


Background
HAIs remain a significant unintended adverse outcome in patient care, posing a challenge to public health due to their substantial impact on patient morbidity, mortality, quality of life, and the economic burden on healthcare services. Reference Haque, Sartelli, McKimm and Abu Bakar1 The ongoing presence of HAIs indicates systemic deficiencies within healthcare delivery systems, despite the availability of simple, cost-effective prevention and control measures. Reference Schreiber, Sax, Wolfensberger, Clack and Kuster2 These deficiencies may be caused by a need for improved care quality and a gap in healthcare professionals” knowledge of HAI management. Reference Schreiber, Sax, Wolfensberger, Clack and Kuster2,Reference Ferguson3
The Breakthrough Series Collaborative (BTS) model is a well-known, widely used approach to drive improvement. 4 The BTS is defined by its short-term, collaborative learning system that encourages institutional growth through interactions with experienced teams and professionals. By employing structured, systematic, and auditable methods, the BTS model bridges the gap between the finest scientific evidence and everyday clinical practice, aiming to achieve significant improvements in patient care. 4
In 2017, the Brazilian Ministry of Health launched the quality improvement (QI) initiative called ‘Saúde em Nossas Mãos’ (SNM), aimed at reducing HAIs in intensive care units (ICUs). In the first three-years of activities (2018–2020), the SNM showed a significant decrease in the baseline incidence density of three critical HAIs: central line-associated bloodstream infections (CLABSI), ventilator-associated pneumonia (VAP), and catheter-associated urinary tract infections (CAUTI) by 43.5%, 52.1%, and 65.8% respectively, Reference Tuma, Vieira Junior and Ribas5 and confirmed as a value-based strategy for preventing HAIs. Reference Oliveira, de Sousa and de Salvo6 During the following three-years of activities (2021–2023), innovative Lean Healthcare tools were integrated into the BTS framework to enhance effectiveness and sustainability. We aimed to report the measured outcomes of this SNM scale-up phase, Reference Parry7 expanding the number of units studied across the Brazilian territory and including pediatric and neonatal ICUs.
Methods
Context
Brazil has implemented several health policies to improve the quality and safety of healthcare services, among which the National Healthcare-associated Infection Prevention and Control Program (Programa Nacional de Prevenção e Controle de Infecções Relacionadas à Assistência à Saúde) 8 and the National Patient Safety Policy (Política Nacional de Segurança do Paciente) 9 are the most representative. Both policies are integral to Brazil’s broader strategy to enhance the quality of healthcare services and patient outcomes. The SNM is embedded within these policies.
The Program for Institutional Development of the Unified Health System (Programa de Apoio ao Desenvolvimento Institucional do Sistema Único de Saúde – PROADI –SUS) 10 is a strategic initiative that establishes a partnership between public health institutions and six private, nonprofit hospitals of excellence to share knowledge, technology, and best practices to foster a more equitable, comprehensive, and high-quality public health system. PROADI-SUS resources fund the SNM.
Study design
A QI report presenting a retrospective analysis based on a quasi-experimental timeseries design of the SNM project. It involved a thorough one-year preintervention period from September 2020 to establish a baseline for the monthly incidence density of the analyzed HAIs. The intervention phase included rigorous monthly data collection to build a comprehensive database for scholarly analysis from September 2021 to December 2023. We adhered to the Standards for QI Reporting Excellence – SQUIRE 2.0 (Supplementary Material – Table 1S). 13
Settings and locations
The SNM invited all public adult, pediatric, and neonatal ICUs across Brazil, emphasizing voluntary participation without financial inducements. The 26 Brazilian states and the Federal District were represented by at least one participating ICU.
Participant selection and engagement strategy
Inclusion criteria focused on public or nonprofit hospitals with over 100 beds, including at least ten ICU beds, identified as high-complexity reference centers within their regions. Exclusion criteria aimed to omit institutions that required a structured quality department, an infection control committee, or leadership consent for participation, as these were considered essential for the effective implementation of the proposed QI activities. Following the nationwide open call, a thorough selection process engaged the first 204 qualifying ICUs, as determined by the project’s budget, prioritizing support and development for public institutions in accordance with the PROADI-SUS mission.
These participating ICU teams were combined with the following interdisciplinary members: intensive care physicians, nurses, respiratory therapists, nurse technicians, and at least one member of the infection control committee.
Intervention
Before launching, the SNM governance team convened a meeting of implementers, clinical experts, and hospital leaders to build consensus around the initiative’s aim, clinical intervention, and implementation strategy. The outputs of the meeting included (i) an aim to reduce HAIs by 50% from the baseline, with a focus on the three most prevalent HAIs, (ii) the clinical intervention (prevention bundles for each HAI), and (iii) the implementation approach addressing a set of system enablers, using QI methods and personalized clinical staff training delivered by a BTS.
The six QI teams, belonging to the six private hospitals of PROADI-SUS, consisted of interdisciplinary members representing key disciplines: infectious disease and intensive care physicians, nursing, respiratory therapists, technical nursing, and at least one member certified in improvement science.
The prevention bundles were based on the concept that a small set of clinical interventions applied together and directed at a specific clinical problem is a more effective clinical strategy than a piecemeal application. Reference Resar, Griffin, Haraden and Nolan11 The SNM infectious diseases experts’ team, including well-known Brazilian clinical and research infectiologists, established diagnostic criteria and treatment bundles for these three HAIs guided by national and international recommendations. Reference Glowicz, Landon and Sickbert-Bennett12–14
QI teams implemented engagement and empowerment strategies throughout the initiative, cultivating a multidisciplinary approach within ICU teams. These activities were performed equally in all the participating ICUs and included the following: (1) eight in-person learning sessions (one nationally and seven regionally) with the participation of 1,200 health professionals; (2) 14 virtual learning sessions with the participation of 4,385 and 2,314 participants respectively, (3) virtual immerse sessions (eight meetings) with the attendance of 15,815 professionals; and (4) reunions (550 visits including leadership huddles, technical encounters, and gatherings to commemorate good results), where more than 17,000 hours dedicated. The time line of these activities is described in the Supplementary Material – Table 2S.
The interventions were based on a dual-component approach, integrating technical issues (i.e., standardization of bundle elements and training all clinical staff on correct execution) and the socioadaptive component, including emphasized leadership engagement, multidisciplinary huddles, feedback loops using real-time visual management tools, and communication strategies to strengthen safety culture. An online platform was also established to facilitate ongoing professional support and the dissemination of educational materials and guidelines.
The learning sessions provided structured peer exchange, while hubs offered targeted one-on-one mentorship to address context-specific barriers. This combined approach ensured that ICUs could concurrently build technical skills and the behavioral conditions needed for sustained adoption. As an innovation, this initiative also incorporated educational games to enhance healthcare workers’ learning. Reference da Silva, Franco and Vieira15
Complementary approach
Lean Healthcare has been used to streamline processes, facilitate the identification and elimination of non-value-added activities, and improve the efficiency and effectiveness of HAI prevention practices. Reference Sartini, Patrone and Spagnolo16 Similarly, Training within Industry (TWI) is a structured methodology that focuses on job instruction, providing a systematic approach to enhancing healthcare professionals” skills and ensuring they are adequately trained. Reference Graupp and Wrona17
To sustain improvements, we used (i) the Kamishibai board, a visual management tool, which was essential for tracking compliance and quickly identifying areas for improvement, ensuring adherence to HAI prevention bundles, Reference Saavedra Bravo, Santos and Petenate18 and (ii) the TWI’s job instruction method was employed to enhance the skills of healthcare workers in the latest HAI prevention techniques, including each item of the prevention bundles. Reference Borem, de Moura and Dos Santos19
Outcomes
The summative assessment of the SNM interventions was based on HAI incidence densities. Diagnostic criteria adhered to the definitions of the National Health Surveillance Agency (Anvisa). 20 Each item of the prevention bundle and hand hygiene compliance was also followed up on, and they serve to formative assess the implementation.
Before implementing changes, support was provided to standardize clinical data entry and ensure the uniform reporting of quality metrics. ICU teams reported the monthly-aggregated data. The estimation of infections prevented was calculated as previously. Reference Tuma, Vieira Junior and Ribas5
Analytical approach
Shewhart U charts were used to monitor the incidence densities over the intervention period using the SimpleQI® platform. This strategy visualizes the continuous progress of key indicators and facilitates feedback and discussion between the QI and ICU teams. All incidence densities were reported per 1,000 devices-days, followed by the lower and upper control lines of the process monitoring.
Complementarily, for this report, graphical and decomposition analyzes of the time series were performed to identify trends and seasonality. The Cox-Stuart test and Fisher’s g were used to verify the significance of the trends and their seasonality, respectively. The Augmented Dickey-Fuller tests were used to verify the series” stationarity and graphical analyzes of autocorrelation and partial autocorrelation. Breakpoints of the time series were verified using the F statistic.
The time series between the two SNM phases was compared using the procedure described by Costa. 21 The residuals were analyzed using the Ljung-Box test. The cross-correlation function (CCF) was used to assess the correlation between time series at different time lags. Reference do RD de Latorre and Cardoso22 The double prewhitening technique proposed by Haugh and Box was used to address the problems listed above. Reference Haugh and Box23 The significance level adopted for these analyzes was 5%. The analyzes were performed in the R statistical programing language, version 4.1.1 (USA).
Results
Of the 204 ICUs initially selected, 16 withdrawals were reported by December 2023, leaving 188 ICUs included in this study: 169 adults, 11 pediatric, and 8 neonatal.
Impact on healthcare-associated infections globally
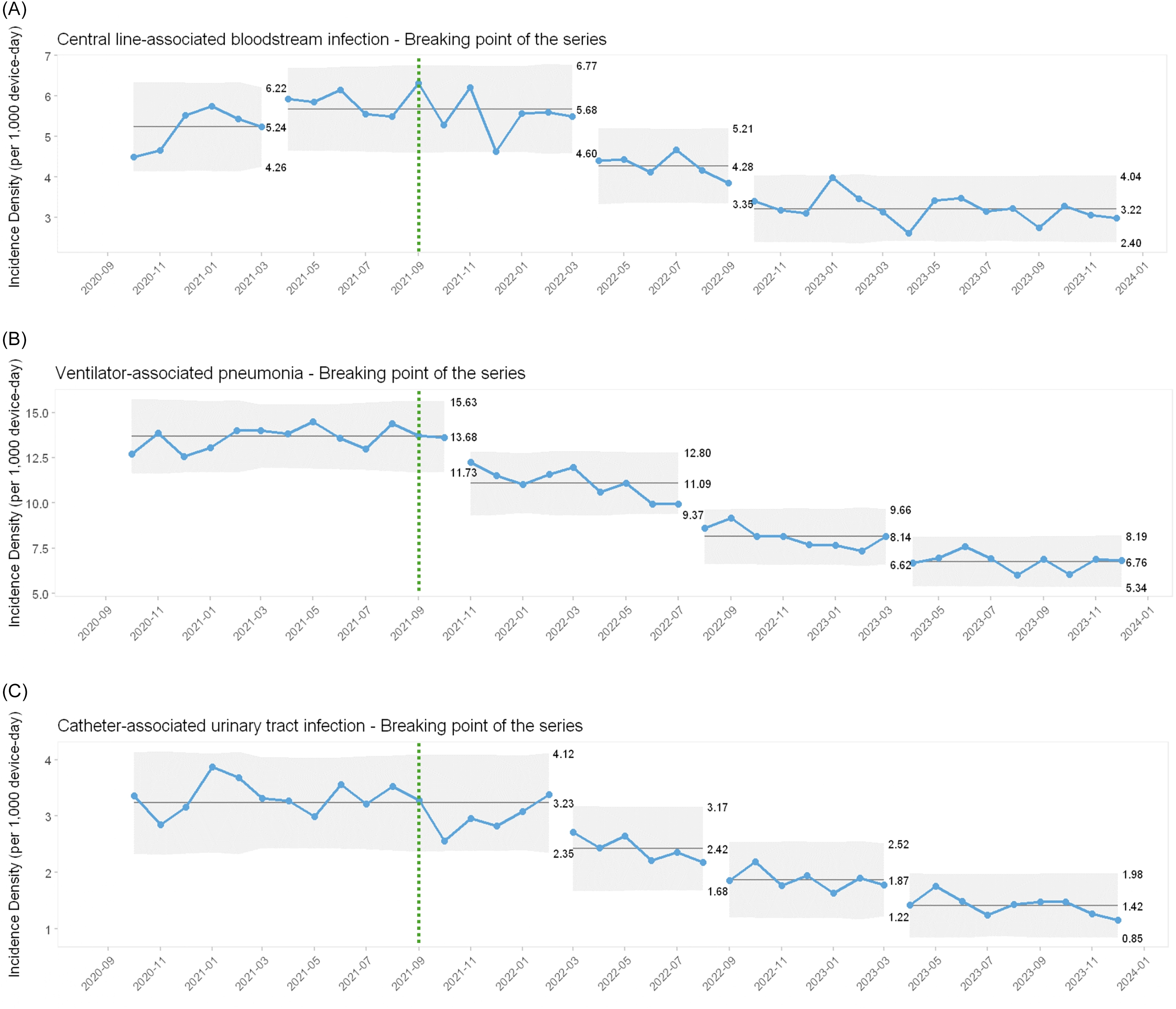
The enrolled ICUs’ HAI incidence density baseline was 5.68 (4.60–6.77), 13.68 (11.73–15.63), and 3.23 (2.35–4.12) per 1,000 device-days for CLABSI, VAP, and CAUTI, respectively. After the intervention period, the incidence density of all HAIs decreased substantially, to 3.22, 6.76, and 1.42 cases per 1,000 device-days for CLABSI (Figure 1A), VAP (Figure 1B), and CAUTI (Figure 1C), respectively, by December 2023. The decrease in incidence density ranged from 43% for CLABSI to 51% for VAP and 56% for CAUTI across all ages.
Control U charts of the Saúde em Nossas Mãos initiative from september 2020 to december 2023. A – central line-associated bloodstream infections; B – ventilator-associated pneumonia; C – catheter-associated urinary tract infections. Dashed green line: project start.

Figure 1 Long description
Panel A: A line graph shows the incidence density of central line-associated bloodstream infections per 1000 device-days from September 2020 to December 2023. The x-axis represents time in months, and the y-axis represents incidence density. The graph includes a dashed green line indicating the project start in September 2021. The incidence density fluctuates over time, with notable peaks and troughs. Panel B: A line graph illustrates the incidence density of ventilator-associated pneumonia per 1000 device-days over the same period. The x-axis represents time in months, and the y-axis represents incidence density. The graph also includes a dashed green line for the project start. The incidence density shows a general downward trend after the project start. Panel C: A line graph depicts the incidence density of catheter-associated urinary tract infections per 1000 device-days from September 2020 to December 2023. The x-axis represents time in months, and the y-axis represents incidence density. The graph includes a dashed green line for the project start. The incidence density shows a general decline after the project start.
The project’s strategies prevented approximately 7,342 infections.
Compliance to hand hygiene and healthcare-associated infection prevention
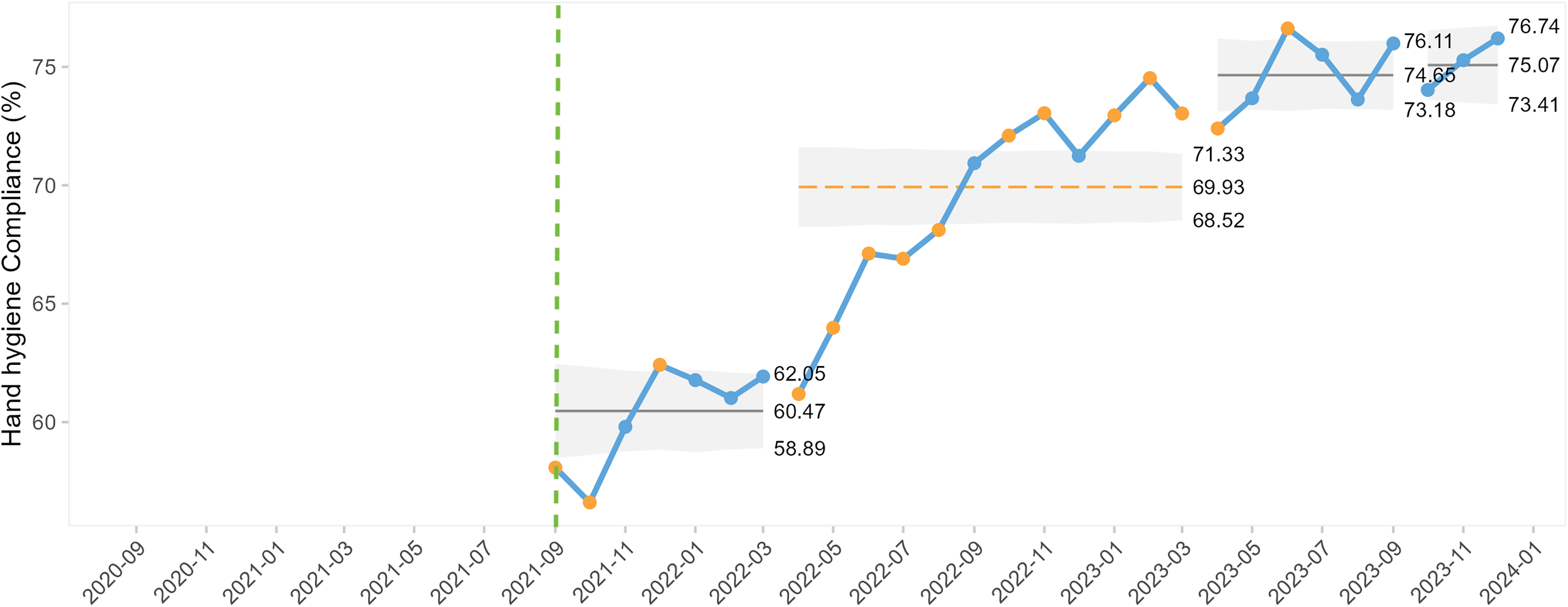
Overall, the compliance with hand hygiene increased from 60% to 75% (Figure 2).
Control U charts for hand hygiene compliance since the Saúde em Nossas Mãos starting in september 2021. Dashed green line: project start.

Impact on healthcare-associated infections in adult ICUs
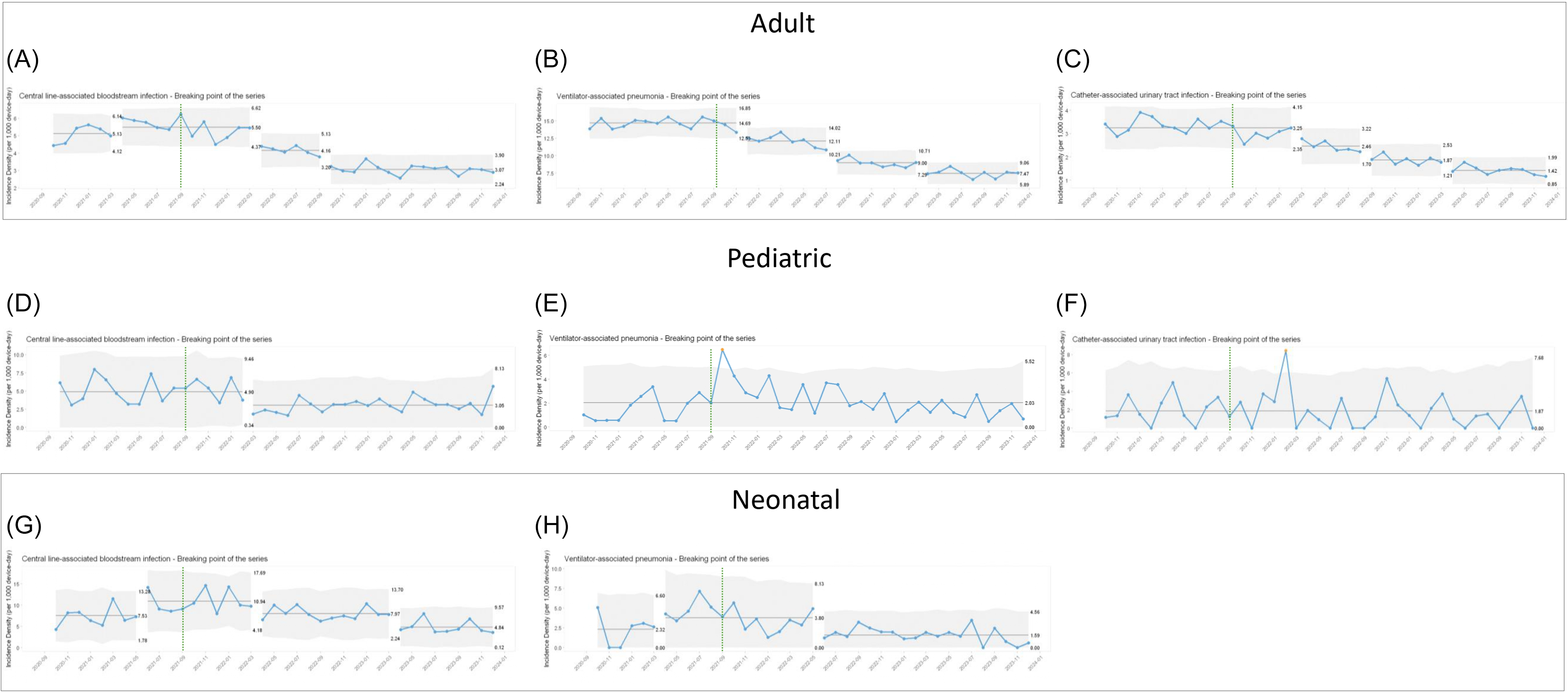
The enrolled adult ICUs’ HAI incidence density baseline was 5.50 (4.37–6.62), 14.69 (12.53–16.85), and 3.25 (2.35–4.15) per 1,000 device-days for CLABSI, VAP, and CAUTI, respectively. After the intervention period, CLABSI (Figure 3A), VAP (Figure 3B), and CAUTI (Figure 3C) decreased by 45%, 49%, and 60%, respectively, to 3.07 (2.24–3.90), 7.47 (5.89–9.06), and 1.42 (0.85–1.99) cases per 1,000 device-days.
Control U charts of the Saúde em Nossas Mãos initiative from september 2020 to december 2023. For adults (A–C), pediatric (D–F), and neonatal (G–H) intensive care units for central line-associated bloodstream infections, ventilator-associated pneumonia, and catheter-associated urinary tract infections, respectively. Dashed green line: project start.

The complementary statistical analysis of the timeseries is provided in the Supplementary material.
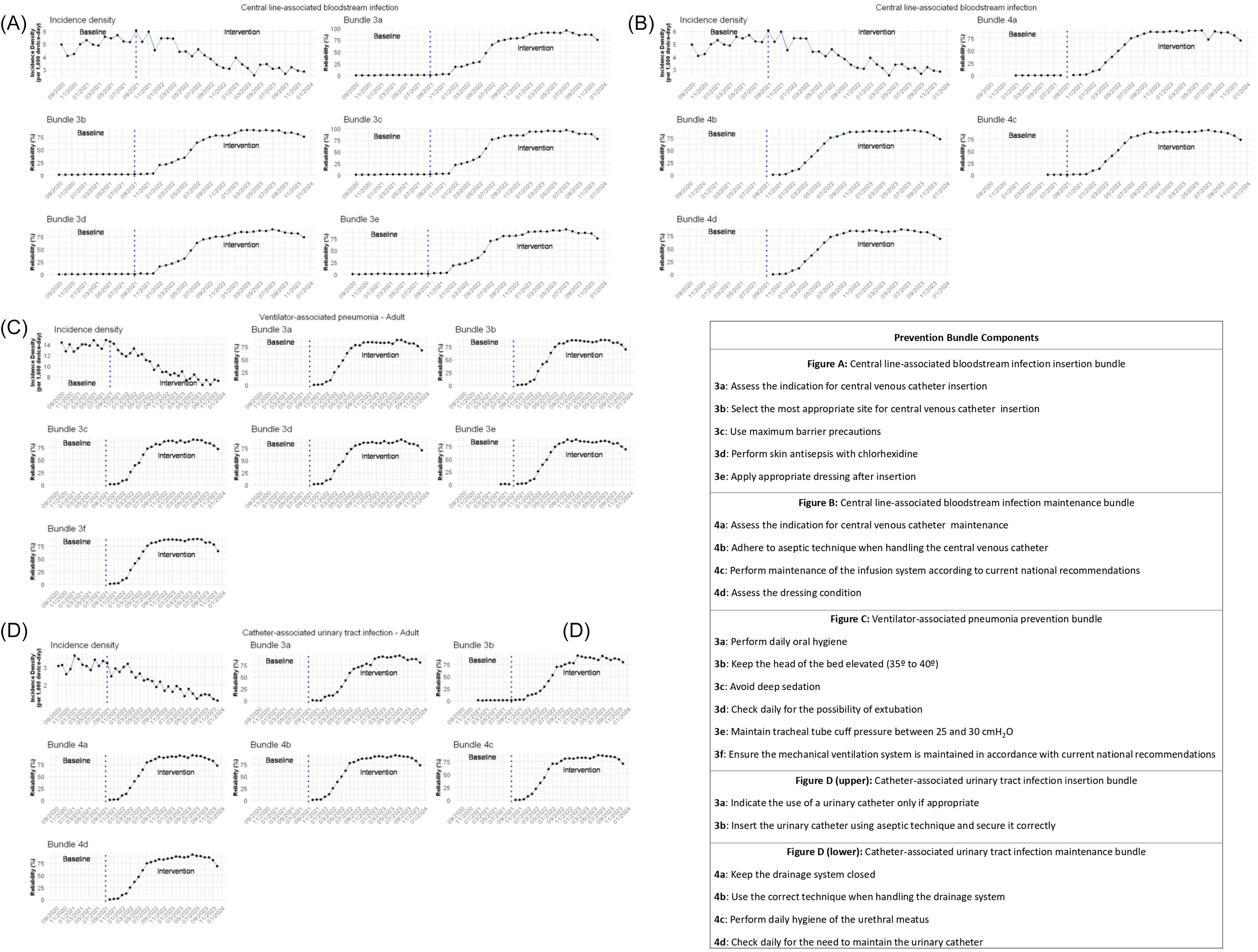
The adhesion to the insertion and maintenance bundles gradually increased, followed by a progressive reduction in the incidence density of CLABSI, VAP, and CAUTI (Figure 4).
Compliance for each item of the prevention bundle in adult intensive care units: A – central line-associated bloodstream infections: insertion bundle; B – central line-associated bloodstream infections: maintenance bundle; C – ventilator-associated pneumonia: prevention bundle; D – catheter-associated urinary tract infections: insertion and maintenance bundle. Dashed blue line: project start.

Figure 4 Long description
Panel A: This panel contains multiple line graphs showing the incidence density of central line-associated bloodstream infections during the insertion phase. Each graph represents a different bundle component, with the x-axis labeled as time and the y-axis labeled as incidence density. The graphs show trends before and after the intervention, marked by a dashed blue line indicating the project start. Panel B: This panel contains multiple line graphs showing the incidence density of central line-associated bloodstream infections during the maintenance phase. Similar to Panel A, each graph represents a different bundle component, with the x-axis labeled as time and the y-axis labeled as incidence density. The graphs show trends before and after the intervention, marked by a dashed blue line indicating the project start. Panel C: This panel contains multiple line graphs showing the incidence density of ventilator-associated pneumonia. Each graph represents a different bundle component, with the x-axis labeled as time and the y-axis labeled as incidence density. The graphs show trends before and after the intervention, marked by a dashed blue line indicating the project start. Panel D: This panel contains multiple line graphs showing the incidence density of catheter-associated urinary tract infections during both the insertion and maintenance phases. Each graph represents a different bundle component, with the x-axis labeled as time and the y-axis labeled as incidence density. The graphs show trends before and after the intervention, marked by a dashed blue line indicating the project start.
Impact on healthcare-associated infections in pediatric ICUs
The enrolled ICUs’ HAI incidence density baseline was 4.90 (0.34–9.46), 2.03 (0.00–5.01), and 1.87 (0.00–6.46) per 1,000 device-days for CLABSI, VAP, and CAUTI, respectively. After the intervention period, CLABSI (Figure 3D) reduced by 39%, reaching 3.05 (0.00–8.13) per 1,000 device-days. No reduction was detected for VAP and CAUTI incidence densities (Figure 3E and 3F, respectively).
The adhesion to the insertion and maintenance bundles gradually increased, followed by a progressive reduction in the incidence density of CLABSI (Supplementary Figure 1S).
Impact on healthcare-associated infections in neonatal ICUs
The enrolled ICUs’ healthcare-associated infection incidence density baseline was 10.94 (4.18–17.69) and 3.80 (0.00–8.13) per 1,000 device-days for CLABSI and VAP, respectively. After the intervention period, CLABSI (Figure 3G) and VAP (Figure 3H) reduced by 56% and 60%, reaching 4.84 (0.12–9.57) and 1.59 (0.00–4.56) cases per 1,000 device-days, respectively. CAUTI is not monitored in neonatal ICUs.
The adhesion to the insertion and maintenance bundles gradually increased, followed by a progressive reduction in the incidence density of CLABSI and VAP (Supplementary Figure 2S).
Discussion
Using a BTS framework to reduce HAI incidence, this nationwide QI collaborative prevented an estimated 7,342 infections, and it simultaneously reduced the incidence densities of CLABSI, VAP, and CAUTI by up to 54% across adult, pediatric, and neonatal ICUs. These findings demonstrate that a large-scale, structured collaborative can achieve significant and simultaneous reductions in multiple device-associated HAIs when evidence-based bundles are combined with rigorous QI methods.
We highlight two points that require careful interpretation. First, the CLABSI baseline was unstable and rising during the preintervention period, consistent with the COVID-19 pandemic’s adverse impact on HAIs in Brazilian ICUs. Reference Tuma, Vieira Júnior and Ribas24 These patterns emphasize the importance of supplementing simple before-and-after comparisons with comprehensive timeseries analyzes when interpreting HAI trends amid rapidly changing epidemiological conditions. Second, the ICU pediatric timeseries analyzes did not show a statistically significant reduction in VAP or CAUTI; however, point estimates indicated a 66% decline between the first six months and the last nine months of the intervention period for VAP, and a 64% decline between the baseline and intervention periods for CAUTI (data not shown).
Our findings are consistent with prior QI collaboratives, including those using the BTS model, which create learning networks and have improved at least one primary outcome in most settings. Reference Wells, Tamir, Gray, Naidoo, Bekhit and Goldmann25 In low- and middle-income countries, where HAI rates are 2–20 times higher than in high-income settings, Reference Allegranzi, Bagheri Nejad and Combescure26 programs that target modifiable risk factors, such as device exposure and length of stay, are crucial. Reference Allegranzi, Bagheri Nejad and Combescure26,Reference Rosenthal, Yin and Lu27 Furthermore, parallel reductions in preventable events, such as HAIs, will likely lead to lower mortality rates and shorter hospital stays. Reference Braun, Chitavi, Suzuki, Soyemi and Puig-Asensio28
The inverse correlation between bundle compliance and HAI incidence across age groups underscores the central role of care bundles in infection prevention. Bundles can produce robust clinical gains when implemented as a package rather than individually. Reference Resar, Griffin, Haraden and Nolan11 Multifaceted QI interventions that incorporate standardized bundles, audit and feedback, and education have repeatedly reduced HAI rates and are recognized as cost-saving, high-value strategies across economic contexts. Reference Negm, Othman, Tawfeek, Zalat, El-Sokkary and Alanwer29 In Brazil, such strategies have been associated with better clinical indicators, enhanced safety, and substantial financial benefits for the public health system. Reference Tuma, Vieira Junior and Ribas5,Reference Oliveira, de Sousa and de Salvo6 In fact, our initiative estimates savings of approximately Intl$175.3 million for the Brazilian unified health system (a return on investment of 890%). Reference Bass, de Meireles and Kiriyama30
Several studies have demonstrated reductions in HAIs after bundle implementation in adult and pediatric ICUs, often within collaborative or comprehensive safety programs. Reference Fresán-Ruiz, Pons-Tomás and de Carlos-Vicente31–Reference Rosenthal, Jin and Yin34 Comprehensive Unit-based Safety Programs and large multidimensional initiatives across hundreds of ICUs have reported sustained decreases in CLABSI, CAUTI, and VAP. Reference Miller, Briody and Casey33,Reference Rosenthal, Jin and Yin34 Our results across 188 heterogeneous ICUs extend this evidence to a nationwide middle-income setting and show that robust outcomes can be achieved at scale when technical interventions are embedded within an organized learning and support structure.
Hand hygiene is a critical factor in HAI prevention. The WHO SAVE LIVES: Clean Your Hands initiative articulates a multimodal strategy that combines system change, training and education, evaluation and feedback, reminders in the workplace, and an institutional safety climate to improve hand hygiene among healthcare workers. Reference Allegranzi, Gayet-Ageron and Damani35 In line with these recommendations, SNM implemented structured training (virtual courses and in-person workshops), ensured access to essential supplies, standardized monitoring indicators, and strengthened feedback and interprofessional communication to foster a culture of shared responsibility. The increase in hand hygiene compliance observed over the project period supports the effectiveness of this approach and likely contributed to the reductions in device-associated HAIs.
Beyond technical interventions, SNM deliberately combined Lean Healthcare tools, job instruction, and visual management to address socioadaptive determinants of practice. Lean methods were used to streamline workflows and eliminate non-value-added steps in HAIprevention processes, while TWI jobinstruction techniques provided structured, bedside-focused training to ensure that staff could reliably execute each bundle element. Reference Saavedra Bravo, Santos and Petenate18,Reference Borem, de Moura and Dos Santos19 The Kamishibai board functioned as a simple, low-cost visual management tool that facilitated daily, point-of-care audits and real-time feedback, supporting sustained adherence to bundles for CLABSI, VAP, and CAUTI. Reference Saavedra Bravo, Santos and Petenate18 These tools, together with automated data capture and dashboarding, strengthened local ownership of data and enabled more timely learning cycles at both the unit and system levels. Furthermore, these strategies aimed to sustain the achieved improvement by providing a structured process embedded in daily care rather than a transitory change, Reference Borem, de Moura and Dos Santos19 a challenge that remains evident in the reported compliance with prevention bundles in the last months of our initiative.
Limitations
This nationwide study has significant limitations. As in other HAIprevention initiatives, adjudication of VAP and the measured incidence of CLABSI and CAUTI may be influenced by local diagnostic and surveillance practices, including the frequency of culture ordering and how definitions are applied; culture stewardship alone can reduce reported CAUTI rates. Reference Mullin, Kovacs and Fatica36 To mitigate this, the study used a pre–post design in which each ICU served as its own control, established a complete one-year baseline, and standardized surveillance processes and case definitions according to Anvisa criteria across all participating units, with training and audits to minimize documentation and reporting variation. Reference Cherifi, Mascart and Dediste37,Reference Beekmann, Diekema and Huskins38
Second, SNM was delivered as a comprehensive package of technical and socioadaptive changes, which ICUs adapted to the local context via PDSA cycles, a core feature of the BTS approach; this supports context-sensitive implementation but limits attribution to individual components. Units differed in resources and baseline infectionprevention practices, yet all applied common evidence-based bundles. Unlike earlier large-scale programs such as Matching Michigan and the national CAUTI-prevention collaborative, which achieved limited or non-significant effects, Reference Bion, Richardson and Hibbert39 SNM explicitly emphasized socioadaptive strategies alongside technical bundle adherence, drawing on Chopra et al.’s framework to strengthen engagement, leadership alignment, communication, and psychological safety. Reference Chopra and Shojania40 Although residual confounding from secular changes in professional behavior cannot be excluded, we identified no concurrent policy shifts or stewardship initiatives that would plausibly explain the magnitude and consistency of the observed reductions, making measurement artifact from altered culturing or surveillance less likely.
Further limitations were discussed in our previous report (2018–2020), Reference Tuma, Vieira Junior and Ribas5 including the academic limitation that the SNM is a QI initiative rather than a research project, including the lack of a control group, comparison with the national trend (contextual factors), missing key variables (e.g., knowledge acquisition), representativeness, and potential selection bias, as well as variability among ICU profiles and patients (e.g., cardiologic, neurologic, etc.).
Future directions
Currently, all implemented strategies (educational materials, assessment tools, infographics, etc.) are being prepared in partnership with the Brazilian Ministry of Health and Anvisa to create a document outlining a multimodal strategy to prevent the three HAI analyzed and to make the implementation guidelines publicly available.
Conclusion
The SNM project has demonstrated a remarkable capacity to reduce HAIs across multiple ICUs through the integrated use of the BTS (emphasizing the synergistic effect of Lean Healthcare and TWI), multidisciplinary team engagement, and adherence to evidence-based preventive bundles. Decreasing the incidence density of three critical HAIs simultaneously highlights the effectiveness of the intervention strategies. It underscores the essential role of continuous, comprehensive training and adherence to best practices in infection prevention, setting a benchmark for future projects aimed at combating HAIs.
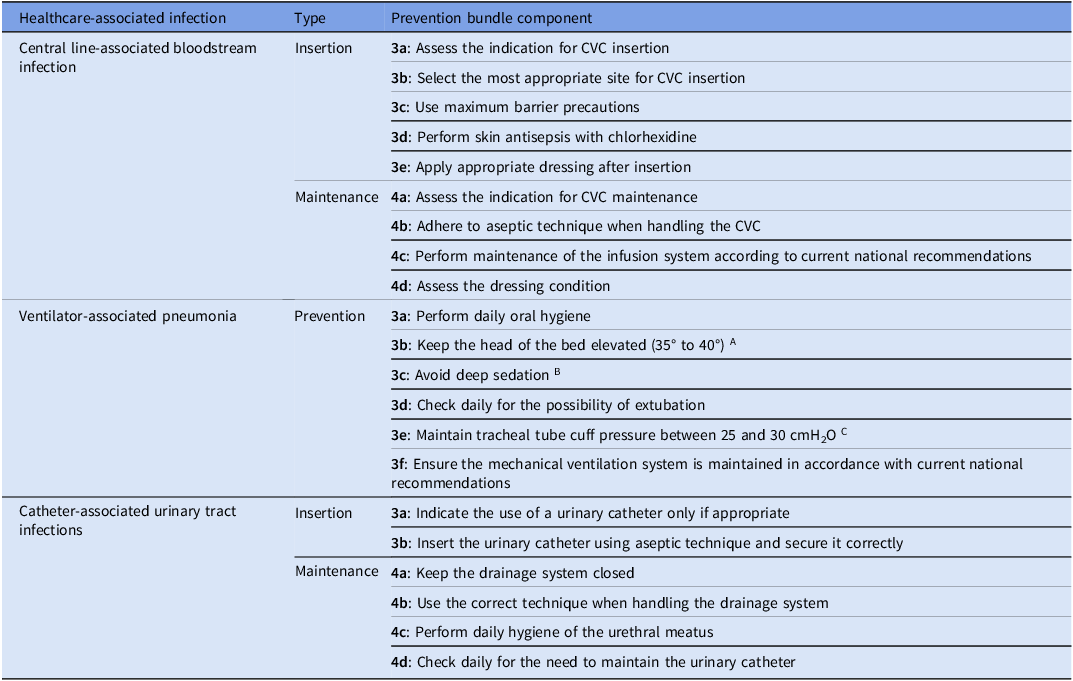
Prevention bundles for each analyzed healthcare-associated infection

Legend. CVC, Central Venous Catheter. Adaptation for pediatric and neonatal intensive care units: A Keep proper position according to targeted population; B Reduce sedation, when possible; C Care of oropharyngeal airway.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2026.10434.
Data availability statement
If data access is required, application and authentication from the project governance are needed.
Acknowledgements
The authors would like to thank all healthcare professionals working in the involved ICUs; this project would not have been possible without their support and motivation. We are also grateful to the PROADI-SUS technical and administrative teams, who supported the development of this project, and to Angela Patricia França for review, writing, and editing support. We also thank the Research Support Center of the Hospital Israelita Albert Einstein, and Anderson Paulo Scorsato for the statistical support.
Author contribution
All authors contributed to data curation, formal analysis, investigation, methodology, validation, visualization, and writing. Additionally, C.M.R., L.Y.U., and C.G.d.B. also contributed to conceptualization, project administration, and supervision.
Financial support
This study received public resources from the Ministry of Health through PROADI-SUS and philanthropic resources from the participating institutions.
Competing interests
All authors declared none.
Ethical standard
For this academic article, access to the SNM database was approved by the local human research ethics committees (Certificado de Apresentação de Apreciação Ética – CAAE 66698023.7.0000.0071) of the six PROADI-SUS institutions, with the consent of the SNM coordinator and the authorization of the ministry responsible. The available database presented indicators of QI processes and did not exhibit any data referring to or mentioning the participating institutions or patients involved.



 Open access
Open access