


Impact statement
Although effective and affordable treatments exist, many people continue to face barriers that prevent them from seeking or receiving help. These barriers include not only the lack of available services and high treatment costs but also fear of stigma, low awareness about mental health and doubts about the usefulness of treatment. Addressing these “demand-side” factors is therefore as essential as expanding services. Our review focuses on this critical challenge. How to encourage people to recognize their need for support and take active steps toward seeking help? Help-seeking is not a single event but a process that involves understanding one’s symptoms, deciding to seek support and following through with that decision. We examined recent evidence on interventions that aim to influence three key components: attitudes, intentions and behaviors. We found a growing body of work in this area, with over 50 new studies published in the past few years. Interventions that combined multiple strategies, such as psychoeducation, stigma reduction, motivational approaches and promotion of available resources, were the most effective. Social contact-based approaches, particularly those delivered through short videos, showed consistent promise in improving help-seeking attitudes and intentions, especially among the general population. However, translating improved attitudes and intentions into actual behavior change remains a challenge. Our findings highlight an important shift in mental health research from focusing primarily on service delivery to understanding how people decide to seek help. By synthesizing recent evidence, this review contributes to a clearer understanding of what works to encourage help-seeking and where the gaps remain. It underscores the need for future research to use theory-driven frameworks, examine mechanisms of change and adopt standardized measures. Focusing on how interventions can effectively move people from awareness to action is essential for reducing the global mental health treatment gap and ensuring that more individuals receive appropriate care.
Introduction
The disparity between the prevalence of mental health conditions and the uptake of mental health care remains high globally, despite the availability of effective and affordable treatments (Kohn et al., Reference Kohn, Saxena, Levav and Saraceno2004; Codony et al., Reference Codony, Alonso, Almansa, Bernert, de Girolamo, de Graaf, Haro, Kovess, Vilagut and Kessler2009; White et al., Reference White, Clough and Casey2018). Barriers perpetuating this treatment gap include both demand-side factors (e.g., perceived lack of confidentiality, trust issues with providers, stigma, low mental health literacy, etc.) and supply-side factors (e.g., lack of mental health care services, insufficient public funding, high out-of-pocket costs, etc.) (Gulliver et al., Reference Gulliver, Griffiths and Christensen2010; Luitel et al., Reference Luitel, Mark, Kohrt, Rathod and Komproe2017; Wainberg et al., Reference Wainberg, Scorza, Shultz, Helpman, Mootz, Johnson, Neria, Bradford, Oquendo and Arbuckle2017; Qin and Hsieh, Reference Qin and Hsieh2020; Babatunde et al., Reference Babatunde, van Rensburg, Bhana and Petersen2021; Sarikhani et al., Reference Sarikhani, Bastani, Rafiee, Kavosi and Ravangard2021). While much research has focused on reducing the treatment gap by addressing supply-side barriers (e.g., using approaches such as task sharing), increasing the availability of mental health services alone does not guarantee greater service uptake (Roberts et al., Reference Roberts, Esponda, Torre, Pillai, Cohen and Burgess2022). There is now a growing interest in addressing demand-side barriers by developing interventions to promote help-seeking for mental health conditions. However, encouraging help-seeking remains a significant challenge for public health (Schnyder et al., Reference Schnyder, Panczak, Groth and Schultze-Lutter2017; Organization, World Health, 2004a, 2004b). Several factors deter individuals from help-seeking for mental health conditions, including low perceived need for treatment or support, low MHL, doubts about the perceived benefits of help seeking (ten Have et al., Reference ten Have, de Graaf, Ormel, Vilagut, Kovess and Alonso2010; Rughani et al., Reference Rughani, Deane and Wilson2011), financial constraints and stigma (Sanders Thompson et al., Reference Thompson, Vetta, Noel and Campbell2004; Andrade et al., Reference Andrade, Alonso, Mneimneh, Wells, Al-Hamzawi, Borges, Bromet, Ronny Bruffaerts and De Graaf2014; Topkaya, Reference Topkaya2015; Umubyeyi et al., Reference Umubyeyi, Mogren, Ntaganira and Krantz2016; Schnyder et al., Reference Schnyder, Panczak, Groth and Schultze-Lutter2017; McLaren et al., Reference McLaren, Peter, Tomczyk, Muehlan, Schomerus and Schmidt2023).
Help-seeking is a dynamic process that begins with recognizing mental health symptoms, followed by expressing the need for support, identifying available help, and ultimately seeking help (Rickwood et al., Reference Rickwood, Deane, Wilson and Ciarrochi2005; Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018) but lacks consensus on definition or measurement, often varying by process stage or help source (professional versus non-professional) (Rickwood and Thomas, Reference Rickwood and Thomas2012). The Theory of Planned Behavior (TPB) has gained substantial attention over the years in understanding help-seeking, focusing on three processes (Ajzen, Reference Ajzen1991; Adams et al., Reference Adams, Gringart and Strobel2022; Naumova, Reference Naumova2022): help-seeking attitudes (overall perception toward seeking help), intentions (plans/decisions to seek help), and behaviors (actually seeking help/support) (Rickwood and Thomas, Reference Rickwood and Thomas2012). TPB suggests that attitudes influence intentions, which predict behaviors (Ajzen, Reference Ajzen1991). Research confirms that TPB effectively predicts intentions and behaviors (McEachanReference McEachan, Conner, Taylor and Lawton2011; Ajzen, Reference Ajzen1991; Armitage and Conner, Reference Armitage and Conner2001) and that intentions mediate the relationship between attitudes and behaviors (Kim and Hunter, Reference Kim and Hunter1993; Glasman and Albarracín, Reference Glasman and Albarracín2006). Rickwood and Thomas (Reference Rickwood and Thomas2012) further advocated for a TPB-based framework to conceptualize and measure help-seeking as a complex process and all three components are crucial for influencing the help-seeking process comprehensively. Following the TPB model, our review focuses on attitudes, intentions and behaviors as primary outcomes because each serves a distinct public health function. Improving attitudes and intentions among the general population is critical for long-term, population-level stigma reduction. Conversely, targeting intentions and actual behaviors is essential for individuals currently experiencing mental health conditions to ensure they transition from recognizing a need to seeking help. By including all populations and contexts, this review comprehensively captures the full spectrum of demand-side strategies necessary to address the treatment gap globally (Rickwood and Thomas, Reference Rickwood and Thomas2012; Adams et al., Reference Adams, Gringart and Strobel2022).
The effectiveness of interventions aimed at improving help-seeking for mental health conditions remains unclear, as evidenced by mixed results in previous literature (Gulliver et al., Reference Gulliver, Griffiths and Christensen2012; Adams et al., Reference Adams, Gringart and Strobel2022). Considering the changing landscape of mental health care and the gaps in current research, our review synthesizes the recent evidence on effective interventions for promoting help-seeking processes (attitudes, intentions and behaviors) for mental health conditions. We synthesize post-2016 RCTs on these outcomes, focusing on recent studies not covered by Xu et al. (Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018), who synthesized RCTs up to 2016 using meta-analysis. Our narrative synthesis approach differs substantially due to greater heterogeneity in post-2016 studies, precluding a meta-analysis. As noted by Rickwood and Thomas (Reference Rickwood and Thomas2012), studies often fail to specify which part of the help-seeking process (e.g., recognition versus action) or which source of help (e.g., formal versus informal) is being targeted. This lack of standardization justifies our broad inclusion criteria, as it allows for a comprehensive mapping of diverse interventions ranging from MHL to social contact, addressing different stages of the process.
Our review aimed to identify and evaluate strategies that effectively improve help-seeking behaviors, attitudes and intentions. We also synthesized MHL, stigma and related mediators as secondary outcomes due to their complex relationship with help-seeking (Jorm et al., Reference Jorm, Korten, Jacomb, Christensen, Rodgers and Pollitt1997; Smith et al., Reference Smith, Tran and Thompson2008; Schnyder et al., Reference Schnyder, Panczak, Groth and Schultze-Lutter2017; Cheng et al., Reference Cheng, Wang, McDermott, Kridel and Rislin2018; Michel et al., Reference Michel, Schnyder, Schmidt, Groth, Schimmelmann and Schultze-Lutter2018; Mackenzie et al., Reference Mackenzie, Heath, Vogel and Chekay2019; McLaren et al., Reference McLaren, Peter, Tomczyk, Muehlan, Schomerus and Schmidt2023).
Methods
The protocol for the review was registered on PROSPERO (CRD42021273843; https://www.crd.york.ac.uk/PROSPERO/view/CRD42021273843) (Nadkarni and Gandhi, Reference Nadkarni and Gandhi2021). This review is developed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist (Page et al., Reference Page, Moher, Bossuyt, Boutron, Hoffmann, Mulrow, Shamseer, Tetzlaff, Akl, Brennan and Chou2021).
Search strategy
Our search was conducted on six databases: Ovid Medline, EMBASE, PsycINFO, Cochrane Central Register of Controlled Trials (CENTRAL), Global Health and Cumulative Index to Nursing and Allied Health Literature (CINAHL). The initial search was in January 2022, updated in May 2023 and focused on “mental health,” “help-seeking” and “randomized controlled trials.” The detailed search strategy is in Supplementary Appendix A.
Eligibility criteria
Our review included randomized controlled trials (RCTs) from any country or setting, with populations either non-clinical (general population) or clinical (individuals with mental health conditions, as defined by ICD, DSM, clinical diagnosis, standardized questionnaires or self-defined psychological issues). There were no age restrictions, and only English publications after December 2016 were considered to capture recent evidence.
Interventions were eligible if they aimed to promote help-seeking for mental health care, with at least one help-seeking outcome (attitudes, intentions or behaviors) as a primary outcome. Controls could be active or inactive. Reviews, meta-analyses, commentaries, opinion pieces, pilot studies, observational studies and non-randomized trials were excluded.
Study selection and data collection
After database search completion, the data were imported to Endnote (The EndNote Team, 2013), with duplicates removed automatically and manually. Records were screened in Covidence (Anon, 2023) by two pairs of reviewers (SI and MGP, MGP and SB) for titles and abstracts, and full texts were independently reviewed by two pairs (NN and MGP, MGP and SB), with reasons for exclusion recorded. Inter-rater reliability showed a Kappa of 0.50 (NN and MGP) and 0.89 (SB and MGP). Disagreements were resolved by a third reviewer (AG or YG). Data extraction was done independently by reviewers (NN, MGP, NH and SB) and reviewed by SB.
Data
We extracted data on help-seeking outcomes as behaviors (self-reported/observable service use, e.g., appointments/helplines), intentions (plans/decisions to seek help) and attitudes (beliefs/willingness) (Rickwood and Thomas, Reference Rickwood and Thomas2012). We also extracted information regarding the type of help accessed (e.g., formal professional services, informal peer support or self-help), categorized the outcome measures by their source (e.g., administrative records, clinical registries or self-report scales) and recorded the specific timeframes for each outcome, which ranged from immediate post-intervention effects to 12-month or 24-month longitudinal follow-ups and lifetime help-seeking history.
While the Attitudes Toward Seeking Professional Psychological Help Scale (ATSPPH) is primarily a measure of attitudes, several included studies (e.g., Amsalem et al., Reference Amsalem, Lazarov, Markowitz, Smith, Dixon and Neria2022; Amsalem, Wall et al., Reference Amsalem, Wall, Lazarov, Markowitz, Fisch, LeBeau, Hinds, Liu, Fisher, Smith, Hankerson, Lewis-Fernández, Dixon and Neria2023) utilized specific items from the scale, such as “openness to treatment seeking” to operationalize help-seeking intentions. We have categorized these results under “intentions” to remain consistent with the authors’ primary research objectives.
Additional data extracted included information about:
-
a) MHL (knowledge about mental health problems) (Jorm et al., Reference Jorm, Korten, Jacomb, Christensen, Rodgers and Pollitt1997; Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018);
-
b) mental illness stigma, including perceived and personal stigma (Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018);
-
c) factors mediating the effect of the help-seeking intervention (Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018).
We initially planned to examine implementation outcomes like feasibility, acceptability and appropriateness, but decided against it due to data heterogeneity and the limited number of studies reporting these outcomes.
Analysis and data synthesis
While Xu et al. (Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018) utilized meta-analysis, the post-2016 literature reflects a significant diversification in modalities (e.g., social media vs. standalone apps) and a shift toward multi-component interventions. We determined that the clinical and methodological heterogeneity, specifically the lack of standardized follow-up intervals and the variety of help-seeking sources (formal vs. informal), would render a pooled effect size misleading. Given the heterogeneity in the interventions and outcome measurement, a descriptive analysis of the included studies is presented in a narrative format (Popay et al., Reference Popay, Roberts, Sowden, Petticrew, Arai, Rodgers, Britten, Roen and Duffy2006). An intervention was considered effective if it showed significant differences in help-seeking outcomes (p ≤ 0.05 or p ≤ 0.01) compared to the control group; otherwise, it was deemed ineffective. Where reported by primary studies, standardized effect size estimates (e.g., odds ratios, Cohen’s d, partial η 2) were extracted and presented alongside statistical significance to aid interpretation of intervention magnitude (see Table 3). These values are presented descriptively to provide context for the reported statistical significance; they are not intended for direct cross-study comparison.
Based on the primary outcomes, we categorized studies into three groups: (a) behaviors, (b) intentions and (c) attitudes. We further categorized interventions based on their delivery settings within the larger groups: school/university-based, facility-based and community-based.
To synthesize the diverse intervention strategies identified, we employed an inductive, iterative approach to categorize intervention components based on their frequency and functional similarity. Given that a majority of the included studies utilized multi-component interventions such as combining psychoeducation with social contact or MI, arranging the results by individual study would have obscured broader research trends. Therefore, we grouped strategies into thematic categories (e.g., “Media-based,” “Social Contact” or “MI Strategies”) focused on identifying functional clusters of strategies to provide a clearer and usable framework for implementation. This mapping process (Table 4), allows for a more practical interpretation of which “active ingredients” are most frequently combined to drive changes in help-seeking attitudes, intentions and behaviors. By focusing on these clusters of strategies, the review highlights intervention formats that are most likely to be feasible in real-world settings.
Risk of bias assessment
The risk of bias was independently assessed by two pairs of three researchers (NN & MGP and MGP & SB). We used the Cochrane Collaboration “Risk of Bias 2” tool (ROB2), which consists of seven domains (sequence generation, allocation concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective outcome reporting and other sources of bias) (Sterne et al., Reference Sterne, Savović, Page, Elbers, Blencowe, Boutron, Cates, Cheng, Corbett, Eldridge, Emberson, Hernán, Hopewell, Hróbjartsson, Junqueira, Jüni, Kirkham, Lasserson, Li, McAleenan, Reeves, Shepperd, Shrier, Stewart, Tilling, White, Whiting and Higgins2019). In case of a difference in assigned scores, the pairs met to review and arrived at a consensus.
Results
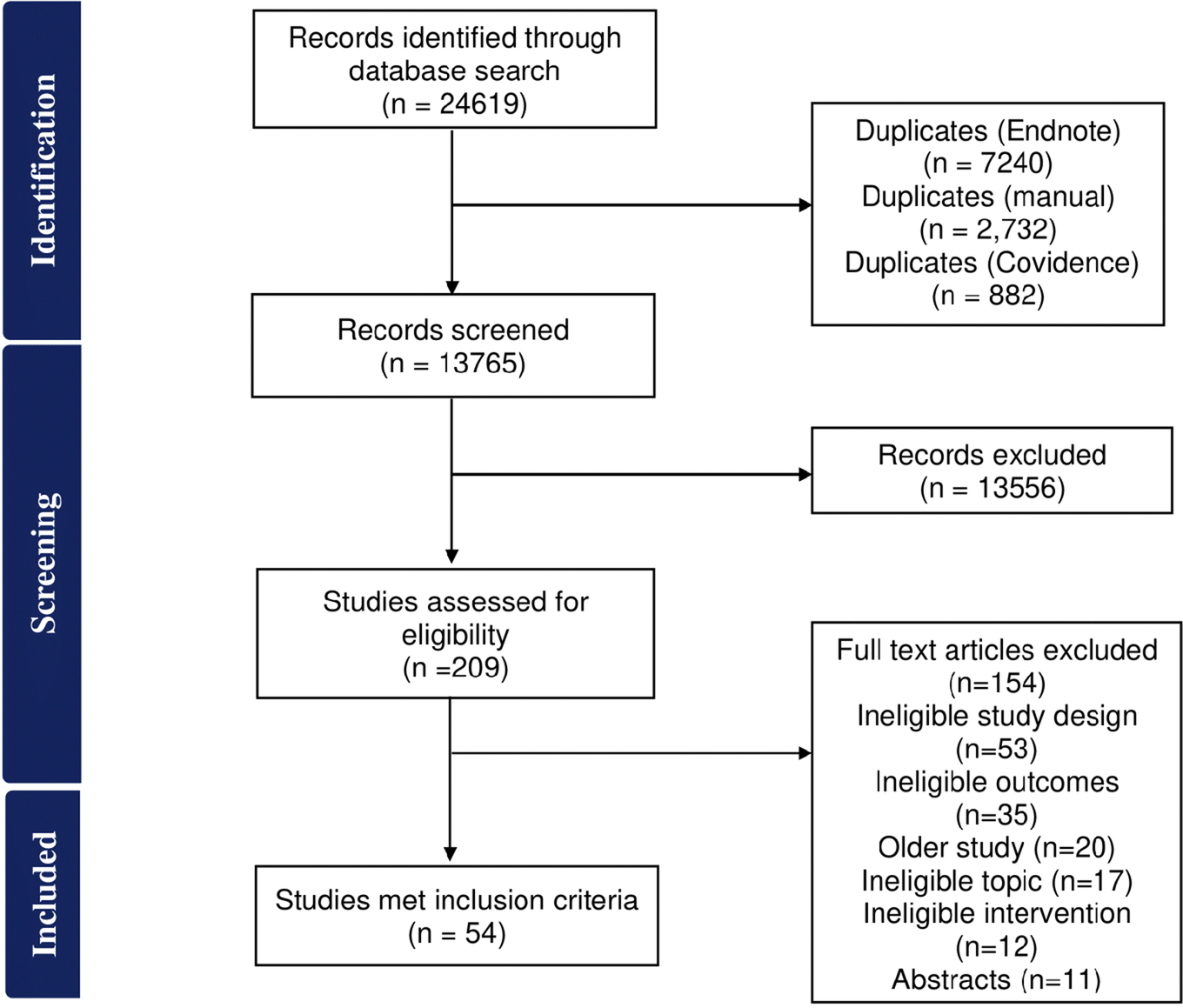
Figure 1 outlines the number of studies included and excluded at each stage. A total of 24,619 records were identified of which 10,854 records were duplicates. Of the remaining 13,765 records, 209 were screened for full-text eligibility, and 54 studies were included as they met the inclusion criteria. Out of 209 full-text articles assessed, the majority (154; 73.7%) were excluded due to an ineligible study design (non-RCTs).
Flowchart for study identification, screening, and inclusion.

Study characteristics
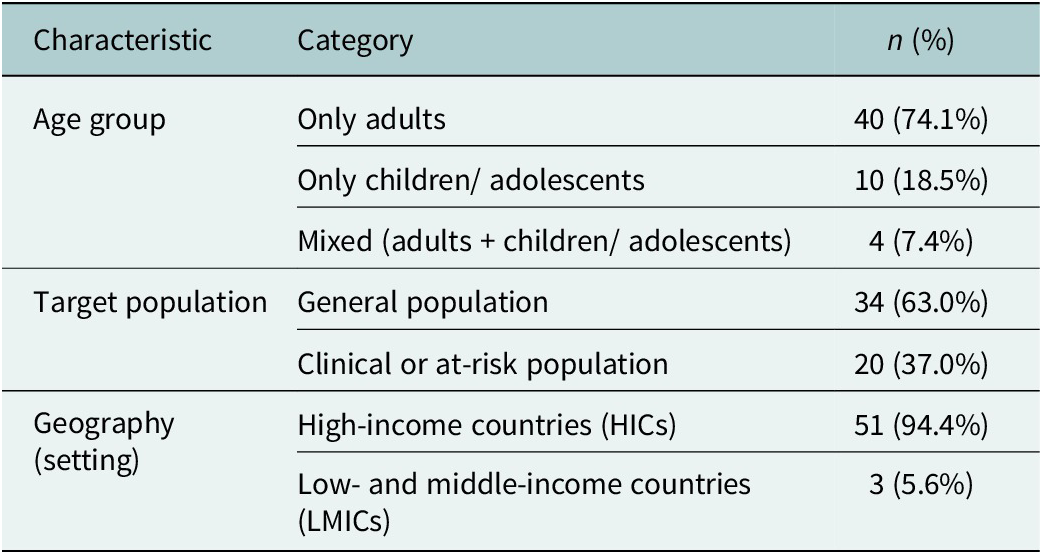
The included studies (n = 54) comprised a total sample size of 679,652 participants (range: 24 to 333,596). Most of the studies were individual RCTs (n = 44), and the rest were cluster RCTs (n = 10). Apart from three studies, which were stepped-wedge RCTs (Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021; Ries et al., Reference Ries, Livengood, Huh, Kerbrat, Fruhbauerova, Turner and Comtois2022; Lee et al., Reference Lee, Bobb, Richards, Achtmeyer, Ludman, Oliver, Caldeiro, Parrish, Lozano, Lapham, Williams, Glass and Bradley2023), all were parallel RCTs. Of the 54 included studies, the vast majority (94.4%; n = 51) were conducted in High-Income Countries (HICs), with the USA (51.8%; n = 28) and Australia (18.5%; n = 10) being the most frequent. Only 5.5% (n = 3) were conducted in lower-middle income countries (India and Nepal) or upper-middle income countries (China) (see Table 1).
Demographic and geographic characteristics of included studies

The 54 included studies involved a total of 679,652 participants. The demographic breakdown (see Table 1) is summarized below.
The majority of studies focused on adults (74.1%; n = 40), with a mean age range of 18–73 years. Children and adolescents were the focus of 18.5% (n = 10) of studies (mean age 11.5–16.8 years), while 7.4% (n = 4) targeted both adults and children/ adolescents (mean age = 12–30.6 years) populations.
Approximately 63.0% (n = 34) of the studies were conducted with the general population, while the remaining 37.0% (n = 20) targeted clinical or at-risk groups, such as those with existing mental health conditions.
Most studies included both genders. However, four used single-gender samples- one all-female study (Holt et al., Reference Holt, Milgrom and Gemmill2017) and three all-male studies (King et al., Reference King, Schlichthorst, Spittal, Phelps and Pirkis2018; Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Achterbergh et al., Reference Achterbergh, Van Rooijen, Van Den Brink, Boyd and De Vries2021).
A portion of the research (n = 10) focused on specialized populations, including at-risk veterans (n = 3) (Ilgen et al., Reference Ilgen, Price, Coughlin, Pfeiffer, Stewart, Pope and Britton2022; Possemato et al., Reference Possemato, Johnson, Barrie, Ghaus, Noronha, Wade, Greenbaum, Rosen, Cloitre, Owen, Jain, Beehler, Prins, Seal and Kuhn2023; Stecker et al., Reference Stecker, Allan, Hoge, Ashrafioun and Conner2023); healthcare workers(n = 2) (Amsalem, Lazarov, et al., Reference Amsalem, Lazarov, Markowitz, Smith, Dixon and Neria2022; Amsalem, Wall, et al., Reference Amsalem, Wall, Lazarov, Markowitz, Fisch, LeBeau, Hinds, Liu, Fisher, Smith, Hankerson, Lewis-Fernández, Dixon and Neria2023), sexual and gender Minorities (SGM) (n = 2) (Achterbergh et al., Reference Achterbergh, Van Rooijen, Van Den Brink, Boyd and De Vries2021; Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023) and one study each in refugees, people experiencing homelessness and women experiencing postpartum stress (Holt et al., Reference Holt, Milgrom and Gemmill2017; Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Kerman et al., Reference Kerman, Nisenbaum, Durbin, Wang, Kozloff, Hwang and Stergiopoulos2023).
Interventions
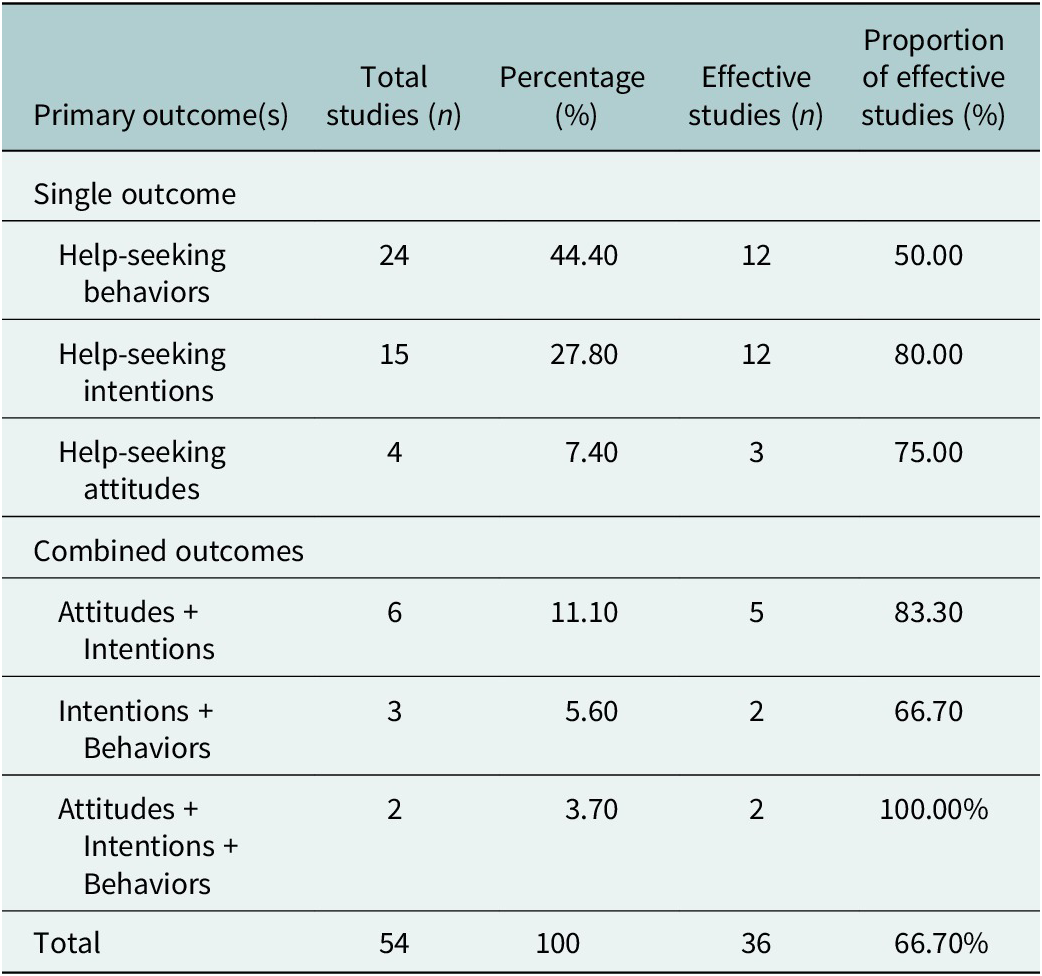
The 54 included studies targeted various combinations of help-seeking outcomes (see Table 2). Nearly half of the studies targeted help-seeking behaviors exclusively (n = 24). Intentions were the sole focus of 15 studies, while only four focused on attitudes.
Summary of help-seeking outcome targets
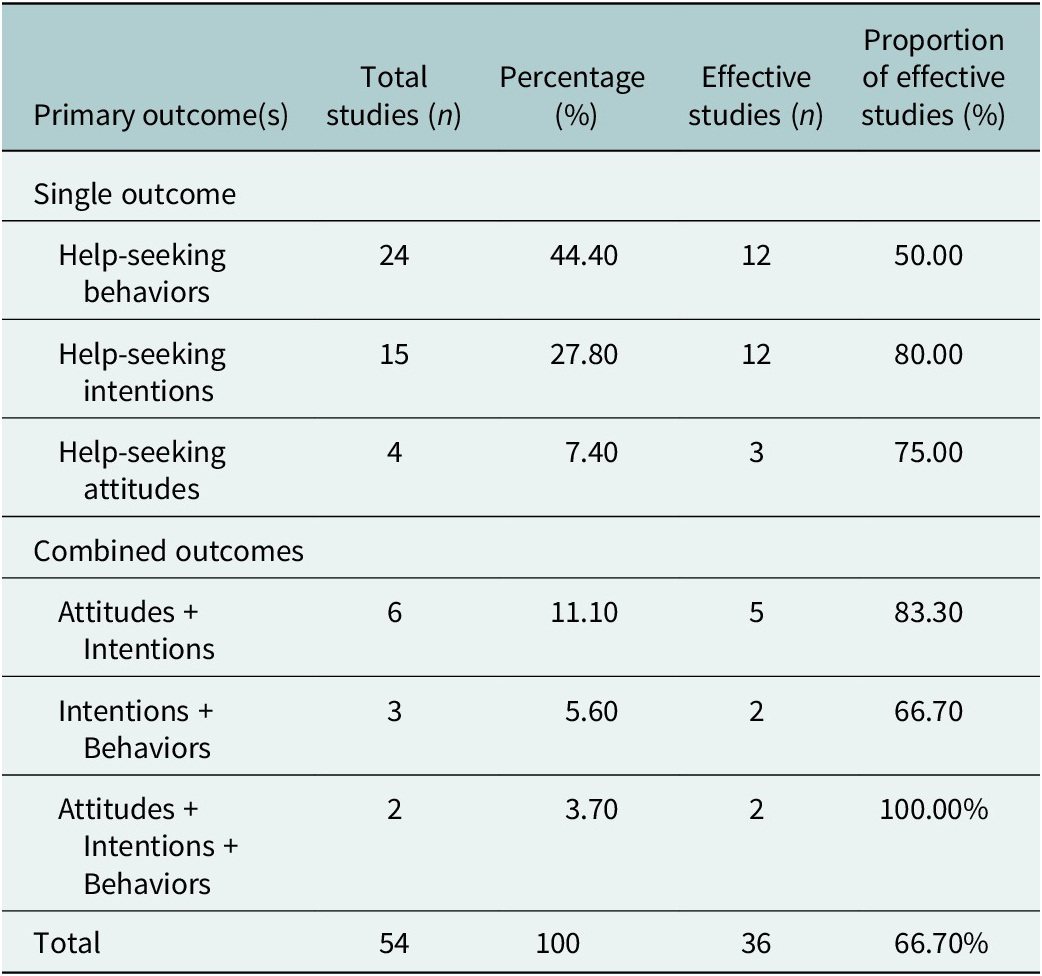
Eleven studies used an integrated approach targeting multiple outcomes. Six targeted attitudes and intentions (Hussain and Alhabash, Reference Hussain and Alhabash2020, Reference Hussain and Alhabash2022; Seidman et al., Reference Seidman, Wade and Geller2022; Tay, Reference Tay2022; Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023; Hollar and Siegel, Reference Hollar and Siegel2023). Three targeted intentions and behaviors (Coleman et al., Reference Coleman, Black, Ng and Blumenthal2019; Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Calear et al., Reference Calear, McCallum, Christensen, Mackinnon, Nicolopoulos, Brewer, Werner-Seidler, Morse, Kazan, Farrer, Kampel and Batterham2022), and two targeted all three outcomes: 3.7% (n = 2) (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020; Tobias et al., Reference Tobias, Landy, Levin and Arch2022).
Across the entire review, 66.7% (n = 36) of the tested interventions were effective in significantly improving at least one primary help-seeking outcome. Detailed characteristics for each individual study, including the specific country and the type of help sought, are provided in Table 3.
Summary of included studies

Mapping of intervention components
To identify the “active ingredients” of these interventions, we grouped components based on their functional similarity and frequency. This mapping, which cross-references strategies with outcomes and the Risk of Bias (RoB 2) assessment, is presented in Table 4.
Mapping of intervention components with outcomes and reported effectiveness

Note: The different colors indicate the level of risk of bias: green indicates a low risk of bias, yellow indicates a moderate risk of bias and red indicates a high risk of bias.
▲ = statistically significant effect in the intervention group; ▼ = statistically non-significant effect in the intervention group.
Following our methodology, interventions were categorized by primary outcomes, delivery settings and where possible, component approaches. This synthesis highlights “promising” interventions defined as those achieving statistical significance (p ≤ 0.05) for effectiveness and demonstrating a notable magnitude of effect (within their specific contexts), such as large odds ratios or effect sizes.
Interventions targeting help-seeking behaviors
Of the 29 studies targeting behavior, interventions in 16 (55.2%) were effective.
University/school settings (n = 6/12 effective studies)
Identification-based pathways: Proactive identification strategies proved efficient at converting problem recognition into service initiation. Automated universal screening (Student Assistance Program, SAP) among high school students (n = 12,909) increased service initiation fourfold (95% CI 2.0–7.9) by directly linking positive screens to SAP-recommended school or community-based services (Sekhar et al., Reference Sekhar, Batra, Schaefer, Walker-Harding, Pattison, Molinari, Rosen, Kraschnewski and Waxmonsky2022). Similarly, interactive avatar-based gatekeeper training for undergraduates (n = 117) that trained peers to recognize struggling students and direct them toward campus resources significantly increased help-seeking at campus counseling centers (OR = 2.3, p < .001) (Coleman et al., Reference Coleman, Black, Ng and Blumenthal2019). In India, a single-session, lay counselor-led classroom sensitization program for adolescents (n = 3,587) achieved an increase in school counseling referrals (OR = 111.36, 95% CI 35.56–348.77, p < .001) (Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021), eliminating access barriers, especially in a resource-constrained setting.
Knowledge with stigma reduction focus: College athletes receiving multi-component customized mental health literacy (athlete-focused) combined with social-contact-based stigma reduction videos and resource promotion (n = 107) showed help-seeking increases (OR = 5.06, p = 0.01) (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020) with the intervention explicitly including role-play exercises where athletes developed personalized help-seeking plans, converting knowledge into concrete action steps. School students receiving a 3-module, 3-h anti-stigma curriculum (didactic teaching, group discussion, homework on stigma/mental disorders) increased formal treatment-seeking when baseline symptom levels were high (OR = 3.90, 95% CI 1.09–13.87, p < .05) (Link et al., Reference Link, DuPont-Reyes, Barkin, Villatoro, Phelan and Painter2020).
Peer-delivered motivation and support: Undergraduate peer counselors trained in motivational interviewing (MI) who delivered a single psychoeducation + MI session to fellow students with needle anxiety (n = 61) significantly increased treatment-seeking behaviors (IR = 2.41, 95% CI 1.29–4.50, p = 0.006) (Finitsis et al., Reference Finitsis, Cruess, Pinnamaraju, Robinson and Woodruff2022).
Healthcare and facility-based settings (n = 4/10 effective studies)
In healthcare settings, high-intensity, clinician-delivered strategies outperformed passive referrals. Linkage models, where dedicated staff use MI strategies to navigate patients from identification to specialized care, demonstrated strong effects among high-risk clinical populations. Primary care linkage workers delivered SBIRT + MI-based case management (Recovery Management Checkups) for SUD patients (n = 266, mean age 48.3 years), resulting in 4.59-fold higher treatment initiation overall (p = 0.001); and more specifically for residential care (AOR = 3.31, 95% CI 1.28–8.57, p < 0.05); and intensive outpatient (AOR = 6.40, 95% CI 1.70–24.1, p < 0.01) (Scott, Reference Scott, Dennis, Grella, Watson, Davis and Hart2023). Similarly, maternal/child health nurses trained in MI conducted sessions with postpartum women (n = 541, mean age 31.5 years) targeting emotional distress, with MI increasing help-seeking OR = 4.0 (95% CI 1.6–10.1, p = 0.004) (Holt, Reference Holt, Milgrom and Gemmill2017). Veterans with PTSD symptoms (n = 234, mean age 50.9 years) who used the PTSD Coach app with clinician support (in-person/telephonic guidance from psychologists) showed OR = 3.91 (p = 0.016) for more than two specialty mental health visits among persistent cases (PCL-5 ≥ 33) (Possemato et al., Reference Possemato, Johnson, Barrie, Ghaus, Noronha, Wade, Greenbaum, Rosen, Cloitre, Owen, Jain, Beehler, Prins, Seal and Kuhn2023). Here, clinicians addressed motivational, technical or informational barriers.
Community-based settings (n = 6/7 effective studies)
Effective strategies in community settings included accessible low-intensity support paired with targeted outreach and stigma reduction to remove logistical and psychological barriers. In Nepal, trained female community health facility volunteers conducted proactive universal screening using the Community Informant Detection Tool across 286,838 health facility visits, identifying cases of depression, psychosis, alcohol/substance use and epilepsy and directly referring individuals to primary care (Jordans et al., Reference Jordans, Luitel, Lund and Kohrt2020). This approach significantly increased treatment registration (r = 0.42, p = 0.04), reflecting a modest but meaningful population-level effect in a low-resource setting.
A 6-week peer-led online support group (HOPE intervention) for adults with moderate-to-severe anxiety (n = 300, USA) deployed trained peer leaders in private Facebook groups, facilitating psychoeducation-based discussions (Ugarte et al., Reference Ugarte, Cumberland, Singh, Saadat, Garett and Young2023). Compared to control groups without peer leaders, intervention participants showed higher help-seeking behavior, such as requesting electronic resources (OR = 10.27, 95% CI 4.52–23.35) and engaging consistently with group posts (OR = 2.8, 95% CI 1.70–4.76). Similarly, telephonic single-session CBT for treatment-seeking (CBT-TS) delivered to military service members and Veterans at risk for suicide (n = 841, untreated at baseline) targeted attitudinal and practical barriers through belief modification that achieved significant treatment initiation (OR = 2.53) at 1 month and persisting (OR = 1.37) at 12 months (p = 0.05) (Stecker et al., Reference Stecker, Allan, Hoge, Ashrafioun and Conner2023). “Man Therapy” (n = 354 men at suicide risk) used masculine humor and language in their gender-responsive psychoeducation and self-help resources to align help-seeking with masculine autonomy, increasing professional help-seeking (OR = 1.55, p = 0.049) (Gilgoff et al., Reference Gilgoff, Wagner, Frey and Osteen2023). “Tell Your Story” (n = 103 refugee men, Arabic/Farsi/Tamil-speaking backgrounds) combined psychoeducation, video-based social contact (refugee men describing symptom experiences and help-seeking journeys) and cognitive reappraisal, which resulted in a specific reduction in self-stigma related to help-seeking itself (d = 0.42). Participants accessed approximately 0.69 additional help-seeking sources at follow-up (B = 0.69, 95% CI 0.19–1.18, p = 0.007), including informal (friends, family and community leaders) and formal sources (GPs, mental health professionals) (Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020).
Six studies also reported secondary outcomes; four of which were effective in decreasing help-seeking stigma (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020; Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Ries et al., Reference Ries, Livengood, Huh, Kerbrat, Fruhbauerova, Turner and Comtois2022; Gilgoff et al., Reference Gilgoff, Wagner, Frey and Osteen2023) and five were effective in improving knowledge about mental health conditions (Coleman et al., Reference Coleman, Black, Ng and Blumenthal2019; Link et al., Reference Link, DuPont-Reyes, Barkin, Villatoro, Phelan and Painter2020; Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021; Ries et al., Reference Ries, Livengood, Huh, Kerbrat, Fruhbauerova, Turner and Comtois2022; Gilgoff et al., Reference Gilgoff, Wagner, Frey and Osteen2023).
Interventions targeting help-seeking intentions
Of 26 studies targeting help-seeking intentions across settings, interventions in 19 (73.1%) proved effective.
University/school settings (n = 4/9 effective studies)
Resource promotion with MHL: Across educational settings, intention change was achieved through resource promotion (providing information about support services and treatment options, such as practical guidance on how to access care, including self-help resources/helplines/directories of local MH services/ professionals), often paired with mental health literacy (MHL) delivered in different formats. Mason et al. (Reference Mason, Johnstone, Riordan, Lie, Rapsey, Treharne, Jang, Collings and Scarf2022, n = 133 undergraduates) tested infographics vs. videos promoting campus services and found the infographic intervention significantly increased help-seeking intentions (M = 3.52 vs. M = 3.05, p = 0.035). Multi-component customized MHL + social contact + resource promotion for college athletes (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020, n = 107) significantly increased intentions for both eating pathology and general mental health help-seeking (η 2 = 0.09, p = 0.003).
Community-based settings (n = 14/16 effective studies)
Social contact: The most prominent strategy involved video-based social contact interventions, particularly tailored to viewer characteristics (e.g., profession, gender and cultural congruence). Seven studies were effective in this cluster: healthcare workers (Amsalem, Lazarov, et al., Reference Amsalem, Lazarov, Markowitz, Smith, Dixon and Neria2022; Amsalem, Wall, et al., Reference Amsalem, Wall, Lazarov, Markowitz, Fisch, LeBeau, Hinds, Liu, Fisher, Smith, Hankerson, Lewis-Fernández, Dixon and Neria2023), essential workers (Amsalem and Martin, Reference Amsalem and Martin2022), male construction workers (King et al., Reference King, Schlichthorst, Spittal, Phelps and Pirkis2018), young adults and adolescents (Kruger et al., Reference Kruger, Pitts, Denenny, DeLuca and Schiffman2022; Amsalem, Jankowski, et al., Reference Amsalem, Jankowski, Pagdon, Valeri, Yang, Markowitz, Neria, Pescosolido, Dixon and Martin2023) and refugee men (Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020).
Integrated psychoeducation + behavioral engagement: Adult and youth interventions combining mental health education with active skill-building or discussion/interactive activities showed significant intention gains. Brief single-session psychoeducation + CBT + MI-based strategies for adults with social anxiety (Tobias et al., Reference Tobias, Landy, Levin and Arch2022, n = 241, d = 0.18, p = 0.06) significantly increased treatment-seeking intentions. Psychoeducation + facilitated group discussion + social contact (tailored to match audience characteristics) + resource promotion for refugee men (Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020, d = 0.27, p = 0.027) and SGM youth (Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023, Δ = 0.17–0.19, p = 0.013–0.018) similarly increased help-seeking intentions.
Self-distancing writing tasks: Two studies testing emotion-regulation writing interventions targeting adults with depressive symptoms demonstrated significant improvements in help-seeking intentions. Hollar and Siegel (Reference Hollar and Siegel2020) conducted a series of three online studies (combined n = 632) in which participants completed writing tasks designed to induce self-distancing while imagining seeking help from the perspective of their ideal future self, significantly increasing help-seeking intentions, with the largest effect observed in Study 3 (n = 574, ηp2 = 0.11, p = 0.011). Similarly, writing prompts designed to induce positive emotional states (n = 136) showed significant intention gains (ηp2 = 0.04, p = 0.032, M = 4.09) (Straszewski and Siegel, Reference Straszewski and Siegel2018).
Among the studies (n = 7) that reported secondary outcomes, five interventions were effective in decreasing stigma (Hollar and Siegel, Reference Hollar and Siegel2020; Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Mason et al., Reference Mason, Johnstone, Riordan, Lie, Rapsey, Treharne, Jang, Collings and Scarf2022; Seidman et al., Reference Seidman, Wade and Geller2022; Amsalem, Wall, et al., Reference Amsalem, Wall, Lazarov, Markowitz, Fisch, LeBeau, Hinds, Liu, Fisher, Smith, Hankerson, Lewis-Fernández, Dixon and Neria2023), one was effective in increasing MHL (Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023) and one was effective in increasing gatekeeper efficacy (Coleman et al., Reference Coleman, Black, Ng and Blumenthal2019).
Interventions targeting help-seeking attitudes
Of the 12 studies targeting attitudes, 10 (83.3%) were effective. Most effective strategies moved beyond providing “facts” to using social contact either via video or peer narratives (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020; Amsalem, Wall, et al., Reference Amsalem, Wall, Lazarov, Markowitz, Fisch, LeBeau, Hinds, Liu, Fisher, Smith, Hankerson, Lewis-Fernández, Neria and Dixon2022; Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023).
Interventions tested in a school/university setting
MHL with interactive/social-contact elements: Universal MHL interventions that mapped symptom-treatment literacy to make help-seeking predictable and evidence-based (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020; Conceição et al., Reference Conceição, Rothes and Gusmão2022; Tay, Reference Tay2022) succeeded in attitudinal change. Conceição et al. (Reference Conceição, Rothes and Gusmão2022, n = 626 first-year university students in Portugal) delivered online psychoeducation combined with social contact and interactive elements (like quizzes), achieving significant attitude improvement (p < .001, Cohen’s f = 0.04). MHL sessions addressing barriers to treatment, such as cost, side effects, intervention modalities and medication myths about antidepressants and antipsychotics demonstrated significantly greater recognition of these interventions as viable treatment options (n = 174; U = 2,774.50–2,799, p < .001) (Tay, Reference Tay2022).
Among the studies (n = 5) that reported secondary outcomes related to stigma in help-seeking and MHL, two interventions were effective in decreasing self-stigma related to help-seeking (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020; Seidman et al., Reference Seidman, Wade and Geller2022) and two were effective in increasing MHL (Tay, Reference Tay2022; Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023).
Risk of bias
Most RCTs assessed with the RoB 2 tool were of moderate quality (n = 23), with common concerns in result selection, outcome measurement and missing data. Bias levels varied due to insufficient data, often resulting in the “no information” option. Detailed assessments are in Supplementary Appendix B.
Discussion
Despite our searches being conducted only 7 years after the Xu et al. (Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018) review, we identified 54 new studies published in this period that tested several help-seeking interventions, highlighting a growing interest in addressing demand-side barriers. Of the included studies, 36 reported interventions were effective in improving one or more outcome measures related to help-seeking.
Help-seeking interventions did not work through a single universal mechanism. Instead, their effectiveness depended on matching the intervention strategies to the main barrier faced by a given population (e.g., lack of awareness, identity-related stigma or practical access problems) for the outcomes targeted (behaviors, intentions and attitudes). For instance, brief digital social contact tended to work best to increase help-seeking intentions in general-population samples with low perceived need; more intensive, motivationally focused work tended to trigger behavior change in clinical populations already in contact with care; and school-based referral models were most effective to trigger help-seeking behavior when adolescents could recognize a problem but could not independently navigate access to services.
Clinical or at-risk populations required higher-intensity engagement addressing internal barriers (ambivalence, competing priorities) rather than external barriers (stigma, awareness) to elicit behavioral help-seeking. Motivational Interviewing (MI) and dedicated linkage models succeed by resolving motivational and logistical barriers simultaneously within the healthcare settings in increasing help-seeking behaviors (Holt et al., Reference Holt, Milgrom and Gemmill2017; Scott et al., Reference Scott, Dennis, Grella, Watson, Davis and Hart2023). Health-system integrated dedicated staff (e.g., primary care linkage workers or nurses) using MI-based strategies to resolve patient-level barriers (ambivalence about efficacy, time/cost constraints, stigma) during extended engagement eliminated post-intention logistical friction, translating into behavioral change. This works for clinical populations who have overcome awareness barriers but face internal motivation barriers, such as “Will treatment work?” or “Can I manage alongside responsibilities?” (Bischof et al., Reference Bischof, Bischof and Rumpf2021). MI addresses these through collaborative exploration of ambivalence. Dedicated linkage staff eliminates appointment scheduling, transportation and treatment selection friction that high-risk populations often struggle to navigate independently. However, these seem to be effective with adult clinical populations with acknowledged symptoms (SUD, postpartum distress, chronic mental illness) and may not be useful for those in crisis or denial of symptoms.
Despite the diversity of intervention approaches across educational, healthcare and community settings, several overarching mechanisms emerged associated with intervention success (McLaren et al., Reference McLaren, Peter, Tomczyk, Muehlan, Schomerus and Schmidt2023). Interventions targeting behavior change, effectiveness emerged through a consistent pattern. Whether via technology-enabled screening, peer training or in-person sensitization, the most effective interventions shared a critical outcome of removing friction between awareness, access and action, though they achieved this through mechanistically distinct approaches. Some interventions addressed the barrier of problem recognition (screening, gatekeeper training), while others addressed barriers of access to knowledge (sensitization with embedded pathways) or psychological ambivalence (peer-delivered MI). Across all settings, effective interventions matched their mechanisms to specific barriers to initiate behavior change, that is, once young people or patients recognized a need, the path to professional support was immediate, accessible and socially legitimized.
Adolescents with emerging symptoms require immediate, frictionless translation from symptom recognition to professional contact. School-based settings that enable direct or self-identification and immediate referral tend to eliminate this decision-making friction (Link et al., Reference Link, DuPont-Reyes, Barkin, Villatoro, Phelan and Painter2020; Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021; Sekhar et al., Reference Sekhar, Batra, Schaefer, Walker-Harding, Pattison, Molinari, Rosen, Kraschnewski and Waxmonsky2022). This creates a "recognition-to-action pathway” without a choice burden, where students learned they have a problem and know exactly how and where to access help. A notable mention of intervention is where students received mental health knowledge via video and discussion, then were given clear referral instructions (meet a counselor directly, drop a box outside their room or teacher referral), all on school premises, eliminating search and transportation barriers (Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021). Adolescents may have low symptom awareness combined with high social barriers to help-seeking, thus embedding identification and referral within the school day eliminates transportation, scheduling and parental navigation requirements. This seems effective for school-enrolled adolescents with emerging (not chronic) symptoms and accessible mental health services.
This review identifies a pronounced intention-behavior gap where, while intentions were effectively changed in 19 of 26 studies (73.1%) and actual behaviors were changed in only 16 of 29 studies (55.2%). This aligns with established literature (Rickwood and Thomas, Reference Rickwood and Thomas2012) suggesting that while social contact and MHL can successfully foster a “willingness” to seek help, the transition to “action” is frequently hampered by structural and psychological “friction.” Interventions that successfully bridged this gap such as the RMC-PC model (Scott et al., Reference Scott, Dennis, Grella, Watson, Davis and Hart2023) in the United States or lay-counselor sensitization (Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021) in India did so by proactively removing the burden of navigation from the individual to institutional systems, and addressing psychological (stigma, ambivalence), structural (navigation, appointment-seeking, treatment selection) and capacity barriers (time, transportation, competing priorities).
Intervention categories that were most commonly found to be effective were psychoeducation/MHL (n = 13), promotion of help-seeking resources (n = 11), social contact (n = 7), MI (n = 4) and screening (n = 3). Psychoeducation/MHL, social contact and help-seeking resource promotions were most effective when combined, improving all three outcomes in both the general population and those with mental health conditions. This aligns with earlier research showing that insufficient knowledge and stigma hinder individuals from seeking help (Mojtabai et al., Reference Mojtabai, Olfson, Sampson, Jin, Druss, Wang, Wells, Pincus and Kessler2011; Schnyder et al., Reference Schnyder, Panczak, Groth and Schultze-Lutter2017; Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018). Social contact interventions especially worked for help-seeking intentions in the general population (Thornicroft et al., Reference Thornicroft, Mehta, Clement, Evans-Lacko, Doherty, Rose, Koschorke, Shidhaye, O’Reilly and Henderson2016; Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018) and MI-based strategies combined with psychoeducation reported effectiveness for improving help-seeking behaviors in at-risk populations and people with mental health conditions (Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018). MHL/psychoeducation was also found to be effective in vulnerable populations like refugees and sexual/gender minorities (Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Han et al., Reference Han, Wang, Zhang, Wang, Ou, Ren, Cai, Liu, Li, Han and Chen2023).
Previous reviews show that help-seeking interventions improve formal help-seeking behaviors in individuals with, or at risk of, mental health conditions (Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018), but are less effective for the general population (Gulliver et al., Reference Gulliver, Griffiths, Christensen and Brewer2012; Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018). Mental health literacy improved help-seeking attitudes (d = .12 to .53) but not behaviors (d = −.01, .02); evidence for other interventions was limited (Gulliver et al., Reference Gulliver, Griffiths, Christensen and Brewer2012). Digital interventions with active personal involvement and social contact have been shown to effectively boost help-seeking intentions and may be more cost-effective than face-to-face methods (Evans-Lacko et al., Reference Evans-Lacko, Hahn, Peter and Schomerus2022). Studies also indicate that multi-component interventions are generally more effective for improving help-seeking outcomes than single-component interventions (Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018; Evans-Lacko et al., Reference Evans-Lacko, Hahn, Peter and Schomerus2022; van den Broek et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia, Patel, Singla, Velleman, Weiss, Garg, Sequeira, Pusdekar, Jordans and Nadkarni2023).
Low-intensity digital interventions, particularly social contact videos, could achieve high population-level impact on help-seeking intentions by making help-seeking appear less stigmatized and acceptable, without requiring additional clinical infrastructure. Most community-based studies targeting intentions that were social-contact-based and delivered online were effective (14 of 16; 87.5%). These effects were often stronger when the people shown in the videos resembled the target audience in age, gender, occupation or cultural background (i.e., demographic tailoring), because this reduces the sense that “people like me do not seek help” (King et al., Reference King, Schlichthorst, Spittal, Phelps and Pirkis2018; Nickerson et al., Reference Nickerson, Byrow, Pajak, McMahon, Bryant, Christensen and Liddell2020; Amsalem et al., Reference Amsalem, Yang, Jankowski, Lieff, Markowitz and Dixon2021; Amsalem et al., Reference Amsalem, Lazarov, Markowitz, Smith, Dixon and Neria2022; Amsalem, Jankowski, et al., Reference Amsalem, Jankowski, Pagdon, Valeri, Yang, Markowitz, Neria, Pescosolido, Dixon and Martin2023). This aligns with social contact theory, which posits that vicarious contact (e.g., via video testimonials) reduces stigma by disconfirming stereotypes and fostering ingroup identification with help-seekers, thereby increasing perceived normativity of help-seeking behavior (Allport, Reference Allport1954; Corrigan et al., Reference Corrigan, Vega, Larson, Michaels, McClintock, Krzyzanowski, Gause and Buchholz2013; Clement et al., Reference Clement, Van Nieuwenhuizen, Kassam, Flach, Lazarus, De Castro, McCrone, Norman and Thornicroft2012). Delivering these materials online also removes practical steps such as signing up for a session or attending a group, which is particularly important for people who do not yet feel a strong personal need for care (yet).
Studies indicate that mechanisms that act on intentions effectively promote behavior change (Xiao et al., Reference Xiao, Wang and Wang2019; Amsalem, Wall, et al., Reference Amsalem, Wall, Lazarov, Markowitz, Fisch, LeBeau, Hinds, Liu, Fisher, Smith, Hankerson, Lewis-Fernández, Neria and Dixon2022). These interventions can facilitate immediate changes in treatment-seeking behaviors by providing online counselor referrals. This underscores the potential of social contact-based video interventions as cost-effective, scalable strategies for promoting help-seeking intentions, attitudes and reducing stigma, particularly in resource-constrained settings (Evans-Lacko et al., Reference Evans-Lacko, London, Japhet, Rüsch, Flach, Corker, Henderson and Thornicroft2012, Reference Evans-Lacko, Hahn, Peter and Schomerus2022). Once produced, brief social contact videos can be disseminated to thousands while maintaining fidelity to the “active ingredient” (e.g., the peer narrative) via social media, clinical portals or websites at near-zero marginal cost per user (Clement et al., Reference Clement, Van Nieuwenhuizen, Kassam, Flach, Lazarus, De Castro, McCrone, Norman and Thornicroft2012; Lehtimaki et al., Reference Lehtimaki, Martic, Wahl, Foster and Schwalbe2021; Buntrock, Reference Buntrock2024; Amsalem et al., Reference Amsalem, Martin, Dixon and Haim-Nachum2025). It also does not require highly trained professionals for delivery, which is a significant availability and economic bottleneck in traditional mental health service expansion. Future research should explore whether incorporating behavior change elements into social-contact video interventions can effectively translate improved intentions and attitudes into actual behavior change.
While most of the evidence originates from high-income countries (HICs), the two LMIC studies provide critical signals for low-resource implementation. Jordans et al. (Reference Jordans, Luitel, Lund and Kohrt2020, Nepal, n = 286,838) demonstrated that community health volunteers conducting proactive screening achieved significant treatment registration by externalizing symptom recognition, essential in contexts with high social barriers to self-disclosure. Parikh et al. (Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021, India, n = 3,587) achieved significantly better outcomes through lay counselor-delivered classroom sensitization with immediate on-site referral options, highlighting that MHL alone fails without embedded physical access in resource-constrained settings. However, this limited evidence (two studies from South Asia) precludes definitive LMIC conclusions. Both succeeded through friction removal (externalized recognition, proximal access), suggesting context-matched structural solutions may generalize, but a lack of geographic diversity (no sub-Saharan Africa, Latin America) and unmeasured cost-effectiveness evidence prevent broad recommendations. For LMIC contexts, digital social contact appears promising as a scalable “gateway” (proven in HICs), while task-shared linkage models (volunteers and lay counselors) could function as essential “bridges” where specialist supply is limited.
One study that reported on mediation analysis found that positive emotions and attitudes together mediated the impact of message appeal on help-seeking intentions, suggesting a serial mediation effect (Hussain and Alhabash, Reference Hussain and Alhabash2022). However, most studies did not examine mediation analyses, limiting insights into optimizing these interventions.
Multi-component interventions were more effective for multiple help-seeking outcomes. Two studies (Martin et al., Reference Martin, Saulnier, Horvath and Anderson2020; Tobias et al., Reference Tobias, Landy, Levin and Arch2022) that effectively improved all three help-seeking outcomes combined psychoeducation, stigma reduction, resource promotion, single-session CBT and motivational strategies, and focused on specific clinical conditions (Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018; van den Broek et al., Reference van den Broek, Gandhi, Sureshkumar, Prina, Bhatia, Patel, Singla, Velleman, Weiss, Garg, Sequeira, Pusdekar, Jordans and Nadkarni2023).
Limitations
The inherent complexity of help-seeking as a construct, characterized by the lack of consensus on definitions and measurements as highlighted by Rickwood and Thomas (Reference Rickwood and Thomas2012), contributed significantly to the heterogeneity observed in our results. This diversity in how studies operationalized “help,” ranging from clinical appointments to online peer engagement, precluded a meta-analysis and underscores the need for the use of more standardized research frameworks in the future. Limited data and outcome variability reported by the included studies prevented meaningful conclusions on implementation outcomes. In an attempt to thoroughly examine the research landscape and limited studies in the area, the quality assessment of studies did not impact the weight given to them in the narrative synthesis. We did not search gray literature or publications in languages other than English, potentially biasing our results. The wide variation in sample sizes, with some as small as 24 participants, limits the precision and generalizability of our findings. Most studies did not explore the mechanisms of change, making it hard to identify which particular components affect help-seeking outcomes. Additionally, limited evidence from LMICs may hinder the applicability of findings to low-resource settings. LMIC-based evidence is restricted to just two countries from South Asia (Jordans et al., Reference Jordans, Luitel, Lund and Kohrt2020; Parikh et al., Reference Parikh, Hoogendoorn, Michelson, Ruwaard, Sharma, Bhat, Malik, Sahu, Cuijpers and Patel2021). Patterns suggest context-matched friction removal is effective, but geographic and systemic diversity across LMICs prevents definitive conclusions. Those implementing in LMIC contexts should conduct local formative research and cost-effectiveness analysis before scale-up.
Conclusion
Our findings align with previous research, confirming the effectiveness of MHL or psychoeducation, MI-based strategies and social contact interventions across multiple help-seeking outcomes (Gulliver et al., Reference Gulliver, Griffiths, Christensen and Brewer2012; Xu et al., Reference Xu, Huang, Koesters, Staiger, Becker, Thornicroft and Ruesch2018; Velasco et al., Reference Velasco, Antonia, Billings, Jimenez and Rowe2020; Evans-Lacko et al., Reference Evans-Lacko, Hahn, Peter and Schomerus2022). Social contact videos emerged to be consistently effective at increasing help-seeking intentions and attitudes.
Future research should focus on examining help-seeking outcomes in alignment with specific theories like TPB, exploring mechanisms of change and using standardized measures (Rickwood and Thomas, Reference Rickwood and Thomas2012). This approach will improve our understanding of how help-seeking can be enhanced and what mediates the relationship between intentions, attitudes and behaviors.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10183.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10183.
Data availability statement
All data analyzed in this study are derived from publicly available sources and are fully reported within the article and its Supplementary Materials. Extraction sheets used in this review are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Ankur Garg (AG) for their help in reviewing and resolving conflicts throughout the abstract and full-text screening process. We also extend our thanks to Neo Hou (NH) for assisting with data extraction and cleaning the data in the extraction sheet.
Author contribution
Conceptualization: A.N.; Data curation: S.B., S.S.I.; Formal analysis: S.B., B.B.; Investigation: S.B., S.S.I., M.P., N.N.; Methodology: A.N.; Supervision: Y.G., R.V., D.R.S., V.P.; Validation: S.B., Y.G., R.V., D.R.S., V.P., A.N.; Visualization: S.B.; Writing – original draft: S.B., B.B., S.S.I.; Writing – review and editing: S.B., B.B., Y.G., R.V., D.R.S., V.P., S.S.I., M.P., N.N., A.N. S.I. drafted an initial version of the manuscript, which was substantially reworked by S.B. to incorporate new data and refine the analysis. S.B. then continued developing revised drafts in collaboration with B.B. All authors contributed to reviewing the revised drafts before finalizing the submitted version of the study.
Financial support
This study was conducted as a part of the formative research for the IMPRESS trial, which aims to assess the effectiveness and cost-effectiveness of a community intervention in enhancing access to care and improving clinical outcomes for depression. The trial has been funded through a grant from the National Institute of Mental Health (NIMH), USA (Grant number R01MH115504). The funder had no role in the design, conduct, analysis or reporting of this systematic review and did not influence its findings or conclusions in any way.
Competing interests
The authors declare that there are no competing interests.




 Open access
Open access
Comments
Professors Judy Bass & Dixon Chibanda
Editors-in-Chief
Global Mental Health
27th October 2025
Manuscript title: Interventions to Improve Mental Health Help-Seeking Attitudes, Intentions and Behaviours: A Systematic Review of Recent Advances
Dear Prof Bass and Prof chibanda,
On behalf of my co-authors, I am submitting our manuscript (referenced above) for consideration in the Global Mental Health journal. This systematic review examines recent evidence on interventions that improve help-seeking for mental health conditions. Specifically, we critically appraise randomized controlled trials conducted since 2016 across diverse populations and settings worldwide.
Mental health conditions are a leading cause of global disability, affecting nearly one billion people and incurring significant social and economic costs. Despite the availability of effective treatments, a substantial treatment gap persists—particularly in low- and middle-income countries, where only about 14% of those in need receive care. While often attributed to limited-service availability, this gap is also perpetuated by demand-side barriers, including stigma, low mental health literacy, distrust of providers, and negative perceptions about help-seeking. Addressing these barriers is essential for encouraging proactive help-seeking, which can enable earlier diagnosis, reduce disease progression, and ease the burden on healthcare systems.
Our review synthesizes evidence on interventions that target help-seeking attitudes, intentions, and behaviours, highlighting both successful approaches and uncovering gaps in the help-seeking research literature, with the goal of guiding future research and practice to bridge the mental health treatment gap.
We believe that the Global Mental Health journal is a fitting home for this work given its commitment to advancing public health practice and translating scientific findings into actionable insights. Our review contributes to health improvement and service enhancement domains by providing evidence on demand-side barriers that affect mental health service utilization. By focusing on help-seeking interventions, our work offers valuable insights into strategies that can have immediate, practical impacts on public mental health practice worldwide.
The authors have no conflicts of interest to report. We thank you for considering this submission, and look forward to your response.
Yours truly,
Abhijit Nadkarni