


Introduction
Generalized anxiety disorder is one of the most prevalent mental disorders worldwide and represents one of the main causes of morbidity and mortality worldwide (Stein and Sareen, Reference Stein and Sareen2015). This disorder has an estimated lifetime prevalence around 3.7% (Ruscio et al., Reference Ruscio, Hallion, Lim, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Andrade, Borges, Bromet, Bunting, De Almeida, Demyttenaere, Florescu, De Girolamo, Gureje, Haro, He, Hinkov, Hu, De Jonge, Karam, Lee, Lepine, Levinson, Mneimneh, Navarro-Mateu, Posada-Villa, Slade, Stein, Torres, Uda, Wojtyniak, Kessler, Chatterji and Scott2017) with a wide variability according to the specific population and population group assessed, and with higher prevalence found in countries with higher economic development (Ruscio et al., Reference Ruscio, Hallion, Lim, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Andrade, Borges, Bromet, Bunting, De Almeida, Demyttenaere, Florescu, De Girolamo, Gureje, Haro, He, Hinkov, Hu, De Jonge, Karam, Lee, Lepine, Levinson, Mneimneh, Navarro-Mateu, Posada-Villa, Slade, Stein, Torres, Uda, Wojtyniak, Kessler, Chatterji and Scott2017).
The measure most widely used for both the screening of generalized anxiety disorder and general anxiety symptoms in the adult population is the Generalized Anxiety Disorder 7-Item Scale (GAD-7; Spitzer et al., Reference Spitzer, Kroenke, Williams and Löwe2006; Gregory K. Farber et al., Reference Farber, Gage, Kemmer and White2023). This self-reported measure consists of seven Likert-type items with a response scale ranging from 0 (‘Not at all’) to 3 (‘Nearly every day’), originally developed for primary care based on symptoms of generalized anxiety disorder included in the 4th Edition of the Diagnostic and Statistical manual of Mental Disorders (DSM-IV). Additionally, the GAD-7 has been also used in different contexts to screen for anxiety symptoms that can be associated with other mental disorders, such as post-traumatic stress disorder (Kroenke et al., Reference Kroenke, Spitzer, Williams, Monahan and Löwe2007; Plummer et al., Reference Plummer, Manea, Trepel and McMillan2016) making the GAD-7 a flexible measure for a variety of study designs and settings (Löwe et al., Reference Löwe, Decker, Müller, Brähler, Schellberg, Herzog and Yorck Herzberg2008; Ruiz et al., Reference Ruiz, Zamorano, García-Campayo, Pardo, Freire and Rejas2011; Johnson et al., Reference Johnson, Ulvenes, Øktedalen and Hoffart2019; Gregory K. Farber et al., Reference Farber, Gage, Kemmer and White2023). It is therefore not surprising that the GAD-7 has been prioritized as the standard measure for assessing anxiety by the Common Measures in Mental Health Science (CMMHS) joint initiative developed by funding bodies and scientific journals (Gregory K. Farber et al., Reference Farber, Gage, Kemmer and White2023).
Originally developed and validated on a predominantly Caucasian (80%) sample of patients from primary care centres across 12 states in the United States (US) (Spitzer et al., Reference Spitzer, Kroenke, Williams and Löwe2006) the GAD-7 has been translated and validated in many different languages such as Arabic (Sawaya et al., Reference Sawaya, Atoui, Hamadeh, Zeinoun and Nahas2016), Chinese (Zeng et al., Reference Zeng, He, Liu, Miao, Chen, Xu and Wang2013), Portuguese (Sousa et al., Reference Sousa, Viveiros, Chai, Vicente, Jesus, Carnot, Gordo and Ferreira2015), Urdu (Ahmad et al., Reference Ahmad, Hussain, Shah and Akhtar2017) or Spanish (García-Campayo et al., Reference García-Campayo, Zamorano, Ruiz, Pardo, Pérez-Páramo, López-Gómez, Freire and Rejas2010). It has shown an acceptable validity across different population groups within countries, including Brazil, Germany, Canada, South Africa or India (Löwe et al., Reference Löwe, Decker, Müller, Brähler, Schellberg, Herzog and Yorck Herzberg2008; Doi et al., Reference Doi, Ito, Takebayashi, Muramatsu and Horikoshi2018; Henn and Morgan, Reference Henn and Morgan2019; De Man et al., Reference De Man, Absetz, Sathish, Desloge, Haregu, Oldenburg, Johnson, Thankappan and Williams2021; Romano et al., Reference Romano, Ferro, Patte and Leatherdale2022). However, this evidence remains fragmentary as in most of the cases it is derived from studies just focusing on a single country. Additionally, despite the prioritization of the use of the GAD-7 for the screening of anxiety and its extended use worldwide, the evidence on the cross-cultural validity (i.e., the degree to which a questionnaire equivalently and accurately measures the same construct across different cultures or cultural groups) of the GAD-7 remains limited. Thus, a synthesis of the existing but scattered evidence on the cross-cultural comparability of the GAD-7 is essential for providing a more robust evidence for its global use as a screening tool for generalized anxiety disorder and, in general, for anxiety as proposed by CMMHS Initiative (Gregory K. Farber et al., Reference Farber, Gage, Kemmer and White2023). Additionally, this evidence would provide easy-to-access information on the value of the GAD-7 as an universal tool for the screenings for anxiety in clinical contexts across different cultural backgrounds.
Our aim was to systematically review, synthesize and assess the available evidence about the cross-cultural validity of the GAD-7, to arrive at an evidence-based recommendation about its cross-cultural use for screening.
Method
Search strategy and study selection
A systematic review of the literature on the cross-cultural validity of the GAD-7 was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA; Page et al., Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan, Chou, Glanville, Grimshaw, Hróbjartsson, Lalu, Li, Loder, Mayo-Wilson, McDonald, McGuinness, Stewart, Thomas, Tricco, Welch, Whiting and Moher2021) the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) framework (Mokkink et al., Reference Mokkink, Knol, Stratford, Alonso, Patrick, Bouter and de Vet2006) and the Popay et al. (Reference Popay, Roberts, Sowden, Petticrew, Arai, Rodgers, Britten, Roen and Duffy2006) guidance on the conduct of narrative synthesis for systematic reviews (Popay et al., Reference Popay, Roberts, Sowden, Petticrew, Arai, Rodgers, Britten, Roen and Duffy2006). The protocol of the systematic review was registered in the PROSPERO database (registration number: CRD42024536741).
The search was performed on April 21, 2024 in four databases MEDLINE, PubMed, APA PsycINFO and Embase, with no restriction on publication date. Studies assessing the cross-cultural validity of the GAD-7 from a quantitative perspective using primary or secondary data were included. Studies focusing on the assessment of other metric properties, such as reliability or other types of validity, or including study samples from just one culture or one population group, i.e., that did not include a comparison group, were excluded. The search terms used for this review were gathered upon consulting the COSMIN strategy for searching databases for studies of psychometric properties (Terwee et al., Reference Terwee, Jansma, Riphagen and De Vet2009; Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018) and were linked to two themes: instrument search (terms related to the GAD-7) and outcome search (terms related to cross-cultural validity). Other suggested themes, such as population (general population) and construct (generalized anxiety disorder), were disregarded upon testing as they seemingly generated a high number of irrelevant results. MeSH terms and keywords (i.e., ‘Cross-cultural comparison’, ‘cultural bias’, ‘general anxiety disorder’, ‘GAD-7’) linked by Boolean operators were used for the search. The complete search strategies used in each database are available in Appendix A. The searches were performed by a single researcher (AM). Studies assessing the measurement properties of the GAD-7 or its items and considering possible differences between two or more cultural groups were included. Non-peer reviewed publications and conference abstracts were excluded.
After removing the duplicated records, the eligibility of the studies was established in three consecutive stages. Firstly, all retrieved records underwent a title and abstract review by two independent researchers (AM, LBJ), and the discrepancies were assessed by a third researcher (JAT). Next, a full text review for those documents meeting the inclusion criteria was performed by AM, PY, LBJ. Discrepancies about the selection of a document for the narrative synthesis after the full text reading were resolved by another researcher (JAT) after his evaluation and consultation with other authors. In addition to the systematic search, a manual search by tracking backwards the citations included in the reference list of eligible papers was conducted to try to find potentially relevant documents fitting in the study objective and inclusion and exclusion criteria. Due to the very specific focus of the review the narrative synthesis was focused on summarizing the results of the studies finally selected based on their quality, rather than on identifying and discussing emerging themes different from the cross-cultural validity of the GAD-7.
Quality assessment
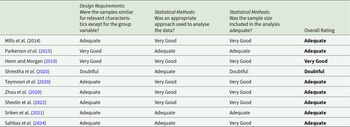
The assessment of the methodological quality of eligible studies was performed by 2 independent reviewers (AM and JAT) using the relevant criteria specific for cross-cultural validity/measurement invariance COSMIN Risk of Bias checklist (Mokkink et al., Reference Mokkink, de Vet, Prinsen, Patrick, Alonso, Bouter and Terwee2018; Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018). These criteria included: (1) whether the group subsamples shared most characteristics apart from the grouping variable (i.e., gender, age, socioeconomic status, potential diagnosis), (2) whether an appropriate methodological approach was deployed to analyse the data and (3) whether the group subsamples were large enough. Each of the studies was rated on each of the three proposed criteria using a four-point scale (very good, adequate, doubtful, inadequate). To determine the overall rating of the methodological quality of each study, the COSMIN manual suggests adopting the ‘worst score counts’ principle, meaning that if a study scored ‘inadequate’ in any criteria, its overall rating should subsequently be considered ‘inadequate’ (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018). This information is depicted in more detail in Appendix B.
In addition to rating the methodological quality, the quality criteria for suitable measurement properties were also examined in the studies finally included in the review, based on COSMIN criteria (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018). Each study was rated as providing sufficient (+), insufficient (–), or indeterminate (?) evidence, based on the analyses conducted and their results in relation to the cross-cultural validity of the GAD-7. The specific quality criteria for consider a questionnaire as a tool with suitable measurement properties are shown in the Appendix C. Upon rating the methodological quality and the outcome for each of the studies finally included based on the study design and statistical methods, the COSMIN manual suggests qualitatively summarizing the evidence and repeating the process for obtaining an overall outcome for the measure (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018). Specifically, the quality criteria for suitable measurement properties were applied to the general summary outcome, indicating whether the GAD-7 has sufficient (+), insufficient (–), inconsistent (±) or indeterminate (?) cross-cultural validity (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018). This rating was based on the ‘75% rule’, meaning that at least 75% of the studies included needed to have found cross-culturally valid results for the GAD-7’s cross-cultural validity to be rated as ‘sufficient’ (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018).
Finally, the evidence leading to the summary outcome was graded as of ‘high’, ‘moderate’, ‘low’, or ‘very low’ quality following a modified version of the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach. (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018). For applying the GRADE approach to the summary result of a measurement property review, the following factors were considered: risk of bias (i.e., the methodological quality of the studies), inconsistency (i.e., unexplained discrepancies across the results of the included studies), imprecision (i.e., potentially low total sample size of the included studies) and indirectness (i.e., evidence deriving from different populations than the population of interest). More detailed information about the COSMIN quality of evidence grading and the GRADE approach can be found in the Appendix D.
Data extraction and synthesis
Following Popay et al. (Reference Popay, Roberts, Sowden, Petticrew, Arai, Rodgers, Britten, Roen and Duffy2006) guidance (Popay et al., Reference Popay, Roberts, Sowden, Petticrew, Arai, Rodgers, Britten, Roen and Duffy2006) three distinct steps were completed for synthesizing the evidence from the studies finally included. First, a preliminary extraction and synthesis of the results was put together by one author (AM) using tabulation along with textual descriptions and the common rubrics suggested by the COSMIN guidelines for rating the methodological quality of the included studies and the nature of the outcomes. Data extraction included author year, GAD-7 language, study population and sample size, methodology, and main study findings. Additionally, specific psychometric analyses were considered (i.e., Confirmatory Factor Analysis or CFA, Differential Item Functioning or DIF). For the data extraction, floor and ceiling effects, as well as any limitations noted in each paper, were also considered. Second, the potential relationships among the available data were explored through subgroup and thematic analysis, including some further tabulation for highlighting overlapping outcomes across the included studies by two authors (AM, JAT). Third, an assessment of the robustness of the synthesis was conducted (AM and JAT) by applying the GRADE quality rating on the summary outcome and following the ‘best evidence synthesis’ as recommended by both the COSMIN group (Prinsen et al., Reference Prinsen, Mokkink, Bouter, Alonso, Patrick, de Vet and Terwee2018) and Popay et al. (Reference Popay, Roberts, Sowden, Petticrew, Arai, Rodgers, Britten, Roen and Duffy2006), where high-quality studies can weigh more heavily on the summary outcome compared to low-quality ones, especially in case of an inconsistency requiring resolution.
Results
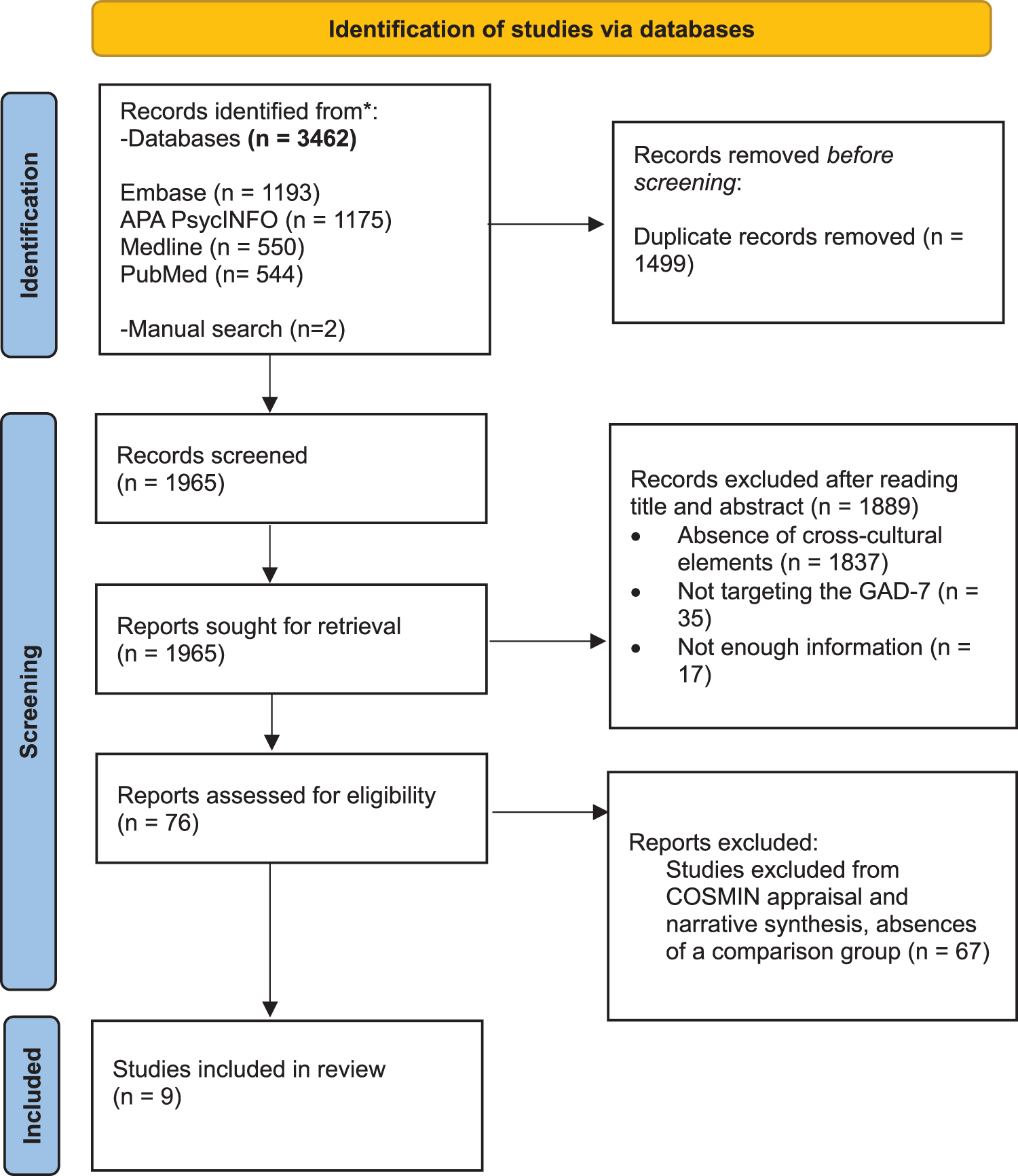
The original search yielded 1,965 unique records, of which all underwent title and abstract review while only 76 qualified for the full text review (Fig. 1). The full text review revealed that 67 of these studies lacked a cultural comparison, i.e., that the validity of the GAD-7 was assessed just considering one population group (culture), resulting in 9 included studies effectively assessing the cross-cultural validity of the GAD-7.
PRISMA flow diagram outlining the screening and selection process for measurement property studies assessing the cross-cultural validity of the GAD-7. Abbreviations: PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines; GAD-7: Generalized Anxiety Disorder-7; n: number of studies; COSMIN: Consensus-Based Standards for the Selection of Health Measurement Instruments.

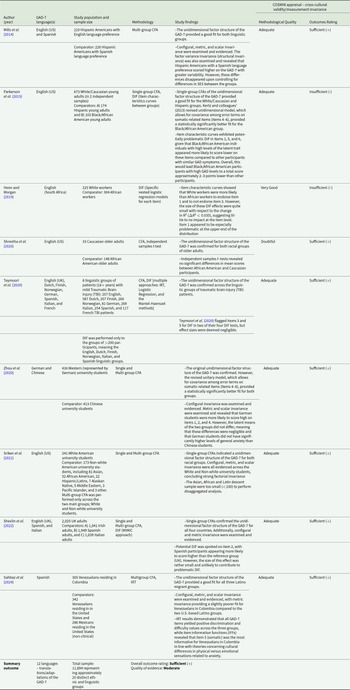
The 9 studies analysed included a total sample of 11,894 (53.7% female) individuals (Mills et al., Reference Mills, Fox, Malcarne, Roesch, Champagne and Sadler2014; Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Henn and Morgan, Reference Henn and Morgan2019; Shrestha et al., Reference Shrestha, Ramos, Fletcher, Kraus-Schuman, Stanley, Ramsey and Amspoker2020; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020; Zhou et al., Reference Zhou, Xu and Rief2020; Sriken et al., Reference Sriken, Johnsen, Smith, Sherman and Erford2021; Shevlin et al., Reference Shevlin, Butter, McBride, Murphy, Gibson-Miller, Hartman, Levita, Mason, Martinez, McKay, Stocks, Bennett, Hyland, Vallieres, Valiente, Vazquez, Contreras, Peinado, Trucharte, Bertamini, Panzeri, Bruno, Granziol, Mignemi, Spoto, Vidotto and Bentall2022; Sahbaz et al., Reference Sahbaz, Cox, Montero-Zamora, Salas-Wright, Maldonado-Molina, Bates, Pérez-Gómez, Mejía-Trujillo, Vos, Scaramutti, Perazzo, Duque, Garcia, Brown and Schwartz2024), representing approximately 20 different ethnic groups (e.g., Hispanics/Latins [Mills et al., Reference Mills, Fox, Malcarne, Roesch, Champagne and Sadler2014; Sahbaz et al., Reference Sahbaz, Cox, Montero-Zamora, Salas-Wright, Maldonado-Molina, Bates, Pérez-Gómez, Mejía-Trujillo, Vos, Scaramutti, Perazzo, Duque, Garcia, Brown and Schwartz2024] and Black/African americans [Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Henn and Morgan, Reference Henn and Morgan2019; Shrestha et al., Reference Shrestha, Ramos, Fletcher, Kraus-Schuman, Stanley, Ramsey and Amspoker2020]), and languages (i.e., English, Spanish, and French [Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020; Shevlin et al., Reference Shevlin, Butter, McBride, Murphy, Gibson-Miller, Hartman, Levita, Mason, Martinez, McKay, Stocks, Bennett, Hyland, Vallieres, Valiente, Vazquez, Contreras, Peinado, Trucharte, Bertamini, Panzeri, Bruno, Granziol, Mignemi, Spoto, Vidotto and Bentall2022]; Table 1). The primary statistical methods included Single and/or Multi- Confirmatory Factor Analysis (CFA) in 8 studies, and logistic regression for Differential Item Functioning (DIF) in 4 studies. The quality of seven of the studies was deemed ‘adequate’ (the comprehensive COSMIN rating results can be found in the Appendix E; Mills et al., Reference Mills, Fox, Malcarne, Roesch, Champagne and Sadler2014; Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020; Zhou et al., Reference Zhou, Xu and Rief2020; Sriken et al., Reference Sriken, Johnsen, Smith, Sherman and Erford2021; Shevlin et al., Reference Shevlin, Butter, McBride, Murphy, Gibson-Miller, Hartman, Levita, Mason, Martinez, McKay, Stocks, Bennett, Hyland, Vallieres, Valiente, Vazquez, Contreras, Peinado, Trucharte, Bertamini, Panzeri, Bruno, Granziol, Mignemi, Spoto, Vidotto and Bentall2022; Sahbaz et al., Reference Sahbaz, Cox, Montero-Zamora, Salas-Wright, Maldonado-Molina, Bates, Pérez-Gómez, Mejía-Trujillo, Vos, Scaramutti, Perazzo, Duque, Garcia, Brown and Schwartz2024).
Summary of findings and COSMIN appraisal ratings for each of the included studies

COSMIN: Consensus-Based Standards for the Selection of Health Measurement Instruments; GAD-7: Generalized Anxiety Disorder-7; CFA: Confirmatory Factor Analysis; DIF: Differential Item Functioning; IRT: Item Response Theory; SES: socioeconomic status.
Considering the overall outcome (Table 1), the GAD-7 had overall sufficient (+) cross-cultural validity. That is, more than 75% (7 out of 9 studies) presented sufficient (+) outcomes to evidence the unitary factor structure of the GAD-7 across the reference and comparator groups, while not detecting any statistically significant DIF in those studies assessing it. The remaining 2 studies demonstrated insufficient (−) cross-cultural validity upon non-negligible indications (Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Henn and Morgan, Reference Henn and Morgan2019), pointing to the presence of measurement biases against the comparator group (Black/African American and Black/South African) associated with the differential function of some of the questionnaire’s items. Additionally, the individual items of the GAD-7 flagged by the reviewed studies as potentially problematic in relation to cross-cultural validity could be found in Table 2. From the 5 studies testing for differences in the specific items using different approaches (Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Henn and Morgan, Reference Henn and Morgan2019; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020; Zhou et al., Reference Zhou, Xu and Rief2020; Shevlin et al., Reference Shevlin, Butter, McBride, Murphy, Gibson-Miller, Hartman, Levita, Mason, Martinez, McKay, Stocks, Bennett, Hyland, Vallieres, Valiente, Vazquez, Contreras, Peinado, Trucharte, Bertamini, Panzeri, Bruno, Granziol, Mignemi, Spoto, Vidotto and Bentall2022), 3 of them pointed out Item 1 (‘feeling nervous, anxious, or on edge’) as potentially problematic in relation to the cross-cultural validity (Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Henn and Morgan, Reference Henn and Morgan2019; Zhou et al., Reference Zhou, Xu and Rief2020) being the most reported item. Items 2 (Zhou et al., Reference Zhou, Xu and Rief2020; Shevlin et al., Reference Shevlin, Butter, McBride, Murphy, Gibson-Miller, Hartman, Levita, Mason, Martinez, McKay, Stocks, Bennett, Hyland, Vallieres, Valiente, Vazquez, Contreras, Peinado, Trucharte, Bertamini, Panzeri, Bruno, Granziol, Mignemi, Spoto, Vidotto and Bentall2022), 3 (Henn and Morgan, Reference Henn and Morgan2019; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020) and 5 (Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020) were reported as potentially problematic in 2 studies each.
GAD-7 items flagged as potentially problematic in relation to cross-cultural validity
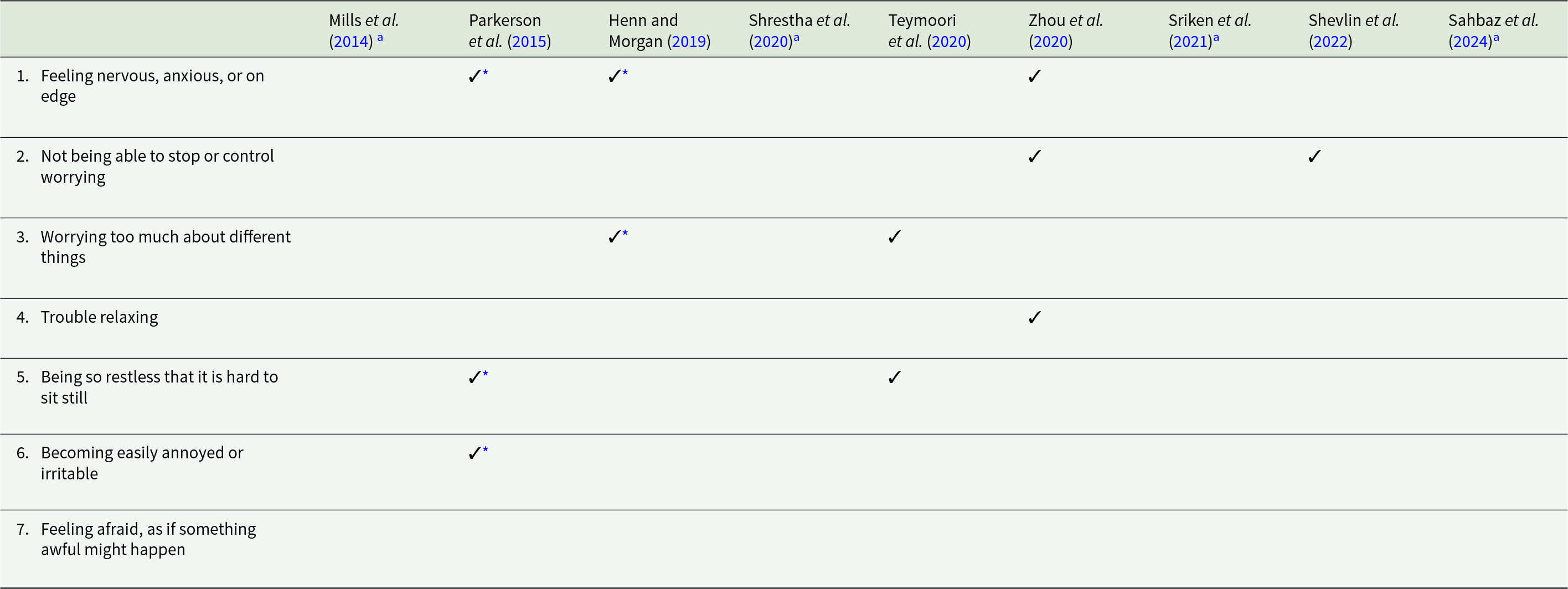
GAD-7: Generalized Anxiety Disorder-7.
a Not specifically tested for Differential Item Functioning (DIF).
* Statistical significant differences (p-value < 0.05).
Synthesizing the findings and summarizing the outcomes, altogether, the available evidence appears of ‘moderate’ quality upon applying the GRADE criteria (Table 3). From the 9 studies finally included, 7 had an adequate quality, 1 very good quality, and 1 doubtful quality. No quality points were lost for either risk of bias, as the majority of the studies included were of adequate methodological quality, nor for imprecision, as the total sample size was larger than 100. No points were deducted for inconsistency, as no serious contradiction was found among sufficient and insufficient/inconsistent results that was not resolved after implementing the ‘75% rule’. However, one quality point was lost for indirectness, as all included studies were performed in the desired context and population (non-clinical) except for two which recruited clinical populations (Shrestha et al., Reference Shrestha, Ramos, Fletcher, Kraus-Schuman, Stanley, Ramsey and Amspoker2020; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020).
COSMIN Appraisal Ratings per Included Study. Comprehensive rating per criterion of methodological quality for each of the included studies
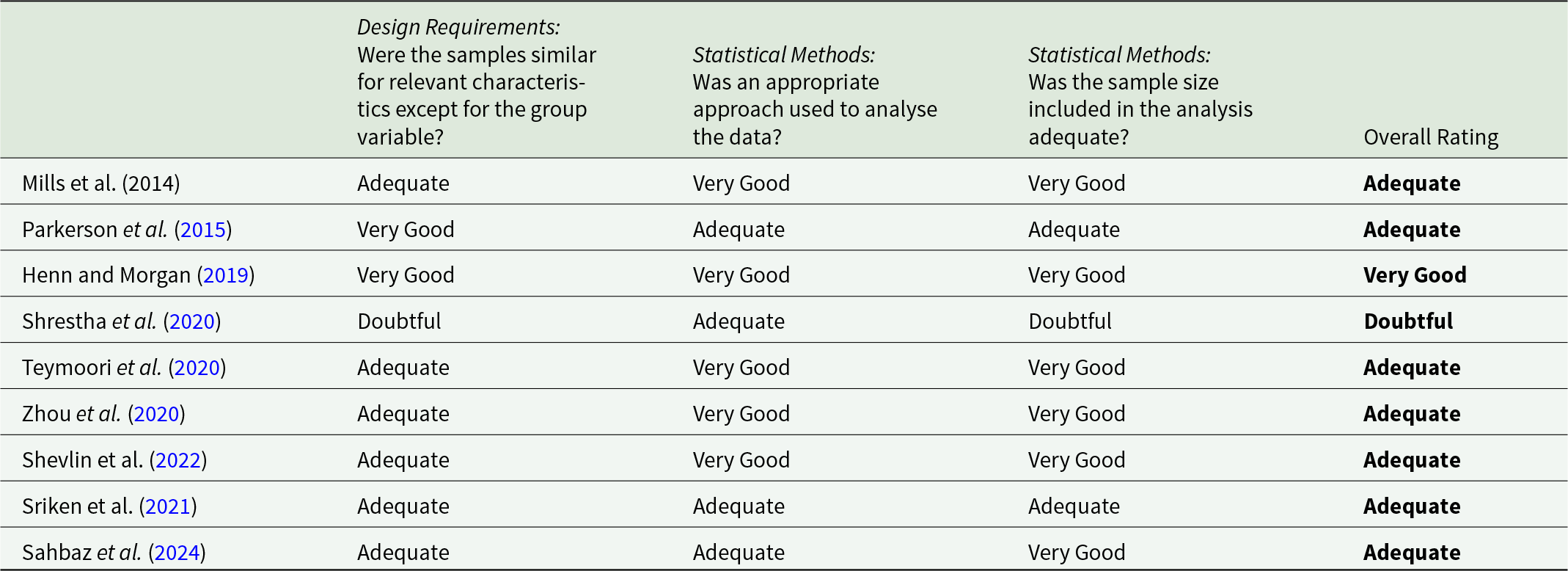
COSMIN: COnsensus-based Standards for the selection of health Measurement Instruments.
Discussion
To our knowledge this is the first study to date that has compiled, assessed and synthesized, the available literature regarding the cross-cultural validity of the GAD-7. Overall, while the evidence about its cross-cultural validity is very limited, the GAD-7 appears to be a cross-culturally valid tool for the assessment of generalized anxiety disorder and anxiety symptoms. The results also highlight a disproportionate paucity of studies on its cross-cultural validity when compared to the vast numbers of studies applying GAD-7 across multiple different cultural contexts. Due to the prioritization of the GAD-7 as a screening measure for anxiety disorders and until new high-quality evidence will be available, these results constitute a key first step for supporting its use for the assessment of anxiety in multi-cultural clinical and community settings, and therefore could constitute the necessary evidence-base for its use in public health and global health decision making in relation to anxiety.
From a public health perspective, the results found could serve to reassure researchers and clinicians that, overall, is likely that the same construct is being measured across different cultures when using the GAD-7. Ensuring the validity of the measure could be helpful to identify and compare the rates of generalized anxiety disorder and anxiety symptoms in different cultural contexts, therefore, aiding the screening and prevention of anxiety disorders at a population level. Besides, considering the cross-cultural performance of the specific items of the GAD-7, the differences found for item 1 between black and white participants in two different contexts could suggest a possible ceiling effect, and this could reflect a lower severity of GAD symptoms than is experienced. As pointed out by previous research (Lewis-Fernández et al., Reference Lewis-Fernández, Hinton, Laria, Patterson, Hofmann, Craske, Stein, Asnaani and Liao2010; Marques et al., Reference Marques, Robinaugh, Leblanc and Hinton2011; Hofmann and Hinton, Reference Hofmann and Hinton2014), these differences could be related to a variety of factors including differing cultural somatic awareness, differing perceptions of stigma or mental health, differing cultural descriptions of anxiety symptoms, or differing use of language. Regarding this, clinicians should take this in count in this specifically populations. However, while further specific research in this area is required, it should be highlighted that the magnitude of the DIF found was small and do not call into question the overall performance of the GAD-7 and its cross-cultural validity as a screening tool for anxiety.
The external validity of the study findings should be discussed as most of the articles reviewed used convenience samples. This convenience sampling allowed the access to large comparable samples and subsamples but compromised the generalizability and representativeness of the findings to other settings and populations. Besides, 6 out of the 9 studies (Parkerson et al., Reference Parkerson, Thibodeau, Brandt, Zvolensky and Asmundson2015; Henn and Morgan, Reference Henn and Morgan2019; Shrestha et al., Reference Shrestha, Ramos, Fletcher, Kraus-Schuman, Stanley, Ramsey and Amspoker2020; Teymoori et al., Reference Teymoori, Real, Gorbunova, Haghish, Andelic, Wilson, Asendorf, Menon and von Steinbüchel2020; Zhou et al., Reference Zhou, Xu and Rief2020; Sahbaz et al., Reference Sahbaz, Cox, Montero-Zamora, Salas-Wright, Maldonado-Molina, Bates, Pérez-Gómez, Mejía-Trujillo, Vos, Scaramutti, Perazzo, Duque, Garcia, Brown and Schwartz2024) were secondary data analyses, i.e., analyses of data collected for other purposes rather than for the study of the cross-cultural validity of the GAD-7. This data reuse could produce their own biases for the study of cross-cultural differences of a measure, particularly in relation to the sample selected and the possible representation and comparability of the different population groups. However, while further representative studies to assess the cross-cultural validity of the GAD-7 are needed, the results derived from convenience samples could serve as a feasible alternative to provisionally support its suitability to be used for the screening of anxiety symptoms in multi-cultural settings.
Different study limitations must be discussed. First, those associated with the COSMIN method used that, for example, has attracted some discussion and criticism around being reliant more on expert opinion than evidence, its focus on classical test theory, and its insufficient focus on underlying constructs measured (McKenna and Heaney, Reference McKenna and Heaney2021; Mokkink et al., Reference Mokkink, Terwee, Bouter, Alonso, de Vet and de Vet2021). However, the COSMIN initiative guidelines are one of the most rigorous approaches for assessing the metric properties of a measure, and that these guidelines follow a continuous revision process making them a suitable alternative for this assessment. Another limitation that should be mentioned is that all the studies reviewed were considered equally for estimating the overall outcome, since the majority exhibited adequate methodological quality (Mokkink et al., Reference Mokkink, Knol, Stratford, Alonso, Patrick, Bouter and de Vet2006). For the purposes of the ‘best evidence synthesis’, we initially considered weighing down or excluding one study that receive a COSMIN rating of ‘doubtful’ quality due to its disproportionate reference and comparator groups in terms of size and within group characteristics.(Shrestha et al., Reference Shrestha, Ramos, Fletcher, Kraus-Schuman, Stanley, Ramsey and Amspoker2020). However, due to its valuable sample we decided not weight down the study, making it one of the only reviewed studies to contribute substantial participant data from hard-to-reach communities that often end up underrepresented in research. Besides, the limitation in relation to specific analyses not focused on the assessment of cross-cultural validity, such as content validity analyses, could be mentioned. While these analyses could show critical aspects of any measure, the primary focus of this review was to assess studies that had already implemented adapted versions of the GAD-7, and to analyse their cross-cultural validity. Moreover, the content validity and other relevant metric properties of the GAD-7 have been previously established in its original development and initial adaptations. As such, this review assumes that the included studies have built upon this foundational work. Finally, it is important to acknowledge that although the present review contains studies including 20 distinct cultural groups, only one study was carried out outside the US and Europe (Henn and Morgan, Reference Henn and Morgan2019), limiting the generalizability of this review globally and indicating a clear knowledge gap in the literature. Despite this, given the wide range of cultures included and until new high-quality evidence will be available, the results from this review offer a preliminary perspective on the cross-cultural validity of the GAD-7, and could be considered key evidence to support its use from a global perspective.
In conclusion, this review highlights an important evidence gap in relation to the cross-cultural performance of the GAD-7. Additionally, while with limitations, the evidence available to date points out that the GAD-7 is likely to be a cross-culturally valid measure for the screening of generalized anxiety disorder and, in general, of anxiety. This information could be helpful for clinicians, researchers and decision makers to accurately assess, compare and therefore address data on anxiety disorders as a clinical and public health issue using a brief and simple instrument. Therefore, while further primary research in this area is needed to strengthen the evidence base about the cross-cultural validity of the GAD-7, the results from this review could serve to provisionally support its use in multi-cultural settings, and to inform clinical, public health and global mental health decision making in relation to anxiety.
Availability of data and materials
All the data derived from the study and the materials used for its development are available upon request to the corresponding author.
Author contributions
All authors conceived and designed the study. JAT, AM, LBJ and PY had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data. AM, PY and LBJ contributed equally and developed the revision process. All authors interpreted the findings derived from the literature review. AM, LBJ, PY and JAT drafted the first manuscript version. JA, GV and JV supervised the study. All authors critically revised the manuscript for intellectual content and gave feedback on the first version. All authors agreed to the submission of the final draft and had final responsibility for the decision to submit for publication. Anastasia Mantzari, Lorena Botella-Juan and Prateek Yadav are equal first authors. Gemma Vilagut, Prof. Jordi Alonso and Jorge Arias-de la Torre are equal last authors.
Financial support
This work is partially funded by the Medical Research Council (MRC) and Guy’s charity, CIBER – Consorcio Centro de Investigación Biomédica en Red, Instituto de Salud Carlos III cofunded by the European Union (grant numbers PI23/00073; PI19/00109), and the Subdirecció General d’Addiccions, VIH, ITS i Hepatitis Víriques of the Secretaria de Salut Pública (Departament de Salut, Generalitat de Catalunya). This article represents independent research part funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. LBJ have a predoctoral contract financed by Junta de Castilla y León – Consejería de Educación (Spain) using the European Social Fund (EDU/842/2022). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests
All authors declare that they have no conflict of interest.
Ethical standards
This study reports the results from a systematic review of the literature based exclusively on data from previously published studies and publicly available sources. As no new data were collected, and no identifiable personal information has been used, ethical approval was not required in accordance with institutional and international ethics guidelines. The review was conducted and reported following established standards for systematic reviews of the literature. The protocol of the systematic review has been registered in the PROSPERO database (registration number: CRD42024536741).
Appendix A. Search filter and results per database
Medline
Search conducted in Medline (via Ovid): 21 April 2024
Results retrieved: 550
Search: ((exp Psychometrics/OR exp Cross-cultural comparison/OR exp Reproducibility of results/OR exp Culture/OR exp Translating/OR exp Factor Analysis, Statistical/OR exp Ethnicity/ OR “Psychometric properties”.mp. OR “Cross-cultural validity”.mp. OR “Cross-cultural validation” .mp. OR “Cross-cultural comparability”.mp. OR “Cross-cultural equivalence”.mp. OR “Cross-cultural measurement invariance”.mp. OR “Cultural difference*”.mp. OR “Cultural bias*”.mp. OR “Construct validity” .mp. OR “Factor structure”.mp. OR “Differential item functioning” .mp. OR DIF.mp. OR “Item response theory” .mp. OR “Confirmatory factor analysis” .mp. OR “Exploratory factor analysis”.mp. OR Translation .mp. OR “Cultural adaptation” .mp. OR Validation .mp. OR “Measurement invariance”.mp.) AND (“Generalized Anxiety Disorder-7”.mp. OR “Generalized Anxiety Disorder-7 (GAD-7)”.mp. OR “General Anxiety Disorder-7”.mp. OR “General Anxiety Disorder-7 (GAD-7)”.mp. OR GAD-7.mp. OR GAD7.mp.))
PubMed
Search conducted in PubMed: 21 April 2024
Results retrieved: 544
Search: ((“Psychometrics “[mesh] OR “Cross-cultural comparison “[mesh] OR “Ethnicity”[mesh] OR “Reproducibility of results “[mesh] OR “Culture “[mesh] OR “Translating “[mesh] OR “Factor Analysis, Statistical “[mesh] OR “Validation Study”[mesh] OR “Psychometric properties”[tiab] OR “Cross-cultural validity”[tiab] OR “Cross-cultural validation “[tiab] OR “Cross-cultural comparability “[tiab] OR “Cross-cultural equivalence”[tiab] OR “Cross-cultural measurement invariance”[tiab] OR “Cultural difference*”[tiab] OR “Cultural bias*”[tiab] OR “Construct validity “[tiab] OR “Factor structure”[tiab] OR “Differential item functioning “[tiab] OR “DIF”[tiab] OR “Item response theory “[tiab] OR “Confirmatory factor analysis “[tiab] OR “Exploratory factor analysis”[tiab] OR “Cultural adaptation “[tiab] OR “Validation “[tiab] OR “Measurement invariance”[tiab]) AND (“Generalized Anxiety Disorder-7”[tiab] OR “Generalized Anxiety Disorder-7 (GAD-7)”[tiab] OR “General Anxiety Disorder-7”[tiab] OR “General Anxiety Disorder-7 (GAD-7)”[tiab] OR “GAD-7”[tiab] OR “GAD7”[tiab]))
APA PsycINFO
Search conducted in APA PsycINFO (via Ovid): 21 April 2024
Results retrieved: 1175
Search: ((exp Psychometrics/OR exp Cross Cultural Validity/ OR exp Cross Cultural Differences/ OR exp Cross Cultural Test Adaptation/OR exp Item Response Theory/OR exp Classical Test Theory/OR exp Differential Item Functioning/OR exp “Item Analysis (Statistical)”/ OR exp Measurement Invariance/OR exp Ethnic Identity/OR exp Foreign Language Translation/OR exp Factor Structure/OR exp Cultural Test Bias/ OR exp Cultural Bias/OR exp “Racial and Ethnic Differences”/OR exp Construct Validity/OR exp Test Bias/OR exp Confirmatory Factor Analysis/OR exp Exploratory Factor Analysis/ OR exp Adaptation/OR Psychometrics.mp. OR “Psychometric properties”.mp. OR “Cross-cultural validity”.mp. OR “Cross-cultural validation” .mp. OR “Cross-cultural comparability”.mp. OR “Cross-cultural equivalence”.mp. OR “Cross-cultural measurement invariance”.mp. OR “Cultural difference*”.mp. OR “Cultural bias*”.mp. OR “Construct validity” .mp. OR “Factor structure”.mp. OR “Differential item functioning” .mp. OR DIF.mp. OR “Item response theory” .mp. OR Ethnicity .mp. OR Translation .mp. OR Adaptation.mp. OR “Cultural adaptation” .mp. OR Validation .mp. OR “Measurement invariance”.mp.) AND (“Generalized Anxiety Disorder-7”.mp. OR “Generalized Anxiety Disorder-7 (GAD-7)”.mp. OR “General Anxiety Disorder-7”.mp. OR “General Anxiety Disorder-7 (GAD-7)”.mp. OR GAD-7.mp. OR GAD7.mp.))
Embase
Search conducted in Embase (via Ovid): 21 April 2024
Results retrieved: 1193
Search: ((exp Psychometry/OR exp Cultural Factor/OR exp Ethnicity/ OR exp “Ethnic of Racial Aspects”/OR exp Ethnic Group/OR exp Ethnic Identity/OR exp Cultural Bias/OR exp Construct Validity/OR exp Factorial Analysis/OR exp Confirmatory Factor Analysis/OR exp Exploratory Factor Analysis/OR exp Validation Study/OR exp Language/OR Psychometrics.mp. OR “Psychometric properties”.mp. OR “Cross-cultural validity”.mp. OR “Cross-cultural validation” .mp. OR “Cross-cultural comparability”.mp. OR “Cross-cultural equivalence”.mp. OR “Cross-cultural measurement invariance”.mp. OR “Cultural difference*”.mp. OR “Cultural bias*”.mp. OR “Factor structure”.mp. OR “Differential item functioning” .mp. OR DIF.mp. OR “Item response theory” .mp. OR Translation .mp. OR “Cultural adaptation” .mp. OR “Measurement invariance”.mp.) AND (“Generalized Anxiety Disorder-7”.mp. OR “Generalized Anxiety Disorder-7 (GAD-7)”.mp. OR “General Anxiety Disorder-7”.mp. OR “General Anxiety Disorder-7 (GAD-7)”.mp. OR GAD-7.mp. OR GAD7.mp.))
Appendix B. COSMIN risk of bias checklist box 5 – cross-cultural validity/measurement invariance

COSMIN: COnsensus-based Standards for the selection of health Measurement Instruments; IRT: Item Response Theory; MGCFA: Multigroup Confirmatory Factor Analysis; N/A: Not applicable.
Appendix C. COSMIN criteria for good measurement properties

COSMIN: COnsensus-based Standards for the selection of health Measurement Instruments; DIF: Differential Item Functioning.
Appendix D. COSMIN quality of evidence grading – the GRADE approach

COSMIN: COnsensus-based Standards for the selection of health Measurement Instruments; GRADE: Grading of Recommendations, Assessment, Development, and Evaluations; n = sample size.


 Open access
Open access