


Introduction
Infection-control measures are evidence-based approaches that are used to prevent mortality and morbidity among patients and HCWs due to preventable infections. Reference Zingg, Storr and Park1,Reference Haque, Sartelli, McKimm and Abu Bakar2 The World Health Organization (WHO) and many collaborating organizations publish recommendations on infection-control programs, and the approach to implementing these programs is summarized in both WHO and national guidelines. 3–6 According to WHO recommendations, each country should have a national infection-control curriculum and training program in collaboration with academic institutions and in line with national guidelines. There should be a policy supporting the implementation and monitoring of the training program, and at least all frontline HCWs and cleaning staff should be required to receive basic infection-control training. Furthermore, a system should also be established to evaluate the program’s effectiveness.
A key component of efficient infection-control in healthcare settings is effective communication between IPC professionals (IPCPs) and HCWs. 7 Clear, consistent, and timely communication helps HCWs better understand IPC guidelines and compliance with basic measures, which encompass hand hygiene and the appropriate utilization of personal protective equipment. Reference Allegranzi, Zayed and Bischoff8 Furthermore, communication gaps may compromise patient safety and care quality by causing inconsistent practices, lower compliance, and increased transmission of infections. Reference Saint, Kowalski, Banaszak-Holl, Forman, Damschroder and Krein9 In Türkiye, the Ministry of Health has prioritized structured healthcare-associated infection initiatives since 2006 and has adopted a multimodal strategy for development since 2019. Reference Bakanlığı10 In addition, healthcare-associated infection rates, causative microorganisms, resistance rates, and surveillance results are published annually, and infection-control programs are implemented in healthcare institutions. Reference Gozel, Hekimoglu, Gozel, Batir, McLaws and Mese11
A multicentre report has been published in Türkiye that measures IPC components and the IPC assessment framework. Reference Azak, Sertcelik and Ersoz12 However, there is no system in place to monitor other components of infection-control programs, particularly for multimodal strategies and effective communication. Furthermore, there is no assessment or data on the level of effectiveness of IPC activities in patient care areas, including the use of effective communication methods, in addition to the education and training activities of infection-control committees. The aim of this study was to evaluate the compliance of infection-control committees with effective communication techniques within the scope of their activities, to assess the perspectives of physicians and nurses working in patient care areas on the impact of IPC activities on IPC compliance, and to obtain feedback regarding effective communication techniques.
Materials and methods
Study design and participants
This study was performed as a multi-center, cross-sectional, online survey conducted between February 1 and April 30, 2025, as part of the self-assessment activities of the IPC program in Türkiye.
The survey was developed by authors based on the WHO multimodal strategy for infection prevention and control and its five core components: system change, education and training, monitoring and feedback, reminders and communication, and organizational safety culture. 7,13
Additionally, questions addressing effective communication techniques were based on established concepts from the health communication and adult education literature, including active listening, empathy, feedback mechanisms, verbal and nonverbal communication, and the use of “I-language” and “you-language.”
We evaluated the compliance of infection-control committees with effective communication techniques within the scope of their activities, as well as the opinions of physicians and nurses working in patient care areas regarding the impact of infection-control committee activities on IPC compliance. We also obtained feedback on effective communication techniques.
Participants were selected using convenience sampling. Healthcare institutions across Türkiye with established IPC programs were invited to participate through professional networks and institutional communication channels. The survey link was distributed electronically to IPCPs and HCWs (physicians and nurses) working in patient care areas via institutional communication channels. Participation was voluntary. Responses were collected anonymously using Google Forms.
IPC specialists (physicians or nurses) or HCWs actively involved in patient care (physicians or nurses) who completed the online survey during the study period were included in the study. Those with incomplete survey responses, HCWs not involved in patient care, and duplicate surveys were excluded from the study.
The questions were grouped within the following headings: demographics of the participants (age, sex, occupation, type of institution, etc.), system change, clarity and accuracy of information transfer, education and awareness, monitoring and feedback on infection-control measures, and reminders at work (Supplement 1).
Ethical approval
This study was approved by Kayseri City Hospital Clinical Research Ethical committee (Date: 28.01.2025, No.: 311).
Statistical analysis
An a priori power analysis for the chi-square (χ2) goodness-of-fit test was conducted using G * Power version 3.1.9.7 to determine the minimum required sample size. A medium effect size (Cohen’s w = 0.30) was selected in line with Cohen’s conventional benchmarks and methodological recommendations for categorical data analyses, where very small deviations from expected distributions are unlikely to be of substantive or practical relevance. The significance level was set at α = 0.05. A high statistical power of 0.95 was deliberately chosen to minimize the probability of Type II error and to ensure sufficient sensitivity to detect distributional deviations of practical importance, particularly in the context of public health–relevant patterns.
The degrees of freedom (df = 4) were derived from the five categorical outcome levels included in the analysis (df = k−1). Under these assumptions, the required minimum sample size was calculated as N = 207. This conservative power specification strengthens confidence that the study is adequately equipped to detect meaningful discrepancies between observed and expected frequencies.
A Google survey form was used for the survey. The data from the survey responses were obtained in Excel format. The responses were evaluated in terms of frequency and compared between groups using the chi-squared test.
Results
Survey overview
A total of 102 IPCPs and 166 HCWs from 96 institutions participated in the survey. Among HCWs, 143 (86.1%) were women, and among IPCPs, 90 (88.2%) were women. The mean career duration was 19.8 ± 9.5 years, and 6 IPC specialists had over 20 years of experience.
Institutional characteristics
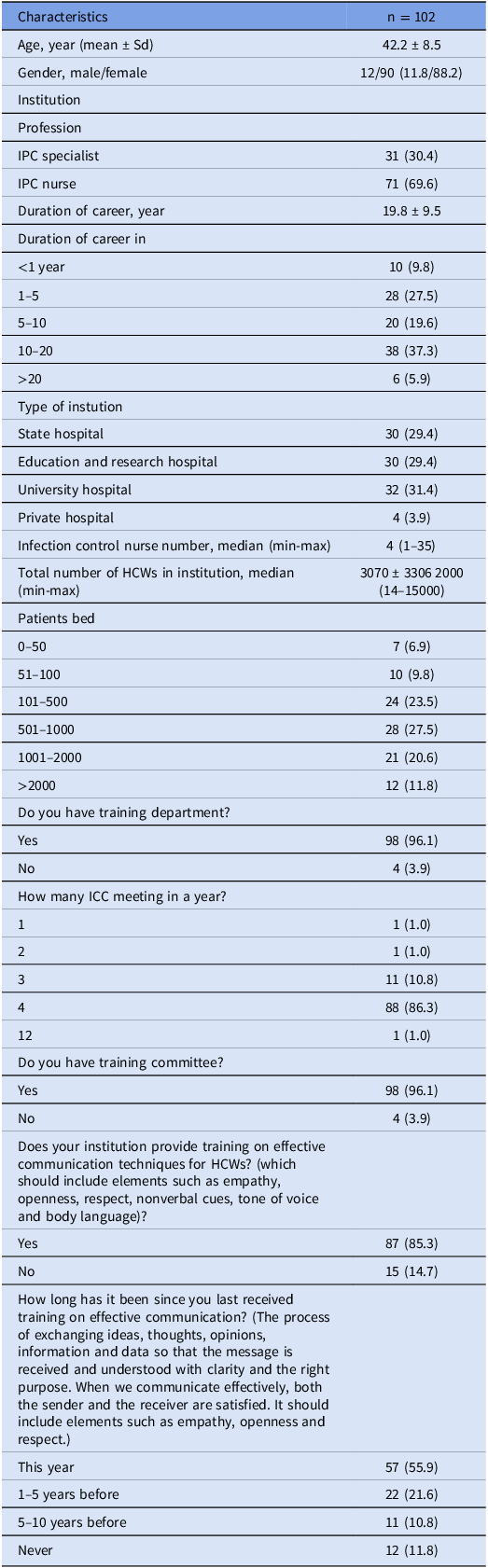
An infection-control committee was established in 98% of participating institutions. Of the IPCPs, 31 (30.4%) were IPC physicians, and 71 (69.6%) were nurses. Only 10 institutions met the ratio of 1 IPC nurse per 150 beds. Quarterly meetings were held by the infection-control committees in 88% of these institutions. Training in effective communication techniques was provided by 85.3% of institutions. Annual training was received by 55.9% of IPC team members and 59.6% of HCWs (Table 1).
Characteristics of Infection Prevention and Control professionals and institutions participating in the survey

Table 1 Long description
The table presents characteristics of infection prevention and control professionals and institutions participating in a survey. It includes 102 rows and multiple columns detailing various attributes. Row 1: Characteristics, n = 102. Row 2: Age, year (mean ± Sd), 42.2 ± 8.5. Row 3: Gender, male/female, 12/90 (11.8/88.2). Row 4: Institution. Row 5: Profession. Row 6: IPC specialist, 31 (30.4). Row 7: IPC nurse, 71 (69.6). Row 8: Duration of career, year, 19.8 ± 9.5. Row 9: Duration of career in <1 year, 10 (9.8). Row 10: Duration of career in 1-5, 28 (27.5). Row 11: Duration of career in 5-10, 20 (19.6). Row 12: Duration of career in 10-20, 38 (37.3). Row 13: Duration of career in >20, 6 (5.9). Row 14: Type of institution. Row 15: State hospital, 30 (29.4). Row 16: Education and research hospital, 30 (29.4). Row 17: University hospital, 32 (31.4). Row 18: Private hospital, 4 (3.9). Row 19: Infection control nurse number, median (min-max), 4 (1-35). Row 20: Total number of HCWs in institution, median (min-max), 3070 ± 3360 (200-15000). Row 21: Patients bed. Row 22: 0-50, 7 (6.9). Row 23: 51-100, 7 (6.9). Row 24: 101-500, 24 (23.5). Row 25: 501-1000, 28 (27.5). Row 26: 1001-2000, 21 (20.6). Row 27: >2000, 12 (11.8). Row 28: Do you have training department? Row 29: Yes, 98 (96.1). Row 30: No, 4 (3.9). Row 31: How many ICC meeting in a year? Row 32: 1, 1 (1.0). Row 33: 2, 1 (1.0). Row 34: 3, 11 (10.8). Row 35: 4, 88 (86.3). Row 36: 12, 1 (1.0). Row 37: Do you have training committee? Row 38: Yes, 98 (96.1). Row 39: No, 4 (3.9). Row 40: Does your institution provide training on effective communication techniques for HCWs? Row 41: Yes, 87 (85.3). Row 42: No, 15 (14.7). Row 43: How long has it been since you last received training on effective communication? Row 44: This year, 57 (55.9). Row 45: 1-5 years before, 22 (21.6). Row 46: 5-10 years before, 11 (10.8). Row 47: Never, 12 (11.8).
IPC, infection prevention and control; HCW, healthcare worker; IPCP, infection prevention and control professionals; ICC, infection Control Committee; Sd, standard deviation.
Perceptions of IPC communication and motivation
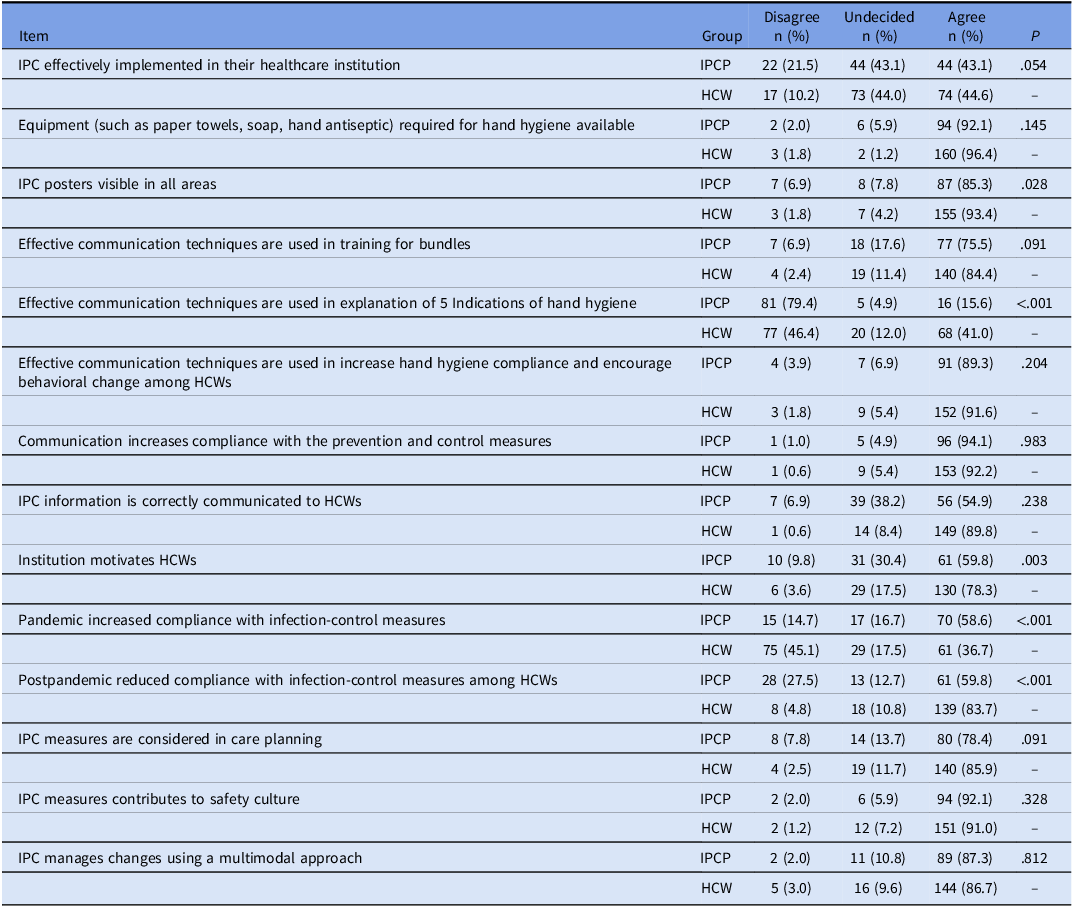
There were 87 (85.3%) IPCPs who considered information posters for infection-control to be adequate in their institutions, while 155 HCWs (93.4%) shared this opinion (P=.028). There were 90 (88.2%) IPCPs and 155 (93.4%) HCWs who considered hand hygiene posters to be adequate (Table 2). When explaining the five indications for hand hygiene, 81 (79.4%) IPCPs stated that they used effective communication techniques, while only 77 (46.4%) HCWs thought that effective communication techniques were used (P < .001).
System changes

IPC, infection prevention and control; HCW, healthcare worker; IPCP, infection prevention and control professionals.
There were 61 (64.7%) IPCPs and 130 (78.3%) HCWs who believed that the institution effectively motivated HCWs to comply with IPC measures. In addition, 44 (43.1%) IPCPs were undecided, while 29 (17.5%) HCWs were undecided (P = .002).
Impact of the COVID-19 pandemic
There were 70 (68.6%) IPCPs who believed that the COVID-19 pandemic had increased compliance with IPC measures, while only 61 (36.7%) HCWs agreed with this view (P < .001). There were 61 (59.8%) IPCPs and 139 (83.7%) HCWs who believed that compliance with IPC measures had decreased after the pandemic (P < .001) (Table 2).
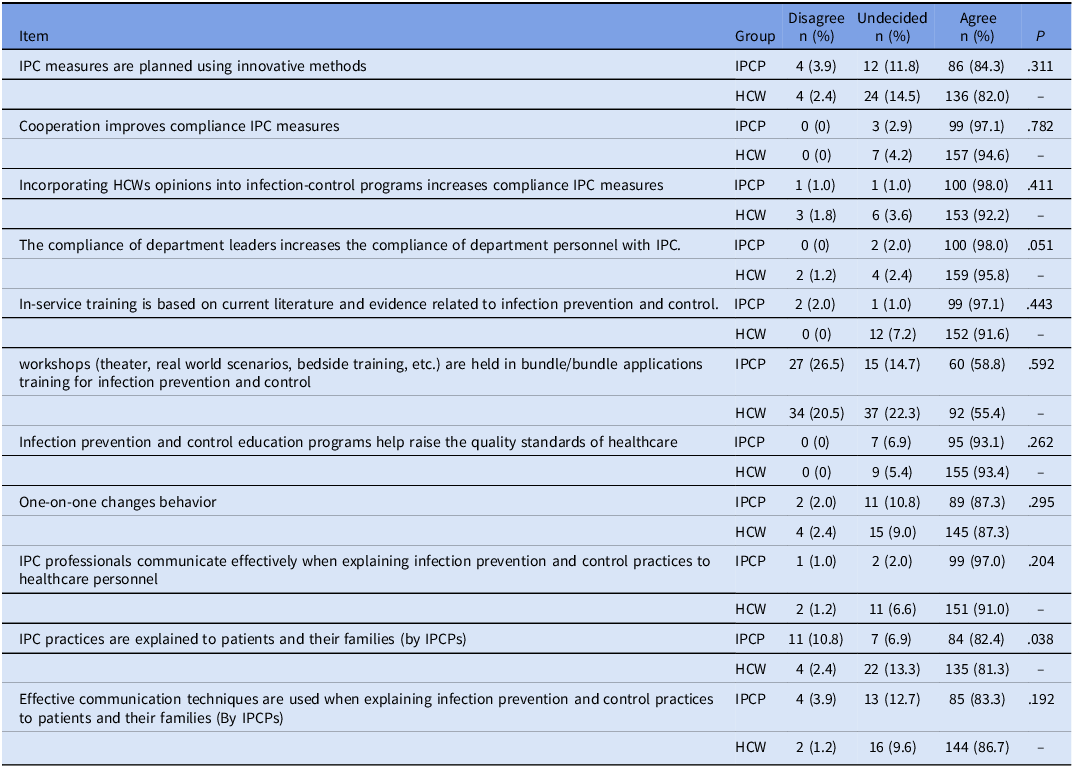
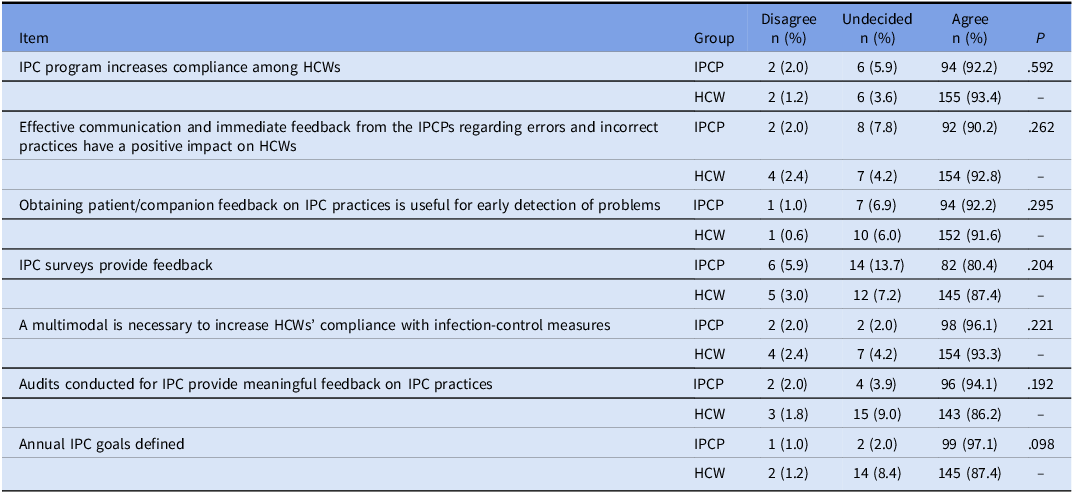
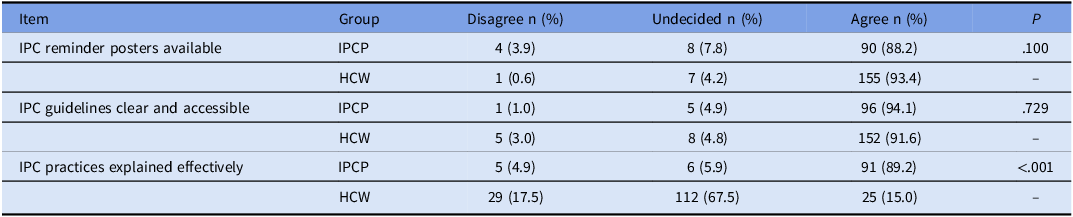
Regarding education and awareness, HCWs and IPCPs mostly shared the same perceptions, as shown in Table 3. Both HCWs and IPCPs agreed that providing feedback on the implementation and compliance of infection-control programs would increase compliance with infection-control measures among HCWs (Table 4). Regarding the bundle training provided by IPC committee, 91 (89.2%) IPCPs and only 25 (15.0%) HCWs participated, which confirmed that effective communication technique was used. However, 112 HCWs (67.5%) reported being undecided (P < .001) (Table 5).
Education and awareness

IPC, infection prevention and control; HCW, healthcare worker; IPCP, infection prevention and control professionals.
Monitoring and feedback of infection-control measures

IPC, infection prevention and control; HCW, healthcare worker; IPCP, infection prevention and control professionals.
Reminders at work

IPC, infection prevention and control; HCW, healthcare worker; IPCP, infection prevention and control professionals.
Discussion
This study evaluated the perceptions of IPC specialists and HCWs in clinics regarding the use of effective communication practices in IPC programs implemented in healthcare institutions in Türkiye. The main finding was that there are significant differences between IPC teams’ perceptions of their own practices and HCWs’ experiences in the field. According to survey reports, IPC experts reported that training and effective communication methods were widely used, but HCWs indicated that the practices were used at lower rates. This situation shows that training and communication are not effectively reflected in the field. This difference in perception is most prominent in the communication of hand hygiene indications and bundle training. There is a lack of visibility or implementation in the areas of education, reminders, feedback, and cultural change emphasized in the WHO’s multimodal strategy. 4,Reference Moghnieh, Al-Maani and Berro14 The literature highlights that the effectiveness of IPC training is determined by its content, presentation method, continuity, and feedback mechanisms, and it is emphasized that the participation and motivation of HCWs are closely related to the communication style of IPC. Reference Sussenbach, Graveland, Voss and Versteeg15–Reference Alhumaid, Al Mutair and Al Alawi17
Differences in perceptions of organizational motivation are also notable. HCWs believe that their institutions are more motivating in terms of IPC, and a higher rate of uncertainty has been observed among IPC specialists. This could be a result of IPC teams having increased responsibilities, workloads, and expectations leading to more critical perspectives. Factors defined by the WHO regarding workload, staff numbers, and bed occupancy rates are known to be key variables affecting IPC practices. 7 In this study, the very low percentage of institutions that were able to achieve the recommended number of IPC nurses indicates that IPC teams face limitations in terms of organizational capacity and human resources for effective communication and training activities.
Differences observed between IPCPs and HCWs have significant implications for clinical practice. The fact that there are significant differences between IPC specialists’ self-reported use of effective communication techniques and HCWs’ perceptions, particularly in hand hygiene training, suggests that IPC programs may be overestimating the effectiveness of communication strategies at the point of care. From a practical perspective, IPC programs should complement traditional training methods with structured mechanisms that actively assess how messages are perceived by frontline staff. Incorporating HCWs’ feedback, using interactive communication approaches such as scenario-based training or feedback methods, and evaluating understanding as well as compliance may help bridge this perception gap. Additionally, IPC committees should consider routinely integrating communication effectiveness monitoring and auditing processes, rather than focusing solely on compliance outcomes. Treating communication as a measurable component of IPC implementation can increase participation, improve compliance with infection-control measures, and support more sustainable behavior change in clinical settings.
The high percentage of HCWs who reported being “undecided” about the use of effective communication during bundle training may reflect several key issues, such as limited exposure to bundle-based training, a lack of clear understanding of what bundle training entails, or insufficient interactive communication during such activities. Regardless of the underlying cause, this finding suggests that bundle training may not be sufficiently visible or clearly distinguishable from other frontline training activities. Therefore, IPC programs should ensure that bundle training is clearly labeled, delivered consistently, and supported by clear communication regarding its objectives and relevance to daily clinical practice.
Perceptions regarding the COVID-19 pandemic also differed significantly between groups. While a high rate of IPC specialists believed that the pandemic has increased IPC compliance, the rate was significantly lower among HCWs. However, there was strong consensus between both groups that compliance decreased in the post-pandemic period. The literature also indicates that awareness and motivation regarding IPC practices increased at the onset of the pandemic, but this interest did not continue in the post-pandemic period. The lack of structural and behavioral strategies to ensure the sustainability of IPC compliance may be a reason for this decline observed in the post-pandemic period. Reference Storr, Twyman and Zingg18–Reference Madran, Demir and Yalcin20
Both groups found that posters and reminder materials were mostly adequate. This indicates that there is no lack of visibility of these physical reminders. However, the perceived gap in education and communication suggests that a fundamental problem may stem not from a lack of knowledge, but from the way that knowledge is communicated. The need for communication supported by cultural change, teamwork, and personalized methods as emphasized by the WHO is consistent with these findings.
This study has some limitations. First, its cross-sectional design and use of a voluntary, online survey may create selection bias and limit causal inferences. Second, the survey was a theory-based tool developed for the specific purposes of this study and was not a pre-validated scale, which may affect the generalizability of the findings. Finally, the results are based on self-reported perceptions and may be subject to response and social desirability bias. Another limitation is that the definition of “effective communication” in some items contains multiple components (e.g., empathy, openness, respect, verbal and nonverbal communication) that may be interpreted differently by participants and could affect construct validity. Furthermore, some items that are conceptually clear in the original Turkish version may appear complex or ambiguous in the English translation. These limitations should be considered when interpreting the findings. The data have a nested structure, with HCWs and IPCPs clustered within the same hospitals. Although group comparisons were made using χ2 tests assuming the independence of observations, responses from the same institution may share organizational characteristics, which could violate this assumption and affect variance estimates. The total number of HCWs and IPC professionals who received the survey invitation was not recorded; therefore, a formal response rate could not be calculated. This may introduce selection bias, as participants with greater interest or engagement in infection prevention and control activities may have been more likely to respond.
This study is important in terms of revealing the current status of IPC programs in Türkiye in terms of their education and communication components. The findings indicate that there is a need for more structured and interaction-focused strategies supported by feedback mechanisms to reduce differences in communication, perception, and implementation between IPC specialists and HCWs. Furthermore, strengthening IPC teams, increasing staffing levels, and integrating training more firmly into corporate policy appear to be critical for sustainable implementation.
Acknowledgements
This study was presented as a paper poster in 8th International Conference on Prevention & Infection Control (ICPIC 2025), and an oral poster in 13th EKMUD (Turkish Infectious Diseases and Clinical Microbiology Specialization Association), 10–14 May, Antalya, Türkiye.
Financial support
None.
Competing interests
The authors declared that no conflict of interest.

 Open access
Open access