

I. Introduction
Corruption is a known barrier to the enjoyment of the right to health and other human rights. It undercuts transparency, accountability, non-discrimination and meaningful participation in civic life.1 The health system in particular is always vulnerable to corruption risks. There are corruption risks throughout it: from the primary health care level to high levels of government policy because of the vast sums of money involved, and the health system’s fragmentation, technical complexity, and multiple stakeholders.Reference Kohler2
In this article, we examine one important form of health system corruption — pharmaceutical company bribery that compromises the pharmaceutical system.Reference Saeed, Kohler, Vian, Pieth and Søreide3 For example, pharmaceutical company bribes and other financial inducements can distort prescribing and compromise regulations that are designed to ensure drug safety and efficacy.Reference Rodwin4 More generally, pharmaceutical industry corruption affects patient safety and health care resource allocation worldwide.Reference Gagnon5
There are two main ways of understanding corruption: the first, which might be called classic corruption, includes illegal acts such as bribery; the second broader conception includes illegal and legal acts, incentives, and dependencies that undermine an institution’s ability to achieve its purpose. Although our focus is on classic corruption, namely bribery, we frame our discussion within the broader concept of institutional corruption.Reference Fotaki6 We understand bribery, defined by Transparency International, as “the offering, promising, giving, accepting or soliciting of an advantage as an inducement for an action which is illegal, unethical or a breach of trust.”Reference Kohler7 This definition conceives bribery broadly and includes both illegal and legal actions.8
In a similar vein, the concept of institutional corruption as conceptualized by Professor Lawrence Lessig includes both legal as well as illegal acts that “pervert institution’s function under conditions that may promote personal benefit.”Reference Lessig9 Lessig writes that:
“Institutional corruption is manifest when there is a systemic and strategic influence which is legal, or even currently ethical, that undermines the institution’s effectiveness by diverting it from its purpose or weakening its ability to achieve its purpose, including, to the extent relevant to its purpose, weakening either the public’s trust in that institution or the institution’s inherent trustworthiness.”10
Accordingly, pharmaceutical policy can be compromised not only by bribery or other illegal acts, but also by influences that undermine the institution’s effectiveness.Reference Rodwin11 For example, the architecture of the pharmaceutical markets fosters “a misalignment of financial incentives and public health…”12 In addition, other legal financial incentives can also undermine an institution’s purpose.
Recognizing its detrimental impact, the Organisation for Economic Co-operation and Development (OECD) Anti-Bribery Convention aims to combat bribery in its member countries. It addresses cross-border bribery acts rather than bribes limited within a single country. The Convention requires member states to criminalize foreign bribery with enforcement monitored by the OECD Working Group on Bribery.13 Despite these efforts, allegations of improper payments from the pharmaceutical sector remain due to the complicated and sometimes non-transparent interactions between corporate interests, government regulation, and international compliance oversight.Reference Gagnon, Faintuch and Faintuch14
The OECD Anti-Bribery Convention is a binding treaty that requires its member countries to criminalize foreign bribery and enact enforcement measures. The OECD Working Group on Bribery monitors state parties’ compliance through peer-reviewed Phase Reports that summarize national investigation and enforcement data. Phase Reports synthesize official case information provided by states. The reports offer cross-country comparisons but rely heavily on the initiatives of domestic agencies rather than direct OECD investigations. As such, the reported cases reflect enforcement priorities and capacities within national jurisdictions.
Globally, health systems rely on transparency and accountability between various actors to guide rational drug selection and achieve equitable access to essential medicines.15 However, it is well-documented across the literature that pharmaceutical companies, a key actor in these systems, engage in bribery whether by offering lavish perks to health care professionals or funneling illicit funds through third-party intermediaries.Reference Brax16 Such practices have a wide array of consequences. They can jeopardize the integrity of clinical decision-making and undermine public confidence in medical practice.17 Though the total cost of corruption within the health sector is unknown, a European study found that corruption in the health care sector is expected to cost up to EUR 56 billion annually.18 This study identified bribes as having led to the purchasing of lower quality medicines at inflated prices, which is damaging to patients both medically and economically.19 These concerns are not limited to a single region or a handful of corporations. Rather, allegations of bribery have emerged in multiple jurisdictions, implicating a range of industry actors and intermediaries.20
Although various national authorities have investigated these schemes, the true scope and scale of bribery in the pharmaceutical sector remains difficult to ascertain.21 Intricate financial arrangements, incomplete reporting, and limited public disclosures often hide or minimize the extent of misconduct.22 In this context, the OECD Working Group on Bribery has become a much-needed source of public information. The Group releases periodic Phase Reports that document alleged bribery incidents and monitor the enforcement of the OECD Anti-Bribery Convention, providing detailed information of bribery-related investigations and enforcement actions against companies in multiple jurisdictions.23 Each individual report contains findings from data that is gathered from an on-site visit, the input of diverse stakeholder perspectives (academic, civil society, and the private sector), recommendations to strengthen compliance with the anti-bribery convention, and follow-up issues that require ongoing monitoring.
To better understand and characterize bribery within the global pharmaceutical industry, this paper provides an initial exploration of the prevalence, characteristics, and patterns of bribery in pharmaceutical sector cases documented within the OECD Working Group on Bribery Phase Reports.
II. Methods
To examine patterns of foreign bribery in the pharmaceutical sector, a targeted review of the publicly available OECD Working Group on Bribery Phase Reports was conducted. Aligning with the objectives outlined above, all publicly available Phase Reports (1999–February 5, 2025) produced by the OECD Working Group on Bribery were systematically searched to identify cases in which pharmaceutical companies were implicated in bribery schemes related to pharmaceuticals (i.e., prescription and over-the-counter drugs). All phase reports were screened using the following inclusion criteria:
-
1. The investigation explicitly implicates a pharmaceutical company in a foreign bribery case; and,
-
2. The bribery scheme is clearly linked to pharmaceutical products through securing regulatory approvals, influencing prescribing patterns, or increasing drug sales.
Cases involving medical devices were excluded from the review. Data from the identified cases was extracted and organized in Excel spreadsheets. Full data extraction table is included in Appendix A . An inductive thematic analysis was then conducted across identified cases to determine similarities and patterns across cases, and illustrative examples were compiled to support the analysis.
III. Results
Searches identified investigations into pharmaceutical industry bribery in five OECD member states that signed the OECD Anti-Bribery Convention. The United States had the highest number of investigations (fourteen cases), followed by Germany (three cases), Denmark (three cases), Greece (one case), and Italy (one case). These investigations implicated 19 pharmaceutical companies, with 14 companies explicitly named: BioTest, Novartis, Johnson & Johnson (J&J), Pfizer, Teva, Eli Lilly, Bristol-Myers Squibb (BMS), SciClone, Nordion, AstraZeneca (AZ), GlaxoSmithKline (GSK), Sanofi, and Novo Nordisk.24 The remaining cases involved companies that were either undisclosed or not publicly specified.25 The characteristics of these investigations are summarized below in Table 1 , accompanied by a narrative description. It is important to emphasize that the analysis is restricted to cases that progress to official investigation and prosecution; thus, it does not capture the full extent of foreign bribery in the pharmaceutical sector. The discrepancy between the small number of detected cases and the extensive use of sophisticated concealment methods suggests that the OECD Convention, while significant in principle, has had only a modest effect on curtailing opportunities for corruption.
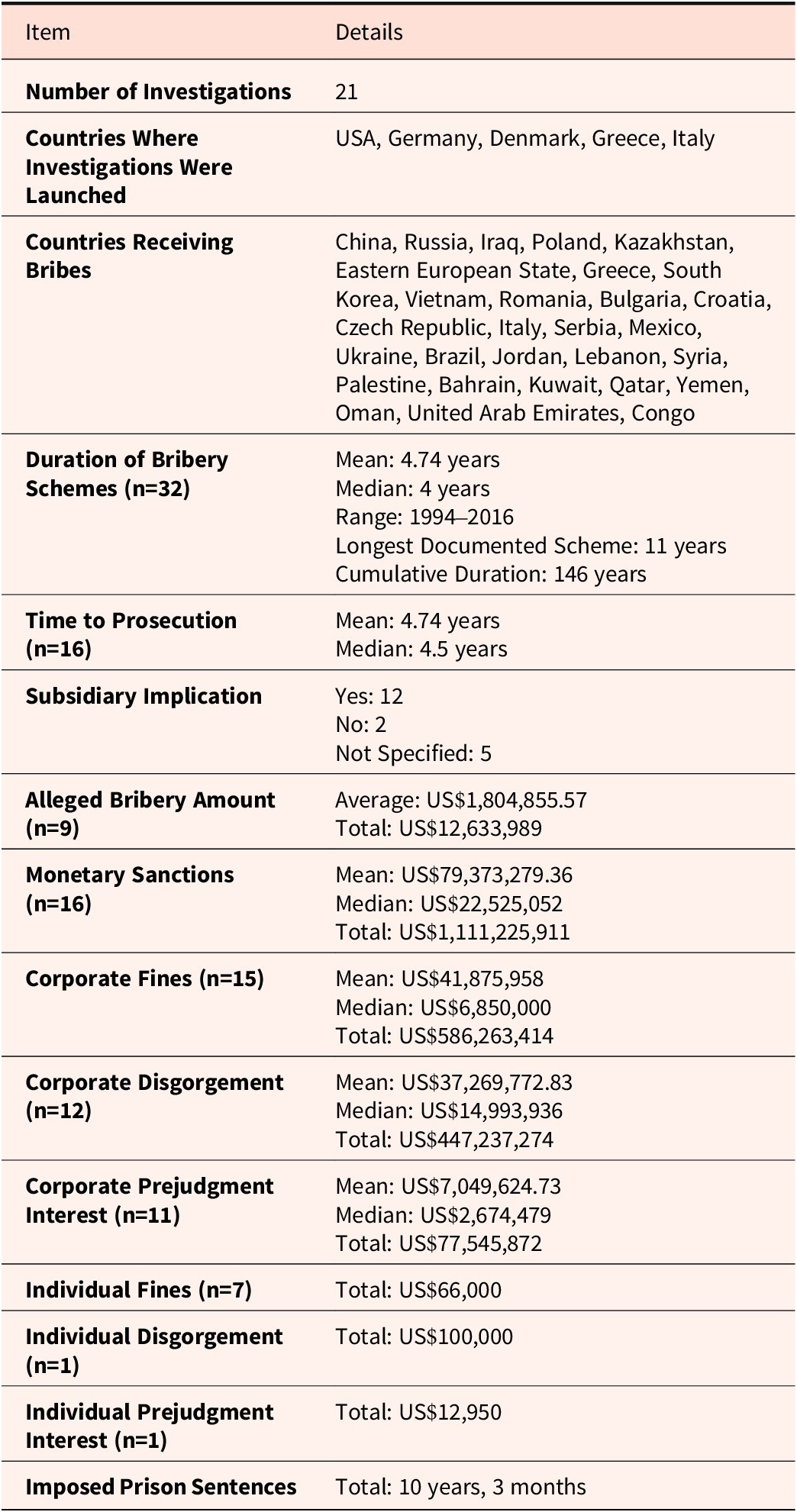
Summary of Bribery Investigations and Enforcement Data Gathered Through OECD Working Group on Bribery Reports

Table 1. Long description
Beginning at the top, the table lists 21 investigations. Countries launching investigations are U S A, Germany, Denmark, Greece, and Italy. Countries receiving bribes include China, Russia, Iraq, Poland, Kazakhstan, Eastern European State, Greece, South Korea, Vietnam, Romania, Bulgaria, Croatia, Czech Republic, Italy, Serbia, Mexico, Ukraine, Brazil, Jordan, Lebanon, Syria, Palestine, Bahrain, Kuwait, Qatar, Yemen, Oman, United Arab Emirates, and Congo. Scheme duration for 32 cases shows a mean of 4.74 years, median 4 years, range from 1994 to 2016, longest scheme 11 years, cumulative duration 146 years. Time to prosecution for 16 cases has a mean of 4.74 years and median of 4.5 years. Subsidiary implication is yes in 12 cases, no in 2, not specified in 5. Alleged bribery amount for 9 cases averages U S dollar 1,804,855.57, total U S dollar 12,633,989. Monetary sanctions for 16 cases average U S dollar 79,373,279.36, median U S dollar 22,525,052, total U S dollar 1,111,225,911. Corporate fines for 15 cases average U S dollar 41,875,958, median U S dollar 6,850,000, total U S dollar 586,263,414. Corporate disgorgement for 12 cases averages U S dollar 37,269,772.83, median U S dollar 14,993,936, total U S dollar 447,237,274. Corporate prejudgment interest for 11 cases averages U S dollar 7,049,624.73, median U S dollar 2,674,479, total U S dollar 77,545,872. Individual fines for 7 cases total U S dollar 66,000. Individual disgorgement for 1 case totals U S dollar 100,000. Individual prejudgment interest for 1 case totals U S dollar 12,950. Imposed prison sentences total 10 years and 3 months.
The total timeframe of the investigations ranged from 1994 to 2016, with the longest recorded scheme lasting 11 years.26 The average scheme duration was 4.74 years, which contributed to a cumulative total of 147 years across all cases.27 The average time from detection to prosecution was 4.6 years.28
Although the true scale of bribery remains difficult to determine due to the opaque nature of these schemes, partial figures uncovered at least US$12,633,989 in illicit payments.29 Total monetary sanctions imposed totaled US$1,111,225,911.30 Of these amounts, companies faced fines totaling US$586,263,414, while disgorgement and prejudgment interest reached US$447,237,274 and US$77,545,872, respectively.31 The largest single sanction, US$519,279,572, was imposed on Teva Pharmaceuticals in 2016.32 Individuals were fined US$66,000 in total, with US$100,000 and US$12,950 assessed in disgorgement and prejudgment interest, respectively.33 In total, courts imposed 10 years and 3 months of prison time in sentencing across all cases though some convictions may have been subject to appeal.34
Subsidiaries played a major facilitating role in bribery cases with confirmed involvement in 12 cases.35 Involvement remained unspecified in 5 cases.36 As an example, Eli Lilly’s Russian subsidiary transferred millions of dollars to offshore companies.37 The company claimed these payments were for “marketing services” but were intended to persuade pharmaceutical distributors and government agencies to buy Lilly’s medications.38 Amongst these payments, approximately US$2 million was sent to an offshore company owned by a government official.39 Another US$5.2 million was directed to offshore entities linked to someone closely connected to a member of Russia’s Parliament.40 Even though the Company acknowledged that these marketing contracts were being used primarily to generate sales opportunities with government clients and that there was little indication any real services were provided, Eli Lilly continued to allow its subsidiary to rely on these agreements for more than five years.41
Bribery payments were directed toward 30 countries.42 The analysis identified a large range of recipient countries with China (eight cases) and Russia (six cases) most frequently implicated.43 Additional instances of bribery were recorded across Eastern Europe, Asia, the Middle East, Latin America, and Africa including Iraq (three cases), Poland (two cases), and Kazakhstan (two cases).44 Other countries implicated in bribery schemes were Greece, South Korea, Vietnam, Romania, Bulgaria, Croatia, Czech Republic, Italy, Serbia, Mexico, Ukraine, Brazil, Jordan, Lebanon, Syria, Palestine, Bahrain, Kuwait, Qatar, Yemen, Oman, Republic of Congo, and the United Arab Emirates.45 Additionally, two cases involved unnamed Eastern European countries, while another case pertained to an unspecified EU country.46
From our analysis of the 21 pharmaceutical bribery cases, 14 originated from the United States. This is due to their enforcement under the United States (US) Foreign Corrupt Practices Act (FCPA). The US concentration may influence patterns seen in the data, as US cases tend to involve sizable penalties and detailed disclosure, whereas other countries may investigate fewer cases or impose different sanctions. Given that pharmaceutical markets and corporate operations are international in scope, national differences in compliance and enforcement frameworks affect the reported cases and observed penalties, although corporate corruption incentives likely transcend borders. Prison sentences totaling over 10 years were imposed across these cases, with the substantial majority from US-based prosecutions. Many countries focus enforcement on corporate fines resulting in an uneven distribution of criminal penalties. This pattern underscores the variance in OECD countries operationalization of the Convention’s provisions on individual liability.
Bribery schemes were identified in countries where state-owned or government-controlled health care systems dominated (OECD 2014a; 2012; 2021; 2022a; 2023; 2018; 2022b). For the purpose of this study, and following the OECD’s classification, we considered countries with state-owned or government-controlled health care to be those where the majority of financing, regulation, and delivery of health services is administered through public institutions, and where government agencies have a central role in procurement and reimbursement of medicines. It is noteworthy that the OECD includes the United States in this classification. This is likely due to the sufficient government involvement in public health programs such as Medicare, Medicaid, and Veterans Affairs (VA). Here, public hospitals and clinics fall under the classification of “foreign officials” under anti-bribery statutes if their staff have the authority to make or influence government decisions.Reference Rush47 Examples of government decisions that can be influenced through bribery schemes are drug approvals, national formulary listings, state reimbursement policies, or bulk purchasing agreements.48
Many of the schemes specifically targeted public hospitals and clinics where employees held purchasing power as well as high-ranking Ministry of Health officials responsible for major drug approvals, reimbursement schedules, and government tenders.49 Across all investigated cases, the bribed individuals could have been both publicly or privately employed physicians, nurses, operating room heads, hospital staff, pharmacists, pharmacy employees, hospital administrators, and procurement or tender committee members.50 Additionally, various government officials such as those from the Ministry of Health, customs agencies, Parliament, and state-run procurement agencies were implicated.51 In at least one instance, consultants from an international organization, in this case the United Nations Development Program (UNDP), were also involved.52
Across cases, company employees at every level from frontline sales and distributor personnel to middle managers, local executives, and even high-ranking corporate officers were directly complicit in planning, executing, or approving bribery strategies.Reference Onwujekwe53 Senior managers authorized inflated payments or disguised expense claims.54 At times, executives approved false documentation or misrepresented financial transactions in official records and audits, and lower-level sales representatives regularly funneled funds or gifts, meticulously tracking prescription volumes or purchase orders to justify continued bribes.55 Frequent internal warnings and compliance reviews, which spotlighted obvious red flags in accounting and documentation, were often ignored or treated as isolated incidents.56
Below, the patterns identified within these cases are discussed, including the disguising of bribes as gifts, the manipulation of research, the misuse or misreporting of funds, compensating officials under the guise of consulting or speaker fees, explicitly bribing regulatory officials, kickbacks, third-party vendors, and charitable front groups.
IV. Patterns of Corrupt Practices in the Pharmaceutical Industry
Sponsorships, Travel, Gifts, and Entertainment as Disguised Bribes
Pharmaceutical companies frequently covered the costs for health care professionals to attend conferences, congresses, and educational meetings.57 However, these payments were often inflated or included lavish, non-work-related perks such as shopping trips, sightseeing tours, and family travel, leading to their classification as bribes.58 In some cases, companies extended personal loans to physicians or officials with no expectation of repayment or transferred cash directly to doctors’ bank accounts under vague billing descriptions.59 Beyond travel-based incentives, schemes featured weekend retreats to spas, bathhouses, and karaoke bars by framing them as educational seminars or symposia.60 Meanwhile, luxury items ranging from digital cameras and expensive wines to wristwatches, jewelry, and cosmetics were gifted alongside more everyday perks such as specialty foods, shopping vouchers, and small electronics.61 In such cases, sales teams meticulously tracked each health care professional’s prescription volume to ensure a return on investment.62 Some demonstrative examples include Novartis Greece, which sponsored doctors for international congresses but threatened to withdraw support if quotas were not met.63 In another case, Johnson & Johnson Romania transitioned from direct cash bribes to covering family vacations.64 Pfizer arranged incentive trips such as ski weekends and sightseeing tours in Bulgaria, the Czech Republic, Italy, and China, while Bristol Myers Squibb China falsified invoices to fund travel and entertainment for government-employed health care professionals.65
Falsified or Manipulated Clinical Studies and Research
Some companies established fraudulent or low-value clinical studies (sometimes labeled as “Phase IV,” “observational,” or “epidemiological” studies) to funnel payments to health care professionals.66 These studies functioned as marketing tools. Sales representatives recruited doctors who prescribed specific drugs and then paid them under the guise of “study fees” or “data collection.” 67 Paperwork was often incomplete or deliberately misleading. For example, Novartis Greece used studies to promote Lucentis rather than conduct genuine research while Novartis Korea funneled payments through a sham neuroscience clinical study in 2013.68 Pfizer Italy also relied on substandard observational studies in which sales teams selected participants by offering them cash and gifts tied to prescription targets.69
Distributor Discounts, Credit Notes, and Margin Manipulation
Another pattern of bribery identified was pharmaceutical firms granting unusually steep discounts or credit notes to distributors who in turn used the excess funds to pay bribes to health care professionals or public officials.70 In some cases, these bribes incentivized doctors to prescribe products, while in others they secured government procurement contracts. Companies falsely recorded the discounts as legitimate marketing or margin expenses, which effectively hid the bribe payments. Novartis Vietnam was one such company that collaborated with a distributor that paid bribes directly to health care providers.71 The company reimbursed up to 50% of these costs through credit notes.72 In other examples, Teva Mexico funneled cash to doctors through a Copaxone distributor by mislabeling the payments as “revenue reductions,” while Lilly Brazil granted a distributor abnormally large discounts (17–19% instead of the standard 10%), concealing a 6% bribe to state officials within the markup.73
Consulting, Speaker Fee, and Medical Roundtables
Hiring health care practitioners or government officials under titles such as “consultants,” “speakers,” or “Key Opinion Leaders” was another common manifestation of bribery identified in this review.74 Individuals were paid for little or no actual work while the expenditures were classified as “advisory services,” “lecture fees,” or “professional consulting.”75 Some cases took this a step further by organizing nominal “medical roundtable” discussions where health care providers were paid honoraria for participation.76 In one example, certain employees routed money through third-party medical journals (ostensibly for advertising) that was then funneled to health care providers as honoraria for attending or speaking at these roundtables.77 Because the events were billed as external meetings, they often bypassed internal compliance or due diligence controls.78 Like other “consultancy” arrangements, these roundtable payments served as covert bribes that were recorded in corporate books as legitimate marketing or professional fees.79 Examples include Novartis Vietnam’s “consultant” payments to hospital staff, Teva Ukraine’s $200,000 in monthly consulting fees to a senior health official, and Pfizer Croatia’s monthly “consulting” plan for a government doctor.80
Bribery of Government Officials for Procurement and Regulatory Approvals
This analysis identified that pharmaceutical firms directly bribed public officials or funneled payments through intermediaries to expedite regulatory approvals, accelerate product registrations, or guarantee contracts in state-run hospitals.81 These arrangements were directed towards ministries of health, procurement agencies, and government-run insurance programs. To conceal the bribes, companies inflated contract prices, manipulated marketing expenses, or forged consulting agreements.82 For example, Teva Russia formed a distribution deal with a company owned by a high-ranking Russian official who then used political influence to secure preferential treatment for their drug product, Copaxone.83 Additionally, Lilly Russia funneled more than $11 million through offshore shell companies tied to Russian politicians and the head of a state-owned distributor.84
United Nations Oil-for-Food Kickbacks
Under the United Nations (UN) Oil for Food Program, pharmaceutical companies were required to sell products to Iraq by way of an UN-supervised system.85 This review identified firms manipulating contract pricing, inflating costs and redirecting the excess funds as disguised “agent commissions” to Iraqi ministries.86 These payments were falsely recorded as legitimate fees or marketing costs while the companies recovered the padded amounts from the UN escrow fund.87 Johnson & Johnson also paid $857,387 in kickbacks disguised as agent commissions to secure contracts with Iraq’s Ministry of Health (Kimadia).88 Additionally, Johnson & Johnson inflated contract prices by 10% in Iraq by disguising the overcharge as “promotional activities” and directing the funds to Iraqi officials.89 Further, Novo Nordisk paid $1.44 million and authorized an additional $1.32 million in inflated commissions to funnel such bribes.90 In another case prosecuted in Italy, an unidentified pharmaceutical company was accused of paying EUR 144,660 in bribes under the program, but charges were later dismissed due to the statute of limitations.91
Shell Companies, Pass-Through Vendors, and False Invoicing
As briefly mentioned above, analysis identified that illicit payments were concealed by companies utilizing third-party vendors, offshore shell entities, or dummy middlemen. These intermediaries were used to route bribes while creating fraudulent invoices for nonexistent services such as “advertising,” “storage,” “consultancy,” or “marketing”.92 In other cases, vague descriptions such as “distribution freight” were used to funnel funds to officials or doctors without raising immediate red flags. Novartis Greece routed money through dummy vendors, inflating scientific activities that were primarily promotional in nature.93 Pfizer Russia funneled hospital rebates into intermediaries and shell companies in Cyprus, Canada, and Hungary under the guise of lobbying or freight fees.94 Eli Lilly Russia entered 96 sham “marketing/service” agreements with 42 third-party offshore entities, paying over $11 million to officials.95 In another example, Nordion used an agent with offshore accounts to disguise bribes as “unofficial costs” in cost estimates to win Russian regulatory approvals.96
Charitable or Philanthropic Fronts
In certain cases, pharmaceutical companies were found to have disguised bribes as charitable donations or contributions to philanthropic foundations connected to public officials. Internal emails and documentation explicitly referred to these payments as quid pro quo arrangements for regulatory approvals or favorable reimbursement decisions.97 For example, Eli Lilly Poland transferred nearly US$40,000 to a high-ranking official’s personal foundation in return for favorable drug reimbursement rulings.98
V. Distinguishing Types of Bribery Cases in the Pharmaceutical Sector
To assess the full public health implications of bribery in the pharmaceutical sector and to provide a cogent analysis of the consequences and severity of corruption documented, the identified cases of bribery can be classified in the following way. The first category involves cases whereby firms increase their profits without directly undermining drug quality. These cases can include practices such as unlawful incentives (kickbacks, lavish hospitality, sham consulting arrangements) provided to prescribers or government procurement officials. These types of bribery are designed to boost sales of approved drugs that otherwise meet quality standards. The immediate consequence is higher company revenue and market share, but prescribers and institutions are steered towards specific products potentially at the expense of cost-effectiveness or optimal patient care. In these scenarios, the drug quality itself is not directly compromised.
Second, there are cases leading to the sale of substandard pharmaceuticals or drug misuse. Bribery here is used to bypass regulatory scrutiny or to facilitate the sale of drugs that fail to meet safety, efficacy, or manufacturing standards in these scenarios. This results in direct public health risks, including the distribution of falsified, substandard, adulterated, or unapproved drugs. Bribes might be paid to inspectors, regulators, or supply chain actors to approve or ignore noncompliance.
Finally, there are hybrid cases where profit-driven corruption is combined with drug quality risks. Some cases combine profits for the firm with increased risks to drug quality or misuse. These can be off-label marketing (promoting drugs for unapproved indications through illicit incentives), which expands sales but may expose patients to unproven or dangerous uses. Similarly, bribes that secure approvals for new products or expanded indications without full regulatory vetting put both company profit and patient safety at risk. Some examples are cases where pharmaceutical sales teams, incentivized by bonuses, promoted drugs for uses not supported by evidence, or bribed officials to overlook inadequate clinical testing, yielding both higher sales and greater patient safety risks. These distinctions clarify both the economic and patient safety dimensions of corruption.
VI. Discussion
This review provides a novel exploration of the cases of bribery in the pharmaceutical sector identified within the OECD Working Group on Bribery Phase Reports. This analysis identified and characterized the 21 investigations of bribery in the pharmaceutical sector documented in the Phase Reports, including information on the monetary totals of the bribes and the profits generated, as well as the sanctions and penalties imposed against the implicated person(s) and/or companies.
In addition to summarizing the case characteristics, a thematic analysis of the Phase Reports revealed key patterns across cases. For example, many of the documented cases were explicitly approved (or at least knowingly tolerated) by high-ranking managers. This suggests that compliance programs may fail when financial incentives outweigh the perceived risks of misconduct. The importance of leadership commitment to ethical business practices is outlined in the OECD Guidelines for Multinational Enterprises on Responsible Business Conduct. 99 Without strong internal oversight and sufficient resources allocated to audits, illicit activities can become entrenched within regional offices and subsidiaries.100
Another recurring pattern was the use of intermediaries and complicated corporate structures to obscure bribes. Multiple cases revealed the involvement of subsidiaries, third-party vendors, or shell companies that processed payments disguised as legitimate transactions. While such arrangements can serve practical business functions, they also create opaque financial pathways that can be exploited for improper purposes.101 Strengthening due diligence requirements and imposing greater scrutiny on distributors, local agents, and other third parties that interact with government officials may help reduce these risks. This review therefore echoes other calls for reforms requiring transparency in intermediary relationships that could curb opportunities for bribery, such as the public disclosure of service fees and public reporting of clinical trial data.Reference Ross102
Bribery is not limited to one region; it was documented across a wide geographic spectrum. The repeated reliance on sham clinical studies, inflated distributor discounts, and disguised consulting contracts supports the idea that certain systemic weaknesses transcend national boundaries.103 Some countries, such as China and Russia, accounted for multiple cases; illicit payments were identified in 30 countries spanning Asia, Eastern Europe, the Middle East, and Latin America. This breadth supports existing literature arguing that corruption in the pharmaceutical industry is not confined to specific high-risk jurisdictions but is an indicator of overarching structural vulnerabilities.104
Braithwaite points out that countries struggle to counter transnational corporate bribery strategies because fragmented “regulatory agencies [are] often outmatched by the global reach of pharmaceutical firms.”Reference Braithwaite105 While multilateral intelligence sharing of corrupt practices may be beneficial to counter the global reach of pharmaceutical firms, the decline of global consensus may necessitate pragmatic regionalism. Regional collaboration can result in information sharing through the creation of centralized databases for tracking bribery patterns such as third-party payments to health care providers in weakly regulated markets. Regionalism addresses the “regulatory arbitrage” exploited by pharmaceutical firms where weak oversight in one country undermines neighboring markets.106 Harmonizing penalties (through shared blacklists of corrupt actors or other means) and standardizing whistleblower protections can allow regional bodies to create a unified deterrent front.
The concerning delays between the initiation of bribery schemes and their eventual detection is also a symptom of the ineffectiveness of corporate compliance frameworks and regulatory oversight. Many schemes persisted for years before being uncovered.107 Similar delays were observed between detection, investigation, and prosecution.108
We contend that bribery persists within the pharmaceutical industry because the risk of detection is low. To clarify, the costs to pharmaceutical firms from bribes consist of the amount of a bribe and the risk of penalties from a bribe (a function of probability of detection multiplied by the size of penalties). Pharmaceutical firms will compare these joint costs with the increased revenue and other benefits from engaging in corrupt practices when considering whether to engage in bribery. In short, pharmaceutical companies as rational profit maximizers (irrespective of legality) will compare the potential gains from bribery against the expected cost of being caught and punished.
Data from the 21 reviewed cases illuminates that total bribe payments paid was about US$12.6 million and total financial sanctions imposed (fines, disgorgement, interest, etc.) was approximately US$1.1 billion. Lengthy delays between scheme initiation and their detection and prosecution, coupled with the potential to contest charges, reduce the effective expected cost of corrupt practices. As a result, high financial penalties do not necessarily translate into meaningful deterrence against corruption. It is also important to consider how national differences in legal structures — some of which impose criminal liability, while others only impose civil penalties — may have an impact on the extent of bribery in the sector.
While our argument, as well as the Convention, is rooted in a deterrence model based on the assumption that corruption emerges from rational cost-benefit calculations, it is important to note that alternative accounts emphasize that corruption is not always reducible to monetary reasoning. For example, Braithwaite argues that in the pharmaceutical industry, corrupt practices are often embedded in institutional norms and market structures.109 Similarly, Feldman and colleagues draw on behavioral ethics to highlight processes of moral slide, organizational pressures, and institutional incentives that normalize misconduct.Reference Feldman110 Incorporating these perspectives suggests that effective anti-bribery regimes must grapple not only with external enforcement and deterrence but also with the internal cultures and behavioral dynamics that sustain corruption.
Our findings reiterate existing calls for more proactive monitoring and audit mechanisms.Reference Peltier-Rivest111 Beyond enforcement of existing anti-bribery frameworks, alternative structural reforms could also lower incentives for corruption. These include reducing the dependence of regulators on industry financing, expanding public or independent funding mechanisms for clinical trials, and adopting centralized procurement models that minimize opportunities for side payments. Transparency reforms, such as mandatory disclosure of all industry payments to health care providers, and enhanced international cooperation on cross-border bribery, may also address the systemic vulnerabilities identified in this study. Improving transparency through the use of advances in data analytics, AI-driven risk detection, and automated financial tracking could also assist with earlier identification of suspicious payment patterns. At the same time, comprehensive legal protections for whistleblowers are needed, as many corruption cases come to light through internal reports, and fear of retaliation can deter these disclosures.Reference Vian112
From a public health perspective, the impact of bribery extends well beyond financial penalties and corporate reputations. Illicit payments that influence prescribing decisions, regulatory approvals, or procurement contracts can distort health care priorities.113 They divert resources toward suboptimal drug choices, inflated costs, or unnecessary treatments.114 Such distortions erode public confidence in health care institutions and can negatively affect patient outcomes when decisions are driven by financial incentives rather than medical need.115 Strengthening policies related to conflicts of interest, mandatory disclosure of payments to health care professionals, and closer surveillance of prescribing trends could help mitigate these negative impacts.
VII. Limitations
Despite these insights, this study has important limitations that likely understate the true scale of corruption. OECD Working Group on Bribery reports capture only those cases made public through official investigations, although the information contained within them is important. Companies not listed on major exchanges or operating in countries with less rigorous enforcement, alongside settlements sealed by confidentiality agreements, may escape scrutiny. Additionally, enforcement vigor across jurisdictions is heterogeneous. Bribery schemes in some regions might remain undisclosed or insufficiently prosecuted.116 These gaps create a “dark figure” of corruption that is never formally documented.117 Future research could integrate data from additional sources such as court filings, media reports, and whistleblower disclosures to develop a more complete understanding of bribery patterns.118 Comparative studies at the national or regional level could also examine how local governance structures and corporate practices influence bribery, which may help inform more effective policy responses.
Conclusion
Through an examination of OECD Phase Reports, this paper identifies and characterizes patterns of bribery in the global pharmaceutical sector. In doing so, this analysis advances empirical understandings of systemic corruption in pharmaceutical markets by quantifying data surrounding bribery in the industry. Our research builds upon and extends three key scholarly conversations. First, by providing measurable evidence that 74% of investigated pharmaceutical firms utilized subsidiaries specifically to circumvent internal controls with bribery schemes persisting for an average of 4.74 years. These findings lend empirical support to the existing literature arguing the entrenchment of regulatory gaps in the pharmaceutical sector. Second, the financial penalties imposed on pharmaceutical companies (totaling US$1.1 billion in sanctions) confirms corruption as institutionalized within the industry. Finally, the analysis of concealment tactics advances our understandings on the complexity of corruption within the pharmaceutical sector and the difficulties surrounding its identification.
In characterizing the cases of bribery identified in the Phase Reports, this study demonstrates the valuable information documented in these reports. Future research should engage with individuals from the OECD Working Group on Bribery, regulatory officials, pharmaceutical industry representatives, and civil society actors to provide further insight into how and why these identified cases of bribery occurred, but also into their resolution and the efficacy of the ongoing monitoring done by the OECD Working Group.
Research and meaningful action on corruption and bribery in the pharmaceutical sector is pressing as global health systems face unprecedented and unstable times in international cooperation and development. In demonstrating and characterizing the prevalence of bribery in the pharmaceutical sector among OECD cases, we emphasize the need for accountability, transparency, and anti-corruption mechanisms tailored to regional needs. Such mechanisms are needed to better prevent, identify, and respond to cases of bribery in the pharmaceutical sector, thereby reducing inefficiencies and increasing access to high-quality pharmaceutical care globally.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/jme.2026.10237.
Acknowledgements
The authors would like to thank Professor Marc Rodwin for his helpful comments and edits on this manuscript. Thanks also to Christopher Adanty for his excellent research assistance. Thanks to Charlotte Zhang for her help with formatting and reference checks. This manuscript was supported by the University of Toronto PERA fund.
Disclosures
The authors have nothing to disclose.



 Open access
Open access