


Impact statement
This scoping review investigates the potential of stabilizing interventions as an alternative approach to exposure-based therapies for treating trauma-related disorders in refugee populations, a group particularly vulnerable to trauma. By offering a comprehensive review of nonexposure-based interventions, this study provides valuable insights into the current state of research on stabilizing interventions for refugees under different living conditions. The 31 studies included in the review were comprised of over 15 different interventions implemented through various formats. They showed mixed results, but most reported a significant reduction in PTSD symptoms compared to waitlist, treatment as usual or in pre–post analyses. These findings highlight the importance of future research that considers the different living conditions of refugees.
Introduction
By the end of 2023, approximately 117 million individuals worldwide – around 1 % of the global population – were forced to leave their places of residence. This displacement occurred within their country of origin, neighboring countries or countries further away (UNHCR, 2024). As refugees are frequently exposed to traumatic events (Abu Suhaiban et al., Reference Abu Suhaiban, Grasser and Javanbakht2019; Nesterko et al., Reference Nesterko, Jäckle, Friedrich, Holzapfel and Glaesmer2019; Acarturk et al., Reference Acarturk, McGrath, Roberts, Ilkkursun, Cuijpers, Sijbrandij, Sondorp, Ventevogel, McKee and Fuhr2021), they are disproportionately affected by trauma-related disorders compared to the general population, with most studies reporting a prevalence rate of posttraumatic stress disorder (PTSD) exceeding 30% (Kaltenbach et al., Reference Kaltenbach, Schauer, Hermenau, Elbert and Schalinski2018; Blackmore et al., Reference Blackmore, Boyle, Fazel, Ranasinha, Gray, Fitzgerald, Misso and Gibson-Helm2020). PTSD is characterized by re-experiencing through intrusions, flashbacks or nightmares, hyperarousal and avoidance of trauma-related stimuli (World Health Organisation, 2020), which can significantly diminish the quality of life (Monson et al., Reference Monson, Caron, McCloskey and Brunet2017; Lefebvre et al., Reference Lefebvre, Fortin and Guay2021). Moreover, in refugee populations, mental health impairments are closely associated with integration difficulties (Schick et al., Reference Schick, Zumwald, Knöpfli, Nickerson, Bryant, Schnyder, Müller and Morina2016). These reasons call for efficient and timely treatment.
Recent research has demonstrated the efficacy of exposure-based therapy interventions for the treatment of PTSD (McLean et al., Reference McLean, Levy, Miller and Tolin2022). As a result, it is now the standard treatment recommendation in several treatment guidelines (International Society for Traumatic Stress Studies Guidelines Committee, 2018; Hamblen et al., Reference Hamblen, Norman, Sonis, Phelps, Bisson, Nunes, Megnin-Viggars, Forbes, Riggs and Schnurr2019; Schäfer et al., Reference Schäfer, Gast, Hofmann, Knaevelsrud, Lampe, Liebermann, Lotzin, Maercker, Rosner and Wöller2019). A defining characteristic of exposure-based interventions is that patients are confronted with traumatic memories or trauma-related stimuli in a therapeutic manner, with the objective of processing the associated emotions (Rothbaum and Schwartz, Reference Rothbaum and Schwartz2002). However, exposure-based interventions are also associated with a higher dropout rate than other psychotherapeutic interventions, possibly related to the distress resulting from the confrontation with intense negative emotions (Lewis et al., Reference Lewis, Roberts, Andrew, Starling and Bisson2020). Outside of controlled clinical study conditions, various factors on the clinician side, such as concerns about worsening symptoms, or on the patient side, such as comorbidities, also contribute to the infrequent implementation of exposure-based therapies. These factors can lead to the adaptation of manualized interventions to better suit individual cases, rather than being strictly implemented as originally designed (Najavits, Reference Najavits2015). As exposure-based interventions might lead to considerable treatment-associated distress through the reprocessing of traumatic experiences and the accompanying emotions (Foa et al., Reference Foa, Zoellner, Feeny, Hembree and Alvarez-Conrad2002), an adequate level of psychological stability is warranted. Moreover, the stability of the therapeutic relationship – encompassing both continuity of treatment, particularly during exposure to traumatic memories and the reliability of the therapist–patient bond to prevent therapy discontinuation – is essential in order to successfully conduct exposure-based interventions (Gjerstad et al., Reference Gjerstad, Nordin, Poulsen, Spadaro and Palic2024).
The prerequisites for exposure-based interventions are particularly hard to fulfill when treating PTSD in refugee populations, as there are many legal and structural obstacles which must be overcome to provide refugees with healthcare (Giacco et al., Reference Giacco, Matanov and Priebe2014). In general, the development of a stable therapeutic relationship can be impeded by a high degree of mistrust often displayed by individuals who have lived through interpersonal trauma (Hembree et al., Reference Hembree, Rauch and Foa2003; Olatunji et al., Reference Olatunji, Deacon and Abramowitz2009). The language barrier is often identified as a significant challenge in clinical healthcare settings, rendering the establishment of a stable therapeutic relationship more challenging. The lack of interpreters (Bell and Zech, Reference Bell and Zech2009) or inadequate reimbursement policies often impede patients from accessing necessary and adequate treatment of any kind (Helmboldt et al., Reference Helmboldt, Nikendei and Kindermann2019). Access to adequate mental health care often depends on a person’s asylum status (Bell and Zech, Reference Bell and Zech2009). Moreover, the uncertainty regarding legal status and housing, commonly faced by refugees, along with cultural challenges, can threaten psychological stability. This may deter mental health professionals from providing exposure-based interventions, especially when treatment continuity cannot be guaranteed (Bell and Zech, Reference Bell and Zech2009). The systemic challenges of mental health care for refugees apply to all mental disorders and therapeutic approaches. They also have an impact on the implementation and execution of studies, making it challenging to collect data of high quality (Panter-Brick et al., Reference Panter-Brick, Eggerman, Ager, Hadfield and Dajani2020; Hinchey et al., Reference Hinchey, Khalil and Javanbakht2023b). Nevertheless, attempts have been made to assess the efficacy of the exposure-based treatments for refugees and asylum seekers, with promising results (Kaltenbach et al., Reference Kaltenbach, Hermenau, Schauer, Dohrmann, Elbert and Schalinski2020), including narrative exposure therapy (NET) therapy in a refugee camp in Uganda (Neuner et al., Reference Neuner2008) and eye movement desensitization and reprocessing (EMDR) in a refugee camp in Turkey (Acarturk et al., Reference Acarturk, Konuk, Cetinkaya, Senay, Sijbrandij, Cuijpers and Aker2015, Reference Acarturk, Konuk, Cetinkaya, Senay, Sijbrandij, Gulen and Cuijpers2016; Yurtsever et al., Reference Yurtsever, Konuk, Akyüz, Zat, Tükel, Çetinkaya, Savran and Shapiro2018). When examining individual studies, the following aspects should be considered: it is important to note that the improvement in PTSD symptoms among participants of NET therapy (Neuner et al., Reference Neuner2008) was reported at the 1-year follow-up, during which most participants in this group no longer resided in the camp, raising questions about whether the symptom improvement was attributable to the intervention or improved living conditions (Mundt et al., Reference Mundt, Wünsche, Heinz and Pross2014). During the follow-up of a group EMDR therapy, no differences were observed between the intervention and control groups, despite an initial reduction in symptoms in the intervention group. The authors primarily attributed this outcome to the persistently stressful living conditions in the refugee camp (Yurtsever et al., Reference Yurtsever, Konuk, Akyüz, Zat, Tükel, Çetinkaya, Savran and Shapiro2018). In a meta-analysis by Turrini et al., no significant effectiveness was found for NET and EMDR in refugee populations (Turrini et al., Reference Turrini, Purgato, Acarturk, Anttila, Au, Ballette, Bird, Carswell, Churchill and Cuijpers2019). This finding contrasts with the results of a meta-analysis conducted by Nosè et al., which specifically investigated psychological interventions for refugees in high-income countries and demonstrated the effectiveness of NET in this setting (Nosè et al., Reference Nosè, Ballette, Bighelli, Turrini, Purgato, Tol, Priebe and Barbui2017). Nonetheless, it should be noted at this point that a meta-analysis by Turrini et al. also identified trauma-focused cognitive behavioral therapy (CBT) as an effective intervention, with sustained effects at follow-up despite the presence of postmigratory stressors (Turrini et al., Reference Turrini, Purgato, Acarturk, Anttila, Au, Ballette, Bird, Carswell, Churchill and Cuijpers2019). While trauma exposure-based interventions have shown effectiveness, albeit with variable levels of evidence, alternative treatment approaches for situations in which the prerequisites for exposure-based interventions are not met could represent a valuable addition to improving the mental health of refugee populations.
Stabilizing interventions, which are commonly well-established in clinical settings (Rosner et al., Reference Rosner, Henkel, Ginkel and Mestel2015; Equit et al., Reference Equit, Maurer, Michael and Köllner2018), represent an alternative treatment approach. They can reduce trauma-related symptoms but can also serve as a preparation for exposure-based interventions as part of a phase-based approach (Willis et al., Reference Willis, Dowling and O’Reilly2023). They are designed to assist trauma survivors in managing trauma-related symptoms without using maladaptive regulation strategies. In psycho-traumatology, the term “stable” is commonly used to describe a person who is capable of coping with trauma-related stimuli, emotions and memories, without risk of serious deterioration in their general physical and mental well-being. This encompasses the absence of behaviors such as self-harm, suicidal ideation, substance abuse and dissociative episodes (Reddemann, Reference Reddemann2011). In this context, stability mainly refers to a trauma survivor’s inner stability (e.g., coping with symptoms) but also includes external aspects and risk assessments, such as social stability (social support system and network), physical and psychological safety (perpetrator contact, living conditions) and the nature of the patient–therapist relationship (Sack and Gromes, Reference Sack and Gromes2013; Seidler et al., Reference Seidler, Freyberger and Maercker2015). While many definitions of stabilization interventions exist, our review uses the definition proposed by Luise Reddemann, as it aligns with the current clinical understanding of stabilization in treating trauma-related disorders. According to Reddemann, stabilization interventions aim to enhance symptom management, emotion regulation and the acquisition of new competencies (Reddemann, Reference Reddemann2011; Reddemann and Piedfort-Marin, Reference Reddemann and Piedfort-Marin2017). This is achieved through regaining a sense of control (Herman, Reference Herman1992), interpersonal safety (Willis et al., Reference Willis, Dowling and O’Reilly2023) and strengthening socio-psychological skills (Ter Heide et al., Reference Ter Heide, Mooren, van de, de and Kleber2016). Stabilization techniques do not make use of traumatic memories. Thus, psychological stability, treatment continuity and the development of a stable therapeutic relationship are of lesser importance than exposure-based therapy.
The necessity of stabilization interventions is a topic of critical debate. Concerns have been raised that stabilization interventions might delay the implementation of evidence-based exposure-based interventions (Neuner et al., Reference Neuner2008; De Jongh et al., Reference De Jongh, Resick, Zoellner, Van Minnen, Lee, Monson, Foa, Wheeler, Broeke and Feeny2016). While many treatment manuals for exposure-based interventions, such as EMDR, incorporate stabilization elements (Foa et al., Reference Foa, Chrestman and Gilboa-Schechtman2008; Shapiro, Reference Shapiro2017), usually evaluations assess the therapy manual as a whole (Rosner et al., Reference Rosner, Henkel, Ginkel and Mestel2015). Therefore, the specific impact of the stabilization elements cannot be determined independently from the overall treatment effect and systematic evidence for the efficacy of stabilizing interventions is lacking (National Institute for Health and Care Excellence, 2018; Berliner et al., Reference Berliner, Bisson, Cloitre, Forbes, Jensen, Lewis, Monson, Olff, Pilling and Riggs2019). Thus, the aim of this scoping review is to provide an overview of the current research on stabilizing, nonexposure-based interventions for refugees with trauma-related disorders through a systematic search of the literature. In light of the expansive scope of this definition, the review will initially present the interventions conducted in the included studies, followed by an analysis of the study designs, including participants and outcomes.
Methods
Search strategy
As this was the first review on stabilizing interventions in refugee populations and considering the large variety of implementations of stabilizing interventions, we decided to conduct a scoping review of the literature. Herein, we adhered to the guidelines laid out by the PRISMA-ScR checklist (Tricco et al., Reference Tricco, Lillie, Zarin, O’Brien, Colquhoun, Levac, Moher, Peters, Horsley and Weeks2018). We conducted a systematic search to identify studies that examine stabilizing interventions and evaluate their effect on the symptom burden of PTSD in adult refugees. With regard to the criterion of whether a study examines a stabilizing approach, we have used the above-mentioned definition by Luise Reddemann (Reference Reddemann2011) as a guideline. The final decision as to whether an intervention was “stabilizing” was the subject of discussion among the reviewers. The screening process was conducted by three independent reviewers (IR, NG, JN). The search was conducted on PubMed, Embase, Web of Science, PsycInfo and CINAHL.
Inclusion criteria
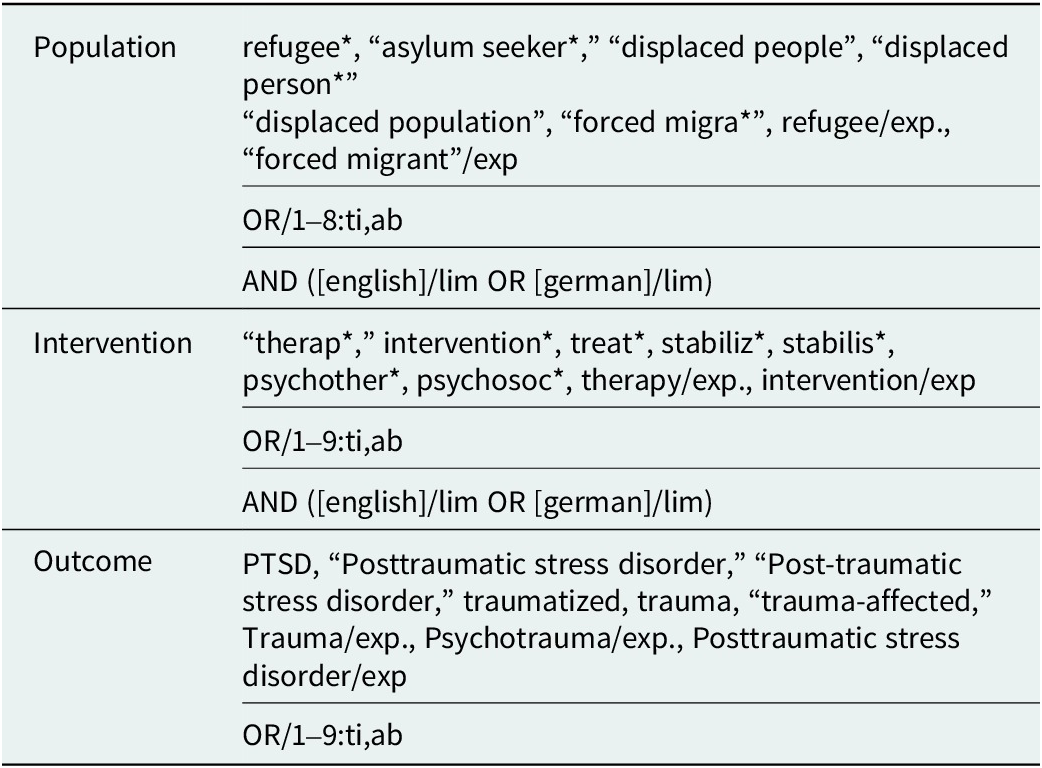
Studies were included if the sample was comprised of refugees or forced migrants worldwide at all stages of flight, i.e. internally displaced persons, people in refugee camps or the postmigration phase at various stages of the asylum process. We included intervention studies, such as randomized controlled trials, as well as single interventions from all regions of the world. The respective interventions could be performed by professionals or lay providers. Individual and group interventions were included. Further, we included studies that evaluated the effect of stabilizing interventions on reducing PTSD symptom load, with PTSD as either the primary or secondary outcome. Initially, we planned to include only studies focusing on adult refugees ≥18 years. However, some projects targeted communities, families or “youth,” with some individuals being under 18 years. Therefore, we adjusted our criteria to include studies in which the majority of participants were adult refugees. Exclusion criteria were other types of publications such as abstracts, conference papers or dissertations, single case studies, systematic reviews and meta-analyses, studies conducted among only underage refugees or qualitative studies. In addition, we excluded studies that did not provide sufficient details about stabilizing interventions, multimodal interventions and interventions that included trauma exposure elements. No date restriction was placed on this search. Only papers in English or German language were included. Additionally, we conducted a forward reference search to identify further publications on the topic. Search terms related to the population were: refugees OR asylum seekers OR forced migration OR displaced people. Search terms related to the outcome were PTSD or posttraumatic stress disorder OR trauma OR traumatized. Search terms related to therapy were therapy OR intervention OR treatment OR psychotherapy OR stabilization. The full search strategy for EMBASE can be found in Table 1. The protocol of this scoping review can be assessed at OSF (https://osf.io/z3dcy).
Key search terms for EMBASE

Note: Date of search: 10.11.2023.
Data extraction and management
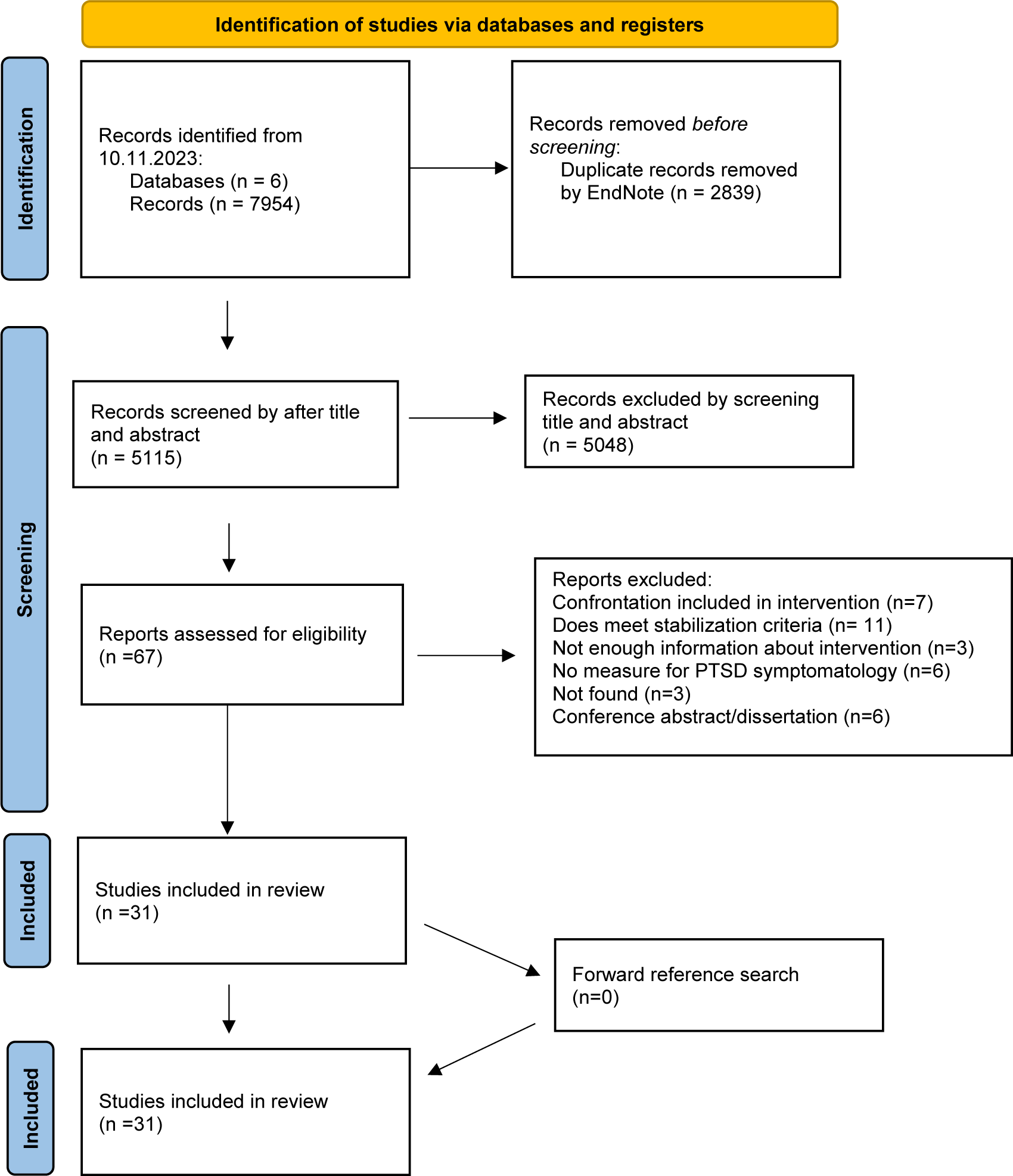
For each included study, information on author and year of publication, study design, country of study conduction, study population, sample size and gender distribution, inclusion criteria, information on the stabilizing intervention, PTSD outcome measure and PTSD symptom outcome was collected by the reviewers on a data collection form. The full screening process is displayed in Figure 1.
PRISMA 2020 flow diagram.

Risk of bias assessment
For each included study, we also conducted a risk of bias evaluation. For this purpose, we utilized the Cochrane evaluation tools, specifically the revised RoB 2 tool for randomized controlled trials (Sterne et al., Reference Sterne, Savović, Page, Elbers, Blencowe, Boutron, Cates, Cheng, Corbett and Eldridge2019) and the ROBINS-I tool for nonrandomized studies (Sterne et al., Reference Sterne, Hernán, Reeves, Savović, Berkman, Viswanathan, Henry, Altman, Ansari and Boutron2016).
Results
Study selection and procedure
We indentified a total of 5,115 studies after automated removal of duplicats (see Figure 1). Following the screening of titles and abstracts, 5,048 results were excluded. The full text was assessed for eligibility for 67 studies. A total of seven studies were excluded because the intervention included exposure-based elements. Another 11 studies were excluded because the specifications in the study design did not meet the definition of stabilization (Kruse et al., Reference Kruse, Joksimovic, Cavka, Wöller and Schmitz2009; Renner et al., Reference Renner, Bänninger-Huber and Peltzer2011; Jespersen and Vuust, Reference Jespersen and Vuust2012; Ter Heide and Smid, Reference Ter Heide and Smid2015; Stammel et al., Reference Stammel, Knaevelsrud, Schock, Walther, Wenk-Ansohn and Böttche2017; Yurtsever et al., Reference Yurtsever, Konuk, Akyüz, Zat, Tükel, Çetinkaya, Savran and Shapiro2018; Shultz et al., Reference Shultz, Verdeli, Ceballos, Hernandez, Espinel, Helpman, Neria and Araya2019; Trilesnik et al., Reference Trilesnik, Altunoz, Wesolowski, Eckhoff, Ozkan, Loos, Penteker and Graef-Calliess2019; Park et al., Reference Park, Park, Elbert and Kim2020; Gever et al., Reference Gever, Iyendo, Obiugo-Muoh, Okunade, Agujiobi-Odoh, Udengwu, Talabi and Nwokolo2023; Graef-Calliess et al., Reference Graef-Calliess, Erdmann, Mohwinkel, Özkan, Finkelstein, Loos, Penteker and Trilesnik2023). Three studies were excluded because the available information about the examined intervention was insufficient (Neuner et al., Reference Neuner, Kurreck, Ruf, Odenwald, Elbert and Schauer2010; Rees et al., Reference Rees, Travis, Shapiro and Chant2013, Reference Rees, Travis, Shapiro and Chant2014). With regard to the intervention, six studies lacked any measure of PTSD symptomatology (Renner et al., Reference Renner, Lind and Ottomeyer2008; Sonne et al., Reference Sonne, Carlsson, Bech, Vindbjerg, Mortensen and Elklit2016, Reference Sonne, Mortensen, Silove, Palic and Carlsson2021; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Aizik-Reebs et al., Reference Aizik-Reebs, Amir, Yuval, Hadash and Bernstein2022; Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022). Three studies could not be found (Renner and Peltzer, Reference Renner and Peltzer2008; Kayal et al., Reference Kayal, Gratton, Blumberg and Walsh2013; Sonne et al., Reference Sonne, Mortensen, Palic and Carlsson2019), and six were conference abstracts or nonpeer-reviewed dissertations (Mojica-Castillo, Reference Mojica-Castillo2003; Stenmark et al., Reference Stenmark, Catani, Elbert and Gotestam2008; Ekstrøm et al., Reference Ekstrøm, Carlsson, Sonne and Mortensen2016; Bryant, Reference Bryant2022; De Graaff et al., Reference De Graaff, Sijbrandij and Cuijpers2022; Stöckli et al., Reference Stöckli, Zöllner, Burchert, Haji, Hosmann, Aebersold, Wabiszczewicz, Heim, Knaevelsrud and Berger2023). A total of 31 studies were included in our final analysis. An overview of the included studies can be found in Table 2. The 31 studies included a total of 2,759 participants (1,192 male, 1,269 female, 298 not known) receiving a stabilizing intervention. An overview of the included interventions can be found in Table 2.
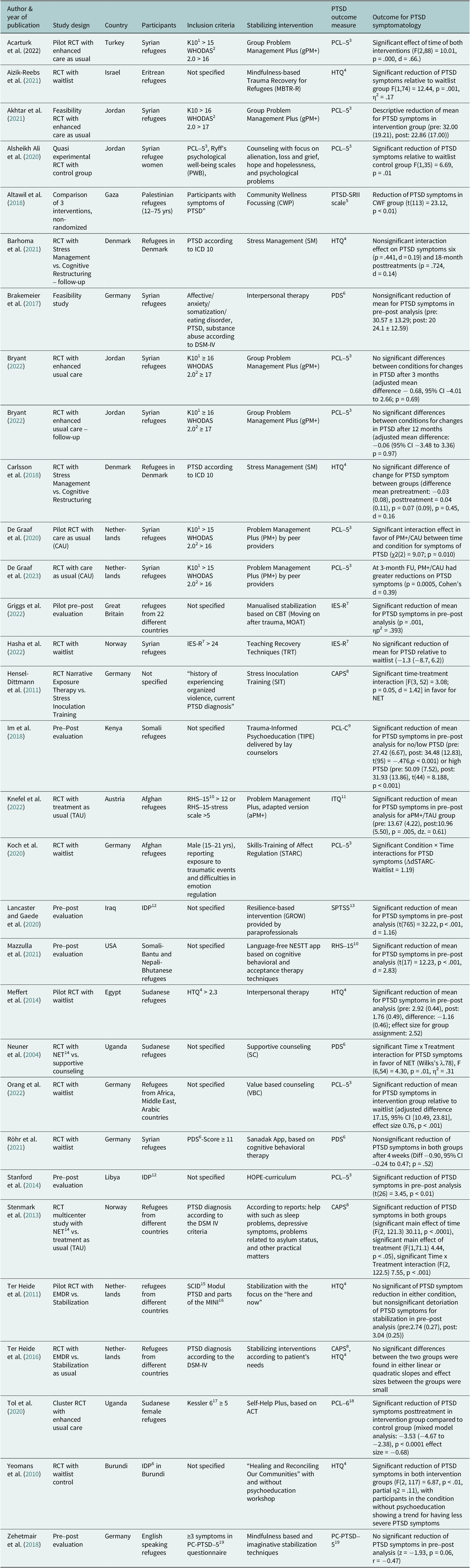
Overview of included studies

Note: ALTAWIL, M., NEL, P., ASKER, A., SAMARA, M. & HARROLD, D. 2008. The effects of chronic war trauma among Palestinian children. Children: The invisible victims of war-An interdisciplinary study: Peterborough: DSM Technical Publications Ltd. 1K10: Kesseler Distress Scale, 10 items,2WHODAS=World Health Organization Disability Assessment Schedule,3PCL-5: Posttraumatic Stress Disorder Checklist, 4HTQ: Harvard Trauma Questionnaire, 5PTSD-SRII Scale: see Altawil et al. (2008), 6PDS: Posttraumatic Diagnostic Scale, 7IES-R: Impact of Event Scale-Revised, 8CAPS: Clinician Administered Scale, 9PCL-C: PTSD Checklist – civilian version, 10RHS-15: Refugee Health Screener-15, 11ITQ: International Trauma Questionnaire, 12IDP: Internally displaced person, 13SPTSS: Screen for Posttraumatic Stress Symptoms, 14NET: Narrative Exposure Therapy, 15SCID: structured clinical interview, for DSM-IV Axis I Disorders (SCID-I), Modul PTSD, 16MINI: Mini International Neuropsychiatric Interview, 17Kessler 6: Kessler Distress Scale, 6 items, 18PCL-6: PTSD Checklist – 6 items version, 19PC-PTSD-5: Primary-Care PTSD-5.
Examined stabilizing interventions
The 31 studies analyzed presented a variety of stabilizing treatment approaches. A total of 15 interventions were conducted in a group format (Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010; Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014; Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018; Zehetmair et al., Reference Zehetmair, Kaufmann, Tegeler, Kindermann, Junne, Zipfel, Herpertz, Herzog and Nikendei2018; Alsheikh Ali, Reference Alsheikh Ali2020; Koch et al., Reference Koch, Ehring and Liedl2020; Lancaster and Gaede, Reference Lancaster and Gaede2020; Tol et al., Reference Tol, Leku, Lakin, Carswell, Augustinavicius, Adaku, Au, Brown, Bryant and Garcia-Moreno2020; Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021; Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al. Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a,Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb; Griggs et al., Reference Griggs, Liu and Cooper2022; Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022), 14 in individual sessions (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004; Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011; Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011; Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013; Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Ter Heide et al., Reference Ter Heide, Mooren, van de, de and Kleber2016; Brakemeier et al., Reference Brakemeier, Zimmermann, Erz, Bollmann, Rump, von Kempski, Grossmüller, Mitelman, Gehrisch and Spies2017; Altawil et al., Reference Altawil, El Asam and Khadaroo2018; Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020; Barhoma et al., Reference Barhoma, Sonne, Lommen, Mortensen and Carlsson2021; Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022; Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022; De et al., Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023) and two as smartphone-based interventions (Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021; Röhr et al., Reference Röhr, Jung, Pabst, Grochtdreis, Dams, Nagl, Renner, Hoffmann, König and Kersting2021).
Seven studies explored the effectiveness of Problem Management Plus (PM+), a transdiagnostic intervention developed by the World Health Organization (WHO) that addresses common mental health issues. PM+ offers strategies to manage stress and addresses problems through different techniques such as relaxation, problem-solving, behavioral activation and enhancing social support (Dawson et al., Reference Dawson, Bryant, Harper, Kuowei Tay, Rahman, Schafer and van Ommeren2015). This intervention modality has been conducted by both professional (Kantor et al., Reference Kantor, Knefel and Lueger-Schuster2017) and peer providers (De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020, Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023), in individual and group formats (Bryant et al. Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a,Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb) and across diverse living conditions (Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022).
Three studies explored the efficacy of mindfulness-based interventions. These included, for instance, mindfulness-based stress reduction for refugees (MBSR-R) (Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021) and mindfulness-related and imaginative stabilization techniques that incorporated exercises such as guided imagery. The effectiveness of Acceptance and Commitment Therapy (ACT) (Tol et al., Reference Tol, Leku, Lakin, Carswell, Augustinavicius, Adaku, Au, Brown, Bryant and Garcia-Moreno2020), which integrates elements of mindfulness strategies with CBT, was also evaluated (Self-Help Plus) (Hayes and Pierson, Reference Hayes, Pierson, Freeman, Felgoise, Nezu, Nezu and Reinecke2005).
Furthermore, three studies examined stress management (SM) as an intervention approach (Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; Barhoma et al., Reference Barhoma, Sonne, Lommen, Mortensen and Carlsson2021). SM or stress inoculation training (SIT) (Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011), both encompass relaxation techniques, attention diversion and behavioral activation. The underlying assumption is that inadequate coping strategies may precipitate pathological stress (Lazarus and Folkman, Reference Lazarus and Folkman1984).
A similar approach was followed by three CBT-based interventions, which specifically addressed the symptom clusters of PTSD rather than general distress (Moving on after trauma, MOAT; teaching recovery techniques (TRT); HOPE-curriculum) (Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014; Griggs et al., Reference Griggs, Liu and Cooper2022; Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022).
Two studies investigated interpersonal therapy as an intervention (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Brakemeier et al., Reference Brakemeier, Zimmermann, Erz, Bollmann, Rump, von Kempski, Grossmüller, Mitelman, Gehrisch and Spies2017). Interpersonal therapy addresses interpersonal problems as significant contributing factors to the developement and progression of mental health impairments, including grief, role transitions, role disputes and interpersonal deficiencies such as social isolation (Lipsitz and Markowitz, Reference Lipsitz and Markowitz2013). The authors of the respective publications examined this therapeutic approach in more detail, arguing that both traumatic experiences, especially those of an interpersonal nature and forced displacement adversely affect interpersonal relationships and can perpetuate negative cycles (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014).
Additionally, we included two smartphone-based interventions (Sanadak app; NESTT app) (Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021; Röhr et al., Reference Röhr, Jung, Pabst, Grochtdreis, Dams, Nagl, Renner, Hoffmann, König and Kersting2021). Both were based on a CBT approach, with one being language-free and incorporating ACT techniques (Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021).
One study explored a transdiagnostic approach to improve emotion regulation skills (Skills-Training of Affect Regulation (STARC)) (Koch et al., Reference Koch, Ehring and Liedl2020). The training has been culturally adapted to the needs of Afghan refugees based on the model of Dialectic Behavioral Therapy (DBT) (Linehan, Reference Linehan2014) and Skills Training in Affective and Interpersonal Regulation (STAIR) (Cloitre et al., Reference Cloitre, Stovall-McClough, Nooner, Zorbas, Cherry, Jackson, Gan and Petkova2010).
The remaining 11 studies examined additional approaches to stabilization, including the evaluation of different kinds of counseling. These included value-based counseling (VBC) (Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022) and counseling that emphasizes grieving and loss, hope and hopelessness and alienation (Alsheikh Ali, Reference Alsheikh Ali2020). Other interventions focused on increasing resilience and dealing with feelings of helplessness (Community Wellness Focussing (CWP)) (Altawil et al., Reference Altawil, El Asam and Khadaroo2018), or on fostering an individual’s religiousness, thankfulness, kindness, hope and courage (GROW) (Lancaster and Gaede, Reference Lancaster and Gaede2020).
Two studies investigated a manual that, in addition to psychoeducation and regulation strategies, also addresses the topics of stigma, migration stress, collective trauma (Trauma-Informed Psychoeducation, TIPE) (Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018) and, respectively, the healing of interpersonal relationships (Healing and Reconciling Our Communities) (Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010).
Finally, three studies employed stabilization (Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011, Reference Ter Heide, Mooren, van de, de and Kleber2016), counseling (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004) or treatment as usual as a control condition, focusing on “sleep problems, depressive symptoms, problems related to asylum status and other practical matters” (Stenmark et al., Reference Stenmark, Catani, Elbert and Gotestam2008). One of the studies focused on enhancing physical safety and well-being as well as the implementation of body-oriented interventions to ease PTSD-related symptoms (Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011). The second study focused on the enhancement of emotional regulation and the development of relational skills (Ter Heide et al., Reference Ter Heide, Mooren, van de, de and Kleber2016). The third study employed a nonstructured counseling intervention, tailored to the patients needs with the aim of controlling for non-specific treatment effects (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004).
Study designs
Different study designs were used to assess the effects of the interventions reviewed. Of the 31 studies, 23 were RCTs (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004; Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010; Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011; Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011, Reference Ter Heide, Mooren, van de, de and Kleber2016; Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013; Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; Alsheikh Ali, Reference Alsheikh Ali2020; De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020, Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023; Koch et al., Reference Koch, Ehring and Liedl2020; Tol et al., Reference Tol, Leku, Lakin, Carswell, Augustinavicius, Adaku, Au, Brown, Bryant and Garcia-Moreno2020; Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021; Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Barhoma et al., Reference Barhoma, Sonne, Lommen, Mortensen and Carlsson2021; Röhr et al., Reference Röhr, Jung, Pabst, Grochtdreis, Dams, Nagl, Renner, Hoffmann, König and Kersting2021; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al., Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a, Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb; Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022; Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022; Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022), of which four were pilot evaluations (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020; Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022). Eight studies compared the intervention with a wait-list control (Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010; Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Alsheikh Ali, Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2020; Koch et al., Reference Koch, Ehring and Liedl2020; Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021; Röhr et al., Reference Röhr, Jung, Pabst, Grochtdreis, Dams, Nagl, Renner, Hoffmann, König and Kersting2021; Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022; Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022), eight further studies had an active control group, mostly compared with treatment as usual (De Graaff et al. Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020, Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023; Tol et al., Reference Tol, Leku, Lakin, Carswell, Augustinavicius, Adaku, Au, Brown, Bryant and Garcia-Moreno2020; Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Knefel et al. Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al. Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a, Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb). Four studies used a stabilizing intervention as an active control group for NET (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004; Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013) or EMDR (Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011, Reference Ter Heide, Mooren, van de, de and Kleber2016). Three studies compared two different interventions, one of which can be classified as stabilizing (Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011;Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; Barhoma et al., Reference Barhoma, Sonne, Lommen, Mortensen and Carlsson2021). The remaining eight studies were conducted as a pre–post analysis (Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014; Brakemeier et al., Reference Brakemeier, Zimmermann, Erz, Bollmann, Rump, von Kempski, Grossmüller, Mitelman, Gehrisch and Spies2017; Altawil et al., Reference Altawil, El Asam and Khadaroo2018; Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018; Zehetmair et al., Reference Zehetmair, Kaufmann, Tegeler, Kindermann, Junne, Zipfel, Herpertz, Herzog and Nikendei2018; Lancaster and Gaede, Reference Lancaster and Gaede2020; Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021; Griggs et al., Reference Griggs, Liu and Cooper2022), with one study comparing three interventions and assigning participants according to need rather than randomly (Altawil et al., Reference Altawil, El Asam and Khadaroo2018).
Participant mental health burden
Inclusion criteria differed between studies in terms of the mental health burden of the study populations: 12 of the studies included refugees with a formal diagnosis of PTSD, assessed with questionnaires such as the HTQ, PDS, IES-R, PC-PTSD-5 (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Zehetmair et al., Reference Zehetmair, Kaufmann, Tegeler, Kindermann, Junne, Zipfel, Herpertz, Herzog and Nikendei2018; Alsheikh Ali, Reference Alsheikh Ali2020; Röhr et al., Reference Röhr, Jung, Pabst, Grochtdreis, Dams, Nagl, Renner, Hoffmann, König and Kersting2021; Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022) or described as according to ICD-10 or DSM-IV/V criteria (Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011, Reference Ter Heide, Mooren, van de, de and Kleber2016; Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013; Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; Barhoma et al., Reference Barhoma, Sonne, Lommen, Mortensen and Carlsson2021), or only “with PTSD” without displaying the diagnostic process or tools (Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011; Altawil et al., Reference Altawil, El Asam and Khadaroo2018), or reporting exposure to traumatic events (Koch et al., Reference Koch, Ehring and Liedl2020). One study included refugees if they met DSM-IV criteria for PTSD, affective, anxiety, somatization, eating disorders or substance abuse (Brakemeier et al., Reference Brakemeier, Zimmermann, Erz, Bollmann, Rump, von Kempski, Grossmüller, Mitelman, Gehrisch and Spies2017). In seven other studies, refugees were included if they showed a general level of psychological distress (De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020, Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023; Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al. Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a, Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb; Knefel et al. Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022), as measured with the Kessler Distress Scale, Kessler 6, WHO Disability Assessment Schedule 2.0 (WHODAS 2.0) or Refugee Health Screener 15 (RHS-15). Nine studies did not specify their inclusion criteria (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004; Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010; Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014; Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018; Lancaster and Gaede, Reference Lancaster and Gaede2020; Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021; Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021; Griggs et al., Reference Griggs, Liu and Cooper2022; Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022). One study (Altawil et al., Reference Altawil, El Asam and Khadaroo2018) compared three interventions aimed at individuals and communities who had been exposed to severely traumatizing experiences.
Outcome
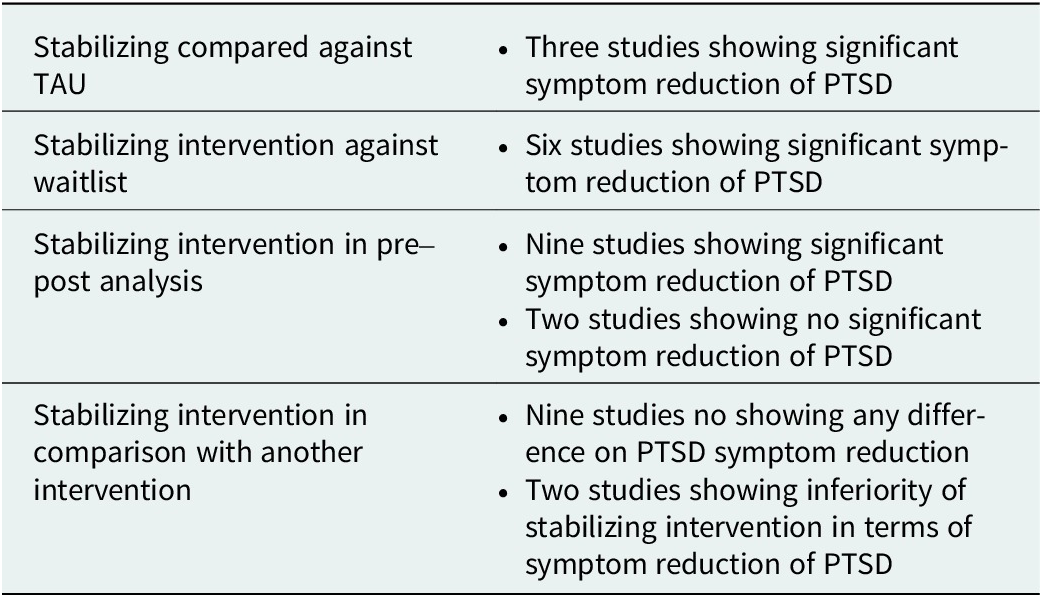
The studies reported varying outcomes for the investigated treatment approaches (see Table 3). Nine studies showed significant reductions in PTSD symptoms for participants in the stabilizing intervention group: compared with treatment as usual, Self-Help Plus, PM+ and Mindfulness-based Trauma Recovery for Refugees (De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020, Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023; Tol et al., Reference Tol, Leku, Lakin, Carswell, Augustinavicius, Adaku, Au, Brown, Bryant and Garcia-Moreno2020) showed positive outcomes. Compared with a waitlist control group, counseling that emphasizes grieving and loss, hope and hopelessness and alienation, TRTs, Skills-Training of Affect Regulation, Healing and Reconciling Our Communities and VBC (Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010; Alsheikh Ali, Reference Alsheikh Ali2020; Koch et al., Reference Koch, Ehring and Liedl2020; Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021; Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022; Orang et al., Reference Orang, Missmahl, Thoele, Valensise, Brenner, Gardisi, Peter and Kluge2022), showed favorable outcomes in six interventions. Eight studies found significant reductions in PTSD symptoms in pre–post analyses of CBT-based stabilization (MOAT), trauma-informed psychoeducation (TIPE), resilience-based intervention (GROW), peer-lead recovery group, community wellness focusing, an adapted version of PM+, interpersonal therapy or a CBT- and ACT-based (NESTT) (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014; Altawil et al., Reference Altawil, El Asam and Khadaroo2018; Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018; Lancaster and Gaede, Reference Lancaster and Gaede2020; Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021; Griggs et al., Reference Griggs, Liu and Cooper2022; Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022). One study using gPM+ reported a reduction in mean PTSD symptom scores without testing for statistical significance (Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021).
Summary of the results

Nine studies found no difference in the efficacy of a stabilizing approach in reducing PTSD symptoms: compared with treatment as usual, PM+, gPM+ did not show a better outcome (C Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al. Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a, Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb). When a stabilizing approach was the control condition (TAU: support with accompanying problems and practical matters), there was a significant symptom reduction in both groups compared with NET, with NET showing a greater reduction (Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013). The use of a CBT-based self-help app (Sanadak) compared with waitlist did not show significant differences in PTSD symptom reduction (Röhr et al., Reference Röhr, Jung, Pabst, Grochtdreis, Dams, Nagl, Renner, Hoffmann, König and Kersting2021). SM compared with cognitive restructuring also showed no significant differences in outcome, with both approaches showing nonsignificant symptom reductions (Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; Barhoma et al., Reference Barhoma, Sonne, Lommen, Mortensen and Carlsson2021). When EMDR was compared with stabilization” with the focus on the here and now” or “according to the patients needs,” no significant differences between the two groups were described (Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011, Reference Ter Heide, Mooren, van de, de and Kleber2016), with one study reporting a nonsignificant deterioration of PTSD symptomatology for the stabilization group (Ter Heide et al., Reference Ter Heide, Mooren, Kleijn, de and Kleber2011). The stabilizing approach was inferior to another intervention (NET) in two studies (Neuner et al., Reference Neuner, Schauer, Klaschik, Karunakara and Elbert2004; Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011). Two further studies assessing interpersonal therapy or the use of guided imagery reported no reduction in symptoms (Brakemeier et al., Reference Brakemeier, Zimmermann, Erz, Bollmann, Rump, von Kempski, Grossmüller, Mitelman, Gehrisch and Spies2017; Zehetmair et al., Reference Zehetmair, Kaufmann, Tegeler, Kindermann, Junne, Zipfel, Herpertz, Herzog and Nikendei2018). A brief summary of the results can be found in Table 3.
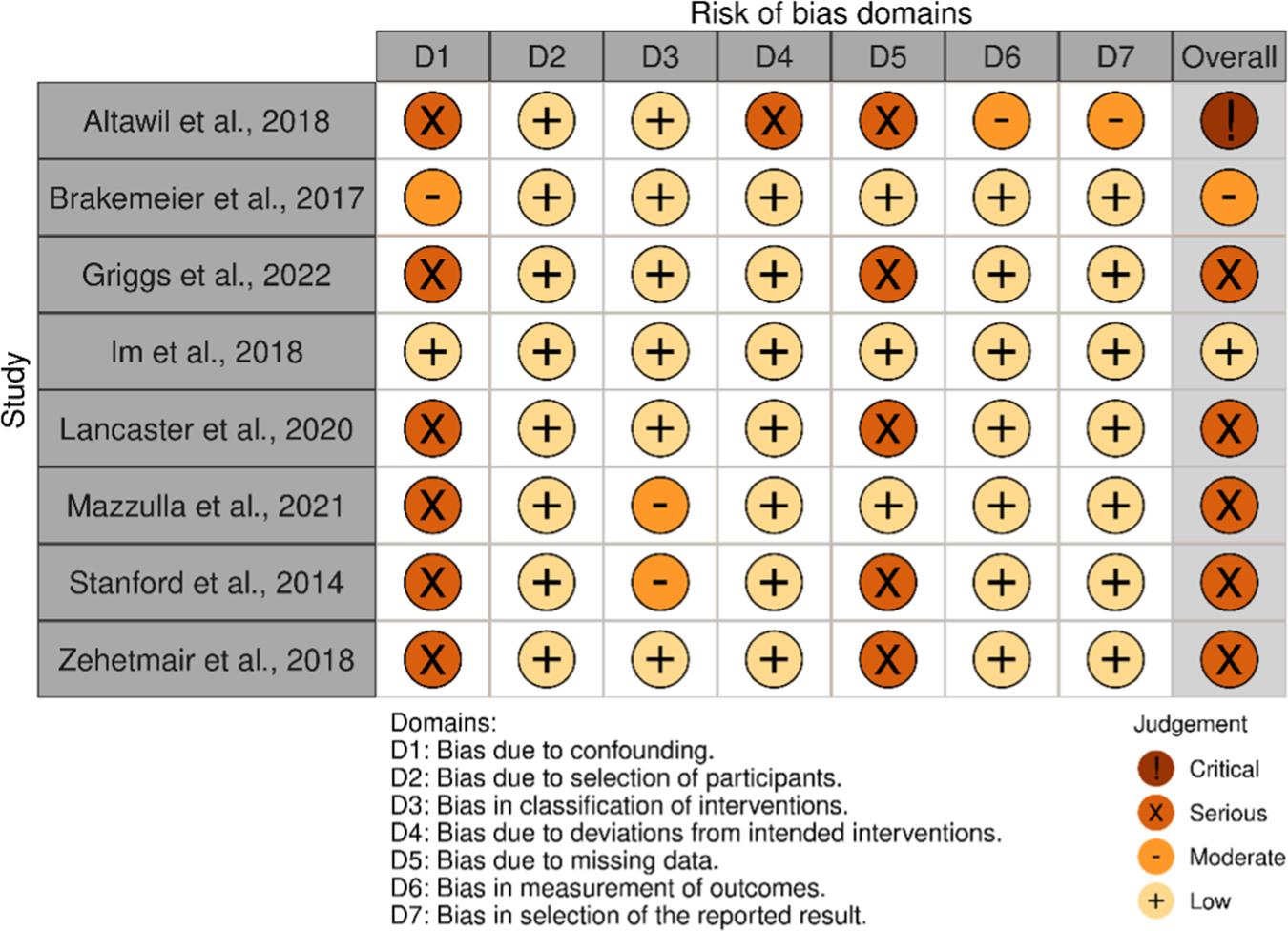
Risk of bias assessment
The results of the risk of bias assessment are presented in two separate figures: Figure 2 for randomized studies and Figure 3 for nonrandomized studies. It is evident that the majority of studies exhibit a high overall risk of bias.
Risk assessment for randomized-controlled trials (RoB2).

Risk assessment for non-randomized trials (ROBINS-I).

Discussion
The aim of this scoping review was to give an overview of the current literature on stabilizing, nonexposure-based interventions for refugees with trauma-related disorders. With a total number of 31 studies examined, six trials reported a significant reduction of PTSD symptom burden after conduction of a stabilizing intervention when compared to waitlist, three when compared to treatment as usual, nine in a pre–post analysis. Nine studies found no difference in the effectiveness of PTSD symptom reduction when compared to another intervention.
Implemented stabilization interventions and underlying definitions of stabilization
The question of how to define stabilization played a significant role throughout the review. Over 15 different interventions were implemented, often in varying formats (e.g., group or individual sessions, professional or lay counselors, app-based approaches) and in some cases with limited details about the interventions. This lack of specificity made precise differentiation between the interventions challenging. It is noteworthy that, in most publications, the interventions were not explicitly described as stabilizing, though the reviewed interventions encompassed various dimensions of stabilization. Several approaches targeted emotional stabilization, employing methods such as skills training and SM to enhance individuals’ capacity to manage anxiety and overwhelming emotions (Carlsson et al., Reference Carlsson, Sonne, Vindbjerg and Mortensen2018; Koch et al., Reference Koch, Ehring and Liedl2020). Mindfulness-based interventions were also prominent, fostering decentering, self-compassion and reduced emotional reactivity (Aizik-Reebs et al., Reference Aizik-Reebs, Yuval, Hadash, Gebreyohans Gebremariam and Bernstein2021; Aizik-Reebs et al., Reference Aizik-Reebs, Amir, Yuval, Hadash and Bernstein2022). These can counteract typical symptoms such as hyperarousal, emotional numbness or negative mood and cognition or feelings of guilt and shame. Other interventions addressed interpersonal difficulties, which are often central to trauma-related disorders, particularly in the context of interpersonal trauma (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Alsheikh Ali, Reference Alsheikh Ali2020). One study focused explicitly on rebuilding community relationships in postcivil war Burundi, emphasizing that restoring trust was pivotal in alleviating PTSD symptoms (Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010). Efforts to address everyday challenges, contributing to social stabilization, were exemplified by the Problem Management Plus intervention (Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022), alongside general counseling approaches and “treatment as usual,” which also provided support in navigating asylum processes (Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013).
It is possible that with a different underlying referential definition, further or different studies would have been included. For example, one study comparing social media-based drama, music and art therapy was excluded because the interventions described did not align with the definitional criteria used as a reference framework (Gever et al., Reference Gever, Iyendo, Obiugo-Muoh, Okunade, Agujiobi-Odoh, Udengwu, Talabi and Nwokolo2023). On the other hand, studies were included in which psychological counseling was conducted, with one study addressing “problems related to asylum status, and other practical matters,” among other aspects (Stenmark et al., Reference Stenmark, Catani, Neuner, Elbert and Holen2013). This raises the question of where the boundaries between psychotherapeutic stabilization, dealing with everyday struggles and social work support lie. Existing literature highlights that prolonged asylum procedures, temporary housing and language barriers exacerbate PTSD symptoms among refugees (Li et al., Reference Li, Liddell and Nickerson2016; Kartal et al., Reference Kartal, Alkemade and Kiropoulos2019). Accordingly, interventions that help to deal with social difficulties could possibly have a stabilizing effect and contribute to the reduction of PTSD symptomatology. Therefore, it may be important to emphasize the aspect of social stabilization more prominently in therapeutic interventions and further investigate its impact.
Contextual factors influencing the effectiveness of stabilization interventions
The overall analysis indicates that the effectiveness of the stabilizing interventions is closely associated with the participants’ living conditions. Some studies found no significant effects of the stabilizing intervention on PTSD symptoms. The reasons given by the authors included the intervention’s focus on addressing daily struggles, while the absence of exposure-based therapy was suggested as a factor in preventing changes in PTSD symptoms (Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022). In another study, challenging environmental conditions such as poverty, separation from family, concern for their safety in the country of origin, and loneliness were identified as limiting factors for therapeutic success (Bryant, Reference Bryant2022; Bryant et al., Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022b), as the same intervention was successful under different living conditions (De Graaff et al. Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020, Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023). Similarly, another study hypothesized that living conditions in a reception center, combined with an uncertain residency status, contributed to the lack of improvement in PTSD symptoms (Zehetmair et al., Reference Zehetmair, Kaufmann, Tegeler, Kindermann, Junne, Zipfel, Herpertz, Herzog and Nikendei2018). It appears that the environmental conditions serve both as an explanatory model for why an intervention does not lead to symptom reduction but are also directly addressed as part of the therapy for stabilization. An uncontrolled study demonstrated that the number of postmigratory stressors, as well as ongoing conflicts in the country of origin, were associated with reduced symptom improvement through therapy. Additionally, an insecure residency status was linked to an increased likelihood of therapy dropout (Djelantik et al., Reference Djelantik, de, Kuiper, Kleber, Boelen and Smid2020). However, a longitudinal study indicated that psychosocial interventions addressing postmigratory stressors primarily led to symptom reduction in depression and anxiety but not in PTSD (Schick et al., Reference Schick, Morina, Mistridis, Schnyder, Bryant and Nickerson2018). Although no definitive conclusions can be drawn in this regard, the significant relevance of postmigratory stressors as an influencing factor can be acknowledged. These stressors repeatedly emerge as a critical issue in therapeutic settings (Bruhn et al., Reference Bruhn, Rees, Mohsin, Silove and Carlsson2018).
The aspect of individual living conditions and the question of whether interventions are adapted to these conditions or even specifically address coping with them has been highlighted by many authors. The need to address daily stressors and postmigration difficulties (Knefel et al. Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022; De Graaff et al. Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023), which are known to contribute to a higher symptom burden (Gleeson et al., Reference Gleeson, Frost, Sherwood, Shevlin, Hyland, Halpin, Murphy and Silove2020), was emphasized. For example, Lancaster and Gaede (Reference Lancaster and Gaede2020) investigated a resilience-based approach that aims to foster a person’s religiousness, gratitude, kindness, hope and courage in order to help them become more resilient. This program relies on nonprofessional providers in a group format and posits that resilience is a necessary skill for living and surviving in a refugee camp. Moreover, the intervention problem management plus focuses on problem-solving strategies, SM, behavioral activation and strengthening social support networks. This aims to address psychosocial challenges (De Graaff et al., Reference De Graaff, Cuijpers, McDaid, Park, Woodward, Bryant, Fuhr, Kieft, Minkenberg and Sijbrandij2020; Bryant, Reference Bryant2022; Bryant et al., Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022b; De et al., Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023). It is important to note, however, that peri- and postmigratory stressors vary significantly in every context. This scoping review included studies on refugees worldwide, whose living conditions are difficult to compare. For instance, individuals living in refugee camps face different challenges than those who have arrived in a destination country and are seeking asylum. Even within the latter group, significant differences exist between those with secure residency status and those without it regarding their mental health burden (Laban et al., Reference Laban, Komproe, Gernaat and de Jong2008) and effectiveness of therapeutic interventions (Ter Heide and Smid, Reference Ter Heide and Smid2015). A systematic analysis of the WHO intervention PM+ reveals that the same intervention produces highly heterogeneous outcomes across different settings (Schäfer et al., Reference Schäfer, Thomas, Lindner and Lieb2023). A comparable large-scale comparison is not available for other stabilization-focused studies with refugees or asylum seekers. To minimize the variability introduced by external factors, different interventions could be compared under similar circumstances rather than comparing the same intervention under different circumstances.
Limited resources and resulting adaptations of stabilization interventions
The challenge of limited resources is a recurring issue in refugee treatment settings and frequently necessitates context-specific adaptations of interventions. Some of the respective examined interventions are easily learnable and implementable by laypersons or peers (Meffert et al., Reference Meffert, Abdo, Alla, Elmakki, Omer, Yousif, Metzler and Marmar2014; Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014; Lancaster and Gaede, Reference Lancaster and Gaede2020; De Graaff et al., Reference De Graaff, Cuijpers, Twisk, Kieft, Hunaidy, Elsawy, Gorgis, Bouman, Lommen and Acarturk2023). This highlights the challenge of limited resources, as interventions delivered by laypersons can reach a larger population compared to those requiring trained mental health professionals. It should be noted that there is also a study on NET conducted by laypersons (Neuner et al., Reference Neuner, Onyut, Ertl, Odenwald, Schauer and Elbert2008), though this is not the case for other forms of exposure therapy, such as EMDR. Additionally, other forms of resource constraints can impact the execution of studies. For example, a study conducted in a camp for internally displaced persons reported shortages of paper and printing facilities for therapy materials (Stanford et al., Reference Stanford, Elverson, Padilla and Rogers2014). Group interventions also appear to be a better format for effective resource utilization. This is also reflected in the studies presented, as 15 of the 31 studies were conducted in a group format. Resource considerations also underpinned the two studies examining interventions via apps, as these are flexible and, once established, resource-efficient. Mazulla et al. addressed another aspect by creating a language-free app to reach a larger number of people (Mazzulla et al., Reference Mazzulla, Fondacaro, Weldon, Dibble and Price2021). The current state of knowledge about smartphone-based mental health interventions for refugees was evaluated in a systematic review. The authors summarized that, up to now, none of the apps examined sufficiently met the needs of the target group (El-Haj-Mohamad et al., Reference El-Haj-Mohamad, Nohr, Niemeyer, Böttche and Knaevelsrud2023). These factors should not only be accounted for in research studies but also considered when designing interventions for implementation outside of a research context. Not only due to limited resources but also to address shared mechanisms underlying common mental health issues, some authors have implemented transdiagnostic interventions that target PTSD alongside other conditions (Koch et al., Reference Koch, Ehring and Liedl2020; Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022). This approach was motivated by the frequent comorbidities associated with PTSD and the recognition that psychological distress among refugees extends beyond PTSD (Fazel et al., Reference Fazel, Wheeler and Danesh2005; Hinchey et al., Reference Hinchey, Nashef, Bazzi, Gorski and Javanbakht2023a), despite the latter often being the primary focus of research (Akhtar et al., Reference Akhtar, Giardinelli, Bawaneh, Awwad, Al-Hayek, Whitney, Jordans, Sijbrandij, Cuijpers and Dawson2021; Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al. Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a, Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogelb; Knefel et al., Reference Knefel, Kantor, Weindl, Schiess-Jokanovic, Nicholson, Verginer, Schäfer and Lueger-Schuster2022). A broader focus also allows for reaching more individuals experiencing psychological distress, which is particularly relevant in resource-limited settings, such as refugee camps or mass accommodations. Moreover, such approaches do not rely on formal diagnoses or corresponding specific interventions, making them more resource-efficient. Additionally, avoiding formal diagnostic procedures can help mitigate potential stigma, which might otherwise hinder access to effective treatment (Lancaster and Gaede, Reference Lancaster and Gaede2020). A systematic analysis of the barriers to mental health care among refugee populations also showed that it was primarily self-stigma and the fear of social consequences that prevented those affected from seeking professional help (Byrow et al., Reference Byrow, Pajak, Specker and Nickerson2020). Another transdiagnostic intervention employed in refugee populations is the common elements treatment approach, which shows a significant reduction in PTSD symptom burden (Bolton et al., Reference Bolton, Bass, Zangana, Kamal, Murray, Kaysen, Lejuez, Lindgren, Pagoto, Murray, Van Wyk, Ahmed, Mohammad Amin and Rosenblum2014; Bogdanov et al., Reference Bogdanov, Augustinavicius, Bass, Metz, Skavenski, Singh, Moore, Haroz, Kane, Doty, Murray and Bolton2021). However, these studies were excluded from this review because the manual for participants in low- and middle-income countries includes gradual exposure and in-vivo exposure (Murray et al., Reference Murray, Dorsey, Haroz, Lee, Alsiary, Haydary, Weiss and Bolton2014).
Needs and limitations of cultural adaptation of stabilization interventions
The studies included also repeatedly highlighted the limited applicability of Western concepts, which may not meet the needs of the target population (Altawil et al., Reference Altawil, El Asam and Khadaroo2018; Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018). For SIT, the lack of cultural adaptation of the intervention for non-Western patients was also identified as a possible explanation as to why the intervention, contrary to the hypothesis, did not lead to significant symptom improvement (Hensel-Dittmann et al., Reference Hensel-Dittmann, Schauer, Ruf, Catani, Odenwald, Elbert and Neuner2011). The use of peers in delivering interventions could better address this aspect during the implementation of the intervention and overcome the language and cultural barriers, thus representing a lower-threshold access to psychosocial care. In some of the interventions, adaptations to the culture of the sample had already taken place within the intervention. For example, the “Community Wellness Focussing” intervention, which was carried out in Gaza, included a session on “Proverbs and Quran exercises” (Altawil et al., Reference Altawil, El Asam and Khadaroo2018). In a study conducted in Burundi in a camp for internally displaced persons on the other hand, the focus was on restoring social relationships within the community (Yeomans et al., Reference Yeomans, Forman, Herbert and Yuen2010). Collaborative work in the community was also a major part of the study with trauma-informed psychoeducation for Somali refugees in Kenya, with sessions on “Stigma, Collective trauma, Collective healing” (Im et al., Reference Im, Jettner, Warsame, Isse, Khoury and Ross2018). In another study, efforts were made to adapt the intervention to the sample by consulting an advisor from the same country. In this case, gender issues and the timing of the intervention were adapted. However, no further details were disclosed (Hasha et al., Reference Hasha, Igland, Fadnes, Kumar, Heltne and Diaz2022).
Implications and summary
It becomes apparent that the authors of the presented studies provided varied responses to the challenge of addressing the complex treatment conditions of traumatized refugees, which is reflected in the heterogeneity of the study designs, interventions and results. The living conditions in which these studies were examined differ considerably. The systemic difficulties in providing psychosocial support for refugees also have an impact on the conduct of studies. The studies presented here, which were conducted under the living conditions in humanitarian settings, are subject to a variety of factors that influence the results, which must be considered in detail (Panter-Brick et al., Reference Panter-Brick, Eggerman, Ager, Hadfield and Dajani2020; Hinchey et al., Reference Hinchey, Khalil and Javanbakht2023b). In 18 out of the 31 studies presented, a significant reduction in PTSD symptoms was observed as a result of the stabilizing intervention. However, a meta-analysis would be necessary to validly assess the effectiveness of stabilizing interventions for refugees, as the methods used in this review cannot provide definitive conclusions on this matter. The focus of the evaluation should consider the living conditions of refugees, as the outcomes of the same intervention may not readily translate from refugee camps to life circumstances in the country of resettlement (Acarturk et al., Reference Acarturk, Uygun, Ilkkursun, Yurtbakan, Kurt, Adam-Troian, Senay, Bryant, Cuijpers and Kiselev2022; Bryant et al., Reference Bryant, Bawaneh, Awwad, Al-Hayek, Giardinelli, Whitney, Jordans, Cuijpers, Sijbrandij and Ventevogel2022a), even though many factors, such as insecure residency status (Laban et al., Reference Laban, Komproe, Gernaat and de Jong2008), family separation (Fogden et al., Reference Fogden, Berle and Steel2020), temporary housing (Ziersch et al., Reference Ziersch, Walsh, Due and Duivesteyn2017; Leiler et al., Reference Leiler, Bjärtå, Ekdahl and Wasteson2019), unemployment (Lai et al., Reference Lai, Due and Ziersch2022) and language acquisition (Kartal et al., Reference Kartal, Alkemade and Kiropoulos2019), are already known to contribute to psychological distress. Furthermore, studies published in non-English languages or found in the gray literature could also be included to provide a more comprehensive and globally representative overview of stabilization approaches. Given the contextual diversity among refugee populations, qualitative studies could furthermore deepen the understanding of how refugees interpret and experience stabilization interventions in relation to their cultural, political and social realities, taking host-country-specific context into account.
Limitations
Some limitations of this scoping review should be acknowledged: both during the screening process and the final selection of studies, stabilization was understood according to the definition provided by Luise Reddemann (Reddemann, Reference Reddemann2011; Reddemann and Piedfort-Marin, Reference Reddemann and Piedfort-Marin2017). Consequently, studies that did not align with this definition or did not offer sufficient information to ascertain their fit were excluded. With regard to the results of the bias assessment, it can be seen that limitations arise primarily due to missing data, which appear to be understandable under the living circumstances mentioned with high fluctuation and social and economic deprivation. In addition, it should be mentioned that there is a certain risk of bias in all studies, as the interventions cannot be blinded and the measurements were always patient-reported outcomes. Another important limitation should be acknowledged: among the included studies, nine did not clearly specify their inclusion criteria. In eight studies, participants were included based on a general psychological burden without further specification, and one study also included participants with other diagnoses. Seven studies reported the presence of a PTSD diagnosis but did not provide details about the diagnostic procedures. Only six studies explicitly defined a PTSD diagnosis as an inclusion criterion and described the respective diagnostic instruments. However, the majority of the studies identified the reduction of trauma-related symptoms as their objective, even if PTSD was not defined as an inclusion criterion. A similar issue applies to the age inclusion criterion: some studies also targeted participants under 18 years old, and, in a few studies, the age of the participants was not entirely clear, leading to ambiguities in defining the target population. We chose not to exclude certain studies based on the following rationale: Refugees are frequently exposed to traumatic events, which is associated with a significantly higher prevalence of PTSD compared to the general population. Although current clinical guidelines recommend exposure-based interventions, such approaches cannot always be implemented for the reasons outlined in our introduction. A strict, linear logic – where only studies are included that demonstrate a direct, simple link between a traumatic event, a formally diagnosed PTSD using a standardized instrument, and an intervention specifically tailored to PTSD symptoms – would have led to an overly narrow selection. Such an approach would not sufficiently reflect the complexity of this research question and research environment, as elaborated in various aspects throughout the discussion. To account for this complexity and to offer a more comprehensive picture of the existing evidence, we deliberately applied broader inclusion criteria in our review.
Conclusion
The findings of this scoping review indicate that a range of stabilizing interventions for refugees have been explored. The 31 studies that were included yielded heterogeneous results, with most showing significant PTSD symptom reduction compared to waitlist, treatment as usual or in pre–post analyses, though some found no differences between interventions, and a few reported the stabilizing approach as less effective or ineffective. Both the heterogeneity of the interventions and the environmental conditions under which the studies were conducted limit the generalizability of the results. Future studies or publications should place greater emphasis on incorporating the specific living conditions under which their results are obtained. Additionally, qualitative studies could provide valuable insights by engaging affected individuals to identify factors they perceive as contributing to symptom improvement.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2025.10028.
Data availability statement
Data sharing is not applicable – no new data is generated.
Author contribution
IR: conzeptualization, data curation, investigation, formal analysis, writing – original draft, writing – reviewing & editing, NG: investigation, formal analysis, writing – reviewing & editing, JN: investigation, formal analysis, writing – reviewing & editing, BB: investigation, formal analysis, writing – rewriting and editing, HCF: resources, CN: supervision, resources, writing – reviewing & editing.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.


 Open access
Open access
Comments
Dear Prof. Bass, Prof. Chibanda,
dear editors and editorial board,
we would like to submit our article entitled “Stabilization Interventions in the Treatment of Traumatized Refugees – A Scoping Review” for publication in Global Mental Health.
It is well known, that refugees and forced migrants are stated as a group in society that is particularly affected by traumatic events in different phases of their escape, leading to a prevalence of post-traumatic stress disorder around 30%. However, the adequate treatment of trauma-related disorders in refugees is hampered by many obstacles, such as the legal basis to stay, language- and cultural barriers as well as limited access to health care. This can lead to difficult treatment conditions and requires consideration in the treatment of symptoms of trauma related disorders. While most guidelines recommend exposure-based approaches for the treatment of post-traumatic stress disorder, stabilizing approaches that aim for an improvement of a patients’ capacity to deal with trauma-related stimuli, emotions, and memories, move into the background. However, they are well established in clinical practice, and often also included in exposure-based interventions. In this scoping review, we therefore shed light on “psychological stabilization” as a therapeutic approach in the context of the treatment of refugees with trauma-related disorders. For this purpose, we conducted a systematic search in 5 data bases, which led to the inclusion of 31 studies. It became evident, that the non-exposure-based therapies that have been examined frequently follow a transdiagnostic approach, as well as interventions that are compatible with cultural values and that laypeople or peers can also implement.
We believe that this manuscript is appropriate for publication Global Mental Health because it puts focus on a therapeutic approach which is little represented in current research but yet has a particular relevance for the population of refugees in the aftermath of traumatic experiences.
Our submission contains original work that has not been previously published elsewhere. The authors have no conflicts of interests to disclose.
Thank you very much for taking the time to read our article and consider it for publication. If you require any additional information, please feel free to contact us at the address stated below. We look forward to hearing from you.
Sincerely,
Dr. med. Irja Rzepka