


Introduction
The development of psychopathology during childhood and adolescence is complex and may follow diverse patterns (Cicchetti and Rogosch, Reference Cicchetti and Rogosch2002; Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020). Psychopathological continuity and discontinuity in developmental pathways are not fully understood, but it is well-established that early mental health problems are not specific and often overlap with different psychiatric diagnoses, also symptoms can change over time, leading to diagnostic crossover to other psychiatric diagnoses (Plana-Ripoll et al., Reference Plana-Ripoll, Pedersen, Holtz, Benros, Dalsgaard, de Jonge, Fan, Degenhardt, Ganna, Greve, Gunn, Iburg, Kessing, Lee, Lim, Mors, Nordentoft, Prior, Roest, Saha, Schork, Scott, Scott, Stedman, Sørensen, Werge, Whiteford, Laursen, Agerbo, Kessler, Mortensen and McGrath2019; Watkeys et al., Reference Watkeys, O’Hare, Dean, Laurens, Tzoumakis, Harris Maclinepi, Carr and Green2024).
Children and adolescents often present with a variety of symptoms and could potentially fit into a number of diagnostic groups, presenting challenges in diagnostic formulation (Gillberg, Reference Gillberg2010). Psychiatric disorders in childhood are often grouped into affective and neurodevelopmental disorders. Affective disorders include depression and anxiety, while neurodevelopmental disorders include attention-deficit/hyperactivity disorder (ADHD), autism and schizophrenia (American Psychiatric Association, 2013; Thapar et al., Reference Thapar, Cooper and Rutter2017). Some people may have more than one diagnosis from the same diagnostic group, while others may have diagnoses from different diagnostic groups at different points in time (Shevlin et al., Reference Shevlin, McElroy and Murphy2017). The overlap between affective and neurodevelopmental disorders aligns with evidence that different mental disorders share some common gene variants (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel, Meier, Ramrakha, Shalev, Poulton and Moffitt2014, Reference Caspi, Houts, Ambler, Danese, Elliott, Hariri, Harrington, Hogan, Poulton, Ramrakha, Rasmussen, Reuben, Richmond-Rakerd, Sugden, Wertz, Williams and Moffitt2020; Gandal et al., Reference Gandal, Haney, Parikshak, Leppa, Ramaswami, Hartl, Schork, Appadurai, Buil, Werge, Liu, White, Horvath, Geschwind, Sestan, Vaccarino, Gerstein, Weissman, Pochareddy, State, Knowles, Farnham, Akbarian, Pinto, Van Baekl, Dracheva, Jaffe, Hyde, Zandi, Crawford, Sullivan, Thompson, Mortensen, Agerbo, Pedersen, Pedersen, Mors, Børglum, Nordentoft, Hougaard, Bybjerg-Grauholm, Bækvad-Hansen, Martin, Dumont, Stevens, Churchhouse, Howrigan, Palmer, Robinson, Satterstrom, Cerrato, Huang, Goldstein, Moran, Julian, Kimberly, Patrick, Turley, Walters, Belliveau, Ripke, Poterba, Daly, Neale, Fromer, Roussos, Johnson, Shah, Mahajan, Schadt, Haroutunian, Ruderfer, Buxbaum, Sieberts, Dang, Logsdon, Mangravite, Peters, Gur, Hahn, Devlin, Klei, Lewis, Lipska, Hirai, Toyoshiba and Domenici2018).
Much epidemiological research focusing on children’s psychopathology has applied a cross-sectional approach to examining emotional and behavioural problems or psychiatric diagnoses (Caspi et al., Reference Caspi, Houts, Ambler, Danese, Elliott, Hariri, Harrington, Hogan, Poulton, Ramrakha, Rasmussen, Reuben, Richmond-Rakerd, Sugden, Wertz, Williams and Moffitt2020; Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020). A growing body of evidence suggests several possible factors contributing to psychopathology, especially during childhood and adolescence (Cicchetti and Rogosch, Reference Cicchetti and Rogosch2002; Plana-Ripoll et al., Reference Plana-Ripoll, Pedersen, Holtz, Benros, Dalsgaard, de Jonge, Fan, Degenhardt, Ganna, Greve, Gunn, Iburg, Kessing, Lee, Lim, Mors, Nordentoft, Prior, Roest, Saha, Schork, Scott, Scott, Stedman, Sørensen, Werge, Whiteford, Laursen, Agerbo, Kessler, Mortensen and McGrath2019). Studies mapping the variety of developmental trajectories of childhood psychopathology can improve our understanding of emotional and behavioural difficulties and psychiatric diagnoses. Several well-conducted studies have examined trajectories of ADHD (Stepp et al., Reference Stepp, Burke, Hipwell and Loeber2012), anxiety (de Lijster et al., Reference de Lijster, van den Dries, van der Ende, Utens, Jaddoe, Dieleman, Hillegers, Tiemeier and Legerstee2019), depression symptoms (de Lijster et al., Reference de Lijster, van den Dries, van der Ende, Utens, Jaddoe, Dieleman, Hillegers, Tiemeier and Legerstee2019; Weavers et al., Reference Weavers, Heron, Thapar, Stephens, Lennon, Bevan Jones, Eyre, Anney, Collishaw, Thapar and Rice2021; Sørensen et al., Reference Sørensen, Plana-Ripoll, Bültmann, Winding, Steen and Biering2025), anti-social behaviour (Harold et al., Reference Harold, Leve, Kim, Mahedy, Gaysina, Thapar and Collishaw2014) and internalizing and externalizing psychopathology (Reef et al., Reference Reef, Diamantopoulou, Van Meurs, Verhulst and Van Der Ende2011; Lancefield et al., Reference Lancefield, Raudino, Downs and Laurens2016). Some have even taken a broader perspective by including all psychiatric diagnoses in their analysis (Senior et al., Reference Senior, Pierce, Taxiarchi, Garg, Edge, Newlove-Delgado, Neufeld and Abel2024; Watkeys et al., Reference Watkeys, Tzoumakis, Dean, Laurens, Harris, O’Hare, Carr and Green2025b). An important dimension to include is young people’s use of medication, as a previous study has shown that more than 80% of all individuals receive some mental health treatment, including prescriptions, during their lifetime (Kessing et al., Reference Kessing, Ziersen, Caspi, Moffitt and Andersen2023). Another study demonstrated that over 30% of youth were prescribed a psychotropic medication and 10% received multiple psychotropic medications (Watkeys et al., Reference Watkeys, O’Hare, Dean, Laurens, Tzoumakis, Harris, Carr and Green2025a). Psychotropic medication use may reflect an underlying psychiatric diagnosis, such as ADHD, that is not necessarily captured in public health registers, particularly when diagnoses are made in healthcare settings where reporting is not complete or systematic (Lauritsen et al., Reference Lauritsen, Jørgensen, Madsen, Lemcke, Toft, Grove, Schendel and Thorsen2010; Mors et al., Reference Mors, Perto and Mortensen2011; Madsen et al., Reference Madsen, Ersbøll, Olsen, Parner and Obel2015). Without incorporating prescription data, these individuals may remain unaccounted for in research, potentially leading to biased or incomplete conclusions. To our knowledge, no single study so far has integrated psychiatric diagnoses, self-reported behavioural data and prescription information simultaneously within the same study population from early childhood to adolescence.
This study was motivated by the need to move beyond isolated data sources to better understand developmental trajectories by integrating symptoms, multiple and repeated diagnoses and medication use. We aimed to explore whether certain groups of children and adolescents with mental health challenges might be under-represented or overlooked in formal healthcare systems, as well as to characterize groups with more complex and/or severe trajectories. Investigating these patterns could provide insights into gaps in clinical recognition and support the development of more nuanced approaches for early identification and intervention. This also acknowledges that some young people and their families may engage with alternative pathways to care. Understanding these psychopathological trajectories and associated symptoms requires large population-based studies capturing formal diagnoses, relevant symptoms and psychotropic medication use in childhood and adolescence. We aimed to examine how children’s psychopathology develops by combining questionnaire-based emotional and behavioural reports, psychiatric diagnoses and psychotropic medication prescription data to identify meaningful trajectory groups in a large Danish population where hospital care is government-funded and medications partially reimbursed.
Methods
Study participants
Participants were drawn from the Danish National Birth Cohort (Olsen et al., Reference Olsen, Melbye, Olsen, Sørensen, Aaby, Andersen, Taxbøl, Hansen, Juhl, Schow, Sørensen, Andresen, Mortensen, Olesen and Søndergaard2001; Strandberg-Larsen et al., Reference Strandberg-Larsen, Cederkvist, Aakjær, Bjerregaard, Brix, Feenstra, Meder, Nohr, Olsen, Tøttenborg, Høst Ramlau-Hansen, Vangsted and Andersen2025) and linked with information from nationwide registers (Schmidt et al., Reference Schmidt, Schmidt, Sandegaard, Ehrenstein, Pedersen and Sørensen2015; Pottegård et al., Reference Pottegård, Schmidt, Wallach-Kildemoes, Sørensen, Hallas and Schmidt2016). The Danish National Birth Cohort is a nationwide cohort study of pregnant women and their offspring born in Denmark between 1996 and 2003. More than 96,000 mother–infant dyads were recruited to the Danish National Birth Cohort during their first antenatal care visit in general practice. For detailed information, visit www.dnbc.dk.
We included dyads where the pregnancy resulted in a live, full-term (>37 completed gestational weeks) singleton birth, and we excluded children diagnosed with major congenital anomalies, according to the EUROCAT guide, before the age of 1 year, diagnosed with conditions affecting the central nervous system before age 7, or with learning disabilities (Fig. 1 and Supplementary Table S1, available online). We included children with available data on emotional and behavioural difficulties from at least two out of three possible time points at 7, 11 and 18 years of age, regardless of the respondent. With this strategy, we maximized the sample size and ensured that we had sufficient data on emotional and behavioural problems to estimate the trajectory groups. Of the total sample, 22,179 (45%) children provided all 3 assessments and 27,182 provided 2 (55%).
Flowchart illustrating selection of participants from the Danish National Birth Cohort.

Study measures
Data on emotional and behavioural difficulties, psychiatric diagnoses and prescribed psychotropic medications were used to identify psychopathological trajectories. Detailed definitions, scoring of measures and included dimensions are described below (Supplementary Table S2). Children who emigrated were labelled as missing in years when they were abroad for more than 6 months.
Emotional and behavioural difficulties
The Strengths and Difficulties Questionnaire (SDQ) assessed children’s emotional and behavioural difficulties at ages 7, 11 and 18 (Goodman, Reference Goodman2001). SDQ is a screening tool designed to assess five areas of socio-emotional and behavioural development in children and adolescents: emotional symptoms, conduct problems, hyperactivity and inattention, peer relationship problems and pro-social behaviour. At 7 years, SDQs were completed by a parent; at age 11, by teachers, parents and/or self-report in prioritized order (Stone et al., Reference Stone, Otten, Engels, Vermulst and Janssens2010), and at 18 years by self-report. We reduced data to two dimensions: the 10-item externalizing subscale combining the conduct and hyperactivity/inattention items, and the 10-item internalizing subscale based on the emotional symptoms and peer relationship items, each ranging from 0 to 20 (Supplementary Table S2) (Goodman et al., Reference Goodman, Lamping and Ploubidis2010). We used the broader SDQ subscales since previous studies have emphasized the advantages of this division in low-risk samples (Goodman et al., Reference Goodman, Lamping and Ploubidis2010).
Psychiatric diagnoses
The Danish health registries allowed the capture of psychiatric diagnoses from all inpatient admissions and outpatient contacts, including public/private psychiatric hospitals, somatic departments and emergency visits from age 1 to 18 years (Schmidt et al., Reference Schmidt, Schmidt, Sandegaard, Ehrenstein, Pedersen and Sørensen2015). We included the main and all subsidiary diagnoses. We established the following three dimensions of psychiatric diagnoses: Neurodevelopmental diagnoses including autism, ADHD and schizophrenia spectrum disorders (ICD-10: F20–F29, F80–F83, F84, F88–F89, F90, F95 and F98.8) (Thapar et al., Reference Thapar, Cooper and Rutter2017), affective diagnoses such as anxiety and depression (ICD-10: F30–39, F40–48 and F93) and mixed psychiatric diagnoses (ICD-10: F50, F51, F91, F94, F98.0–98.7, F98.9, F99 and F60–F69) (Supplementary Tables S2, S3 and S5). Children received one count for each unique diagnosis within any of these diagnostic groups per year of life. Psychiatric diagnoses registered before a child’s first birthday were omitted due to potential unreliability.
Redeemed psychotropic medication
Diagnoses given by private practice specialists and general practices are not included in the National Patient Register (Mors et al., Reference Mors, Perto and Mortensen2011). To capture as many cases of psychopathology as possible (Mors et al., Reference Mors, Perto and Mortensen2011; Madsen et al., Reference Madsen, Ersbøll, Olsen, Parner and Obel2015), we included redeemed prescriptions for psychotropic medications from The Danish National Prescription Registry (Pottegård et al., Reference Pottegård, Schmidt, Wallach-Kildemoes, Sørensen, Hallas and Schmidt2016), both to capture children with more severe conditions receiving substantial medication and to identify milder cases, as psychotropic treatment for children and adolescents is initiated by psychiatrists but may subsequently be maintained by general practitioners (GPs), potentially resulting in ongoing treatment without repeated diagnostic registration. We generated yearly binary indicators from 1 to 18 years and grouped children with at least one redeemed prescription (psychostimulants, antidepressants, anxiolytics, antipsychotics and melatonin) (Supplementary Tables S2, S4 and S5).
A study protocol was uploaded to Open Science Framework before initiating any analyses: https://osf.io/3pwk5.
Statistical analyses
We used group-based multi-trajectory modelling (GBMTM) (Nagin et al., Reference Nagin, Jones, Passos and Tremblay2018) to determine trajectories of psychopathological difficulties based on the multiple measurement outcomes: emotional and behavioural difficulties assessed by SDQ, psychiatric diagnoses and psychotropic medications. GBMTM is a latent class technique suitable for taking full advantage of multidimensional longitudinal data on various complementary markers of an underlying latent construct, e.g., the development of psychopathology measured for the same individual, to derive a data-driven description of the composite underlying construct. Participants were scheduled for the same time points (annual or questionnaire-based), but some observations were missing due to, e.g., non-response, which is accommodated within the GBMTM. Using GBMTM, we obtained the number of trajectory groups that best described our data, the trajectory for each group according to our predefined dimensions (internalizing and externalizing difficulties, psychiatric diagnoses and prescribed psychotropic medications, see Supplementary Table S2), and an estimate that describes the probability of each individual belonging to a specific trajectory group.
We identified trajectories separately for boys and girls because of differences in behaviour and psychiatric disorders between boys and girls (Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020). Retention weights based on propensity scores were included when estimating the trajectories to minimize bias due to selective attrition (Supplementary Note S1). The propensity score was predicted from maternal psychiatric diagnosis, paternal psychiatric diagnosis, child psychiatric diagnoses, parity, maternal age, alcohol consumption during pregnancy, maternal smoking during pregnancy, maternal educational level, urban/rural residence and quantiles of household income. For covariates with missing data used in the propensity score calculation, missing values were assigned a separate category, since missingness, especially in questionnaire data, can be informative. Covariates were drawn from the Danish National Birth Cohort interviews, national registries or both.
We ran the GBMTM with up to six trajectory groups to determine the best-fitting model (Supplementary Tables S6 and S7). All dimensions were modelled using polynomials from linear to quartic (orders 1 to 4), except the SDQ, which had only three time points and was therefore limited to quadratic (order 2). Model selection was pursued in three steps: The best-fitting model was identified by comparing the Bayesian Information Criterion (BIC) of each model. We examined each model’s substantive interest, i.e., whether or not each new group added distinct and meaningful information. Additionally, we verified the adequacy of the preferred model by examining the Average Posterior Probability of Assignment to the trajectories (APPA, >70%) and use of the Odds of Correct Classification (OCC, ≥5) (Nagin et al., Reference Nagin, Jones, Passos and Tremblay2018). The model was developed on a random sample of 80% of the data and the performance was checked on the remaining 20%.
Analyses were conducted in SAS 9.4 using proc traj.
Results
In this study, psychopathological trajectories were examined by analysing data across childhood and adolescence for 23,361 boys and 26,000 girls in the GBMTM analysis.
Childhood psychopathological trajectories
The GBMTM analysis resulted in the selection of six distinct trajectory groups for both boys and girls. The BIC improved when adding groups (Supplementary Tables S6 and S7). We did not observe the emergence of very small groups (less than 2% of the included participants), and each added group appeared to make a distinct conceptual contribution.
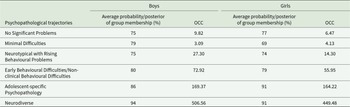
The models met established cut-offs for model adequacy, with the APPA ranging between 0.75 to 0.94 for boys and 0.74 to 0.91 for girls, indicating that the model had good assignment accuracy and provided an adequate fit to the data. OCC ranged between 3.09 and 506.56 for the boys’ model and between 4.13 and 449.48 for the girls’ model with means of 131.5 and 116, respectively (Table 1).
Validation of chosen model: Group membership probabilities and OCC for 6 group-based latent trajectories of psychopathology in 49,361 participants from the Danish National Birth Cohort

Average probability/posterior of group membership (i.e., the probability that a specific participant belongs to the trajectory group) greater than 70% and OCC greater than 5 represents a good model fit.
We identified six distinct trajectories characterized by diagnostic patterns and the timing of psychopathology or its absence. For clarity and communication, we assigned descriptive labels to these trajectories, serving as practical references. The trajectory names and detailed descriptions are presented in Table 2. Only one of the trajectories differed substantially between boys and girls, requiring distinct labelling (Boys: ‘Early Behavioural Difficulties’, girls: ‘Non-clinical Behavioural Difficulties’). The estimated trajectories for psychopathological difficulties during childhood and adolescence are presented in Table 2, Figures 2 and 3.
Boys’ psychopathological trajectories in the Danish National Birth Cohort based on reported emotional and behavioural problems (SDQ) and register information on psychiatric diagnoses and psychotropic medication prescriptions obtained from a sample of 23 361.

Girls’ psychopathological trajectories in the Danish National Birth Cohort based on reported emotional and behavioural problems (SDQ) and register information on psychiatric diagnoses and psychotropic medication prescriptions obtained from a sample of 26 000.

Labels, characteristics and percentages of the six trajectory groups

Around three out of four children (78.3% boys and 69.1% girls) belonged to the ‘No Significant Problems’ or the ‘Minimal Difficulties’ trajectories. The children belonging to the ‘No Significant Problems’ or the ‘Minimal Difficulties’ trajectories had very few emotional and behavioural difficulties and almost no diagnoses. Children belonging to the ‘Adolescent-specific Psychopathology’ or the ‘Neurodiverse’ trajectories received neurodevelopmental, affective and mixed diagnoses, so diagnoses from one dimension did not eliminate diagnoses from another dimension. Across ages, most trajectories showed similar trends in emotional and behavioural difficulties, i.e., we observed the same trend over time. Additionally, some of the trajectories had similar emotional and behavioural difficulties courses, e.g., the ‘Neurodiverse’ and ‘Early Behavioural Difficulties’ trajectories for the boys and the ‘Neurodiverse’ and ‘Non-clinical Behavioural Difficulties’ for girls, but with considerably different diagnostic and prescription patterns.
We observed substantial differences in the distribution of maternal age, education level, parental psychiatric diagnoses, symptoms of infant colic, marital status, alcohol consumption during pregnancy and size for gestational age between children with ‘No Significant Problems’ and children of all other trajectories (Supplementary Table S8). The children with ‘No Significant Problems’ were more likely to be born into a household with higher maternal age and education, as well as fewer psychiatric diagnoses. These children also displayed fewer signs of colic as infants and were not as often born small for gestational age. We observed small differences in the characteristics of two trajectories that showed similar emotional and behavioural patterns but did not receive psychiatric diagnoses and redeemed medication to the same extent: the ‘Neurodiverse’ trajectory to the ‘Early Behavioural Difficulties’ (for boys) or ‘Non-clinical Behavioural Difficulties’ (for girls) trajectory. These trajectories differed in that the children in the ‘Neurodiverse’ trajectory, in general, came from families who had higher rates of parental psychiatric disorders compared to the ‘Early Behavioural Difficulties’/‘Non-clinical Behavioural Difficulties’. In addition to potential socioeconomic inequalities, this may also reflect greater awareness and help-seeking among parents with psychiatric diagnoses, potentially contributing to earlier assessment and higher rates of diagnoses in this group.
Discussion
We identified six trajectories reflecting distinct developmental patterns of emotional and behavioural difficulties, psychiatric diagnoses and psychotropic medication use across childhood and adolescence characterized by different developmental patterns across childhood and adolescence. Differences between trajectories were apparent from early childhood and became more pronounced over time. We observed that a small group of children, 6% of boys and 8% of girls (‘Adolescent-specific Psychopathology’ and ‘Neurodiverse’), had the highest burden of registered psychiatric diagnoses and psychotropic medication use over time. Although several trajectories showed elevated emotional and behavioural difficulties, these two groups were primarily distinguished by sustained contact with psychiatric treatment rather than high SDQ scores alone. This is a key strength of the study, as trajectories were identified using both symptom questionnaires and registry data, extending beyond approaches based solely on self- or parent-reported measures (Reef et al., Reference Reef, Diamantopoulou, Van Meurs, Verhulst and Van Der Ende2011; Stepp et al., Reference Stepp, Burke, Hipwell and Loeber2012; Harold et al., Reference Harold, Leve, Kim, Mahedy, Gaysina, Thapar and Collishaw2014; Lancefield et al., Reference Lancefield, Raudino, Downs and Laurens2016; de Lijster et al., Reference de Lijster, van den Dries, van der Ende, Utens, Jaddoe, Dieleman, Hillegers, Tiemeier and Legerstee2019; Weavers et al., Reference Weavers, Heron, Thapar, Stephens, Lennon, Bevan Jones, Eyre, Anney, Collishaw, Thapar and Rice2021). Two trajectories showed substantial difficulties without any contact with psychiatric healthcare services, as indicated by the absence of diagnoses or prescribed medication, characterized either by emotional and behavioural difficulties from early childhood or by rising emotional and behavioural problems in adolescence. It remains unclear whether these trajectories reflect sub-diagnostic levels of difficulties or unmet needs among children not identified by services.
We observed various combinations of diagnostic patterns and timing across trajectories. Rather than showing clear evidence of heterotypic continuity, our findings indicate increasing comorbidity over time: difficulties in one domain tended to co-occur with difficulties in other domains within trajectories characterized by adverse psychopathology. For instance, neurodevelopmental diagnoses generally stabilized over time, as shown by others (Solmi et al., Reference Solmi, Radua, Olivola, Croce, Soardo, Salazar de Pablo, Il Shin, Kirkbride, Jones, Kim, Kim, Carvalho, Seeman, Correll and Fusar-Poli2021), whereas affective and mixed diagnoses increased with age, especially in the ‘Neurodiverse’ trajectory. This pattern aligns with previous studies reporting high levels of psychiatric comorbidity across development (Plana-Ripoll et al., Reference Plana-Ripoll, Pedersen, Holtz, Benros, Dalsgaard, de Jonge, Fan, Degenhardt, Ganna, Greve, Gunn, Iburg, Kessing, Lee, Lim, Mors, Nordentoft, Prior, Roest, Saha, Schork, Scott, Scott, Stedman, Sørensen, Werge, Whiteford, Laursen, Agerbo, Kessler, Mortensen and McGrath2019; Caspi et al., Reference Caspi, Houts, Ambler, Danese, Elliott, Hariri, Harrington, Hogan, Poulton, Ramrakha, Rasmussen, Reuben, Richmond-Rakerd, Sugden, Wertz, Williams and Moffitt2020; Watkeys et al., Reference Watkeys, O’Hare, Dean, Laurens, Tzoumakis, Harris Maclinepi, Carr and Green2024, Reference Watkeys, Tzoumakis, Dean, Laurens, Harris, O’Hare, Carr and Green2025b; Krantz et al., Reference Krantz, Dalsgaard, Osler, Jorgensen, Jorgensen and Jørgensen2025).
We observed that emotional and behavioural difficulties measured on the SDQ may be present without a (registered) associated diagnosis or psychotropic medication. This supports the view that the population burden of mental health problems in children and adolescents substantially exceeds the proportion who receive a formal psychiatric diagnosis through public services, highlighting a ‘hidden’ group who may manage difficulties outside the public psychiatric system, either intentionally or unintentionally, in line with previous work (McGorry et al., Reference McGorry, Mei, Dalal, Alvarez-Jimenez, Blakemore, Browne, Dooley, Hickie, Jones, McDaid, Mihalopoulos, Wood, El Azzouzi, Fazio, Gow, Hanjabam, Hayes, Morris, Pang, Paramasivam, Quagliato Nogueira, Tan, Adelsheim, Broome, Cannon, Chanen, Chen, Danese, Davis, Ford, Gonsalves, Hamilton, Henderson, John, Kay-Lambkin, Le, Kieling, Mac Dhonnagáin, Malla, Nieman, Rickwood, Robinson, Shah, Singh, Soosay, Tee, Twenge, Valmaggia, Van Amelsvoort, Verma, Wilson, Yung, Iyer and Killackey2024).
We initially aimed to categorize diagnoses into externalizing and internalizing groups, reflecting the SDQ subscales. However, to ensure greater clinical translation, and following clinician advice, we chose to use the grouping of neurodevelopmental and affective disorders instead. While we recognize that externalizing disorders, such as conduct and oppositional behaviours, are widely acknowledged as important in characterizing childhood psychopathology and its progression (Speranza et al., Reference Speranza, Liotti, Spoletini and Fortunato2023; Watkeys et al., Reference Watkeys, Tzoumakis, Dean, Laurens, Harris, O’Hare, Carr and Green2025b), we prioritized a classification that better aligns with clinical diagnostic practices. This decision reflects a practical focus, though we acknowledge that other studies have taken alternative approaches.
Up to 13% (15% in Denmark (Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020)) of all children and adolescents are diagnosed with at least one mental disorder before reaching 18 years of age (Polanczyk et al., Reference Polanczyk, Salum, Sugaya, Caye and Rohde2015) and with evident trends across period and birth cohorts (Momen et al., Reference Momen, Beck, Lousdal, Agerbo, McGrath, Pedersen, Nordentoft and Plana-Ripoll2025). In our study, we were able to identify approximately half of this group, around 6% of boys and 8% of girls, who had multiple and persistent mental health problems throughout childhood and adolescence. This distinction highlights that our study focuses on those with more consistent and diverse mental health difficulties rather than all individuals who have ever received a diagnosis.
Previous studies show that the DNBC under-represents individuals with lower socioeconomic status and childhood psychiatric diagnoses, while loss to follow-up further reduces the sample (Jacobsen et al., Reference Jacobsen, Nohr and Frydenberg2010; Howe et al., Reference Howe, Cole, Lau, Napravnik and Eron2016; Madsen et al., Reference Madsen, Hohwü, Zhu, Olsen and Obel2020). As the participants are generally healthier and more advantaged, the findings may have limited generalizability to under-represented groups. We applied weighting (i.e., cloning) to minimize this issue (Petersen et al., Reference Petersen, Jørgensen, Mathisen, Osler, Mortensen, Molbo, Hougaard, Lange and Lund2024)
The trajectories for boys and girls were generally comparable with a few exceptions: We found a male trajectory (‘Early Behavioural Difficulties’), which received neurodevelopmental and mixed diagnoses in pre-adolescence accompanied by high levels of emotional and behavioural difficulties. Both their emotional and behavioural difficulties scores and the number of diagnoses decreased in mid-childhood. The closest parallel female trajectory (‘Non-clinical Behavioural Problems’) has persistently high emotional and behavioural problem scores, but no psychiatric diagnoses. This suggests that a male trajectory exists with possible transient mental health problems, with no parallel female trajectory. In contrast, the ‘Neurodiverse’ trajectory shows a very different prescription pattern between girls and boys, with boys’ prescriptions peaking and falling around age 14, whereas girls’ prescriptions continue to rise, accompanied by a rise in affective diagnoses only observed in girls at this age.
Irritability or emotional dysregulation are features of affective disorders in children and adolescents, perhaps linked with unrecognized neurodevelopmental diagnoses (Eyre et al., Reference Eyre, Hughes, Thapar, Leibenluft, Stringaris, Davey Smith, Stergiakouli, Collishaw and Thapar2019). This aligns with the increase in affective disorders we observe from pre-adolescence among girls in the ‘Neurodiverse’ trajectory. Difficulties related to an underlying psychiatric condition may also explain the delayed onset of affective disorders, often co-occurring with neurodevelopmental diagnoses in boys belonging to the ‘Adolescent-specific psychopathology’ trajectory. The identified trajectories likewise concur with previous longitudinal studies showing that the peak age of diagnosis of neurodevelopmental disorders is earlier among boys than girls, and that affective diagnoses are more common and diagnosed later among girls compared to boys (Dalsgaard et al., Reference Dalsgaard, Thorsteinsson, Trabjerg, Schullehner, Plana-Ripoll, Brikell, Wimberley, Thygesen, Madsen, Timmerman, Schendel, McGrath, Mortensen and Pedersen2020). Children in the ‘Neurodiverse’ trajectory received most of the diagnoses and psychotropic prescriptions. This trajectory was also the one with the highest proportion of parents with a registered psychiatric diagnosis. Social inequality and mental health are strongly associated (Fryers et al., Reference Fryers, Melzer and Jenkins2003), so it was not surprising that we found that the parents of children in the ‘Neurodiverse’ trajectory had the lowest educational level and more often lived without a partner. It was, however, unexpected to find two trajectories with similarly increased emotional and behavioural problem scores (Early Behavioural Problems and Neurodiverse for boys/Non-clinical Behavioural Problems and Neurodiverse for girls), but with only one of them receiving psychiatric diagnoses and redeeming psychotropic medication prescriptions. While the overall differences between these two trajectories are small, children who receive a diagnosis are more likely to have parents with psychiatric diagnoses. These patterns could be explored in more detail by sex to determine whether clearer differences emerge.
The identification of the trajectories is dependent on the way diagnoses are registered in datasets. Children’s psychiatric diagnoses are only traceable in our data through hospital contacts. Although research suggests that most individuals with ADHD do not fully recover from the condition (Ismail and Shapiro, Reference Ismail and Shapiro2019), we can only track the psychiatric diagnoses of children and adolescents as long as they received some kind of management in a hospital setting. However, this does not necessarily mean that their psychiatric conditions have resolved. The trajectories are also a product of our categorization of each diagnosis and the dimensions required to perform the group-based multi-trajectory model.
Our study has some major strengths: The modelling of trajectories from infancy to late adolescence was based on a unique combination of questionnaire‐based reporting of emotional and behavioural difficulties, clinically registered psychiatric diagnoses and prescriptions in an exceptionally large cohort. Linking our cohort data to register data enabled us to weight our GBMTM analyses, thereby limiting bias due to the inevitable selective attrition.
This study also has some limitations. We have given an overview of how both diagnosed neurodevelopmental, affective and mixed diagnoses develop during childhood and adolescence, so trajectories of specific psychiatric diagnoses, such as autism, or small variations within dimensions would not be clear from our study. The limit of six dimensions precluded us from including SDQ pro-social scale scores as well as specific psychotropic medications. SDQ reports came from different informants over time, which was not accounted for in the analysis. Ideally, data from multiple respondents at each time point would have been used (Bergström and Baviskar, Reference Bergström and Baviskar2021), although this was not feasible. Likewise, we were unable to account directly for changes in diagnostic and prescription patterns during the examined period caused, for example, by overall rates of psychotropic medication use among individuals with autism spectrum disorder increasing over time (Rasmussen et al., Reference Rasmussen, Bilenberg, Thomsen Ernst, Abitz Boysen and Pottegård2018). Furthermore, psychiatric diagnoses from private practice psychiatrists and GPs were not included in our data (Mors et al., Reference Mors, Perto and Mortensen2011; Madsen et al., Reference Madsen, Ersbøll, Olsen, Parner and Obel2015); thus, our outcome measure will capture the more severe cases of psychopathology. This might exclude some children with mild symptoms treated by GPs without a registered diagnosis or children treated elsewhere, which may affect the external validity of our results. Before 2012, GPs could prescribe these medications independently, but subsequently, psychiatrists in Denmark were required to initiate treatment for those under 18 (The Ministry of the Interior and Health, Denmark, 2012). We included children diagnosed by private psychiatrists who were prescribed psychotropic medication by including data on psychotropic prescriptions; however, only allowing one annual count could have impacted our findings.
Our findings demonstrate that 6–8% of children/adolescents have substantial persistent mental health difficulties and utilize mental health services. Two of the trajectories experience similar emotional and behavioural difficulties, but children in only one of these trajectories receive psychiatric treatment, specifically those who are characterized by a higher burden of recorded familial psychiatric diagnoses. Future studies should extend our work by examining how the trajectories are associated with general well-being, mental health, educational attainment and social status later in life. Factors associated with resilience to adverse outcomes could also be examined. Finally, research that aims to find early predictors of the membership of different trajectories is desirable to identify children at risk of mental health problems at an early stage.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796026100596.
Availability of data and materials
This study is based on data from the Danish National Birth Cohort. Researchers can apply for the use of these data at http://www.dnbc.dk. The data analysis was performed using SAS 9.4 using proc traj. The code utilized in this study corresponds to the code provided in the proc traj statement. It has been sourced from the official public repository, accessible at https://www.andrew.cmu.edu/user/bjones/index.htm, ensuring fidelity to the original methodology and implementation. Figures were created in R.
Acknowledgements
This study was a part of a PhD fellowship that was supported by TRYGfonden (grant number 125227) and Lilly & Herbert Hansen’s foundation (Jr. No. 0156). The DNBC was established with a significant grant from the Danish National Research Foundation. Additional support was obtained from the Danish Regional Committees, the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Health Foundation and other minor grants. The DNBC Biobank has been supported by the Novo Nordisk Foundation and the Lundbeck Foundation. Follow-up of mothers and children has been supported by the Danish Medical Research Council (SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B), the Lundbeck Foundation (195/04, R100-A9193), The Innovation Fund Denmark 0603-00294B (09-067124), the Nordea Foundation (02-2013-2014), Aarhus Ideas (AU R9-A959-13-S804), University of Copenhagen Strategic Grant (IFSV 2012) and the Danish Council for Independent Research (DFF – 4183-00594 and DFF – 4183-00152).
We would like to thank Jakob Kragstrup for providing valuable feedback on the manuscript, which helped to clearly highlight the importance and relevance of this paper.
Financial support
This research was funded by TRYG-foundation (grant number 125227) and Lilly & Herbert Hansen’s foundation (Jr. No. 0156). The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the study.
Competing interests
There are no competing interests to declare.
Ethical standards
The Committee on Biomedical Research Ethics approved the DNBC, and all women who participated in the study gave informed written consent. The participants born into DNBC were informed about their participation, rights and how to drop out when turning 18 years old. This study was approved by the DNBC steering committee (ref. 2020-06).







 Open access
Open access