


Introduction
Globally, child mortality has declined appreciably since 1990, however, geographic disparities exist (Liu et al., Reference Liu, Oza, Hogan, Chu, Perin, Zhu and Black2016; Taylor et al., Reference Taylor, Blau, Bassat, Onyango, Kotloff, Arifeen and Winchell2020). It remains heavily concentrated in sub-Saharan Africa (SSA), where children are between six and 15 times more likely to die compared to children in more developed regions (Sharrow et al., Reference Sharrow, Hug, You, Alkema, Black, Cousens, Croft, Gaigbe-Togbe, Gerland, Guillot and Hill2022). In 2019, the child mortality rate in the SSA stood at 76 per 1,000 live births, translating into approximately one in 13 children dying before age five (UNICEF & World Health Organization, 2020). Numerous studies have attributed child mortality to preventable causes such as diarrhoea, pneumonia, malaria, and poor nutrition, which can be avoided if health systems invest in a few effective interventions (Bryce, Reference Bryce, el Arifeen, Pariyo, Lanata, Gwatkin and Habicht2003; Vaivada et al., Reference Vaivada, Lassi, Irfan, Salam, Das, Oh and Bhutta2022). As SSA governments have scaled up such interventions (Gera et al., Reference Gera, Shah, Garner, Richardson and Sachdev2016), observers have pointed out the lack of commensurate and sufficient attention toward family planning (Jacobstein et al., Reference Jacobstein, Bakamjian, Pile and Wickstrom2009; May, Reference May2017; Dodson et al., Reference Dodson, Dérer, Cafaro and Götmark2022; Sully et al. Reference Sully, Shiferaw, Seme, Bell and Giorgio2022). This is despite recommendations that contraception is a cost-effective and high-yield intervention to improve child survival (The World Health Organization, 2013; World Health Organization, 2007).
Guidance on the benefits of family planning for children is based on findings that intervals shorter than 36 months and longer than 59 months are associated with elevated risks of child mortality and other adverse outcomes (Hobcraft et al., Reference Hobcraft, McDonald and Rutstein1985; Cleland et al., Reference Cleland, Conde-Agudelo, Peterson, Ross and Tsui2012; Conde-Agudelo et al., Reference Conde-Agudelo, Rosas-Bermudez, Castaño and Norton2012). In general, findings on the birth spacing-child mortality relationship have been consistent, with research having demonstrated it in a variety of developmental and geographic contexts over decades (Cleland & Sathar, Reference Cleland and Sathar1984; Miller et al., Reference Miller, Trussell, Pebley and Vaughan1992; Curtis et al., Reference Curtis, Diamond and McDonald1993; Ronsmans, Reference Ronsmans1996; Whitworth and Stephenson, Reference Whitworth and Stephenson2002; Becher et al., Reference Becher, Müller, Jahn, Gbangou, Kynast-Wolf and Kouyaté2004; Fotso et al., Reference Fotso, Cleland, Mberu, Mutua and Elungata2013; Molitoris, Reference Molitoris2017). Most of these investigations have focused on the effects of children’s preceding birth intervals (PBI) (e.g., Rutstein, Reference Rutstein2005; Islam et al., Reference Islam, Billah, Islam, Rahman and Khan2022). In 2008, Rutstein et al. pooled data on over one million births from 52 Demographic and Health Surveys and conducted analyses, which reported that PBI less than 24 months was associated with a 60% increase in mortality risk during infancy, while those between 24 and 36 months face a 10% increase, compared to those born after intervals of four years (Rutstein, Reference Rutstein2008). The effects of short subsequent birth intervals (SBI) have received less attention. This is so, in part, because of the need to circumvent the challenge of reverse causality, which may arise if the death of a child is the cause rather than the outcome of a short SBI. However, large cross-national studies have found that short SBI are associated with a two-fold risk of death between the ages one and two and smaller effects during late childhood (Hobcraft et al., Reference Hobcraft, McDonald and Rutstein1985). Koenig et al. (Reference Koenig, Phillips, Campbell and D’Souza1990) reported that for mortality during children’s second and third year, risks decline systematically with longer SBI (Koenig et al., Reference Koenig, Phillips, Campbell and D’Souza1990).
Despite the evidence base, there remains a tendency to overlook family planning as a strategy to prevent child deaths, particularly in SSA. This has been attributed to attitudes of African policymakers, the influence of donors and competing priorities, and challenges inherent in evaluating family planning programmes (May, Reference May2017). In addition, research findings on the birth spacing-child mortality relationship still elicit a degree of doubt (Klebanoff, Reference Klebanoff2017). This paper first reviews grounds for such scepticism and then presents an analysis of data compiled in rural Tanzania between 2000 and 2015 that assesses whether SBI and PBI durations are associated with childhood mortality.
Birth interval duration and child mortality: mechanisms and measurement
Over time, researchers have questioned explanations for the adverse consequences of a short birth spacing for child survival. These explanations have centred on three causal mechanisms: biological effects related to the ‘maternal depletion syndrome’, behavioural effects that arise from competition between closely spaced siblings, and disease transmission in overcrowded households (Palloni and Tienda, Reference Palloni and Tienda1986; Winikoff and Castle, Reference Winikoff, Castle, Winikoff and Castle1987; Whitworth and Stephenson, Reference Whitworth and Stephenson2002). The maternal depletion syndrome refers to a pattern of closely spaced pregnancies that provides inadequate time for the mother to fully recover from the physiological and nutritional demands of childbearing, delivery, and breastfeeding (Zhu et al., Reference Zhu, Rolfs, Nangle and Horan1999). Under such circumstances, an inhospitable intrauterine environment in the succeeding pregnancy may increase the likelihood of child loss. Although this relationship is buttressed by strong empirical support from studies in both high- and low-income countries (Conde-Agudelo et al., Reference Conde-Agudelo, Rosas-Bermúdez and Kafury-Goeta2006; Davanzo et al., Reference Davanzo, Hale, Razzaque and Rahman2008), studies from high-income countries (Sweden, Australia, and Canada) have called it into question. These drew upon longitudinal datasets and a case-cross over design in which intervals with adverse outcomes were compared against other birth intervals from the same mother that did not have adverse outcomes (Ball et al., Reference Ball, Pereira, Jacoby, de Klerk and Stanley2014; Class et al., Reference Class, Rickert, Oberg, Sujan, Almqvist, Larsson and D’Onofrio2017; Erickson and Bjerkedal Reference Erickson and Bjerkedal1978; Hanley et al., Reference Hanley, Hutcheon, Kinniburgh and Lee2017). Although these analyses found no association between short PBI and child health, they could not adjust for unmeasured factors that change between pregnancies, had limited sample sizes, and took place in wealthy countries. Sibling competition rests on the hypothesis that, in settings of scarce resources, close spacing produces conditions in which one child is prone to suffer from limited investments in food, care, and nutrition. Research on this mechanism has taken place in low-income contexts and suggested that this tendency is less influential than prenatal factors (Boerma and Bicego, Reference Boerma and Bicego1992). Other studies in low-income environments have suggested that closely spaced births may contribute to overcrowding and, thereby, help facilitate the transmission of infectious disease (Aaby, Reference Aaby1988).
Sceptics have raised concerns regarding common causes that might give rise to both short intervals and child mortality. A salient example of one such common cause is truncated breastfeeding, which deprives an infant of crucial nutrients and accelerates mothers’ return to fertility after giving birth (Molitoris, Reference Molitoris2018a). However, studies that controlled for breastfeeding durations found that the link between short intervals and child mortality persisted (Kuate Defo, Reference Kuate Defo1997; Manda, Reference Manda1999; Retherford et al., Reference Retherford, Choe, Thapa and Gubhaju1989). High-income country studies, such as those mentioned above from Sweden, Australia, and Canada, have suggested that endogeneity due to residual confounding of unobservable maternal and household characteristics has biased estimates of the ‘birth spacing-mortality’ association. In response, Molitoris (Reference Molitoris2017, Reference Molitoris2018b) employed the same statistical approaches using data from 19th-century Sweden and contemporary Bangladesh and found that shorter birth intervals increased the risk of childhood mortality (Molitoris, Reference Molitoris2017, Reference Molitoris2018b). Other studies which employed a ‘within family’ fixed effects approach found that associations between birth intervals and mortality remained (Mayo et al., Reference Mayo, Shachar, Stevenson and Shaw2017; Shachar et al., Reference Shachar, Mayo, Lyell, Baer, Jeliffe-Pawlowski, Stevenson and Shaw2016). Other studies have addressed the endogenous effects of mother-specific factors through random-effects models, showing that it makes little difference for the association of interest (Curtis et al., Reference Curtis, Diamond and McDonald1993; Whitworth and Stephenson, Reference Whitworth and Stephenson2002). Kozuki and Walker (Reference Walker2013) used 47 Demographic and Health Survey (DHS) datasets to examine the effect of PBI length on neonatal and child deaths employing conditional logistic regression. This study reproduced findings reported that shorter birth intervals are associated with higher child mortality, but that negative impacts may only occur in high parity births (Kozuki and Walker, Reference Walker2013). Kravdal (Reference Kravdal2018) addressed the same challenge by fitting multilevel-multiprocess models that control for time-invariant observed mother-level characteristics using DHS data from 28 countries in SSA. This analysis concluded that avoiding a short birth interval reduces the risk that an index child will die, but that the effect is weaker than suggested by simpler models (Kravdal, Reference Kravdal2018). Finally, Molitoris (Reference Molitoris2019) controlled for unobserved heterogeneity by estimating within-family linear probability models on 4.5 million births from 77 countries captured in 207 DHS datasets. This study reported that intervals shorter than 36 months increased the probability of infant death, however, this relationship varies regionally, with adverse effects concentrated in settings at low levels of development (Molitoris et al., Reference Molitoris, Barclay and Kolk2019).
Doubts about the benefits of birth spacing for children also relate to studies’ disproportionate dependence on retrospective surveys. For example, of the 65 studies highlighted in the influential systematic review of Rutstein (Reference Rutstein2005), 62 used data from birth histories from the DHS, which are vulnerable to biases that stem from the omission of dead children and misdating of births (Potter, Reference Potter1988; Pullum, Reference Pullum2006; Rutstein, Reference Rutstein2005). Fotso and colleagues (Reference Fotso, Cleland, Mberu, Mutua and Elungata2013) reported on an extension of this systematic review in which they relaxed eligibility criteria to allow consideration of 18 additional studies that used registration, prospective cohort, or demographic surveillance data. Of these, only four were conducted in SSA and all before 2000. Doyle et al. (Reference Doyle, Morley, Woodland and Cole1978) found no significant difference between the mean PBI of index children in western Nigeria who died and those who survived (Doyle et al., Reference Doyle, Morley, Woodland and Cole1978). A study using prospective data from 1974–1981 in rural Kenya reported no effect of a short PBI on index children’s survival and could not establish effects of SBI (Boerma and van Vianen, Reference Boerma and van Vianen1984). Ronsmans (Reference Ronsmans1996) utilised longitudinal data on children born in rural Senegal between 1983 and 1989. Results indicated that PBI of less than one year were associated with higher risk of neonatal and post-neonatal mortality, that PBI between one and two years had no effect, and that children with SBI less than two years faced mortality risks that were four-fold higher than their counterparts with longer SBI (Ronsmans, Reference Ronsmans1996). A fourth study used surveillance data from Burkina Faso compiled between 1992 and 1999 and found that PBI of less than 18 months raised the risk of infant mortality by 36% but had no effect later in childhood, and that SBI of less than 18 months was associated with a 1.5 times higher risk of mortality between ages one and five (Becher et al., Reference Becher, Müller, Jahn, Gbangou, Kynast-Wolf and Kouyaté2004). Fotso and colleagues (Reference Fotso, Cleland, Mberu, Mutua and Elungata2013) analysed data on 13,502 births from 2003 to 2009 compiled by the Nairobi Urban Health and Demographic Surveillance System. Their study reports that a PBI less than 18 months is associated with a two-fold of infant mortality risks, while a PBI between 18 and 23 months increases this risk by 18%, and that children born within 18 months of an elder sibling are more than twice as likely to die between ages one and two (Fotso et al., Reference Fotso, Cleland, Mberu, Mutua and Elungata2013).
Three conclusions can be drawn from this review of the literature. Despite debates over the mechanisms through which birth interval spacing affects child survival, a considerable and methodologically diverse body of evidence points to a strong relationship, especially in low-income country settings. Second, this finding is overwhelmingly reliant on retrospective data, and while the few longitudinal analyses generally corroborate findings of an association, their results are not consistent. Third, longitudinal investigations of the child mortality response to birth spacing in SSA are few, mostly dated and were conducted in West African countries. Though Fotso and colleagues fill this gap, their study was situated in urban Nairobi in the 2000s, where total fertility rates were between 2.6 and 2.8 births per woman of reproductive age (Kenya National Bureau of Statistics & ICF Macro, 2010). These are appreciably lower than fertility levels in rural parts of East Africa, where approximately 80% of the population in the region resided during that period (Kamer, Reference Kamer2022). For example, in the study areas in rural Tanzania during this time, fertility rates stagnated between 5.5 and 5.0 (Sheff et al., Reference Sheff, Jackson, Kanté, Rusibamayila and Phillips2019). These observations gave impetus for this paper.
Study hypotheses
This study drew upon longitudinal data on the reproductive and child survival trajectories of mothers and childred in three rural districts of Tanzania and evaluated the effect of PBI and SBI durations on the survival of more than 25,000 children born between 2000 and 2015. It was first hypothesised that relatively short SBI and PBI would be associated with heightened risks of child mortality; however, the effects of short SBI would be most pronounced among children between 12 and 59 months of age, whereas the effects of short PBI would be most acute during the neonatal and post-neonatal period. The analysis then sought to determine whether the mortality responses to birth spacing were moderated by certain influences: children’s year of birth, maternal age, household socio-economic status, and birth parity. This analysis was guided by the secondary hypotheses that the protective effect of birth spacing would be most pronounced among children most exposed to these risk factors, that is, among children born during early years of the cohort and before large investments in child mortality reduction interventions, those born to adolescent mothers, those born in relatively poor households, and children whose births were high parity. The results of this secondary analysis are presented in Appendix C.
Methods
Data and setting
The data for this study came from the Ifakara and Rufiji Health and Demographic Surveillance Systems (HDSS) in Morogoro and Pwani regions of Tanzania (Geubbels et al., Reference Geubbels, Amri, Levira, Schellenberg, Masanja and Nathan2015; Mrema et al., Reference Mrema, Kante, Levira, Mono, Irema, De Savigny and Masanja2015). In 2011, the Ifakara HDSS covered approximately 238,000 people in 68 communities of Kilombero and Ulanga districts. The Rufiji HDSS covered approximately 124,000 residents of 33 communities. Between 2000 and 2015, both HDSS collected birth, death, migration, and marriage data continuously in all households through visits conducted in four-month intervals from 2000 to 2012, and six-month intervals subsequently. In biennial intervals, censuses were conducted to enumerate old and new households, validate data on new household formation, and update data on socio-demographic characteristics of households.
This study analysed HDSS data compiled from 2000 to 2015, a period during which child mortality in the study population declined by 45% (Kanté et al., Reference Kanté, Nathan, Jackson, Levira, Helleringer, Masanja and Phillips2016). Included were prospectively recorded reproductive events experienced by women who were residents of households in the HDSS areas and were 15–18 at the onset of surveillance activities. All births were included, whether singleton or multiple births, if they were of children of HDSS-registered mothers. Data permitted calculation of person-months of observation of children who were considered recorded exits and re-entries into the sentinel population, transitions to 60 months of age as of the end of the cohort, and loss to follow-up. Data were subject to right censoring if under-five-year-old children remained active in the cohort when surveillance operations ended on December 31, 2015.
SBI and PBI were measured as the number of months between the date of birth of the index child and the date of birth of the subsequent and preceding children, respectively. In both analyses, SBI and PBI durations were represented as a five-category polytomy: first born/last born/only child (i.e., no interval of interest), and intervals less than 18 months, 18–23 months, 24–35 months, and 36 months or higher. Since this is different from the WHO recommendation of 33 months between births, this paper repeated the main effect same analysis, but using the WHO definition of short (<33 months), well-spaced (33–71 months), and widely spaced (≥72 month). The results of this analysis are reported in Appendix B. The SBI analyses addressed the potential for reverse causality by excluding observations of children whose duration in the population was shorter than the period succeeding their birth and until the birth of their next-born sibling, as suggested by an earlier analysis of this relationship that employed Bangladeshi data (Koenig et al., Reference Koenig, Phillips, Campbell and D’Souza1990). Thus, for the analysis of the effect of the SBI on mortality, the study population is smaller population (n = 23,189) than that which is used to analyse the effect of the PBI (n = 25,762).
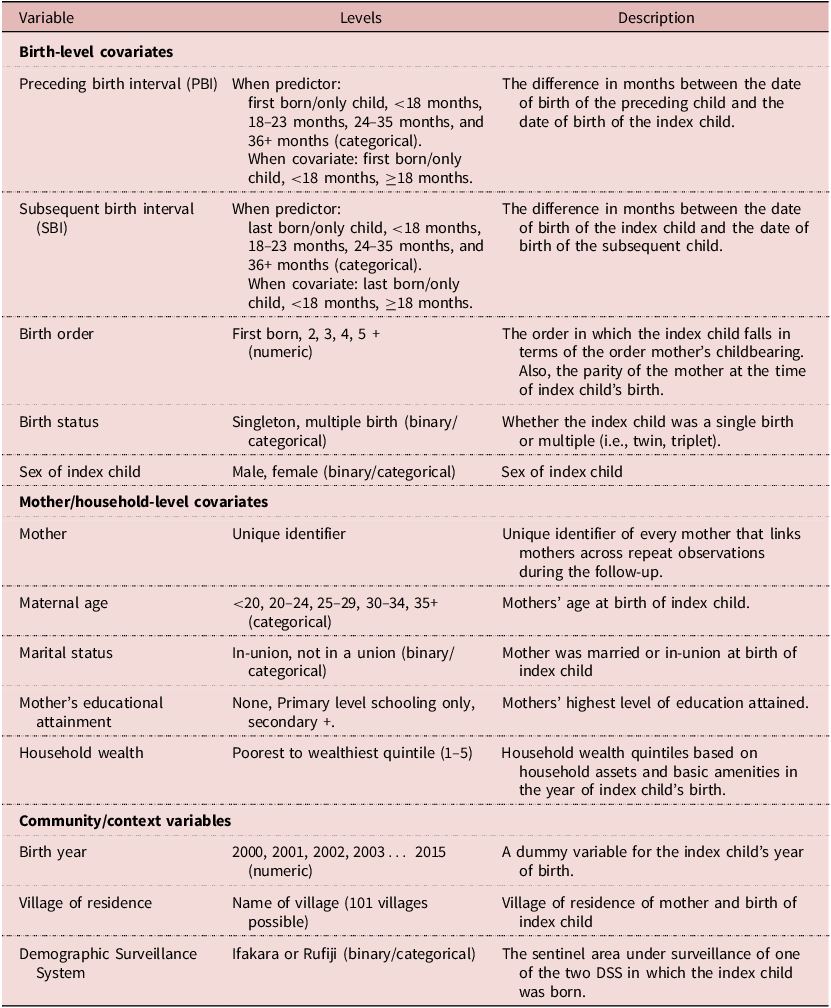
The outcomes reported by this analysis are the relative risks of childhood mortality, expressed as hazards ratios that are associated with differences in the categorical measure of the predictors. It is possible to analyse effects of differences in the categorical predictors, SBI and PBI, on mortality in the neonatal (less than one month), post-neonatal (1–11 months), early childhood (12–23 months), mid-childhood (24–35 months), and late childhood period (36–59 months). As well, it is feasible to examine these relationships in aggregated age groups such as the post-infant period (12–59 months). This examination emphasised different segments of the under-five course in its analyses of the SBI and PBI relationships, respectively. Given the need to exclude many infant deaths from the analysis of the SBI, this piece of the analysis aimed to detect potential associations between length of mothers’ SBI and the of risk early-, mid-, and late-childhood mortality, as well as all post-infant mortality. The PBI analysis assessed the main effect associations for mortality risks during all segments of child mortality described above. The covariates that were captured by the HDSS and used in the analysis were all time-invariant as they refer only to the time of children’s entry to the cohort. See Table 1. Approximately 13% of observations had missing data for household wealth status (n = 3,320) at the time of birth. It was established that the missingness was distributed at random in the study population. To avoid removing potentially valuable data, this was addressed by imputing missing values using multiple imputation through chained equations.
Description and definition of the variables used in the study

Statistical procedures
Data sets from the Ifakara and Rufiji HDSS were pooled for this analysis. First, relationships between childhood mortality and SBI and PBI lengths and other potentially confounding characteristics were analysed descriptively. Then, non-parametric Kaplan–Meier (KM) survival curves were generated to inform decision-making related to the statistical model. The initial intuition was to employ Cox proportional hazards models using death as the event of interest and the index child’s life span until age five as the duration variable that is subject to right censoring in cases where death is not observed. Such models were fit with the full set of covariates listed in Table 1 for the mortality effects of SBI and PBI, respectively. Testing these models for proportionality assumptions revealed that the full models did not meet this requirement of the semiparametric methods proposed by Cox (Abseysekera, Reference Abseysekera2009). Accordingly, the analysis employed parametric methods. This involved comparing goodness of fit between adjusted proportional hazards and accelerated failure time (AFT) models that specified different parametric distributions (Weibull, lognormal, loglogistic, exponential). Such models were fit for reporting neonatal, post-neonatal, 12–23-month and 12–59-month mortality risks that were associated with different categories of PBI and SBI. A comparison of each model based on their respective Akaike Information Criteria (AIC) found that the parametric Weibull AFT provided the best fit for the SBI and PBI models, respectively. The AFT models yielded results interpretable as the mean change in the characteristic life of the index child associated with unit differences in levels of the predictor, i.e., accelerated (or decelerated) survival time associated with alternate categories of SBI and PBI. Given the hierarchical nature of the data, a set of Weibull AFT models was estimated in which frailty terms were incorporated that specified assumed distributions of heterogeneity due to characteristics that were likely to affect the survival of subjects that were ‘clustered’ in certain groups (Kong et al., Reference Kong, Archer, Moulton, Gray and Wang2010). Specifically, models were compared that addressed clustering of births within villages, mothers, and both. AICs were compared and the decision was made to account for the effect of unobserved heterogeneity resulting from repeated observations of birth intervals in each observed reproductive history. Conditional on this random effect, and incorporating the fixed effect for the other covariates listed in Table 1, the model, which was used for the main effects analysis and corresponds to the Weibull distribution, is written as:
 $$ln(h(t/x,z)=p(t^{p-1})+\mathop{\sum}\limits_{j=1}^{J} \beta_j\; X_{ij}+\mathop{\sum}\limits_{k=1}^{K} \gamma_k Z_{ik}+ \epsilon_{ij}+\epsilon_i $$
$$ln(h(t/x,z)=p(t^{p-1})+\mathop{\sum}\limits_{j=1}^{J} \beta_j\; X_{ij}+\mathop{\sum}\limits_{k=1}^{K} \gamma_k Z_{ik}+ \epsilon_{ij}+\epsilon_i $$
Weibull regression models applied in this analysis capture the underlying hazard of child mortality that is known to be high immediately after childbirth and decline monotonically with advancing time. In this model, t is the number of days from the birth of child i to the time s/he exited the population due to death, outmigration, aging beyond five years, loss to follow-up, or right censoring at the conclusion of the cohort in 2015. The conditional hazard, h(t/ x, z), defines the risk of child mortality at time t conditional on level of the predictors on birth interval lengths, X, and birth-level, mother/household and contextual covariates Z. Weibull distribution parameter, p, defines the shape of the underlying hazard as time continues. The vector represented by X ij define the J levels of birth interval length for child i (first or last born/only child, <18 months, 18–23 months, 24–35 months, and ≥36 months), and Z ik comprises of the K characteristics of child i that are included in the model for purposes of covariate adjustment (Table 1). β has the interpretation of the ratio of the median survival times comparing different levels of birth interval durations with those classified in the reference category (<18 months), while γ means the same, however, comparing median survival times for different levels of covariates. Both β and γ are vectors of parameters to be estimated by the maximum likelihood. ε ij and ε i are error terms for the within- and between-mother effects, respectively. To assess whether the child mortality response to birth spacing is conditional on risk factors, incorporated into Equation 1 were vectors of parameters for terms representing interaction between birth interval duration categories and covariates on children’s birth year, maternal age at childbirth, household wealth status and children’s birth order, which were also estimated by the maximum likelihood.
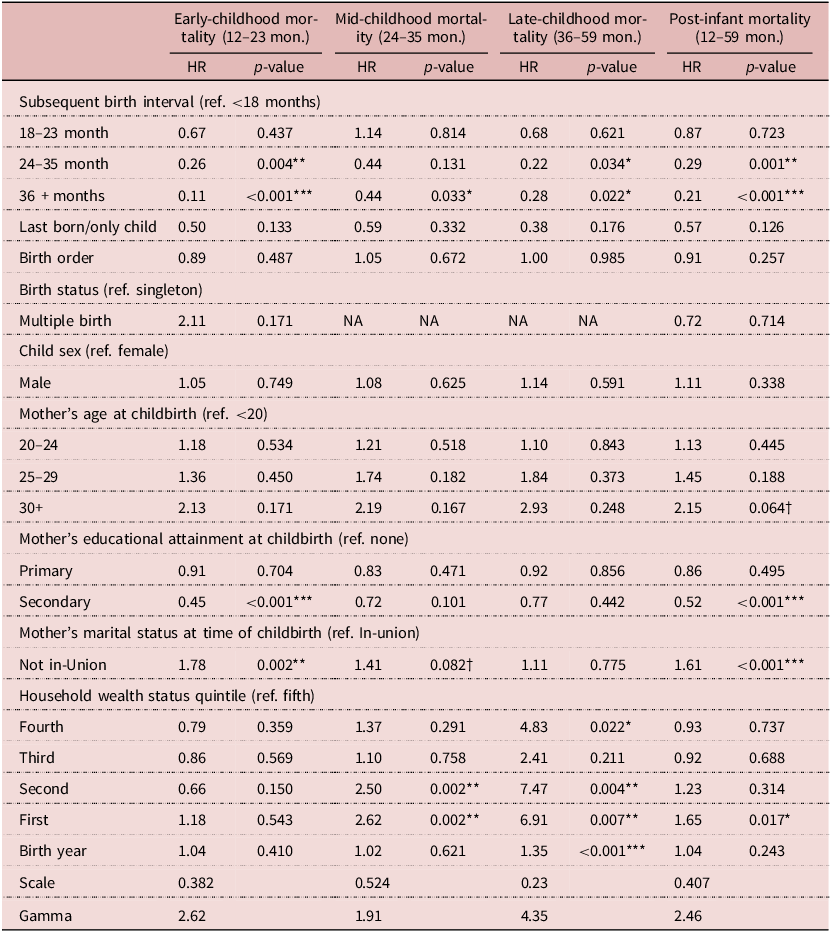
Tables 3 and 4 report the results of the main effect analyses as conversions of the raw coefficients reported by the AFT model that are rendered as the ratio of the hazards of childhood mortality for unit differences in the respective predictors. Tables 3 and 4 report the results for the effect of SBI on mortality in all segments of post-infant mortality (i.e., early childhood, mid-childhood, late childhood, and all post-infant mortality) and PBI on mortality risk in all under-five age segments.
Results of Model 1, a parametric Weibull frailty model (hazard ratios and p-values) on the effect of subsequent birth interval durations on early childhood, mid-childhood, late childhood, all post-infant mortality (n = 23,189)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
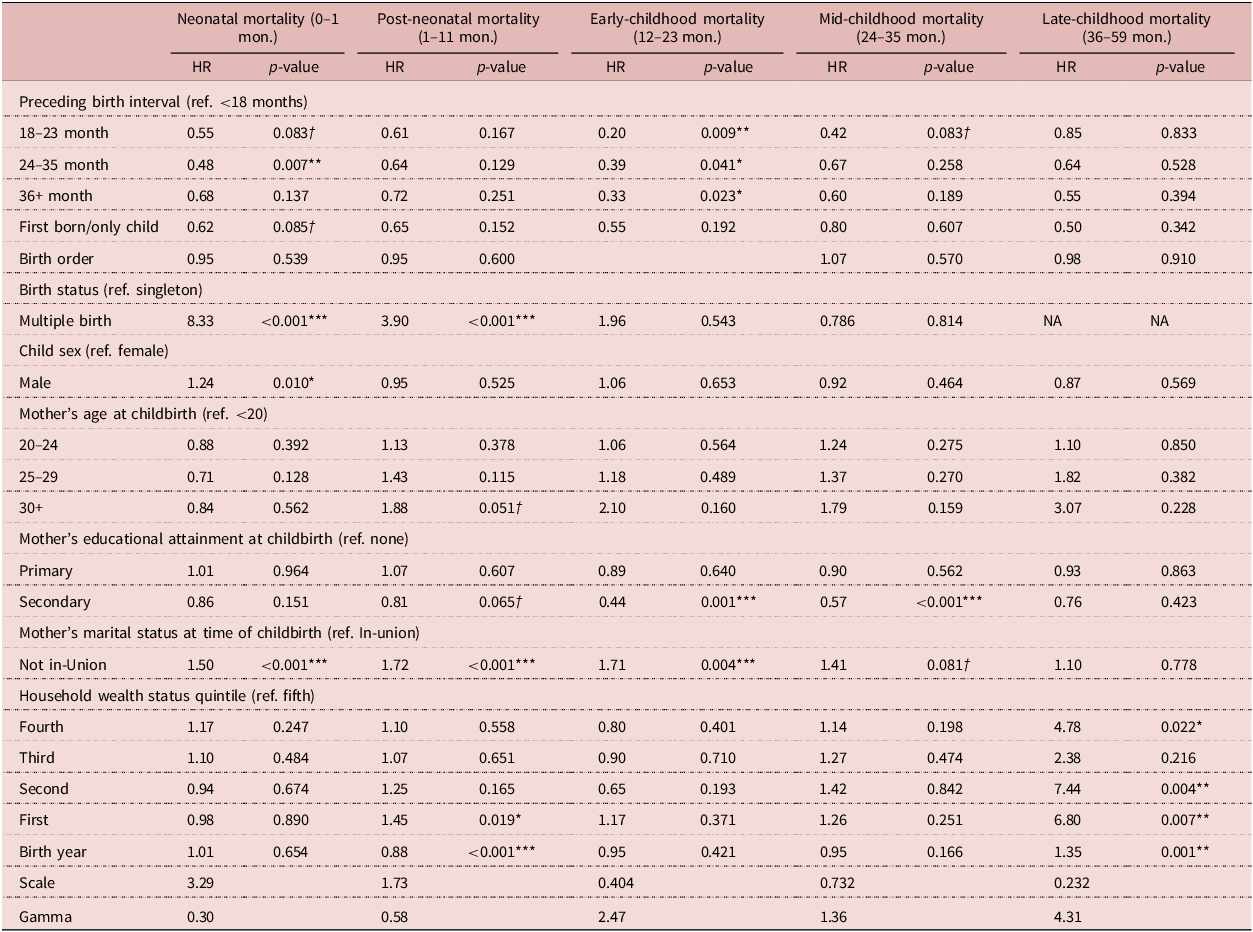
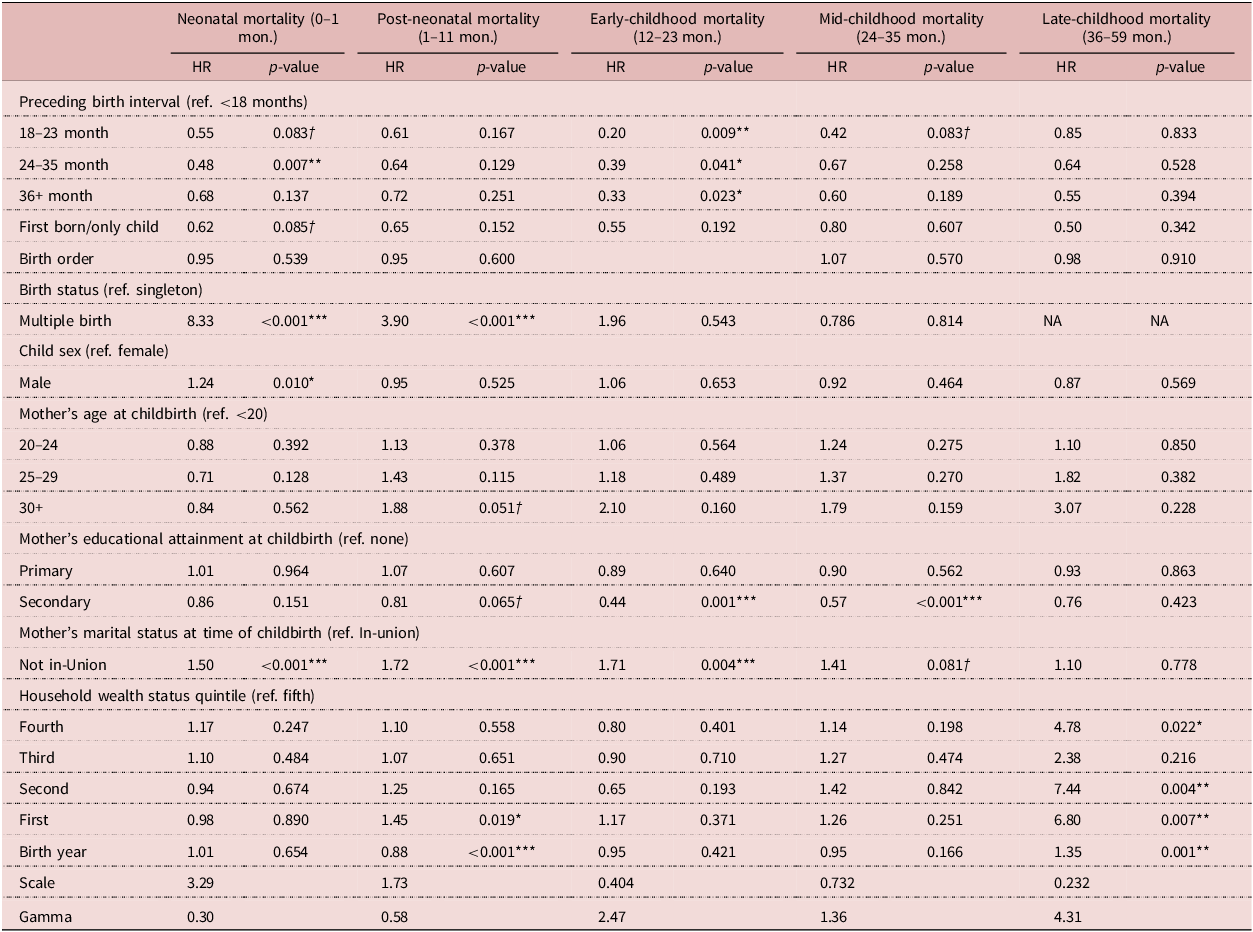
Results of Model 1, a parametric Weibull frailty model (hazard ratios and p-values) on the effect of preceding birth interval durations on neonatal, post-neonatal, early childhood, mid-childhood and late-childhood mortality (n = 25,762)
*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
For each relationship of interest, four analyses were carried out. The first, Model 1, is the main effect analysis, whereas Models 2–4 provided robustness checks to increase confidence in the analysis and assess the degree to which selection and endogeneity might have impacted the results. Model 1 includes the key predictor (SBI or PBI) and the related covariates on children’s birth characteristics, mother/household characteristics and community/context covariates (the full model – see Equation 1). Model 2 only includes the key predictor and children’s birth and community-context covariates, and Model 3 only models the key predictor as a continuous variable and its square, which aims at estimating the effects of each additional month of SBI or PBI on child mortality risk. Model 4 is a linear probability model for each main effect on the risk of child mortality that is adjusted for birth year as a set of dummy variables.
Tables 3 and 4 contain results from fitting Model 1 to estimate the fully adjusted effects of SBI and PBI on childhood mortality by age segment. The results of Models 2–4 corroborate Model 1 results and are presented in Appendix A. The results of the analysis that adopts the WHO definition of short-, well- and widely spaced births but is otherwise analogous to the Model 1 analysis are presented in Appendix B. Finally, the results of the interaction analysis that was performed to determine whether the main effect associations that were detected by Model 1 were moderated by children’s birth year (Model 5), maternal age at childbirth (Model 6), household wealth (Model 7) and children’s birth order (Model 8) are presented in Appendix C. All analyses were conducted using in R Studio version 4.0.3.
Results
Sample characteristics and descriptive results
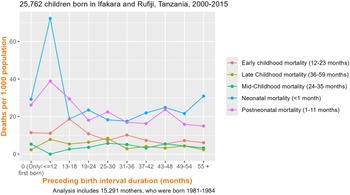
The relationship between the SBI and post-infant mortality was visualised after the exclusion of children whose exit from the population occurred prior to the closure of their mothers’ SBI (Figure 1). This revealed a clear trend in the relationship between children’s death and the timing of the mothers’ subsequent birth, namely that after the first year, child mortality peaked among those with younger siblings born 13–18 months after them and then precipitously declined as SBI durations expanded.
The relationship between subsequent birth interval durations and child mortality risk among 23,189 children and 13,127 mothers in Ifakara and Rufiji Health and Demographic Surveillance Systems, Tanzania, 2000–2015.

Then, different child mortality patterns were descriptively analysed, given variation in duration of PBI (Figure 2). Whereas levels of late-childhood mortality were relatively stable across the PBI trajectory, a downward shift was observed among children in the neonatal, post-neonatal, and to a lesser extent, early childhood period as PBI lengths expanded.
The relationship between preceding birth interval durations and child mortality risk among 25,762 children and 15,291 mothers in Ifakara and Rufiji Health and Demographic Surveillance Systems, Tanzania, 2000–2015.

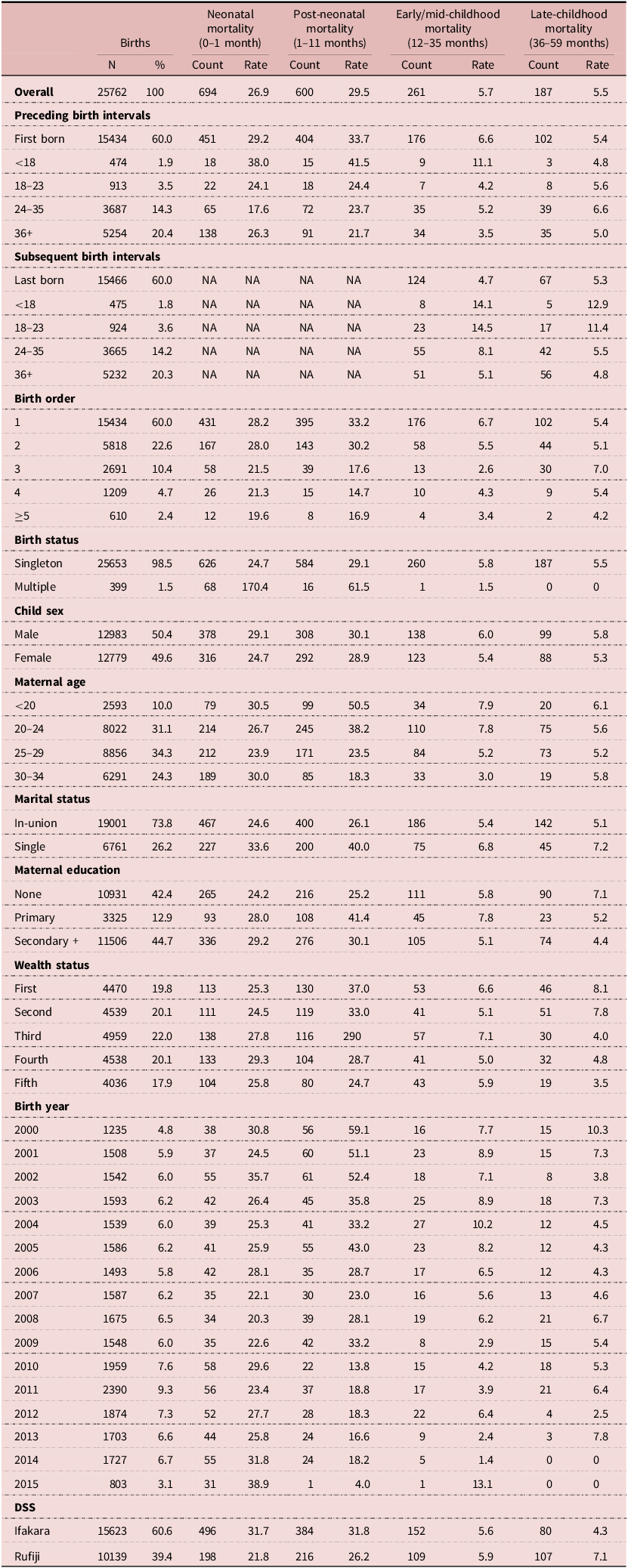
Table 2 presents the characteristics of the 25,762 births that took place in the study areas between 2000 and 2015. Noticeable is the relatively high proportion of intervals that were associated with first births, 60% (n = 15,434). This reflects the young age structure of the female population that was subset for the analysis. 9,310 of such births were only children who never had a sibling. Of the remainder, less than 2% of the sample were born within 18 months of their elder or immediately younger sibling, and 3.5% between 18 and 23 months of the preceding or subsequent birth. Approximately one-fifth of all births recorded in the HDSS took place three years more after mothers completed their preceding pregnancy. Mortality rates, particularly in the first year of life, were most pronounced among those with PBI less than 18 months and, in the case of post-neonatal mortality, became lower monotonically as PBI levels increased. However, this relationship reversed among neonates with PBI of 36 months and over: Mortality was higher among these neonates than among neonates with shorter PBI of 18–35 months. Concerning SBI, mortality between age one and five was most pronounced among those whose younger siblings were born less than 18 months and between 18 and 23 months after they were born. Across all categories of childhood, mortality risk was highest among firstborn children and declined monotonically as birth order progressed. This was especially apparent with regards to neonatal and post-neonatal mortality. Among neonates, mortality risk was highest among very young and relatively older mothers; however, among children at all other stages of childhood, mortality risks tended to be highest among mothers under 20 years of age and consistently lower among mothers in older age categories. Except for the neonatal period, lower socio-economic status at the household-level tended to be associated with higher levels of mortality risk. Despite the presence of some outliers, a similar trend was observed among children in the same categories of childhood with respect to birth year, with higher risks of mortality tending to have occurred in earlier years.
Births and mortality rates of children in Ifakara and Rufiji HDSS, 2000–2015

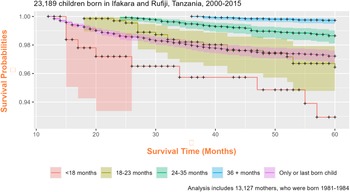
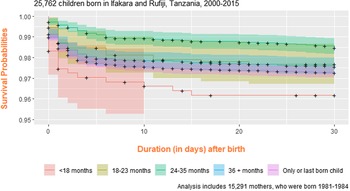
Figures 3–5 are KM survival functions for post-infant mortality by SBI length, and for neonatal mortality and mortality between ages one and two by PBI length. The same illustrations for all other childhood age groups are available from the corresponding author. All curves illustrate a pronounced survival disadvantage for children with short birth intervals compared to counterparts whose intervals were more widely spaced.
Kaplan–Meier survival estimates for children 12–59 months old based on the duration of their subsequent birth intervals. Estimates obtained from records of 23,189 children and 13,127 mothers in Ifakara and Rufiji Health and Demographic Surveillance Systems, Tanzania, 2000–2015.

Kaplan–Meier survival estimates of newborns 0–1 month old based on the duration of their preceding birth intervals. Estimates obtained from records of 25,762 children and 15,291 mothers in Ifakara and Rufiji Health and Demographic Surveillance Systems, Tanzania, 2000–2015.

Kaplan–Meier survival estimates for children 12–23 months old based on the duration of their preceding birth intervals. Estimates obtained from records of 25,762 children and 15,291 mothers in Ifakara and Rufiji Health and Demographic Surveillance Systems, Tanzania, 2000–2015.

Multivariate analysis of subsequent birth interval and childhood mortality
To understand the effect of SBI length, Models 1, the main effects model, was fit to detect an association with mortality in early childhood (12–23 months), mid-childhood (24–35 months) and late childhood (36–59 months), and all post-infancy (12–59 months) (Table 3). This showed that SBI length had no effect on death in mid-childhood, but strong effects on mortality in the early- and late-childhood and all post-infancy. Model 1 results are reported in Table 3. Even after removing the possibility of reverse causation in the data, the fully adjusted model, Model 1, revealed that among children whose survival exceeded that of their respective SBI, relatively long SBI were associated with lower mortality risks during early childhood (12–23 months), late childhood (36–59 months) and all post-infancy. With regards to the cumulative post-infant results, although no significant effect was detected when comparing index births with SBI of 18–23 with those that were less than 18 months, the analysis found that the risk of death between months 12 and 59 among children whose younger sibling was born between 23–35 months was 0.29 times lower than that of those with an SBI less than 18 months (HR = 0.29, 95% CI: 0.13, 0.61). An SBI of 36 months or greater exerted an even greater protective effect (HR = 0.21, 95% CI: 0.09, 0.44). To assess whether this model was over-parameterised, these results were compared with those reported by Models 2–4, which were adjusted for birth-level and contextual-level covariates only and reported very similar results (Tables A1, A2 and A3 in Appendix A).
Multivariate analysis of the preceding birth interval and childhood mortality
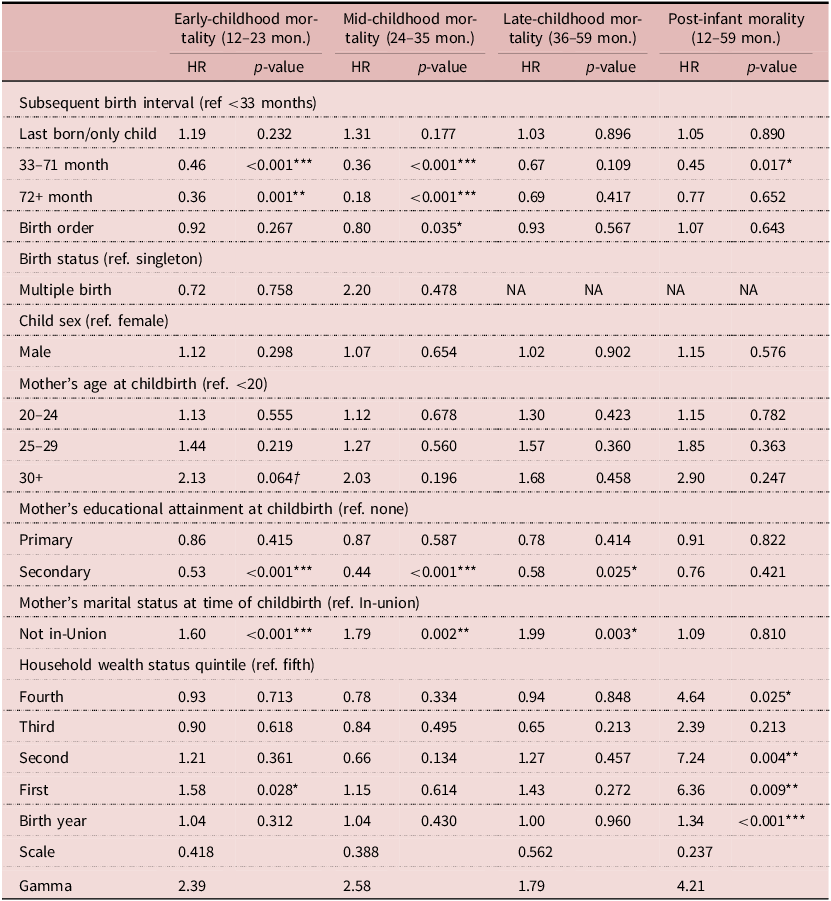
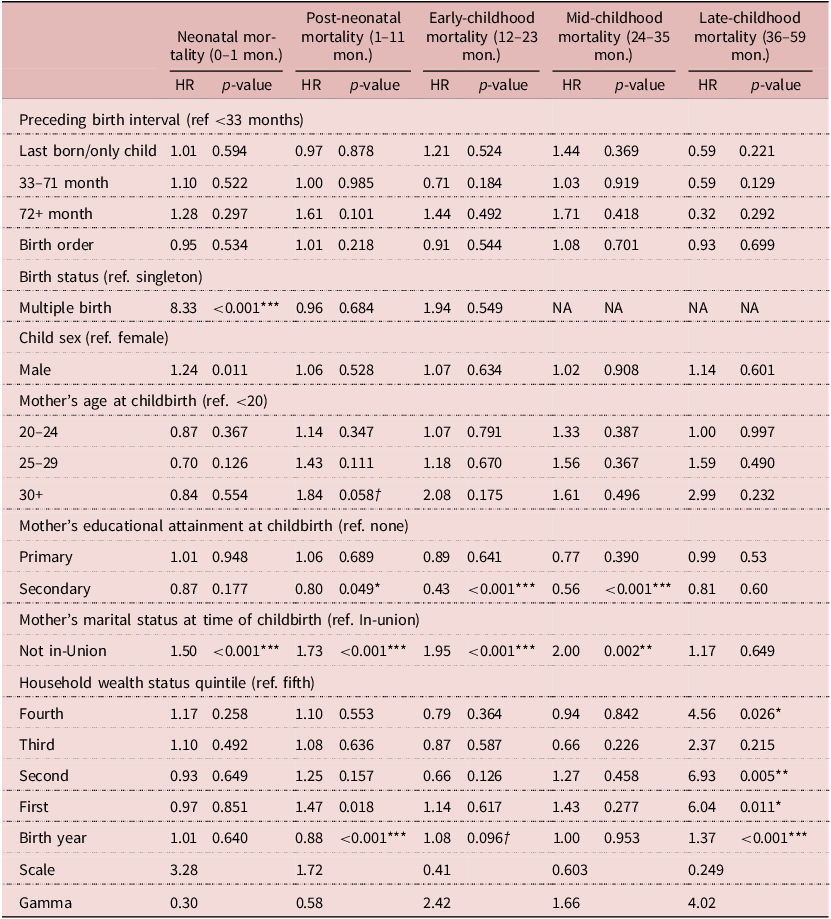
Model 1 was refitted to determine whether PBI was associated with mortality risk in the neonatal, post-neonatal, early childhood, mid-childhood and late childhood. Significant effects were reported for the main effect relationship of PBI duration on neonatal and early childhood mortality only. See Table 4. Comparing index births with PBI that are 24–35 months with those that are <18 months, Model 3 shows that the former had a neonatal mortality risk that was 0.48 times lower (HR=0.48, 95% CI: 0.27−0.77). The analysis also revealed signs of protective effects of being a first born (HR = 0.62, 95% CI: 0 14, 1.03) and having PBI of 18–23 months (HR = 0.55, 95% CI: 0.05, 0.98), relative to PBI of 18 months or less, on the risk of death in a child’s first month, however those findings were only marginally significant. Regarding the risk of dying in a child’s second year, the fully adjusted model reported that when comparing all index children with all other categories of PBI to those with PBI less than 18 months, except for firstborn and only children, the risk of mortality was significantly lower. Index births with PBI 18–23 months had a risk of dying in months 12–23 that was 0.20 times lower than those with very short PBI (HR = 0.20, 95% CI: 0.06, 0.67). Similarly, the risk of dying during this period among those with PBI 24–35 months and at least 36 months were 0.39 (HR = 0.39, 95% CI: 0.18, 0.79) and 0.33 (HR = 0.33, 95% CI: 0.14, 0.72) times lower. To assess whether this model was over-parameterised, these results were compared with those reported by Models 2–4, which were refitted to test the PBI hypothesis, adjusting for birth-level and contextual-level covariates only and reported very similar results (Tables A1, A2 and A3 in Appendix A). Results of fitting the same models, however, employing the WHO birth interval classification, are reported in Tables B1 and B2 in Appendix B. Although this analysis produced similar results for SBI as those shared in Table 3, it did not find any statistically significant relationships between short PBI (<33 months), well-spaced births (i.e., PBI of 33–71 months), widely spaced births (i.e., PBI > 71 months), and child mortality. The results of the investigation of high-order interactions that was conducted in response to the secondary hypotheses that the protective effect of birth spacing would be most pronounced among children most exposed to these risk factors are reported in Tables C1, C2 and C3 of Appendix C. These findings suggest that there may be a tendency for the effects of birth spacing to be especially protective among children that were born relatively early in the 15-year cohort compared to those born later, among children from households that were relatively wealthy compared to those that were poorer and among children that were born to mothers that were relatively old than among children of mothers that were younger.
Results of Model 1, a parametric Weibull frailty model, (hazard ratios and p-values) on the effect of subsequent birth interval durations on early childhood, mid-childhood, late childhood, all post-infant mortality when short birth interval is classified as <33 months duration, well-spaced birth intervals are 33–71 months and widely spaced intervals are >71 months (n = 23,189)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
Results of Model 1, parametric Weibull frailty model, (hazard ratios and p-values) on the effect of preceding birth interval durations on neonatal, post-neonatal, early-childhood, mid-childhood and late-childhood mortality when short birth interval is classified as <33 months duration, well-spaced birth intervals are 33–71 months and widely spaced intervals are >71 months (n = 25,762)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
Discussion
The analyses presented in this paper evaluated the relationship between SBI and PBI lengths and child mortality in a rural East African population amid demographic change. A strength of this work is that the data were longitudinal, which rendered it less susceptible to errors that have biased associations between birth spacing and child death inferred from retrospective data. The paragraphs that follow summarise this paper’s key findings vis-à-vis the hypotheses that motivated the analysis, that relatively short SBI and PBI would be associated with heightened risks of child mortality; however, the effects of short SBI would be most pronounced among 12–59 months-old children; and the effects of short PBI among neonatal and post-neonatal children. The discussion contextualises the results within the literature that was previously published on this subject and the underlying mechanisms, biological and behavioural, through which birth spacing affects child survival and health. Finally, limitations of the analysis that is presented in this paper and implications of findings for policy and programmes are reviewed and discussed.
This analysis reported strong effects of birth spacing on mortality among children older than 12 months, and weaker effects on mortality risk in the first year of life. Compared with children whose SBI is less than 18 months, those whose mothers waited 24–35 months and over 36 months had a 71% and 79% lower risk of dying between 12 and 59 months of age. This finding is consistent with the few previous analyses that also detected substantially higher risks of dying during the post-infant period associated with relatively short SBI (e.g., Hobcraft et al., Reference Hobcraft, McDonald and Rutstein1985; Koenig et al., Reference Koenig, Phillips, Campbell and D’Souza1990). While this finding is consistent, also, with the first hypothesis, the findings regarding PBI were not. At variance with expectations, the analysis of main effects found that PBI lengths most significantly affected children during their second year of life in which 80% lower risk of mortality was conferred even by spacing between 18 and 23 months compared to the effect of intervals less than 18 months, with smaller protective effects exerted by PBI of 24–35 months and over 36 months in duration. Yet, at variance with the hypothesis of a strong effect of longer PBI on infant survival, no effect of PBI was detected regarding the risk of post-neonatal death, and effects on neonatal death were only marginally significant or smaller than early childhood effects. From this, it appears that in this rural, Tanzanian population, channels linking birth spacing and child health are not mutually exclusive and can co-occur in the same settings, and that channels may affect both the older and younger siblings. While short PBI may operate through physiological mechanisms to the detriment of neonatal survival, the findings suggest that birth intervals may affect children more via behavioural responses that play out later during childhood as families contend with the converging demands of rearing multiple children, oftentimes lacking sufficient means for doing so. This result is surprising since most studies have found stronger effects on birth spacing on survival through children’s first year (Islam et al., Reference Islam, Billah, Islam, Rahman and Khan2022). Yet, these findings echo those of Fotso et al. (Reference Fotso, Cleland, Mberu, Mutua and Elungata2013), whose results suggest that in slum areas of Nairobi in the 2000s, sibling competition for scarce parental and household resources may be a more important pathway of influence than maternal depletion (Fotso et al., Reference Fotso, Cleland, Mberu, Mutua and Elungata2013).
Although the relationship between inter-pregnancy intervals and child survival is well-established in the literature, there is less empirical evidence on the links between closely spaced childbearing, between-sibling inequities in care and resource allocation, and morbidities that can heighten child mortality risk. Dewey and Cohen (Reference Dewey and Cohen2007) assessed evidence from 52 studies and reported that approximately half found that PBI of at least 36 months was associated with a 10–50% reduction in childhood stunting and wasting, whereas the remaining studies found no association or were inconclusive (Dewey and Cohen, Reference Dewey and Cohen2007). Rutstein’s analysis of 52 DHS surveys that were conducted from 2000 to 2005 found a consistently positive association between birth interval durations and child nutritional status outcomes (Rutstein, Reference Rutstein2008). Fink and colleagues synthesised data sets from 153 DHS across 61 countries conducted from 1990 to 2011 and reported that birth intervals of less than 12 months and between 12 and 23 months were associated with higher risks for stunting compared to a 24–35 month gap between pregnancies (Fink et al., Reference Fink, Sudfeld, Danaei, Ezzati and Fawzi2014). Miller and Karra (Reference Miller and Karra2020) used longitudinal data on a cohort of over 4,000 children from four low- or middle-income countries and found declines in child health at age one among children born within three years of an older sibling compared with those born after three years, however that closely spaced children experienced “catch up” growth as they age (Miller and Karra, Reference Miller and Karra2020). Sear and Coall offer an evolutionary perspective that emphasises a potentially helpful role of an older sibling who, as households adapt to changes in family size and economic circumstances, can assist with chores and the care of a younger brother or sister while parents work (Sear and Coall, Reference Sear and Coall2011). Such sibling cooperation can enhance the health and survival of children if there is a gap between siblings’ births that can sufficiently help prevent competition over household resources (Bocquier et al., Reference Bocquier, Ginsberg, Menashe-Oren, Compaoré and Collinson2021).
Other studies examined this issue by adopting a focus on sibling size rather than birth interval durations. For example, in his investigation of this relationship in 19th–20th century Sweden, Oberg (Reference Öberg2015) pointed out that the inverse relationship between sibling size and child height was persistent over several decades and most pronounced at a time when dependency ratios had peaked and when the study population started a large and precipitous fertility decline (Öberg, Reference Öberg2015). Desai (Reference Desai1995) used data from DHS of 16 less developed countries to examine the relationship between family size and children’s physical growth. The exercise suggested that the effect of family size on child growth depends on the extent to which parents bear the cost of rearing children and the level of economic development (Desai, Reference Desai1995). A study in Ethiopia sought to understand the relationships between differences in sibling size and inequities in household consumption expenditure and found that the two were negatively associated, but only among families in rural areas (Desta, Reference Desta2014). Future studies should explore more deeply whether variation in birth spacing and sibling size is affected by socio-economic context, importantly, whether it is associated with inequities in household resource allocation and parental child-rearing practices in SSA societies. Doing so would, importantly, help elucidate the mechanism that is suggested by this study and previous works concerning the behavioural effects that arise from competition between closely spaced siblings.
The early advent of a subsequent pregnancy also may instigate sibling competition for breastfeeding. Bohler and Bergström (Reference Bøhler and Bergström1996) used longitudinal data from Bhutan to demonstrate that short birth spacing led to premature weaning and reduced growth rates of older siblings (Bohler and Bergström, Reference Bøhler and Bergström1996). An earlier study showed how shorter birth intervals may impact younger siblings through increased competition for maternal nutrition during the breastfeeding pregnancy overlap (Boerma and Bicego, Reference Boerma and Bicego1992). Findings from a United States-based study indicated that women who became pregnant after shorter inter-pregnancy intervals were more likely to breastfeed during the succeeding pregnancy and suffer a miscarriage (Molitoris, Reference Molitoris2019). A study by Manda (Reference Manda1999) showed that breastfeeding status does not significantly modify the effect of PBI on infant and child mortality risks but does partially reduce the effect of SBI (Manda, Reference Manda1999). It’s critical to point out that the breastfeeding mechanism is both biologically and behaviourally based. Evidence from Peru indicated that the continuation of breastfeeding of older children during a succeeding pregnancy was associated with changes in breastmilk composition that reduce its nutritional value for both older and younger siblings (Marquis and Peeny, Reference Marquis, Penny, Diaz and Marín2002; Marquis et al., Reference Marquis, Penny, Zimmer, Diaz and Marín2003).
It is important to recognise that this study had limitations. First, in the absence of data predating the start of the cohort and to avoid the problem of unobserved childbearing, this analysis focused on an early segment of women’s reproductive lives. It is possible that the risks conferred by multiple pregnancies compound at later stages of women’s reproductive years, which may explain why the results shared in this paper offer less support for the maternal depletion hypothesis than it provide for the sibling competition mechanism. Second, the challenge of endogeneity arises in analyses on this subject when unobservable maternal and household characteristics mediate the selection process that determines children’s exposure to short birth intervals and whether they survive. While this may undermine the analysis that is reported in this paper, the analytic approach that was employed, i.e., to account for within-mother clustering by incorporating random effects in the models, is bolstered by evidence from low- and middle-income country studies that short birth interval effects remain even after addressing endogeneity concerns. Furthermore, methodologies known to address this issue may have been inappropriate for the data discussed in this paper. For example, Molitoris and colleagues employed a maternal fixed effects approach to address endogeneity concerns, which implied a need to restrict the sample to mothers who had at least three births (e.g., Molitoris et al., Reference Molitoris, Barclay and Kolk2019). Applying this approach to the data of this study would have resulted in an appreciable reduction in the sample size, which was skewed toward low parity births. Third, it should be noted that this study took place in the sentinel areas of HDSS in which, from 2000 to 2015, there were several impact evaluations of child survival programmes. It is unclear whether the same results would have been reported from the same analysis if it took place in another, more representative setting within Tanzania. Fourth, the HDSS from which data were obtained for this study did not collect information on variables such as fertility preferences, contraceptive use and spousal relationship dynamics, even though such information would have enabled a more expansive analysis of the familial conditions and behaviours that help shape the mortality response to birth spacing. Finally, even though the dating of vital events is almost certainly superior when data are collected through longitudinal demographic surveillance systems compared to retrospective research, prospective studies are not immune to errors of omission.
Conclusion
The findings from this analysis lend support to the argument that birth spacing constitutes a child survival intervention and suggest that the benefits of this practice are mediated through different mechanisms that operate concurrently in populations and affect older and younger siblings. As a corollary, family planning programmes may be particularly important in SSA, where child mortality is relatively high and cultural norms support birth spacing behaviour, but where the practice of family planning remains relatively low in comparison to other global regions. Since fertility remains high in SSA, a sizeable proportion, if not majority, of the child population has both older and younger siblings and therefore will benefit from investments in programmes that encourage longer inter-pregnancy intervals. In particular, culturally sensitive and programming strategies aimed at promoting the uptake and continued use of contraception during the postpartum period, and integrating opportunities for this into routine maternal, newborn and child health care interactions, may prove very crucial to these efforts. Although more focused research on factors that condition the mortality response to birth spacing is needed, this study indicated that the benefits of birth spacing are most felt among children with advantages in terms of household wealth. Family planning programmes should, thus, be designed and implemented in ways that help to ensure that their benefits are equitable. Revitalising efforts to help women space pregnancies in the context of strengthening primary health care and focusing on equity will accelerate achievement of child survival goals.
Acknowledgements
The authors gratefully acknowledge the funding and advisory support of the Doris Duke Charitable Foundation and Comic Relief UK, and the contributions of staff of the Health and Demographic Surveillance Systems of the Ifakara Health Institute including Amri Shamte, Matthew Alexander, Francis Levira, Eveline Geubbles, Rose Nathan.
Funding
This work was supported by the Doris Duke Charitable Foundation (grant number DDCF2009058a) and Comic Relief UK (grant number 112259).
Competing interests
The authors have no conflicts of interest to declare.
Ethical standard
Approval for the research that was carried out for this manuscript was granted by the ethical review boards of the Ifakara Health Institute (IHI/IRB/No. 16-2010), the National Institute for Medical Research of Tanzania (NIMR/HQ/R.8a/Vol.I/1203), and the Institutional Review Board of Columbia University Medical Center (Protocol AAF3452).
Appendix A
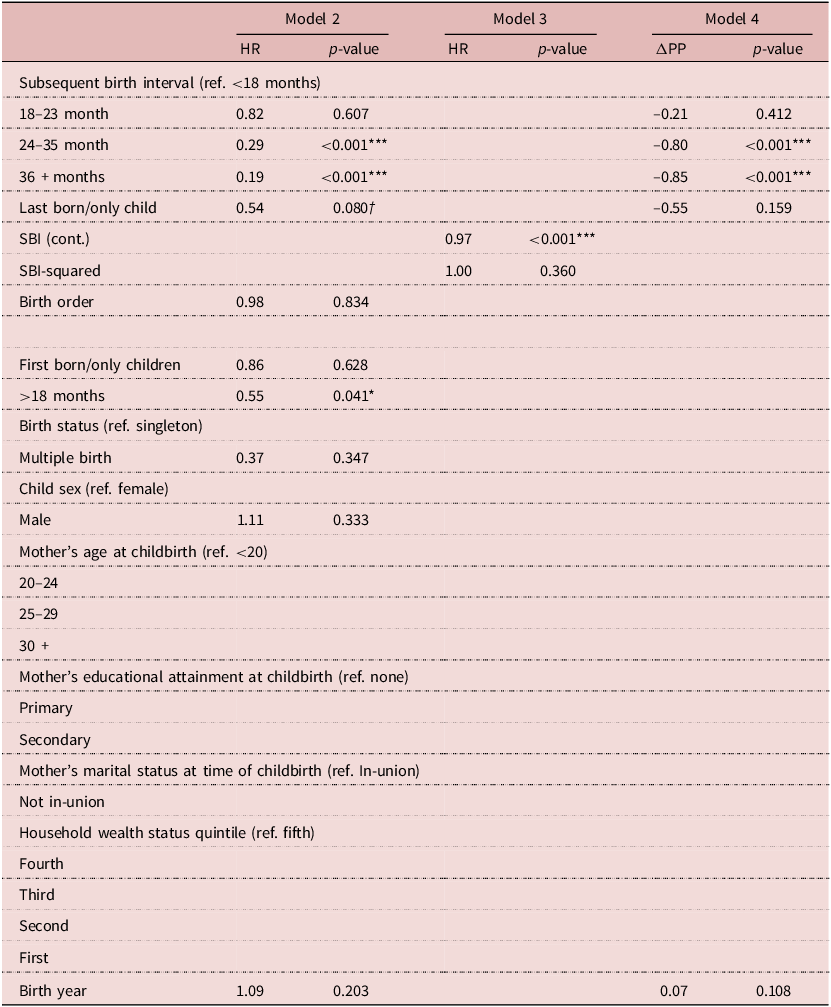
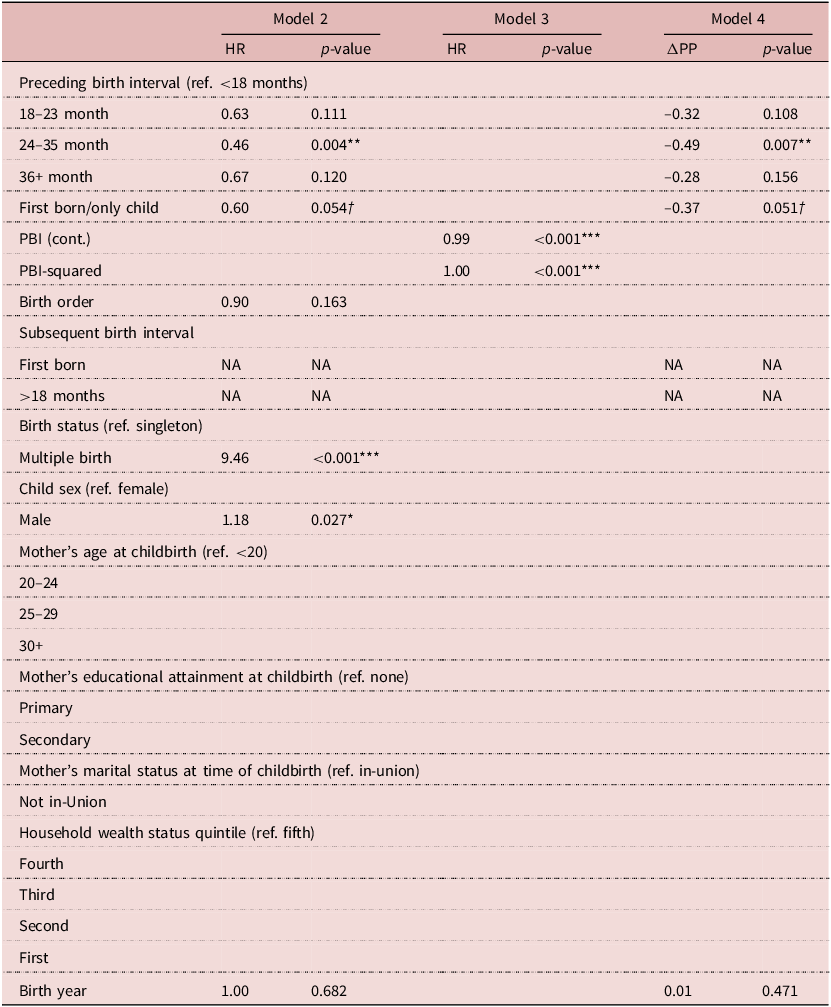
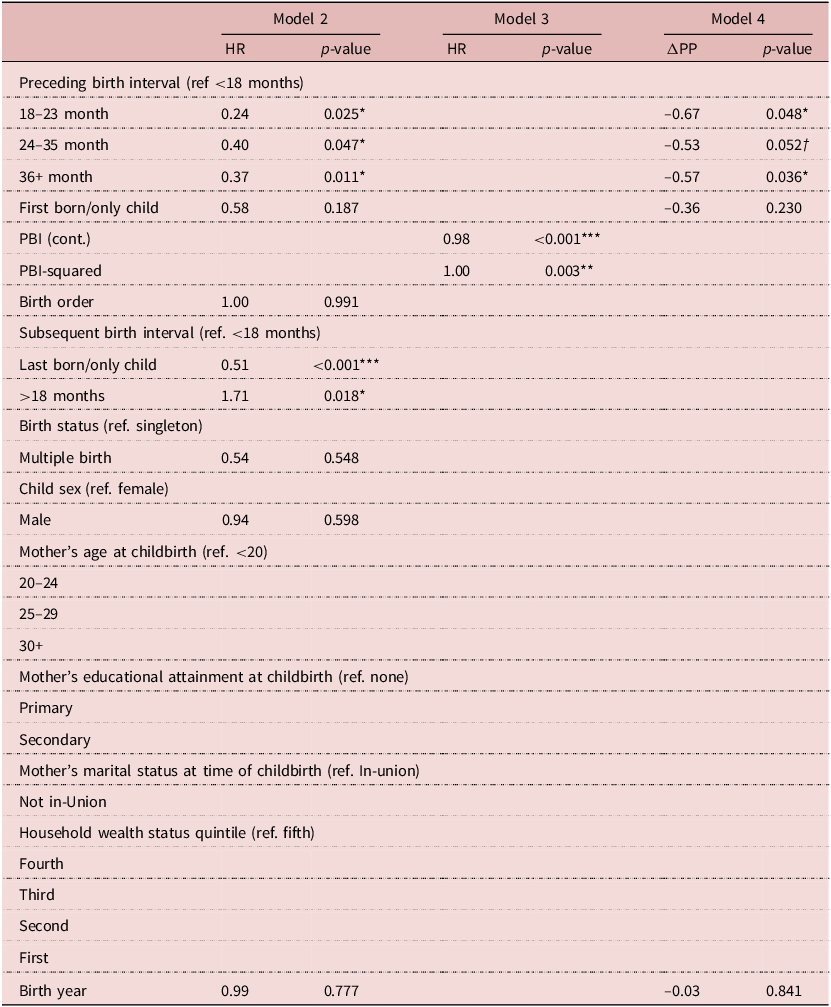
Models 2–4 were fitted to assess whether the main effects model (Model 1), which tested the hypotheses that longer SBI and PBI durations are associated with lower risk of child mortality, was over-parameterised. Model 2 only includes the key predictor and children’s birth and community-context covariates, and Model 3 only models the key predictor as a continuous variable and its square, which aims at estimating the effects of each additional month of SBI or PBI on child mortality risk. Model 4 is a linear probability model for each main effect on the risk of child mortality that is adjusted for birth year. Here, it is demonstrated that, as is reported in the manuscript, over-parameterisation did not meaningfully affect the results reported in Tables 3 and 4. Tables 2, 3 and 4 present the results of Models 2–4 with respect to the relationship between SBI duration and post-infant mortality (Table A1), PBI duration and neonatal mortality (Table A2) and PBI duration and early-childhood mortality (Table A3).
Results of parametric Weibull frailty model (hazard ratios and p-values) on the effect of the subsequent birth interval and other determinants on child mortality in Ifakara and Rufiji, Tanzania 2000–2015 (n = 23,189)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
ΔPP = Change in the predicted probability (of post-infant mortality).
Results of parametric Weibull frailty model (hazard ratios and p-values) on the effect of the preceding birth interval and other factors on neonatal mortality in Ifakara and Rufiji, Tanzania 2000–2015 (n = 25,762)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001, †
$\; \le \;$
0.001, †
 $p \le $
0.1.
$p \le $
0.1.
ΔPP = Change in the predicted probability (of post-infant mortality).
Results of parametric Weibull frailty model (hazard ratios and p-values) on the effect of the preceding birth interval and other factors on 12–23-month year-old mortality in Ifakara and Rufiji, Tanzania 2000–2015 (n = 25,762)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
ΔPP = Change in the predicted probability (of post-infant mortality).
Appendix B
Because the parametrisations of the independent variable for SBI and PBI duration are different from the WHO recommendation of 33 months between births, sensitivity analyses were conducted whereby the main effects analysis was repeated but using the WHO definition of short (<33 months), well-spaced (33–71 months) and widely spaced (≥72 births).
Appendix C
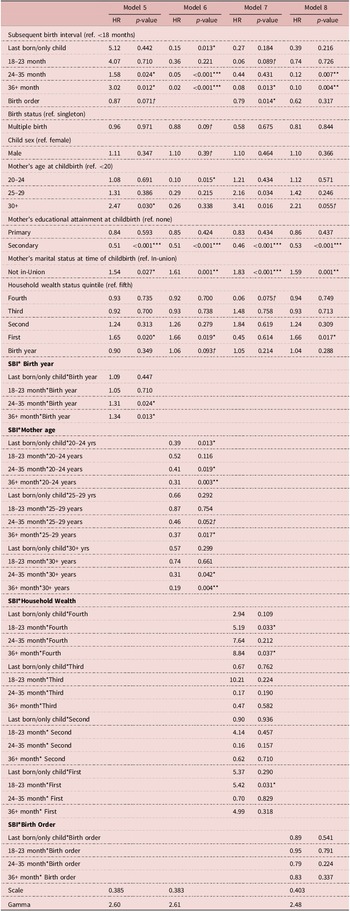
To assess whether the child mortality response to birth spacing is conditional on risk factors, the main effects analyses (i.e., Model 1) were adapted by incorporating into the model vectors of parameters for terms representing interaction between birth interval duration categories and covariates on children’s birth year (Model 5), maternal age at childbirth (Model 6), household wealth status (Model 7) and children’s birth order (Model 8), which were also estimated by the maximum likelihood. Models 5–8 were fit to detect whether the above risk factors moderated the main effect associations that were detected with respect to the effects of SBI on post-infant mortality (Table C1), PBI on neonatal mortality (Table C2), and early-childhood mortality (Table C3). These results are the coefficients of the AFT models after their conversion as the ‘ratio of hazard ratios’ that compare the strength of the main effect relationships between groups that differ in terms of exposure to the above risk factors.
Results of parametric Weibull frailty model (hazard ratios and p-values) to test for the presence of effect modification of the relationship between subsequent birth interval duration and post-infant mortality in Ifakara and Rufiji, Tanzania 2000–2015 (n = 23,189)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
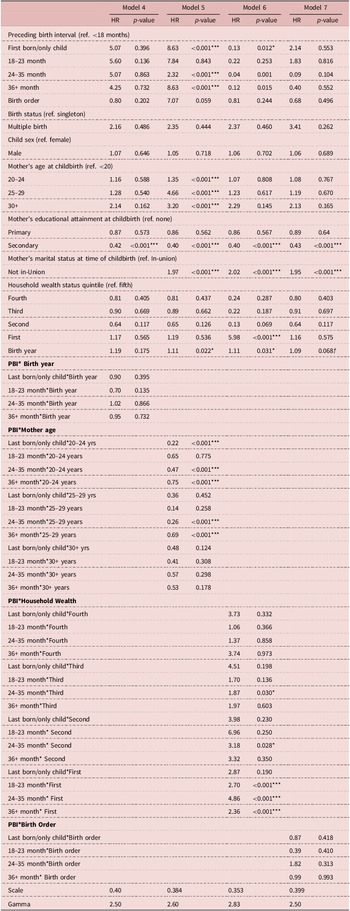
Results of parametric Weibull frailty model (hazard ratios and p-values) to test for the presence of effect modification in the relationship between preceding birth interval duration and neonatal mortality in Ifakara and Rufiji, Tanzania 2000–2015 (n = 25,762)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
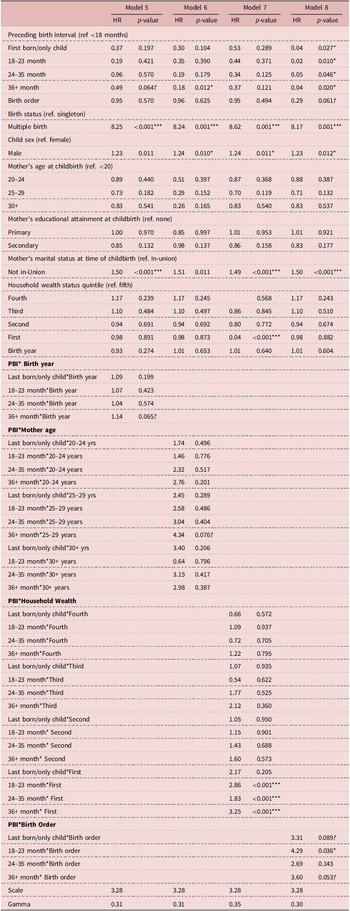
Results of parametric Weibull frailty model (hazard ratios and p-values) to test for the presence of effect modification in the relationship between preceding birth interval duration and early-childhood mortality in Ifakara and Rufiji, Tanzania 2000–2015 (n = 25,762)

*p
 $\; \le \;$
0.05, **p
$\; \le \;$
0.05, **p
 $\; \le \;$
0.01, ***p
$\; \le \;$
0.01, ***p
 $\; \le \;$
0.001,
†
$\; \le \;$
0.001,
†
 $p \le $
0.1.
$p \le $
0.1.
Regarding children’s birth year, Model 5 in Table C1, which compared post-infant children born one year apart, found that the risk of death given exposure to SBI durations of 24–35 months and ≥36 months was 1.31 and 1.34 times higher among the children born later than those born earlier (HRR = 1.31, 95% CI: 1.03, 1.64; HRR = 1.34, 95% CI: 1.06, 1.69). Regarding maternal age, Model 6, which compared post-infant children born to mothers aged 15–19 to those aged 20–24, reported that the mortality risk given exposure to no SBI (last born or only children) was 0.39 times lower among children with older mothers (HRR = 0.39, 95% CI: 0.10, 0.71). Within the same comparison, the mortality risk given exposure to SBI between 24–35 and ≥36 months was 0.41 and 0.31 times lower among children born to older mothers (HRR = 0.41, 95% CI: 0.13, 0.83; HRR = 0.31, 95% CI: 0.06, 0.78). Model 6 revealed similar results when comparing children born to mothers between 15 and 19, and those born to mothers between 25 and 29, and mothers who were 30 or older. Model 7 tested for effect modification related to household socio-economic status. After comparing that the post-infant mortality risks associated with SBI of children born in the fourth socio-economic quintile to those born in the fifth (i.e., the second to most wealthy to the wealthiest quintiles), it reported that mortality risks associated with 18–23 month and ≥36 month SBI were 5.19 and 8.84 times higher among children born in households in the fourth quintile (HRR = 5.19, 95% CI: 2.76, 8.99; HRR = 8.84, 95% CI: 4.09, 13.02). In addition, when comparing post-infant mortality risks associated with SBI duration between children born in the poorest (quintile 1) to the wealthiest (quintile 5), Model 7 found that the post-infant mortality risk associated with 18–23-month SBI was 5.42 times greater among children in the first quintile (HRR = 5.42, 95% CI: 2.23, 8.14). Model 8 did not detect evidence of interaction between children’s birth order (i.e., the parity of the birth) and SBI duration on post-infant mortality risk.
Models 5–8 were refitted to assess whether the above risk factors moderate the main effect association between PBI durations and neonatal mortality (Table C2). They reported no indication of interaction between PBI and the year in which children were born and maternal age on neonatal mortality risk. However, Models 7 and 8 revealed findings that suggest effect modification in relation to household socio-economic status and children’s birth order. Comparing the neonatal mortality risks associated with PBI of children born in the first socio-economic quintile to those born in the fifth (i.e., the poorest to the wealthiest quintiles), Model 7 found that neonatal mortality risks associated with 18–23 month, 24–35 month and ≥36 month PBI were 2.86, 1.83 and 3.25 times greater among children born in the poorest quintile (HRR = 2.86, 95% CI: 1.11, 4.21; HRR = 1.83, 95% CI: 1.00, 3.04; HRR = 3.25, 95% CI: 1.97, 5.13). In addition, the analysis that compared the neonatal mortality risks associated with PBI of 18–23 months between newborns of relatively high and low parity births found that the risk of mortality was 4.29 times greater among higher parity births (HRR = 4.29, 95% CI: 2.92, 6.21).
Table C3 contains the same analysis, however, for the risk of early-childhood mortality associated with PBI length. This reported no significant interaction effects with regard to children’s year of birth and birth order, while, conversely, Models 6 and 7 reported significant effects of interaction between PBI durations and maternal age at childbirth and household socio-economic status. Regarding maternal age, Model 6 indicated that the benefits of relatively long PBI were stronger among older mothers: comparing 12–23-month-old children born to mothers aged 15–19 to those aged 20–24, the mortality risk given exposure to no PBI (last born or only children) was 0.22 times lower among children with older mothers (HRR = 0.22, 95% CI: 0.05, 0.62). Within the same comparison, the mortality risk given exposure to PBI between 24 and 35 and ≥36 months were 0.47 and 0.75 times lower among children born to older mothers (HRR = 0.47, 95% CI: 0.18, 0.89; HRR = 0.75, 95% CI: 0.38, 1.00). Model 6 revealed similar results when comparing main effect associations between children born to mothers between 15 and 19 and those born to mothers 25–29. This analysis also reported effect modification in relation to household socio-economic status (Model 7). For example, comparing the 12–23 month mortality risks associated with PBI of children born in the first socio-economic quintile to those born in the fifth (i.e., the poorest to the wealthiest quintiles), Model 7 demonstrated that mortality risks associated with 18–23 month, 24–35 month and ≥36 month PBI were 2.70, 4.86 and 2.36 times greater among children born in the poorest quintile (HRR = 2.70, 95% CI: 1.64, 4.09; HRR = 4.86, 95% CI: 3.35, 6.12; HRR = 2.36, 95% CI: 1.40, 4.79).
Regarding the analyses that are reported in Tables C1–3 above, it was hypothesised that the protective effects of longer SBI and PBI would be most pronounced among children subjected to conditions that placed them at particular risk of early death. Although the findings are not conclusive, they are illuminating and may give directions to new avenues of research. Children’s year of birth proved to modify the effect of SBI and post-infant mortality. With long intervals demonstrating especially protective effects during years that pre-dated large-scale investments in health systems strengthening and improving maternal and child health (Masanja et al., Reference Masanja, Savigny, Smithson, Schellenberg, John, Mbuya and Mshinda2008; Afnan-Holmes et al., Reference Afnan-Holmes, Magoma, John, Levira, Msemo, Armstrong and Lawn2015). Molitoris et al. (Reference Molitoris, Barclay and Kolk2019) pointed out a similar finding in their more expansive analysis of birth spacing and child mortality that compared patterns between children born in countries that varied in terms of economic development. In this paper, the finding of effect modification by household wealth status helps bring nuance to that interpretation. For all three sets of main effects, the protective effects of birth spacing were most pronounced among children born in wealthier households. This suggests that while the survival benefits of birth spacing may help to offset societal-level risks related to poor health system access and quality, they tend not to help address micro-level challenges that occur when poor households increase family size. On the contrary, this analysis observed that birth spacing and household wealth may interact synergistically to the benefit of well-spaced children born to relatively wealthy families.
One significant finding was reported regarding effect modification of parity. Contrary to expectations, this indicated that the benefits of lengthier spacing were more pronounced among lower parity births. This at least suggests that while lengthy birth spacing does not help to offset neonatal mortality risks associated with high parity (e.g., Kozuki & Walker), it can amplify the benefits of low parity status on neonatal survival. While it was conjectured that lengthier birth spacing would be more impactful among children born to adolescent mothers, this analysis reported the opposite. Regarding the effect of SBI and PBI on post-infant and early-childhood mortality risks, it found that lengthier spacing tended to have a more pronounced effect among children born to mothers older than 20 than among their teenage counterparts, a finding that is broadly consistent with other literature on this subject. For example, Finlay et al. (Reference Finlay, Norton and Guevara2017) in their analysis of DHS data from 33 countries in SSA found that adjusting for short birth intervals did not completely offset the negative effect of young age at birth on child survival outcomes (Finlay et al., Reference Finlay, Norton and Guevara2017). As a corollary, while birth spacing may not help to offset risks related to high parity and adolescent pregnancy, its interaction with low parity and adult pregnancy may be synergistic and tend to enhance survival prospects of children of high birth order or with relatively old mothers.



 Open access
Open access