



-
• Across baseline (T1) and ∼1-year follow-up (T2), leukocyte, neutrophil and monocyte counts, the neutrophil-to-lymphocyte ratio (NLR), and complement C3–C4 remained elevated, indicating a persistent low-grade inflammatory trait in first-episode psychosis that endures into remission.
-
• ROC and logistic models showed that cellular (NLR) and humoral (C4) indices – together with years of education – meaningfully discriminated patients from controls, whereas CRP behaved as a state-dependent marker of acute exacerbation.
-
• From a systems-level perspective, innate immune activation in the acute phase (e.g., higher NLR) aligned with negative symptoms, while adaptive signatures in remission (IgG/IgE) tracked with positive and general psychopathology, supporting immune subtyping and personalised, immune-informed strategies.
This study has several limitations. First, recruitment was suspended due to the onset of the COVID-19 pandemic, which restricted our ability to expand the sample size for both patient and control groups; accordingly, the modest cohort size limits generalisability. Second, although we examined a broad range of clinically accessible immunological parameters, we did not assess cytokines, chemokines, kynurenine-pathway metabolites, or specific IgG subclasses and anti-neuronal antibodies. These markers are central to inflammatory signalling and may provide more granular insights into adaptive immune alterations. Our system-level approach therefore reflects a pragmatic, clinically feasible immunological profile rather than a comprehensive molecular panel. Third, antipsychotic exposure varied at follow-up, and the sample size did not permit meaningful statistical adjustment for treatment type or duration. However, baseline (T1) blood samples were obtained at or immediately before treatment initiation, minimising potential confounding in the acute-phase analyses. Future studies with larger cohorts and expanded biomarker panels – including cytokines, immunoglobulin subclasses, and neuroimmune markers – are needed to replicate and refine these findings.
Introduction
Schizophrenia and related spectrum disorders are early-onset psychiatric conditions marked by withdrawal from social life and impairments in perception, cognition, and emotion. Despite advances in treatment, they remain highly burdensome in clinical and societal contexts. According to WHO data, schizophrenia is the third most disabling mental illness, especially affecting men aged 30–49 (World Health Organisation, 2018). Its lifetime risk is approximately 1%, with an annual incidence of 15–22 per 100,000 individuals (Kirkbride et al., Reference Kirkbride, Errazuriz, Croudace, Morgan, Jackson, Boydell, Murray and Jones2012; World Health Organisation, 2018; Solmi et al., Reference Solmi, Seitidis, Mavridis, Correll, Dragioti, Guimond, Tuominen, Dargél, Carvalho, Fornaro, Maes, Monaco, Song, Il Shin and Cortese2023).
Recent studies suggest that serious infections – ranging from the prenatal period to adulthood – as well as autoimmune disorders, may increase the risk of schizophrenia (Bergink et al., Reference Bergink, Gibney and Drexhage2014; Müller & Müller, Reference Müller2017; Sørensen et al., Reference Sørensen, Debost, Agerbo, Benros, McGrath, Mortensen, Ranning, Hjorthøj, Mors, Nordentoft and Petersen2018; Gangadin et al., Reference Gangadin, Enthoven, van Beveren, Laman and Sommer2024). While there are conflicting studies, research and follow-up studies support the potential relationship (Benros et al., Reference Benros, Pedersen, Rasmussen, Eaton, Nordentoft and Mortensen2014; Korhonen et al., Reference Korhonen, Paul, Wåhlén, Haring, Vasar, Vaheri and Lindholm2023; Rømer et al., Reference Rømer, Jeppesen, Christensen and Benros2023).
Recent studies have examined the neutrophil-to-lymphocyte ratio (NLR) in schizophrenia due to its links with systemic inflammation and oxidative stress (Varsak et al., Reference Varsak, Aydin and Eren2015; Kulaksizoglu & Kulaksizoglu, Reference Kulaksizoglu and Kulaksizoglu2016; Steiner et al., Steiner et al., Reference Steiner, Frodl, Schiltz, Dobrowolny, Jacobs, Fernandes, Guest, Meyer-Lotz, Borucki, Bahn, Bogerts, Falkai and Bernstein2020; Zhu et al., Reference Zhu, Zhou, Zhu, Yan, Han, Tan and Li2022). In addition to its diagnostic relevance, NLR has also been associated with symptom severity in psychotic disorders (Bioque et al., Reference Bioque, Catarina Matias-Martins, Llorca-Bofí, Mezquida, Cuesta, Vieta, Sílvia, Lobo, González-Pinto, Moreno, Roldán, Martinez-Aran, Baeza, Bergé, García-Rizo, Mas Herrero, Bernardo, González, Álvaro, Recio, Selma, Tonda, García-Corres, Jéssica, Cón, Modrego-Pardo, Jé, Pérez-Rando, Vázquez, Cristeto, Sanchez-Moreno, Gimenez-Palomo, Castro-Fornieles, de la Serna, Contreras, González-Blanco, Sáiz, Gutiérrez-Fraile, Zabala, Sanchez-Pastor, Rodriguez-Jimenez, Usall, Butjosa, Pomarol-Clotet, Sarró, Ibáñez Ángela, Sánchez-Torres and Balanzá2022; Cavaleri et al., Reference Cavaleri, De Pietra, Gazzola, Crocamo, Bartoli and Carrà2024; Wang et al., Reference Wang, Chen, Guan and Li2024). Its predictive value, affordability, and simplicity make it a valuable marker (Zhu et al., Reference Zhu, Zhou, Zhu, Yan, Han, Tan and Li2022; Cavaleri et al., Reference Cavaleri, De Pietra, Gazzola, Crocamo, Bartoli and Carrà2024).
Acute-phase reactants such as C-reactive protein (CRP), Ferritin, C3, C4 and Serum Amyloid A (SAA) play a role in inflammation and indicate the presence and severity of inflammation. Most studies have reported elevated CRP levels in psychotic patients (Hartwig et al., Reference Hartwig, Borges, Horta, Bowden and Davey Smith2017; Gonzalez-Blanco et al., Reference Gonzalez-Blanco, Garcia-Portilla, Garcia-Alvarez, de la Fuente-Tomas, Garcia, Saiz and Bobes2018; Misiak et al., Reference Misiak, Stańczykiewicz, Kotowicz, Rybakowski, Samochowiec and Frydecka2018, Reference Misiak, Bartoli, Carrà, Stańczykiewicz, Gładka, Frydecka, Samochowiec, Jarosz, Hadryś and Miller2021; Fond et al., Reference Fond, Godin, Boyer, Berna, Andrianarisoa, Coulon, Brunel, Bulzacka, Aouizerate, Capdevielle, Chereau, D’Amato, Dubertret, Dubreucq, Faget, Leignier, Lançon, Mallet, Misdrahi, Passerieux, Rey, Schandrin, Urbach, Vidailhet, Llorca, Schürhoff and Leboyer2019), although some studies have not observed significant changes (Yee et al., Reference Yee, Nurjono, Ng, Teo, Lee and Lee2017). There are also studies that have found associations between CRP levels and Positive and Negative Syndrome Scale (PANSS) scores (Singh & Chaudhuri, Reference Singh and Chaudhuri2014; Misiak et al., Reference Misiak, Stańczykiewicz, Kotowicz, Rybakowski, Samochowiec and Frydecka2018). Research on the relationship between ferritin and psychosis and psychotic exacerbations is limited, but some studies have indicated ferritin levels during psychotic exacerbations, correlated with symptom severity (Kim et al., Reference Kim, Stewart, Park, Jhon, Lee, Kim, Kim, Amminger, Chung and Yoon2018). In psychotic patients, increased levels of C3 and C4 have been observed, and they are positively correlated with negative symptoms (Hakobyan et al., Reference Hakobyan, Boyajyan and Sim2005; Mayilyan et al., Reference Mayilyan, Arnold, Presanis, Soghoyan and Sim2006, Reference Mayilyan, Weinberger and Sim2008; Ali et al., Reference Ali, Abd El-Azeem, Hamed, Ali, Abd Al-Kader and Hassan2017; Mongan et al., Reference Mongan, Sabherwal, Susai, Föcking, Cannon and Cotter2020; Chen et al., Reference Chen, Gou, Chen, Xiu, Fan, Tan and Tian2022; Zhang et al., Reference Zhang, Zeng, Ye, Gao, Hu, Xu, Wei, Tang, Liu, Chen, Li, Wan and Wang2023). However, there are studies indicating no differences in first-episode psychosis patients (Morgan et al., Reference Morgan, Kopczynska, Zelek, Touchard, O’Donovan, Murray, Mondelli and Gaughran2017). C4 gene variants have been discussed as potentially explaining increased risk in autoimmune diseases and as potential targets for new treatments (Nimgaonkar et al., Reference Nimgaonkar, Prasad, Chowdari, Severance and Yolken2017; van der Walt et al., Reference van der Walt, Stein and Zoghbi2025). Studies in mice have revealed that SAA can cross the blood-brain barrier and induce a depressive-like condition related to its effects on the central nervous system (CNS) (Jang et al., Reference Jang, Lee, Jeong, Sung, Choi, Song, Kim, Jang, Kim, Joo, Lee, Choo, Kim and Ryoo2017). Additionally, in a study involving outpatient psychiatric patients, elevated levels of SAA were found to be associated with depression and fatigue (Bryleva et al., Reference Bryleva, Keaton, Grit, Madaj, Sauro-Nagendra, Smart, Halstead, Achtyes and Brundin2017).
Although early studies examined total immunoglobulin levels in psychotic disorders, findings were inconsistent and based on outdated methodologies (Pulkkinen & Soininvaara, Reference Pulkkinen and Soininvaara1985; Allansmith & R.M.A.A.S. Reference Allansmith and R.M.A.A.S.1973; Ramchand et al.,Reference Ramchand, Wei, Ramchand and Hemmings1994). Renewed interest in recent years highlights the need for comprehensive and modern investigation (Delaney et al., Reference Delaney, Fallon, Alaedini, Yolken, Indart, Feng, Wang and Javitt2019; Pollak et al., Reference Pollak, Vincent, Iyegbe, Coutinho, Jacobson, Rujescu, Stone, Jezequel, Rogemond, Jamain, Groc, David, Egerton, Kahn, Honnorat, Dazzan, Leboyer and McGuire2021).
Meta-analytic evidence strongly supports the involvement of immune dysregulation in psychosis, particularly in first-episode samples (Halstead et al., Reference Halstead, Siskind, Amft, Wagner, Yakimov, Shih-Jung Liu, Walder and Warren2023). Several large-scale reviews have demonstrated elevated pro-inflammatory cytokines – such as IL-6, TNF-α, IL-1β and IL-8 – as well as increased CRP levels in both schizophrenia and antipsychotic-naïve first-episode psychosis (Halstead et al., Reference Halstead, Siskind, Amft, Wagner, Yakimov, Shih-Jung Liu, Walder and Warren2023; Patlola et al., Reference Patlola, Donohoe and McKernan2023). These abnormalities appear most pronounced at illness onset and tend to partially normalise with treatment, suggesting that immune activation may represent an early pathophysiological feature (Dunleavy et al., Reference Dunleavy, Elsworthy, Upthegrove, Wood and Aldred2022). Complement activation, kynurenine pathway alterations, and T-cell dysregulation have also been described across meta-analytic studies, highlighting the need for integrative, system-wide approaches (de Bartolomeis et al., Reference de Bartolomeis, Fornaro, Scopetta, Ricci, Irano, De Simone, Comai, Iasevoli and Caiazza2025; Su et al., Reference Su, Su, Tang, Chen, Su, Chen and Zhang2025).
This study aims to comprehensively examine immunological mechanisms in first-episode psychosis (FEP) by assessing cellular, humoral, and acute-phase inflammatory parameters in a first episode and substance-free cohort. While previous studies often focused on isolated immune markers or subgroups, our design offers an integrative perspective by investigating the interplay among multiple immunological subsystems within the same patient sample. In doing so, we seek to move beyond reductionist approaches and highlight the necessity of a systems-level understanding. Just as neural circuits cannot be fully understood in isolation from one another, immune subsystems – such as cellular immunity, complement pathways, and antibody-mediated responses – must be evaluated in relation to each other to better elucidate their roles in psychosis onset and progression. By minimising confounders and prioritising internal consistency, our approach provides novel insight into early immune alterations in psychosis and their possible prognostic implications.
Methods
Sample and participants
Patients were recruited from the outpatient clinics and emergency department of Ege University Faculty of Medicine, Department of Psychiatry. Inclusion criteria for the patient group were: first-time presentation with psychotic symptoms; no history of manic episodes; absence of diagnostic criteria for psychotic depression or manic episodes at admission; and no diagnosis of alcohol use disorder or history of substance use. We excluded individuals with a lifetime history of psychotropic medication use exceeding one month, regardless of indication (e.g., prior depressive or anxiety episodes). However, if they had used antipsychotic or mood stabiliser medication at any time before the time of application, even for less than 1 month, they were not included in the study. This criterion ensured that long-term or substantial psychotropic exposure – which may influence immune parameters – did not confound baseline measurements.
Healthy controls were selected among individuals with no prior diagnosis of chronic or recurrent psychiatric disorders and who did not meet diagnostic criteria at the time of evaluation for psychotic disorders, depression, mood disorders, anxiety disorders, obsessive-compulsive disorder, post-traumatic stress disorder, or alcohol use disorder. They also had no history of substance use.
Individuals with any somatic or systemic condition that could influence immune parameters were excluded. This included: (a) chronic or acute inflammatory, autoimmune, endocrine, or infectious diseases; (b) cardiometabolic disorders such as diabetes or hypertension; and (c) regular use of anti-inflammatory, immunomodulatory, corticosteroid, or other medications known to affect immune function, and none had first-degree relatives with such conditions. Only individuals who met all inclusion criteria and volunteered to participate were included in the sample.
Study procedure
The first phase of the study was conducted as part of an observational protocol led by T.S. All patients who met the inclusion and exclusion criteria were invited to participate. At least six months later, each participant was re-contacted by phone and invited for a follow-up assessment, which constituted the second phase of the study, coordinated by Dr. Ö.Ö. Healthy controls were evaluated only during the first phase. Healthy controls were recruited from hospital staff, university students, and community volunteers with no history of psychiatric or chronic medical disorders.
Accordingly, all patients underwent assessments at two time points: T1 (baseline) and T2 (six months later). During both assessments, a standardised case report form was completed, documenting sociodemographic data, systemic review, comorbid medical conditions, and current treatments. Diagnostic evaluation was conducted using validated forms of the Structured Clinical Interview for DSM Disorders (SCID-I), and symptom severity was assessed using PANSS and the Brief Psychiatric Rating Scale (BPRS) (Andersen et al., Reference Andersen, Larsen, Kørner, Nielsen, Schultz, Behnke and Bjørum1986; Kostakoğlu et al., Reference Kostakoğlu, Batur, Tiryaki and A. ve Göğüş1999; Özkürkçügil et al., Reference Özkürkçügil, Aydemir, Yıldız, Esen Danacı and Ertuğrul1999).
To minimise bias in symptom assessment, clinicians were blinded to participants’ baseline laboratory and clinical data. The first set of assessments was performed by T.S, and the second by Ö.Ö.
Following each clinical evaluation, venous blood samples were collected to analyse immunological parameters. Laboratory tests included complete blood count (CBC), CRP, ferritin, SAA, immunoglobulins (IgG, IgA, IgM, IgE), complement components (C3, C4). All samples were delivered on the same day by the evaluating clinician to the Biochemistry and Immunology Laboratories of Ege University Medical Faculty Hospital. Blood samples were collected between 08:00 and 10:00 a.m. after overnight fasting. CBC parameters were analysed using an automated haematology analyser. CRP, SAA and ferritin were measured using nephelometric assays. Complement components and immunoglobulins were quantified via turbidimetric immunoassay. All samples were processed on the same day.
At T1, blood samples were drawn at the first clinical presentation, prior to or within a few days of antipsychotic initiation. In all cases, antipsychotic exposure before T1 did not exceed three days. Given the minimal and heterogeneous duration of exposure and the small follow-up sample (n = 20), we did not statistically adjust for antipsychotic treatment.
Statistical analysis
All statistical analyses were performed using SPSS version 22 (Statistical Package for the Social Sciences). Independent variables included age, sex, and immunological parameters obtained at baseline (T1) and follow-up (T2). Dependent variables were symptom severity scores assessed via the PANSS and BPRS.
To compare baseline blood parameters (T1) between patients and healthy controls, independent samples t-tests were used for normally distributed variables and Mann–Whitney U tests for non-normally distributed variables. Normality of continuous variables was assessed using skewness and kurtosis values, with distributions between –1.5 and +1.5 considered approximately normal.
To evaluate within-subject changes across time points (T1 vs. T2), paired samples t-tests (for normally distributed data) and Wilcoxon signed-rank tests (for non-normally distributed data) were conducted. This allowed differentiation between state-dependent markers (those that changed over time) and trait markers (those that remained stable).
In addition, correlations between immunological parameters (at both time points) and symptom severity (PANSS and BPRS scores) were analysed using Pearson’s correlation for normally distributed variables and Spearman’s rank correlation for others. Then, all correlations were re-run after excluding the patients whose diagnosis evolved to bipolar disorder at follow-up. Correlations between changes in blood levels of immunological markers and changes in symptom severity over time were also examined.
ROC analysis was performed to evaluate the diagnostic utility of inflammatory markers – found to be elevated in patients compared to healthy controls at both time points – for predicting disease status at T1. Based on optimal cut-off values, these markers were dichotomised (high/low) and included in a logistic regression analysis along with sociodemographic variables. Due to the small sample size and intercorrelations among several predictors, not all variables were included in the model. Model fit was assessed using the Hosmer–Lemeshow test.
A significance threshold of p < 0.05 was applied for all analyses.
Results
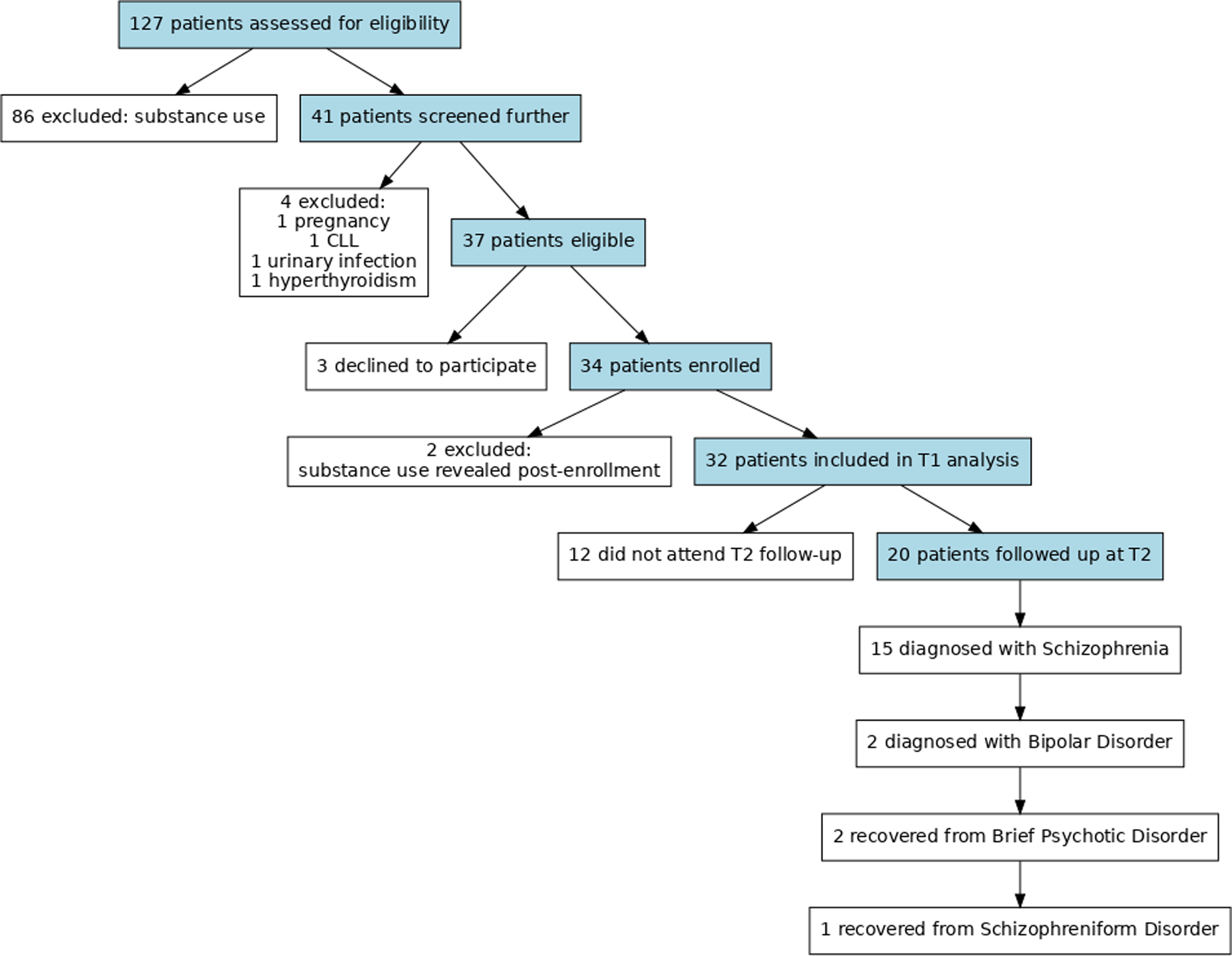
A total of 127 patients were initially referred for participation. As illustrated in Figure 1, 86 individuals were excluded due to substance use, either self-reported or confirmed by routine urine toxicology screening. One patient was excluded due to pregnancy and the potential confounding physiological changes associated with it. Another patient was excluded despite being in remission due to a prior diagnosis of chronic lymphocytic leukaemia (CLL). One male patient with a urinary tract infection and another under follow-up for hyperthyroidism were also excluded.
Flowchart of participant recruitment and follow-up. The diagram illustrates participant screening, exclusion criteria, baseline inclusion (T1), and follow-up assessment (T2) in the first-episode psychosis cohort.

Three patients declined to participate after initial eligibility screening. Two additional patients were excluded post-consent when they disclosed substance use after remission and blood sampling. In total, 32 patients were included in the initial phase of the study (T1). At baseline, 56% of the patients (18/32) had been diagnosed with brief psychotic disorder and 44% (14/32) with schizophreniform disorder.
A control group of 26 healthy volunteers with similar sociodemographic characteristics was included. Due to the onset of the COVID-19 pandemic, recruitment was halted, and the study was concluded with the available sample size. To prevent heterogeneity, no additional data were collected during or after the pandemic or vaccination periods.
All 32 patients included in the initial phase of the study (T1) were contacted by phone at least six months after their initial assessment and invited to participate in the follow-up phase (T2). Two patients could not be reached via the contact information previously provided. Four patients reported relocating to another city and were unable to return to the hospital. Six patients declined participation, stating that they either felt recovered or were currently receiving treatment at another facility. Consequently, 20 patients were included in the follow-up phase (T2). The second assessments were conducted on average 374.25 days after the first interview (range: 208–564 days). At follow-up, the diagnostic distribution had changed: 75% (15/20) met the criteria for schizophrenia, 10% (2/20) for bipolar disorder, 10% (2/20) had recovered from brief psychotic disorder, and 5% (1/20) had recovered from schizophreniform disorder as shown in Figure 1.
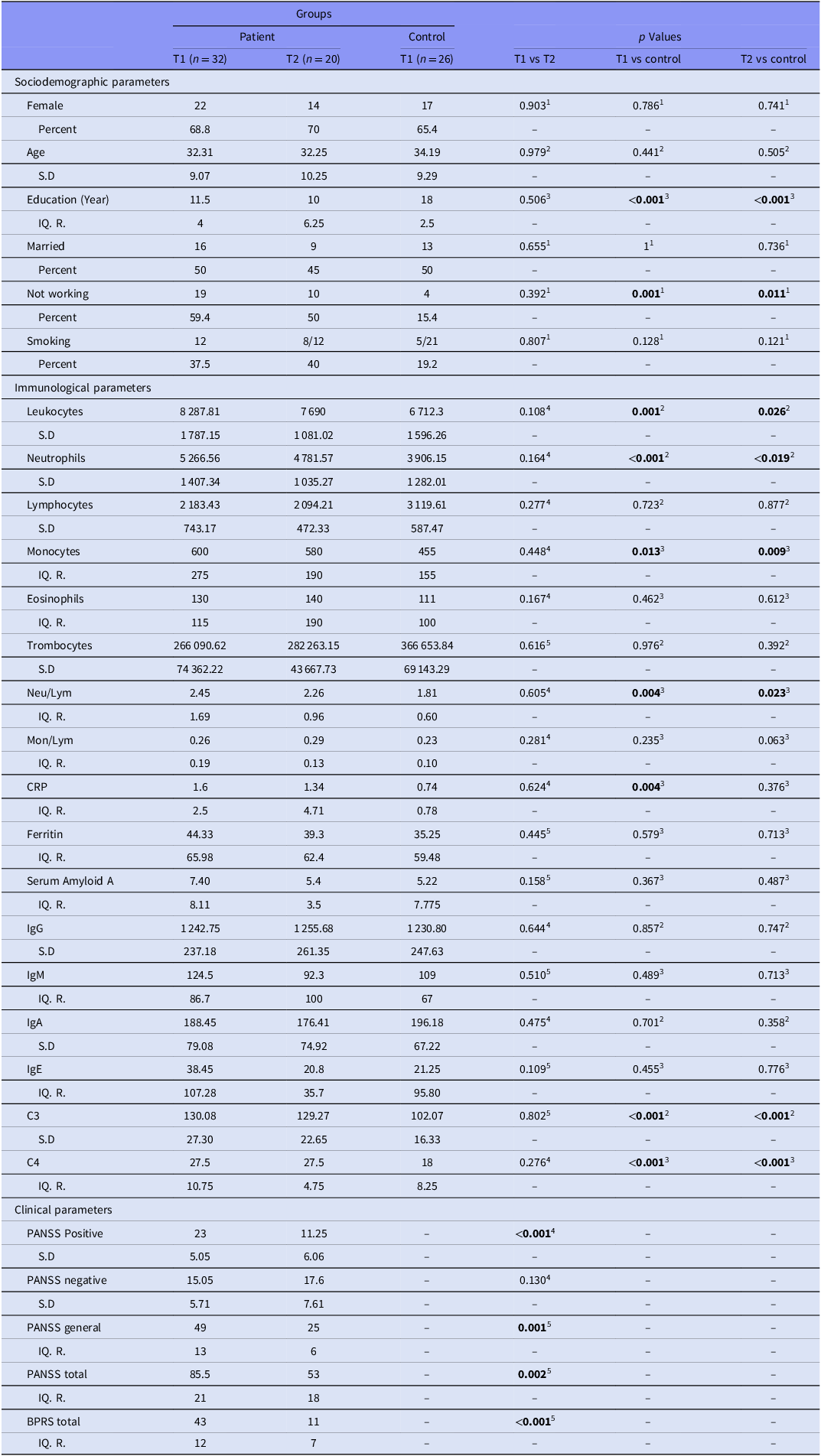
A comparison of the sociodemographic characteristics of patients and controls is presented in Table 1. No statistically significant differences were found between the groups in terms of age, gender, marital status, employment, or smoking status. However, years of education were significantly lower and unemployment was higher in the patient group. There were no significant sociodemographic differences between the patients who participated in both phases (T1,T2) and those who participated only in the first phase (T1).
Descriptive analysis of the cohort

Neu/Lym, neutrophils/lymphocytes; Mon/Lym, monocytes/lymphocytes; CPR, C-reactive protein; IgG, Immunoglobulin-G; IgM, Immunoglobulin-M; IgA, Immunoglobulin-A; IgE, Immunoglobulin-E; C3, complement-3; C4, complement-4; PANSS, positive and negative syndrom scale; BPRS, brief psychiatric rating scale; S.D, standart deviation; IQ.R, interquartile range.
Bold values indicate statistical significance (p < 0.05).
1 Chi-square test.
2 Independent samples t test.
3 Mann–Whitney U test.
4 Paired t test.
5 Wilcoxon test.
Regarding immunological parameters, leukocyte, neutrophil, monocyte counts, C3, C4 levels, and the neutrophil-to-lymphocyte ratio were all significantly elevated in patients compared to healthy controls at T1and T2, and CRP was just elevated in T1 as shown in Table 1. Regarding immunological parameters, none of the previously altered biomarkers showed a statistically significant change between T1 and T2.
Changes in patients’ mean PANSS and BPRS scores are presented in Table 1. After approximately one year of follow-up (T2), significant reductions were observed in PANSS positive (PANNS-P), PANSS general (PANNS-G), PANSS total (PANSS T), and BPRS scores compared to T1. No significant change was detected in the PANSS negative (PANSS-N) subscale.
Correlations between symptom severity and immunological parameters
Patient age at baseline, years of education, and follow-up duration were also tested for correlations with clinical scale scores. Follow-up duration was examined only in relation to clinical status at T2. No statistically significant associations were found between these demographic variables and clinical outcomes at any time point.
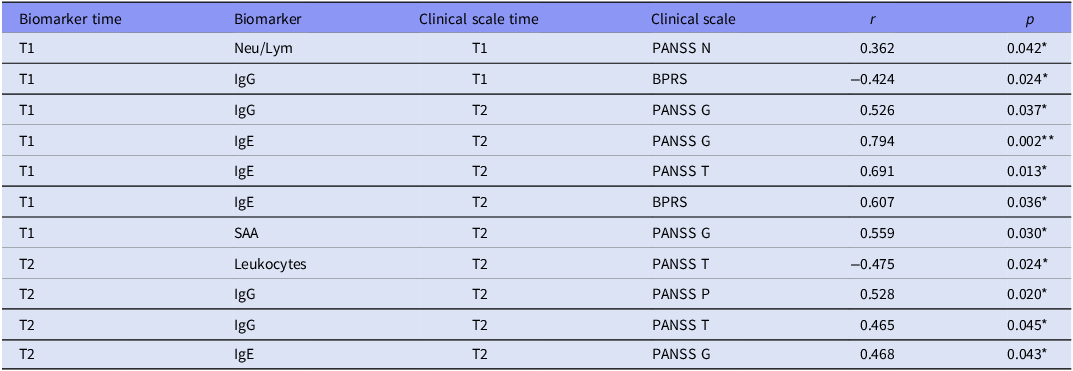
Table 2 presents the immunological markers that showed significant correlations with symptom severity at either T1 or T2. At T1, the NLR was positively correlated with PANSS-N scores. IgG levels were negatively correlated with BPRS score.
Correlations between symptom severity and immunological parameters

All analyses were conducted using Spearman correlation due to non-normality.
* p < 0.05.
** p < 0.01.
At T2, leukocyte counts were negatively correlated with PANSS-T. IgG was positively correlated with both PANSS-P and PANSS-T score. IgE was correlated positively with PANS-G.
IgE at T1 showed a positive correlation with PANS-G, PANSS-T, and BPRS scores at T2. Additionally, SAA at T1 was negatively correlated with PANSS-G at T2. IgG levels at T1 were positively correlated with PANSS-G scores at T2. Among clinical scales, only PANSS-N scores at T1 were significantly and positively correlated with PANSS negative scores at T2 as expected. Of all the biomarkers associated with clinical outcomes, only IgE levels at T1 and T2 were significantly correlated with each other (r = 0.953, p < 0.001); this result is not shown in the tables.
As a sensitivity analysis, all correlations were re-run after excluding the two patients whose diagnosis evolved to bipolar disorder at follow-up. Although this resulted in minor numerical fluctuations in the correlations, the overall system-level interpretation remained unchanged: cellular immune markers (neutrophils, neutrophil/lymphocyte ratio) were negatively associated with T2 symptom severity, while humoral markers (IgG, IgE) showed positive associations with T2 symptom dimensions. This stability confirms that our findings are robust to diagnostic trajectory.
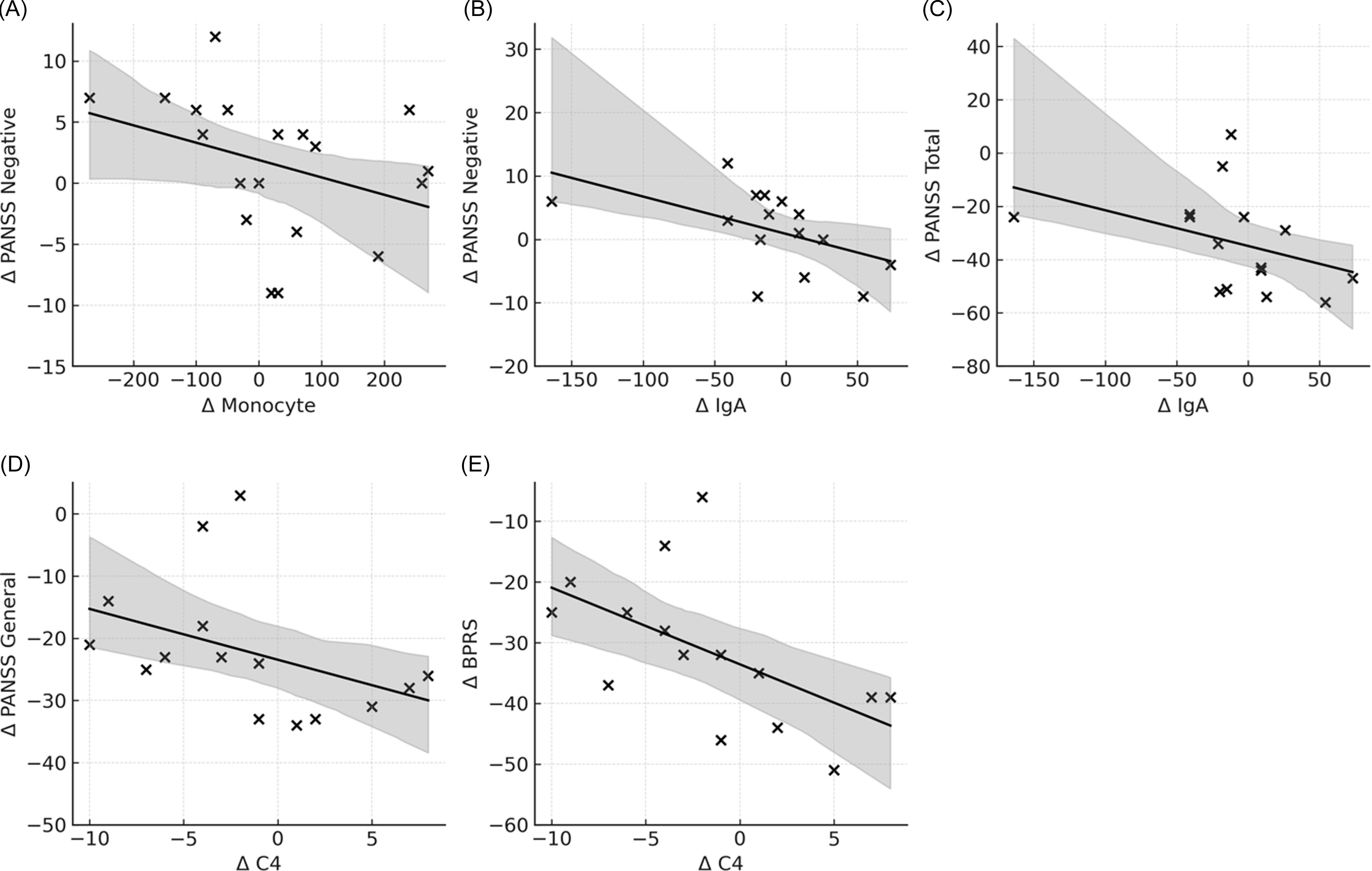
Analysis of Δ biomarker–Δ symptom relationships from T1 to T2 revealed significant negative correlations: changes in monocyte levels were associated with changes in PANSS negative scores (r = –0.490, p = 0.033); changes in IgA were correlated with changes in PANSS negative (r = –0.578, p = 0.024) and PANSS total scores (r = –0.519, p = 0.048); and changes in C4 were related to changes in PANSS general psychopathology (r = –0.651, p = 0.009) and BPRS scores (r = –0.684, p = 0.005), presented in Figure 2.
Associations between changes in immunological markers and symptom severity over time. Scatter plots depict correlations between Δ (T2–T1) changes in selected immune parameters and changes in PANSS scores. Solid lines represent linear regression fits.

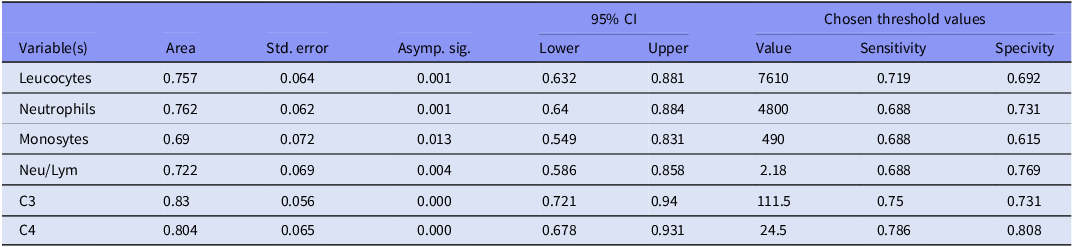
ROC analysis and logistic regression
ROC analysis was conducted to evaluate the diagnostic utility of inflammatory markers that were elevated in patients compared to healthy controls at both time points in predicting disease status at T1. The results of the ROC analysis, along with the selected cut-off values, are presented in Table 3.
ROC analysis for immunological parameters and chosen thresholds at T1

Neu/Lym, neutrophils/lymphocytes; C3, complement-3; C4, complement-4.
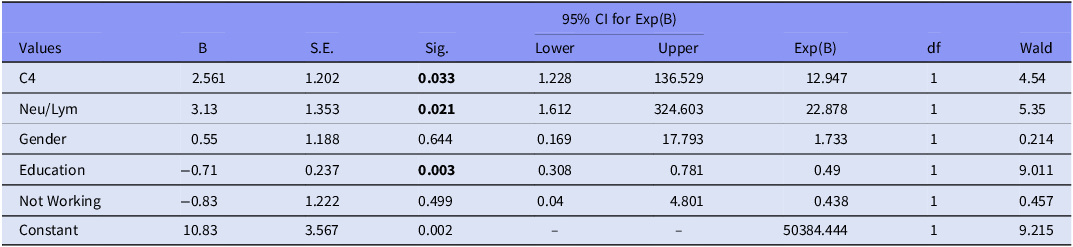
Among sociodemographic variables, gender, education level (years of education), and employment status (unemployment) were included in the model, as education and employment differed significantly between groups. Age was excluded due to a strong correlation with years of education. To reduce multicollinearity and improve model interpretability, C4 was selected to represent the humoral immune system and the NLR for cellular immunity, as they showed relatively higher sensitivity and specificity.
Model fit was assessed using the Hosmer–Lemeshow test (p = 0.964), and the Nagelkerke R 2 value was 0.830, indicating good overall model performance. According to the regression results, higher levels of C4 and NLR, as well as fewer years of education, were significantly associated with being in the patient group. In contrast, gender and unemployment did not have a significant effect, presented in Table 4.
The logistic regression model applied according to chosen threshold values to predict FEP at T1

Bold values indicate statistical significance (p < 0.05).
Hosmer–Lemeshow: p = 0.964; Nagelkerke R 2 = 0.830.
Neu/Lym, neutrophils/lymphocytes; C3, complement-3; C4, complement-4.
The C4 and Neu/Lym levels represent high blood levels according to the threshold values specified in Table 3.
Discussion
In this longitudinal cohort of first-episode psychosis, we found a persistent elevation of innate immune markers (leukocytes, neutrophils, monocytes and NLR) across both acute and remission phases, supporting a trait-like inflammatory pattern. Complement components C3 and C4 were also consistently elevated, whereas CRP behaved as a state-dependent marker restricted to the acute phase. By contrast, immunoglobulin profiles showed phase-specific associations with symptoms, and both NLR and C4 demonstrated predictive value in distinguishing patients from controls. These findings highlight differential and dynamic involvement of innate and adaptive mechanisms in psychosis. Diagnostic shifts after one year are expected in FEP cohorts. Importantly, sensitivity analyses excluding the two participants who developed bipolar disorder did not alter the pattern of immunological associations.
Consistent with previous studies, including Zahorec’s foundational work and subsequent findings in psychosis populations (Varsak et al., Reference Varsak, Aydin and Eren2015; Yüksel et al., Reference Yüksel, Ertek, AUğraş and Göka2018; Mazza et al., Reference Mazza, Lucchi, Rossetti and Clerici2019; Clausen et al., Reference Clausen, Christensen, da Re and Benros2024), our results demonstrated persistently elevated leukocyte, neutrophil, monocyte counts, and NLR in patients compared to healthy controls. These markers remained unchanged over time, suggesting a sustained inflammatory state and its potential role as a trait marker in first-episode psychosis. Meta-analyses by Jackson and Miller (Reference Jackson and Miller2020) and Mazza et al. (Reference Mazza, Lucchi, Rossetti and Clerici2019) have shown that leukocyte, neutrophil, monocyte levels, as well as NLR and monocyte-to-lymphocyte (MLR) ratios, are elevated in both schizophrenia and FEP compared to healthy controls (Dudeck et al., Reference Dudeck, Nussbaumer, Nickl-Jockschat, Guest, Dobrowolny, Meyer-Lotz, Zhao, Jacobs, Schiltz, Fernandes and Steiner2025). In longitudinal studies, NLR and MLR remained elevated in FEP despite partial symptom improvement, with only modest reductions over time (Steiner et al., Steiner et al., Reference Steiner, Frodl, Schiltz, Dobrowolny, Jacobs, Fernandes, Guest, Meyer-Lotz, Borucki, Bahn, Bogerts, Falkai and Bernstein2020; Bioque et al., Reference Bioque, Catarina Matias-Martins, Llorca-Bofí, Mezquida, Cuesta, Vieta, Sílvia, Lobo, González-Pinto, Moreno, Roldán, Martinez-Aran, Baeza, Bergé, García-Rizo, Mas Herrero, Bernardo, González, Álvaro, Recio, Selma, Tonda, García-Corres, Jéssica, Cón, Modrego-Pardo, Jé, Pérez-Rando, Vázquez, Cristeto, Sanchez-Moreno, Gimenez-Palomo, Castro-Fornieles, de la Serna, Contreras, González-Blanco, Sáiz, Gutiérrez-Fraile, Zabala, Sanchez-Pastor, Rodriguez-Jimenez, Usall, Butjosa, Pomarol-Clotet, Sarró, Ibáñez Ángela, Sánchez-Torres and Balanzá2022; Wang et al., Reference Wang, Chen, Guan and Li2024). Monocyte-related markers were more stable, showing limited change even after extended follow-up.
In line with this literature, CRP was elevated only at baseline in our cohort and normalised at follow-up, supporting its role as a state-dependent marker of acute exacerbation rather than a persistent inflammatory trait (Lestra et al., Reference Lestra, Romeo, Martelli, Benyamina and Hamdani2022; Halstead et al., Reference Halstead, Siskind, Amft, Wagner, Yakimov, Shih-Jung Liu, Walder and Warren2023; Su et al., Reference Su, Su, Tang, Chen, Su, Chen and Zhang2025). Correlation analyses revealed that NLR at T1 was positively associated with PANSS negative scores, while IgG at T2 correlated positively with PANSS positive scores. These findings suggest that in the acute phase, innate immune activation may be linked to negative symptoms, whereas in remission, adaptive immunity may be more closely related to positive symptom severity (Rodrigues-Neves et al., Reference Rodrigues-Neves, AónioF and Gomes2022). Additionally, leukocyte count, SAA, and IgE levels did not correlate with positive or negative symptoms but showed associations with general psychopathology scores (PANSS general, PANSS total, and BPRS). This pattern may indicate that these markers are more closely linked to broader symptom domains such as affective symptoms, cognitive impairments, or somatic complaints. The study that clozapine reduces both total immunoglobulin levels and symptom severity in treatment-resistant schizophrenia further supports this notion (Griffiths et al., Reference Griffiths, Mellado, Chung, Lally, McQueen, Sendt, Gillespie, Ibrahim, Richter, Shields, Ponsford, Jolles, Hodsoll, Pollak, Upthegrove, Egerton and MacCabe2024).
Our findings align with this literature: leukocyte, neutrophil, monocyte counts and NLR were significantly elevated in the patient group at both time points, and high baseline NLR was associated with increased likelihood of being in the psychosis group. No significant within-patient changes were observed over time. Correlation analyses further revealed a positive association between NLR and PANSS negative scores at baseline and a negative association between leukocyte count and PANSS total scores at follow-up. However, as reported in previous studies, the relationships between inflammatory markers and symptom domains remain inconsistent across samples (Steiner et al., Steiner et al., Reference Steiner, Frodl, Schiltz, Dobrowolny, Jacobs, Fernandes, Guest, Meyer-Lotz, Borucki, Bahn, Bogerts, Falkai and Bernstein2020; Leung et al., Reference Leung, Wong, Shea, Chan, Chang, Mo and Chan2023; Wang et al., Reference Wang, Chen, Guan and Li2024; Dudeck et al., Reference Dudeck, Nussbaumer, Nickl-Jockschat, Guest, Dobrowolny, Meyer-Lotz, Zhao, Jacobs, Schiltz, Fernandes and Steiner2025).
CRP is a sensitive marker of systemic inflammation, known to rise during acute psychotic episodes and decrease during remission or treatment (Singh & Chaudhuri, Reference Singh and Chaudhuri2014; Bora, Reference Bora2019; Lestra et al., Reference Lestra, Romeo, Martelli, Benyamina and Hamdani2022). Several studies have identified elevated CRP levels in both schizophrenia and first-episode psychosis, independent of antipsychotic use, and have linked CRP to symptom exacerbations (Miller et al., Reference Miller, Buckley, Seabolt, Mellor and Kirkpatrick2014; Fernandes et al., Reference Fernandes, Steiner, Bernstein, Dodd, Pasco, Dean, Nardin, Gonçalves and Berk2016; Delaney et al., Reference Delaney, Fallon, Alaedini, Yolken, Indart, Feng, Wang and Javitt2019; Fond et al., Reference Fond, Godin, Boyer, Berna, Andrianarisoa, Coulon, Brunel, Bulzacka, Aouizerate, Capdevielle, Chereau, D’Amato, Dubertret, Dubreucq, Faget, Leignier, Lançon, Mallet, Misdrahi, Passerieux, Rey, Schandrin, Urbach, Vidailhet, Llorca, Schürhoff and Leboyer2019; Noto et al., Reference Noto, Maes, Nunes, Ota, Rossaneis, Verri, Cordeiro, Belangero, Gadelha, Bressan and Noto2019; Steiner et al., Steiner et al., Reference Steiner, Frodl, Schiltz, Dobrowolny, Jacobs, Fernandes, Guest, Meyer-Lotz, Borucki, Bahn, Bogerts, Falkai and Bernstein2020;). Some evidence also suggests associations with cognitive impairment (Dickerson et al., Reference Dickerson, Schroeder, Stallings, Origoni, Katsafanas, Schwienfurth, Savage, Khushalani and Yolken2014; Misiak et al., Reference Misiak, Stańczykiewicz, Kotowicz, Rybakowski, Samochowiec and Frydecka2018; Fathian et al., Reference Fathian, Løberg, Gjestad, Steen, Kroken, Jørgensen and Johnsen2019), although results remain mixed (Hope et al., Reference Hope, Hoseth, Dieset, Mørch, Aas, Pål, Djurovic, Melle, Ueland, Agartz, Ueland, Westlye and Andreassen2015).
Early studies from the 1960s and 1970s reported altered immunoglobulin profiles in psychotic patients, including elevated IgG and IgA levels, though findings were inconsistent and limited by outdated methodologies (Solomon, Reference Solomon1969; Allansmith et al.,1973; Pulkkinen & Soininvaara, Reference Pulkkinen and Soininvaara1985). More recent research has renewed interest in humoral immunity. Elevated IgM levels were reported in schizophrenia (Keshel et al., Reference Keshel, Sadough, Omidinia and Rahmanzadeh2013), while a more recent study found reduced total IgG and IgG1 levels in both schizophrenia and bipolar disorder (Hamdani et al., Reference Hamdani, Bengoufa, Oélia, Rël, Le Guen, Daban-Huard, Bennabi, Delavest, Lépine, Boukouaci, Laouamri, Houenou, Séphane, Richard, Lecorvosier, Yolken, Rajagopal, Leboyer and Tamouza2018; Maes et al., Reference Maes, Kanchanatawan, Sirivichayakul and Carvalho Aé2019). However, (Delaney et al., Reference Delaney, Fallon, Alaedini, Yolken, Indart, Feng, Wang and Javitt2019) found no significant differences in immunoglobulin levels among ultra-high risk (UHR), FEP, and control groups. These findings suggest potential immunoglobulin alterations in psychosis, though the direction and clinical significance remain to be clarified (Pollak et al., Reference Pollak, Rogers, Nagele, Peakman, Stone, David and McGuire2018). The inverse association between ΔIgA levels and changes in negative symptom severity further supports a role for mucosal–immune interactions in symptom persistence, as emerging evidence suggests that IgA-mediated regulation of gut microbiota composition and barrier integrity may influence low-grade systemic inflammation and neurobehavioral outcomes (Maes et al., Reference Maes, Kanchanatawan, Sirivichayakul and Carvalho Aé2019). Our findings extend prior work by showing that IgG was negatively associated with global symptom severity at baseline but positively associated with positive and total symptoms during remission. This shift suggests a phase-dependent involvement of adaptive immunity, potentially reflecting compensatory or regulatory responses emerging after acute stabilisation.
Dysregulation of the complement system has been implicated in schizophrenia pathophysiology (Mayilyan et al., Reference Mayilyan, Arnold, Presanis, Soghoyan and Sim2006; Nimgaonkar et al., Reference Nimgaonkar, Prasad, Chowdari, Severance and Yolken2017; Cropley et al., Reference Cropley, Kittel, Heurich, Föcking, Leweke and Pantelis2023; Zhang et al., Reference Zhang, Zeng, Ye, Gao, Hu, Xu, Wei, Tang, Liu, Chen, Li, Wan and Wang2023; Su et al., Reference Su, Su, Tang, Chen, Su, Chen and Zhang2025), with evidence suggesting it may contribute to aberrant synaptic pruning (Sekar et al., Reference Sekar, Bialas, de Rivera, Davis, Hammond, Kamitaki, Tooley, Presumey, Baum, Van Doren, Genovese, Rose, Handsaker, Carroll, Stevens and McCarroll2016). Multiple studies have reported elevated C3 and C4 levels in patients with schizophrenia and psychosis (Boyajyan et al., Reference Boyajyan, Khoyetsyan and Chavushyan2010; Nimgaonkar et al., Reference Nimgaonkar, Prasad, Chowdari, Severance and Yolken2017; Zhang et al., Reference Zhang, Zeng, Ye, Gao, Hu, Xu, Wei, Tang, Liu, Chen, Li, Wan and Wang2023), with some findings indicating even higher levels in untreated individuals. However, results remain inconsistent: some studies found no significant differences between patients and controls (Morgan et al., Reference Morgan, Kopczynska, Zelek, Touchard, O’Donovan, Murray, Mondelli and Gaughran2017; Laskaris et al., Reference Laskaris, Zalesky, Weickert, Di Biase, Chana, Baune, Bousman, Nelson, McGorry, Everall, Pantelis and Cropley2019), while others reported elevation in only one component (Cropley et al., Reference Cropley, Kittel, Heurich, Föcking, Leweke and Pantelis2023). Similar to CRP and cell count parameters, neither complement level was associated with symptom severity, echoing previous reports of inconsistent relationships between complement activity and clinical presentation (Enache et al., Reference Enache, Nikkheslat, Fathalla, Morgan, Sôn, Drake, Deakin, Walters, Lawrie, Egerton, MacCabe and Mondelli2021; Zhang et al., Reference Zhang, Zeng, Ye, Gao, Hu, Xu, Wei, Tang, Liu, Chen, Li, Wan and Wang2023; Su et al., Reference Su, Su, Tang, Chen, Su, Chen and Zhang2025).
The pattern of Δ correlations suggests that patients whose monocyte, IgA and C4 levels remained more stable over time showed greater symptomatic improvement, consistent with a regulated rather than fully suppressed immune tone (Susai et al., Reference Susai, Föcking, Mongan, Heurich, Coutts, Egerton, Whetton, Winter-van Rossum, Unwin, Pollak, Weiser, Leboyer, Rujescu, Byrne, Gifford, Dazzan, Koutsouleris, Kahn Ré, Cotter and McGuire2023). Monocytes and complement components such as C4 have been repeatedly implicated as bridges between innate and adaptive responses in psychosis, and slower declines in these markers may reflect a homeostatic or compensatory immune profile that supports recovery (Susai et al., Reference Susai, Föcking, Mongan, Heurich, Coutts, Egerton, Whetton, Winter-van Rossum, Unwin, Pollak, Weiser, Leboyer, Rujescu, Byrne, Gifford, Dazzan, Koutsouleris, Kahn Ré, Cotter and McGuire2023; van der Walt et al., Reference van der Walt, Stein and Zoghbi2025). This interpretation is broadly consistent with a large body of literature demonstrating elevated pro-inflammatory cytokines (e.g., interleukin-6, interleukin-1β) and interferon-related signalling during acute psychotic episodes, followed by partial normalisation during remission, suggesting dynamic rather than static immune dysregulation (Hubbard & Miller, Reference Hubbard and Miller2019; Enache et al., Reference Enache, Nikkheslat, Fathalla, Morgan, Sôn, Drake, Deakin, Walters, Lawrie, Egerton, MacCabe and Mondelli2021; de Bartolomeis et al., Reference de Bartolomeis, Fornaro, Scopetta, Ricci, Irano, De Simone, Comai, Iasevoli and Caiazza2025). Taken together, our longitudinal findings are broadly compatible with a model in which an initially dysregulated immune state gradually shifts toward a more regulated configuration. Reduced blood levels may also reflect migration of immune components from the circulation into tissues. Monocytes and C4 can cross the more permeable blood–brain barrier in schizophrenia and contribute to synaptic pruning, while IgA has been implicated in the gut–brain axis (Maes et al., Reference Maes, Kanchanatawan, Sirivichayakul and Carvalho Aé2019). However, these immune elements are also locally produced within tissues, and circulating IgA does not necessarily reflect mucosal activity. Therefore, peripheral immune measures may not directly represent tissue-level processes. However, this interpretation remains speculative, as tissue-specific immune activity was not directly assessed in our study.
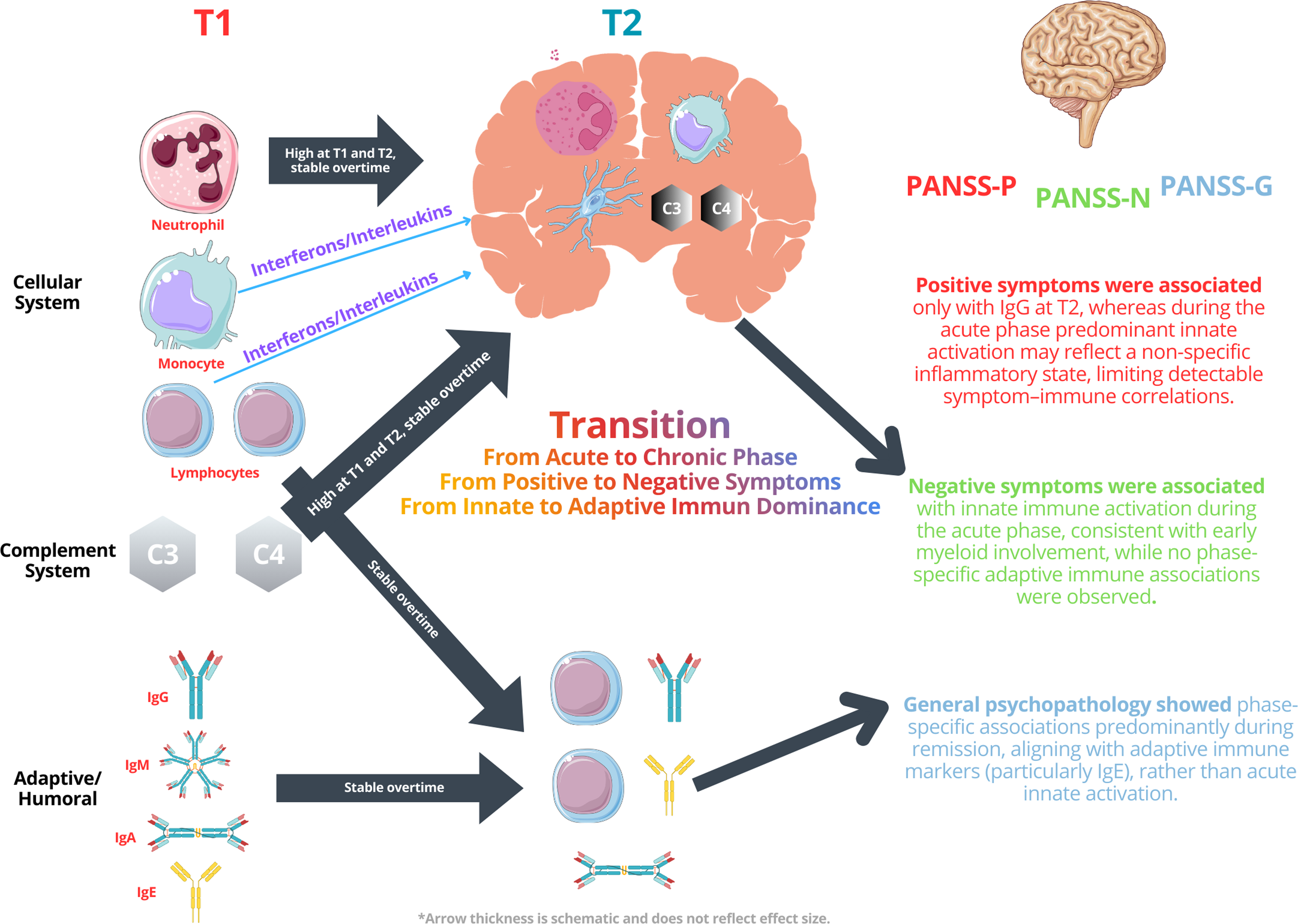
A systems-level integration of our results suggests that psychosis may arise from a coordinated disturbance across multiple immune subsystems rather than isolated abnormalities in individual markers. The stable elevation of neutrophils and monocytes in both phases of illness is consistent with early myeloid activation, which has been proposed proposed to parallel changes in microglial functional states rather than microglial density or transcriptional profiles in psychosis (Snijders et al., Reference Snijders, van Zuiden, Sneeboer, Berdenis van Berlekom, van der Geest, Schnieder, MacIntyre, Hol, Kahn Ré and de Witte2021; Zhuo et al., Reference Zhuo, Tian, Song, Jiang, Chen, Cai, Ping, Cheng, Zhou and Chen2023). Elevation of complement factors C3 and C4 – key mediators linking innate responses with synaptic regulation – may represent a downstream amplification of this process. In contrast, the phase-specific associations of IgG and IgE with symptom domains at T2 point toward a delayed engagement of adaptive immunity, potentially reflecting compensatory or regulatory mechanisms. This pattern supports a model in which innate pathways predominate during acute exacerbation, whereas adaptive signatures modulate symptom expression during remission. Rather than viewing these abnormalities as independent phenomena, our findings align with a dynamic, interconnected immune network in which subsystem interactions shape both illness onset and symptom trajectories, as shown in Figure 3.
System-level model of immune dysregulation across illness phases in first-episode psychosis. The schematic summarises the proposed interaction between innate immune activation during the acute phase and adaptive immune involvement during remission, based on longitudinal findings of the present study.
Source: Image(s) adopted by Servier Medical Art (https://smart.servier.com), licensed under CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/).

To sum-up, our findings support the presence of a persistent, low-grade inflammatory state in first-episode psychosis, marked by stable elevations in both innate and adaptive immune markers. While individual parameters offer valuable information, their diagnostic and clinical relevance becomes more apparent when interpreted within a system-level framework. This integrated immunopsychiatric perspective may provide a more accurate understanding of the pathophysiological mechanisms underlying psychosis and guide future research toward personalised, immune-informed treatment strategies.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/neu.2026.10076.
Acknowledgements
This article is based on two medical specialty theses conducted at Ege University Faculty of Medicine: “Investigation of Immunological Parameters in First-Episode Psychosis” by T.S., and “Investigation of Immunological Parameters Six Months After Treatment in First-Episode Psychosis” by Ö.Ö. The study integrates and expands upon the data collected in both theses under a unified research framework.
We would like to express our special thanks to Dr Sibel Kaplan Sarıkavak and Dr Hande Özkalaycı for their scientific and motivational support throughout this study. We are also deeply grateful to our cats – Ruhi, Üzüm and Fıstık – and to Ozan Özkalaycı for their unwavering emotional support.
The authors thank all nurses of Ege University Medicine Faculty Department of Psychiatry for their contributions. We thank all our resident doctor colleagues for referring patients to participate in the study.
Author contributions
All authors made substantive intellectual contributions to the conceptualisation of our study. T.S. and Ö.Ö. facilitated the collection of patients’ and samples’ data, entered the data and conducted the statistical analysis, contributed to interpreting the analyses and preparing the draft. This article represents a merged publication based on both authors’ individual medical specialty theses. D.İ.H. and H.E. reviewed the interpretations of the analyses and the draft. E.N.M. and A.Z.S. ensured the review of the draft from an immunological perspective. T.S., Ö.Ö., and D.İ.H. finalised the draft.
Funding statement
This study was granted by TUBITAK (The Scientific and Technological Research Council of Turkey) with project number 119S188 and Ege University Office of Scientific Research Projects with the number 20934. The funding sources had no role in the study design, collection, analyses, and interpretation of the data, writing of the report, or the decision to submit the paper for publication.
Competing interests
We declare that there are no conflicts of interest among the authors.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Ethical approval was obtained from the Ege University Clinical Research Ethics Committee with decision number 18-3/35 dated 06.03.2018 and 19-4.1T/28 dated 17.04.2019.
Generative AI disclosure
During the preparation of this work, the authors used ChatGPT (OpenAI) to improve the readability of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the final version. All scientific content, analyses, and interpretations were developed solely by the authors.



 Open access
Open access