


Background
Wolff–Parkinson–White syndrome has been associated with congenital cardiac abnormalities such as corrected transposition of great arteries Reference Keller and Søorensen1 and Ebstein’s anomaly of tricuspid valveReference Delhaas, Sarvaas and Rijlaarsdam2 and cardiomyopathies including left ventricular non-compaction and hypertrophic cardiomyopathy.Reference Howard, Valdes and Hope3,Reference Perosio, Suarez and Bunster4 Familial clustering of Wolff–Parkinson–White syndrome has also been reported.Reference Vidaillet, Pressley, Henke, Harrell and German5 Despite these well-known associations, direct genetic aetiology is rarely implicated in patients with Wolff–Parkinson–White syndrome.Reference Gollob, Green, Tang and Roberts6 We report a 17-year-old girl with Wolff–Parkinson–White syndrome and left ventricular non-compaction cardiomyopathy due to a rare genetic variant in PR-domain containing protein 16 (PRDM16). The report is supplemented by a comprehensive review of literature.
Case report
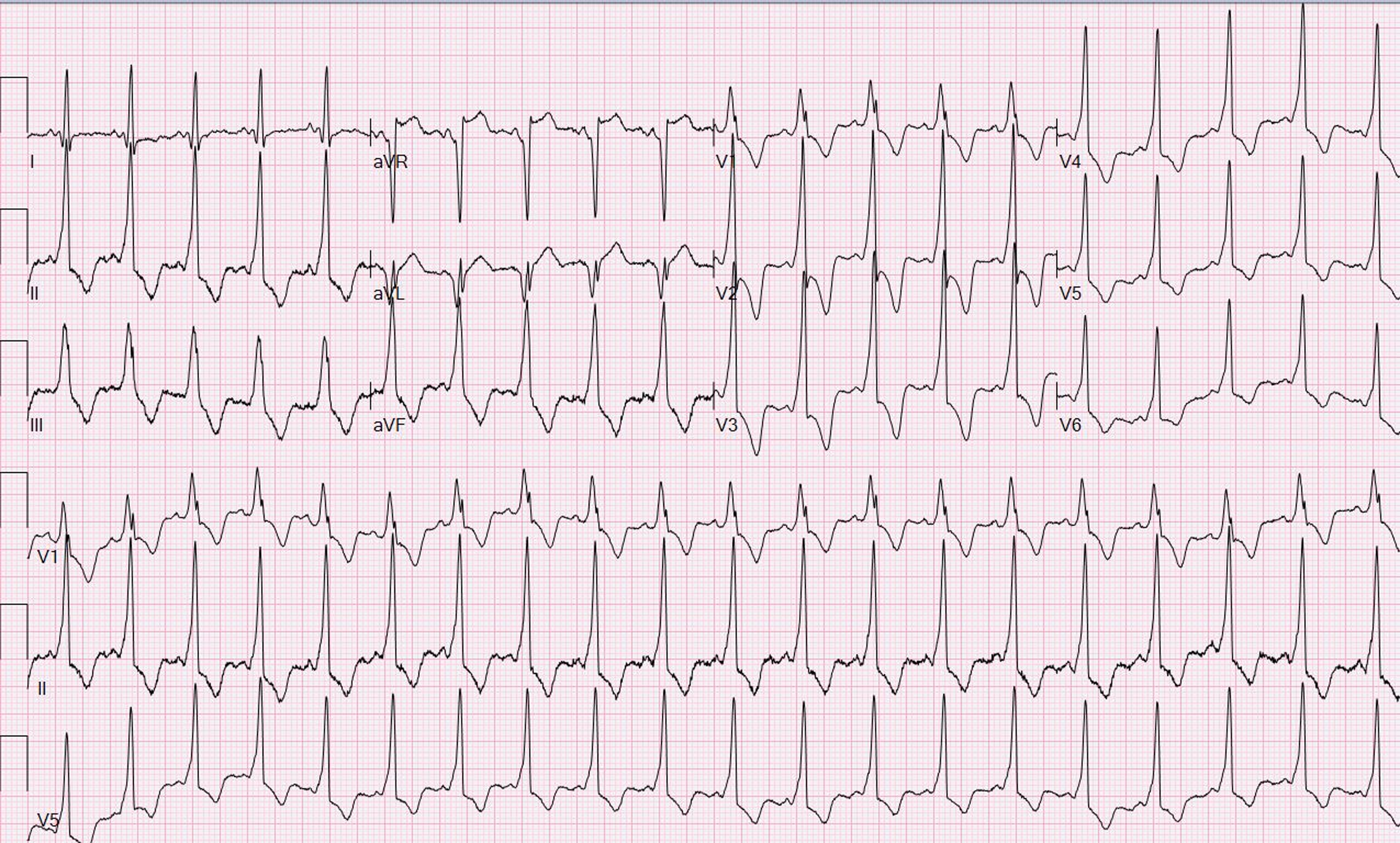
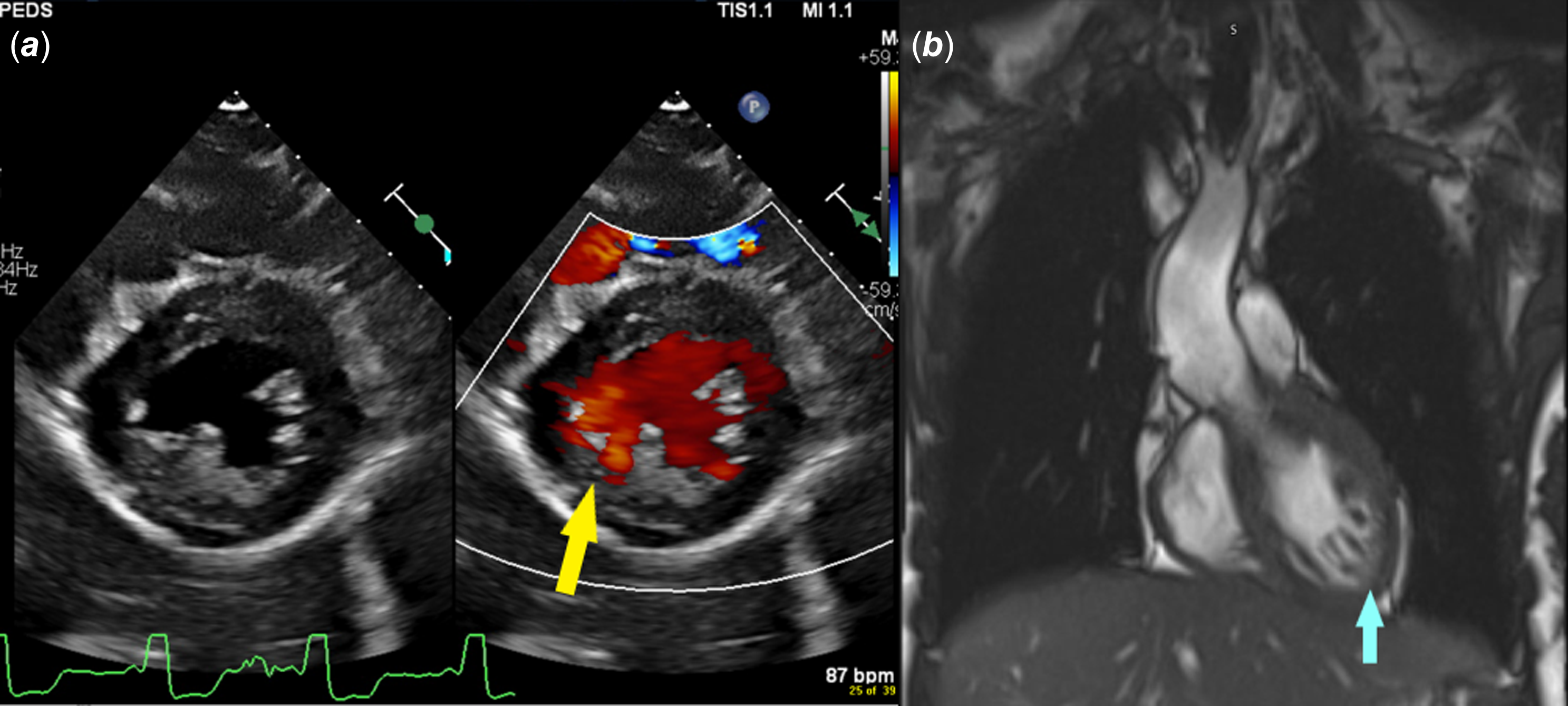
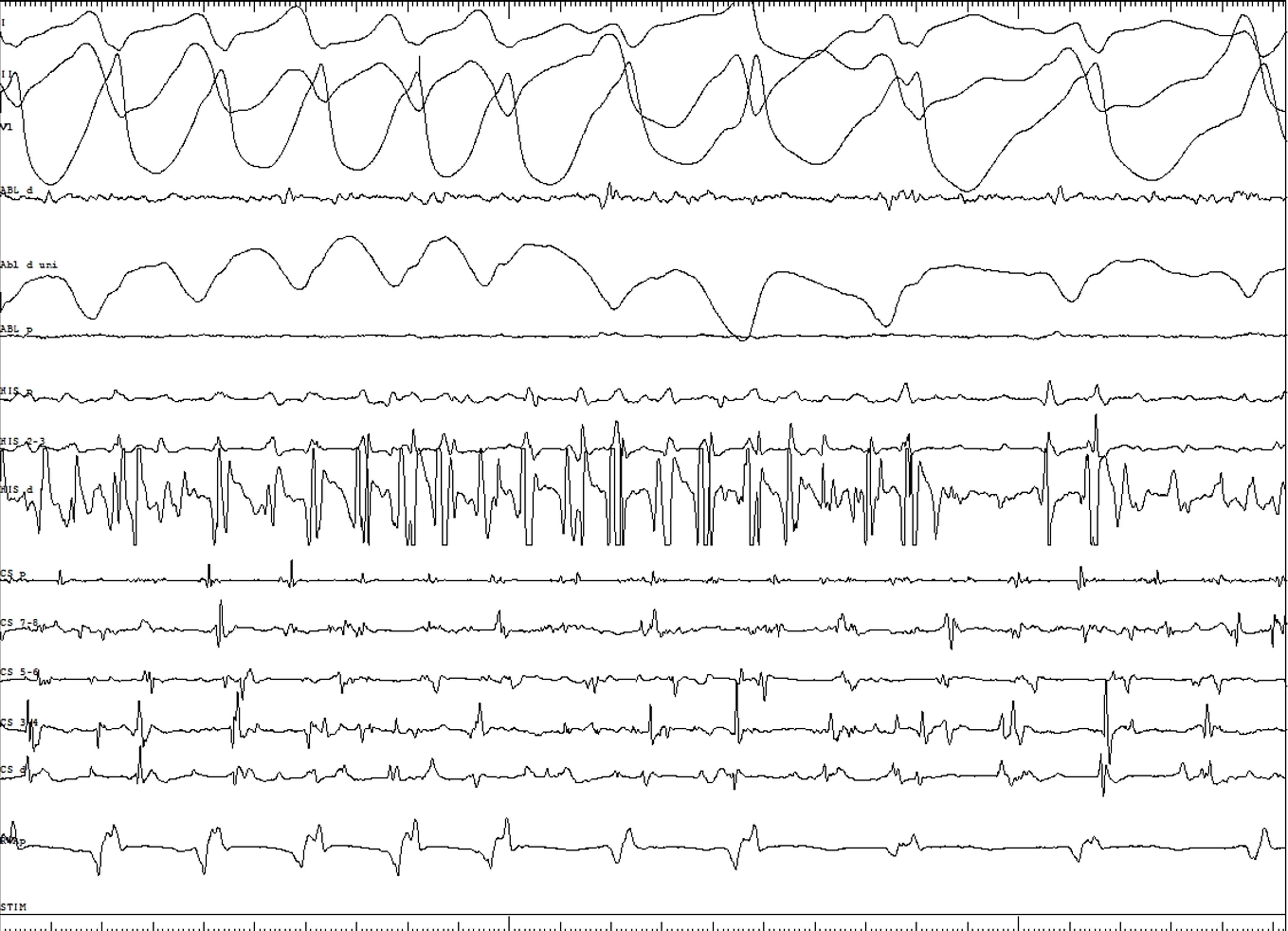
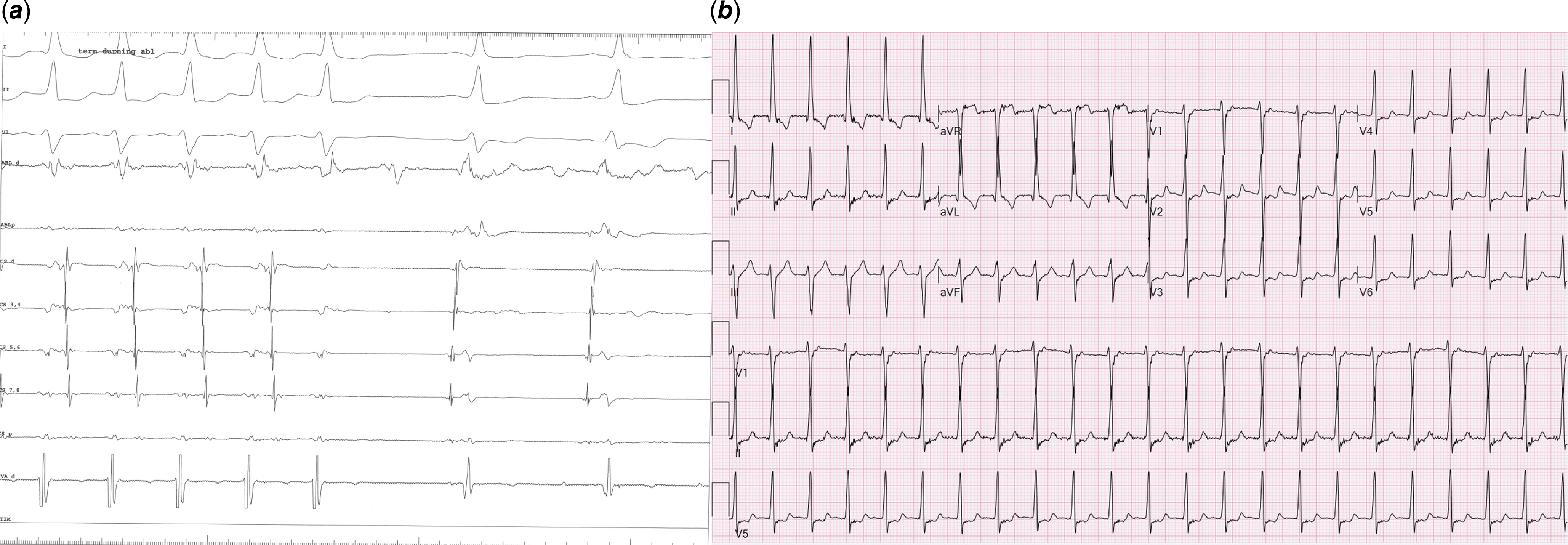
A 17-year-old girl presented with palpitations and Wolff–Parkinson–White pattern on electrocardiogram (Figure 1). Her echocardiogram was suggestive of left ventricular non-compaction with preserved ejection fraction (Figure 2A, Video 1). This was confirmed on cardiac magnetic resonance imaging per criteria proposed by Petersen et al (Figure 2B, Video 2).Reference Petersen, Selvanayagam and Wiesmann7 She underwent an exercise stress test during which pre-excitation persisted at a peak heart rate of 171 beats per minute suggesting a possible high-risk pathway. She subsequently underwent an electrophysiology study during which orthodromic reentrant tachycardia was induced (cycle length of 460 msec) with programmed atrial stimulation. On decremental atrial pacing, the accessory pathway block cycle length was < 200 milliseconds and the shortest preexcited RR interval during atrial fibrillation measured 174 msec (Figure 3), findings which confirmed the pathway to be high risk. The episode of atrial fibrillation resulted in haemodynamic instability and required immediate cardioversion. Mapping was therefore only performed during pre-excited sinus rhythm. Earliest ventricular activation during sinus rhythm was noted over a broad area in mid coronary sinus and superolateral mitral annulus. However, application of radiofrequency energy at these sites was not successful in eliminating pre-excitation (Figure 4). She was started on sotalol until she underwent another EP study a month later. This time, the earliest ventricular activation during sinus rhythm was recorded over a broad area located from 2 to 4 o’clock along the mitral valve annulus. Empiric radiofrequency ablation was performed at the site. Orthodromic reentrant tachycardia was induced following initial ablations (Figure 5A), but no tachycardia could be induced following consolidation of the site. No ventriculoatrial conduction was noted following consolidation. Anterograde accessory pathway conduction, however, persisted, but antegrade pathway block occurred at an atrial pacing cycle length of 450 msec suggesting that the pathway had been modified. Eighteen months following the second ablation, the patient presented to the emergency department in supraventricular tachycardia, which was terminated with adenosine (Figure 5B). She is currently treated with flecainide 75 mg twice daily and is doing well.
12-lead electrocardiogram shows ventricular pre-excitation with left anterior pathway location.
Panel A: parasternal short axis 2D echocardiographic still frame image with colour compare shows left ventricular non-compaction. With colour, flow is noted within crypts. Panel B: the diagnosis is confirmed on a cardiac MRI which shows a ratio of non-compacted mass to total mass of 34 % (> 25% diagnostic of non-compaction).
Shortest preexcited RR interval during atrial fibrillation measures 174 msec suggesting a high-risk pathway.
Broad area of RF ablation along the lateral mitral annulus (Panel A) and coronary sinus (Panel B) failed to eliminate pre-excitation.

Panel a shows loss of retrograde pathway conduction with RF ablation during the second EP study. Panel B shows narrow QRS SVT (orthodromic reentrant tachycardia) 18 months after second ablation which required adenosine for termination.
The family history was negative for arrhythmias or cardiomyopathies. Genetic testing (Invitae arrhythmia and cardiomyopathy panel, San Francisco, CA) revealed a variant of uncertain significance in the PRDM16 (c.2666C > T, p.Pro889Leu). This sequence change replaces proline with leucine at codon 889 of the PRDM16 protein. This missense mutational change has been observed in individuals with Wolff–Parkinson–White syndrome.Reference Coban-Akdemir, Charng and Azamian8 There is also preliminary evidence supporting a correlation with autosomal dominant left ventricular non-compaction (MedGen UID: 349005) and dilated cardiomyopathy (OMIM: 615373). This variant is present in population databases (rs201814961, gnomAD 0.03%). ClinVar also contains an entry for this variant (Variation ID: 487607).
She lives with her adoptive parents and has 5 half-siblings from the same biological mother but different fathers. These siblings have undergone testing and have had negative genetic testing, electrocardiograms, and echocardiograms. She also has a full biological sibling who lives with her biological father. She is, however, not in contact with her biological family, and it is therefore not known whether her full biological sibling and her biological parents have been tested.
Discussion
The prevalence of Wolff–Parkinson–White varies from 3 to 11% in patients with left ventricular non-compaction,Reference Howard, Valdes and Hope3,Reference Tian, Yang and Zhou9,Reference Paszkowska, Mirecka-Rola and Piekutowska-Abramczuk10,Reference Sevinc Sengul, Ergul and Ayyildiz11 which is much higher than the estimated 0.1–0.3% prevalence reported in the general population.Reference Cohen, Triedman and Cannon12 It is hypothesised that primitive AV connections can persist in patients with left ventricular non-compaction due to an arrest in cardiac development, resulting in direct continuity between the atrial and ventricular myocardium across the fibrous annulus.Reference Ichida13 More importantly, in a large cohort of patients with left ventricular non-compaction, 84% of patients with Wolff–Parkinson–White pattern were reported to have cardiac dysfunction compared to 52% of those without Wolff–Parkinson–White pattern suggesting that ventricular pre-excitation could be associated with a risk of cardiac decompensation in patients with left ventricular non-compaction.Reference Howard, Valdes and Hope3
The familial form constitutes approximately 20–40% of all patients with left ventricular non-compaction.Reference Ichida14 The first genetic mutation reported in children with left ventricular non-compaction involved the TAFAZZIN gene in patients with Barth syndrome.Reference Bleyl, Mumford and Thompson15 However, accumulating genetic data indicates that left ventricular non-compaction is genetically heterogeneousReference Finsterer and Stöllberger16 with mutations in MYH7, TTN, and MYBPC3 being the most common.Reference Towbin, Lorts and Jefferies17 Wolff–Parkinson–White syndrome is mostly sporadic with rare reports of genetic associations.Reference Gollob, Green, Tang and Roberts6,Reference Coban-Akdemir, Charng and Azamian8 The gain-of-function mutation in PRKAG2, which encodes the gamma-2 regulatory subunit of adenosine monophosphate activated protein kinase, is most commonly implicated in familial Wolff–Parkinson–White syndrome. Hypertrophic cardiomyopathy is often an associated finding in these patients.Reference Wolf, Arad and Ahmad18 In addition, variants in genes associated with hypertrophic cardiomyopathy such as MYH6 (c.5653G > A; pGlu1885Lys) and MYH7 have also been associated with Wolff–Parkinson–White syndrome.Reference Bowles, Jou and Arrington19,Reference Bobkowski, Sobieszczańska and Turska-Kmieć20
PRDM16 (positive regulatory domain 16) functions as a compact myocardium-enriched transcription factor and is involved in the activation of genes required for compact myocardium growth and in the repression of genes associated with trabeculae formation. In PRDM16 knockout mice, the development of left ventricular non-compaction likely results from a shift in the transcriptional profile of compact cardiomyocytes.Reference Wu, Liang and Zhang21 Consistent with data from PRDM16 knockout mice, PRDM16 mutations have been associated with non-syndromic forms of left ventricular non-compaction in humans.Reference Arndt, Schafer and Drenckhahn22 In particular, truncating variants in PRDM16 have been associated with severe left ventricular non-compaction.Reference Mazzarotto, Hawley and Beltrami23 The frequency of PRDM16 variants in patients with left ventricular non-compaction has been estimated at 0.5 to 4%.Reference Dong, Fan and Tian24,Reference Peña-Peña, Trujillo-Quintero, García-Medina, Cantero-Pérez, De Uña-Iglesias and Monserrat25
Besides association with left ventricular non-compaction, patients with PRDM16 mutation have been noted to have Wolff–Parkinson–White pattern and supraventricular tachycardia.Reference Coban-Akdemir, Charng and Azamian8 The first reported patient was Caucasian who carried a de novo missense mutation [c.2666C > T, p. (Pro889Leu)], which is identical to the mutation carried by our patient. The second reported patient was Hispanic and had an inherited missense mutation [c.2855C > T, p. (Thr952Met)]. He also had atrial septal defect, ventricular septal defect, and hypothyroidism. They both, however, did not have any evidence of cardiomyopathy. There are two other submissions in ClinVar of PRDM16 mutations in patients with Wolff–Parkinson–White syndrome including [c.1642C > A (p.Pro548Thr)] and [c.706G > A (p.Asp236Asn)]. The second patient also had left ventricular non-compaction. Thus, there is accumulating evidence that genetic mutations in PRDM16 can be associated with both Wolff–Parkinson–White syndrome and left ventricular non-compaction. This, however, is the first detailed report where a genetic mutation in PRDM16 resulted in a combined phenotype of both Wolff–Parkinson–White syndrome and left ventricular non-compaction.
Less than 100 patients with Wolff–Parkinson–White and left ventricular non-compaction have been reported till date. Characteristics of these patients with both Wolff–Parkinson–White syndrome and left ventricular non-compaction are summarised in Table 1. It is noteworthy that despite left ventricular non-compaction being left-sided disease, the accessory pathways in patients with left ventricular non-compaction can either be left or right sided. Brescia et al and Paszkowska et al each described a patient each with Wolff–Parkinson–White pattern within their left ventricular non-compaction cohorts, but no accessory pathway was identified on the electrophysiology study suggesting that the patients had pseudo pre-excitation.Reference Paszkowska, Mirecka-Rola and Piekutowska-Abramczuk10,Reference Brescia, Rossano and Pignatelli46 Howard et al reported that 12 out of their cohort of 38 patients with Wolff–Parkinson–White syndrome and left ventricular non-compaction underwent an ablation procedure with a reported acute success rate of 83%. Four patients with cardiac dysfunction were successfully ablated, with 3 showing improvement in cardiac function.Reference Howard, Valdes and Hope3 The authors concluded that the presence of an accessory pathway in left ventricular non-compaction contributed to left ventricular dyssynchrony and eventually systolic dysfunction, which could increase the risk of arrhythmias and sudden cardiac death. They emphasised that ablation could improve left ventricular ejection fraction in these patients, implicating Wolff–Parkinson–White pattern as a bad prognostic indicator in patients with left ventricular non-compaction.Reference Howard, Valdes and Hope3
Characteristics of patients with WPW and LVNC

WPW = Wolff–Parkinson–White; LVNC = Left ventricular non-compaction; M = Male; F = Female; A = Asian, AA = African; C = Caucasian; H = Hispanic; SVT = Supraventricular tachycardia; VE = Ventricular ectopy; NSVT = Non-sustained ventricular tachycardia; VF = Ventricular fibrillation; AF = Atrial fibrillation; EF = Ejection fraction; N = Normal; PHTN = Pulmonary hypertension; CXR = Chest X-ray; VUR = Vesicoureteral reflux; AS = Anteroseptal; APERP = Accessory pathway effective refractory period; ORT = Orthodromic reentrant tachycardia; RF = Radiofrequency; LVH = Left ventricular hypertrophy; HCM = Hypertrophic cardiomyopathy; BAV = Bicuspid aortic valve; LV = Left ventricle; ICD = Implantable cardioverter defibrillator; LHON = Leber’s hereditary optic neuropathy.
Electrophysiologic characteristics of PRDM16-associated accessory pathways have not been well characterised. Our patient had a broad and likely epicardial pathway that could not be completely ablated despite two attempted ablations by experienced operators suggesting that accessory pathway ablation in patients with PRDM16 mutation associated with Wolff–Parkinson–White syndrome, and left ventricular non-compaction may be challenging due to complex pathway characteristics. These findings inform the need for systematic evaluation of association between PRDM16 mutation, left ventricular non-compaction, and Wolff–Parkinson–White pattern.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951124036631.
Data availability statement
The majority of data associated with this study are provided in text and figures. Additional data will be made available upon request.
Financial support
This study was supported by an internal grant from the Department of Pediatrics at West Virginia University.
Competing interests
All authors have reported that they have no relationships relevant to the contents of this paper to disclose.









 Open access
Open access