


Introduction
The 22q11.2 deletion syndrome (22q11DS) is a recurrent copy number variant disorder that affects approximately 1 in 2,000–6,000 births (Refs Reference Swillen and McDonald-McGinn1, Reference Oskarsdottir, Vujic and Fasth2). Common complications of 22q11DS include conotruncal cardiac defects and subsequent neonatal hypoxia, endocrine dysregulation, including hypocalcemia secondary to parathyroid insufficiency, cleft palate and immune abnormalities (Ref. Reference Kobrynski and Sullivan3). None of those features occurs invariably in every affected patient, but the factors that determine the particular combination of outcomes in any individual case remain obscure.
In approximately 87% of 22q11DS patients, the hemizygous deletion occurs in a 3 megabases (3 Mb) ‘typically deleted’ region (TDR) containing 46 unambiguous protein-encoding genes (Refs Reference Motahari, Moody, Maynard and LaMantia4, Reference Karbarz5). In approximately 10% of patients, there is a nested deletion of approximately 1.5 Mb that uses the same proximal break point but a different distal break point that lays within the ‘typically deleted’ 3 Mb region (Refs Reference Shaikh, Kurahashi, Saitta, O’Hare, Hu, Roe, Driscoll, McDonald-McGinn, Zackai, Budarf and Emanuel6-Reference Kerstjens-Frederikse, Kurahashi, Driscoll, Budarf, Emanuel, Beatty, Scheidl, Siegel-Bartelt, Henderson, Cytrynbaum, Nie and Teshima8). Because one copy of the affected genes is still present in 22q11DS patients, the disease can be viewed as dysregulation (vs. obliteration) of pathways entailing these genes.
Clinically, patients with 22q11DS have a diminished number and function of T lymphocytes, and can present with a variety of immunological disorders that vary in their features, severity and changes with ageing (Ref. Reference Morsheimer, Brown Whitehorn, Heimall and Sullivan9). Much of the focus has been on T-cell defects but other immune cells, including B-cells, are also affected (Refs Reference Gennery, Barge, O’Sullivan, Flood, Abinun and Cant10, Reference Smith, Driscoll, Emanuel, McDonald-McGinn, Zackai and Sullivan11).
The immune abnormalities in 22q11DS are often attributed to thymic aplasia or hypoplasia, which occurs due to improper migration of neural crest cells during embryonic development (Ref. Reference Gennery12). Despite a decreased number of T-cells, several autoimmune diseases have been described in the syndrome (Ref. Reference Gennery12). The exact mechanism responsible for autoimmunity in 22q11DS is complex and likely varies among individuals. Possible mechanisms include impaired central negative selection of T cells, reduced number or function of Tregs and altered dendritic cell populations (Refs Reference Gennery12, Reference Costagliola, Cappelli and Consolini13). There is also evidence of increased percentages of inflammatory Th1, Th17 and memory T-helper cells in adults (Ref. Reference Vergaelen, Schiweck, van Steeland, Counotte, Veling, Swillen, Drexhage and Claes14).
Thymic hormones (e.g., thymosin, thymopoietin and thymulin) play an essential role in regulating T-cell differentiation and maturation and could play a role in the autoimmune aspects of 22q11DS (Ref. Reference Besman, Zambrowicz and Matwiejczyk15). These hormones are released into the general circulation and have a range of effects on other immune cells (NK, macrophages) as well as cytokines (Ref. Reference Besman, Zambrowicz and Matwiejczyk15). Thus, the deficiency of thymus-derived hormones in 22q11DS could have effects beyond the thymus itself. In autoimmune diseases, such as lupus and autoimmune arthritis, there is a decrement in circulating thymosin α1 levels (Ref. Reference Pica, Chimenti, Gaziano, Bue, Casalinuovo, Triggianese, Conigliaro, Di Carlo, Cordero, Adorno, Volpi, Perricone and Garaci16), and this hormone has been suggested as a possible therapeutic for autoimmunity (Ref. Reference Besman, Zambrowicz and Matwiejczyk15). In 22q11DS, the administration of thymosin has been used with the aim of enhancing T-cell number and function, although it is not currently used to treat the disorder (Ref. Reference Barrett, Wara, Ammann and Cowan17).
Although the enhanced risk for autoimmunity in 22q11DS is recognised, the accumulating evidence for this is often from case reports and has not been subjected to a systematic review. We considered the heterogeneity of study designs, populations, sample selection, quality and sample sizes in this first systematic review of the subject. Given that this is a multisystem illness, articles are often published in different specialty journals, and this underscores the need to gather this diverse research and clinical reports in a systematic fashion. In the current article, we provide a comprehensive and unbiased summary of the available literature on the presence of autoimmune disease in 22q11DS.
Methods
Eligibility criteria
Peer-reviewed and preprint edition studies that described autoimmune manifestations among people with 22q11DS (including DiGeorge, Velocardiofacial, Shprintzen and CATCH 22 Syndromes) and other conditions resulting from the same 22q11 microchromosomal deletion were selected. Autoimmune conditions were derived from the list of autoimmune disease referenced from the National Institutes of Health (NIH) (Ref. 18). Exclusion criteria included patients without 22q11.2 deletion, studies that did not report autoimmune outcomes, qualitative studies, conference proceedings, abstracts, studies published before 1968 and those not written in English.
Literature search
A comprehensive search for eligible studies was conducted in PubMed, Web of Science, EMBASE, CINAHL and Cochrane (Reviews and Trials) databases and was completed in October 2023 (Table 1). Search terms were divided into those for autoimmune conditions and for 22q11DS, with Boolean operators to search combinations of keywords. Full search strings can be found in Supplementary Table 1.
Databases and eligible studies on autoimmunity in 22q11DS

Data extraction
The PRISMA diagram (Figure 1) depicts the selection process. A total of 984 articles were imported into Covidence software, a web tool for managing systematic reviews. There were 182 duplicates removed, and two reviewers conducted independent screening of titles and abstracts using established inclusion and exclusion criteria.
PRISMA flow diagram of systematic review on 22q.11.2 Deletion Syndrome and autoimmunity.

This was followed by independent full-text screening of 154 studies. A third reviewer resolved any conflicts. Full-text screening involved deeper scrutiny of reported autoimmune diseases, details of the study population and study design. Autoimmune diseases corresponded to the list of conditions reported by the NIH (Ref. 18) to ensure standardisation and clinical relevance. Reasons for exclusion were documented at each stage of the screening process.
In the final review, 82 articles were included. Case reports and case series assessing autoimmune features in 22q11DS patients were included. Data were extracted systematically by defined study, participant and autoimmune diagnostic characteristics. Study characteristics extracted include title of the paper, lead author, year of publication, journal name, country in which study was conducted, specific geographic location, and aim of study. Data on methods included study design, funding sources, author conflict of interest, number of participants and inclusion and exclusion criteria. We collected participant data, including gender, race and/or ethnicity, age (reported the median age; otherwise, reported the mean age) and recruitment method. The presence of neuropsychiatry conditions was also documented. Autoimmune diseases were tabulated among the study population. To further confirm and analyse the reports of autoimmune statuses, information on the type and presence of autoantibodies was collected.
To evaluate transparency and risk of bias, quality assessment was conducted in Covidence using the Newcastle–Ottawa Scale (NOS) (Ref. Reference Wells19) and an adapted NOS for cross-sectional studies (Ref. Reference Herzog, Alvarez-Pasquin, Diaz, Del Barrio, Estrada and Gil20). For the studies, selection was analysed through the representativeness of the 22q11DS group (exposed), the selection of the comparison or control group, the definition of 22q11DS and any demonstration that the outcome was not present at baseline. Comparability on the basis of design, assessment of outcome/exposure, follow-up duration and adequacy of follow-up (cohort studies) and nonresponse rate for both groups (case–control) was also included to assess quality.
Results
There was a heterogeneous mix of study designs. Details of the 82 studies included in our review are in Tables 2 and 3. There were 34 studies that were either case–control, cohort or cross-sectional studies, most of which had an approximately equal male-to-female ratio (Table 2). Furthermore, 15 studies were retrospective, 10 studies were prospective, 2 studies were both prospective and retrospective, 5 studies were cross-sectional, 1 study was a mixed study (cross-sectional and cohort) and 1 study was not clear (Ref. Reference Klocperk, Paračkova, Bloomfield, Rataj, Pokorny, Unger, Warnatz and Šediva21). Cohort studies reporting a percent affected typically used incidence proportion. The majority of the studies were case reports or case series (n = 48), with 58.3% of the case reports being female participants (Table 3). Twenty one studies were conducted in North America (18 in the United States, 2 in Canada, and 1 in Mexico), 38 in Europe (7 in UK, 2 in Belgium, 2 in the Czech Republic, 2 in Finland, 4 in France, 1 in Germany, 1 in Greece, 14 in Italy, 1 in the Netherlands, 2 in Norway, 1 in Spain, and 1 in Sweden), 22 in Asia (1 in China, 1 in Iran, 3 in Israel, 8 in Japan, 1 in Korea, 1 in Kuwait, 1 in Qatar, 1 in South Korea, 2 in Taiwan, and 3 in Turkey) and 1 in South America (Brazil) (Tables 2 and 3). Notably, no studies have been reported from the African continent.
Cohort, case–control and cross-sectional studies on autoimmunity in 22q11.2 deletion syndrome

ADD: attention-deficit disorder; ADHD: attention-deficit/hyperactive disorder; AECA: antiendothelial antibody; AIHA: autoimmune haemolytic anaemia; AIN: autoimmune neutropenia; ANA: antinuclear antibody; ASD: autism spectrum disorder; GPC: gastric parietal cell; HC: healthy control; IBD: inflammatory bowel disease; IgA: immunoglobulin A; IgG: immunoglobulin G; ITP: immune thrombocytopenic purpura; JRA: juvenile rheumatoid arthritis; nc: not clear; ND: neurodevelopmental; NP: neuropsychiatric; RA: rheumatoid arthritis; RhF: Rheumatoid factor; SM: smooth muscle.
a n is the number in the study with each following autoimmune condition.
Case reports and case series on autoimmunity in 22q11.2 deletion syndrome

AIHA: autoimmune haemolytic anaemia; ANA: antinuclear antibody; IgA: immunoglobuIin A; IgG: immunoglobulin G; IgM: immunoglobulin M; ITP: immune thrombocytopenic purpura; JRA, juvenile rheumatoid arthritis; TSH: thyroid-stimulating hormone.
Regarding racial/ethnic distribution, 18 studies provided race information, out of which approximately 80% of the participants were white. Only 24 studies reported neuropsychiatric or neurodevelopmental conditions, including autoimmune psychosis among individuals with 22q11DS (Table 4).
Neuropsychiatric/developmental manifestation in 22q11.2 deletion syndrome

ADD: attention-deficit disorder; ADHD: attention-deficit/hyperactive disorder; ASD: autism spectrum disorder; ID: intellectual disability.
a Original text used the term ‘mental retardation’ and that the current preferred terminology is ‘intellectual disability’.
Out of the 82 studies reviewed, 65 studies included a blood work-up for autoimmunity, and 17 studies used medical records to retrieve information about autoimmune conditions, mostly retrospective studies. Seven studies were not primarily investigating autoimmune conditions but reported them as part of their findings.
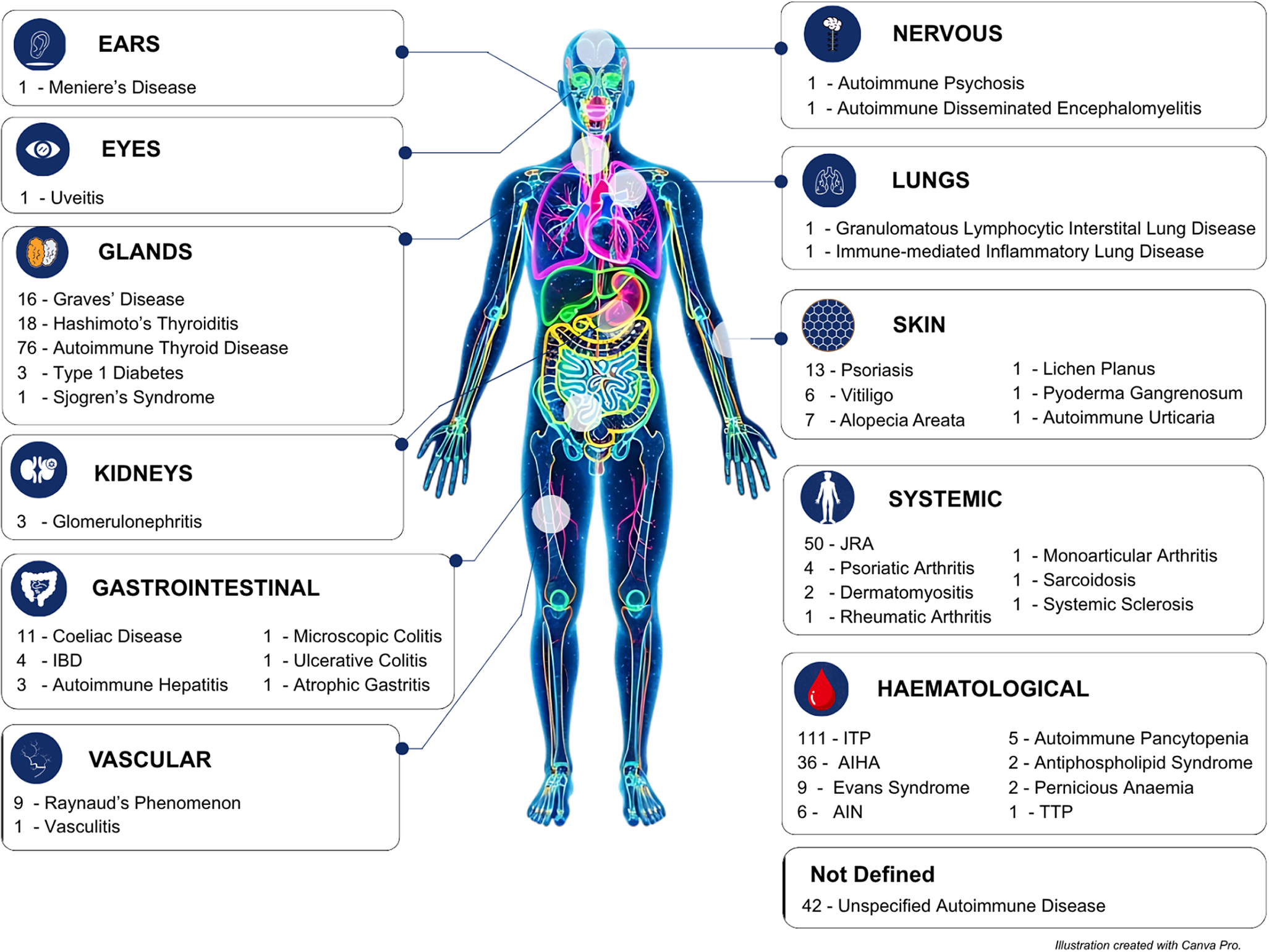
Figure 2 shows an overview of the autoimmune diseases detected in our review. We identified 40 autoimmune diseases and disorders. For 42 cases identified in three studies (Refs Reference McLean-Tooke, Spickett and Gennery22–Reference Wahrmann, Kainulainen, Kyto and Lempainen24), the autoimmune disease was not specified. Organ-specific autoimmune diseases were more frequently reported than systemic autoimmune diseases (Table 5). The most common autoimmune conditions in our review were immune thrombocytopenic purpura (ITP; 111 cases), and autoimmune thyroid diseases, which comprise Hashimoto’s and Graves’ disease (110 cases) but were sometimes not fully specified. In addition, autoimmune connective tissue diseases, particularly juvenile rheumatoid arthritis (JRA; 50 cases), were also common. Notably, 19 of these autoimmune conditions were rare and reported only once (in one individual with 22q11DS): autoimmune urticaria, autoimmune psychosis, atopic gastritis, acute disseminated encephalomyelitis, granulomatous lymphocytic interstitial lung disease, lichen planus, monoarticular arthritis, Meniere’s disease, pyoderma gangrenosum, rheumatoid arthritis, sarcoidosis, systemic sclerosis, Sjogren’s syndrome, thrombotic thrombocytopenic purpura, uveitis, ulcerative colitis, vasculitis, microscopic colitis and immune-mediated inflammatory lung disease. Nine autoimmune conditions were observed in five individuals or fewer (Figure 2).
Overview of autoimmune diseases by organ/system in 22q11DS patients. Note: This figure illustrates the number of reported cases of autoimmune diseases categorised by the affected organ or system in individuals with 22q11DS. Each system is represented by a labelled icon, with specific autoimmune conditions and their corresponding case counts. The most frequently affected systems include the haematological and glandular systems. A total of 42 cases were classified as unspecified autoimmune diseases, reflecting papers that did not name specific autoimmune conditions but instead being generally present. Supplementary Table 2 also contains cellular and molecular functions of genes within the typically region in 22q11DS. AIHA: autoimmune haemolytic anaemia; AIN: autoimmune neutropenia; IBD: inflammatory bowel disease; ITP: immune thrombocytopenia; JRA: juvenile rheumatoid arthritis; TTP: thrombotic thrombocytopenic purpura.

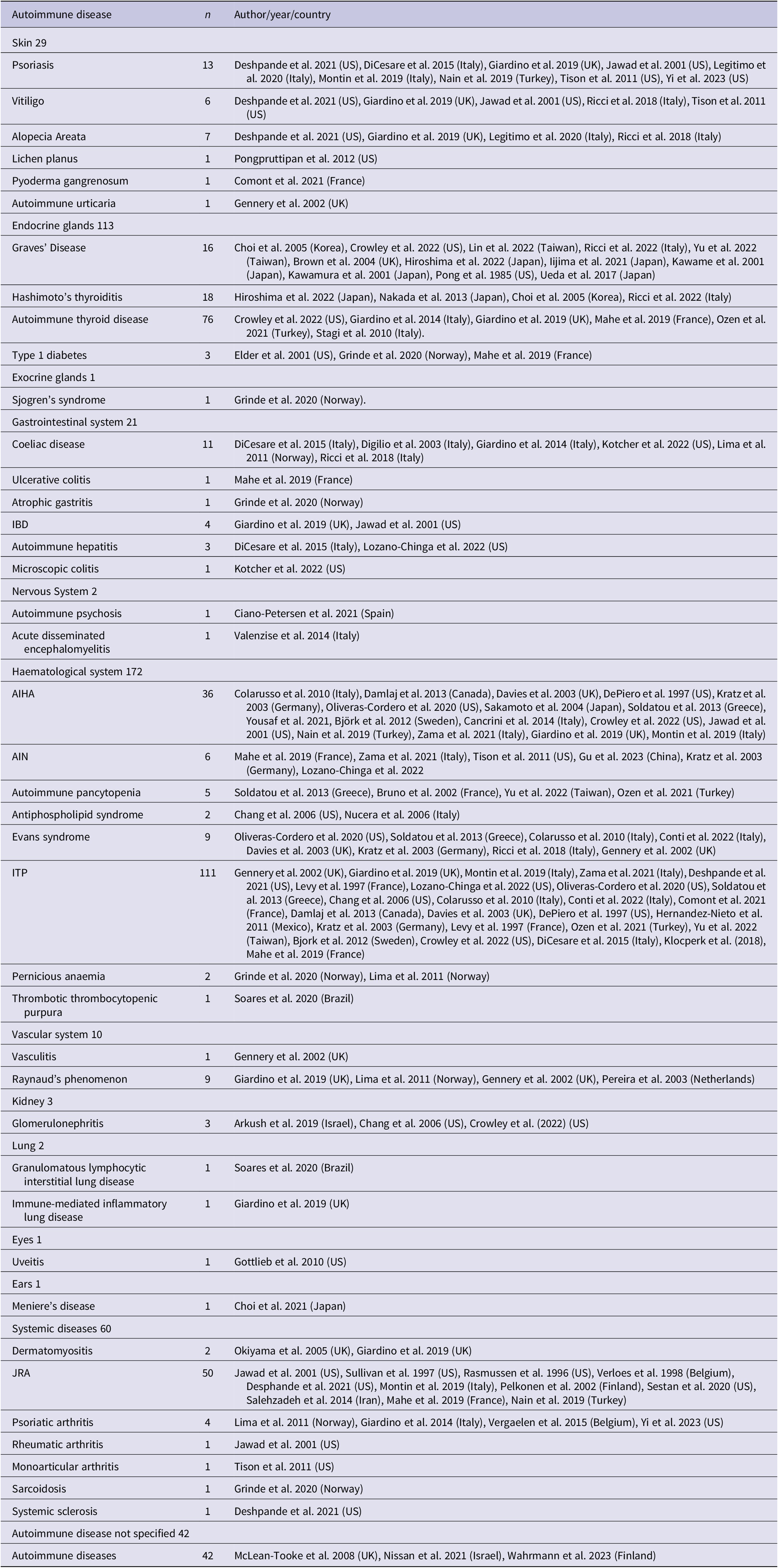
Summary of autoimmune diseases by organ/system in 22q11.2 deletion syndrome

AIHA: autoimmune haemolytic anaemia; AIN: autoimmune neutropenia; IBD, inflammatory bowel disease; ITP, immune thrombocytopenic purpura; JRA, juvenile rheumatoid arthritis.
Some articles reported autoantibodies in 22q11DS (Tables 2 and 3). Two studies included in our review did not report on autoimmune conditions; rather, they reported autoantibodies (Refs Reference Sedivá, Bartůnkova, Zachova, Polouckova, Hrusak, Janda, Kocarek, Novotna, Novotna and Klein25, Reference Ongen, Sağ, Temel and Eren26).
Skin
Twenty-one studies conducted in France, the United States, Italy, the United Kingdom and Turkey reported autoimmune conditions related to the skin among individuals with 22q11DS (Table 5). Psoriasis (n = 13) was the most common autoimmune condition affecting the skin, reported in nine articles. Other conditions included vitiligo (n = 6) reported in five articles, alopecia areata (n = 7) reported in four articles and autoimmune urticaria (n = 1) reported in one article. Lichen planus, pyoderma gangrenosum and psoriasis were documented as case reports. No autoantibodies related to the skin were reported.
Endocrine and exocrine glands
Twenty-four studies conducted in the United Kingdom, Japan, the United States, Korea, Taiwan, Italy, Norway, France and Turkey reported three autoimmune conditions involving the endocrine glands: autoimmune thyroid disease (comprising Graves’ disease and Hashimoto’s thyroiditis) and type 1 diabetes. Collectively, there were 110 cases of autoimmune thyroid disease reported. Three cases of type 1 diabetes were reported in three studies (Norway, the United States and France). Sjogren’s syndrome, the only autoimmune condition involving exocrine glands in our review, was reported in a study conducted in Norway (Table 5).
Gastrointestinal
Thirteen studies conducted in the United States, Norway, Italy, France and the United Kingdom reported autoimmune conditions involving the gastrointestinal system among individuals with 22q11DS. Coeliac disease (n = 11) was the most common gastrointestinal autoimmune condition, reported in six studies. Two studies reported inflammatory bowel disease (IBD; n = 4), although the type of IBD was not specified. However, one case of ulcerative colitis was reported in an article conducted in France. Autoimmune hepatitis (n = 3) was reported in three studies, and atrophic gastritis (n = 1) was reported in one article.
Neurological system
Two studies conducted in Spain and Italy, respectively, reported autoimmune psychosis (n = 1) and acute disseminated encephalomyelitis (n = 1) as case reports.
Haematological system
Sixty-four studies reported autoimmune conditions involving the haematological system. ITP was the most common autoimmune condition in our review, accounting for 64.5% of haematological cases. A study conducted in the United Kingdom (Ref. Reference Giardino, Radwan, Koletsi, Morrogh, Adams, Ip, Worth, Jones, Meyer-Parsonson, Gaspar and Gilmour27) reported that autoimmune cytopenia was the most common autoimmune condition in their cohort. Other conditions involving the haematological system include autoimmune haemolytic anaemia (n = 36), reported in 17 studies; autoimmune neutropenia (n = 6), reported in 6 studies; autoimmune pancytopenia (n = 5), reported in 4 studies; antiphospholipid syndrome (n = 2), reported in 2 studies; Evans syndrome (n = 9), reported in 6 studies; pernicious anaemia (n = 2), reported in 2 studies; and thrombotic thrombocytopenic purpura (n = 1), reported in 1 article. These studies were conducted in Italy, the United Kingdom, the United States, Canada, Sweden, the Czech Republic, Norway, France, Turkey, Taiwan, Kuwait, China, Mexico, Germany, Puerto Rico, Israel, Qatar, Greece and Brazil.
Vascular system
Five studies reported autoimmune conditions related to the vascular system. Raynaud’s phenomenon (n = 9), reported in four studies, and vasculitis (n = 1), reported in one article, were the two autoimmune conditions identified in our review involving the vascular system. These studies were conducted in Europe (the United Kingdom, Norway and the Netherlands), with two Raynaud’s phenomenon cases documented as case reports.
Kidney
Three studies conducted in the United States and Israel reported glomerulonephritis (n = 3), with two of the three studies being reported as case reports. No other autoimmune conditions involving the kidney were reported.
Eyes/ears
Uveitis (n = 1), an autoimmune condition involving the eye, was reported as a case report in an article conducted in the United States, and Meniere’s disease (n = 1), an autoimmune condition involving the ears, was also reported as a case report in an article from Japan.
Lungs
Granulomatous lymphocytic interstitial lung disease (n = 1) and immune-mediated inflammatory lung disease (n = 1) were reported in one article each.
Systemic autoimmune rheumatic diseases
Eleven studies reported seven systemic autoimmune conditions. JRA (n = 50) was the most common systemic autoimmune condition, reported in 11 studies conducted in Europe (Sweden, Italy, the United Kingdom, France, Turkey, Finland and Belgium) and one case conducted in Iran. Fourteen of these studies were case reports. Psoriatic arthritis (n = 4) was reported in four studies conducted in Italy, Norway Belgium and the United States. Dermatomyositis (n = 2) was reported in two studies conducted in the United Kingdom, whereas rheumatoid arthritis (n = 1), monoarticular arthritis (n = 1), sarcoidosis (n = 1) and systemic sclerosis (n = 1) were reported in one article each conducted in the United States and Norway.
Quality assessment
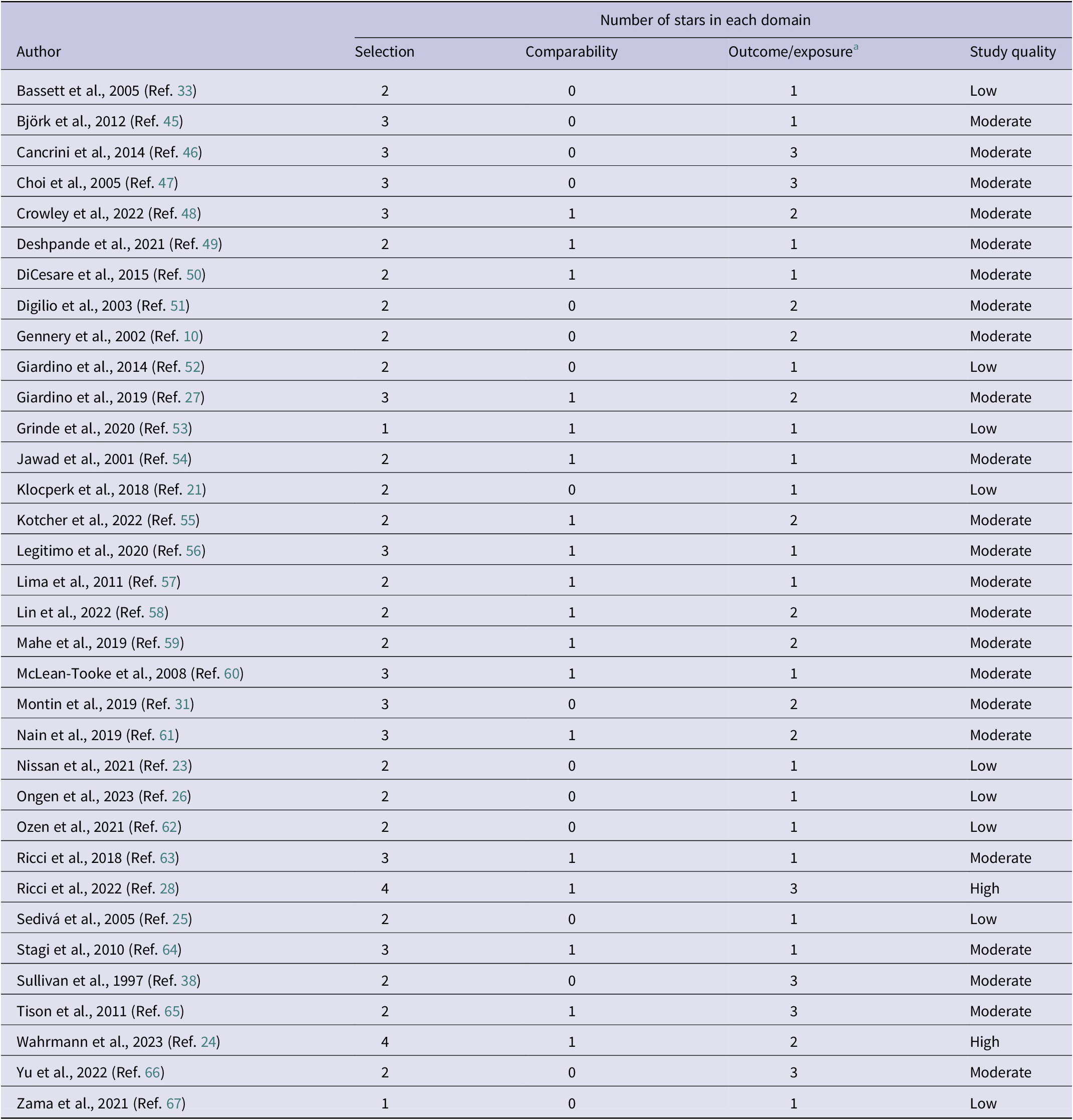
The quality of the included studies (cohort, case–control and cross-sectional) was assessed using the NOS. This scale measures study quality based on selection, comparability and the ascertainment of exposure/outcome. The scale has an eight-item instrument for cohort or case–control studies, and the rating system ranges from 0 to 9 stars. Studies with scores ≥7 points represented low risk of bias (high quality), 4–6 points as moderate risk of bias (intermediate quality) and those with a score of 1–3 points as high risk of bias (low quality).
Two of the 34 studies had a low risk of bias with a score of 7 (high quality). Twenty-three studies scored 4–6, showing moderate risk of bias and, thus, intermediate quality. Nine studies had a high risk of bias scoring between 1 and 3 points (Table 6).
Newcastle–Ottawa Quality Assessment Scale for cohort, case–control and cross-sectional studies

a Outcome for cohort and cross-sectional studies; exposure for case–control study.
Of the studies with low quality, the percentage of 22q11DS patients with autoimmunity was estimated to be 2.1%–29.4%. For studies with moderate quality, autoimmunity was estimated to be present in 0.7%–47% of 22q11DS patients. For the two studies with high quality, Ricci et al. (Ref. Reference Ricci, Sarli, Lodi, Canessa, Lippi, Azzari and Stagi28) reported that 21.9% had autoimmunity. The specific autoimmune diseases reported were Hashimoto’s thyroiditis and Grave’s disease. For Wahrmann et al. (Ref. Reference Wahrmann, Kainulainen, Kyto and Lempainen24), 29.6% had autoimmunity. However, the specific autoimmune diseases were not reported.
Overview and discussion
We performed a systematic analysis of the diverse evidence and heterogeneity of autoimmune diseases in 22q11DS. Autoimmunity is recognised clinically as a complication of 22q11DS, and there have been several excellent reviews (Refs Reference McLean-Tooke, Spickett and Gennery22, Reference Sullivan29, Reference Giardino, Romano, Lougaris, Castagnoli, Cillo, Leonardi, La Torre, Soresina, Federici, Cancrini and Pacillo30). However, there has not been a systematic, comprehensive and unbiased evaluation of the evidence. We performed this review utilising a transparent and rigorous methodology to thoroughly review and assess 82 studies across a variety of designs.
Collectively, the reviewed literature was comprised of diverse and inconsistent study designs. A large number of studies were case reports or case series. Many studies did not describe a thorough rationale for the selection of patients or research subjects. Thus, selection bias is likely, and a pooled prevalence estimate could be unreliable because many studies lacked a clear quantification of the total population under consideration at a given time. Nevertheless, our systematic approach provides the framework for future studies, and we identify major gaps in literature.
Our analysis suggested several facets of autoimmunity in 22q11DS, including the hierarchy of the specific organ systems involved. Haematological autoimmune findings were the most common, reported in 64 studies. These included ITP, which comprised 24% of the diagnosed autoimmune diseases, autoimmune haemolytic anaemia (8%) and Evans syndrome (2%). A prior study also suggested that blood cells are the most common target of autoimmunity in 22q11DS (Ref. Reference Montin, Marolda, Licciardi, Robasto, Di Cesare, Ricotti, Ferro, Scaioli, Giancotta, Amodio and Conti31). This same study reported that specific T- and B-cell immunophenotypic anomalies predicted subsequent haematological autoimmunity (Ref. Reference Montin, Marolda, Licciardi, Robasto, Di Cesare, Ricotti, Ferro, Scaioli, Giancotta, Amodio and Conti31).
Autoimmune thyroid disease was also common, accounting for 24% of the overall cases of autoimmune diseases we counted. The thyroid is often affected by autoimmunity in the general population (Ref. Reference Ricci, Sarli, Lodi, Canessa, Lippi, Azzari and Stagi28), and we found that both Graves’ disease and Hashimoto’s thyroiditis were well represented among the cases. In a longitudinal study of children with 22q11DS, 16 of the 73 patients (21.9%) developed autoimmune thyroid disease before 18 years of age, and 20.5% developed Hashimoto’s thyroiditis, whereas only 1.4% developed Graves’ disease (Ref. Reference Ricci, Sarli, Lodi, Canessa, Lippi, Azzari and Stagi28). We found that many studies did not specify the type of autoimmune thyroid disease detected.
Various gastrointestinal autoimmune diseases were identified in our study, with coeliac disease being the most common. This may be relevant to the psychiatric manifestations of 22q11DS, because coeliac disease is associated with schizophrenia (Ref. Reference Eaton, Mortensen, Agerbo, Byrne, Mors and Ewald32), and individuals with 22q11DS have an extremely high rate of schizophrenia (Refs Reference Bassett, Chow, Husted, Weksberg, Caluseriu, Webb and Gatzoulis33, Reference Murphy, Jones and Owen34).
However, only 24 papers reported on neuropsychiatric or neurodevelopmental conditions among individuals with 22q11DS. These disorders included autism spectrum disorder, developmental delay, attention-deficit/ hyperactive disorder and schizophrenia. This is not surprising because these disorders are known to be exceptionally common in 22q11DS (Ref. Reference Jonas, Montojo and Bearden35), but we could not calculate whether autoimmunity impacted their prevalence or presentation because the relevant studies reviewed are not conductive to this analysis (see above). Hypocalcemia, caused by hypoparathyroidism, is a well-established complication of 22q11DS and has been reported to be associated with haematological autoimmunity as well as neurodevelopmental delay (Refs Reference Montin, Marolda, Licciardi, Robasto, Di Cesare, Ricotti, Ferro, Scaioli, Giancotta, Amodio and Conti31, Reference Muldoon, Ousley, Kobrynski, Patel, Oster, Fernandez-Carriba, Cubells, Coleman and Pearce36).
Autoimmune diseases of the skin were detected in several different studies in Europe and the United States, with psoriasis, vitiligo and alopecia areata being the most common. Autoimmunity conditions of the eyes, lung and kidney were also reported, although these were relatively rare. Thus, multiple organs are affected by autoreactive immune mechanisms in 22q11DS.
Systemic autoimmune conditions were also common, which underscores the need for diverse specialists in treating and diagnosing patients with 22q11DS (Ref. Reference Oskarsdottir, Boot, Crowley, Loo, Arganbright, Armando, Baylis, Breetvelt, Castelein, Chadehumbe and Cielo37). An increased rate of JRA in 22q11DS was suggested over 25 years ago (Ref. Reference Sullivan, McDonald‐McGinn, Driscoll, Zmijewski, Ellabban, Reed, Emanuel, Zackai, Athreya and Keenan38), and this is one of several skeletal disorders affecting patients with 22q11DS (Ref. Reference Homans and Castelein39). We also found evidence for autoimmune conditions of the vascular system (i.e., Raynaud’s phenomenon and vasculitis).
Genes that are in the TDR participate in a wide variety of cellular and molecular processes, and we would expect many of these processes to be affected by the underexpression of these genes. This could interact with autoimmunity in several ways. For example, thyroid dysfunction is known to occur in 22q11DS due to the underdevelopment of the third and fourth pharyngeal pouches (Ref. Reference Weinzimer40), and an autoimmune attack on this gland could exacerbate or complicate hypothyroidism. Another possible mechanism involves the underexpression of 22q11DS genes in immune cells or in the target organ of autoimmunity This could result in the breaking of immunotolerance by abnormalities in immune receptors, cell trafficking, or apoptosis in immune tissues or the target organ. Whether a given individual with 22q11DS develops an autoimmune disease may depend on their human leukocyte antigen type, genetic polymorphisms outside the TDR and their particular environmental exposures.
The confidence in the estimated frequency of autoimmune diseases in 22q11DS is limited because of the inclusion of many studies with methodological limitations. This is reflected in the low and moderate scores on the NOS scale, mostly identified in the selection and comparability domains. Some studies did not adjust for confounders, whereas others did not report on the comparability of the groups included. Thus, these weaknesses lead to a potential for bias, indicating that the observed frequency of autoimmune diseases in 22q11DS is imprecise.
Comanagement of patients with 22q11DS in a multidisciplinary setting is warranted. This approach addresses the diverse medical and psychosocial needs of patients. Ideally, clinics specialising in 22q11DS will be arranged so that a patient can visit multiple specialists (e.g., haematologist, immunologist, endocrinologist, cardiologist, speech therapist and psychologist) on the same day based on their particular needs. For example, such a clinic might operate once a month with all specialists being available that day.
Gaps and limitations
Our review identified several gaps in the clinical and research evidence connecting 22q11DS to autoimmunity. Collection of the articles included in this review was completed by October 2023, thereby missing newer reports. The majority of the studies (59%) were case reports. Among the rest of the studies, the rationale for the selection of the individuals included was often not clearly stated. Most studies were from Europe, with most of the rest being from either North America or Asia. There was substantial heterogeneity in both the age of the patients and the criteria or methodology used for diagnosis. Many of the reports of diseases known to be caused by autoantibodies did not perform autoantibody testing. A finding in our quality metrics for case–control, cohort and cross-sectional studies indicated a wide range of quality and potential biases. Nonetheless, the reliance on the NOS can involve some subjective interpretation, which was minimised through independent assessment by two reviewers. However, a degree of uncertainty remains.
To maximise the number and type of studies included in our review, we used a broad definition of autoimmune disease based on criteria put forth by the NIH (United States). It is possible that some of the autoimmune conditions that we captured may have had a more complex aetiology besides (or in addition to) autoimmunity.
Although a meta-analysis would be desirable, this systematic review found that the data are not very conducive to meta-analysis. There was substantial methodological and statistical heterogeneity even among the case–control and cohort studies. Different diagnostic criteria and outcome measures were used, and the ambiguity as to the source of the sample and population argues further against attempting to pool studies for meta-analysis until more primary data become available.
Despite these limitations, this review fills a major gap by our in-depth analysis, which elucidates the variety of autoimmune diseases detected in 22q11DS, and their comorbidity with neuropsychiatric disorders. The benefits of shedding light on this important topic outweigh the limitations.
Expert and topical summary
This systematic review confirmed that autoimmunity is a component of 22q11DS. However, there is a major need for a thorough epidemiological evaluation of autoimmune prevalence across organ systems, as well as to determine relevant comorbidities and disease course in ethnically and geographically diverse populations affected by 22q11DS. Montin et al. (Ref. Reference Montin, Marolda, Licciardi, Robasto, Di Cesare, Ricotti, Ferro, Scaioli, Giancotta, Amodio and Conti31) estimated the prevalence of autoimmunity among 358 persons with 22q11DS to be 24%. The current review broadens the view of 22q11DS and demonstrates the diverse organ systems affected.
Neuropsychological disorders are a very common feature of 22q11DS (Refs Reference Bassett, Chow, Husted, Weksberg, Caluseriu, Webb and Gatzoulis33, Reference Murphy, Jones and Owen34, Reference Karayiorgou, Gogos, Galke, Jeffery, Nestadt, Wolyniec, Antonarakis, Kazazian, Housman, Driscoll and Pulver41, Reference Fiksinski, Hoftman, JAS and Bearden42), and an autoimmune aetiopathogenesis is possible in some of these cases (Ref. Reference Jeppesen and Benros43); however, we found that few of the case–control and cohort studies reported expressly on psychological or specific neurodevelopmental conditions. This emphasises the need for a deeper investigation of the pathophysiological connection between autoimmunity and neuropsychiatric manifestations of 22q11DS.
There has been substantial progress in the last two decades on understanding the immunology of autoreactivity in 22q11DS, which is also informed by researching other inborn errors of immunity (Ref. Reference Giardino, Romano, Lougaris, Castagnoli, Cillo, Leonardi, La Torre, Soresina, Federici, Cancrini and Pacillo30). This immunological work holds promise for new therapies, and relevant mouse models of 22q11DS can help inform both pathophysiology and aid in the development and testing of therapeutic modalities (Ref. Reference Crockett, Kebir, Benallegue, Adelman, Gur, Sullivan, Anderson and Alvarez44).
An ensemble of specialists work to improve the lives of persons with 22q11DS. The work of all these specialties will benefit from a better understanding of the wide spectrum of autoimmune manifestations in this disorder.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/erm.2026.10031.
Acknowledgements
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of Emory University.
Funding statement
No specific funding was received for this work.
Competing interests
The authors declare that there are no competing interests relevant to this work.
Ethical standard
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines.




 Open access
Open access