


Introduction
In the United States, an estimated 356,461 people were assessed by Emergency Medical Services (EMS) for out-of-hospital cardiac arrests (OHCA) in 2015. Reference Virani, Alonso and Aparicio1 Nearly 37% of OHCA cases that were witnessed by bystanders survived to hospital admission as compared to 28% of all presentations in 2019. Reference Virani, Alonso and Aparicio1 Only 13.2% of the bystander-witnessed OHCA had good neurologic survival (defined as Cerebral Performance Category [CPC] 1 or CPC 2) compared to 8.5% of all presentations. Factors that have been shown to be associated with increased rates of survival from non-traumatic OHCA include: witnessed arrest by bystander or EMS, bystander cardiopulmonary resuscitation (CPR), presenting with a shockable rhythm, and return of spontaneous circulation (ROSC) in the field. Reference Sasson, Rogers, Dahl and Kellermann2,Reference Wampler, Collett, Manifold, Velasquez and McMullan3 The strongest predictor of survival to hospital discharge is ROSC in the field, with approximately one in every three victims surviving. Reference Sasson, Rogers, Dahl and Kellermann2 Despite having other positive predictor factors, it is unlikely that a patient will survive until discharge without ROSC in the field; this emphasizes the need for quality care in the out-of-hospital setting. Reference Sasson, Rogers, Dahl and Kellermann2 Early CPR is important for survival, which emphasizes the necessity of bystander CPR, particularly in areas where EMS response times may be longer. Reference Cummins4
Increasing rates of bystander CPR to improve OHCA outcomes has been a topic of research for some time. Reference Vaillancourt, Stiell and Wells5 Efforts to increase bystander CPR include: dispatch-assisted CPR instructions, teaching family members of patients with cardiac disease, training videos, practice with manikins, and teaching the concepts of diffusion of responsibility and ambiguity. Reference Vaillancourt, Stiell and Wells5 Dispatch-assisted CPR and bystander CPR have been associated with improved rates of shockable rhythm upon arrival of EMS, improved rates of ROSC in the field, and improved one-month favorable neurological outcomes in patients who suffer OHCA. Reference Panchal, Berg and Cabanas6–Reference Nikolaou, Dainty and Couper9 Dispatch-assisted CPR instruction has been shown to increase the rates of bystander CPR; however, the best method of providing these instructions has not been determined. Reference Eisenberg, Hallstrom, Carter, Cummins, Bergner and Pierce10 Dispatch-assisted CPR has traditionally been provided via audio-only instruction via a telephone or cellular phone. In recent years, the use of telemedicine has become more prevalent. Reference Ortega, Rodriguez and Maurer11 Perhaps its use could be extended to increase bystander CPR rates, which in turn may lead to increased survival rates.
GoodSAM (GoodSAM; London, England) is a platform that integrates with the computer-assisted dispatch system present in the San Antonio Fire Department’s (SAFD; San Antonio, Texas USA) public safety answering point where incoming 9-1-1 calls are taken. Reference Smith, Lall, Fothergill, Spaight and Perkins12,Reference Smith, Griffiths, Fothergill, Vlaev and Perkins13 The software allows for the telecommunicator to send a link to the caller’s mobile phone. Once the link is activated, the telecommunicator can see and hear the patient using the camera and microphone on the caller’s phone. The software also estimates a pulse rate using artificial intelligence. Utilizing this software, SAFD has been able to effectively triage patients and render appropriate care throughout the COVID-19 pandemic. Recently, its use has been extended to victims of cardiac arrest. This platform provides telecommunicators visual and auditory information to perform a more accurate assessment of respiratory and circulatory status. This information provides insight about the need to perform CPR and provides feedback regarding the quality of CPR. Figure 1 demonstrates a dispatcher correcting hand position of a simulated caller performing CPR. Additionally, the caller may feel more comfortable performing CPR knowing that the telecommunicator has visualized the patient and can coach them through the process in real time. Reference Smith, Griffiths, Fothergill, Vlaev and Perkins13
Dispatcher Using Video Telecommunication to Correct Hand Position during CPR.
Abbreviation: CPR, cardiopulmonary resuscitation.

It was hypothesized that telecommunicator use of video telecommunication will be associated with increased rates of bystander CPR.
Methods
Study Design
This was a proof-of-concept, retrospective review of a convenience sample of recorded information for the SAFD cardiac arrest dispatch records. The dates included in the analysis were July 2021 through February 2022.
Study Setting
The SAFD utilizes an all-paramedic, uniformed member dispatch system. The fire department is the sole 9-1-1 provider for the seventh largest city in the United Sates and services approximately 1.4 million residents within a 460-square-mile area with approximately 160,000 medical responses per year. The SAFD utilizes a 100% field experienced paramedic dispatch system; dispatchers utilize an internally designed Medical Priority Dispatch System, produced by a collaboration in part with the SAFD Command Staff. GoodSAM is available for use and deployment for any 9-1-1 call, and the telecommunicator has broad discretion as to timing of sending the link for use.
Protocol and Data Acquisition
For every SAFD patient where cardiac resuscitation is attempted, the UT Health San Antonio Department of Emergency Health Sciences Office of the Medical Director (OMD; San Antonio, Texas USA) maintains a comprehensive quality improvement registry. Attempted resuscitation was defined as any patient who received chest compressions or positive pressure ventilation and was not deemed to meet obvious death criteria (ie, lividity, rigor mortis, decapitation, incineration, or decomposition). Exclusion criteria were: children, traumatic circulatory arrest, or missing data. This registry is populated via a phone debriefing between a civilian training officer and lead paramedic after the resuscitation is complete. The OMD registry is then used as the data source to submit to the Cardiac Arrest Registry to Enhance Survival (CARES; Centers for Disease Control and Prevention and Emory University School of Medicine; Atlanta, Georgia USA). The OMD registry was the data source for this research study.
Every dispatch-recognized cardiac arrest that was able to be crossmatched to an OMD OHCA registry case was dichotomized to a group based on whether or not video telecommunication was used by the telecommunicator. Inclusion criteria were all consecutive cases where SAFD EMS attempted resuscitation from cardiac arrest. Exclusion criteria were when video telecommunication was used and no OMD registry case was identified, indicating whether bystander CPR was performed or not, and cardiac arrests that were witnessed by EMS personnel.
Data from dispatch records included: were dispatch CPR instructions given; caller compliance with instructions; type of CPR performed; witness of the arrest; and who performed the CPR prior to the arrival of SAFD EMS.
A case was recorded as having received pre-arrival CPR if the initial CPR was performed by anyone other than a first responder or EMS clinician responding to the scene. This included CPR performed by bystanders, family members, and health care professionals that were not part of the responding EMS units. A caller would be assumed to have complied with dispatch instructions if dispatch instructions were recorded as being given, and the initial CPR was performed by a family member, bystander, or health care professional.
The protocol was approved by the UT Health Center San Antonio institutional review board under protocol number 20210665EX.
Data Analysis
Descriptive statistics were used to characterize patients included in the overall dataset. SPSS Statistics Version 28 (IBM Corp.; Armonk, New York USA) was used for analysis of the data using Pearson chi-square tests in addition to likelihood ratios to compare the group for whom video telecommunication was used and the group for whom video telecommunication was not used. Results were considered statistically significant if P < .05.
Results
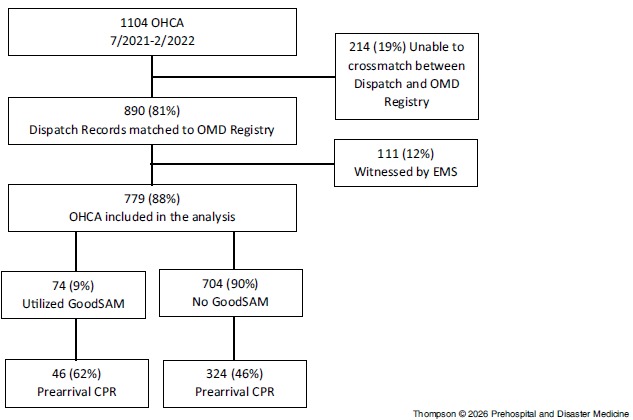
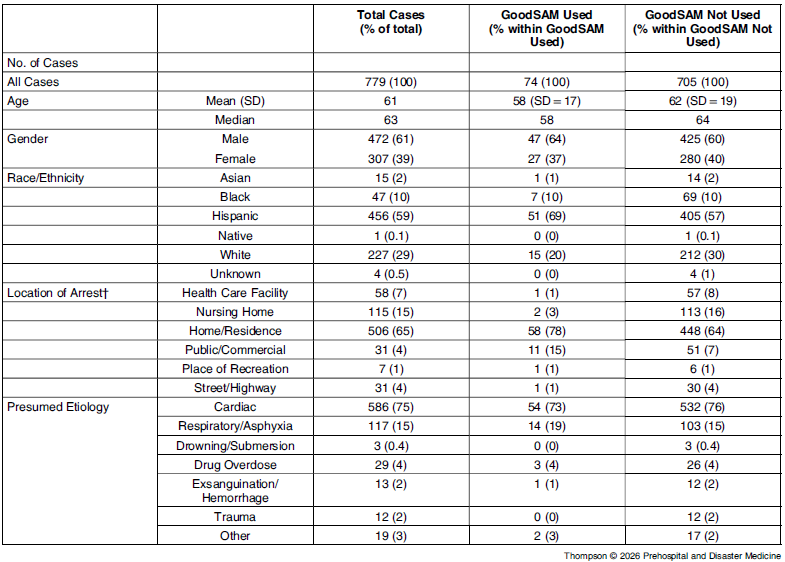
The SAFD responded to 1,104 OHCA cases from July 2021 through February 18, 2022 (Figure 2). Of those cases, 890 (81%) dispatch records ware matched with OMD cardiac arrest registry patients (Figure 2). Of these, 111 (12%) were excluded from analysis because the arrest was witnessed by EMS (Figure 2). Of these remaining 779 cases, 74 (9%) utilized video telecommunication in the telecommunicator assessment of the patient and CPR guidance (Figure 2). The demographics of the 779 cases included in the cohort, as well as the location of arrest and presumed etiology, are shown in Table 1.
Study Design.
Abbreviations: OHCA, out-of-hospital cardiac arrest; OMD, Office of the EMS Medical Director; EMS, Emergency Medical Services; CPR, cardiopulmonary resuscitation.

Cohort Demographic Information

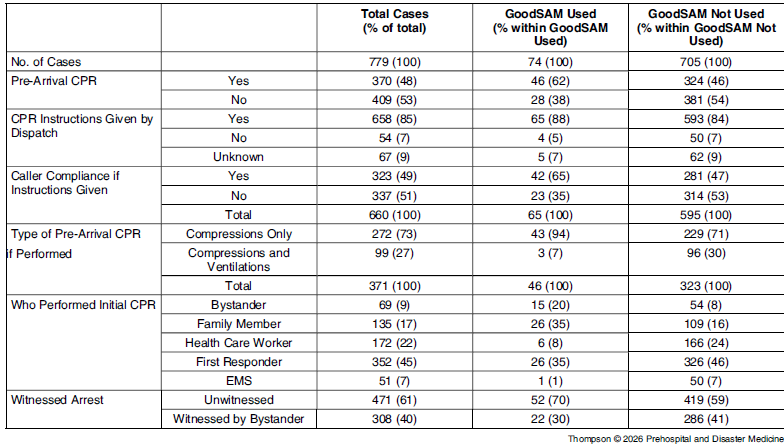
In the primary outcome, for cases where video telecommunication was utilized, 62% received pre-arrival CPR by a bystander, family member, or health care worker, versus when video telecommunication was not used, only 46% received pre-arrival CPR with a difference of 16.2% (95% CI, 4.6% to 27.9%; P = .008; Table 2). Caller compliance with CPR instructions in the video telecommunication group was also higher at 65% compared to 47% with audio-only telecommunication group (Table 2). A larger proportion of the persons performing pre-arrival CPR were family members (35% versus 17%) when compared to the cases where video telecommunication was not used (Table 2). Persons with whom video telecommunication was used were more likely to perform compressions only CPR (Table 2). There were no differences between the proportion of witnessed and unwitnessed events, or whether or not CPR instructions were given by dispatch between the video telecommunication and control groups.
Descriptive Statistics, Pearson Chi-Square Tests, and Likelihood Ratio

Abbreviations: EMS, Emergency Medical Services; CPR, cardiopulmonary resuscitation.
Discussion
In this study, EMS dispatcher utilization of video telecommunication during call taking for suspected cardiac arrest resulted in significantly higher rates of performance of pre-arrival CPR. The literature demonstrates that bystander CPR is a critical link in the chain of survival and that improving the compliance with telecommunicator medical instructions holds the potential to significantly improve outcomes. Reference Sasson, Rogers, Dahl and Kellermann2,Reference Maier, Luger and Baubin14
The SAFD uses an all-paramedic, field-experienced dispatch system, with 100% of call takers and dispatchers holding paramedic certification. The SAFD dispatchers utilize an internally designed Medical Priority Dispatch System developed through collaboration between the SAFD Command Staff and the OMD. This system provides dispatchers with considerable flexibility in making deployment decisions and managing available resources. Reference Mapp, Darrington, Velasquez and Wampler15 Video telecommunication has been associated with increased rates of caller compliance. Callers may feel more comfortable performing CPR when a trained telecommunicator uses video to coach them through the process. There were no differences between groups in whether telecommunicators provided CPR instructions, suggesting that telecommunicators are equally able to recognize cardiac arrest with or without video support.
In 2021, Linderoth, et al published a feasibility study using the same platform as the SAFD. In this study, they demonstrated significant improvement in CPR quality. Reference Linderoth, Rosenkrantz and Lippert16 Inclusion in this study utilized similarly experienced paramedic dispatchers and analyzed the quality of bystander CPR. The San Antonio study is more focused on the success of the paramedic dispatcher to provide the confidence in bystanders to intervene. This is especially important in those cardiac arrest patients who continue to have agonal breathing after circulatory collapse. Reference Bang, Herlitz and Martinell17
Most of the pre-arrival CPR was compressions only. This seems reasonable given that most laypersons are not going to have access to advanced airway management equipment and may be reluctant to perform mouth-to-mouth ventilations. Reference Vaillancourt, Stiell and Wells5 This is the area where video-assisted CPR and real-time feedback on CPR can have the greatest impact and potential to improve outcomes.
Limitations
This is a retrospective, chart review study and therefore cannot determine causation. The major confounder to this data is that utilizing video telecommunication requires dispatch utilization, caller participation, and it might be that persons who are more willing to accept the link to their phones are more likely to perform pre-arrival CPR, regardless of the use of telemedicine or not. Secondly, the video application relied on the caller calling from a smart phone with video capability. Since most cardiac arrests occur at home in older individuals, this specific population may be less likely to be calling from a smart phone (ie, land line or flip phone). This limitation likely impacted the study and may in-part explain the low utilization of the technology during cardiac arrest. Additionally, this study relied on reports given to the OMD by the medics after the arrest rather than dispatch data. Therefore, in some cases, CPR may have been started but then subsequently stopped prior to EMS arrival, and the responding medics may not have known that it was ever performed and therefore did not report it. Finally, there are missing reports from the data for patients who received CPR, leading to incomplete data regarding all the cardiac arrests. Likely, there is not an association between the report not being turned in and pre-arrival CPR; this is likely to be more personnel-dependent or related to how busy the system was at the time of the cardiac arrest call, leading to medics not having time to complete the report.
Conclusion
In this paramedic-staffed urban dispatch system, using video telecommunication to perform paramedic clinical dispatch telemedicine was associated with an increased rate of pre-arrival CPR. Further research will be required to show outcome-related results to determine if video telecommunication can be used to increase survival in patients suffering OHCA.
Acknowledgements
The authors would like to acknowledge Chief Bradley Pool for his contributions to the designing of this study and his leadership in obtaining the necessary data; as well as Joi Shumaker and Alan Lewis for their dedication to the upkeep of the OMD registry and uploading to CARES.
Author Contributions
ST and CJW designed the study and performed the data collection and analysis; ZB, LV, RP, MM were dispatch experts that provided insight and manuscript preparation. DM and DW provide resources for the study and manuscript preparation and revision.
AI Technology
No AI was used in the preparation of this document; the GoodSAM technology has integrated AI that provides the dispatchers with pulse rate and breathing rate.
Conflicts of interest/funding/disclaimer
The authors report there are no competing interests to declare. The views expressed are those of the authors and do not reflect the official views or policy of the Department of Defense or its Components. The authors do not have any financial interest in the companies whose materials are discussed in this manuscript and no federal endorsement of the companies and materials is intended.


 Open access
Open access