


Significant outcomes
-
• While many studies have described forms of ‘traditional illnesses’ related to bewitchment in sub-Saharan Africa, very few have elucidated the details of specific forms of bewitchment in particular locales and their impact on health-seeking behaviours today.
-
• Second, this study highlights the ways in which biomedical and traditional forms of healthcare currently co-exist in this context, albeit generally in parallel, siloed structures of diagnosis and treatment.
-
• Our findings suggest, when added to the previous literature, that xifula continues to represent a significant explanatory model of illness in present day Limpopo Province, South Africa. Although some studies have described the phenomenon of xifula, few have examined this ailment as in-depth. By understanding how different societies conceptualise illness, we can better develop effective and sustainable localised healthcare.
Limitations
-
• This research used snowball sampling and is thus not intended to be representative.
-
• Additionally, only women caretakers were recruited for this study. Thus, it is unclear if a study that included men would report the same findings.
-
• Lastly, there may be a social desirability bias, where participants say what they believe staff want to hear, in order not to risk further involvement in subsequent waves of data collection.
Introduction
Previous research in Africa has established that health beliefs and help-seeking behaviours are strongly impacted by local religious and cultural formulations (Hammond-Tooke, Reference Hammond-Tooke1981; Semenya et al., Reference Semenya, Potgieter and Erasmus2012; Jors et al., Reference Jors, Büssing, Hvidt and Baumann2015; Cooper, Reference Cooper2016). In addition, medical theories have long contextualised illness within the realms of spiritual and social causation across sub-Saharan Africa (Hammond-Tooke, Reference Hammond-Tooke1989; Gyasi et al., Reference Gyasi, Asante, Abass, Yeboah, Adu-Gyamfi and Amoah2016; Opoku et al., Reference Opoku, Manu and Enin Antwi2018).
Studies of traditional beliefs in sub-Saharan Africa often identify illness aetiology based on spirit possession and bewitchment (Ngoma et al., Reference Ngoma, Prince and Mann2003; Falen, Reference Falen2018). More specifically, bewitchment – imprecations sent by others with the intention to cause harm – is viewed as a common explanatory model of illness as confirmed by many studies in sub-Saharan Africa (Crawford & Lipsedge, Reference Crawford and Lipsedge2004; Edwards, Reference Edwards2011; Sodi et al., Reference Sodi, Mudhovozi, Mashamba, Radzilani-Makatu, Takalani and Mabunda2011).
Bewitchment in Africa has been described as a moral framework that helps individuals and societies make sense out of disease and misfortune (Hammond-Tooke, Reference Hammond-Tooke1981). This religio-cultural phenomenon has significant consequences for understanding illness, care-seeking behaviours, as well as treatment and eventual recovery in this context (Hammond-Tooke, Reference Hammond-Tooke1989).
Although Western biomedical explanations for illness have slowly been incorporated into African health systems in the last century, the belief in supernatural powers as explanations for illness and misfortune remains widespread (van der Zeijst et al., Reference van der Zeijst, Veling, Makhathini, Susser, Burns, Hoek and Susser2021). Therefore, illnesses are often characterised as ‘traditional’ or ‘Western’ depending on their origin and their ability to be treated either biomedically or by local spiritual healers (Haram, Reference Haram1991; Steen & Mazonde, Reference Steen and Mazonde1999; Kovačič, Reference Kovačič2020; Pemunta & Tabenyang, Reference Pemunta and Tabenyang2020).
Many studies have examined how conditions such as non-communicable diseases have been commonly ascribed to bewitchment (Carrazana et al., Reference Carrazana, DeToledo, Tatum, Rivas-Vasquez, Rey and Wheeler1999; Ngoma et al., Reference Ngoma, Prince and Mann2003; Sorsdahl et al., Reference Sorsdahl, Stein, Grimsrud, Seedat, Flisher, Williams and Myer2009). In many traditional African belief systems, difficult-to-treat health problems are often attributed to bewitchment, as biomedical doctors are often unable to efficaciously resolve such ailments (Ngobe, Reference Ngobe2015; Louw & Duvenhage, Reference Louw and Duvenhage2016). This study examines one such cultural concept of distress (CCD), known as xifula, in Limpopo province, South Africa.
Methods
Study background, sampling, procedures, and measures were described in a previous publication (Galvin et al., Reference Galvin, Coetzee, Leshabana, Masebe, Lebepe, Moolla, Tarullo, Rockers and Evans2024; Galvin et al., Reference Galvin, Coetzee, Leshabana, Masebe, Lebepe, Moolla and Evans2025). This was a cross-sectional, qualitative study nested within a larger study, the Developing Belief Network (DBN) Study, which is conducting research across 16 countries and 50 distinct cultural and religious settings (Weisman et al., Reference Weisman, Ghossainy, Williams, Payir, Lesage, Reyes-Jaquez, Amin, Anggoro, Burdett, Chen, Coetzee, Coley, Dahl, Dautel, Davis, Davis, Diesendruck, Evans, Feeney, Gurven, Jee, Kramer, Kushnir, Kyriakopoulou, McAuliffe, McLaughlin, Nichols, Nicolopoulou, Rockers, Shneidman, Skopeliti, Srinivasan, Tarullo, Taylor, Yu, Yucel, Zhao, Corriveau, Richert and Belief Network2024). The data collected for this sub-study were part of the second wave of data collection conducted in Greater Tzaneen Municipality, Limpopo Province, South Africa, in 2024. The primary objective of the DBN study is to document the cultural influence on children’s (a) acquisition and development of religious knowledge and behaviours and (b) transmission of this knowledge and these practices to other individuals. Other questions the DBN study sought to answer include (1) How does the acquisition of religious cognition and behaviour vary within and between populations? and (2) How do processes of social learning support the development of religious cognition and behaviour?
The DBN study employed a snowball sampling strategy, in which the Tzaneen-based study team collaborated with community health workers at six local primary healthcare facilities participating in the DBN study to identify eligible participants. Later, the study team asked the enrolled participants if they knew anyone else who might be interested in participating in the study. If so, the study team obtained contact details and contacted potential study participants to assess their eligibility and willingness to participate in the qualitative interviews. Those eligible and willing were invited to participate and attend a scheduled study visit at the study office in Tzaneen.
Participants were included in this study if they were: 1) caregivers of children between 5 and 11 years of age; 2) 18 years or older; and 3) fluent in Xitsonga and Sepedi (a dialect of Northern Sotho). It is important to note that these eligibility criteria applied to the larger DBN study, and caregivers were co-enrolled in both the main DBN study and this sub-study. The interviews for both were combined, and therefore, participants were interviewed on a single occasion, saving time and resources for participants and the study team. The sample for this analysis was therefore a convenience sample of participants enrolled in the main DBN study. As these participants were taken from the larger DBN study, and since women are generally the primary caregivers across cultures, all participants were women.
Study visits were conducted at a private study office in Tzaneen, and participants were provided transportation to and from their homes. On the day of their visit, participants who were invited to participate in the study spoke with a member of the study team who explained the study and obtained written informed consent. Participants were asked to sign a study consent form as well as an audio consent form so that the interview could be recorded and later transcribed and translated. All communication and study documents were conducted in local languages (English, Xitsonga, and Sepedi) by a local study team who were trained on all study procedures, including participant confidentiality and informed consent.
Interviews took roughly 45 minutes to complete. Participants received a small reimbursement of R150 (approximately $10 USD) to compensate them for their time lost and any out-of-pocket expenses they may have incurred. They were also provided with refreshments during the visit.
Participants were asked to provide information about their age, monthly household income, employment status, education level, ethnic group, religious affiliation, marital status, and the number of children in their household. Participants were also asked if they knew of an illness known as xifula (in Xitsonga language) or sefolwana (in Sepedi language). It is important to note that these are two of several words in both languages that refer to malicious supernatural forces (Fortrell et al., Reference Fottrell, Tollman, Byass, Golooba-Mutebi and Kahn2012). As xifula is more commonly cited in the scientific literature, authors will use this term in the paper. If participants had heard of this illness, they were then asked how the illness is acquired and transmitted, how it affects sufferers, and what symptoms it causes. They were then asked how this illness could be treated, and whether it should be treated by traditional healers, biomedical doctors, or both. Lastly, participants were asked if they knew anyone who had suffered from this ailment and, if so, what they knew about those experiences. Saturation was assessed by systematically analysing data during collection, tracking code frequency to identify when new codes stop appearing, and ensuring that no new conceptual categories are emerging.
The questionnaire was originally developed in English, and all translations into Sepedi and Xitsonga were culturally validated by team members prior to incorporation into the questionnaire. Wording was maintained consistently across participants, and assessors asked semi-structured follow-up questions as needed. All interviews were audio recorded and transcribed. Three study enumerators reviewed all transcripts and translated them into English. The analysis utilised a directed content analysis method that combined deductive and inductive aspects of code development (Hsieh & Shannon, Reference Hsieh and Shannon2005). Analysis was performed using the constant comparative method in which data were constantly being analysed while being collected to continuously compare new information to identify patterns and refine concepts (Silverman, Reference Silverman2005). This iterative process helped in creating theories that are grounded in the data itself, rather than starting with pre-existing frameworks. Themes were developed and refined by the three study enumerators and study PI (MG) and lead researcher (AM), resulting in a final set of codes. Two coders ultimately fully assessed each transcript in NVivo. Following coding, coders met to resolve discrepancies and finalise codes. Main thematic codebook elements included identification of main elements composing xifula, causes of xifula, symptoms of xifula, and treatments of xifula, with subcategories of codes under each theme. The codes are presented as follows in the Results section below. Data was analysed using NVivo software. The survey data were collected and stored in REDCap, an electronic data capture tool hosted by the University of the Witwatersrand, to maintain confidentiality (Harris et al., Reference Harris, Taylor, Minor, Elliott, Fernandez and ONeal2019).
The study was approved by the Human Ethics Research Committee (Medical) at the University of the Witwatersrand, Johannesburg (Clearance number: M210914). All participants provided written informed consent to participate in the study and to have their interview audio recorded.
Results
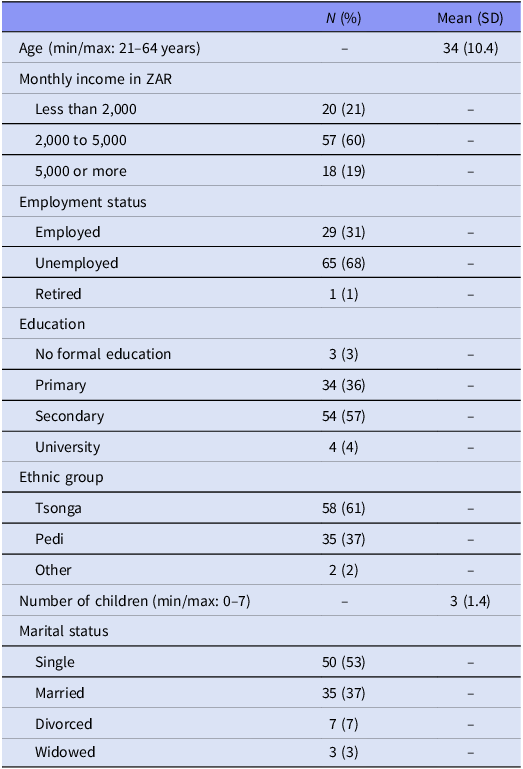
This study examined a population of rural women living near the city of Tzaneen. Ninety-five individuals (n = 95) completed the study interview and were therefore included in this analysis (see Table 1). Participants ranged in age from 21 to 69 years. The population of this study was predominantly poor, with 81% of households having a monthly income of less than 5,000 ZAR (approximately $275). Only 31% of participants were employed, although many had husbands who were employed. More than half (57%) had completed high school or a secondary school education. The ratio of Tsonga to Pedi participants was 3:2.
Sample characteristics (n = 95)

What is xifula?
According to participants, xifula is an illness that is related to ‘bewitchment’. As one respondent says, ‘Xifula comes from witches at night. It can affect anyone, it just depends on the person trying to bewitch you’ (Participant 34). Others agreed, saying ‘Xifula is done by people, it is witchcraft (vuloyi)’ (Participant 16). This reference to bewitchment as ‘things that happen at night’ was commonly referred to by participants in both Sepedi (dilo tša bošego) and Xitsonga (swilo swa vusiku) throughout the interviews for this study. In addition, participants also frequently referred to bewitchment as ‘done by people’, referencing the idea that others are sending illness or misfortune via supernatural means according to traditional African religious practices (Participant 42).
What are the causes of xifula?
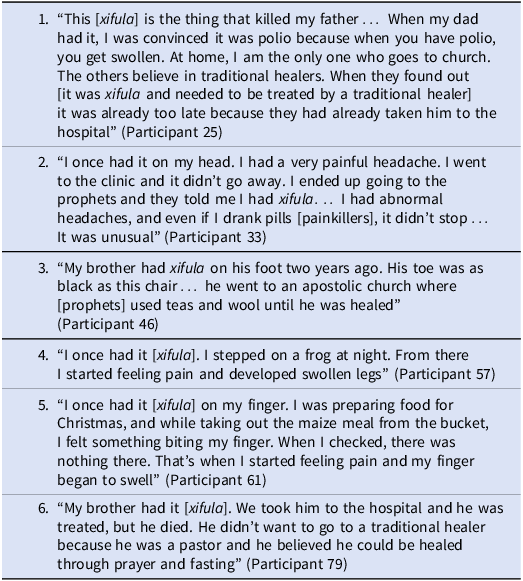
The vast majority of participants interviewed identified the causes of xifula as a form of bewitchment that impacts the limbs – specifically, the hands and arms, or the legs and feet. Therefore, one contracts xifula by ‘walking or stepping on something’ or ‘handling money or other objects’. As these objects were often said to be placed in the individual’s path or handed to them with the intention of bewitching them, ‘it [xifula] almost always affects the legs or hands’, one respondent says (Participant 44). ‘I grew up knowing that there is xifula, seeing people’s feet getting swollen. They say people send it onto you by putting it where they know you’ll pass by so you can step on it’, another remarked (Participant 25). Another described how ‘sometimes when walking around in your yard you might suddenly feel a piercing pain in your body and you may start shivering, indicating you’ve been impacted by xifula’ (Participant 84). Secondarily, a few participants report that you can get xifula by ‘eating something’ which has been bewitched, as well. This can result in chronic headaches as a symptom of xifula, as described in the second account in Table 2. One participant even described stepping on a frog in his path as seen in the fourth account in Table 2.
Additional accounts of participants who experienced close encounters with xifula

Nevertheless, as previously described, xifula most commonly impacts the limbs. As one respondent says, ‘a person is hit on the hand or foot. They [witches] put something in your path. It touches or scratches you, and the area becomes wounded. Some people get it by stepping on something, others get it by receiving money. Like cash in their hand… But you won’t be affected unless it [the bewitchment] is directed at you’ (Participant 19). This description highlights the way in which individuals are perceived to be targets for bewitchment by either placing an object in your path that affects the feet and legs, or given money which impacts the hands and arms. ‘They give it to you through money so that you take it in your hand, or they put it in your path and make you walk on it and you end up falling down; then it [xifula] shows when you start limping’ (Participant 20).
It is also important to emphasise that xifula is a targeted attack where only the intended victim can be affected. As one respondent describes, ‘Xifula only affects whoever they [the witches] have put it for. If they put something in the path of the intended victim and they stepped on it, then the leg can get swollen and rot and have unusual wounds’ (Participant 39). In this sense, Xifula is not so much an illness that anyone can get by coming into contact with it, but rather the individual who contracts it is the victim of a targeted attack.
What are the symptoms of xifula?
Most participants reported that the most common symptom of xifula is swelling of the legs or hands. The next most commonly reported symptom is a wound or rash on the legs or hands that won’t heal. ‘Xifula wounds do not heal, they always cause pain’, one respondent said (Participant 27). ‘You realise what it is when the wound doesn’t heal’, another remarked (Participant 48). This ability to identify xifula by a wound that will not heal is a key characteristic of bewitchment, according to many participants. ‘It is something that always causes pain on the body, it can be on the hand on the foot and it always causes pain that never goes away. Sometimes it can be a burning sensation and you have to put the foot or hand in cool water to calm down the pain. The main factor is that the pain never goes away’, according to one respondent (Participant 78).
There were a large variety of descriptions of symptoms of xifula, usually as a rash, a wound, a boil, or swelling of the limbs. As one respondent described, ‘if my leg is affected it may get swollen, change colours, and eventually become black’ (Participant 62). Participants noted how often xifula can start as a minor ailment, but then grows into a larger and larger problem. ‘It [xifula] starts as a small wound next to a nail on the thumb. You will experience a painful swelling in the thumb which does not heal’, one person said (Participant 40). After a long period without healing, however, xifula can begin to represent a significant threat to the individual’s health. ‘If it is on your hand it can destroy your hand’, another respondent remarked (Participant 38). One respondent noted how he once had xifula in his ‘private parts’, remarking ‘I couldn’t sit, it hurt a lot… for this reason a lot of people keep quiet about it’ (Participant 87). Several participants noted xifula can ultimately result in death if not treated in a timely and appropriate manner, as seen in the sixth account in Table 2.
What is the treatment for xifula?
Nearly all participants noted that xifula cannot be treated at the hospital or by Western biomedical professionals. Rather, xifula requires a traditional healer to treat. While some respondents say that prophet healing or praying at church might help, the vast majority emphasised that African traditional healing is the primary means of curing xifula. As one said, ‘these are traditional supernatural things that they [witches] use to make people sick… the Western doctors won’t see anything when you are consulting with them’ (Participant 41). Another respondent noted how doctors can also misdiagnose xifula: ‘doctors might tell you that you have diabetes, whereas it is really xifula’ (Participant 35).
Some participants insisted that xifula ‘is not treatable at the clinic’ (Participant 35), or argued that ‘if you consult a doctor, it [xifula] won’t heal’ (Participant 47). Others claim that consulting a doctor may result in xifula that appears to improve, but the improvement will not last: ‘someone can go to the hospital now, then feel better at first, but then later get worse. The hospital doesn’t help’ (Participant 36). Yet, others argued that ‘going to the hospital makes it [xifula] worse,’ sometimes even resulting in the death of the patient (Participant 52).
However, if patients seek treatment from a traditional healer, the xifula can be cured. ‘If you go to the clinic, you will not improve, but if you go to the traditional healer, you become better’, claimed one (Participant 55). While some respondents claimed that prophets can also heal xifula, as seen in accounts 2 and 3 of Table 2, nearly all emphasised the importance of staying away from Western medicine. As one respondent stated, ‘prophets can use wool to tie around your hands and legs. They can also use their teas. But it cannot be healed the Western way’ (Participant 74).
Discussion
There is a small but growing scientific literature examining the relationship between traditional African beliefs and illness in sub-Saharan Africa (Patel, Reference Patel1995; Sylvia, Reference Sylvia2000; Azevedo, Reference Azevedo2017; Anizoba, Reference Anizoba2021). The primary goal of these studies is to understand how ‘folk beliefs’ influence illness causation as well as decision-making processes for treatment (Golooba-Mutebi & Tollman, Reference Golooba-Mutebi and Tollman2007a). As these concepts often do not feature in policy discussions, it is important to highlight their significant continued impact on pathways to healthcare in sub-Saharan Africa.
Xifula, as a particular diagnosis in the Xitsonga language, falls under a broader category of bewitchment, which has many translations in Xitsonga including ‘ku dlukula’, ‘xifulana’, ‘ku wutla rigadyi’, ‘khubalo’, ‘xidyiso’ or ‘xifula’ (Fottrell et al., Reference Fottrell, Tollman, Byass, Golooba-Mutebi and Kahn2012). In English, other translations might include words such as ‘witchcraft’, ‘evil spirit’, or ‘devil spirit.’ One study examining xifula in Limpopo province, South Africa found similar findings to this study (Stadler, Reference Stadler1996). Witches often ‘send’ misfortune by burying something under the entrance to someone’s house, which results in a boil and later a small sore appearing on the ankle or leg. Stadler describes how informants were sure they had been bewitched once the sore proved incurable by doctors at the clinic or hospital. Similar to this study’s findings as well, without appropriate treatment xifula could result in permanent disability or death.
Another more recent study in Limpopo examined patients suffering from leg paralysis and the perception of it being caused by xifula (Boene et al., Reference Boene, Mocumbi, Högberg, Hanson, Valá, Bergström and Munguambe2020). In this study, participants described how xifula was often attributed to bewitchment caused by family members, such as in-laws. One woman with drop-foot described how her xifula was caused by her sisters-in-law and was currently being treated by traditional healers who rubbed herbal remedies on fresh razor blade cuts on her skin.
A third study examining xifula in Limpopo similarly recounts how patients contracted it by jumping over or stepping on ‘medicines laid along a path or at the entrance to a homestead by a witch’ (Golooba-Mutebi & Tollman, Reference Golooba-Mutebi and Tollman2007a, p. 66). These medicines are referred to as xidyiso, which once ingested, turns into a live organism that eats the victim from inside the body. Authors found symptoms can include wounds and swelling of the limbs, in addition to severe head or stomach aches, and even stroke-like symptoms. In one case study, a young man repeatedly sought care from doctors without success. After visiting several traditional healers, he was ultimately cured by a local inyanga – or traditional herbalist – who was visiting his family at the time.
These studies therefore confirm many findings of this study, particularly that individuals with xifula are victims of bewitchment, which largely impacts the limbs via wounds, swelling, or paralysis. The participants in these studies also primarily sought care from traditional African healers. While these studies did not generally describe patients being successfully treated by prophets or other forms of Christian healing, future research could examine the relationship between traditional healers who use African versus Christian forms of healing for illnesses such as xifula.
While it is difficult to determine the precise extent to which xifula impacts modern-day populations in Limpopo province, folk beliefs concerning illness and its causation continue to significantly influence an individual’s decision about whether to select allopathic or traditional treatment. As symptoms of xifula often include various forms of bodily swelling and skin lesions – common symptoms of advanced stages of HIV/AIDS – some researchers argue that xifula might have seen a resurgence since the 1990s (Golooba-Mutebi & Tollman, Reference Golooba-Mutebi and Tollman2007b). Others argue that growing populations and increased land conflicts may have resulted in increases of xifula historically (Gengenbach, Reference Gengenbach1998). Ultimately, however, anthropologists have found that traditional African explanatory models of illness, such as xifula, emphasise why something occurred rather than how – a perspective that Western medicine does not typically adopt – and may therefore remain relevant for this reason (Hammond-Tooke, Reference Hammond-Tooke1981, Reference Hammond-Tooke1989). It is important to note that this study does not adjudicate biomedical causation but rather documents beliefs and pathways to care.
Xifula could likely be characterised as a CCD as defined by the Diagnostic and Statistical Manual similar to others such as ‘Maladi Moun’ in Haiti which also refers to bewitchment, or illness sent by one person supernaturally with the intent to cause misfortune or harm (Galvin et al., Reference Galvin, Michel, Pierre, Manguira and Cénat2023). Additionally, members of this study team have also conducted several studies regarding religio-cultural concepts of illness related to bewitchment in the South African context and may be relevant to readers of this study (Galvin et al., Reference Galvin, Chiwaye and Moolla2023a; Galvin et al., Reference Galvin, Byansi, Chiwaye, Luvuno and Moolla2023b; Galvin et al., Reference Galvin, Chiwaye and Moolla2024a; Galvin et al., Reference Galvin, Coetzee, Leshabana, Masebe, Lepebe, Moolla, Tarullo, Rockers, Cameron and Evans2026)
Lastly, this study has several limitations. First, this research used snowball sampling and is thus not intended to be representative Additionally, only women caretakers were recruited for this study. Thus, it is unclear if a study that included men would report the same findings. Similarly, these findings from caregiver perspectives within the DBN recruitment rather than population beliefs. Lastly, there may be a social desirability bias, where participants say what they believe staff want to hear, in order not to risk further involvement in subsequent waves of data collection. However, it is not clear in which direction this would have impacted the data.
Conclusion
This study examined the illness referred to as xifula among female caretakers in rural Limpopo province, South Africa. It found that xifula is an illness caused by bewitchment that primarily affects the limbs of the patient and is only treatable by traditional healing. This research, therefore, highlights the need for context-specific education about the diagnosis and treatment of common ailments, based on beliefs about afflictions, their causes, and appropriate treatments. As biomedical and traditional healthcare currently exist as parallel, siloed structures of diagnosis and treatment in Africa, there should also be efforts to bridge the divide between the two. Ultimately, understanding how societies interpret the essential factors that impact their health, as well as how health-seeking behaviours are influenced by local cultural notions and perceived aetiologies of illness, can help inform more effective, sustainable interventions and health promotion efforts.
Data availability statement
Deidentified data and other study information is available upon request from corresponding author with publication.
Acknowledgements
This study was supported in part by personnel, office space, and resources from the South African field site of a large-scale collaborative research effort by the DBN (developingbelief.com), a network of researchers affiliated with a variety of institutions, working in diverse field sites around the world. The DBN is funded by Award #JTF61542 from the John Templeton Foundation.
Author contributions
MG formulated the study questionnaire, conceptualised the research question, analysed study data, and wrote the manuscript. LC oversaw data collection and reviewed and edited the manuscript. PL, NM, and SL collected study data. AM, PL, NM, and SL analysed study data. AM, AT, PR, DE reviewed and edited the manuscript.
Funding statement
This study was funded by a grant from the John Templeton Foundation.
Competing interests
The authors declare they have no conflict of interest.

 Open access
Open access