


A growing workforce paradox
The UK psychiatry medical workforce has faced persistent recruitment and retention challenges for several decades. Reference Halder and Mulliez1 In recent years, however, the dominant narrative has shifted. Recent recruitment rounds have attracted record numbers of applications, driving an unprecedented rise in competition ratios. 2 In the 2025 recruitment cycle, over 10 000 applicants competed for fewer than 500 psychiatry core training posts, resulting in a competition ratio of approximately 21:1. Reference Bowie3 However, this figure should be interpreted with caution, as rising application numbers reflect not only increased interest in psychiatry but also multi-specialty applications and the growing proportion of international medical graduates (IMGs). Reference Aveyard and Asbridge4 Nonetheless, it suggests an increasingly competitive environment in which to apply to the specialty.
Despite this apparent surge in interest at the point of entry, these strong recruitment figures coexist with substantial workforce gaps at more senior levels, suggesting that the challenge lies not in attracting applicants but in retaining doctors throughout the training pathway, alongside supporting career progression in non-training roles, particularly at the transition into consultant roles. The national workforce census shows that 27% of consultant posts and 32% of specialty, associate specialist and specialist (SAS) posts are vacant or filled by non-substantive psychiatrists, indicating substantial gaps at senior levels (RCPsych, 2025). 5 National workforce data show a striking pattern: near-equivalent outflows offset inflows. For example, in 2020, 1536 psychiatrists joined the National Health Service (NHS) while 1455 left, producing almost no net gain. Reference Dave6 Attrition is not evenly distributed across the training pathway: analysis of the UK Medical Education Database (UKMED), a national dataset tracking UK doctors’ training progression, shows that attrition is greatest at the transition from core to higher specialty training, with 57% of trainees not progressing directly from core training year 3 (CT3) to higher specialty training year 4 (ST4). Reference Silkens, Sarker and Medisauskaite7 The same study suggests that non-progression at this stage may relate to factors including examination requirements, limited availability of higher training posts and wider training pressures. Reference Silkens, Sarker and Medisauskaite7 The Royal College of Psychiatrists (RCPsych) has explicitly acknowledged this disconnect between recruitment activity and higher-level capacity: only 268 full-time equivalent consultant psychiatrists joined the NHS workforce in the 8 years to March 2024, against a target of 1040, with vacancy rates in mental health trusts more than double those in acute trusts. 8 Together, these trends point to a recruitment–retention paradox: psychiatry now attracts unprecedented competition at entry, yet remains unable to generate corresponding growth in its senior workforce.
A conceptual gap: the recruitment–retention divide in workforce planning
The current workforce discourse in psychiatry tends to treat recruitment, selection and retention as separate policy domains. Recruitment initiatives focus on increasing exposure and application numbers through the RCPsych Choose Psychiatry campaign, while retention strategies concentrate on well-being and mid-career support. 8 What is largely missing is a way of examining whether the doctors drawn into psychiatry and selected into training are aligned with the clinical realities of psychiatric practice over time. This division obscures the systemic links between who enters psychiatry, how doctors are selected and who ultimately remains. In practice, progression through training is increasingly non-linear with delayed completion, movement between programmes and less-than-full-time training. Reference Lock and Carrieri9 When rising recruitment pressure is being channelled into a system unable to convert volume into sustained progression, apparent gains at entry may fail to translate into long-term workforce capacity and sustainable staffing, as observed across the wider health and care system. Reference Anderson, O’Neill, Macleod Clark, Street, Woods and Johnston-Webber10 This highlights the need for training structures that better support progression through key transition points. Reference Silkens, Sarker and Medisauskaite7
The focus on rising competition ratios as indicators of improved recruitment, however, can obscure underlying weaknesses in the workforce pipeline. In psychiatry, rising application numbers may reflect not only interest in the specialty but also structural factors that shape application behaviour. The UK psychiatry workforce remains highly dependent on IMGs. Reference Lagunes-Cordoba, Maitra, Dave, Matheiken and Oyebode11 In parallel, post-COVID changes to national selection processes, particularly the use of the Multi-Specialty Recruitment Assessment (MSRA) as the sole selection criterion for core psychiatry training, have made it easier for applicants to apply strategically across multiple specialties. In this context, rising application volume may reflect labour-market pressures rather than a proportional increase in person–specialty alignment. Reference Aveyard and Asbridge4 Figure 1 provides a conceptual anchor for the model by illustrating how the interaction between person–specialty alignment and retention over time generates four distinct workforce outcomes. Where alignment and retention are both high, a sustainable workforce emerges; where alignment is high, but retention is low, the system loses well-matched clinicians; where alignment is low, but retention is high, staff remain despite limited role fit; and where both are low, persistent misalignment and turnover occur.
A conceptual anchor for the model by illustrating how the interaction between person–specialty alignment at selection and retention over time generates four distinct workforce outcomes.

This pattern highlights the need for a framework that considers entry into psychiatry alongside downstream workforce outcomes. In this Feature, we address this gap by introducing the pressurised leaky funnel, a systems-based conceptual model that builds on established pipeline metaphors used in workforce research to integrate recruitment, selection and retention into a single structure. By linking upstream recruitment pressures with cumulative attrition downstream, the model offers a framework for reinterpreting recent recruitment trends and for supporting more coherent, whole-pathway approaches to psychiatry workforce planning (see Fig. 2).
The pressurised leaky funnel model for the psychiatry workforce.

The pressurised leaky funnel
Stage 0: Exposure and intent
Exposure to psychiatry during undergraduate and early postgraduate studies shapes career interests and early professional identity. The literature consistently identifies clinical placement quality, stigma, role modelling and perceived status as key influences on whether psychiatry is experienced as a feasible and attractive future career. Reference Choudry and Farooq12 National initiatives, including undergraduate curriculum reform, have successfully widened the funnel’s mouth by destigmatising the specialty. Reference Halder and Mulliez1 However, rather than being fixed at entry, interest in psychiatry evolves gradually, with many doctors deciding to pursue the specialty later in training after positive postgraduate experiences. Reference Wolstenholme, McKinnon and Lloyd13 Early exposure to psychiatry may not fully reflect the clinical realities of the specialty, such that recruitment may partly reflect broader interests in holistic and relational models of care rather than a specific commitment to psychiatry. Some applicants may therefore be drawn to psychiatry for its perceived alignment with these values, which may not always translate into sustained commitment as the realities of practice become clearer, potentially contributing to downstream attrition or transition into other specialties. Reference Choudry and Farooq12
Stage 1: Application
The current surge in applications to psychiatry likely reflects a mix of intrinsic motivations and strategic application behaviours. Psychiatry has increasingly become an entry route into the NHS workforce or a geographically flexible backup option, rather than a committed career choice. As Ferreira et al Reference Ferreira14 rightly pointed out, as competition intensifies across medicine, doctors are casting a wider net, driving an ‘application inflation’ that dilutes the true commitment to a specialty. The limitations of competition ratios as indicators of workforce sustainability are illustrated by recent data: while the competition ratio for core psychiatry training has surged to 21.8:1, higher specialty ratios remain comparatively low at 1.39:1. This unprecedented 20-fold discrepancy suggests a highly heterogeneous applicant pool at the point of entry, although the pool for higher training is substantially narrower, having already been filtered through core training selection and progression.
National workforce data further illustrate this heterogeneity at the level of applicant composition: UK graduates comprise only 19% of appointable applicants for core psychiatry training, while IMGs comprise 81%. Recent NHS England analysis under the Medical Training (Prioritisation) Act suggests that psychiatry competition ratios may fall substantially, from approximately 12.4:1 to 2.4:1. 15 These workforce data suggest that the increase in psychiatry applications reflects highly heterogeneous motivations, rather than a true increase in the specialty’s popularity alone.
Stage 2: Selection
Selection represents the systems that attempt to filter upstream volume into quality. In recent years, the MSRA has become the sole ranking tool for core psychiatry training posts and has demonstrated predictive validity for subsequent examination performance. Reference Tiffin, Morley, Paton, Chakraborty and Patterson16 However, evidence linking MSRA performance to psychiatry-specific competencies, retention or long-term workforce outcomes remains limited. As a generic assessment used across multiple specialties, the MSRA does not have specific weighting for attributes central to psychiatric practice, such as tolerance for uncertainty and relational capability. This constrains robust appraisal of whether current selection processes identify candidates best matched to the emotional and relational demands of the specialty.
In this context, the current selection mechanism may function as a relatively blunt instrument that prioritises efficiency while offering limited insight into broader person–specialty fit. Reference Challinor and Whyler17 Selection systems inevitably signal what a specialty values. Heavy reliance on formal metrics may still under-capture attributes central to psychiatric practice, such that misalignment only becomes apparent later in training, creating a ‘latent leak’ in which specialty-specific fit is filtered after entry. Reference Brenner, Balon, Coverdale, Beresin, Guerrero and Louie18
Stage 3: Training environment
The training environment tests theoretical ‘fit’ against clinical reality and becomes the primary site of attrition. During psychiatry training, trainees often encounter a collision between their expectations of the specialty and the realities of clinical practice, characterised by rota instability, professional isolation and high emotional demands. Reference Medisauskaite, Alexander, Rich, Knight, Adesalu and Silkens19 Attrition is also concentrated early in psychiatry training and has been associated with factors such as working conditions, autonomy and flexibility, rather than examination failure or lack of ability. Reference Lock and Carrieri9,Reference Medisauskaite, Alexander, Rich, Knight, Adesalu and Silkens19 This stage is particularly challenging for IMGs and minoritised groups, who face the compounded pressures of discrimination and differential attainment. Reference Lagunes-Cordoba, Maitra, Dave, Matheiken and Oyebode11 Without the buffer of high-quality supervision and team belonging, Reference Varvari, Tribe, Moghaddam and Shiner20 system-level factors contribute to burnout and actively erode the resilience and commitment of its workforce, driving resident doctors’ decisions to take breaks from or exit training. Reference Lock and Carrieri9 The ongoing industrial action by resident doctors serves as a potent indicator of this systemic dissatisfaction, where the perceived erosion of pay and conditions has tipped the scales against retention. These conditions systematically erode motivation and belonging as early assumptions about the specialty are tested against clinical reality, alongside wider concerns that psychiatrists’ professional autonomy has been progressively eroded in contemporary practice. Reference Howard21 The increasing introduction of new roles within mental health services may improve service delivery; however, it may also introduce role ambiguity and additional supervision demands, with negative implications on training experience and team functioning. Reference Sanger, Hodgson, Wood, Nelson and Long22
Stage 4: Career outcomes
The final output of the funnel represents a complex recalibration of career goals. This stage reflects cumulative identity-based misalignment and declining expectancy of a sustainable consultant role. While some leakage, such as less-than-full-time working, portfolio careers and planned leave, represents healthy adaptation to modern practice, and highlights the importance of supportive structures that enable retention following return, late-stage attrition often signals a fundamental failure of the effort–reward bargain. Senior clinicians are less likely to leave due to person–environment misfit than because the sustainability of the role has diminished under sustained workload pressures. Increasing structural rigidity may drive late-stage attrition, as limited flexibility in job planning leaves some clinicians with little alternative but to exit the NHS when they might otherwise have preferred reduced or portfolio roles. Reference Lock and Carrieri9,Reference Anderson, O’Neill, Macleod Clark, Street, Woods and Johnston-Webber10
Theoretical mechanisms of the model
The stages of the pressurised leaky funnel describe where workforce loss occurs across the psychiatry training pathway. The purpose of this section is to explain why these losses occur by linking each stage to established theories from medical education and organisational psychology (see Table 1).
Theoretical foundations of the pressurised leaky funnel, showing how different lenses explain behaviour and attrition across the psychiatry training pathway

Stage 0: Exposure and intent
Early interest in psychiatry is shaped by social identity processes. Exposure to role models, clinical environments and the culture of the specialty influences whether individuals begin to see psychiatry as a career that fits who they are and who they might become.
Stage 1: Application
The applicant inflation at the funnel mouth can be explained by social-cognitive career theory, which proposes that individuals are more likely to pursue careers in which they believe they can succeed (self-efficacy) and that are expected to deliver valued outcomes (outcome expectations). Reference Lent, Brown and Hackett23 In the current psychiatry recruitment context, generic selection tools and labour-market constraints increase the perceived attainability of a psychiatric training post, which may inflate application volume even when longer-term fit with the specialty remains uncertain.
Stages 2–3: Selection and training environment
The workforce dynamics during selection and training stages are captured by the concept of person–specialty alignment, which encompasses both identity-based fit (whether doctors see themselves as psychiatrists) and work-based fit (whether the realities of psychiatric practice are sustainable for them). Identity-based fit is explained by social identity and self-categorisation theory, which proposes that individuals adopt group identities when they perceive a match between their own attributes and the perceived characteristics of the group. Reference Turner, Hogg, Oakes, Reicher and Wetherell24 Work-based fit is explained by person–environment fit theory, which conceptualises alignment between individuals and their work environments as a key determinant of job satisfaction and retention, with misalignment associated with stress and attrition. Reference Medisauskaite, Alexander, Rich, Knight, Adesalu and Silkens19 In psychiatry training, this alignment is not fixed at entry but socially constructed and tested over time through exposure to emotionally demanding clinical work, supervisory relationships and the informal or ‘hidden’ aspects of training culture. Reference Choudry and Farooq12
Stage 3: Training environment
Psychiatrists’ decisions to remain or quit training can also be explained by self-determination theory, which proposes that sustained motivation depends on the fulfilment of three psychological needs: autonomy, competence and relatedness. Reference Ryan and Deci25 Training environments characterised by workload pressure, isolation and limited supervision systematically frustrate these needs, increasing intentions to leave. Reference Medisauskaite, Alexander, Rich, Knight, Adesalu and Silkens19
Stage 4: Career outcomes
By the later stages of training and early consultancy, early commitment to psychiatry is tested against the realities of responsibility and long-term role sustainability. Late-stage exits can be understood through the interaction between professional identity formation and expectancy theory. Professional identity formation, defined here as the developmental process through which doctors internalise the norms of psychiatry and come to see themselves as psychiatrists, is vulnerable to erosion in stigmatised and marginalised specialties. Reference Brenner, Balon, Coverdale, Beresin, Guerrero and Louie18,Reference Varvari, Tribe, Moghaddam and Shiner20 Expectancy theory further suggests that clinicians act as rational agents who continually weigh the effort required to complete training against the perceived likelihood and value of the rewards, such that exit becomes rational when a sustainable consultant role is no longer seen as attainable. Reference Vroom26 Together, these theories explain why different parts of the workforce funnel leak, linking application behaviour, selection and retention within a single explanatory framework.
Implications for workforce reform
Broadening the definition of workforce success
Current workforce indicators, such as competition ratios and fill rates, capture entry interest but offer only a partial view. To build a sustainable workforce, workforce planning must move beyond recruitment metrics, incorporating progression rates, time-to-completion and consultant retention to capture longitudinal throughput and identify where capacity is being lost. Reference Anderson, O’Neill, Macleod Clark, Street, Woods and Johnston-Webber10,Reference Brown, Hoverd, Montgomery, Burford and Vance27 This reframes workforce sustainability away from short-term staffing levels towards systems that support progression and long-term contribution. Reference Brown, Hoverd, Montgomery, Burford and Vance27 In this context, this may also reflect a misalignment between how psychiatry is structured in training and the generalist, complexity-oriented nature of contemporary clinical practice. Reference Whitty and Powis28 This raises the possibility that psychiatry training could be more closely aligned with other community-based, generalist specialties (e.g. general practice and palliative care). Recent policy changes, including the Medical Training (Prioritisation) Act, which has now become law, are expected to reduce headline competition ratios. 15 However, the pressurised leaky funnel highlights that workforce sustainability will remain constrained unless downstream progression and retention are addressed in parallel. Viewed through the lens of Fig. 1, the central challenge for workforce reform is to move the system away from patterns of low alignment and low retention and towards the quadrant representing sustainable workforce capacity. This requires attention not only to how doctors enter psychiatry, but also to how training environments sustain commitment over time.
Optimising recruitment and selection for person–specialty fit
Selection operates at the interface between upstream pressures and downstream outcomes. If person–specialty fit shapes retention, selection systems must do more than rank candidates by academic performance alone. Selection would ideally assess professional alignment using evidence-based approaches: potentially structured scenario-based or reflective interviews. Reference Anderson, O’Neill, Macleod Clark, Street, Woods and Johnston-Webber10 However, such approaches carry significant resource implications, including increased demands on clinician time and administrative capacity. Any expansion of selection processes should therefore be accompanied by evaluation of cost-effectiveness and be assessed in relation to their impact on downstream outcomes such as training progression and retention. Key to this process will be the valid assessment of non-academic attributes salient to practice in the specific specialty. Reference Patterson, Knight, McKnight and Booth29 Each component of a selection process must add value and be based on evidence to support its fit to the selection process’s aim, rather than on received wisdom. The RCPsych’s recent establishment of a National Recruitment and Selection Processes Task and Finish Group to review selection tools represents a step towards balancing efficiency with alignment. 2 Prioritising attributes salient to psychiatric practice may reduce the ‘latent leaks’ associated with early misalignment.
Cultivating retention through the training environment
The model positions the training environment as a central determinant of retention. Evidence consistently links workload, supervision quality, psychological safety and team belonging to trainee well-being and intentions to remain in psychiatry. Reference Medisauskaite, Alexander, Rich, Knight, Adesalu and Silkens19 Treating stable team structures as core educational infrastructure, rather than peripheral well-being initiatives, reframes retention as a structural responsibility for organisations. Addressing differential training experiences, particularly for IMGs and minoritised residents, remains essential to workforce sustainability. Reference Lagunes-Cordoba, Maitra, Dave, Matheiken and Oyebode11
The pipeline becomes most vulnerable at transition points (e.g. core to higher training), where role expectations shift and professional identity is actively renegotiated. Supporting professional identity formation at these stages may mitigate leakage by helping trainees make sense of the demands of psychiatric work through continuity of supervision and role modelling, Reference Varvari, Tribe, Moghaddam and Shiner20 which recognises professional identity as a socially shaped process that can be supported by training environments. RCPsych initiatives such as the Retention Charter and Thrive in Psychiatry reflect this perspective, which explicitly positions retention as a system-level responsibility rather than an individual failing. 8
Recommendations and future directions
The pressurised leaky funnel model shows that current workforce strategies, while successful in generating upstream interest, cannot deliver sustainable capacity unless they explicitly address downstream progression and retention. The model identifies a set of strategic directions for leaders, educators and researchers.
For workforce leaders
The model shows that improved recruitment gains represent a false economy when leakage persists through the middle of the pathway. Shifting metrics from fill rates to progression into consultancy, and investing in stabilising transitions and the middle-grade workforce, may yield greater returns than targeting workforce entry or exit. Organisations can use the retention charter’s self-assessment ratings (foundation, intermediate, mature) as longitudinal quality improvement metrics to identify specific structural leaks. 8 Organisations should regularly review feedback from residents and consultants and iteratively refine the local retention environment to meet workforce needs, including targeted support for induction and career navigation for IMGs. Reference Lagunes-Cordoba, Maitra, Dave, Matheiken and Oyebode11 To address late-stage leakage (Stage 4), organisations can implement flexible job planning for senior psychiatrists and convert potential exits into retained contributions.
For educators
Where applicant volume pressurises the funnel, education can promote informed choice and act as a filter for fit. Realistic job previews and recruitment materials that reflect the emotional and systemic demands of psychiatric practice may reduce application numbers while improving downstream retention. Induction programmes should move beyond logistics and focus on professional identity formation and hidden curriculum to further support alignment. Organisations should measure organisational belonging using validated tools and treat it as a key performance indicator of workforce health. 8 Senior psychiatrists should receive leadership development and formal support in navigating the complexities of modern medical leadership. 8
For researchers
Despite longstanding workforce concerns, the evidence base explaining why psychiatrists leave training and senior roles remains limited and in many areas outdated. Compared with other medical workforce domains, psychiatry has received relatively little sustained empirical investigation, leaving important questions about the mechanisms of attrition insufficiently understood. The model therefore supports a shift from cross-sectional snapshots towards longitudinal workforce research. Given the absence of routine stage-specific attrition reporting, linked national datasets such as the UKMED offer a particularly valuable resource for examining how selection processes, training experiences and responses to workforce interventions shape retention and workforce exit outcomes over time. Reference Silkens, Sarker and Medisauskaite7 Although the current selection mechanism demonstrates good exam predictability, Reference Tiffin, Morley, Paton, Chakraborty and Patterson16 empirical research has yet to establish whether current selection methodologies are associated with long-term workforce outcomes. Reference Challinor and Whyler17
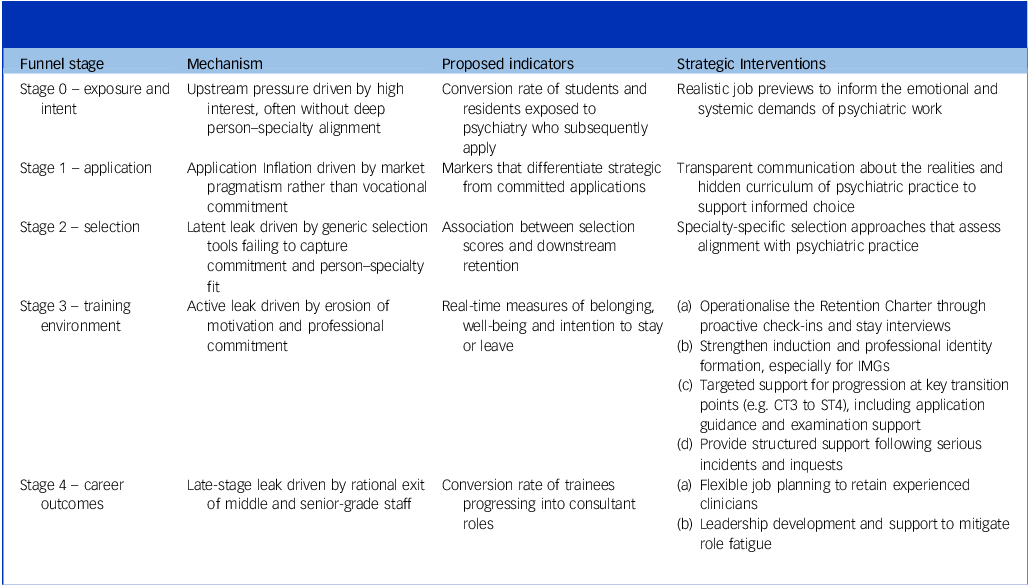
The transition from core to higher specialty training represents the point of greatest attrition, yet the profession still relies heavily on exit interviews to understand this loss. These are inconsistently conducted and offer limited opportunity for early intervention. A strategic shift is therefore needed towards prospective longitudinal research capable of examining how professional identity, working conditions and career expectations evolve over time. Such work could help clarify the mechanisms underlying attrition and inform the development and evaluation of organisational interventions, including approaches such as ‘stay interviews’ designed to identify friction points before a decision to leave is made. 8 Taken together, these gaps highlight the need for a coordinated programme of workforce research in psychiatry, combining primary data collection with implementation and evaluation of organisational interventions to better balance service demands, patient needs and the sustainability of the senior workforce. Table 2 links each stage of the funnel to potential indicators and targeted interventions.
Translating the pressurised leaky funnel into action: proposed indicators and system-level interventions across stages of the workforce pathway

IMG, international medical graduate; CT3, core training year 3; ST4, higher specialty training year 4.
In conclusion, the narrative of the UK psychiatry workforce has shifted from a crisis of recruitment to a paradox of retention, in which high applicant volume coexists with persistent downstream shortages. The pressurised leaky funnel model illustrates how increasing pressure at the point of entry cannot compensate for cumulative losses across training and into senior roles. Addressing this paradox, therefore, requires a shift in how workforce success is understood. By operationalising the RCPsych Retention Charter as a quality improvement framework and refining selection to prioritise person–specialty alignment, organisations can reshape the training pathway. The goal is no longer simply to attract doctors to psychiatry, but to create conditions that enable them to remain, develop and contribute over the long term. Workforce leaders and educators should view retention not as a downstream problem to be fixed late in a career, but the cumulative outcome of how psychiatrists are recruited, trained, supported and valued from day one.
Data availability
Data availability does not apply to this article as no new data were created or analysed.
Acknowledgements
We would like to thank Dr Thomas Scurr from the University of Exeter, and Dr Emily Chruscikowski and Dr Jessica Nicholls-Mindlin from the Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University; Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust; and NIHR Newcastle Biomedical Research Centre (BRC), Newcastle upon Tyne, UK, for their critical review of our article.
Author contributions
J.J.L. conceptualised and wrote the first draft of the manuscript. B.B., A.L., A.D., H.A. and G.V. critically revised the manuscript. All authors approved the final version.
Funding
This work was not supported by any specific funding agency, commercial or not-for-profit organisation.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.