

Sexual harassment in medicine is a common, global problem hiding in plain sight. (Reference Fnais, Al-Nasser and Zamakhshary1–Reference Ranganathan, Wamoyi, Pearson and Stöckl3) It is difficult to detect, measure and eradicate, (Reference Vargas, Brassel, Cortina, Settles, Johnson and Jagsi4; Reference Benya, Widnall and Johnson5) partly because there is a complex web of medical organisations involved in managing the doctors involved. Multiple organisations are responsible for responding to harassment, but individual policies and processes are often opaque, complex and partial. (Reference Stone, Phillips and Douglas6) Survivors describe reporting mechanisms that are difficult to navigate, and many survivors experience considerable harm arising from the reporting process. (Reference Stone, Phillips and Douglas6; Reference Bond, Clarke, Adcock and Steele7) Few feel there was significant benefit to reporting sexual harm. (Reference Stone, Douglas, Mitchell and Raphael8)
The United Nations Chief Executives Board, in its report on victim-centred approaches to sexual harassment, discusses the importance of giving victim-survivors choice and agency. The report suggests ‘engaging with a victim/survivor in a way that respects their rights, needs, wishes and dignity, protects them from retaliation, re-traumatization and discrimination, keeps them informed, and supported’. It emphasises the importance of respect for the victim’s/survivor’s dignity, focusing on empowering the survivors, and therefore enabling them to choose the way they respond to abuse. (9)
Survivors may have one or more goals when managing harassment. Some will seek justice, wanting to expose the perpetrator’s behaviour and hold them publicly accountable for their misconduct. Others will want to ensure colleagues are safe from the perpetrator’s behaviour and will be keen to ensure they protect more vulnerable colleagues in the future. Some will simply want a chance to heal. Although some countries, including Australia, emphasise the positive duty to report, this approach fails to recognise the impact of reporting to survivors, and does not recognise the importance of choice for survivors trying to regain confidence and a sense of agency.
Structure
In this part, we examine the multiple disciplines involved in the prevention and management of sexual harassment and describe common dilemmas faced by the organisations tasked with managing harassment in the medical workplace. Every organisation has strengths and capacities, but they also have limitations in their ability to manage sexual harassment. In this part, we have asked experts to analyse the problem from within their discipline, and describe the strengths and limitations of their organisational approach.
In the first chapter, Searle examines the psychological evidence behind sexual harassment, and abuse and discusses some of the dilemmas. While sexual harassment clearly causes harms to employees and clients, exposing sexual harassment can cause reputational damage and reduce trust in the organisation. There is also evidence that the reporting process can be highly traumatic for survivors. The perpetrator is likely to be more senior than the survivor, and may well be a high-profile asset for the organisation. The survivor is likely to be a more junior and more temporary employee with less notional value to the workplace. This power differential makes management particularly difficult, as the perpetrator may not be easy to replace. There is also a fine balance needed between openness and transparency, protecting the survivor from re-traumatisation and victimisation when their name becomes known in association with the harassment.
The chapter on law examines some of the barriers to justice and fairness in legal systems. As a barrister, Freckelton brings his detailed understanding of the cultural and structural barriers to reporting through legal channels. He uses three case studies from Australia to illustrate the challenges of reporting sexual harm through criminal and civil courts and tribunals, recognising how the system itself causes harm to survivors. He describes how legal processes may fail, so that despite the personal and professional risks a complainant endures, the outcome may not prevent future harm, or deter the perpetrator from future misconduct.
Ringin presents her work on human rights organisations, discussing their achievements and limitations. Although human rights frameworks have led to standard setting across the world, they offer little to an individual in terms of timely redress. However, the value of human rights work lies in collective advocacy. Common data, language and criteria enable grassroots organisations to agitate for collective rights at a local and national level. Over time, human rights principles can drive changes in legislation, so that workers can be protected under law.
Health professionals, including doctors, are in a unique position because they may be accountable to a medical regulator as well as to local legislation. Medical regulators exist to set and maintain professional standards, so that the public are protected from health professionals who demonstrate practice that puts the public at risk. With sexual harassment, there are different regulatory standards around the world, and in chapter 13, Reid uses her leadership of the International Association of Medical Regulatory Authorities (IAMRA) to highlight the common key processes of medical regulation agencies internationally and the significant differences between them. Medical regulators hold an important role in disciplining practitioners whose behaviour does not explicitly meet the legal threshold required for consideration in local courts. However, the differences between agencies and jurisdictions can mean it is difficult for a survivor to clearly understand and utilise these processes effectively.
Chapter 14, on medical education, highlights several major limitations for survivors who are still doctors in training. The steep professional hierarchy and the blurring of roles in teaching and supervision mean learners may be very dependent on their senior colleagues for career progression. This means that doctors in training may be reluctant to report sexual harassment due to concerns about the impact on their careers. In addition, workplace-based learning means doctors in training may be managed under two distinct policy frameworks: one at the workplace and one with the institution who oversees their learning. This can mean that survivors may have difficulty understanding their options when attempting to report abuse. They may also choose to avoid reporting simply because they move between teams relatively rapidly, and so may choose to endure the abuse and ‘move on’ rather than begin a lengthy reporting process that will last longer than their placement. Finally, the chapter explores the challenges of identifying, remediating, and, if necessary, removing doctors in training from the profession.
Hastings-Truelove and Flynn outline some of the challenges faced by doctors when they seek therapy. Apart from the obvious blurring of boundaries when seeking therapy inside a community that causes harm, there are defence mechanisms used by doctors that can impede the ability of survivors to seek and engage in therapy at all. In this chapter, the authors explore strategies to encourage survivors to seek care, and to overcome the stigma and shame that often accompanies trauma.
Finally, Roberts and Ahluwalia use their experience in the UK to explore how each of these disciplines can be integrated to ensure that survivors are able to access care showing how organisations can draw on multidisciplinary approaches to prevention and management. This chapter discusses an integrated and holistic approach to preventing, responding to and managing sexual abuse of doctors, focusing on organisational as well as individual factors. Using a case study, they explore how different organisations can work together to achieve better outcomes in prevention and management.
Introduction
A recent comparative work-psychology-based study of UK health professionals’ fitness to practise revealed two important results. (Reference Searle, Rice, McConnell and Dawson1) First, despite differences in the relative numbers of registrants, there were striking similarities between the misconducts of doctors, nurses, and allied health professionals. Second, despite divergence in registrant numbers, one type of malpractice – sexual misconduct – emerges more frequently from male doctors relative to other professionals. Indeed, no cases were found among women doctors, nor amongst midwives. Findings confirm earlier studies with incidents being more frequent in specialties including obstetrics and gynaecology, psychiatry and family medicine. In this chapter I draw on social cognitive theory (Reference Bandura2; Reference Bandura3) to consider three inter-related factors (behavioural, person, and the environment) and then review research evidence of how they contribute to the creation and sustainment of sexual violence for this profession. Through this approach, distinct personal, social and environmental influences are identified that would enable better detection, amelioration and prevention of sexual misconduct in medicine. I start by arguing that this form of misconduct is distinct, especially in the health context and specifically this profession. I use the term ‘sexual misconduct’ to underline behaviours that are at odds with what is expected of professionals, and I deliberately use the terms ‘targets’ and ‘perpetrators’ to discuss these incidents, thereby aiming to shift attention away from victimhood and its notions of passivity and helplessness. I note that there is as yet no satisfactory term to refer to those who are on the receiving end of these actions.
Sexual Misconduct Matters to Some Professions More Than Others
Research into counterproductive work behaviours (e.g. Reference Robinson and Bennett4–Reference Spector, Fox, Penney, Bruursema, Goh and Kessler5) has distinguished different forms of transgression. Critically, taxonomies separate interpersonally focused deviance from that which is directed at the organization, for example sexual harassment versus expenses fraud. The former is a far more severe transgression, because it violates social norms. (Reference Robinson and Bennett4) Sexual misconduct can be considered one of the most transgressive, interpersonally directed forms of counterproductive work behaviour due to its explicit, immoral, sexually aggressive content. (e.g. Reference Bowes-Sperry, Tata, Luthar, Sagie, Stashevsky and Koslowsky6–Reference Pina and Gannon10) It endures as one of the most pervasive forms of interpersonal violence against women. (Reference Fitzgerald11)
Sexual misconduct by a professional is a significant concern – in health and social care it can be a violation not only of professional standards but also of significant organizational requirements, endangering patients and service-users, with consequences for the wellbeing of other employees. (Reference Searle and Rice12) As I outline, sexualized contexts can be a symptom of a stressful workplace, with such relationships a means to access resources. They create distinct workplace dynamics between staff members that blur important boundaries between work and personal lives. More widely, such behaviours can damage public trust in employing institutions and regulators.
Until recently, sexual misconduct incidents have been viewed in isolation. However, following prolific sexual abuse cases, including those connected to the Catholic Church and to the UK’s prolific serial abuser Jimmy Savile, who used his status to access people in hospitals and the BBC, more insidious concerns have arisen: these abuses occurred in a health context, and show the exploitation of organizational weaknesses by perpetrators for their own nefarious ends. (Reference Bandura13) Further, the wilful obscuring of events by institutions betrays those who have been targeted. (Reference Heffernan14) The #MeToo movement has galvanized targets to come forward and share their experiences. (Reference Hershcovis, Vranjes, Berdahl and Cortina15) The scale of these reports renders obsolete the simple scapegoating of individuals; instead, it raises more pressing and uncomfortable questions about complex social environments and their roles in enabling and facilitating such incidents. Extending the perspective from a straightforward perpetrator–target dyad clarifies the adverse consequences for witnesses and others. (Reference Cesario16) Instead, it draws attention to the various social networks and complex environments that are critical in the creation, perpetuation, and even exacerbation of sexual violence by virtue of developing, sharing, accepting, and acquiescing to deviant values, norms, and behavioural models. (Reference Bandura13)
In the context of the medical profession, this misconduct can be regarded as far more significant and therefore likely to have more important consequences for targets. First, doctors are exhorted on entering the profession (e.g. the Hippocratic Oath) to behave with humanity and compassion. It is also enshrined in codes of conduct (17). Sexual misconduct inflicts harm on others, (Reference O’Leary-Kelly and Bowes-Sperry18) and therefore stands in direct opposition to the expected behaviour of a professional. Second, the role of physician elevates the individual’s social status, (Reference Bandura13) making that person a powerful authority figure in most societies. As it is non-consensual, sexual misconduct is a far more profound violation of trust, argued to be akin in form and impact to a parent’s abuse of a child. (Reference Galletly19) Finally, through perceptions about the training they have received, doctors have elevated presumptive trust: patients and the public assume those in this role are trustworthy. (Reference Kramer20) Indeed, prior idealized notions of professions have helped obscure their misconduct, making others reluctant to believe the claims of targets. (Reference Clements, Dawson and das Nair21)
Given the high status of perpetrators, and the trust that is placed in them, their targets’ initial responses and capacity to raise concerns are likely to challenge the status quo. A typical response to sexual assault is shame (Reference Bhuptani, Messman-Moore, O’Donohue and Schewe22) Targets also experience short-term freezing and withdrawal coping responses, which can be misinterpreted by perpetrators as acquiescence, thus prolonging the abuse. (Reference Fitzgerald, Drasgow, Hulin, Gelfand and Magley23) Targets’ responses can further compound their sense of shame (Reference Smirles24) and feeling that they are somehow responsible, with recent #MeToo cases exposing the fallacy of enduring rape myths regarding targets’ silence. (Reference Hershcovis, Vranjes, Berdahl and Cortina15) Yet these erroneous views persist, and are accepted more by men, (Reference Diehl, Rees and Bohner25) especially those with similar sexual aggressive behaviours. (Reference Diehl, Glaser and Bohner26) Where the target is a trainee, silence arises from fear of significant detrimental career consequences if they complain. (Reference Stone, Phillips and Douglas27) Indeed, a common tactic of perpetrators is to discredit the target with powerful others to whom the target has less access. (Reference Scott and Martin28) Therefore, a high-status perpetrator, such as a male physician, can benefit from the significant skew to their power relative to their target. We will now consider the three co-related factors of social cognitive theory. (Reference Bandura2)
Key co-determinants of transgressive behaviours.

Behavioural Factors
Sexual misconduct includes ‘unwelcome sexual advances, requests for sexual favours, and other verbal or physical conduct of a sexual nature’. When directed at co-workers it ‘unreasonably interferes with an individual’s work performance, or creates an intimidating, hostile, or offensive work environment’. (Reference Pina, Gannon and Saunders29) Further, as such misconduct includes non-consensual and coercive behaviour, it can be covert, with perpetrators deliberately secretive in their actions, leading to diverging accounts between the parties and no means of independent verification. (Reference McDonald30) The opacity of these events and the lack of independent verification can make those informed be reluctant to take further action. (Reference Bandura13)
Sexual misconduct can be separated, distinguishing aggressive from sexualised actions, (Reference Larsen, Nye and Fitzgerald31) with the former more typical in gender harassment (i.e. unwanted conduct related to an individual’s sex or the sex of another person, rather than unwanted conduct of a sexual nature), (Reference Larsen, Nye and Fitzgerald31; Reference O’Leary-Kelly, M, Bowes-Sperry, Bates and Lean8) and is often associated with rejection. (Reference Stockdale, Gruber and Morgan32) Critically, sexual misconduct is a goal-directed behaviour, often occurring concurrently with other forms of interpersonal violence. (Reference O’Leary-Kelly, Paetzold and Griffin33) Extant research suggests three drivers for this response. First, it is a means of dissipating negative affective responses that arise from prior adverse experiences, which perpetuates a cycle of aggression. (Reference Berkowitz34) Adverse experiences are common in the medical profession, with negative emotions elicited from caring for patients, or working in resource-constrained and time-pressed contexts. (Reference Kumar35)
The second driver is retributive, responding to perceived injustices by punishing those deemed responsible. (Reference O’Leary-Kelly, Paetzold and Griffin33) Prior study shows both men and women punish women for being ‘uppity’, meaning they deviated from feminine ideals towards more masculine characteristics including assertiveness, independence, and dominance. (Reference Berdahl36) Similar agression is also shown towards men who deviate from traditional masculine stereotypes. Retaliation against women is more marked in previously male-dominated professions, where they are considered as taking ‘men’s jobs’. (Reference Willness, Steel and Lee37) Such behaviours are deployed to maintain unequal and female-hostile social workplace hierarchies (Reference Page and Pina9; Reference McDonald30; Reference Berdahl38).
Self-presentation is the final motivation, supporting the perpetrator’s desired social image (the ‘big man’), (Reference O’Leary-Kelly, Paetzold and Griffin33) protecting or enhancing a sex-based status. (Reference Berdahl38) This can include more instrumental personal sexual gratification. (Reference Pina, Gannon and Saunders29)
Research shows discernible differences in perpetrators’ various goal choices, highlighting the severity, type, duration, and frequency of incidents and their targets. (Reference Lucero, Allen and Middleton39) For example, some perpetrators focus on a few targets for more persistent abuse, while opportunists are characterized by their wider range of targets and incidents. In contrast, ‘harassers’ denotes repetitive and stable behaviours, which can escalate in severity, becoming more prolific; critically, in these cases sanctions are less effective. (Reference Lucero, Allen and Middleton39)
A study has examined health professionals’ misconduct and identified strong predictive and recidivist patterns to the sexual misconduct behaviour of doctors. (Reference Spittal, Bismark and Studdert40) The research highlights an important and perplexing failure of prior sanctions. Social cognitive theory has also identified four mechanisms that individuals use to allow them to morally disengage from their transgressive activities and still maintain a positive self-image. (Reference Bandura41) Indeed, working in a morally praiseworthy profession can leave doctors more vulnerable to other cognitive distortions, including moral licensing, (Reference Klotz and Bolino42) where these good deeds can provide a moral credit to off-set against their immoral actions. (Reference Griep, Germeys and Kraak43) As a result, medical doctors may be more vulnerable than other professions from falling prey to such perverse cognitions. Research on sexual perpetrators has identified particular use of moral disengagement strategies, including blaming targets for their own deviance, especially amongst those with traditional sex-role beliefs (Reference Jensen and Gutek44) and sexist attitudes. (Reference De Judicibus and McCabe45) Recent study of sexual misconduct that included medical doctors showed greater incidence of these tactics when compared to other health professionals – notably, denying that any incident had occurred or injury had been caused, and implying a dehumanized target was responsible. (Reference Berdahl, Raver and Zedeck46) Further, those in the profession were less likely to try and displace responsibility onto others, probably in recognition of their more senior work roles.
Critically, engaging in this behaviour affects environments, which in turn alters perpetrators’ behaviour. (Reference Bandura13) Prior study has identified important personal and organizational influences regarding these behaviours. (Reference Fitzgerald, Drasgow, Hulin, Gelfand and Magley23)
Personal Factors
Interpersonal factors are important in determining how individuals perceive their environments, and how they behave. (Reference Bandura13) They include biological and intrapsychic influences, such as competencies, belief systems, self-conceptions, emotional states, goals, attitudes, and values.
An important recurring demographic for sexual misconduct is gender, it largely, but not exclusively, being committed by men, typically those with sexist attitudes (Reference Berdahl, Raver and Zedeck46). Disbelief from professionals about female perpetrators, however, contributes to exacerbating its adverse consequences for targets. (Reference Clements, Dawson and das Nair21) Studies show both men and women can target those they perceive as transgressing traditional gendered roles. Targets include senior ‘uppity’ women, and men in previously female-dominated occupations. (Reference Berdahl36, Reference Berdahl38, Reference Kabat-Farr and Cortina47) However, the consequences of sexual misconduct have been argued to be less severe for male targets. (Reference Waldo, Berdahl and Fitzgerald49) Such relative arguments are always problematic as such events have long-lasting impacts. Similar target demographics were found in a recent UK study of health professionals’ sexual misconduct, revealing offending medical doctors to be exclusively male, and more frequent targeting of vulnerable women, critically younger and lower seniority, and also those with mental-health concerns. (Reference Berdahl, Raver and Zedeck47) These targets are in line with Scott and Martin’s (Reference Scott and Martin28) arguments about cynical targeting of naïve and unreliable witnesses.
Research on the nexus of behaviour and personal factors reveals important differences in the interpretation of social interactions, with men more likely to misconstrue women’s behaviour as being ‘more than simply friendly’, regardless of the women’s status or responses. (Reference Johnson, Stockdale and Saal50) Further personal determinants of perpetrators include their sexual attraction to targets, as well as particular personality traits, notably their strong need for control and power. A study shows that men with low levels of agreeableness and high hostile sexism can use sexual violence as retaliation for perceived earlier interactional organizational injustices. (Reference Krings and Facchin51) Similar reactions were found in men with low subjective power and influence who were promoted, exploiting their new status to rectify prior injustices, especially by targeting female co-workers who had thwarted their earlier sexual advances. (Reference O’Donohue, Downs and Yeater52; Reference Williams, Gruenfeld and Guillory53) These retaliatory reactions show the role of prior situational triggers for some men.
Environmental Factors
Environments are important in motivating and regulating transgressive behaviours, (Reference Bandura13) positioning individuals as meshed in socially situated causal structures, rather than as autonomous moral agents.
Critically, sexual misconduct is sustained by being culturally embedded, as shown by pervasive sexist attitudes and beliefs across most societies, (Reference Russell and Oswald55) and their maintenance within institutions. (Reference Fitzgerald11) As a result, targets are predominantly women, particularly those with lower socioeconomic and hierarchical status in a workplace. Women’s economic precarity and lower status can exacerbate their vulnerability to become targets, in that their economic dependence on their jobs reduces their capacity to complain, or to be believed in the face of higher status males (Reference O’Leary-Kelly, M, Bowes-Sperry, Bates and Lean8; Reference McDonald30; Reference Easteal and Judd56).
Bandura (Reference Bandura13) distinguishes three ways in which individuals impact environments. First, in imposed environments, individuals have limited control over the physical and psycho-cultural aspects that impinge on and constrain them. Goffman (Reference Goffman54) has noted how these institutional forces also affect patients and service users. Individuals can vary their understanding of, and responses to, such constraints. Second, selected environments offer individuals far greater latitude, including choice of profession, that offers more fine-grained means to shape working environments, select departments and even shifts, or to access a variety of contexts through locum working. Might this be a factor in explaining why there are different distributions of these behaviours across distinct specialties? The selection of an environment offers professionals greater opportunities and levels of oversight. Finally, as perpetrators gain power they have further means to more nefariously shape places, creating environments, in order to advance their misconduct. Over time, these deliberate behaviours alter the local workplace climate and wider cultures to facilitate their malfeasance. These climates quickly form, with facilities where employees live-in further insulating them from alternative views. Through micro-social-engineering, important and facilitatory social networks can be forged to support evolving deviant activity patterns. The permissive norms that develop are integral to facilitating sexual harassment climates, (Reference Pina and Gannon10) and the resultant environments are central to enabling those with chronic predispositions to harass to act on their proclivities. (Reference Page and Pina57)
Extant study shows more sexual misconduct occurs in workplaces without a corrective influence of professionalism, with limited employee knowledge of complaint procedures, and where there are pervasive sexist attitudes. (Reference O’Hare and O’Donohue58) In workplaces where there is a sex-based hierarchy, sexist attitudes can become entrenched. (Reference Willness, Steel and Lee37) Cultures with high levels of competition and gendered power relations, and where informal networks are significant, can facilitate sexual misconduct. (Reference Hennekam and Bennett59) Reporting of concerns often involves contacting human resources, who have less power and status in health care organization, making it difficult to challenge senior clinicians with high status (e.g. surgeons).
Aside from facilitating misconduct, environments can also be important in inhibiting transgressive behaviours (Reference Bandura13) (see figure 10.2). First, individuals are crucial to self-regulation, restraining actions that violate their own standards of behaviour – even if these activities are unlikely to be noticed by others. Inhibition stems from moral values, motivating individuals to avoid the resultant guilt, remorse, and self-criticism that would arise from a transgressive act. However, working in a profession of ‘good deeds’ can provide moral credits that can off-set immorality. (Reference Griep, Germeys and Kraak43) Self-control is a finite resource which can be eroded by ongoing efforts. (Reference Baumeister, Bratslavsky, Muraven and Tice60) Research indicates higher instances of impulsive sexual behaviour by those with low self-control of overall traits, and where recent events have depleted the strength of their self-control, diminishing their capacity to stifle sexual thoughts and resist temptation. (Reference Gailliot and Baumeister61)
Co-determinants and sanctions that inhibit transgressive behaviours.
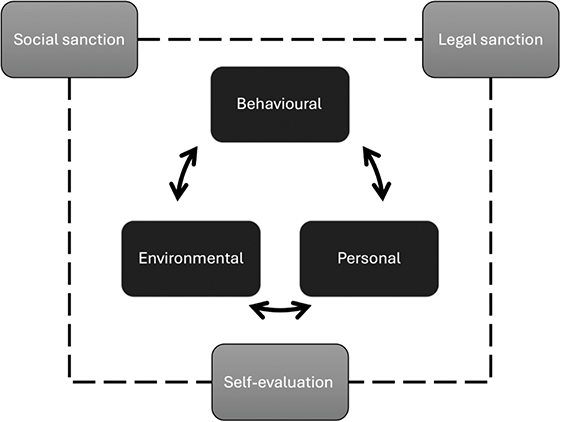
Individuals’ self-regulatory capability can be undermined by environmental factors, critically by stress associated with either their roles or managing uncertainty. (Reference Fox, Spector and Miles62) However, studies reveal men’s capacity to inhibit transgressive tendencies is more affected by stress than women’s ability to do likewise. (Reference Spector and Zhou63) This capacity is also affected by emotions, with a nurse-based study of less serious deviant conduct showing how anger- or anxiety-inducing events caused a temporary moral disengagement. (Reference Fida, Paciello, Tramontano, Fontaine, Barbaranelli and Farnese64) The study found such events ‘compromise’ workers’ capacity to be aware of others, and their adverse responses diminished their means to self-sanction. Strikingly, one response to stressful workplaces can be to seek protection from a more senior person, which proliferates more sexualized climates. (Reference Berdahl and Aquino65) In these workplaces, boundaries between individuals can become confused, making them less safe places for patients as well. A second and distinct source of inhibition is formal regulator sanctions, (Reference Bandura13) externally imposed by regulation of health professions and national legislation. Workplaces also have their own specific formal policies and practices.
Notably, in the context of this form of misconduct, inhibitory capability appears eroded. First, despite being illegal within most societies, sexual violence is growing at least in part due to low reporting and conviction levels. (Reference Fitzgerald11) Second, detailed comparative study of UK health professionals’ sexual misconduct shows doctors are less likely to be permanently suspended, even where there are repeated incidents. (Reference Berdahl, Raver and Zedeck47) This may lead some within this profession to perceive that serious sanctions are less likely. Reducing the fear of perceived sanction reduces their effectiveness, and may be a factor contributing to the recidivism found for sexual misconduct. (Reference Spittal, Bismark and Studdert40) Finally, different professions working in the same contexts are regulated applying different standards and sanctions to their actions, with serious case reviews raising concerns about the divergence of processes and resultant sanctions. (Reference Hodson66; Reference Peng and Zeng67) However, sanction ambiguity for sexual perpetrators can lead them to downplay the risk to them of sanctions, using a variety of moral disengagement mechanisms to distance themselves from their actions. (Reference Berdahl, Raver and Zedeck47) Bandura (Reference Bandura13) contends that ambiguity, coupled with a lack of societal engagement in tackling this form of interpersonal violence, reduced the inhibitory impact of sanctions.
Finally, social sanction is also fear-based. (Reference Bandura13) However, perpetrators can choose workplaces with enabling, rather than inhibiting, social networks. (Reference Bandura13) Prior study of sexual misconduct reveals how social sanctions can be subtly undermined, through pervasive sexist work attitudes, the erosion of professionalism, and curtailing knowledge of the complaint procedures. (Reference O’Hare and O’Donohue58) Male perpetrators of sexual violence often garner sympathy rather than censorship. (Reference Bagenal and Baxter68) The cultural embedding of sexist attitudes within societies restricts the impact of social sanctions. Further, research shows the efficacy of social norms varies; critically for this profession, fear of being socially ostracized is more acute for those with lower self-efficacy, (Reference Peng and Zeng69) and sanctions are rarely directed at those with high job performance. (Reference Quade, Greenbaum and Petrenko70) Therefore, elites who are delivering are not impacted, especially those regarded as doing important work. (Reference Bagenal and Baxter68) More lenient standards are also applied to those who are regarded as being otherwise morally praiseworthy, rather than understanding that these positive actions provide the psychological means for them to appease their immorality. (Reference Griep, Germeys and Kraak43)
Through the more insidious efforts of perpetrators to select and create environments, social objections can be undermined. For example, the fostering of uncertainty about what constitutes sexual misconduct can make bystanders reluctant to intervene. (Reference Bennett, Banyard and Garnhart71) Although they might feel some responsibility to support and protect vulnerable others, (Reference Hershcovis, Neville, Reich, Christie, Cortina and Shan72) their lack of confidence about formal reporting procedures (Reference Hershcovis, Parker and Reich73) and cynicism about their organization’s tackling of sexual harassment, along with unethical local climates, combine to suppress reporting. (Reference Cheung, Goldberg, King and Magley74) In contrast, training that helps to establish clear boundaries between acceptable and deviant conduct can make bystanders more certain about how to act. (Reference Searle, Rice, McConnell and Dawson1; Reference Lee, Hanson and Cheung75)
By selecting and micro-social-engineering choices about where and with whom to take breaks or extra-curricular activities, important divergent group norms are formed, (Reference Pina and Gannon10) and perpetrators can strategically diminish the level of social sanctions they might receive. (Reference Scott and Martin28) Yet research shows how incidents reported by colleagues are among those receiving the highest sanctions. (Reference Spittal, Studdert, Paterson and Bismark75)
Leaders are critical as powerful role models to others, with their actions enhancing others’ agency to respond to and challenge incivility. (Reference Hershcovis, Neville, Reich, Christie, Cortina and Shan72) Medical doctors are often stalwarts of their communities, especially if they are more conservative rural locations, leaving individuals reluctant to raise suspicions. (Reference Spittal, Bismark and Studdert40; Reference Spittal, Bismark and Studdert76) However, leaders can also undermine social sanctions through the use of moral disengagement to reframe and diminish others’ transgressions. (Reference Dang, Umphress and Mitchell78) Indeed, in stressful workplaces sexualized environments often emerge, with senior staff (majority male) exploiting the ‘protection’ they offer lower-level employers though the use of favours and rewards. (Reference Berdahl and Aquino65) Through establishing more sexualized climates, awareness and concerns about apparently consensual sexual behaviour of co-workers become blurred, making colleagues reluctant to intervene or challenge. (Reference Aquino, Sheppard, Watkins, O’Reilly and Smith79) A further, innocuous veneer can be added to these antics by using humour to deflect attention away from the deleterious work and wellbeing consequences of sexual misconduct; (Reference Berdahl and Aquino65) in addition, others’ moral disengagement is facilitated by removing the actions’ moral dimensions in order to reconstruct them as benign. (Reference Page, Pina and Giner-Sorolla80) Or doing so through moral credits that allows perpetrators to be positioned as morally praiseworthy. (Reference Griep, Germeys and Kraak43) Norms inform ethical behavioural choices and comprise both macro (national culture) and micro (peer) influences. (Reference Westerman, Beekun, Stedham and Yamamura81) They extend to include norms that tacitly support, facilitating misconduct by their silence. (Reference Hershcovis, Vranjes, Berdahl and Cortina15) Paradoxically, instead of reducing local workplace deviance, fear of social sanctions is used against those who are not involved. (Reference Jahanzeb and Fatima82) In these ways perpetrators mould contexts that facilitate their proclivities, encouraging others to think they can do likewise, and further stifling the voices of those with concerns. (Reference Hershcovis, Vranjes, Berdahl and Cortina15)
Examining specific evidence regarding sexual harassment in a health context confirms that despite the establishment of oaths and professionals’ ethical training, these workplaces continue to report incidents of misconduct. (Reference Locke and Hicks83–Reference Nielsen, Kjær, Aldrich, Madsen, Friborg, Rugulies and Folker85) Further, study of medical specialties indicates some critical professions with raised levels of misconduct, specifically family medicine, obstetrics/gynaecology, and psychiatry. (Reference Sansone and Sansone86) Similar professions were indicated in a UK study, pointing to workplace hotspots, including: hospitals; GP surgeries and other private consulting spaces; and those with vulnerable service-users such as care homes, mental-health providers, and institutions for young people. (Reference Searle, Rice, McConnell and Dawson1) Further attention is required to understand why it is more pervasive in particular professions, whether this attracts distinct types of individuals, and the working context. Research profiling risks has identified elevation among doctors working in rural workplaces. (Reference Spittal, Bismark and Studdert76) Co-workers in these locations might have more pervasive traditional sexist attitudes, (Reference Berdahl38) combined with greater reverence for doctors that provides perpetrators with secluded consulting rooms, unchallenged opportunities to undertake intimate examinations, and access to vulnerable patients in communities that can be shamed into silence.
There is a more pervasive cultural embedding of sexual misconduct, with females working in health targeted not only by male professionals, (Reference Berdahl, Raver and Zedeck47) but also by patients. (Reference Phillips and Schneider87; Reference Gabay and Shafran Tikva88) The consequences of these harmful experiences can be exacerbated by line managers who fail to recognize and treat the incidents as serious staff assaults, adding further stress, which can culminate in professionals’ decisions to quit. Responses, including keeping a list of perpetrators who should not be sent female trainees, actively contribute to a culture of abuse, with 91% of women doctors in a recent survey reporting experiencing sexism, yet only 48% feeling it could be reported. (Reference Bagenal and Baxter68)
A study that has matched sexual misconduct events in health care to their wider workplace climate reveals these environments are likely to erode self-regulation resources, through pervasive incivility and violence. (Reference Searle, Rice, McConnell and Dawson1) There are clear associations between these incidents and workplaces with long working hours (self-regulation), high levels of interpersonal violence from both staff and service-users, and poor quality of communication between staff and management. In contrast, workplaces with lower incidents of misconduct had taken steps to clarify boundaries and procedures through high levels of diversity and inclusion training.
There is growing evidence of the relevance of a socio-cognitive framing of professionals’ misconduct, with an Australian comparative health professions study creating predictive risk scores by combining personal details (sex, age), behaviours (number of prior complaints and cause for complaint), and selected environment (profession and specialty). (Reference Spittal, Bismark and Studdert40) Critically, it showed risk profiles for doctors and dentists were highly predictive, identifying troubling repeating behavioural patterns, including for sexual misconduct. These suggest areas where sanctions might be less effective. However, a meta-analytic criminal justice study of sexual harassers highlights that those at greatest risk are the least likely to complete treatment programmes. (Reference Olver, Stockdale and Wormith89) In synthesizing these studies, important personal and environmental facets are revealed which could be used to both screen out individuals from some or all medical careers, and to enhance efforts upstream to identify potential hotspots and ensure all staff are clear about sexual misconduct behaviours and how to report their concerns. While this patently remains a widespread societal issue, #MeToo scandals have raised awareness of the social and institutional factors that are implicit in these incidents. This chapter argues this misconduct is both conceptually and empirically more likely to be undertaken by male doctors. Given the marked recidivist trajectories for this transgressive behaviour, rather than reduced sanctions, educators, regulators and employers should establish higher standards to protect their female workforce and patients, especially in delivering family medicine, as well as mental and female health services. Greater attention should be paid to how workplaces may deplete individuals’ capability to self-regulate, recognising that the content of the work, the associated emotions, and working in resource-depleted organisations can adversely affect individuals’ behaviours. Since social and workplace factors can transform proclivities into misconduct, we need a multi-strand approach to seriously tackle these incidents.
Introduction
A number of legal consequences can follow when a medical practitioner behaves in a non-consensually sexualised way towards a junior doctor or a medical student in or involving the workplace. Such conduct can result in the institution of criminal prosecution for indecent assault, battery, or rape. (Reference Wood1) It can also have the consequence in some jurisdictions of a civil action for damages for either sexual harassment or assault. (Reference Rabin2) Action can be taken by the employer to remove the person from their employment, (Reference Male3; Reference Wood1) although there are occasions when such actions have been contested in the courts after a hospital has terminated a doctor’s employment, (Reference Buist4) and action can be taken by the health regulator to remove the practitioner’s registration or impose conditions upon it. (Reference Wood1) There is also the potential for the person who is the subject of a complaint to take retributive measures for defamation against a complainant. (Reference Doolittle5) In addition, there are instances where an employing institution comes to know of a medical practitioner’s predatory propensities. (Reference Bensimon and Woods6; Reference Nundy, Desiraju and Nagral7) If it can be proved that an employer was aware of the risks of an employee engaging in such conduct, by reason of prior behaviour or information to which the employer is otherwise privy, there is the potential for occupational health and safety litigation to be commenced against an employer, such as a hospital, for failing to provide a safe workplace.
This chapter explores the structural and other impediments to reporting of sexual assaults or harassment by doctors upon other health practitioners, particularly upon junior doctors.
Non-Reporting in the Criminal Context
Reporting by women of a variety of forms of sexual assaults committed against them is low. (Reference Rennison8) A Latin American study, for instance, estimated that only 5% of adult victims of sexual violence reported incidents to the police. (Reference JM, Bott, Guedes and Dartnall9) While figures vary internationally, the overwhelming majority of such assaults are not communicated to investigating or prosecuting authorities, and while young women and those from ethnic minorities, including First Nations women, are at particular risk of sexual assault, (10) they report comparatively rarely. Males also experience a high level of hesitation to report sexual assaults, (Reference JM and AE.11–Reference Riccardi16) although there has been a suggestion that males do not experience as many adverse emotional sequelae from sexual harassment and are hesitant to categorise it as such. (Reference AH, Scholcoff, JL, Nickoloff, KE and Jackson17)
Much is known and can be learned from other contexts about the reasons for diffidence on the part of victims to report sex crimes to police and prosecutorial authorities. There are many different forms of fear that can inhibit such reporting. Among these, there is a fear of the investigative process and of court procedures; a fear of retaliation from the offender and persons associated with the offender; a fear of not being believed; and a fear of being blamed, as well as self-blame, embarrassment, shock and denial. (Reference Belden18–Reference Ceelen, Dorn and UJL.20) A culture of self-sacrifice in medicine runs the risk of normalising inappropriate behaviours in the workplace to a point where harassment can come to be considered ‘part of the job’. (Reference Stone21) Cultural considerations which affect preparedness to make a report of assault can also be highly relevant. (Reference MR, Danis, DL and Gallagher22) There can be concerns too on the part of victims about the consequences of a report of sexual assault for perpetrators whose standing in the community they do not wish to imperil. (Reference MR, Danis, DL and Gallagher22)
Accusing perpetrators can have a range of adverse economic consequences for victims (Reference Allen23) should they fail to be renewed in their workplace contract or if they are assessed as unsuitable for an ongoing position. A 2021 Australian study also suggested that women must meet unrealistic expectations and engage with doubt and suspicion when they make a complaint, whereas accused mens’ actions in gaining consent to their conduct are not scrutinised as rigorously. (Reference Minter, Carlisle and Coumarelos24) Put another way, there can be complex balances between victims’ needs and expectations and those of others, (Reference Hansen, Stefansen and Skilbrei25) which can militate against reporting of sexual improprieties.
In addition, there is a further noxious element to the reporting experience – when complainants are not believed, including by police, they can experience deleterious health consequences. For instance, a Canadian study, using open-ended and semi-structured interviews with twenty-three sexual assault survivors, who were sexually assaulted but not believed by police, found a number of negative health outcomes for survivors. (Reference McQueen, Murphy-Oikonen, Miller and Chambers26) These included broken expectations which resulted in loss of trust and secondary victimisation, loss of self, and cumulative health and social effects. There can also be alienation from the workplace, shame, the emotional effects of being ostracised, depression and suicidality.
Reporting Sexual Assault and Harassment in the Workplace
Sexual harassment in the workplace generally is persistent, prevalent and under-reported to authorities. (Reference MacDermott27; 28) A component of this can be a perception of futility in making a report, which can play a role in maintaining or even deepening a ‘culture of silence’. (Reference Rabin29) A series of significant studies has been published on the issue. In 2016, for instance, the Trade Union Council (30) in the United Kingdom issued a report, ‘Still Just a Bit of Banter?’, which concluded that approximately 52% of women suffered sexual harassment in the workplace (including nearly a quarter who had experienced unwanted touching and a fifth who had experienced unwanted sexual advances) and identifying that 80% of them did not report it. The problems complained about were mostly from male colleagues, and nearly one-in-five victims stated that their direct manager or someone else with direct authority over them was the perpetrator.
The BBC released two polls in October and November 2017; they found that 53% of women and 20% of men (37% overall) said they had experienced sexual harassment at work or a place of study, and one in ten of the women who had been harassed said they had been sexually assaulted; the second poll concluded that 40% of women and 18% of men had been sexually harassed at work, 9% in the previous year alone. Importantly, of the women who said they had been harassed, 63% said they did not report it to anyone, and 79% of male victims did not report it. (31)
More recently, a 2022 investigation by UN Women UK found that 97% of women aged 10–24 have been sexually harassed, and 96% have not made a report because of a belief that it would not change anything. (32) Of course, much depends upon definitions, as well as subjective experiences. However, it is apparent that the norm is for sexual assaults and harassment not to be reported – the dark figure of its incidence is difficult to identify, with most light on the phenomenon being shed by anonymous surveys. To a similar effect, high levels of sexual harassment have been reported among junior doctors in the United Kingdom (Reference CT, Arshad and Cuming33; 34) and in the United States (34; Reference EM, AL and Pereira-Lima35) including among resident physicians, particularly by self-report surveys. (Reference EM, AL and Pereira-Lima35–Reference Gavin38)
When sexual assault or harassment occurs in a workplace, there are additional considerations which can deter victims from reporting. First, there are the complexities of workplace dynamics and concerns that may be experienced about ongoing vocational viability if a complaint of harassment is lodged about a colleague and, especially, about a superior. (Reference Kadota39) Most harassment targets do not report their experience (Reference LF, SL and Bailey40–Reference ME, LM, LM and Palieri44) out of a fear, with justification, that they will experience deleterious consequences in their career and ostracism and even retribution from fellow-workers and management. This is exacerbated if the person who is the subject of the complaint is organisationally powerful or senior in status to the complainant. (Reference ME, LM, LM and Palieri44) Put another way, the power imbalance in the unwanted sexual conduct can provide strong reasons not to report what has occurred. In the aftermath of the Caroline Tan case in Australia (see below), the surgeon, Dr Gabrielle McMullin, observed that Dr Tan’s career had been ruined by the successful sexual harassment litigation that she initiated (see below) and that ‘realistically’ she would have been better off giving her supervisor ‘a blow job’. (Reference Medew45)
There can be worries, too, about stigma and victim-blaming (Reference Bongiorno, Langbroek and Ryan46) which discourage people from disclosing sexual harassment in the workplace and perceptions that it is pointless to initiate a complaints process because it will not be assertively pursued or is unlikely to result in constructive changes to safety in the workplace. Kadota (Reference Kadota39) has related being discounted as an ‘emotional female’ when she raised concerns about conditions for doctors and about sexual harassment in the workplace in relation to junior doctors. Too often there is little by way of support from colleagues and other medical practitioners (47; Reference Stone, Phillips and Douglas48). Issues of confidentiality can also loom large in a workplace where leakage of information about a complaint can result in a variety of adverse consequences from colleagues.
The next sections of this chapter deal with experiences of medical practitioners who have reported sexual impropriety by other medical practitioners. The case examples selected for discussion are provided because of their being illustrative of different issues affecting the preparedness of medical practitioners to report diverse forms of sexual conduct engaged in towards them by other medical practitioners. The discussion of each is based upon publicly available information.
The Dr Xenos Litigation
Dr Caroline Tan was a registrar in her third year of training in neurosurgery in 2004 at the Monash Medical Centre, in Melbourne, Australia. (49) Dr Chris Xenos was a senior neurosurgeon who worked principally in private consulting rooms but also for part of the week at the Monash Medical Centre.
From about December 2004 Dr Tan developed a supportive professional relationship with Dr Xenos and from time to time discussed her professional progress with him. From January 2005 Dr Xenos invited Dr Tan to his private rooms adjacent to the hospital for what he proposed as extra tuition. She declined these requests as they were made for times that were not convenient to her but in due course stated that at that stage she did not perceive them as other than professionally motivated. However, on 15 February 2005 she accepted an invitation from Dr Xenos to meet him at his rooms so he could review some neurosurgery topics with her as part of her training. She arrived in the early evening and, after small talk about artwork on the walls, he led her into his room by the hand and, when she turned her back to look at material on his desk, he suddenly approached her from behind, spun her around and embraced her. He kissed her on the lips, put his hand on her breast, pinning her against the desk, and as she twisted around to get out of his grasp, she saw his erect penis out of his zipper. He explicitly propositioned her but she escaped his grasp, blurted out ‘how could you’ and ran out of the premises to her car. She maintained that Dr Xenos followed her and suggested he drive her home. She declined his offer and drove away on her own.
Dr Tan asserted that she was distraught after the incident and spent the night crying. However, she ‘decided not to make any complaint to her employer as she was concerned that it would be her word against that of a senior and respected consultant in the very area in which she was working’. (49) Further, she was conscious that Dr Xenos was involved in her training assessment and she did not want to be seen as a troublemaker: she ‘thought that her accreditation as a neurosurgeon, and her future career, might well suffer if she made a complaint’. (49) She claimed that Dr Xenos went about his usual work in the following days and pretended that nothing had happened. She tried to confront him about the incident but he told her that she needed to ‘move on’ and it was clear to her that he was going to pretend the incident had not taken place. She was deeply embarrassed about what had occurred, felt in a quandary about what to do and, although at first she decided not to make an official complaint, felt profoundly affected in her capacity to work in the same environment as Dr Xenos. She did make private complaints to others. However, ultimately she took civil action alleging that Dr Xenos engaged in sexual harassment towards her in the course of her employment in contravention of section 87 of the Equal Opportunity Act 1985 (Commonwealth). The case was assertively contested by Dr Xenos. It was heard by Judge Harbison of the Victorian Civil and Administrative Tribunal.
During the Tribunal hearing Dr Tan was extensively cross-examined about the incident. She was unable to give any evidence about the physical characteristics of Dr Xenos’ penis that she claimed she had seen. Dr Xenos gave sworn evidence that the incident never took place. He said that he had fallen into a pattern of giving private tutorials to Dr Tan because she had declined to participate in tutorials with another doctor. He called extensive evidence about his good character, suggesting that it was unlikely that he would have engaged in conduct of the kind alleged by Dr Tan.
Judge Harbison confirmed that the burden of proof for the allegations lay upon the person making them, Dr Tan. She found Dr Tan to be impressive in her veracity and consistency of accounts but also found Dr Xenos largely to present in an impressive manner. Judge Harbison observed that she was ‘very much aware that there is little that a person, wrongfully accused of sexual harassment can do in his own defence except to emphatically deny that the event took place’. (49) She commented that there were no witnesses who could corroborate the accounts of either Dr Tan or Dr Xenos and stated that were she faced with two equally compelling versions of events by the two parties, Dr Tan’s case would have to fail.
Evidence was adduced, though, that Dr Tan complained to others and that she did so before she received an unsatisfactory assessment of her performance. Judge Harbison described Dr Tan’s complaint evidence as striking in its extent and to be interlocking. (49) Dr Xenos sought to portray Dr Tan’s allegations as motivated by malcontent with her assessment and contended that she would ‘escape rejection by a tirade of complaints about standards of teaching, and personal complaints against other medical staff’ from an early juncture in her studies. (49) Ultimately, Judge Harbison found Dr Tan’s evidence as to the incident of harassment to be credible and that the evidence adduced by Dr Xenos about her poor work performance prior to her making the complaint not to be supported by documentary evidence. Thus, her Honour rejected the argument mounted by Dr Xenos that Dr Tan’s motive in making her harassment complaint was one of disappointment at the adverse evaluation of her performance. Rather, Judge Harbison found that the conversations that took place by Dr Tan with others were consistent with her ‘finding more and more difficulty with her work as a result of her emotional reaction to the incident of harassment, but not being prepared to make a formal complaint of harassment, or acknowledge her difficulty in coping as a result, because of her position as a trainee’. (49)
Judge Harbison found Dr Xenos to have ‘deliberately exaggerated the timeframe during which [Dr Tan] demonstrated substandard work, to make it more closely fit his suggestion that she had fabricated her claim’. (49) Judge Harbison observed that Dr Tan had endured cross-examination that was far-ranging and repetitive: ‘Throughout it her evidence remained consistent and credible. She remained courteous, even when asked the same question many times over. She showed extraordinary poise and composure under pressure.’ (49)
At first Dr Tan had simply sought an apology as a remedy in her sexual discrimination action but withdrew this application during the process of submissions after the conclusion of evidence on the basis of how assertively the case had been fought by Dr Xenos and the fact that any apology ordered by Judge Harbison would not be genuinely given. (49) Judge Harbison concurred, expressing the view that in a sexual harassment case the ordering of an apology should only be done rarely. She preferred to make an order for damages. However, she noted that there was no evidence to support an award of special damages or loss of earnings. By the time of the hearing Dr Tan had concluded her qualifications as a neurosurgeon and, while her period of training had been delayed, there was no evidence that that was because of the conduct of Dr Xenos.
In assessing the damages that she should award in favour of Dr Tan, Judge Harbison observed that Dr Tan had been ‘terribly affected by the incident. I even venture to say that her reaction has been unusually severe and, to some extent, out of proportion with the incident itself. She has reacted to it as a gross violation of her body and her trust.’ (49) She took into account that Dr Xenos was in a position of power over Dr Tan and that he knew her performance had previously been under a cloud, rendering her especially vulnerable to Dr Xenos’ overtures. She found that Dr Xenos ‘deliberately and falsely denied the harassment’, attempting to smear the character of Dr Tan, exploring every aspect of her professional competence in a context in which neurosurgery is a speciality in Australia with only approximately 150 practitioners. A consequence is that the great majority of Australian neurosurgeons would know of Dr Tan’s case and therefore that Dr Tan’s ‘enjoyment of her profession … will now be significantly tarnished by the sexual harassment which I have found proved’. (49) Dr Tan failed her final assessment and thus had not yet become fully qualified as a neurologist. Judge Harbison awarded her AUD100,000 in damages. (49)
However, in important respects, aside from establishing an important precedent, Dr Tan’s win proved to be a pyrrhic victory. In due course she completed her qualifications but by 2015 her experience was that she had been shunned by other surgeons who had repeatedly overlooked her in applications that she made for positions in both public and private hospitals. Dr Xenos, by contrast, remained in employment at Monash Health although he was warned that any further misconduct would have serious consequences for him, and he was not permitted to continue supervising trainees. As of 2015 Dr Tan was disillusioned and stated that she would have been better off if she had submitted to Dr Xenos’ harassment. She denounced the Australasian College of Surgeons as an ‘Anglo-Saxon old boys club’ that favoured men (Reference Medew45) and drew little comfort from her litigation success.
Dr Tan’s case illustrates many of the internationally recognised phenomena about the consequences of a junior doctor making a complaint about sexual harassment or discrimination against a senior colleague. Her case before the Victorian Civil and Administrative Tribunal extended for eight days and was keenly contested, with every aspect of Dr Tan’s performance as a trainee being scrutinised and denigrated by the senior practitioner who, ultimately, was found to have sexually harassed Dr Tan. The whole experience was extremely high profile and, while, Dr Tan was financially successful, an outcome was that her entry into the profession was delayed, and she suffered the outcome experienced by most whistleblowers (Reference Freckelton50) in that she was marginalised in her profession and found it extremely difficult to secure employment as a specialist doctor.
The Kaye Litigation
A high profile and deeply troubling case involving a senior medical practitioner in Victoria, Australia, came before that state’s medical disciplinary tribunal, the Victorian Civil and Administrative Tribunal (VCAT) in 2025. (56) It involved an allegation brought by the Medical Board of Australia that one of Australia’s most highly regarded neurosurgeons, a ‘world-renowned figure’, Professor Andrew Kaye, had engaged in unwanted sexual conduct towards a young female medical practitioner, an unaccredited neurosurgery registrar (Dr A), whom he supervised. The allegation was that in the context of having pressured her to drink whisky in his rooms, knowing she had to return to the operating theatre, he touched her in a sexualised way and thereby breached professional boundaries. (56)
Professor Kaye was a graduate of the University of Melbourne in 1973 and was appointed Professor of Neurosurgery at the University in 1992 and the James Stewart Professor of Surgery and Head of the Department of Surgery at the Royal Melbourne Hospital in 1997. Subsequently, he chaired the Board of Examiners for the final year of Medicine at the Faculty of Medicine, Dentistry and Health Sciences at the University of Melbourne for many years and was also appointed in 2010 by the New Zealand Government to Chair the Board of the New Zealand South Island Neurosurgery Service. He is the author of a leading neurosurgery textbook (Reference Kaye60) and many leading scholarly articles.
The allegations brought by the Medical Board of Australia related to Professor Kaye’s interactions with the registrar during 2019. The registrar alleged that Professor Kaye asked her in the days leading up the incident whether she was married and told her that she was ‘a remarkable person’. (56) She described arrangements that he made to release her from other work commitments and a requirement from him that she come to his office and drink whisky with him, in the course of which she detailed that he made unwanted sexual overtures towards her, sitting beside her on his couch with his office door closed.
Professor Kaye assertively disputed almost all aspects of the Board’s allegations and maintained that they were made after he chastised the registrar for coming to work wearing a backpack, and his having spoken to a nurse expressing concern about the registrar’s having worn face-piercing jewellery to surgery. However, he accepted that he did drink whisky alone with her in a closed office, which he characterised as unwise in retrospect. Thus, his concession was as to imprudent behaviour on his part in leaving himself exposed to false allegations, but no more than that. His senior counsel accused the young practitioner of fabricating multiple aspects of her accounts and cross-examined her at some length in this regard. However, she adhered to her accusations in relation to Professor Kaye’s conduct. On the issue of his credibility, the Tribunal commented in relation to his knowledge of the registrar’s having consumed whisky with him that: ‘it is almost unthinkable for someone of Dr Kaye’s eminence and high standards to not take some action, for example, directing Dr A not to return to surgery, chastising her at a later time and/or reporting her to the hospital. Dr Kaye’s failure to take any action is inconsistent with the events occurring as he states.’ (56)
In 2019/2020 (after the incident) Professor Kaye left his role at the Royal Melbourne Hospital and his directorship of the prominent Hawthorn Football Club. He emigrated to Israel, with his wife, surrendering his Australian registration (56), and became the Hadassah Medical Organization’s Director of Neurosurgery Resident Training, stating that: ‘I wanted to contribute to Israel, and I felt guilty that I had not done it earlier.’ On his departure, the former Victorian Premier, Jeff Kennett, communicated to Hawthorn’s members and supporters appreciation for Professor Kaye’s service, describing him as ‘perhaps Australia’s leading neurosurgeon, with huge leadership responsibilities’.
Ultimately, when the matter was resolved in 2025, the registrar’s account was accepted by VCAT and Professor Kaye was disbelieved on his oath. The Tribunal commented that: ‘people process trauma in different ways and it is not necessarily the case that Dr A would remember every detail of the events.’ (56) Professor Kaye was found to have exerted pressures on the registrar and in relation to the sexualised overtures that he made towards her. It observed that ‘in the context of Dr Kaye being an eminent and influential neurosurgeon, … Dr A felt pressured to drink the whisky and did drink the whisky’. (56) It accepted that he asked her a series of questions about her family and personal life, inviting her in the confines of his office to call him by his first name. The Tribunal found that Dr Kaye made physical contact with the junior doctor on a series of occasions and was in contact with her by personal text messages, which was conduct that was uncharacteristic of his normal behaviour. It expressed ‘comfortable satisfaction’ that Professor Kaye failed to maintain professional boundaries in inviting the junior doctor to his office for a non-clinical or non-academic purpose and that she felt pressures to drink the whisky he offered her. Similarly, it was comfortably satisfied that he:
placed his right hand on Dr A’s left leg and hands; attempted to stroke Dr A’s hands; and touched Dr A’s arm, left thigh, hip, back and bottom. This conduct was in the context of Dr Kaye sitting close to Dr A on the couch in his office with the door closed, suggesting to Dr A that she call him Andrew rather than Prof while they were in the office, and occurred immediately after Dr Kaye said to Dr A, in reference to the wall of another building immediately outside his office window, ‘… I prefer it that way, because it’s private and no one can see inside’. Dr Kaye’s demeanor to Dr A had changed the previous day when he discovered Dr A’s interest and knowledge of whisky. He had immediately become more friendly to her and commenced sending personal text messages to Dr A. (56)
Thus, it rejected Dr Kaye’s accounts generally, finding key parts of his answers to be internally inconsistent and also inconsistent with other evidence. It rejected his assertion that any physical contact he had with the registrar was accidental and non-sexual in intent. It concluded that Professor Kaye failed to maintain professional boundaries in that he engaged in uninvited conduct of a sexual nature towards his registrar. (56: at [164])
There have been few more internationally eminent specialist medical practitioners in Australia than Professor Kaye. The degree to which his stature and position in the medical profession and also within the general community must have been intimidating for the young neurosurgery registrar at the time of his misconduct and in the course of the hearing before VCAT cannot be understated. Notably, through very experienced senior counsel, he sought to impugn all aspects of the registrar’s credibility and reliability. Nonetheless, it is apparent that the Tribunal engaged in a close analysis of the evidence and found the registrar, albeit ‘softly spoken and ‘somewhat nervous’, to be ‘honest and credible’ in her evidence, (56) while Professor Kaye was not.
The Kearsley Litigation
Another outcome that can follow as a matter of law from sexual harassment of a junior doctor, a registrar, by a more senior practitioner is the preferring of criminal charges. It was this that occurred in relation to Dr John Kearsley, who, at the time of the commission of criminal offences against a junior doctor, was a Professor and Director of Radiation Oncology at the Cancer Care Centre at St George Hospital in Sydney, New South Wales, in Australia. He was aged sixty. He pleaded guilty to administering an intoxicating substance, Lorazepam, a benzodiazepine, to enable him to assault the Registrar indecently at a private dinner at his apartment after which he perpetrated a further indecent assault. The victim was a Fellow of the Royal Australian and New Zealand College of Radiologists and a registrar at Liverpool Hospital on secondment from St George Hospital. At the relevant time she was subject to supervision by Dr Kearsley. She informed him that she had failed her Fellowship examinations, and he invited her for dinner. The offending took place in the course of the dinner which took place to enable discussions about her career.
Initially Dr Kearsley denied the Registrar’s allegations but ultimately pleaded guilty to the two charges in the District Court of New South Wales (51). Judge Hock noted that Dr Kearsley stated that he was very apologetic to the Registrar and expressed shock and disbelief at the suggestion that he had touched her inappropriately, asserting that his conduct was inconsistent with everything that he believed in: ‘He explained that he had been under significant pressure and had experienced alcohol blackouts and would undertake treatment to deal with his problem. He was devastated that he had put her in this predicament and offered any third party assistance he could give her, including counselling and mediation with health professionals for both of them.’ (51)
A victim impact statement was tendered to the District Court, explaining that the Registrar suffered ‘constant intrusive thoughts and questions about why I was chosen to be the victim of such a despicable crime’. She said that she had experienced adverse consequences for her mental health from what had occurred – she had been robbed of her confidence and self-worth and had been treated for two years for post-traumatic stress disorder. Somewhat surprisingly, Judge Hock stated that she was not satisfied that Dr Kearsley’s offending was premeditated. She received a large volume of testimonials on behalf of Dr Kearsley, reports from forensic psychiatrists which suggested that at the relevant time Dr Kearsley was suffering from a major depressive disorder, and an apology from Dr Kearsley. A psychiatrist commissioned by the prosecution expressed the view that Dr Kearsley had an adjustment disorder with depressed and anxious mood and an alcohol-use disorder at the time of committing the offences. Judge Hock accepted that Dr Kearsley’s intoxication and psychiatric conditions at the time of the offences provided a context for his conduct, although they did not excuse it, and that there was only a tenuous link between his psychiatric conditions and his putting a drug in the registrar’s drink and his sexually assaulting her. She accepted that Dr Kearsley was genuinely remorseful and unlikely to reoffend. She sentenced Dr Kearsley to an aggregate sentence of imprisonment of four years and three months’ imprisonment with a non-parole period of two years and three months.
However, Dr Kearsley appealed his sentence to the New South Wales Court of Criminal Appeal. (52) He was successful. The court resentenced Mr Kearsley, taking into account that by that stage he had ‘lost his profession and position of good standing in the community and has been the subject of adverse media publicity. This has had a detrimental effect upon his mental health.’ (52) The Court of Criminal Appeal found that the sentencing judge had erred in failing to address explicitly in her reasons the objective gravity of the offence, which in respect of the drugging was ‘moderate’ and in respect of the indecent assault was ‘low to moderate’. The Court did not regard the principles of general deterrence as of particular significance in the case by reason of Dr Kearsley’s psychiatric conditions but that his ‘subjective case’ was very strong. (52) The Court did note that the offences were aggravated by the relationship between Dr Kearsley and the registrar ‘generated by his position as a senior medical practitioner and her position as a junior medical practitioner seeking his professional guidance’. (52) The outcome was that Dr Kearsley’s appeal was allowed, and he was resentenced to a reduced term of eighteen months’ imprisonment, with an immediate release, and his entering into a good behaviour bond for the balance of his sentence.
The fact that sexual impropriety is rarely a one-off form of conduct (Reference Rimmer53) was illustrated by Dr Kearsley. He was later convicted of indecently assaulting the daughter of an elderly prostate cancer patient. His modus operandi was familiar. He invited the victim to lunch at his office at St George Hospital, including giving her champagne, and then took her for a tour of the facilities. During the tour, he said: ‘Your mother died of breast cancer didn’t she?’ and then offered to give her an impromptu breast examination. She agreed but he then proceeded to touch her naked breasts inappropriately and to squeeze her nipples. On this occasion he received a wholly non-custodial sentence. The magistrate ordered Dr Kearsley to carry out 340 hours of community service. (Reference Ford54)
A number of issues emerge from the Kearsley case where Dr Kearsley’s victim was a medical practitioner. Although there was a manifestly predatory component to the conduct of the practitioner, and he occupied a supervisory role over his victim, a registrar, the appellate criminal court reduced his jail sentence as a result of taking into account the seriousness of his conduct and the fact that the perpetrator was able to assemble an impressive body of good character evidence and evidence from mental health professionals that he was unlikely to re-offend. Although he was later convicted a second time of sexual assault on the relative of a patient, he came before the court dealing with his indecent assault on the registrar as a person with no prior convictions and the sentence of imprisonment that he received was significantly reduced. Given the conduct in which he engaged, whether the sentence ultimately imposed was such as to acknowledge the egregious breach of trust involved in his criminal conduct and is such as to deter others minded to behave in a similar way is open to grave question.
The Handsjuk Litigation
Dr AB, a general practitioner, was referred to Dr Handsjuk, a psychiatrist, for treatment for symptoms of social anxiety, low self-esteem, disordered eating and depression. (55) She was treated by him for some fifteen years. The question placed before the Victorian Civil and Administrative Tribunal by the Medical Board of Australia was whether it was proved on the balance of probabilities that between approximately 1998 and 2003 Dr Handsjuk had engaged in professional misconduct in the form of intimate physical contact and/or sexualised conduct with Dr AB. After a four-day hearing, much of which involved Dr AB being rigorously cross-examined, the Tribunal concluded that Dr Handsjuk had no case to answer.
Dr AB provided extensive detail of many of her allegations but said that there were limits to what she could recall given how frequently the intimate contact took place between her and her psychiatrist. In explaining the delay in her lodging a formal notification against her psychiatrist, Dr AB said it took a long time for her to realise how devastating and damaging the interaction with Dr Handsjuk had been for her and until she became strong enough to report the conduct.
Ultimately, the Tribunal found that Dr AB had misconstrued objective facts (55) and took into account that at no time did Dr AB accuse Dr Handsjuk of sexual impropriety in her written communications with him, although she did verbalise a range of other aggrievements. The Tribunal found that Dr AB’s credibility was frequently undermined and observed that ‘Serious allegations with career and reputation ending repercussions require precise evidence which can survive careful scrutiny’. (55)
Thus the outcome was that Dr AB was disbelieved on her oath and the Tribunal was not satisfied that Dr Handsjuk engaged in the professional misconduct alleged against him by Dr AB. A few weeks after the Tribunal handed down its decision, Dr AB committed suicide.
The case involving Dr AB as a complainant illustrates the vulnerability of many medical practitioner complainants when they make serious allegations against professional colleagues and how difficult it is for many of them to make the hard decision to report such conduct to the investigative authorities. In addition, the interaction between the psychiatric pathology that motivates them to seek therapeutic assistance in the first place renders a medical practitioner who is a patient of another doctor very vulnerable. It can intersect in a complex way with the therapy with which they are provided, whether that therapy be orthodox or iconoclastic, proper or predatory. These considerations make resolution of complaints of sexual impropriety by a practitioner who is the alleged assailant’s patient particularly complex and sensitive. However, for the complainant (as well as the practitioner accused of professional misconduct) the proceedings are extremely stressful.
Conclusion
This chapter has identified a range of considerations that tend to dissuade most persons who are the victims of sexual assault or sexual harassment from reporting what has happened to them and from initiating litigation – whether it be criminal, civil or disciplinary. However, although sexual assaults and harassment tend to be recidivist forms of behaviour, when the victim is a medical practitioner and it is another doctor who has been responsible for the conduct, additional considerations at a structural level tend to deter reporting. There is the fear about how the report will be dealt with in the workplace – in particular, whether there will be a rigorous and fair investigation – and whether embarrassing details will seep out or be leaked by the person who is the subject of the complaint. Structurally, most victims are junior doctors and most perpetrators are senior practitioners who are highly valued by the establishment, often a hospital. This imbalance of power is very confronting for most victims and, save if there is independent corroboration of what has taken place, raises challenging issues of proof, and requires determination and great courage on the part of the victim.
Junior doctors also fear reprisals and secondary victimisation from the institution and, more particularly, the perpetrator and persons associated with them. In addition, becoming known as a ‘complainant’ tends to be an adverse step in terms of employability, as shown by the experience of Dr Tan, who was successful in her sexual harassment claim but unable to secure the employment she aspired to in the aftermath of the litigation that she initiated and in which her allegations were accepted as well-founded. In addition, perpetrators who are senior in their profession often fight accusations very determinedly (not unusually with the de facto support of their institution and colleagues) and impugn many aspects of junior doctors’ assessments, achievements and conduct, turning the focus of decision-makers onto the victim, away from the perpetrator. Dr Tan’s case, as well as the case involving Professor Kaye, exemplify this.
Too often the ultimate sanction imposed on a senior practitioner is relatively benign, because highly paid legal representation can muster arguments that denigrate the complainant, as occurred with Professor Kaye, and suggest there were mitigating factors for what occurred, emphasising the high regard in which the perpetrator is held, and assembling multiple testimonials as to their good character. This is not generally an option for the victim. Dr Kearsley’s case is exemplary of these dynamics.
Finally, as shown by the Dr Handsjuk case, the experience of making any kind of a serious complaint by a doctor who is another practitioner’s patient is extraordinarily stressful and can be perceived as stigmatising and deeply confronting, especially for a practitioner who has ‘gone out on a limb’, given sworn evidence and been rigorously cross-examined. If the complaint is ultimately not believed, and frequently complainants are fearful that their account will not be accepted as against the account of a senior practitioner, who is much valued by an institution, the impact upon the complainant can be devastating. Psychiatric vulnerability for a complainant, because of pre-existing pathology or because of the sequelae from assaults or harassment, can be highly counter-therapeutic and may constitute a rational reason for a decision not to report unethical sexualised conduct.
Thus, there are many practical impediments to doctors who are other practitioners’ patients junior doctors and medical students disclosing sexual assaults and harassment in the workplace. It is important for investigation of such matters to be efficient, independent and professional, and it is fundamental that processes should be set in place to do as much as can be done to avoid secondary victimisation of a complainant. It is vital that complainants be afforded as much practical and psychological support as possible, too, during and in the aftermath of the legal and complaints processes. However, the ‘real world’ experience of whistleblowers tends to be that there are multiple and enduring adverse consequences to becoming a complainant against professional colleagues. This phenomenon is not easily addressed, given the power disparities within institutions such as hospitals between medical students and junior doctors on the one hand and senior medical staff on the other. It is for this reason that potential complainants are often discouraged from proceeding with their complaints and that relatively few such cases proceed to a criminal, civil or disciplinary hearing.
Introduction
An occurrence of abuse, whether it be sexual, physical, emotional and/or psychological, between medical practitioners has immediate individual and collective impact. Providing adequate avenues for redress, as well as safeguarding workplaces and employment for practitioners, should be a priority in any instance where abuse has, or could, occur. The framework of human rights has the potential to add value to this endeavour. Having existed in many forms throughout history, human rights has developed into the commonly understood doctrine it is today and now permeates global discourse, featuring prominently in international, regional, and domestic laws and institutions.
Using the term ‘instrument’ to refer to various treaties, conventions, agencies, and institutions that operate within this framework, this chapter will begin with an examination of the core human rights instruments, the Universal Declaration of Human Rights, the International Covenant on Economic, Social and Cultural Rights and the International Covenant on Civil and Political Rights. It is from these instruments that the specific rights which are arguably contravened in the instance of abuse between medical practitioners, such as the right to life, liberty and the security of person, freedom from torture and the right to physical and mental health, are articulated. The chapter will then consider particular international, regional, and domestic instruments stemming from these core instruments and the processes through which a rights violation can be alleged.
Perusing the strengths and weaknesses of the framework, it will be asserted that while there are limitations for what the human rights framework can offer an individual in terms of redress, the benefits on a collective measure are much greater. The human rights framework provides a common language, standards and processes that are understood globally. This allows for collective agitation on domestic, regional, and international levels which can result in real and substantial change such as through the implementation of standardised complaints procedures, unambiguous legislation, comparable penalties, and multilateral treaties. Utilising this framework in parallel with other redress schemes, such as legal criminal action, is therefore suggested to ensure the needs and desires of the individual survivor, as well as the needs of other practitioners and the wider society, are adequately addressed.
What Are Human Rights?
Systems of law throughout history have consistently featured, as stated by Geoffrey Robertson KC, ‘the notion that individuals, wherever in the world they live, possess a few basic powers which no political order can remove’. (Reference Robertson1) From the Code of Hammurabi to Magna Carta, religious texts to the Rights of Man, individuals have been afforded protection from the sovereign State, as well as their fellow citizens, concerning some areas of life. (Reference Robertson2) The right to a fair and public hearing is arguably replicated from clause 40 of Magna Carta, ‘to no man will we sell, to no man will we deny or delay justice or right’, (Reference Robertson3) while the right to private property can arguably be seen in the religious commandment ‘thou shalt not steal’. (Reference Robertson4)
The level of importance and respect granted to such rights has expanded over time. First formulated in the negative sense, that which an individual or the State was not permitted to do to another individual, the modern understanding of rights is often framed in the positive sense, that which the State must action in order to fulfil. (Reference Robertson3) So too, what is recognised as a right has developed, with subjects previously considered to be privileges achieving rights status. These changes and fluctuations are clearly demonstrated in the experience of the last fifty years or so, with international human rights law transitioning from abstraction to a fully fledged area of law and expertise in its own right. (5)
This evolution of human rights has been accompanied by the debate around the universality of human rights. Are there rights that are automatically claimed by all individuals, and which cannot be abrogated? Are there rights that transcend culture, society, religion, and political structure? Human rights have been regularly criticised as a Western imperialistic notion that disregards the lived experiences of most of the global community. (Reference Mende6; Reference Ahdanisa and Rothman7) Proponents of human rights cite the commonality found in generally abhorred behaviours, such as murder, piracy and slavery, to bolster the argument in favour of universality. (Reference Shestack8) This debate has prompted the creation of four schools of thought on the matter: the natural scholars (rights as given), the deliberative scholars (rights as agreed upon), the protest scholars (rights as fought for) and the discourse scholars (rights as talked about). (Reference Dembour9)
This debate aside, it is inescapable that the human rights discourse has infiltrated the international, regional, and domestic spheres. Language concerning rights, and the subsequent protections that must be enacted to safeguard them, are prominent features of organisations, legislation, and treaties. (Reference Madigan10) Whether or not individuals, institutions and/or States agree with the applicability, or even existence of certain rights, they are forced to engage with the notion. This forced engagement provides a unique opportunity for individuals to articulate their grievances using language that is widely understood and familiar. Such a position is useful when approaching an issue such as the topic of this book.
A final comment on human rights is necessary in the context of abuse between medical practitioners. While it is acknowledged that survivors of such abuse are diverse and include cis-gender males, the overwhelming majority of survivors identify as women, a reality that cannot be ignored and is reflected in the language and focus of many of the instruments canvassed in this chapter. This should not be interpreted to mean that other gender identities should not be afforded similar protection, nor that they escape the abuse that is the topic of this book; rather, such a derogation reinforces the fact that those who identify as women have historically been, and continue to be, targeted at a detrimentally higher proportion than other identities. Nevertheless, as the frameworks offered by human rights instruments are predicated on an idea of equality regardless of gender, the use of this lens can still positively impact the experience of all individuals. It is asserted, therefore, that the human rights framework has the potential to provide redress for any survivors of abuse.
Overarching Human Rights Instruments
Perhaps the most well-known international document concerning the articulation of a body of rights is the Universal Declaration of Human Rights (the Declaration; UDHR). (Reference Res11) Established by the United Nations General Assembly Resolution 217 A on 10 December 1948, (12) the Declaration names thirty rights as those which are declared to be universal, such as the right to security and liberty, the right to education, and the right to freedom of thought.
In 1966, the United Nations General Assembly further espoused the doctrine of human rights by adopting two treaties that complemented the Declaration: The International Covenant on Economic, Social and Cultural Rights (ICESCR) (15) and the International Covenant on Civil and Political Rights (ICCPR) (12; Reference Res13). While some rights appear in all three instruments, this simply further demonstrates the fundamental importance of these rights in all spheres of human engagement. Together, these three instruments are considered the ‘International Bill of Human Rights’, establishing human rights law globally, and resulting in an additional eighteen international human rights treaties (12; 15). Table 12.1 outlines the rights identified from the International Bill of Human Rights which are those arguably involved in the instance of abuse between medical practitioners.
| INSTRUMENT | ARTICLE | RIGHT |
|---|---|---|
| UNIVERSAL DECLARATION OF HUMAN RIGHTS (UDHR) | 3 | Right to life, liberty, and the security of person |
| 5 | Freedom from torture or cruel, inhuman, or degrading treatment or punishment | |
| 6 | Right to recognition before the law | |
| 7 | Right to equality before the law | |
| 8 | Remedy through law for violation of rights | |
| 12 | Right to privacy | |
| 23 | Right to work | |
| 25 | Right to health and wellbeing | |
| INTERNATIONAL COVENANT ON CIVIL AND POLITICAL RIGHTS (ICCPR) | 7 | Freedom from torture or cruel, inhuman, or degrading treatment or punishment |
| 9 | Right to life, liberty, and the security of person | |
| 16 | Right to recognition before the law | |
| 17 | Right to privacy | |
| 26 | Right to equality before the law | |
| INTERNATIONAL COVENANT ON ECONOMIC, SOCIAL AND CULTURAL RIGHTS (ICESCR) | 6 | Right to work |
| 7 | Right to just and favourable conditions at work | |
| 12 | Right to health |
It is important to comment on a few of the rights in Table 12.1. The right to privacy enshrined in these instruments includes the right to judicial protection against attacks on privacy. Article 7(b) of the ICESCR specifically notes the right to safe and healthy working conditions, while article 12 includes both physical and mental health. Finally, the right to life, liberty, and security in article 3 of the UDHR is much broader than article 9 of the ICCPR, which relegates this right to detention situations.
Other International Instruments
Stemming from the UDHR, ICCPR and ICESCR are specialised instruments, such as treaty bodies, UN agencies and international agreements, that are tasked with managing and monitoring, in a more specific and nuanced manner, particular rights. Membership or ascension to these instruments often requires States to submit regular reports and allow compliance monitoring, from which invaluable data and statistics are gained. This information then provides the foundation for the formulation and development of global policies and procedures to instigate change. The following are those considered to be most applicable concerning the topic of this chapter.
Treaty Bodies
There are ten treaty bodies in operation with the focus of each being a particular treaty. (16) The Committee on the Elimination of Discrimination against Women (the Committee) oversees the implementation of the Convention on the Elimination of Discrimination against Women (CEDAW) (17; Reference Res18). Adopted by the United Nations General Assembly in December 1979, CEDAW calls on State parties to eliminate discrimination against women in all areas of life, ensure the development and advancement of women, and permit the Committee to scrutinise the compliance of the State through regular reporting and accounting. (19) CEDAW articles of interest include articles 2 and 5, which speak directly to the protection of women in the workforce. These articles require signatories to eliminate cultural or social patterns of conduct which affect women. In addition, article 11 calls for the protection of the workspace so that women can realise the right to protection of health and safety in working conditions. In addition to the primary document, CEDAW also has the Optional Protocol to the Convention, which permits individuals or groups to complain to the Committee directly and also allows the Committee to initiate inquiries into ‘grave or systematic violations of women’s rights’. (20) For these options to be actionable, the relevant State must have signed up to the Optional Protocol separately. At the moment, 189 States have ratified CEDAW, (20) with 115 States signed up to the Optional Protocol. (21)
Agencies
Specialised agencies of the United Nations operate to enhance certain rights. The International Labour Organization (ILO) is one such agency. Established in 1919 as part of the Treaty of Versailles at the end of the First World War, the ILO is the overarching global agency of the United Nations that unites governments, employers, and workers in programmes to ensure decent working conditions for everyone. (22; 23) The aims of the ILO, highlighted in the 1944 Declaration of Philadelphia, are to ensure that ‘all human beings, irrespective of race, creed or sex, have the right to pursue both their material well-being and their spiritual development in conditions of freedom and dignity, of economic security and equal opportunity’, as in article II, and that the ILO should aim to guarantee ‘adequate protection for the life and health of workers in all occupations’, as in article III(g) (24). The ILO itself has conceived other conventions, again concerning the rights of workers, such as the adoption in 1958 of the Discrimination (Employment and Occupation) Convention, aimed at removing discriminatory behaviours and practices in the workplace. Currently, the ILO has 187 member states, including States such as China, Russia, Iran, and the United States. (22)
UN Women is an entity created by the United Nations General Assembly in July 2010 to address the issue of gender equality and the empowerment of women. (25) A specific area of concern for UN Women is the economic empowerment of women. UN Women supports programmes and policies that encourage women into the workforce, but also highlights the multiple barriers that women face upon entrance. (25) Aligning with the ILO, CEDAW and the Beijing Declaration, UN Women emphasises the requirement of protections in the workplace for women in order to achieve their full potential.
International Agreements
Closely aligned with the aims of CEDAW is the international agreement the Beijing Declaration and Platform for Action. (26) This declaration was adopted at the Fourth World Conference on Women in September 1995, and nominated twelve areas that were deemed crucial in order to rectify the global state of inequality. (27) A topic of concern is the intersection of women and the economy, which highlights the need for women to have access to properly paid work in conjunction with safe and harassment-free workspaces. (27) The notable difference about this particular declaration was the accompanying Platform for Action, which set out clear actions that could be taken to achieve success. Concerning women and the economy, strategic objective F.6(180)(c) calls for governments and businesses ‘to enact and enforce laws against sexual and other forms of harassment in all workplaces’. (25) Since the adoption in 1995 by 189 States, the Beijing Declaration has been reviewed every five years with successes and failures duly noted. (27)
Asserting Rights through the International System
The human rights framework has multiple instruments aimed at protecting the rights of individuals; however, the practical steps which must be undertaken to make a complaint and therefore enforce these rights is complicated. In the international sphere, whether or not an instrument is binding on a State depends on its categorisation. For example, of the three overarching instruments, the ICCPR and the ICESCR are treaties, as opposed to the Declaration, which is not. The ICCPR and the ICESCR therefore provide a more solid avenue for recourse than the Declaration because when a State ratifies a treaty, they agree to be bound by its contents. Essentially, while the Declaration announces that which States can recognise, the ICCPR and ICESCR nominate that which States have to recognise post-ratification and places an obligation on the State to respect, protect and fulfil those rights. (28) The Beijing Declaration and the Platform for Action, along with UN Women, are as limited as the Declaration in regard to enforcement in this sense too.
There are some instruments that defy this trend. While the ILO is an agency, it has a complaints mechanism in its constitution and so does have the ability to receive and manage complaints. There are also additional complaint pathways, through the Human Rights Council and the Special Procedures Mechanism, which do not require ratification of a particular treaty to be accessed, although as demonstrated below, such avenues have their own practical limitations.
Treaty Bodies
Submitting an individual complaint to a treaty body requires treaty ratification and, as in the case of the treaties in this chapter, ratification of the Optional Protocol permitting individual complaints. Where to submit a complaint depends upon which treaty an individual is asserting their rights through: the Human Rights Committee receives individual complaints concerning the ICCPR; the Committee on Economic, Social and Cultural Rights receives complaints concerning the ICESCR; and the Committee on the Elimination of Discrimination against Women receives complaints concerning CEDAW.
For a complaint to be accepted by a treaty body, domestic avenues must have first been exhausted. (29) If accepted, the complaint process remains confidential until finalised, in which a report makes it public. (29) The complainant can request interim measures to protect the complainant against reprisal or harm while the complaint is being decided. (29) As the decision has the weight of a treaty behind it, the outcome is quasi-judicial and legally enforceable. (29) The decision takes on average two to three years to be handed down; however interim measures can be enacted within forty-eight hours. (29)
Human Rights Council
Submitting a complaint to the Human Rights Council can be made by an individual who is a national of a member State of the United Nations. (29) There are strict eligibility criteria, however, such as the complainant having exhausted all domestic options before the complaint can be accepted. (29) The complaint must be part of a consistent pattern of gross and reliably attested violations of human rights – a hurdle that may be impassable regarding the topic of this book. (29) The complaint remains confidential; however the process is long and a positive outcome for the complainant is in no way guaranteed. (29)
Special Procedures
Like the Human Rights Council, ratification by a State of a particular treaty is not needed for an individual to submit a complaint; the complainant just must be a national of a member State of the United Nations. (29) To submit to the Special Procedures mechanism, the complaint must be covered by a Special Procedures Mandate. (29) The mandate holder may then elect to accept the complaint or not. (29) If accepted, the complaint becomes public and is incorporated into one of three annual reports. (29) Response times can be as little as twenty-four hours; however, the process can be lengthy depending on the amount of detail received in the complaint. (29) There is no need for domestic remedies to be exhausted. However, as there is a gatekeeper to this process (the mandate holder), success is in no way guaranteed. (29)
Complaints to the International Labour Organization (ILO)
Sometimes the only way for a complaint to be made is by another member State. This is the process with the ILO, as outlined in articles 26 to 34 of the ILO Constitution. (30) Receipt of a complaint leads the ILO to determine whether or not a Commission of Inquiry should be instituted. (30) There have been fourteen Commissions of Inquiry in response to a total of sixty-seven complaints. (31)
Evaluating the International Human Rights Enforcement Capability
How useful are these processes to address the issue of abuse between medical practitioners? It is evident from the discussion above that there are numerous avenues through which a complaint could proceed. What is also evident is that the complaint process is complicated, is guarded by barriers and gatekeepers, and often, is used as a last resort. In the situation of the ILO, the individual ability to complain is non-existent. The process is also lengthy, requiring a complainant to endure potentially years of uncertainty, and in the end, publicity, in order to assert their rights.
The remedies available may also not be desired by an individual complainant. Treaty body decisions are final and cannot be appealed; however, the decision only contains recommendations on how the State should rectify the breach and is not a directive. (32) Should a breach be found and no action be taken by the State, the treaty body has no enforcement recourse; rather the case is simply left open until the treaty body is content that satisfactory actions have been taken. (32) In a similar vein, the mandate holder of the Special Procedure mechanism can only offer views or recommendations and has no enforcement potential. (33)
The Human Rights Council’s strongest option is to recommend that the High Commissioner for Human Rights provide technical cooperation, capacity-building assistance or advisory services to the State concerned. (34) Under the ILO, article 33 permits a member State to impose sanctions if the recommendations required by the Commission of Inquiry are not fulfilled. Parties to the complaint under the ILO also have the ability to refer the matter to the International Court of Justice (ICJ), under article 29, the decision of which is final. (Reference Thomann35) The practical implementation of an ICJ decision, however, still falls to the State in question and is unenforceable by the ICJ itself. (Reference Kuc36)
Another limitation of the international enforcement of human rights is that the rights enshrined in these documents are broad. Interpretation must therefore be undertaken to apply the right to the situation of the complaint, an interpretation which may not be shared by the decision maker. In this same manner, an individual may have to rely on a combination of rights and may need to research extensively the purpose and intent of drafters in order to successfully lodge their complaint. In considering the complaint procedure, remedies and application, the limits of pursuing action under the international sphere of this framework become stark.
Regional Human Rights Instruments
Turning to the potential of utilising human rights through a regional instrument, options are readily available. Many regions have initiated human rights recourse options such as the African Court on Human and Peoples’ Rights (ACHPR), (37) the European Court of Human Rights (ECtHR), (38) and the Inter-American Court of Human Rights (IACtHR). (39) These instruments safeguard many of the same rights already enumerated in the instruments above (prohibition on discrimination, right to personal liberty, right to physical and mental health, etc.); however, they are also notably creations of their regional tendencies; the African Court, for example, has the right to self-determination from colonialism enshrined in article 20.
These regional instruments mirror many of the same benefits and challenges experienced by the international sphere. The rights are broadly articulated, the process is barred to individuals unless the mechanism has been permitted access by the nominated State (only eight States have allowed the ACHPR to receive complaints from non-governmental organisations [NGOs] and individuals), (40) and enforcement is reliant on State compliance (the ECtHR openly declaring that ‘the Court is not responsible for the execution of its judgement’). (41) The remedies available, however, are more appealing; both the IACtHR and the ECtHR can offer compensation to address the physical and, at times, moral harm inflicted on the individual. (42) The ECtHR also often orders that the declaration of a violation is a sufficient remedy. (42) The ACHPR can order compensation or reparations, and in situations of ‘extreme gravity and urgency’ is authorised to order provisional measures under article 27 of the Protocol to the African Charter on Human and Peoples’ Rights on the Establishment of an African Court on Human and Peoples’ Rights. (43) Such remedies are focused on the individual, rather than the vague and ambiguous requirement to ‘review’, as offered by the international sphere.
It is also through cases using such instruments that the interpretation of broad rights to suit the facts of a particular situation are exposed. At the ECtHR in the case of Buturugă v Romania, the Court upheld that cyberbullying is a breach of article 3 (prohibition on torture and inhuman or degrading treatment or punishment) and article 8 (right to respect for private and family life). (44) Though the core issue was domestic violence, this case holds potential precedential value. The situation could be deemed analogous, and therefore provide a blueprint of language, nomination of rights in breach and remedies, that could be utilised by a complainant in the instance of abuse between medical practitioners. With an immense case load (the ACHPR has finalised 172 cases since 2009), (45) these instruments may reveal a number of cases that can act as a guide to prospective complainants in regard to law interpretation, rulings and remedies. Having first needed to exhaust domestic options before turning to the regional instruments, (46; 47) however, it is to this sphere that attention must now be turned.
Domestic Human Rights Instruments
The possibilities offered by the human rights framework through domestic instruments are quite different to the options explored above. At once, human rights at this level can be both subtle and explicit. Protection and enforcement can be maintained through legislation, the criminal justice system, dedicated organisations, and NGOs, as well as through policies and standards instilled in individual employment sectors and workplaces. Noting that the abuse between medical practitioners often occurs in the workplace, the examples proffered below focus solely on this arena.
First and foremost, domestic legislation can be connected with the international treaty ratification process or may stand alone. As explained above, where a treaty is ratified, the State agrees to be bound by its contents. This offers two-pronged protection: first through the domestic law which has been authorised to protect that right and second through the complaint mechanism of the international treaty. Domestic legislation concerning rights may appear as constitutional enshrinement, such as the Bill of Rights in the United States, (48) or through specific rights legislation, such as in New Zealand. (49) It may also appear through employment legislation, such as the federal Fair Work Act 2009 in Australia, or through work, health and safety legislation. Enforcement of legislated rights occurs through the judicial system, with the apex court of the State being the final arbiter. As chapter 11 is exploring the legal avenues available, it is not necessary to explore that particular route here, except to mention that these processes are often arduous and should not be proffered lightly.
At a domestic level, human rights are often safeguarded by various organisations. Some of these organisations have the ability to accept complaints and conduct a dispute process, while others focus on advocacy. The Australian Human Rights Commission (AHRC), for example, has a dedicated sex discrimination team, regularly releasing reports including on workplace abuse and harassment. (50) The AHRC can accept complaints, utilising conciliation to resolve disputes. (51) Should a complainant not be satisfied with the outcome, the Federal Courts are the final arbiter in the matter. (51) Organisations which focus on advocacy include NGOs such as Amnesty International, Human Rights Watch and United for Human Rights. These organisations monitor specific human rights and use grassroots tactics and strategies to agitate for change.
A final domestic avenue regarding human rights is through industry-specific advocacy. These are very local, and sometimes employer specific, options, which have the benefit of knowledge concerning working conditions, standards, and practices. The Royal Australasian College of Surgeons, for example, works to provide training and standards-setting in Australia and New Zealand, and has a dedicated advocacy arm. (52) Industry unions, such as the Australian Medical Association, represent doctors in their employment rights. (53) Enterprise bargaining agreements, which are documents dictating conditions of work and standards applicable at a nominated workplace, are also useful tools to commence a complaint, as they often contain a dispute resolution mechanism which the employer is required to follow.
Having documented the options above, it is clear that the domestic sphere offers avenues that are more specialised and nuanced than those proffered by the regional or international sphere. In this way, it is almost difficult to identify the rights that are being protected as they are often enmeshed within standards, legislation and polices. Using one or more of the options mentioned above may assist a complainant in resolving their particular issue in a manner more palatable than that which may occur through a regional or international instrument. In any event, it is worth remembering that such domestic routes, particularly legal when available, are often required to be pursued before escalation to a global instrument is permitted.
Discussion
The question becomes: is the human rights framework an appropriate lens through which to view and tackle the issue of abuse between medical practitioners? The answer depends on what the survivor seeks. If the survivor wishes to act in an individual manner, seeks specific remedies such as compensation or their abuser to be penalised through incarceration or financial means, the ability of the human rights framework to achieve this in a practical and efficient manner appears underwhelming at best. Such a result is really only possible through the legal enforcement of such rights, and therefore only available where the State has afforded the survivor such legal recourse through domestic legislation.
The benefits offered by this framework are evident when used in a collective fashion. Human rights can be used to lobby States and advocate for specific change, utilising the language, global standards and data that are collected through the instruments in conjunction with the lived experience of survivors. Through such agitation, individuals may be able to achieve change on a local level, such as harassment and abuse being included in enterprise bargaining agreements, to a more national or regional level, including the development of legislation or memoranda of understanding between States regarding standards of behaviour.
The rights framework is evidently reactive rather than proactive. Experiences lead to change for future generations, rather than immediate and satisfying results for the wronged individual. Success may also be incremental, with changes and societal shifts slowly taking form over years and decades. It cannot be ignored that there has been significant success in utilising the rights framework for various campaigns: equal pay between women and men, abolition of the death penalty and climate action have used the rights framework and substantial agitation to bring global actors, including States and corporations, into agreement about standards. Of course, even collective action has its drawbacks; some survivors may not wish to publicise their experience, national defamation laws may affect what survivors can release without a criminal conviction, and overall the process is lengthy.
In this way, perhaps the best method of utilising the rights framework is in conjunction with other means, such as through the criminal law pathway. Using the framework, language and statistics offered by human rights may bolster other recourse actions taken by the individual and complement both the need for immediate action and inspire collective change. The power of human rights can no doubt be harnessed to achieve results in one way or another.
Conclusion
Human rights language and standards have permeated the lived reality of most States. The interpretation and enforcement of these rights is where the framework lacks the ability to achieve immediate and effective individual change. While the individual may not receive the benefits, collective agitation using the language and information collected globally can affect national legislations and laws that may prevent future individuals from experiencing the same abuse that their predecessors did. In order to be completely effective, the use of this framework may best be utilised in partnership with a more definitive lens, such as through legal recourse. Ultimately, this framework offers something to the project of addressing the issue of abuse between medical practitioners but cannot provide a definitive silver bullet.
Introduction
Medical regulatory authorities (MRAs) around the world share similar objectives: to protect patients by employing effective regulatory tools to manage risk and ensure that doctors are fit to practise and contribute to the provision of high-quality health care. The term ‘medical regulatory authority’ refers to an organization recognised by the government of a specific country, state or province as being responsible for the regulation, and/or registration/licensure, of medical practitioners, whereby such practitioners are entitled to practise the profession of medicine. They are commonly referred to as Medical Boards or Medical Councils.
In 1994, the Federation of State Medical Boards of the United States (FSMB) hosted the first International Conference on Medical Regulation in Washington, DC. The conference was attended by representatives of Australia, Canada, Ireland, New Zealand, South Africa, the United Kingdom and the United States. Observers attended from Egypt, Israel, Mexico and Taiwan.
Designed to initiate dialogue among the attendees, the conference focused on the status of medical regulation in the participating nations, examined current research and identified future research needs. In September 2000, medical regulatory authorities from Australia, Canada, Ireland, New Zealand, South Africa, Sweden, the United Kingdom and the United States formed the International Association of Medical Licensing Authorities, which was formally incorporated in 2004 in the State of Texas, USA as the International Association of Medical Regulatory Authorities (IAMRA).
IAMRA’s vision is that everyone around the world is treated and cared for by safe and competent doctors. Its stated purpose is to promote effective medical regulation worldwide by supporting best practice, innovation, collaboration and knowledge sharing in the interest of public safety and in support of the medical profession.
IAMRA recognises that effective regulation makes a vital contribution to patient and workplace safety. The challenge for medical regulators is to create relevant and effective systems that can respond to the rapidly changing environments in which doctors work, changes in health care and communication technologies, and evolving health care delivery systems.
Given the mobility of the medical workforce, IAMRA recognises that the impacts of medical regulation can be felt across the world; what happens in one jurisdiction has the potential to affect another, both positively and adversely. Facilitating interconnectedness and collaboration is the mechanism by which IAMRA fosters best practice and collegiality in medical regulation.
IAMRA does not promote a particular model of medical regulation or dictate how MRAs should operate, recognising that regulatory models are influenced by cultural factors, the structure of the health care system, the legal framework in which regulatory authorities operate and the resources available. Even within IAMRA’s membership, many different models of regulation and degrees of independence and autonomy are represented, including autonomous self-regulating MRAs, MRAs responsible to government, MRAs within a national or state government, and hybrid models.
In addition, the composition of Boards and Councils within MRAs is similarly variable. Some are comprised entirely of members elected by the profession. Others are appointed by their government. Many have legal members, but the involvement of community members is not universal, and even when present, community members may experience difficulty having their voices heard.
Recognising this diversity, one of IAMRA’s objectives is to provide resources to assist members as they navigate the challenges and competing priorities of regulating the medical profession in their own jurisdiction.
Whatever model is employed, regulation of the medical profession generally involves the same key processes aimed at ensuring that doctors are fit to practise as outlined in Table 13.1. The processes relevant to the issue of sexual harassment of doctors by other doctors are setting and enforcing standards of practice, managing complaints and managing unsatisfactory professional conduct/behaviour.
Health care systems are complex, and patient safety requires individual doctors to be fit to practise, teams to operate effectively, and the health care system to be provided with the necessary resources and infrastructure. Not all of these factors are within the sphere of influence of MRAs, but MRAs are in the unique position of having statutory powers to set standards, manage complaints and ensure that medical practitioners practise medicine according to those standards. While an employer may take action that is applicable within a particular workplace, they probably will not have authority or influence over a doctor who moves their practice to another location. This is an important consideration in the management of all professional conduct matters, including sexual harassment.
| Initial licensure – a process during which a doctor’s qualifications and experience come under careful scrutiny, along with other fitness to practise considerations. |
| Renewal of licensure – a process requiring consideration of a doctor’s continuing competence and fitness to practise. |
| Setting and enforcing standards of practice. |
| Managing complaints – a process which may highlight fitness to practise concerns. |
| Managing unsatisfactory professional conduct/behaviour – a process that may result in disciplinary action as well as restrictions of the doctor’s practice. |
| Managing impairment– a process whereby impaired doctors are able to continue in practice, if the impairment does not impede their ability to provide safe and effective care. |
| Managing poor performance – a process generally focused on remediation, but which may require restrictions on the doctor’s practice or disciplinary action, if appropriate. |
| Reinstatement of licensure – a process whereby the reinstatement of a doctor’s licence is considered, following a period of voluntary or imposed revocation. |
| Establishing and maintaining relationships with stakeholders. |
Note: Those particularly relevant to sexual harassment and abuse between doctors are in bold.
Standards of Practice
IAMRA recognises that a multitude of attributes contributes to a doctor’s fit to practise. (1) In the list below, those in bold are most relevant to the topic of sexual harassment in medicine.
They must possess a recognised and relevant qualification;
They must always practise in accordance with their training and competence;
They must demonstrate professionalism through their ongoing commitment to maintaining their competence throughout their working life;
Their personal health must not adversely impact their practice;
They must make safe and appropriate judgments, recognise when their performance is compromised and act accordingly;
They must always demonstrate professionalism in their interactions with patients and colleagues;
Their professional conduct and behaviour must always reflect the expectations of the community and the trust placed in them.
‘Professionalism in their interactions with patients and colleagues’ is recognised by IAMRA because of the potential for unprofessional conduct towards colleagues to adversely impact on clinical teams, whether that conduct occurs in the workplace or outside it. Sexual harassment, perpetrated by a doctor, falls squarely into this domain. The argument frequently put forward in the defence of a medical practitioner accused of sexual harassment of a colleague, that the conduct did not involve patients, can be refuted when the impact of such behaviour on clinical teams and on the integrity and reputation of the medical profession is recognised.
Regulators’ Expectations of Medical Practitioners
MRAs generally expect that medical practitioners will exhibit behaviours and attitudes that reflect the expectations of those with whom they interact and the society in which they work. Professional misconduct is variously named and defined in the particular legislation MRAs administer, and there is a spectrum of professional behaviour that may constitute grounds for disciplinary action against a practitioner. Universally, the sexual assault of a patient would constitute grounds for disciplinary action, but MRAs’ policies and codes of conduct in relation to sexual harassment of colleagues are not always explicit. However, many MRA’s have documented a clear expectation of how doctors should conduct themselves in relation to their colleagues. Some examples follow.
International Examples of Relevant Standards of Practice
Australia
The Medical Board of Australia document, Good Medical Practice: a code of conduct for doctors in Australia, (2) provides a comprehensive standard, stating:
1.2 Use of the code
Doctors have a professional responsibility to be familiar with Good Medical Practice and to apply the guidance it contains.
This code will be used:
to assist the Medical Board of Australia in its role of protecting the public, by setting and maintaining standards of medical practice against which a doctor’s professional conduct can be evaluated. If your professional conduct varies significantly from this standard, you should be prepared to explain and justify your decisions and actions. Serious or repeated failure to meet these standards may have consequences for your medical registration.
and
5.4 Discrimination, bullying and sexual harassment
There is no place for discrimination (including racism), bullying and sexual harassment in the medical profession or in healthcare in Australia. Respect is a cornerstone of good medical practice and of patient safety. It is a feature of constructive relationships between medical practitioners, their peers and colleagues on healthcare teams, and with patients. Discrimination, bullying and sexual harassment adversely affect individual health practitioners, increase risk to patients and compromise effective teamwork by healthcare teams.
Good medical practice involves:
5.4.1 Being fair and showing respect for peers, colleagues, co-workers, students on health care teams and patients.
5.4.2 Not discriminating against, bullying or sexually harassing others.
5.4.3 Providing constructive and respectful feedback to colleagues, trainees, international medical graduates and students, including when their performance does not meet accepted standards.
5.4.4 Being open to receiving constructive feedback.
5.4.5 Doing or saying something about discrimination, bullying or sexual harassment by others when you see it and reporting it when appropriate.
Good medical practice in the management of discrimination, bullying or sexual harassment requires a timely, proportionate and fair response, including:
5.4.6 Having zero tolerance for discrimination, bullying and sexual harassment.
5.4.7 Providing respectful and timely feedback to another medical or health practitioner about behaviour that does not meet accepted standards.
5.4.8 Early, timely, local and fair management of concerns about discrimination, bullying and sexual harassment whenever possible, including through existing employer complaints resolution processes to help minimise harm and build a culture of respect.
5.4.9 Appropriate information sharing, within the law, by all relevant parties such as employers and specialist medical colleges, to support effective resolution and remediation, when possible.
5.4.10 Referring concerns about discrimination, bullying or sexual harassment to the Medical Board when there is ongoing and/or serious risk to patients, students, trainees, colleagues or health care teams (in addition to mandatory reporting obligations).
British Columbia, Canada
The College of Physicians and Surgeons of British Columbia, in their practice standard on sexual misconduct, (3) states;
Registrants must be aware of and never exploit the power imbalance in a registrant–learner or registrant–coworker relationship. Registrants must not make sexual comments or gestures toward a learner or co-worker or enter a close personal or sexual relationship with a learner or co-worker while directly or indirectly responsible for mentoring, teaching, supervising, or evaluating that individual.
New Zealand
The Medical Council of New Zealand / Te Kaunihera Rata o Aotearoa standard on unprofessional behaviour (4) states:
As a doctor, you have an obligation to be respectful and professional as your behaviour may affect how a health team functions, how care is delivered to patients, and the public’s trust and confidence in the medical profession.
It also states:
Unprofessional behaviour may erode trust, and create division and conflict with other members of the health care team, including all who are involved in the patient’s care. It can affect the morale and mental well-being of others, as well as the inclusivity, collegiality and culture in your practice setting or workplace.
Singapore
The Singapore Medical Council (SMC) document, Ethical Code and Ethical Guidelines (ECEG), (5) states:
The SMC takes the view that serious disregard of or persistent failure to meet the standards set out under the ECEG can potentially lead to harm to patients or bring disrepute to the profession with loss of confidence in the healthcare system and consequently may lead to disciplinary proceedings.
D5. Colleagues under supervision
Teaching, supervising and mentoring junior doctors and other healthcare professionals is an important part of professional life and forms part of your obligation to improve the care of patients in the community. This means:
(2)You must not abuse your position as a teacher or supervisor to exploit supervisees for personal gain or gratification. You must not enter into emotionally intimate or sexual relationships with your supervisees while they are under your charge.
United Kingdom
The General Medical Council document, Good Medical Practice, (6) states:
Good Medical Practice describes what is expected of all doctors registered with the General Medical Council (GMC). It is your responsibility to be familiar with the Good Medical Practice standards and the explanatory guidance which supports it, following the guidance they contain.
These standards require the doctor to work collaboratively with colleagues, outlining the following expectations:
52. You must help to create a culture that is respectful, fair, supportive, and compassionate by role modelling behaviours consistent with these values.
53. You should be aware of how your behaviour may influence others within and outside the team. …
56. You must not abuse, discriminate against, bully, or harass anyone based on their personal characteristics, or for any other reason. By ‘personal characteristics’ we mean someone’s appearance, lifestyle, culture, their social or economic status, or any of the characteristics protected by legislation – age, disability, gender reassignment, race, marriage and civil partnership, pregnancy and maternity, religion or belief, sex and sexual orientation.
57. You must not act in a sexual way towards colleagues with the effect or purpose of causing offence, embarrassment, humiliation or distress. What we mean by acting ‘in a sexual way’ can include – but isn’t limited to – verbal or written comments, displaying or sharing images, as well as unwelcome physical contact…
58. If you witness any of the behaviours described in paragraphs 56 or 57 you should act, taking account of the specific circumstances. … We recognise some people may find it harder than others to speak up4 but everyone has a responsibility – to themselves and their colleagues – to do something to prevent these behaviours continuing and contributing to a negative, unsafe environment.
59. If you have a formal leadership or management role and you witness – or are made aware of – any of the behaviours described in paragraphs 56 or 57, you must act. You must:
a. make sure such behaviours are adequately addressed
b. make sure people are supported where necessary, and
c. make sure concerns are dealt with promptly, being escalated where necessary.
United States of America
A Federation of State Medical Boards (FSMB) paper entitled ‘State Medical Board recommendations for stronger approaches to sexual misconduct by physicians’ (Reference King, Chaudhry and Staz7) primarily addresses the issue of sexual misconduct directed towards patients, but does include reference to harassment between doctors in the following statement:
The medical profession must promote a culture in which sexual misconduct in any form is not tolerated. Such behaviour undermines professional attainment, and when that behaviour is tolerated, overtly or tacitly, it reduces the likelihood of bystander reporting and erodes professional culture in a patient-centered system. Sustaining this effort across the entire profession and in every clinical setting, both inpatient and outpatient, will be critical to maintaining the public’s trust. (Reference King, Chaudhry and Staz7)
MRAs whose codes of conduct explicitly state that sexual harassment of colleagues constitutes a breach of professional standards are in a strong position to take action against a medical practitioner who is not compliant with the code. Even if an MRA is not explicit about its expectations, there may still be mechanisms available by which it can deal with the issue. For example, laws under which MRAs operate frequently require registered/licensed medical practitioners to be ‘of good character’, or words to that effect. However, reliance on this inexplicit requirement alone can be problematic in the prosecution of individual cases.
Regulatory Response to Complaints of Sexual Harassment
MRAs generally become aware of departures from acceptable standards of conduct through notifications or complaints, but for the reasons explained elsewhere in this book, the victims of sexual harassment may be reluctant to come forward.
In general, MRAs would expect that sexual harassment would, in the first instance, be dealt with in the workplace, supporting the victim/s and addressing the perpetrator’s behaviour. However, in more egregious cases, for example, sexual assault or repeat harassment, should, in addition, be referred to the MRA so that the conduct can be viewed through the lens of professional standards, public protection and community expectations. Importantly, the MRA can deal with the issue at the level of the practitioner’s registration/licensure, unlike the employer, whose remit may only relate to their employment in a specific location.
In some jurisdictions, practitioners and the courts are required to notify the MRA when a medical practitioner is subject to criminal charges or convictions in relation to certain offences, and this is a valuable intersection between the criminal justice system and the medical regulatory system. It may be possible for both processes to proceed in parallel, the MRA dealing with the practitioner’s fitness to practise medicine and the courts determining if a criminal act has been perpetrated.
In addition, mandatory notification legislation, present in some jurisdictions, may place an obligation on registered health practitioners to notify the MRA of concerns about the conduct or fitness to practise of another registered practitioner. This obligation may also apply to medical practitioners who are colleagues or employers of the alleged perpetrator.
Important in this discussion is the realisation that MRAs are wholly reliant on receiving notifications or complaints about sexual harassment and sexual assault; they are not in the business of workplace surveillance. In the case of sexual harassment, it is often preferable for a complaint to be made by an employer, rather than the victim, so as not to place the victim in direct opposition to the perpetrator.
When made aware of sexual harassment or sexual assault perpetrated by a medical practitioner against another medical practitioner (or indeed, any other colleague), MRAs are generally well placed to deal with the issue with legislated and effective tools; this is even more so when the decision-making board/council has a good gender balance, community representation and a clear understanding of contemporary professional and community standards.
When an MRA becomes aware of an issue of sexual harassment or sexual assault, a typical response would involve some or all of the following steps:
Seeking the practitioner’s response, unless the complainant does not wish their identity to be disclosed. This can be an impediment to an individual complaint going further, as the principles of procedural fairness are such that in order to provide a full response, the practitioner needs to know the details of the accusation. It is often helpful for there to have already been a workplace-based investigation, particularly if multiple victims have come forward;
Reviewing past notifications and complaints about the practitioner, looking for a pattern of similar or other relevant behaviour;
Low level intervention, if appropriate, such as a warning letter or counselling interview;
Consideration of urgent, interim action. Depending on the legislative framework, this action may be taken for the health and safety of the public, or more generally, in the public interest. In the most egregious cases, interim action may include actions such as suspension of the practitioner’s registration or imposition of conditions on their registration pending further investigation;
Full and detailed investigation, possibly including multidisciplinary assessment of the practitioner to consider the risk of recidivism;
Prosecution by the MRA or their agent when the investigation points to unsatisfactory professional conduct or professional misconduct.
When findings are made against a medical practitioner, action by the MRA or its agent may take a variety of forms, including:
Reprimand or censure, placed on the practitioner’s record;
Suspension of their registration/license for a specified period of time;
Restricted or conditional registration/licensure;
Monetary fine;
Deregistration, erasure, license revocation;
Notification of other jurisdictions in which the medical practitioner is known to be registered;
Inclusion of relevant information on certificates of registration/licensure status in circumstances where the medical practitioner seeks registration/licensure in another jurisdiction.
Conclusion
From the regulatory perspective, most, if not all, medical regulatory authorities view sexual harassment of a medical practitioner by another medical practitioner to be unsatisfactory professional conduct or professional misconduct, because the distress caused to the victim of sexual harassment and the potential for the clinical team to be disrupted as a result are detrimental to public health and safety, and contrary to the reasonable expectations of the medical and non-medical community about standards of behaviour of medical practitioners.
While it is usually appropriate for lower-level instances of sexual harassment of colleagues to be dealt with in the workplace in the first instance, consideration should be given to referring more egregious cases and repeat offenders to the medical regulatory authority, which can, in all likelihood, take action, including urgent action, applicable in all locations in which the medical practitioner practises. If the medical practitioner is known to be registered/licensed in another jurisdiction, that jurisdiction can be notified. Similarly, if the medical practitioner seeks registration/licensure in another jurisdiction, the medical regulatory authority can provide relevant information on a certificate of registration/licensure status, or similar, ensuring that the practitioner is held accountable wherever they choose or seek to practise.
Introduction
Medical students come to the field with a range of pre-existing competencies, attitudes, cultural assumptions, privilege and values. Medical educators must teach, train, supervise and assess, but they may also hold other roles simultaneously, acting as managers, employers and senior colleagues. Because of the breadth of workplace-based learning required in medicine, most doctors teach, beginning when they are in quite junior roles. Almost invariably, clinicians take on these roles without any training or experience in management, education, or assessment. Medical educators also facilitate professional identity formation, acting as mentors and role models. Some of these roles may be difficult to integrate, because they have contradictory goals and require different pedagogy. The situation is made more complex by the increasing role of interprofessional learning across the variety of clinical disciplines and professions present in the health care workplace.
In this chapter, we examine several core responsibilities of medical educators in the field of professionalism. First, medical educators are responsible for teaching and assessing professional conduct, and where possible, remediating poor performance. They are also responsible for selecting suitable medical students, and graduating doctors who demonstrate appropriate professional conduct. Finally, medical educators lead educational teams, managing the multiple roles of supervising, teaching, assessing and managing learners, and in doing so, they create, sustain and manage the hierarchies in which sexual harassment often occurs.
Professionalism in the Curriculum: Defining Competencies
Professionalism is a conceptually complex idea, that encompasses a number of dimensions that appear easy to understand in principle, but remarkably difficult to operationalise in practice. At its most basic, professionalism ‘signifies a set of values, behaviours, and relationships that underpins the trust the public has in doctors’. (Reference Birden, Glass, Wilson, Harrison, Usherwood and Nass1) While it is easy to agree that doctors should demonstrate psychologically safe interpersonal behaviours, defining what those behaviours are in any given context of place and time can be challenging. This complexity is represented in the multiple codes of conduct under which doctors train and work. Integrating expectations from workplaces, training institutions, regulatory organisations, legislation and other codes requires enormous flexibility on the part of medical educators in a highly dynamic area of practice.
At present, there is an emphasis on competency-based curriculum and assessment, and so professionalism tends to be captured in these expected codes of practice (see chapters 6 and Reference Wilkinson, Wade and Knock13). These competencies are represented in the written curriculum, where expected behaviours are defined, taught and assessed. Ideally, of course, the doctor in training will demonstrate their knowledge of expected behaviour, but will also consistently demonstrate these skills in an authentic professional environment. (Reference Epstein and Hundert2; Reference Bird and Gilligan3) The problem with codes is that it is easy to incorporate aspirational goals that are poorly defined, resulting in standards that are difficult to interpret and impossible to meet. In the past, medical organisations such as colleges, universities and regulatory bodies were the final arbiters of whether a trainee could be recognised as a professional. Now, assessments of professionalism need to match contemporary expectations of defensible assessment, particularly if a doctor in training is removed from a programme.
Unfortunately, professionalism can easily be described in practice as ‘hard to define, but I’ll know it when I see it’. (Reference Ferguson4) This subjectivity is no longer acceptable as a benchmark. (5; 6) Difficulties arise when highly intelligent learners mimic professional competencies but generate ill-defined unease in their colleagues and supervisors, often due to their attitudes or expressed values. Detecting and quantifying the risk of sexual misconduct is complex. Medical educators need to address the challenge of capturing valid subjective perceptions by members of the teaching team without introducing unacceptable bias or perceptions of bias. In some countries, given the cost of training, failing a student may result in litigation, which inevitably means assessments must be legally robust in addition to being educationally valid and reliable.
Because professionalism is much broader than definable competencies, many codes of conduct include ‘competencies’ that are actually attitudes, personal character traits, or aspirational goals, and they may even pose ethical conflicts. For instance, in the Australian context, the good practice guide requires doctors and medical students to provide ‘constructive and respectful feedback to colleagues, trainees, international medical graduates and students, including when their performance does not meet accepted standards’. (5) It is unrealistic to expect doctors in training to give ‘constructive and respectful feedback’ to their seniors, colleagues or interprofessional teams unless there is a recognition of established hierarchies, acceptable modes of communication (including interprofessional communication) and a high degree of existing psychological safety. In the UK, the General Medical Council has produced similar standards, including the following: ‘you must be compassionate towards colleagues who have problems with their performance or health. But you must put patient safety first at all times.’ (6) It is understandable how difficult this statement may be to implement in practice. Both sets of standards place the responsibility of working safe hours on the individual, requiring a doctor to recognise the impact of fatigue on the doctor’s health and ability to care for patients, and requires them to endeavour to work safe hours wherever possible. (5; 6) Placing the responsibility of managing workload on an individual ignores the role of organisational culture and expectations, and is particularly unrealistic for junior doctors with little institutional power. Clearly, behavioural competencies may not, and perhaps cannot, extend across the entire field of professional expectations.
Sociologists may comment that professionalism can be understood as a role that doctors play in society. (Reference Martimianakis, Maniate and Hodges7) This perspective implies that professionals build trust by demonstrating ‘trustworthiness’ and an attitude of service to the needs of the community. (Reference Swick8) At the same time, professionalism can be understood as an expression of power and a means of social control. (Reference Martimianakis, Maniate and Hodges7) ‘Professionals profess’ writes Hughes, in the 1950s, ‘They profess to know better than others the nature of certain matters, and to know better than their clients what ails them or their affairs.’ (Reference Hughes9) This positioning of the doctor within the health care social system, and society more broadly, is part of the hidden curriculum. (Reference Martimianakis, Maniate and Hodges7) There are boundary issues between professions to be negotiated and understood, but also issues around race, gender and class. (Reference Hill, Samuels, Gross, Desai, Zelin and Latimore10; Reference Nieblas-Bedolla, Christophers, Nkinsi, Schumann and Stein11) When doctors learn to be doctors, operating within the social systems that medicine inhabits, they learn to inhabit systems of power and privilege. (Reference Rabinowitz, Reis, Van Raalte, Alroy and Ber12) This is where the hierarchies in which sexual harassment occur and can thrive. No wonder medical educators require considerable skill in teaching, assessing and remediating professional conduct with doctors in training.
Professionalism as a Behaviour: Teaching and Assessment
Because professionalism is an area of practice that is difficult to define, it is exceedingly difficult to assess in a defensible way. ‘The difficulty of its assessment’, writes Tim Wilkinson et al., ‘is nearly as great as the value we place on it.’ (Reference Wilkinson, Wade and Knock13) The risk of a doctor sexually harassing a colleague is usually captured when assessing interpersonal skills and teamwork. (Reference Berger, Niedra, Brooks, Ahmed and Ginsburg14; Reference Jha, Bekker, Duffy and Roberts15) Assessments are designed to test the positive competencies (such as teamwork, respect for diversity, professional manner and appropriate boundaries) as well as detecting ‘red flags’ which may indicate a risk of professional misconduct. (Reference Ainsworth and Szauter16–Reference Karp18)
One way of conceptualising professionalism involves a modified form of Miller’s Pyramid. In its early version, Miller proposed a hierarchy of learning, beginning with knowledge. Competence is often demonstrated through applying a skill in a constructed environment, such as simulation, before performing the skill in its usual context, and finally demonstrating competence consistently in the workplace. (Reference Miller19) Since then, other scholars have proposed an additional layer of the pyramid, describing mastery, when a learner now ‘thinks, acts and feels’ like a professional (see figure 14.1). Wilkinson et al. discuss a blueprint for assessing professionalism, mapping assessment techniques and frameworks against professionalism aims. (Reference Wilkinson, Wade and Knock13) In the following, we examine the ‘layers’ of Miller’s Pyramid with respect to sexual safety, and the way pedagogies and assessments intersect.
Amending Miller’s Pyramid to include professional identity formation. Reproduced with permission. (Reference Cruess, Cruess and Steinert20)
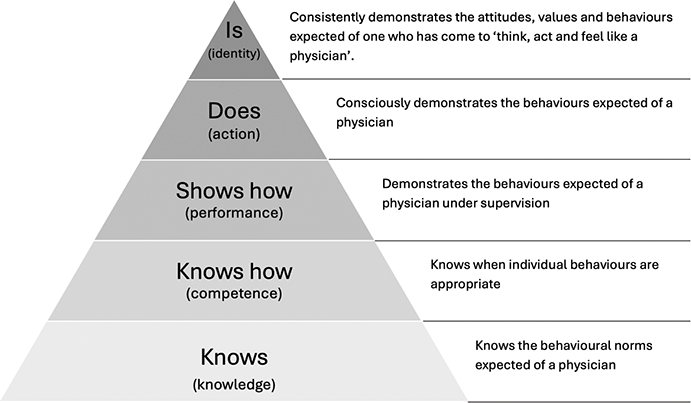
Figure 14.1 Long description
The pyramid diagram represents the progression of physician competencies through five levels, from bottom to top: 1. Knows (knowledge): Knows the behavioural norms expected of a physician. 2. Knows how (competence): Knows when individual behaviours are appropriate. 3. Shows how (performance): Demonstrates the behaviours expected of a physician under supervision. 4. Does (action): Consciously demonstrates the behaviours expected of a physician. 5. Is (identity): Consistently demonstrates the attitudes, values and behaviours expected of one who has come to think, act and feel like a physician.
Knowledge
At its basic ‘layer’, the doctor in training must be able to describe their professional obligations with respect to sexual boundaries, intimate examinations and other potential areas of misconduct. Teaching may involve didactic presentations, readings, and discussions and there may be a requirement to assess knowledge of the codes under which a student must learn. Pen and paper testing and other traditional forms of assessment, such as multiple-choice questions and short answer questions, can determine mastery of the knowledge required. An example of a knowledge task may involve describing the requirements of a particular code of conduct or providing a definition of sexual harassment.
Competence
In Miller’s Pyramid, competence means being able to apply a skill theoretically, such as working with scenarios rather than in authentic practice. (Reference Rethans, Norcini, Barón-Maldonado, Blackmore, Jolly and LaDuca21) In medicine, this is where teaching techniques can diversify. Students may still learn in didactic settings, but increasingly, medical education utilises problem-based learning, a system where groups work together to better understand and solve clinical problems. An example would be drawing a flowchart to represent the process of making a complaint, or defining which examples constitute harassment.
There are a number of self-assessed tools to assist doctors in training to examine and, if necessary, challenge their own professional assumptions and beliefs, and these can enhance their skills in reflective practice. (Reference Guraya, Guraya and Almaramhy22–Reference Launer24)
Performance
Performance involves demonstrating a skill in its appropriate context. In the professionalism space, techniques such as simulation may be used, using role plays, discussions or virtual worlds. These tasks may be addressed in peer groups, interprofessional teams, with actors or virtually. Doctors in training need to grasp the idea that professional conduct is situated in a particular time and place, and therefore medical educators may ask students to adopt a theoretical or personal position, examining the problem with multiple points of view. Although peer-norming is important, the aim is also to build ‘professional reasoning’: the capacity to make and remake one’s professional identity to suit the requirements of the role.
The difference between competence and performance can depend on the environment in which doctors learn. Doctors in training are highly motivated to adopt attitudes and behaviours that seem successful to them. (Reference Bandura25) Apprenticeship in a clinical setting involves taking interpersonal risks in an environment where ambiguity and uncertainty are expected. Tackling dilemmas around boundaries are essential transformational learning opportunities that drive maturation from apprentice to master. (Reference Torralba, Jose and Byrne26) This is often uncomfortable for the learner, and medical educators need to provide supportive spaces where students can take learning risks, including challenging their own beliefs or values.
Culturally, there is a range of discomfort with uncertainty. Given the high stakes of medical assessment, many students will be keen to unearth the ‘right’ answer to any given ethical problem. Greene’s dual-process theory of moral judgment (Reference Conway and Gawronski27; Reference Bago and De Neys28) asserts that both emotional and cognitive processes contribute jointly to moral decision making, with doctors in training deciding what is ‘right’ through analysis but also by their ‘gut feeling’ or ‘conscience’. For many doctors in training, this is a steep learning curve. Most doctors enter medicine with an empirical knowledge-based background, and these individuals can struggle with the nuanced and contextualised nature of ethical decision making and professional conduct.
These types of conversations need to be led by mentors and supervisors: when is it acceptable to have a relationship with a junior colleague? When is an obscene comment from an elderly patient with dementia considered ‘harassment’ and when it is considered frontal lobe disinhibition? Can it be both? What is the ‘professional’ response to a remark from a senior supervisor in the tea-room that you consider inappropriate? How does a doctor manage discomfort, painful interactions and vicarious trauma?
The acquisition of values, attitudes, behaviours and skills that represent ‘the way we do things around here’ is known as the hidden curriculum (see chapter 6). The hidden curriculum represents norms and values built into the training process, sociocultural behaviours and relationships that students need to master to effectively function in a social role. (Reference Wren29) Because doctors in training cover a very broad range of learning environments from primary to tertiary settings, and ‘cradle to grave’, their cultural and social immersion is complex and evolving. Acceptable behaviour in community paediatrics may be quite inappropriate in a tertiary intensive care unit. Doctors in training are influenced through a spectrum of observed and experienced situations which may range from extremely positive to negative. (Reference Rees, Alfes and Gatenby30–Reference McGurgan, Calvert, Narula, Celenza, Nathan and Jorm32)
Pedagogy in this space needs to involve some form of reflective learning, usually accompanied by opportunities to debrief with peers and colleagues, so that each learner can begin to build their own professional identity and test their assumptions in their future workplace. Medical educators may facilitate these discussions using lectures, workshops, formal discussions, peer debriefing and other forms of learning to enable learners to test their assumptions against their peers and their senior colleagues. Learners often need to ‘out’ the hidden curriculum, making the implicit explicit in order to examine its values, assumptions and impact, so they can decide whether to incorporate these ideas or discard them in the formation of their own identity.
Good medical educators have considerable skill in examining, describing and communicating tacit knowledge, but not all teachers do. Schön’s vision of ‘professional artistry’ includes different kinds of competence that practitioners display in unique, uncertain, and conflicted situations of practice. (Reference Schön33; Reference Schön34) Not all clinicians can consciously understand and describe how and why they are performing a skill while they are doing it, so the thinking required to rationalise professional performance is not always available to a doctor in training. This is one reason why the hidden curriculum is so powerful. Without insightful educators, and time to teach and reflect, hidden assumptions remain unexamined, unnamed and potentially unconscious. This means the doctor in training lacks the words and concepts to make sense of their experience, and may not question the cultural assumptions they have absorbed.
One difficulty that occurs in this area is that such discussions can easily replicate existing forms of privilege and hegemony. Team members from more privileged backgrounds can fail to recognise the microaggressions that are experienced daily by their less privileged colleagues.(Reference Michalec and Hafferty35–Reference Chuang, Nuthalapaty, Casey, Kaczmarczyk, Cullimore and Dalrymple37) Hierarchies based on gender, class or race may worsen if those people who are unaffected by them are allowed to dominate discussions, because important narratives of harassment and discrimination will be lost. These narratives need to be heard, because sexual harassment is more common for doctors in training who have lived experience of discrimination and disprivilege; all team members have a role in addressing this.
Assessing the acquisition of professional skills is challenging. Some skills are easily demonstrated (e.g. observing a student seeking informed consent). Others require a portfolio of complementary assessment techniques. Multi-source feedback, from supervisors, interprofessional colleagues, patients and peers, along with self-reflection, can identify doctors in training who are having difficulty acquiring the necessary professional skills. Clinical supervisors are good at making global assessments, identifying the learner whose interpersonal skills seem less professional or appropriate. The challenge is that the assessment needs to be defensible, and where possible, objective, as multi-source feedback is easy to interpret as a scapegoating exercise for students who may be socioculturally diverse. The reverse is also true. A student who is privileged has the potential advantage to use their social network and hegemony to optimise their ratings. Balancing the validity of an assessment with its reliability is always a challenge in the professionalism curriculum.
Action
As the learner becomes more senior, consistent professional conduct is expected. Assessments may focus on particular requirements of training, such as managing a team of learners in a psychologically safe way, or responding to inappropriate comments from patients on the wards. The education team need to have a way to manage critical incidents at this level, e.g. where a doctor in training has crossed sexual boundaries with a patient or colleague, or is perceived as unsafe by members of their team. There is professional learning for those reporting, as well as those who are reported.
Assessment can occur at multiple levels, and with multiple tools and techniques. (Reference Mak-Van Der Vossen, Van Mook, Van Der Burgt, Kors, Ket, Croiset and Kusurkar38) Milder forms of sexual harassment, such as inappropriate humour, can often be assessed and managed through conversation with the learner and their team, and with private feedback. More serious and/or persistent inappropriate behaviour can be escalated to any of the organisations involved in training. (Reference Brennan, Price, Archer and Brett39) Depending on the context and severity, these often require formal reporting processes, including law. Boundary crossing will often require targeted remediation, where the learner is subject to more intense supervision and further assessment. (Reference Launer24; Reference Regan, Hexom, Nazario, Chinai, Visconti and Sullivan40; Reference Arnold, Sullivan, Quaintance, Cruess, Cruess and Steinert41)
The more challenging issue is developing skills in recognising and managing sexual harassment. When a learner finds the behaviour of a colleague uncomfortable, there is an ethical and professional skill in knowing how to respond. In medical education, the training about professionalism and the development of professional identity are often related to issues that come up in difficult interactions with patients, such as inappropriate medication requests, patients who are angry, or people who offer inappropriate gifts. Being able to manage these interactions is important, but there is also an unspoken assumption that difficult behaviours and interactions always come from patients, seldom from colleagues, and especially not from supervisors or trainers.
Identity
At this point, learners embody the role of doctor, and should be experienced in managing contextual complexity. Often at this point, doctors are teaching as well as learning, and have highly developed professional values. They have also developed an understanding of the differences between the overt and hidden curriculum and the written and enacted professional expectations in any workplace.
The growing gap between what is taught and what is learned in the hidden curriculum, what is said and what is done in policy and what is expected and what is achievable in clinical practice means a doctor may have become inured against trusting organisational statements, policies, processes and codes. Medicine constantly evolves, but the pace of change has increased. On the ground, there is fragmentation of clinical responsibilities, a rise in consumer expectations, worsening inequity and fewer resources for care. However, the professionalism codes present what Michalec and Hafferty see as a ‘nostalgic’ view of professionalism, with doctors expected to deliver highly individualised, bespoke care in resource poor environments that can’t afford it. (Reference Michalec and Hafferty35) The outcome of this gulf between what is expected and what can be delivered means an understandable loss of trust. In this environment, the willingness of a doctor to report professional misconduct is significantly reduced. Medical educators need to have advanced skills in describing hidden assumptions and values. In this way, medical education may be able to lead cultural change by challenging inappropriate attitudes within learning teams.
Professionalism as a Trait: Managing Selection and Exclusion
Selection is a complex process which should reflect the academic, clinical, personal and professional potential of students without entrenching systemic bias. (Reference Cleland, Blitz, Cleutjens, oude Egbrink, Schreurs and Patterson44) Medical Schools are increasingly trying to attract students who have the personality characteristics that suit the professional requirements of medicine. Professionalism has been described as a feature of the doctor’s character, not just their behaviour. (Reference Asil, Bannatyne, Craig, Forrest, Stokes-Parish and Szkwara42; 43) Personal traits (Reference Rabinowitz, Reis, Van Raalte, Alroy and Ber12) have become a part of many selection processes, in the hope that a medical school can ‘weed out’ candidates who do not demonstrate the appropriate attitudes or values. This is a challenging enterprise, because many defensible tools used to demonstrate personal characteristics can be manipulated by those who choose to do so, or use norms based on white, privileged cohorts that disadvantage those with diverse backgrounds. Interviews, a mainstay of selection, can be rehearsed, and rehearsal can be more effective if the candidate has links with previously successful candidates, another example of privileging those who already live with privilege. (Reference Cleland, Blitz, Cleutjens, oude Egbrink, Schreurs and Patterson44)
Some universities use situational judgment tests (SJTs), which seem to be less influenced by socioeconomic status than other forms of assessment. (Reference de Leng, Stegers-Jager, Born and Themmen45) The SJT presents applicants with challenging situations they may encounter during medical school, and claim to measure traits like integrity, honesty, humility and sincerity. (Reference de Leng, Stegers-Jager, Born and Themmen45) There is some evidence that the presence of some personality traits predicts clinical performance, (Reference McLarnon, Rothstein, Goffin, Rieder, Poole and Krajewski46) and an example of using emotional intelligence screening is given in Table 14.1. However, there is considerable doubt in the academic literature that any process of this type is able to detect those with sociopathic or other dysfunctional personality traits. (Reference Knights and Kennedy47)
| Bond University in Queensland, Australia has introduced emotional intelligence (EI) testing as part of the selection process for its medical programme, with the aim of enrolling a cohort of students with the strong social skills needed to succeed at university and in the workplace. Bond University is a full fee paying university and has over 1,000 applications for its 120 places. In the past, it used a combination of academic performance and Multiple Mini Interviews to select students. However, it recently introduced an EI test, using this test and a test of academic performance to screen candidates prior to interviews. (Reference Asil, Bannatyne, Craig, Forrest, Stokes-Parish and Szkwara42) |
| Interpersonal skills, such as the ability to recognise one’s own emotions, help others understand theirs, display a breadth of emotional vocabulary and communicate well, are critical to a medical career. Professor Kirsty Forrest, who leads the programme, believes this approach means they select students who will have a better bedside manner, and better teamwork and collaboration skills. |
| ‘It is also about kindness. We believe that the competitiveness just to get into a medical programme can result in students being very unkind to each other. If they are kinder to each other during their years of education – and kind to themselves – it will lead to them displaying compassion when they are in the workforce and dealing with patients.’ |
| ‘There has often been a perception that medical professionals should display no emotion, and this is likely contributing to the higher instances of poor wellbeing and mental health issues in medical students and practising doctors. |
| ‘There has been talk of how medical school “knocks” the empathy out of students and we are looking at the bigger picture of how to ensure that is not the case. We are discussing the possibility of changing the way we test students to put the focus on the learning process rather than assessment, so we remove some of that competitiveness.’ (43) |
Professionalism as a Value: Learning to Balance Rights and Obligations
Medicine has deep ethical roots, but also has persistent ethical challenges. It is notable that the Hippocratic Oath codifies doctors to ‘abstain from all intentional wrong-doing and harm, especially from abusing the bodies of man or woman, bond or free.’ (Reference Minar48) Yet as with all institutions, what is codified may not be followed, and even if it was, the original version of the oath also commits the student ‘to hold my teacher in this art equal to my parents … when he is in need of money to share mine with him …’, so it is easy to imagine how abusive supervisory relationships developed and even flourished with these types of messaging.
In training, self-care takes a secondary role to patient safety. Its notable that it was not until 2017 that the World Medical Association added any wording related to health professional personal wellbeing (49) in their Physicians’ Pledge. (Reference Parsa-Parsi50) The 2017 World Medical Association’s decision to add ‘I will attend to my own health, well-being, and abilities in order to provide care of the highest standard’ to the Physicians’ Pledge (Reference Parsa-Parsi, Kloiber, Kurihara, Greco and Dhai51) indicates the importance that doctors now place on this aspect of their contract with society. (Reference Minford and Manning52) However, in an environment where it is normalised to subordinate one’s own needs in the interests of the patient, this emphasis can be problematic. Learners are expected to tolerate abusive power structures, starting with the simple reality of long hours. The idea of medicine being a vocation rather than just a job valorises the idea of self-sacrifice, ‘setting yourself on fire to keep others warm’.
In Stone et al.’s study of survivors of sexual harassment in medicine, (Reference Stone, Phillips and Douglas53) they describe a case where a young doctor is offered an opportunity to learn to suture. Her supervisor stood behind her as she attended to the patient, who was conscious. While she was suturing, her supervisor was fondling her bottom. ‘There was nowhere to go, it was a bed up against a wall, so you’re in a very small space’, she said. ‘But I think, also, because the patient was conscious, it felt like the right line to take was to continue looking very professional with everybody.’ For this doctor, it meant literally placing her body between the abuser and the patient, and silencing her needs ‘to continue looking very professional’.
The more junior a doctor is, the more unhealthy or harmful experiences become normalised. (Reference McGurgan, Calvert, Celenza, Nathan and Jorm54) Early in most junior doctor careers, traumas are part of the job. New doctors witness humanity at its most vulnerable and authentic, experiencing suffering, grief, loss and death, perhaps for the first time. The doctor is expected to tolerate this emotional, philosophical and potentially spiritual load, be a stable support for the patient and those around them, and then ‘get on with their job’. Once it is normal to dehumanise and compartmentalise the accepted horrors of a career in medicine, it is not a huge step to do the same with other behaviours – the wandering hand, the lingering gaze or worse.
Professionalism as Power: Supervisory Hierarchies and the Risk of Harassment
Doctors are in training for over a decade, in a series of highly hierarchical teams. These teams create an ideal opportunity for the misuse of power. When exploitation is normalised, it is challenging for junior doctors to manage inappropriate or harmful behaviour. Each team has a nested code of norms and relations within and between members and systems. Doctors in training are ‘itinerant workers’, engaging fleetingly with these nested systems – short rotations give little opportunity for them to build trust and understanding within a workplace, or to develop a sense of belonging and integration into teams comprised of more permanent members in each clinical placement. (Reference Gafson, Sharma and Griffin55) These nested systems of team and workplace have more permanence for members like nurses who can expect to ‘outlast’ the doctor in training. Doctors in training are short term investments: they enter a team which has its pre-existing systems of power and privilege already firmly in place, and then they leave, to become ‘someone else’s problem’. The more permanent team members are fluent in the currencies of informal power that flow in that team and workplace, while doctors in training are necessarily just starting to learn the language. Meanwhile, new and relatively inexperienced doctors are unaware of the usual or normative culture, workload or expected degree of functioning, and are therefore unable to identify what is ‘normal’ from a worker’s rights perspective. (Reference Epstein and Hundert2)
The Training Environment
Doctors train in a series of rotations over many years, and may only stay with a team for a few months at a time; this creates potential for a high degree of stress and vulnerability. (Reference Bernabeo, Holtman, Ginsburg, Rosenbaum and Holmboe56) The doctor in training is in a precarious social and professional position. There is a level of invisibility and a lack of support if they encounter poor workplace culture. They have a short period of time to become part of the team, to ‘fit in’, to build relationships, to impress key individuals, and to achieve certain goals such that they are either furthering their own career or are in a position to do so. This often comes at the expense of their wellbeing and autonomy. The well-documented infantilisation of doctors in training reduces the capacity of a doctor in training to raise concerns, as they are often seen as too junior to make valid judgments. (Reference Chervenak, McCullough and Grünebaum57)
Training has been likened to an extended job interview, and can be as long as fifteen to twenty years. If unprofessional behaviours that everyone has either normalised or chosen to ignore are reported, the ‘whistleblower’ (Reference Jones, Blake, Adams, Kelly, Mannion and Maben58) will always be known as the one who broke trust. They are also at the mercy of the more permanent members of the team, who are often responsible for providing the assessments that will allow the learner to progress in training. Even the most motivated doctors recognise that there is a risk to their reputation if they raise concerns, and this means many will just try to get through a toxic experience or rotation. ‘I don’t think it will make a difference’, they say, ‘I don’t want to make a fuss. I don’t want it to ruin my career.’ (Reference Hewitt, Chreim and Forster59; Reference Rich, Viney and Griffin60)
Pressures grow as trainees have their own families and dual-career partnerships that dictate their location. Raising concerns about sexual misconduct or workplace culture problems within a specialty runs the risk of a trainee being ‘blacklisted’ within the community, particularly if those involved are core to the community. Despite this, during postgraduate training there are some protections afforded by being in a formal programme. Trainees typically have points of contact outside of their clinical training, such as training programme directors and/or specialist college liaison officers that may be based outside of their unit and able to provide confidential advice and assistance.
If not in a formal training role, a doctor’s position is even more perilous. These doctors are often directly employed and educated by the department they work in, typically for three to six month contracts that may or may not be extended. These positions are rarely accredited for training, so the specialist colleges have no governance in determining whether the job descriptions and/or support provided is suitable for a doctor in training. This vulnerability is further accentuated if the doctor is working on a visa, as their employment is critical to visa validity. Being out of formal training or on a visa can therefore make a doctor extremely vulnerable. As international medical graduates are more likely to be in these positions, this introduces an element of racism into which doctors are most vulnerable to sexual misconduct in medicine.
Managing Learning Environments
Medical education teams play a core role in establishing and maintaining quality control over learning environments. Bullying, harassment and discrimination in learning environments are connected to culture, and can go beyond the unprofessional behaviour of one individual. (Reference Rich, Viney and Griffin60) It therefore makes sense to have systems in place which capture and monitor the ‘health’ of the workplace, in terms of the safety and inclusion of groups of trainees who are required to work there. This process involves the development and operation of trusted and reliable reporting systems which collect data in an ongoing way, and which include mechanisms to investigate and intervene in areas where concerns are highlighted. This is not a ‘one size fits all’ approach; these systems need to be appropriately tailored to fit the needs and nuances of each particular workplace and its stakeholders.
There are a variety of approaches which have been adopted and evaluated at different levels, with varying degrees of success. Systems in place can include one or both components (gathering information and taking action), and can be at the level of the team or the institution or across state of national jurisdictions. In New Zealand, HOTSPOTS, a system designed to identify and tackle bullying, discrimination and harassment for medical students from one university, has now been implemented at a national level. Although focused on medical students’ experiences, it covers clinical workplaces in half of New Zealand’s District Health Boards, plus around 200 general practices. HOTSPOTS was implemented in clinical placement sites in New Zealand’s North Island in 2019, with an aim of improving psychological safety in clinical learning environments. Longitudinal data indicates that this has been achieved, with the number of HOTSPOTS reducing over time. (Reference Shionoya61)
HOTSPOTS is an anonymous, online, system for collecting and reporting medical students’ experiences of bullying, discrimination, harassment, inclusion and respect (BDH & IR) on clinical placements. Definitions of BDH are taken from the University’s definitions for those constructs. Quantitative data is collected by a six-monthly survey sent to senior students, which also contains links to existing pathways for making informal and formal complaints regarding BDH as well as links to support services, giving a clear ‘zero tolerance’ message and highlighting support services. This also makes the point that HOTSPOTS is an additional reporting mechanism to other existing processes. Aggregated student data allows identification of clinical sites which are ‘outliers’ in terms of concerning or excellent practices. Individualised reports are made for senior staff, containing that site’s data with some comparator data (but not disclosing data from other clinical sites). Meetings are scheduled between the medical programme and clinical leaders (chief medical officers and heads of departments), where HOTSPOTS reports are discussed, actions planned and follow-ups put in place. A summary of all actions taken is reported back to all students and staff, cementing trust in the HOTSPOTS system and boosting future response rates.
The HOTSPOTS system takes the known drivers of unprofessional behaviour into account. It tackles harmful workplace cultures, empowers ‘workers’ by giving them a method of speaking up, encourages social responsibility and increases managers’ awareness and urgency of issues. (Reference Deal and Kennedy62) HOTSPOTS also incorporates the essential elements of an intervention designed to address these issues. Although systematic reviews and meta-analyses in this area are lacking and therefore there is minimal evidence about the most effective interventions, previous studies have identified likely effective elements: a focus on behaviour change and methods of addressing systemic contributors.
HOTSPOTS incorporates the key dynamics to consider in an intervention designed to address unprofessional behaviour, such as harassment. (Reference Collier63) It seeks and addresses systemic issues without identifying individuals, has a clear mechanism of action with safe, anonymous reporting, is inclusive and not designed to target one specific group of people, and encourages bystander engagement. In addition, it was designed using a mixture of theory and implementation science with flexible components, where leaders can choose the most appropriate actions for their own context, as well as have transparent reporting mechanisms of issues identified and actions taken.
There are, however, challenges to the creation and implementation of such systems. Importantly, there is the fact that there are many stakeholders, who may have differing views about what information should be reported and what should not be reported, who collects the data, who is able to access it and how it might be followed up; therefore successful systems need significant collaboration. Data regarding health and safety issues are regarded as highly sensitive as it may be linked to complaints. This includes human resources processes or key performance indicators, and there may be legal issues as well as ethical ones to be taken into account. Indeed, the way in which a new reporting system might fit in with any already existing systems and policy is one of the key considerations in its design and implementation. The New Zealand experience of creating and implementing the HOTSPOTS system was that consultation took over two years for stakeholders to reach agreement.
A known challenge to reporting systems is lack of engagement by those who are being asked to provide data. This is commonly due to fears of lack of confidentiality, damage to reputation or career retribution. A system which is perceived as unsafe and untrusted, or where data can be accessed by those with a conflict of interest – such as a role involving trainee assessment or appointment – is unlikely to be successful. Unclear leadership is another factor, as lack of clarity regarding oversight, accountability, motivation to take action and following through with interventions will not effect change. Lastly, if reporting systems do not report meaningful data back to those at the frontline, this can foster doubt that actions are taken, and decrease trust and engagement with the system.
Supervision and the Problem of Hierarchy
Perpetrators often use the implicit trust in the student–teacher relationship to initially groom, then habituate their target to increasing sexual related contact. (Reference Stone, Phillips and Douglas53). Although emphasis on ‘trust’ in medical professionalism is apt, like most virtues it is a nebulous construct, which can be manipulated and abused. (Reference Shionoya61) Culture is defined by Deal and Kennedy, as ‘the way we do things around here’. (Reference Deal and Kennedy62) When the doctor in training has constantly shifting contexts, and ‘the way we do things around here’ is fluid, so it is understandable that professional norms are confusing and difficult to interpret. Medicine has a number of cultural norms and organisational structures which can be manipulated by sexual predators. Historically, doctors and medical students have been encouraged to repress their own needs for the ‘greater good’ of others. There is a view that professionalism is all about subordinating personal identity for a greater ideal. Michael Yeo, a philosophy professor at Laurentian University in Sudbury, Ontario describes this perspective on professionalism: ‘I subordinate my personal identity to the role – that is, essentially, what I think professionalism comes down to. If the core idea is symbolically putting on the white coat, you are able to put aside your own identity.’ (Reference Collier63)
As the more powerful person in the relationship, all medical educators, whether they are hospital-based or university-based, are responsible for managing student–teacher relationship boundaries. The boundaries between doctors in training and medical educators are personal, as well as professional. Learners in medicine have close relationships with their supervisors, partly due to the long hours and residential requirements of medicine, but also due to the nature of learning. Medicine can raise highly personal challenges. The nature of the work includes ethical, personal, spiritual and emotional threats, and doctors in training can turn to their senior colleagues for advice and support. This can mean a blurring of personal and professional relationships that can lead to highly positive interactions that shape a doctor’s career, or unacceptable boundary violations. Medical Educators should be guardians of safety, acting in the best interests of students. They are accountable should violations occur. Students, because of unequal power relations, may find it difficult to negotiate boundaries or to defend themselves against boundary crossing.
Boundaries are therefore negotiated, and contexts and roles change throughout training. This means the learner is highly vulnerable to boundary violation, because their understanding of appropriate boundaries fluctuates. It may be quite normal, for instance, for a rural supervisor to invite visiting students to a family dinner, particularly if the town has few options for an informal meeting and the supervisor is concerned that the student is feeling isolated and lonely. The same student may not realise that a similar invitation to the home of the Professor of Surgery in a busy urban teaching hospital may be a significant breach of acceptable professional boundaries.
The supervisory hierarchy is often the context in which sexual harassment occurs, because the learner is vulnerable; they depend on their seniors for teaching, supervision and academic progression. Medical educators may hold considerable institutional power and prestige, holding influential positions within a region or their specialty. In some medical training cultures, exploitation is expected. In return for learning opportunities and positive formative assessments, some will be expected to donate labour, including the ubiquitous unpaid overtime. This exploitation may even be formalised as patronage, where a patron expects their junior colleague to assist with domestic tasks, such as shopping, cooking, or childminding, in return for learning opportunities. (Reference Blunt, Turner and Lindroth64) Bribery is not uncommon. When exploitation is normalised like this, and hierarchical systems are not clear, junior colleagues are particularly vulnerable to other forms of abuse, including sexual exploitation.
In the literature around sexual misconduct, it is common to hear that the person responsible for safety or reporting was inappropriate or conflicted, perhaps because they were a friend or partner of the perpetrator, or were perpetrators themselves. Many in the education space feel profound senses of guilt, anger and shame about the knowledge that sexual assault, sexual harassment and rape are happening in spaces where the most vulnerable learners in the medical community exist. To manage these feelings, bystanders may ‘turn a blind eye’ to harassment to preserve their own power, prestige, privilege, and position in the professional community and/or succumb to cognitive dissonance to maintain their view of the profession as collegiate, professional and safe.
Interpersonal Dynamics in the Supervisory Relationship
Supervisory relationships are complex, and not all learners are treated equitably. (Reference Recupero, Cooney, Rayner, Heru and Price65) Doctors and doctors in training come into these relationships primed by broader expectations, and framed by the cultural norms of the workplace. Supervisors can express highly dominant behaviour, fuelled by existing privilege and reinforced by the hierarchical system in which they work. Gendered cultural norms can be reinforced by religion, science, morality, media, education, legal systems, culture and tradition. Because supervisors are often cossetted in their dominant position, there may be little motivation to change. (Reference VeneKlasen, Miller and Milligan66)
When supervisors exhibit dominant behaviour, learners can reflexively exhibit subordinate beliefs and behaviour, avoiding confrontation and resorting to indirect forms of responding. In focusing on what the supervisor wants and needs, they may be increasingly silenced, and develop self-deprecating and self-defeating beliefs, which can be weaponised to increase vulnerability when supervisors sexually harass or abuse their subordinates.
Power and Leadership
The shadow side of leadership is the misuse of power, (Reference Saxena, Meschino, Hazelton, Chan, Benrimoh and Matlow67) including sexual harassment, which is essentially an act of power and dominance. While there are many ways of understanding how power operates in medicine, in this chapter, we explore VeneKlasen et al.’s model of ‘power, people and politics’. (Reference VeneKlasen, Miller and Milligan66). The advantage of the model is that it grounds an approach to advocacy, using mutual support and collaboration to reduce social conflict and promote equity; VeneKlasen et al. believe that there is the potential for common ground if communities build collective strength.
VeneKlasen et al. describe four types of power:
1. Power over describes the formal and informal power structures that create hierarchy and increase or decrease agency in individuals.
2. Power with describes the ability of individuals to work together to advocate for change. Collective strength can be utilised to create change, and reduce the risk of the powerless being harmed in the process.
3. Power to describes the potential of an individual to shape their own lives and the world around them. The positive use of this capacity is the ability of individuals to provide and receive mutual support, and contribute to joint agency. When weaponised, it describes the ability of an individual with power to act on others in a way that increases their own agency, and diminishes or harms the other.
4. Power within describes the internalisation of beliefs about personal power and agency that shape and maintain vulnerability and agency. Power within describes a person’s sense of self-worth and self-knowledge and includes an ability to recognize individual differences while respecting others.
In the Table 14.2, the various roles of a supervisor are described using VeneKlasen’s model. It is normal to take multiple simultaneous roles in medical education. In Australian general practice, for instance, a supervisor may be an employer, teacher, mentor, sponsor and role model, as well as a supervisor. This means power can be augmented, but it can also be confusing. Supervisors can use multiple forms of power to influence the target, and this can mean the target is deeply vulnerable in the relationship.
Table 14.2 focuses on the negative implications of each relationship, but each relationship is grounded in a positive educational role. Ideally, supervisors provide exceptional workplace training, modelling good practice and facilitating learning. Mentors, sponsors and role models can be remembered for a doctor’s entire career, having a deep impact on their confidence, competence and career trajectory. It is this positive influence that means learners typically enter these relationships with optimism, openness and trust; it is an unfortunate reality that at times this trust is misplaced. Good supervisors can inadvertently enable grooming by others who are perpetrators, because the learner allows themselves to be vulnerable and trusting on the basis of previous positive supervisory relationships.
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Supervisors have legitimate organisational power, which means they can control access to learning tasks (e.g. allocating doctors in training to certain patients with certain needs). They can use this power to coerce juniors to comply by granting or withholding learning opportunities, or using feedback forms/incident reports to reward or punish. Senior doctors hold expert power by virtue of their knowledge, skills and abilities and can offer or withhold their knowledge and skills from doctors in training. They can also humiliate or embarrass learners. | Supervisors are in a workplace, and therefore exercise their power in public spaces. This means they can leverage the power of the team, and the social power of stigma and shame when they supervise in front of clinical teams and patients. They are members of a profession that the learner aspires to join, and have the organisational weight of the institution behind them. | Supervisors can use feedback processes to impede progression and restrict access to essential learning opportunities. They can build or destroy a learner’s confidence and reputation by disciplining them in front of colleagues. They can give or withhold the learning young doctors need. They can also provide formal or informal handover to future supervisors, affecting a doctor’s reputation. | Supervisors have the power to affect a learner’s sense of self-esteem and self-efficacy. They can organise a learner’s work schedule so that learning is more difficult, or the learner is less able to succeed. |
| Teachers have organisational and informational power, and are able to design and deliver curriculum according to their perceptions of the needs of doctors in training. Medical teaching can enforce hierarchies, especially when they use humiliation and flattery to manage their students. Teachers can teach or withhold teaching on equity, diversity and inclusion principles, and can emphasise/de-emphasise the importance of professionalism in practice. Teachers can give learners mental models to manage interpersonal conflicts in the workplace and encourage or discourage peer learning and peer support. They are usually responsible for managing reports of misconduct from teachers and learners. | Medical teachers operate in institutions, like universities or professional colleges. There is considerable referent power in the name of those institutions that allow them to exercise control over the learners. They also have the organisational power of evidence-based educational practice, which enables them to teach confronting material like equity, diversity, inclusion, ethics and professionalism. Some jurisdictions have the weight of Medical Boards, and their codes of conduct mandated, influencing curriculum and educational design. | Teachers decide who is taught through selection and how they are taught, including the use of peer learning, which can come with its own layers of power and influence. Teachers can prescribe remediation, and advance or restrict academic careers. Teachers set the dominant attitudes attached to a professional identity, and decide how learners understand what is expected in terms of interpersonal behaviour. Teachers manage the discipline of learners who don’t demonstrate appropriate behaviour and ensure learning environments are safe. | Teachers have the power to affect a learner’s sense of self-esteem and self-efficacy. This is particularly the case if the curriculum is overloaded, the teaching is not fit for purpose, or discrimination is normalised. They can model discriminatory attitudes that cause harm, and make certain students feel alienated and inadequate. |
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Assessors have legitimate organisational power, and career progression provides a powerful opportunity for coercion. Soft skills, like communication and teamwork, are particularly subject to conscious and unconscious bias in workplace assessments. In designing assessments, assessors have the opportunity to foreground or background unprofessional conduct | Assessors work with teachers and supervisors to regulate access to the profession by mobilising other educators and supervisors. They use institutional power to ground their assessment processes and decisions, and have institutional policies in place to support their decisions to remove learners from training. | Assessors have the power to remove learners from training and require them to undertake remediation. They also drive learning by setting assessment tasks. | Assessment is a high stress, high stakes activity, which is also expensive. Doctors are often perfectionistic and self-critical. Failure on assessment can have significant consequences for their careers and wellbeing |
| Managers have legitimate organisational power, making decisions around workload, work placement, accommodation and facilities, and work opportunities. Access to accommodations like leave and part-time work are subject to managerial approval. Managers also interpret and act on feedback from supervisors, patients and peers, and enact the policies of their organisation, including the management of consequences for employees who breach professional guidelines. | Managers work in a hierarchy, and use this institutional power to regulate learning. Managers use external sources of power, like law and regulation, to ground their policies, but also regulate when they are used. | Managers have the power to negotiate salaries and working conditions. They also employ the supervisors, so they are able to discipline supervisors who demonstrate sexual misconduct. They may also choose to discipline the survivor. | When managers follow institutional sexual harassment policies, many survivors report feeling invalidated and retraumatised. Many feel their privacy has been breached and experience stigma and shame. |
| Role models are granted informal referent power, using their influence to inspire and motivate others. They often operate via the hidden curriculum. By modelling particular attitudes and behaviours, they can improve trust in the team. They can also leverage their professional reputations to normalise less desirable attitudes like discrimination or hide less desirable behaviours, like sexual harassment. | Role models work within clinical teams, and can have significant groups of followers. In dysfunctional teams, this can mean weaker members of the team experience alienation, bullying and harassment by the ‘gang’ of followers. | Role models have the power to shift the dominant narrative in the workplace. In medicine, a role model can be an excellent clinician, but demonstrate harmful interpersonal behaviours. This can lead to inappropriate team behaviour and an unsafe workspace. | Poor role models can cause alienation, shame and loss of self-esteem in learners who are not accepted by the team. |
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Mentors can be informally chosen, and be granted referent power, but they can also be allocated as part of a mentor scheme, which grants them legitimate organisational power. Mentors have information and skills that can be shared, granting them power to coerce. | Mentors are usually respected members of the profession with considerable referent power. They can be charismatic leaders, which means they have a community in the profession who trust them. This means it can be challenging for the learner to identify them as untrustworthy. | As mentors, they can legitimately ask about personal life and experience, and this may lead to informal meetings in informal settings, which can be unsafe. They can also get to know their mentees well, and this knowledge can be weaponised to coerce learners. | Mentors can interpret and communicate their beliefs about the learner, and this can reduce self-esteem and confidence. Because the mentorship involves personal issues, this can mean interpreting the learner’s feelings and beliefs, and not just their professional performance. This can be a form of grooming. |
| Sponsors are often available to some and not to others. Sponsors have organisational power, including access to opportunities. They can choose to advance a doctor in training by offering opportunities (e.g. a clinical position or promotion, membership of a steering group, or an invitation to a professional dinner). Like patrons, they can use ‘favours’ in exchange for their sponsorship. Sponsors may privilege certain learners over others, leading to discrimination, e.g. the ‘boys club’ culture. | Sponsors usually bring a chosen learner into an existing group as a way of extending their networks and furthering their careers. The ‘boys club’ of medicine is based on this behaviour, and can amplify discriminatory attitudes. The advantages of developing a powerful network means the sponsor holds considerable power. | Sponsors can offer or decline to offer opportunities, and when offered can give or withhold support. | The inclusion or exclusion from powerful social networks affects personal and professional self-esteem. It can also influence a learner’s personal and professional identity. |
| Patrons have considerable organisational power, and in the communities where this role is normalised, learners have little choice but to comply with their requests or demands. In these settings, learners are vulnerable to being exploited, as they rely on their patrons for career progression, or even access to employment. Patrons can escalate their demands, beginning with culturally legitimate requests, but escalating to discriminatory behaviour or frank harassment and abuse. | Patrons exist in a powerful system that reinforces the subordinate role of learners and their own dominance. Patronage occurs in an existing social system where there is already bribery, corruption and favours as currency. Reinforcing that system in medicine reinforces other patriarchal norms and expectations. | Patrons can choose their learners, and can design abusive systems of ‘favours’ in exchange for learning, which increases the vulnerability of learners. | Patronage increases a learner’s sense that they are subordinate and decreases their sense of worth and agency. |
| Role | Power over | Power with | Power to | Power within |
|---|---|---|---|---|
| Leaders allocate precious resources: money, personnel, time and curriculum. They also decide how many people get to train, and who gets to lead. In a sense, they allocate power. However, they also negotiate with overarching organisations, influencing how governments allocate resources to their specialities or schools, and how much power they can wield. Within clinical environments, leaders negotiate the balance between service, research and learning, which can expand or limit their opportunities. | Leaders can influence entire systems, entrenching standards, expectations and structures that privilege some and disprivilege others. They also stand between the profession and the funders, including governments, influencing the impact broader policies have on the medical workplace. Because of their high position, they can be difficult to challenge. | Leaders have the ultimate say in a doctor in training’s selection into the profession, or their exit from the profession. They drive cultural expectations and have the capacity to influence the way the system behaves. | Leaders can have a powerful influence over a doctor in training, because of the steep medical hierarchy. This increases their capacity to silence targets, and increases their ability to cause sexual harm. |
Visible and Invisible Forms of Power and Agency
Senior clinicians have institutional power, but they also have considerable influence simply because their clinical mastery is recognised and respected. Foucault writes that ‘It is not possible for power to be exercised without knowledge; it is impossible for knowledge not to engender power’. (Reference Gordon and Foucault68) It is important to recognise the status this clinical mastery brings. In her victim impact statement, a survivor of sexual assault in Australia clearly articulates the importance of this power differential: ‘Before pleading guilty to these assault charges, the perpetrator used to hold a high position in a well-known cancer centre hospital and he was a respected member of the community. I, on the other hand, was still a trainee.’ (Reference Stone, Phillips and Douglas53)
The perpetrator in this case demonstrates both reputational power, which is invisible, and the power that comes with titles and roles, which in his case included his professorship. Visible power consists of the formal rules, structures, authorities, institutions and processes of institutional decision making. Policies can be part of structural bias, privileging one group over another or making it impossible for a subgroup to participate in the workplace fairly. An example is the capacity to work part-time, or to take maternity leave during training. While cast as ‘fair’, these policies impact women disproportionately, and are one reason why there is such profound gender inequity in medicine. Another is ‘bullying up’, where a more privileged junior doctor may intimidate their supervisor by using the privilege of their social status, such race, gender, class or other forms of privilege.
One unexpected impact of shifts in professional expectations is the over emphasis of individual power to influence systemic problems. For instance, in Australia, Good Medical Practice (69) outlines the professional expectations of doctors and doctors in training, and has made a number of recent modifications that place greater emphasis on the individual’s role in meeting patient needs. The guide details the expectations that the doctor will maintain productive collegiate relationships. It is normal in sexual harassment for survivors to question their role in the abuse, and this contributes to silence and shame. Encoding abuse as an individual problem contributes to this shame by inappropriately placing the responsibility on the survivor to manage their own harm, without recognising the broader roles and responsibilities of the systems in which doctors train.
Conclusion
Medical education is a complex field, with a variety of roles that are often inter-related and inter-connecting. Medical educators are responsible for deciding who enters training, and who graduates as a fully qualified specialist. They determine the curriculum, the way professionalism is taught and assessed, the competencies that are assessed at each level of training, and whether remediation opportunities are offered. In doing so, they manage learning environments, and develop the educational skills within the teaching team. This means they are responsible for monitoring professional conduct in teachers and supervisors, and addressing misconduct when or if it arises. They also take roles in monitoring and supporting the wellbeing of doctors in training.
Medical educators should ideally have advanced skills in describing, assessing, teaching and monitoring implicit and explicit learning. One of their key roles is to find effective, contextually sensitive and specific ways to assess interpersonal skills, behaviours and attitudes, and to use institutional power to manage the perpetrators of unprofessional conduct, including sexual harassment. In order to do so, they need to have sufficient institutional power to act on those assessments, ensuring learning environments are safe and learners are well supported.
Doctors often begin teaching as students during medical school, and as such the ‘medical teachers’ role varies from those with rudimentary near-peer tutoring to educational leadership in large institutions. Medical education is invariably part of larger systems which exercise considerable institutional power, creating hierarchies that can be leveraged to enable abusive behaviour to thrive, and significant potential for blurred boundaries.
Professionals build trust, by demonstrating ‘trustworthiness’ through an attitude of service to the needs of the community. Medical educators teach and model professional conduct from the earliest stages of medical training. Educational leaders ‘teach the teachers’ and should ensure professional behaviours are consistently modelled, whether the educator is a new tutor or the leader in a large institution. The academic work in this space involves developing, assessing and applying educational strategies to promote safe and effective professionalism learning throughout medical training, including the effective assessment and remediation of professional misconduct at all stages of professional development.
Introduction
Medicine, in training and in professional practice, has long contended with a culture that has turned a blind eye to bullying, harassing and abusive behaviours by members of its profession. (Reference Arnold, Zargham, Gordon, McKinley, Bruenderman and Weaver1; Reference Frank, Brogan and Schiffman2) The effects of bullying and harassment in the workplace can be far reaching and can affect more than the relationship between the victim and their abuser: there can also be a ‘ripple effect’ which can impact other work relationships as well as domestic relationships. (Reference Lewis and Orford3) Women, in particular, are at risk to be the victims of gendered forms of bullying or harassment. In a sample of clinician researchers, 30% of women reported having experienced sexual harassment compared with 4% of men. In one systematic review, staff, attending physicians, and senior doctors were cited most frequently as the sources of such behaviours. (Reference Fnais, Soobiah, Chen, Lillie, Perrier and Tashkhandi4) Women were also more likely than men to describe more severe forms of harassment (e.g. subtle bribery to engage in sexual behaviour, threats to engage in sexual behaviour, or coercive advances). (Reference Jagsi, Griffith, Jones, Perumalswami, Ubel and Stewart5)
For a variety of reasons, physicians are notoriously bad at seeking assistance when issues arise in their own lives, especially when they perceive that those issues may have an adverse impact on how they are perceived professionally. (Reference Sanfey, Fromson, Mellinger, Rakinic, Williams and Williams6; Reference Wear, Aultman and Borges7) Help-seeking behaviours can be impacted by a desire to not appear ‘weak’ to colleagues, loyalty to the team, (Reference Wear, Aultman and Borges7) or a fear of retaliation due to power dynamics within the work environment. (Reference Sanfey, Fromson, Mellinger, Rakinic, Williams and Williams6; Reference Wear, Aultman and Borges7) Concerns related to stigmatization (Reference Adams, Lee, Pritchard and White8) and confidentiality (Reference Bianchi, Bhattacharyya and Meakin9) can make it difficult for individuals to seek help when they are experiencing physical or mental distress. Given these barriers to care, it may be even more difficult for individuals to either report instances of harassment or abuse or seek help for symptoms that may arise as a result.
Decisions on whether to report harassment or not can become even more complicated, as terms such as sexual harassment and sexual abuse are often used interchangeably. When looking at female medical students’ experiences of sexual harassment, Wear, Aultman and Borges (2007) found that most ignored ‘sexual innuendo, explicit sexual banter, or crude language in general’ as just part of the culture of medicine, particularly in surgery. (Reference Wear, Aultman and Borges7) Students in this study also had different understandings of when something should be reported. For some, it was when comments moved beyond crude to degrading; for others it was when physical contact moved from ‘persistent arm, shoulder, or back touches’ to what felt like sexual touching. (Reference Wear, Aultman and Borges7) None of the women in this study had ever reported a colleague’s behaviour. Rather, the researchers found that students would alter their own routines to avoid known offenders (standing further away from a ‘touchy’ person, signing up for shifts to avoid working with a particular individual, or removing themselves from conversations). (Reference Wear, Aultman and Borges7)
These early experiences in medical school have an impact on professional identity formation, especially during clerkship, and creates expectations for what it is to be a ‘woman doctor’. (Reference Babaria, Abedin, Berg and Nunez-Smith10) Identity formation is a dynamic process achieved through socialization, which results in individuals joining the medical community of practice. (Reference Cruess, Cruess, Boudreau, Snell and Steinert11) Babaria et al. (2015) note that while female clerkship students were able to find ways to confront and respond to inappropriate behaviour from male patients, none of the women interviewed in their study felt able to confront or report inappropriate behaviour from male attendings. In their study, a few attendings (senior medical consultants or specialists) were responsible for the behaviour, but every participant over two service rotations reported inappropriate behaviour from them. These young women recognized the power dynamics in their situations and felt that reporting would only make their situations worse. The authors noted that for female clerkship students, having numerous inappropriate interactions with male supervisors reaffirmed their identity as one of a ‘sexualized token’, who was less valued in the hierarchy of medicine. (Reference Babaria, Abedin, Berg and Nunez-Smith10) Having these experiences early in medical training can have lasting effects on how women identify what it means to be a ‘woman doctor’ and may contribute to non-reporting of harassment later in their professional careers.
Culture of Medicine
The culture of medicine is complex, and sometimes contradictory. Many of us enter this career because we see it as a calling. We enter the first day of medical school with an elevated and idealized vision of the profession which never truly leaves us, and in turn, we pass that vision on to the next generation of learners. On the one hand, holding on to that idealized notion of the profession is not a bad thing, and may in fact help us through some of those days that are harder than others. The danger to clinging to this image of our profession, however, is that we may automatically become defensive when it is challenged. When we hear of a colleague who has sexually harassed or abused a trainee or a colleague, it may challenge our own professional ideals, leading us to try to justify or excuse the behaviours to maintain our sense of professional safety.
Compounding this complexity is the public’s view of medical professionals. As the rhetoric throughout the COVID-19 pandemic has made explicit, physicians are often viewed as heroes by the public. A fundamental tenet of the social contract that physicians have with the patients they serve is that physicians are meant to heal, and at the very least not to cause harm. According to Creuss and Creuss, (Reference Cruess and Cruess12) the public’s expectations of the medical community include not only the assured competence of their physicians, but also that physicians adhere to standards of morality, integrity and honesty, trustworthiness, and accountability, and that they support promotion of the public good. (Reference Cruess and Cruess12) Because of this, accusations or even rumours of sexual harassment or abuse can create patterns of cognitive dissonance which perpetrators can exploit. People are trained from a young age to trust physicians, and this can include extending the benefit of the doubt to physicians accused of sexual wrongdoings.
In Canada, we are guided by the CanMEDS Framework, which identifies and describes the abilities physicians require to effectively meet the health care needs of the people they serve. Within the Professional Role, competencies for physicians demand that we ‘recognize and respond to unprofessional and unethical behaviours in physicians and other colleagues in the health care professions’ and that we ‘participate in peer assessment and standard-setting’. (13) The framework articulates the ideal even as it recognizes that not everyone will live up to this standard and that it is up to all of us to hold individuals accountable.
A 2018 report from the National Academies of Sciences, Engineering and Medicine found that:
Greater than 50 percent of women faculty and staff and 20–50 percent of women students encounter or experience sexually harassing conduct in academia.
Women students in academic medicine experience more frequent gender harassment perpetrated by faculty/staff than women students in science and engineering.
Women students/trainees encounter or experience sexual harassment perpetrated by faculty/staff and also by other students/trainees.
Women faculty encounter or experience sexual harassment perpetrated by other faculty/staff and also by students/trainees.
Women students, trainees, and faculty in academic medical centres experience sexual harassment by patients and patients’ families in addition to the harassment they experience from colleagues and those in leadership positions. (Reference Johnson, Widnall and Benya14)
These findings may come as a shock to some people working in the profession who have either never experienced harassment or have not recognized harassment when they have witnessed it. The report identified a number of characteristics within medical culture that create higher levels of risk for sexual harassment to occur. These include:
Male-dominated environment, with men in positions of power and authority.
Organizational tolerance for sexually harassing behavior (e.g. failing to take complaints seriously, failing to sanction perpetrators, or failing to protect complainants from retaliation).
Hierarchical and dependent relationships between faculty and their trainees (e.g. students, postdoctoral fellows, residents).
Isolating environments (e.g. labs, field sites, and hospitals) in which faculty and trainees spend considerable time. (Reference Johnson, Widnall and Benya14)
Within this culture, it can be an incredibly daunting prospect for a victim of sexual harassment to come forward. There may be shame associated with being the victim of harassment, or fear of retaliation from the abuser or from the organization. Hart (2019) found that participants ‘were less likely to recommend a woman for promotion if she self-reported sexual harassment relative to otherwise identical women who experienced nonsexual harassment or whose sexual harassment was reported by a co-worker’ (Reference Hart15, p. 534). She also found that women who self-reported sexual harassment were perceived as less moral, warm, and socially skilled than the woman whose co-worker reported her sexual harassment. (Reference Hart15)
Consequences of Sexual Harassment
Individuals who have experienced a traumatic event such as sexual harassment, particularly from one’s colleague/supervisor/peer, are likely to have a psychological and/or behavioural response. The possible responses vary. They range from the most common responses, known as distress reactions, through to risky health behaviours and frequently psychiatric disorders (Reference Brower and Riba16).
Distress reactions commonly experienced include anger, demoralization, fear, a sense of increased vulnerability, irritability, lowered self-esteem, self-blame, humiliation, shame and increased self-isolation. Physical manifestations are common as a result of psychological distress and exposure to sexual harassment and trauma. This may include insomnia, nightmares and somatic symptoms including, but not limited to, headache, nausea, dizziness, muscle tension and fatigue. Individuals may engage in behaviours which further put their health at risk. Behavioural responses, which are often attempts to self-soothe, may include disordered eating, or increased tobacco, alcohol or cannabis use. Psychiatric disorders occur in some individuals following a traumatic event. Post Traumatic Stress Disorder, Depression, Generalized Anxiety Disorder, Panic Disorder and suicidal thinking are all potential outcomes of a traumatic experience such as sexual harassment. (Reference Johnson, Widnall and Benya14)
Superimposed upon these very common responses to sexual harassment are the aspects that are peculiar to the situation whereby a physician is harassed by a physician. Physicians are taught from a very early stage in their education about the necessity for Professionalism. It is an identified competence which needs to be acquired and maintained by all physicians. (13) Professionalism is taught and learned as an expression of the values held by physicians. It includes attributes such as honesty, integrity, and being trustworthy and ethical in one’s actions with patients, colleagues and administrators. It is at the core of medical practice and forms an essential component of medicine’s contract with society. (Reference Cruess and Cruess12; Reference Cruess, Cruess and Steinert17) The internal conflict that arises for the individual who has been sexually harassed is therefore profound. There is shock and a sense of disbelief. There is confusion about what has happened and whether they have in some way contributed to the situation. There is uncertainty about what to do, whether they should speak and to where might they safely turn. (Reference Stone, Phillips and Douglas18)
In the face of the contradiction between what is espoused in the profession and what has occurred, the individual finds themself in a tremendously vulnerable position. They are reluctant to seek care because of the established medical hierarchy and an existing power imbalance between themself and the leadership. They have concerns about whether there will be confidentiality should they report their experience, and questions about the potential consequences they will face. Will this affect their career and if so, in what way? Will there be retaliation and if so from whom? Will their peers provide support, or will they face ostracism? There is a fear that they will not be believed.
This uncertainty falls on a previously well-established foundation of reluctance that most physicians feel when needing to seek medical care, particularly mental health care. A systematic review of the literature conducted by Kay et al. (Reference Kay, Mitchell, Clavarino and Doust19) revealed that 71% of doctors described themselves as embarrassed when seeing another doctor. This embarrassment was reported in multiple articles as heightened if the physician was experiencing a mental health problem. Admitting to not only needing care but needing to reveal the circumstances of being traumatized because of sexual harassment by a colleague is doubly shameful.
Given that there may be multiple very serious and detrimental responses to being sexually harassed by one’s colleague, it is imperative that health care providers be prepared to provide appropriate interventions. Each individual who has had this traumatic experience will be in need of support including supportive care. Most people who have experienced harassment will have symptoms. The goals of care are to reduce their levels of distress, assist them to restore their confidence and sense of competence, and minimize the possibility of ongoing, longer-term symptoms and impairment. Recognizing that some individuals will require a more formal intervention, it is critical to have access to a therapist who is experienced in, and knowledgeable about providing, health care to physicians. (Reference Myers and Gabbard20)
Therapist’s Perspective
An experienced therapist will be well prepared to engage with a patient who has experienced trauma, including sexual harassment or assault. (Reference Johnson, Widnall and Benya14) However, the presentation of a patient, who may be a medical student, resident or colleague, may be particularly challenging. The physician therapist can relate to the medical practitioner who is presenting to them as a patient and therefore they will be able to understand, and empathize with, this individual. However, if the therapist is an attending physician in the same organization in which the harassment/assault occurred, there will almost certainly be a personal response. The physician therapist is also a colleague and peer of the identified perpetrator. The initial response may be one of disbelief. This could be expected and certainly exaggerated if the identified perpetrator is well known throughout the organization and/or an organizational leader. This has been referred to as the Therapist’s Dilemma. Where does one’s loyalty lie? A therapist cannot provide care to a patient if they are unable to accept the veracity of the patient’s experience. If that were the situation, the therapist would necessarily withdraw from the provision of care and arrange for a colleague to assume that role.
Much more likely is that the physician therapist may have initial responses of shock, disappointment, and disillusionment. This treating physician shares the same cultural heritage referred to above with respect to the profession. There is almost certainly an existing pride and loyalty to the profession which has now come into question. Where are the standards that the therapist has come to rely upon, as guidance for professional behaviour, being upheld? Who is responsible for ensuring that these standards are in place as policies and also being respected in terms of process? How will the duty of confidentiality influence the therapeutic process? How will the engagement in therapy influence the therapist’s relationship with their organization and its leadership? These questions and more will be challenges that the therapist will need to reflect upon and consider very carefully as they enter into a therapeutic relationship with the individual seeking care. These issues have the potential to put the therapist into substantial personal conflict. Their commitment must be primarily to the patient if they have accepted the responsibility of providing care. They therefore must recognize the potential impact on their collegial relationships within the organization and be prepared to navigate that reality.
Responsibilities
One aspect that the therapist should consider is any legal responsibilities they may have within the jurisdiction in which they practise. The laws relating to duty to disclose vary from country to country, and even between geographic regions within countries. In Ontario, Canada, the College of Physicians and Surgeons of Ontario mandates a duty to report when a physician has committed a sexual boundary violation with a patient. There is clear policy detailing appropriate and inappropriate behaviour for physicians towards their patients. (21) However, there are no such clear policy protections for professional boundary violations between physicians.
As discussed in detail in the chapter on medical regulation (chapter 13), many countries lack clear legal obligations or guidelines for how to handle physician sexual boundary violation with colleagues, and therefore, issues of whether to report or not are relegated to the far murkier category of ethical obligations. Both the Canadian Medical Protective Association (CMPA) and the Canadian Medical Association Code of Ethics and Professionalism include provisions for an ethical responsibility to report unprofessional behaviour by colleagues. (22; 23) In both documents, the suggestion is to report unprofessional behaviour to an ‘appropriate authority’ such as the chief of the department.
When the physician therapist discovers this unprofessional behaviour about a colleague within the context of a therapeutic relationship, that guidance becomes far less clear. The physician therapist may find themselves questioning where their ethical obligation lies in this case: with the profession or with the patient? Reporting the offender may feel like the ethically responsible thing to do for the safety of the profession, but doing so against the wishes of the patient risks irrevocably damaging the therapeutic relationship. It is important to understand that patients seeking treatment for sexual harassment, assault or trauma are on a path towards healing, and that while they may not wish to disclose or report initially, they may want to at some point in the future. Building a strong therapeutic relationship based on trust will allow discussions about reporting to be part of an ongoing conversation.
Approach to Therapy
Recovery from trauma is not an easy journey. In this case, the trauma itself is exacerbated by the violation being executed by one’s own colleague. Therefore, therapy must be approached first and foremost from a position of establishing an environment of safety. It is critical to remember that those who have suffered from being sexually harassed are very vulnerable. The creation of a safe therapeutic environment with a therapist who is trusted and engaged holds greater promise for recovery. It is important, therefore, that the therapist understands the science of safety and the need to establish trust and the social engagement system. This is knowledge that is encompassed within the polyvagal theory and is beneficial knowledge for therapists who are embarking on this type of therapy. (Reference Dana24)
The polyvagal theory was first described by Stephen Porges in 1994 (25) and has contributed substantially to our understanding of the biology of safety and danger, as well as the complex connection between our brain, mind and body. Over the past two decades trauma therapy has been based increasingly on an understanding of neuroscience. It therefore holds the possibility for multiple approaches to therapy. It is critical to understand that ‘there is no one “treatment of choice” for trauma’ (Reference Van der Kolk26, p. 214). There are multiple approaches to therapy with the potential to ameliorate the patient’s symptoms and assist them to increasingly regain their ability to self-regulate.
Although there is currently a penchant for what are described as evidence-based therapies, addressing the complexity of the impact of trauma necessitates the recognition that one size will not fit all. Research that has been conducted in neurobiology and psychotherapy has shown that the brain can change and adapt to facilitate recovery from trauma. Therefore, being sensitive to the needs of this individual patient and having multiple modalities at hand will inform the therapeutic trajectory for this patient.
Trauma therapy includes approaches to the development of relaxation skills including a focus on breathing. Focused breathing exercises can change both the brain and physical symptoms in the body. Trauma therapy also includes body-based approaches: grounding techniques; movement-based techniques, such as yoga; through to Somatic Experiencing; (Reference Levine27) Somatic Therapy; (Reference Rothschild28) mindfulness; and meditation practices.
Trauma therapy also incorporates cognitive strategies including Cognitive Behavioral Therapy, Prolonged Exposure, Eye Movement Desensitization and Reprocessing, and Internal Family Systems therapy. This list is not exhaustive but reflects the complexity of the patient who has had a traumatic experience and the multiple ways that the therapist may approach the treatment. The treatment will be determined by the presenting status of the patient and influenced by their personal journey through the therapeutic process.
Finally, in terms of the approach to therapy it is essential that the therapist is cognizant of the inevitability that this patient will be experiencing an underlying sense of shame. This experience is a common phenomenon for victims of trauma and most often exacerbated when one is traumatized by someone to whom the victim was close or dependent upon (Reference Van der Kolk26). For this reason, the therapist must understand that the very first phase of therapy that is required, which is the establishment of a relationship of safety and trust, may be a slow process which requires time and patience. Rothschild, an expert trauma therapist, identifies that the ‘alleviation of shame’ and ‘self-forgiveness for not being able to prevent or stop what occurred’ are two of the key issues in trauma therapy (Reference Rothschild28). In all cases, well-informed therapy is likely to include a focus on self-compassion.
Quite clearly it is evident that the scenario is complex and extremely challenging for the physician who finds themself in the situation of having been assaulted. It poses a problem which may seem to be insurmountable. With a skilled and experienced therapist who has a wide range of tools in their armamentarium, a goal of stability, with the associated ability to cope and self-regulate, is possible.
Conclusion
The pervasive culture of bullying, harassment, and abuse within the medical profession has far-reaching consequences for individuals, as well as the culture of the profession. The fear of retaliation, stigma, and career repercussions often silences victims, perpetuating a cycle of harm. To address this problem, it is essential to create a culture of respect and accountability within medical institutions. This includes offering intelligent, personalized mental health support services to victims and survivors. Additionally, it is crucial to foster a supportive and inclusive environment where individuals feel able to speak up and seek help without fear. By prioritizing the wellbeing of health care providers and promoting a culture of respect, we can create a healthier and more equitable medical profession.
Introduction
In this chapter we discuss issues faced by doctors in relation to sexual abuse. We consider organisational and institutional factors such as cultures of workplaces which can either predispose or help prevent occurrences of sexual abuse. We discuss principles and arguments for an interdisciplinary and generalist approach in the management of individuals exposed to sexual abuse, using a case discussion as an example. We also discuss the application of an integrated approach to influence change in systems at scale to reduce prevalence of sexual abuse.
In considering the integrated approach, we describe the remits of postgraduate medical training, regulatory organisations and legal systems in the UK. It is likely that similar systems and processes exist in other countries as well – the important matter is the transferable processes and issues rather than specific frameworks. We reflect on impacts for doctors subject to sexual abuse, and the range of resultant health and professional issues. Where relations between doctors have deteriorated to the level of sexual abuse, we highlight a range of other professional breaches we have also encountered, which may further compound the negative impacts and long-term health of the victims. We take the view that the possibility of such further complexity be explored in cases of doctors abused by doctors.
In order to respond, we describe principles that allow a holistic approach to be taken to address wide ranging impacts on victims. We consider factors in medicine which may lend themselves to abuse of positions of trust to raise awareness. We recommend changes to the management of doctors in training and culture of health care systems to reduce incidence, react with compassion and fairness, and reduce the negative impacts – both personal and professional – to the doctors involved.
Earlier parts in this book have documented what is currently known about sexual harm of doctors by doctors. Research into causes, prevalence and impact of sexual harassment and abuse in medicine (Reference Ceppa, Dolejs, Boden, Phelan, Yost, Donington, Naunheim and Blackmon1; Reference Vargas, Brassel, Cortina, Settles, Johnson and Jagsi2) is being undertaken. It is clear that sexual harm has been and is a common experience, (Reference Fnais, Soobiah, Chen, Lillie, Perrier, Tashkhandi, Straus, Mamdani, Al-Omran and Tricco3) and it has highly significant impacts for victims, including detrimental physical, mental, social and occupational sequelae. (Reference Vargas, Brassel, Cortina, Settles, Johnson and Jagsi2; Reference Lim and Cortina4) Risk factors identified by Bhaji and Altomare (Reference Bahji and Altomare5) for all forms of discrimination and harassment (not just sexual) included training status, gender, ethnicity, culture, sexual orientation and language spoken. The significant majority of perpetrators are men, (Reference Halim and Riding6) and the structure of training, power differentials and dynamics of work in medical workplaces (Reference Ceppa, Dolejs, Boden, Phelan, Yost, Donington, Naunheim and Blackmon1) can create environments where perpetrators’ behaviour is both triggered and difficult to address. In chapter 3 on ‘the role of men’ we discuss why sexual abuse occurs in the medical workplace in greater detail.
What We Know about Sexual Abuse of Doctors by Doctors
Sexual abuse is defined as unwanted sexual attention, which can be verbal or non-verbal, and involve coercive behaviours or unwanted physical contact, through to violent assault. (Reference Lim and Cortina4; Reference Fitzgerald, Gelfand and Drasgow7) As noted in the #metoo campaign, (Reference Burke8) coercion into sexual favours linked to suggestions of opportunities for career advancement also occurs within medicine. (Reference Bhattacharyya9) This leads to a pernicious situation for victims, who have invested several years of study and naturally hold career aspirations, then being in a position of fear that disclosure will negatively impact their future careers.
Research into causes, prevalence and impact of sexual harassment and abuse in medicine (Reference Ceppa, Dolejs, Boden, Phelan, Yost, Donington, Naunheim and Blackmon1; Reference Vargas, Brassel, Cortina, Settles, Johnson and Jagsi2) is being undertaken. Results show significant negative impacts on physical and mental health (Reference Lim and Cortina4) as well as confidence at work. Even the mildest form of abuse (persistent verbal sexualised attention) can impair career progression due to these negative health impacts. Furthermore, studies show that victims are often reticent to report, citing perceptions of negative reactions from colleagues, fear due to power differentials between perpetrator and victim, concerns that confidential access to supportive systems may be lacking, and worries that negative effects on career progression, health and feelings of self-worth (Reference Lim and Cortina4; 8) will result. Therefore, it is incumbent upon organisations and systems such as health care employers, postgraduate medical education bodies and regulators (e.g. General Medical Council) to listen, offer a safe space to disclose and then act effectively.
To consider systems factors that may predispose to abuse within health care settings, or conversely reduce risk, we need to visit evidence highlighting prevalence of abuse, and any relevant individual or organizational risk factors. We consider a range of international systematic reviews in relation to medical sexual abuse to understand who the victims may be.
The experience of abuse is common among the health care workforce and has negative impacts. Fnais et al.’s (Reference Fnais, Soobiah, Chen, Lillie, Perrier, Tashkhandi, Straus, Mamdani, Al-Omran and Tricco3) international systematic review revealed statistically significant greater harassment of women. A systematic review on bullying, undermining behaviour and harassment in the surgical workplace by Halim and Riding (Reference Halim and Riding6) showed increased rates of sexual harassment in women across a number of countries, disciplines and contexts. Such experiences impact career decisions, with students moving away from specialties where they experienced harassment. (Reference Ceppa, Dolejs, Boden, Phelan, Yost, Donington, Naunheim and Blackmon1; Reference Halim and Riding6) Risks for medical students seem to be more pronounced for women, ethnic minority groups and LGBT students. (Reference Vargas, Brassel, Cortina, Settles, Johnson and Jagsi2; 6) A study of fourteen US medical schools (10) showed that 83% of female respondents had suffered sexual discrimination or harassment, while 41% of male medical students also had this experience. The effects on this group of wider bullying and harassment included stress, poor work satisfaction, depression, and suicidal ideation. More broadly, risk factors identified by Bhaji and Altomare (Reference Bahji and Altomare5) for all forms of discrimination and harassment included training status, gender, ethnicity, culture, sexual orientation and language spoken, in that order of prevalence.
Who are the perpetrators of sexual abuse in medicine, and how do they interact with victims? In their 2019 report, Searle et al. (Reference Searle, Rice, McConnell and Dawson11) consider the 275 cases in the UK of a range of clinical health care professionals where sexual misconduct with either colleagues or patients was reported to the health care regulators. Eighty-eight per cent of the perpetrators were male. Of those in the study who were doctors, 100% of the 94 perpetrators were male. Colleagues were the target in 32% of all cases, and in 54% the location of abuse was the workplace.
In chapter 3 on the role of men, we discuss theories to explain why sexual abuse in the workplace may occur, including the four factor theory, (Reference O’Hare and O’Donohue12) which cites individual psychological factors alongside those individuals overcoming personal or organisational restraints. These themes have been developed further in the creation of scales such as the ‘Likelihood to Sexually Harass Scale’. (Reference Pryor and Wesselmann13)
The UK literature evidences increased prevalence of sexual abuse within medicine where predisposing vulnerabilities of the victim exist. (Reference Ceppa, Dolejs, Boden, Phelan, Yost, Donington, Naunheim and Blackmon1) Very often there is disparity in power, both in terms of seniority and commonly also in gender. We explore these themes in more detail in chapter 3.
Environments Where Abuse Takes Place
If we are to reduce prevalence of sexual abuse within medicine, and also to manage cases effectively, we need to consider environmental factors. Searle et al. (Reference Searle, Rice, McConnell and Dawson11) report on the types of workplaces where incivility is common or tolerated. She describes the link between this and professionals losing connection with their professional standards of behaviour, in the extreme leading to sexual abuse. Several potential predisposing factors exist within medical environments. Firstly, power imbalances (Reference Haque and Waytz14) create fear of negative personal and career impacts arising from disclosure. Secondly, a high-pressure environment, long hours and disruptive work patterns impact on work-life balance. This can lead to feelings of dehumanisation (Reference Haque and Waytz14) and increased risk of perpetrating abuse. Some signs of dehumanisation include loss of empathy and moral disengagement, factors also noted in those perpetuating sexual abuse.
Parallels in terms of loss of empathy, responsibility and moral disengagement were found when professionally led self-regulatory systems failed in terms of patient care in the Bristol and Mid Staffordshire scandals. Here the adverse events were poor patient outcomes, but again with environmental culture highlighted as one where poor professional behaviours were thriving. Investigation revealed inappropriate protection by the organisation of colleagues whose performance was poor, failure to proactively investigate poor outcomes, and negative treatment of whistle-blowers. (Reference Pryor and Wesselmann13) If we are to respond appropriately to disclosure of sexual abuse in the medical profession and address under reporting, it is imperative that such organisational failures in self-regulation are addressed.
The Professional Standards Authority (PSA) (Reference Francis15) in the UK acts to improve the regulation and registration of health and social care workers, and the organisations they work for, with the ultimate aim of protecting patients. The PSA’s first published guideline provides a framework to support the prevention of sexual abuse and the care of victims and provides a framework for reporting. (16) Sadly, sexual abuse still occurs and remains underreported in the National Health Service (NHS). (Reference Searle, Rice, McConnell and Dawson11)
We have drawn attention to cultures predisposing to abuse and should also consider the converse. Many organisations build better cultures, protect patients, and manage professional groups by effectively self-regulating through a range of both formal processes and informal peer networks. Such networks involve the sharing of ideas around professional values. Examples of formal protective processes include identifying Freedom to Speak Up Guardians in each trust or developing educational supervisors and programme directors who undergo regular accreditation and feedback from learners. Freedom to speak up within the NHS comes under the remit of the National Guardian’s office. It is an independent body with the remit of driving culture change in the NHS and promoting disclosure regarding any issues which may adversely affect patient care. There are appointed Freedom to Speak Up Guardians in each NHS Trust who promote disclosure and to whom staff can disclose any concerns.
Sanfey and Ahluwalia (Reference Sanfey and Ahluwalia17) describe the value of increased clinical engagement to develop open cultures and early self-correction both individually and organisationally, leading to a high-functioning NHS organisation. The professionalism discussed is focused on behaviours that improve clinical outcomes, although other professional behaviours are also considered. Further research would be needed to consider if their proposed approach also applies to prevention of sexual abuse in the health care workplace.
Critical to the development of an effective self-regulating workplace is the empowerment of bystanders to act when seeing and hearing behaviours that are part of the slippery slope towards sexual abuse. This has been noted to be a current weakness in many health care settings (Reference Flynn18), and if any of the 25% to 83% (19; Reference Park, Cho and Hong20) of health care workers citing sexual harassment could be protected before attack or outright abuse occurs, positive impacts across our systems would be substantial. Secondly, rigid hierarchy is also cited as a significant risk and especially when this results in a more significant gender and power imbalance at senior compared to junior level. (Reference Flynn18) Work within health care settings to encourage open reflection of all professional and team behaviours across professional levels and groups would do much to empower both bystanders and potential victims to act before matters have deteriorated. Research into the optimal organisational response to early stages of sexual harassment would also be helpful. Where sexual abuse has occurred, clearly there is a need for significant accountability, and its lack has been cited as a frequent reason for failure to report. Much may be learnt from other organisations. Buchanan et al. describe strategies developed in the US military, including the need for regular self-assessment of the organisation for harassment. (Reference Buchanan, Settles, Hall and O’Connor21) They recommend education and policies on prevention, open systems to allow disclosure, decisive action and remediation.
| Potential impact | Cultural factors in the workplace |
|---|---|
| Increased likelihood of abuse |
|
| Reduced likelihood of abuse |
|
We now consider the scenario where sexual abuse of a doctor in training occurs. Within the NHS, there is organisational provision responsible for postgraduate medical training. Within this education and workforce arm of the NHS, a network of trained educational supervisors and directors of medical education exists. Educational supervisors include training programme directors who run regular educational groups for their training cohorts, coming to know them well, and who often are the trusted mentors to whom events are disclosed. A training programme director in the UK is a postgraduate educator employed to provide education, career and holistic guidance during training. Training for supervisors includes developing skills in provision of educational supervision and pastoral care, encouraging peer support, and promoting a culture of multi-source feedback.
In addition to support/provision from the postgraduate medical education body, the employing NHS providers will have clinical supervisors who oversee daily clinical practice, also directors of medical education who have oversight of their educational provision and educational teams. Health care settings have access to human resources departments, and more recently in the UK Freedom to Speak Up Guardians and guardians of safe working who have a specific remit to be a point of contact for reports of any concerns around workplace behaviours or working patterns. However, people in these roles do not as yet have specific training in managing sexual abuse of doctors. Not all abuse is managed within the organisation. Some are reported directly to the police, particularly if the abuse involves an attack, acute intimidation, or administration of drugs.
It is clear that the management of a doctor who has suffered sexual abuse will involve understanding a range of their needs, which may span health, education, employment and legal aspects. Offering a holistic understanding of the range of these issues and having the ability to work with the doctor concerned through an integrated and person-centred approach opens opportunities to effectively address the concerns and impacts being experienced. This is similar to the skills used by generalist clinicians in their medical practice, offering opportunities to tackle complex, uncertain and dynamic situations (19) where, clinically, doctor and patient together actively explore and interpret the issues and context. In the case of abuse of doctors by doctors, where the victim may find difficulty seeking and accepting help, such an approach may be empowering and much needed in view of the complexity of the problems being faced. Reeve (Reference Reeve22) describes the use of exploration and interpretation, or interpretive medicine, as helping to unleash creative capacity for progress during the experience of illness or effects of trauma. We propose that such an approach provides a strong theoretical foundation for working with abused doctors and clinicians.
It is essential that victims have the element of choice in terms of disclosing abuse. Choice of confidante may be based on developing earlier trust or on recommendation from a peer, and personal preference is sometimes influenced by factors such as age or gender. Some victims prefer the confidante to be a close and supportive colleague, while others prefer as much anonymity as possible, so disclosing to someone removed from their work environment. In addition to concerns about disclosure on career progression and attitude of peers, sensitivity should be shown to the fact that by disclosing such events, the doctor may feel they have exposed a very vulnerable and personal part of themselves. Disclosure itself to another member of the medical profession may in itself feel like a breach of personal boundaries, so as supervisors and medical directors we must ensure that victims feel safe, protected and respected at all times.
Interventions through an Integrated Lens
We now move on to consider interventions, within the UK organisational framework. Mental health issues in doctors are common, (Reference Brooks, Gerada and Chalder23) disclosed late, frequently severe, can involve self-medication due to access to prescribing, and may require specialised help. In the UK, the Practitioner Health Programme (Reference Brooks, Gerada and Chalder24) and NHS Practitioner Health (25) are free services for doctors with mental health, alcohol, or drug related problems where they can be seen confidentially. These services have been instrumental in assisting the management of the cases known to us where sexual abuse has led to mental health issues. Therefore, our recommendation is that where sexual abuse is disclosed, the victim be referred to a confidential medical service.
In our experience of managing perpetrators of sexual abuse, consideration needs to be given to whether the perpetrator has committed an offence and whether they have breached their duty as a doctor (26) and also as a supervisor (if in this role). A complex role for case managers ensues, such as reporting abuse to the appropriate regulatory authorities as a responsibility in protecting the public and staff, and in upholding the profession’s standards, and considering the legal implications of the abuse, including reporting to the police where appropriate. In addition, teams should have an awareness of issues for perpetrators who frequently suffer psychological and physical consequences in the aftermath of discovery, and note that there is an increased suicide risk in doctors undergoing investigation. (Reference Horsfall27) Therefore, alongside support for victims and referral of the perpetrator to appropriate bodies, case managers should make perpetrators aware of the potential need to access medical or psychological assistance for themselves.
Timely health care, education and career support and appropriate time off can transform outcomes to for victims of sexual harassment. The failure to arrange support or address such issues can have significant consequences for the victim, organisation and even patients, if judgment is impaired due to ill health. In one case managed by our team, clinical judgment of the victim remained impaired for some years, leading to a breakdown in employer relationships and referral to the General Medical Council. This not only led to ongoing emotional trauma but also to negative career impacts. Even if realisation of complex professional breaches comes late, with careful case management, medical assistance, and astute perception on the part of the regulator regarding the complex and non-recurrent causes of the professional breaches, career and health can be restored.
The maxim ‘first do no harm’ should be considered in relation to unintended consequences of organisations involved in medical education, regulation and employment. Examples where inadvertent harm could be caused include situations where different organisations have jurisdiction over the two parties in the sexual abuse and use different thresholds for action. This can sometimes lead to perceived inequity in the management of the different parties. For example, a victim, encouraged to move geographically to another place (for work and protection), also stands to lose familiar environments and peer-support networks.
It is not uncommon for differing views regarding the management of perpetrators to emerge as well. We have experienced differences of opinion in relation to the threshold at which perpetrators should be referred to regulatory authorities for breaches of trust such as the prescribing or administration of medication to victims. One of the previously published concerns of victims of abusive sexual relationships, (Reference Watters and Hillis28) regardless of professional group, has been that not only is there an abuse of power inherent in the case, but that the perpetrator with higher career status is perceived to be less likely to have negative career consequences. This can magnify the feelings of injustice, and in our opinion this is an area for the relevant organisations to keep in mind in the handling of such cases. If inequity of outcome were to be addressed, it would be likely that victims would feel empowered to disclose. Beyond this, there is evidence that work can be done to improve the self-regulatory potential of organisations (Reference Miedema, MacIntyre, Tatemichi, Lambert-Lanning, Lemire, Manca and Ramsden29) and improve their protective influence. Our recommendations would therefore be to take organisational level action to reduce the incidence of abuse, facilitate early disclosure, and ensure that organisational barriers do not further disadvantage victims of abuse.
When dealing with cases of abuse among doctors in training it is common practice to offer colleagues a safe space and supportive case manager to explore the wishes (with regards to dealing with their trauma and concerns) of the doctor, sensitively screen for the full range of possible (physical, psychological, educational and social) complications, and outline options for further help. It is common practice for the care and management of doctors in such difficulty to be undertaken by a team of professionals that includes a senior clinical educator (acting as a responsible officer) and senior managers with expertise in managing such complex situations. All cases involving alleged sexual harassment or abuse would be discussed regularly, negotiating a firm plan of action that remained in place until a satisfactory conclusion had been reached. This team can ensure that the affected learner is directed to appropriate resources and services including the practitioner health programme, (30) occupational health, professional support unit, and legal support, and liaise with employing organisations where abuse is alleged to have taken place. The professional support unit sits in each region. It provides a free service for doctors and other health care professionals in training to address a range of issues which can impact on confidence and progression in training. It typically sits independently of specialty training schools, which can be beneficial to provide separation from any structures where the perpetrator works.
| Service | Reason for recommendation | Services offered |
|---|---|---|
| Case management |
|
|
| Employer |
|
|
| Police and legal action |
|
|
| Occupational health |
|
|
| Practitioner Health Programme |
|
|
| General Medical Council |
|
|
Reflections from Experience
In this part we share reflections drawn from our experience of managing trainees who have directly or indirectly experienced sexual abuse. We have also drawn out themes from an anonymised case study from another participating country to protect the identity of the victim. In our experience looking after doctors in training, most cases involved women abused by men. The effects of such abuse have resulted in complex mental and physical ill health, as well as affecting work performance and relationships. Most commonly there has been a significant power differential such as supervisor–supervisee or a line manager relationship where there has been an abuse of trust.
By the very nature of sexual abuse there has been a breach of ethical and professional standards, and in our experience, this may spread across several professional domains beyond that of sexual abuse. We recommend that managers of such cases should be alert to this possibility. Transgression of professional boundaries, in addition to those of a sexual nature, may occur during or in the aftermath of sexual abuse. Medication abuse is one such example. Drug administration by the perpetrator is a rare but devastating action as part of sexual assault, made more likely by doctors having access to medications. In a number of cases we managed, psychotropic medication (normally used for anaesthesia or pain relief) was obtained either to perpetrate a sexual assault or prescribed as part of an ongoing abusive relationship, both resulting in significant psychological harm to the victims. Further complicating health factors resulting from abuse can include a range of sexual health and reproductive issues, severe mental health disorders and self-harm. Breach of professional and sexual boundaries on organisational premises may also affect other colleagues and patients, if any events are witnessed or suspected
Consideration of Illustrative Case
The case in Table 16.3 brings together several issues which need to be considered in the context of this book related to the perpetrator and the victim. Taking an integrated approach to support the victim and in the management of such a case is essential.
| May is a twenty-nine-year-old registrar in obstetrics and gynaecology, working in a major teaching hospital in London. She is the only daughter in her family and immigrated to the UK as a young child from Singapore. Her parents have high expectations of her, and she has worked hard all her life, with academic scholarships and extracurricular achievements in music. She graduated with honours and decided on a career in obstetrics and gynaecology after her clinical rotation in this discipline as a student. |
| Although she has a good academic record, May has had some difficulty as a foundation doctor. She is slight and softly spoken, and somewhat anxious, and she has found it difficult to assert herself in clinical teams, often staying back late to ensure things are done well. She admits she has always been a perfectionist. May had a long-standing relationship with another medical student at university, but she broke up with her boyfriend when she decided he was ‘too controlling’. |
| This is her first term as a registrar in the Obstetrics and Gynaecology team. She has found the term very difficult, as she sees the other registrars as ‘more extroverted and definitely more competent’ than her, and she has had trouble maintaining her confidence. In addition, there have been some interpersonal issues with the midwives on the wards. |
| One of the consultants on her team is a highly respected senior obstetrician, with a reputation as an excellent gynaecological surgeon. However, she has been feeling increasingly uncomfortable with his behaviour and his comments recently. At first, she felt singled out as he was very encouraging, and commented that ‘he always felt safe leaving his patients in her hands’ because she ‘went above and beyond to care for them’. He seemed interested in her as a person, and asked her about her family, and her support system. However, his remarks have become more personal, with comments about her appearance, with a recent comment ‘your ex-boyfriend doesn’t know what he’s missing out on’. He invited her out for dinner one night when she was working late, and although she declined, he has continued to ask her again and text her after work so she can ‘meet him for drinks’. Because she feels isolated in the team, she hasn’t felt able to disclose this to her fellow registrars, but she became increasingly anxious about seeing him at work. At one point, she was sure he followed her home. |
| Last month, he was assisting in theatre on a gynaecological operation, and he insisted she suture one of the incisions. He stood behind her, giving her instructions, and she could feel his erect penis rubbing against her back. She was aware that there were other members of the team in theatre, and felt she couldn’t say anything, so she finished the operation and then left the hospital, telling administration team members that she was unwell. She has not been back to work since. |
| May has had escalating anxiety whenever she thinks about work and has nightmares about this consultant. She is also experiencing insomnia and has lost 5 kg because she has ‘no appetite’. She has been avoiding seeing her friends and family. May finally consulted her GP, who encouraged her to seek further help. She knows she ‘should’ report this but feels too ‘ashamed’ to do so. She is afraid this will mean the end of her career. |
In this scenario, little is known about the perpetrator, other than his gender, seniority, and a positive reputation professionally. While for the purposes of the book more detail about his personal life could have been given, in reality junior doctors and teams may not have much other background information about their senior colleagues, and especially in the case of a perpetrator grooming their victim. Perpetrators are likely to be able to seek more information than they share. It is normal practice for senior colleagues to inquire about a junior doctor’s life as part of a mentoring relationship, but it is unusual for junior staff to be comfortable asking personal questions of their supervisors. Perpetrators may be even less likely to share personal information if this is likely to act as a barrier to a closer relationship with the person they are grooming (e.g. if they are married). Perpetrators are likely to use their position of power and ‘good standing’ to encourage communication with a potential victim, and to encourage trust within the relationship, which sadly may then be abused. In this case the perpetrator holds a position of power clinically and as a potential career mentor. This case also exemplifies another risk for abuse – opportunity and use of ‘tools’ within their career armoury to abuse. In this case the physical opportunity of proximity to operate, under the guise of assistance for learning a practical procedure, was used, and particularly when the victim could not ‘escape’ at the time without abandoning the patient procedure or calling for help when in an area surrounded by colleagues of the well-respected consultant.
This case also highlights several elements in relation to the victim. Elements referenced in this case include the victim’s junior status (and resulting power imbalance), gender, and lack of formal or informal support networks – all risk factors that may have reduced her likelihood of ‘speaking out’. In addition, her described lack of confidence, ‘less extrovert’ personality and possibly a tendency to feel ashamed instead of feeling affronted further add to the risk of not reporting the first signs of breaking through normal professional boundaries. This book, in examining abuse of doctors by doctors, highlights that this is a truly global phenomenon, sadly, and that such issues need addressing worldwide. It may be the case that working in an environment that is not your country of origin further increases feelings of disempowerment and leads to underreporting. In addition, there may be differences in cultural tendencies to report sexual infringements, which this book explores. The word ‘ashamed’ is used in this case and may be relevant in this context.
In terms of management of this case through an integrated lens, it is appropriate that a holistic approach be taken. The victim may have chosen the person to whom they wish to disclose carefully, and sensitive handling of this discussion is paramount. The person to whom they disclose may feel shock, sometimes initial disbelief, and also a feeling of intense urgency to act or react. Working collaboratively with the victim to gain permission to draw in an appropriate case manager, so that a productive relationship can be formed, is very important in reducing the traumatic impact on the reporting junior doctor. The importance of judging pace of any stepwise support and investigation at the rate accepted by and appropriate for the victim is also critical.
Personal preferences in terms of communication style and interventions should be considered. For example, some victims will feel empowered by knowing that such abuse is not uncommon and that there are systems and services to offer support. Underreporting emphasises that other victims can feel a real lack of confidence, but signalling that there is progress with increasing numbers of victims speaking up can help. Some victims will not be motivated by systems factors, and this should also be respected.
All victims should be offered the chance to address their individual experience and narrative with highly skilled services. As highlighted in the case, a range of physical and psychological ill health can result from such abuse, and appropriate medical care from the trainee’s GP, occupational health, or specialist services such as the practitioner health programme would be offered. In this case May has clear physical and psychological symptoms of anxiety and depression, leading to a break down in ability to cope or attend work. Victims need to be informed about their options, including the appropriate bodies that could be involved in the investigation of their abuse (e.g. employers, legal systems, etc.), the likely manner in which investigation could occur, and the possible outcomes for each potential course of action.
It is critical that victims build back confidence in themselves, and also the systems which should support them, with factually correct and appropriate information. Any fears or needs around the victim’s educational and career journey should then also be addressed. Interventions would need to match the trainee’s needs and personal situation as well as their wishes. This may range from sick leave during investigation, treatment and recovery, through to adjusting the place of work depending on the teams or perpetrator implicated in the abuse. Understanding context and the doctor’s wishes around the full range of complex issues will be central to assisting in the doctor’s next steps following the trauma.
Conclusion
In this chapter we describe principles around integrated management of sexual harassment and abuse to ensure that the consequences of abuse (physical, psychological, educational and social) are acknowledged, and victims are supported to safety and healing. It is also increasingly recognised that such abuse takes place in organisational and social contexts and that policy and practice are required for effective prevention. We must also acknowledge that abuse of doctors by doctors is a sub-set of a much larger issue – abuse of individuals based on differences in power and social status.
Education and training have an important role to play in recognising and preventing abuse. Awareness raising (Reference O’Hare and O’Donohue12) as well as bystander training has been recommended, (Reference Bahji and Altomare5) and can help organisational culture to recognise the inappropriateness of sexual harassment and abuse in the workplace. There is much potential here to help empower doctors at an early stage to identify inappropriate behaviour before outright abuse or attack occurs. Clearly all staff should feel empowered to take positive action, so men and women play an incredibly important role in assisting with this remit, and in giving the target a voice if they do not feel sufficiently empowered to report alone.
Our review of the literature with a particular context of the doctor in training suggests that much further research is needed if we are to have a better understanding of the drivers and motivations of perpetrators as well as the most effective strategies for preventing such abuse, or rehabilitating perpetrators. Such information will be critical for teams managing the needs of victim and perpetrator. Finally, ensuring that workplaces facilitate speaking out and the culture is one of investigating and acting on any reports of abuse is paramount. (Reference Halim and Riding6) The organisation holding formal guidance and policies on appropriate behaviours (Reference Willness, Steel and Lee31) must accept the responsibility of leading cultural change by consistently addressing reports of misconduct if they are to be effective in this most fundamental arena of staff safety and wellbeing.
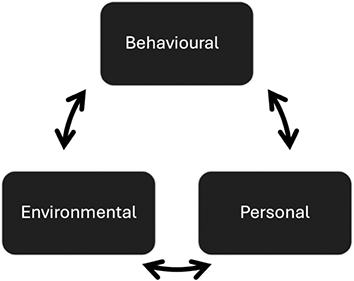
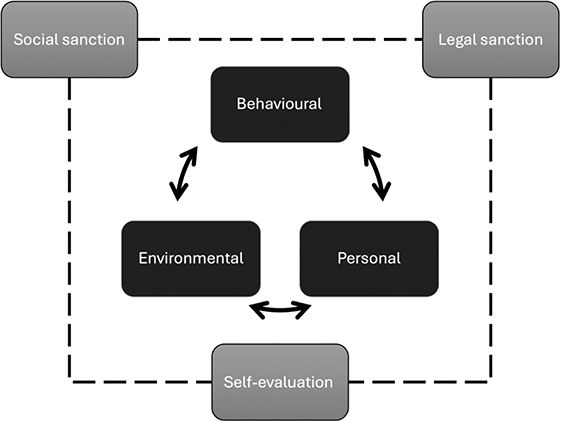
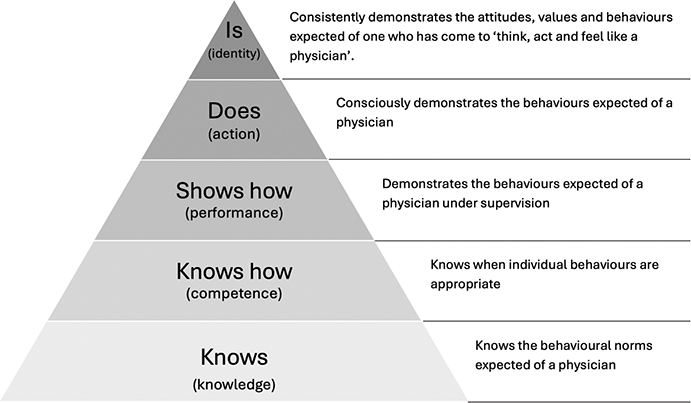

 Open access
Open access