID-19 on health-care interactions and ACP to develop or modify ACP checklists and resources to maintain efficient clinic visits, support care quality, and make appropriate referrals for this population (Fahner et al. Reference Fahner, Beunders and Van der Heide2019).
At the individual level, we found that participants experienced negative mental health consequences and diminished quality of life as the social networks of daily life were paralyzed by the pandemic (Kasar and Karaman Reference Kasar and Karaman2021). Mental and emotional health experiences included fear, panic, thoughts of wanting an early and natural death, and coping with the many pandemic lifestyle changes. In the absence of adequate opportunities to plan for ACP due to social system breakdowns, clinicians should be aware that clients with depression may have been more likely to use ACP, but also more likely to opt to not extend life (McMahan et al. Reference McMahan, Barnes and Ritchie2020). Clinicians should screen for mental health disorders (e.g., depression) in conjunction with ACP to understand preferences and guide recommendations.
At the behavior and individual levels, the study findings contribute to the literature by strengthening the understanding that ACP was not among life priorities affected by the pandemic. Participants with established ACP and end-of-life plans (e.g., life insurance) and those that avoided ACP did not report any adjustment to their planning activities because of COVID-19. Participants with established planning may have had an easier time maintaining those plans by periodically checking in with family or updating paperwork during doctor visits. Conversely, participants without existing plans continued to avoid planning. Initiating ACP may require more resources and motivation than was available during this crisis. This finding may have occurred due to the mesosystem breakdown (e.g., telehealth vs. in-person clinic visits) during the pandemic that would typically support complex, difficult discussions around death. Future studies should explore COVID-19-specific barriers to planning for low-income, older adults including technology access, health-care use and quality, social support, and mental health and create targeted approaches to address systemic barriers as part of widespread crisis management strategies.
The study findings have further policy and research implications. COVID-19 continues to have far-reaching effects on the societal structures that support socialization, quality of life, and ACP. In addition to the recommendations for individual clinicians, hospital administrators and state policymakers should recognize ACP as a priority to support clinicians with the time, resources, competence, and confidence necessary to facilitate ACP opportunities for low-income individuals who are ACP avoidant. Public health departments may use targeted media messaging to increase awareness of ACP to empower personal and familial autonomy (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021). Legal barriers should be addressed by simplifying documentation procedures (e.g., reducing notary requirements) and allowing multimedia ACP forms (e.g., audiovisual), particularly during times of crisis (Hirakawa et al. Reference Hirakawa, Saif-Ur-Rahman and Aita2021).
Future community-based participatory research should explore COVID-19 factors that enabled or hindered ACP among low-income, older adults and design targeted, culturally tailored approaches to address these barriers. Researchers should innovate with community health workers and leaders to enhance ACP knowledge at the community and individual level. For instance, researchers may design and test mindfulness-based ACP methods for adults with mental health challenges to gradually incorporate ACP subject matter after developing skills to cope with mortality (Cottingham et al. Reference Cottingham, Beck-Coon and Bernat2019).
Strengths and limitations
This report presented a narrative of low-income, older adults’ perceptions of the pandemic’s influence on everyday life and ACP views. Findings were limited by not using member checking, but trustworthiness of study results were bolstered in the following ways (Morse et al. Reference Morse, Barrett and Mayan2002). Transcripts were generated by a professional transcription service and then compared with the original audio files for accuracy. Coders performed multiple, iterative rounds of coding to promote data familiarity (credibility). We did not directly ask each participant about COVID-19 history; however, these interviews were held while several participants continued COVID-19 precautions given their age and only 1 reported previous illness. Transferability of study findings must be interpreted with similar populations (e.g., housed) and settings (e.g., urban) in mind, but was strengthened by recruiting from multiple sites and purposive sampling to represent broad, diverse perspectives. Dependability of the final 2 themes was enabled by the consistency of the participant responses, which allowed for data saturation (i.e., data were redundant, and no new themes were discovered). Confirmability of the findings was supported by using an audit-trail, field notes, 2 independent coders, using a standardized, well-tested interview guide, and cultivating personal awareness of biases (e.g., conflict of nursing perspective with research).
Conclusion
COVID-19 has diminished social contact and quality of life among low-income, older adults, but we found that ACP views or behaviors remained stable. When ACP is viewed within the Social Ecological Model, the findings suggest that COVID-19 had a greater impact on daily life socialization and overall quality of life than ACP activities, which were perceived as superfluous. These factors may impact ACP and should be assessed as part of routine clinical checkups. Additionally, health care and state policy should prioritize ACP to contribute to system-wide supports that will enable health-care professionals within and beyond the community setting to initiate ACP.
Our next steps include a detailed exploration of how frequency and quality of health-care interactions during the pandemic affected ACP opportunities. We will use community-engaged approaches to assess pre-existing and pandemic-influenced ACP barriers to design tailored ACP education programs for community professionals, workers, and peers who are sustainable during times of large-scale crisis.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951523000688.
Competing interests
None.



 Open access
Open access