

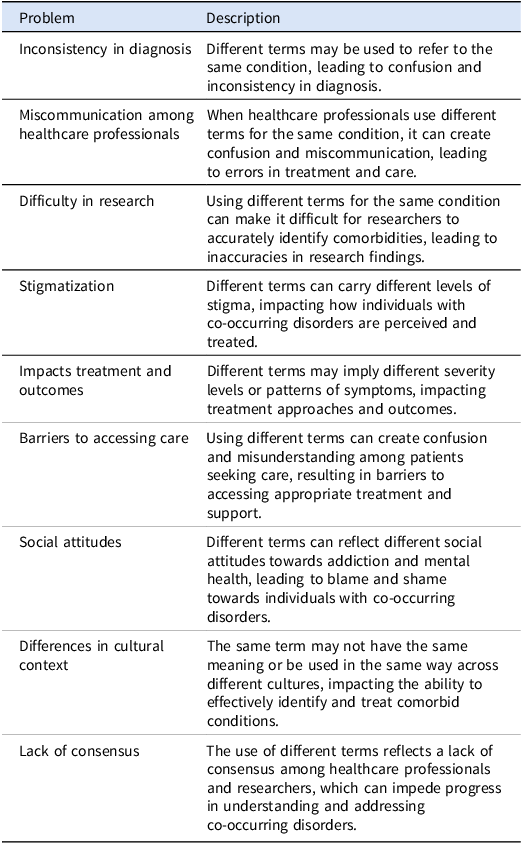
The coexistence of a substance use disorder (SUD) and another psychiatric disorder in the same individual has been described in the literature over the years using various terms, including psychiatric comorbidity, dual disorders, comorbidity, and dual pathology, among others. This lack of terminological consensus has affected all stakeholders – patients, their families, healthcare professionals, and researchers – in multiple ways (see Table 1). While a universally accepted definition remains elusive, there is an increasing call for standardizing the term “Dual Disorders” (Szerman et al. Reference Szerman, Torrens, Maldonado, Balhara, Salom, Maremmani, Sher, Didia-Attas, Chen and Baler2022).
Short description of problems derived from the “undefinition” of dual disorders

Multiple epidemiological studies have shown that co-occurring psychiatric disorders are common among individuals with SUD. The prevalence of this comorbidity varies widely (approximately 30–80%), depending on several factors, including the substance involved (e.g., stimulants, opioids, cannabis), gender, and the studied population (e.g., general population, treatment-seeking or non-treatment-seeking patients, prisoners, homeless individuals, migrants) (Alonso et al. Reference Alonso, Angermeyer, Bernert, Bruffaerts, Brugha, Bryson, Girolamo, Graaf, Demyttenaere, Gasquet, Haro, Katz, Kessler, Kovess, Lepine, Ormel, Polidori, Russo, Vilagut and Almansa2004; Farrell et al. Reference Farrell, Howes, Bebbington, Brugha, Jenkins, Lewis, Marsden, Taylor and Meltzer2001; Jacobi et al. Reference Jacobi, Wittchen, Hölting, Höfler, Pfister, Müller and Lieb2004; Reginsson et al. Reference Reginsson, Ingason, Euesden, Bjornsdottir, Olafsson, Sigurdsson, Oskarsson, Tyrfingsson, Runarsdottir, Hansdottir, Steinberg, Stefansson, Gudbjartsson, Thorgeirsson and Stefansson2018; Torrens et al. Reference Torrens, Mestre-Pintó and Domingo-Salvany2015).
People with dual disorders, compared to those with a single disorder (either SUD or another psychiatric condition), exhibit worse clinical and social prognoses (Torrens et al. Reference Torrens, Rossi, Martinez-Riera, Martinez-Sanvisens and Bulbena2012). They generally present with more severe psychopathological symptoms, a higher risk of suicide, increased substance use relapses, higher treatment dropout rates, lower medication adherence, and more medical comorbidities (e.g., HIV, hepatitis). Additionally, they experience higher rates of emergency department visits and hospitalizations, greater unemployment, increased involvement in violence and illegal activities, and a heightened risk of social exclusion (Torrens et al. Reference Torrens, Mestre-Pintó and Domingo-Salvany2015; Volkow et al. Reference Volkow, Torrens, Poznyak, Sáenz, Busse, Kashino, Krupchanka, Kestel, Campello and Gerra2020; Volkow and Blanco Reference Volkow and Blanco2023). Thus, these patients with dual disorders, place a high burden on society.
Despite extensive knowledge about this association, both non-SUD mental disorders and SUDs are often underdiagnosed and undertreated. This is partly due to persistent challenges in understanding and categorizing these conditions, as well as the difficulties in identifying and implementing the most appropriate treatment (Szerman et al. Reference Szerman, Torrens, Maldonado, Balhara, Salom, Maremmani, Sher, Didia-Attas, Chen and Baler2022; United Nations Office on Drugs and Crime [UNODC], 2022; Volkow et al. Reference Volkow, Torrens, Poznyak, Sáenz, Busse, Kashino, Krupchanka, Kestel, Campello and Gerra2020).
The diagnosis of dual disorders presents two fundamental challenges. First, the acute and chronic effects of substances often mimic the symptoms of various mental disorders, making it difficult to distinguish between psychopathological symptoms caused by substance use, withdrawal, or an independent psychiatric condition. Second, psychiatric disorders are classified as syndromes – patterns of symptoms with some clinical validity – rather than well-defined diseases with known pathophysiology and reliable biological markers. Overall, differentiating between primary psychiatric disorders, substance-induced disorders, and the expected effects of substance use or withdrawal is a key aspect of diagnosing dual disorders (Torrens et al. Reference Torrens, Mestre-Pintó and Domingo-Salvany2015). To facilitate this complex diagnostic process, various clinical tools are available, including standardized clinical interviews, which aid in establishing a diagnosis, and screening instruments (e.g., interviews, scales) designed to detect potential comorbid conditions (Torrens et al. Reference Torrens, Mestre-Pintó and Domingo-Salvany2015). The choice of tool depends on several factors, such as the context (clinical, epidemiological, or research), the assessment objectives (single or multiple diagnoses), the time available for evaluation, and the expertise of the assessing professionals.
Across many European countries, two primary barriers hinder the effective management of dual disorders. First, there is a significant divide between mental health care services and substance use treatment networks, leading to fragmented care. Second, treatment services often lack the necessary integrated expertise to effectively address both types of disorders, resulting in suboptimal outcomes for patients (Mueser et al. Reference Mueser, Noordsy, Drake and Fox2003; Torrens et al. Reference Torrens, Mestre-Pintó and Domingo-Salvany2015).
The “wrong door syndrome” describes the challenges individuals with dual disorders face in accessing appropriate treatment services (UNODC, 2022). This occurs when a person seeks help from a medical or mental health provider who lacks the expertise or resources to address both substance use and psychiatric conditions – a phenomenon known as diagnostic overshadowing. As a result, these individuals often do not receive the integrated, comprehensive care necessary to manage both conditions simultaneously, leading to poorer outcomes. Furthermore, people with dual disorders are frequently excluded from clinical studies evaluating treatment efficacy, which limits the development of evidence-based guidelines tailored to this population.
Dual disorders are highly prevalent and significantly worsen clinical severity, impair psychosocial functioning, and diminish the quality of life of affected patients. Identifying co-occurring mental disorders in patients with SUD is crucial for tailoring the most effective treatment approach. The effective detection and treatment of dual disorders is a major challenge that health policymakers and professionals in addiction and mental health must address in the coming years. The therapeutic approach to dual disorders – whether pharmacological, psychological, or both – must take a holistic view of both conditions from the outset to determine the best treatment option for each individual.
Acknowledgements
We acknowledge the use of ChatGPT (OpenAI) for assistance in revising and improving the English language of this manuscript.
Author contributions
All authors contributed to the writing and revision of this short communication.
Funding statement
MT, FF and JIM RD24/0003/0001 are funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union.
Competing interests
The authors confirm they have no conflict of interest to declare.

 Open access
Open access