

1. Extraction
For the bulk of the 20th century, researchers and clinicians primarily justified the biomedical research enterprise on utilitarian terms: insofar as the scientific research had the prospect of benefitting society as a whole, saddling the risks and burdens associated with research on particular individual participants was considered to be ethically justified, at least under certain conditions. Some researchers explicitly articulated that these burdens can be imposed on individuals without their consent. For instance, Louis Lasagna, a major figure in the middle of the 20th century, otherwise known for advocating for higher scientific standards for biomedical research, put it in the following terms: “In clinical investigation, as in other societal activities, the good of the individual and the good of society are often not identical and sometimes mutually exclusive … I believe it is inevitable that we will continue to benefit on occasion form the contributions — sometimes involuntary — of the few.”Reference Lasagna, Mendelsohn, Swazey and Taviss1
People with intellectual and ddevelopmental disabilities (IDD) were often among the “few” whose bodies were involuntarily used as a means for the purported social good. They were selected in part due to the eugenic logics dismissive of their common humanity prevalent in medicine at the time and in part due to researcher expediency that comes with studying institutionalized or incarcerated populations.Reference Chapman, Ben-Moshe, Chapman and Carey2 Consider, for example, the experiments at the Willowbrook State School, where children with IDD were deliberately infected with hepatitis to track the trajectory of the disease, or the radiation experiments at the Walter E. Fernald School where, without parental knowledge, residential students (again with IDD) who were members of the “Science Club” participated in non-therapeutic nutrition studies that included the ingestion of radioactive iron and calcium.3 These are some of the more egregious examples of how researchers exposed people with IDD to risks in the name of research.Reference Iacono and Carling‐Jenkins4 However, it is important to note how pervasive a practice it was for people with IDD to be recruited for research purposes. Take. for instance, the prevalence of biomedical research that was conducted in prison settings in the past. Currently US prisons and jails confine a disproportionate amount of inmates with IDD, and these disparities were even more glaring in the 1960s and 70s, with up to 40% of inmates at the time likely to have had an IDD.Reference Vallas5 By 1972, more than 90% of all investigational drugs were first tested on US prisoners.6 Some may want to separate the vulnerabilities that come with intellectual disability from those that come with institutionalization and incarceration. But it is important to realize how often people with IDD were subjected to research due in part to their involuntary confinement.
Moreover, these studies were conducted at a time when ethical standards for research were largely self-regulated and enforced in a piecemeal fashion. There was a general expectation that agreement to participate in research should be sought and that researchers’ conduct should be publicly defensable, especially to one’s scientific peers. However, the primary mode of enforcement for research misconduct was the researchers’ own conscience and the threat to their personal and professional reputation. As Robert Baker chronicles, “even in America’s leading institutions, the mechanisms of research review in the 1960s were pro forma, undermined by researchers’ laissez-faire morality, their reluctance to submit to peer review, and their hesitation to pronounce judgment on each other.”Reference Baker7
It is useful to look at the underlying structural context and power relations endemic of institutionalization that gave rise to these practices — both in residential schools like Willowbrook and more broadly in prison settings. The totalizing nature of prisons, state schools, and hospitals for the “feeble-minded” offered for researchers a convenient sample of subjects who could be closely monitored, scheduled, and compared.Reference Goffman8 But also in these settings, researchers who worked closely with the medical directors and institutional superintendents were able to get away with more and were less accountable when they conducted research on these stigmatized groups of people. Consider this description of the conditions for research in the Ferald School, according to the The Massachusetts Task Force, in their investigation of the radiation experiments:
Until the 1970s … There were no human rights committees or institutional review boards. If the Superintendent (in those days required to be a medical doctor) “cooperated” in an experiment and allowed residents to be subjects, few knew and no one protested. If nothing concerning the experiments appeared in the residents’ medical records, if “request for consent” letters were less than forthright, or if no consent was obtained there was no one in a position of authority to halt or challenge such procedures.
Just as those who were institutionalized were hidden from public view, so was the research that was conducted on them.9
While extraction and abuse were often the outcomes of research conducted in these settings, we suggest that domination was an underlying structural condition that made such outcomes possible. Institutionalization created a domain for domination on the part of researchers over the will and livelihood of their research subjects, who were also under their custodial care as their wards.
Tom O’Shea delineates two features of domination. First, domination takes place when someone has the capacity to subject you to their power, not only when they actually exercise that capacity. This insight draws on Cicero’s description of the particular evil of slavery: “the most miserable feature of this condition is that, even if the master happens not to be oppressive, he can be so should he wish.”Reference Skinner, van Gelderen and Skinner10 Insofar as researchers were generally left to their own discretionary power about what constitutes ethical research and justifiable risks, researchers had such a capacity. Individual researchers may have cared about their participants and acted beneficently towards them; however, there was little infrastructure or regulatory safeguards to hold them accountable for the decisions that they were making. Peer judgment did serve as an accountability measure, but such tools were effective only insofar as researchers’ peers could successfully level criticism, a task complicated by (1) shared biases and blindspots and (2) a relative freedom of researchers to circumscribe their peer group to like-minded people.11
The second feature of domination is the arbitrary nature of the power wielded by the dominating party. On O’Shea’s description, “the master dominates because his power over the slave is controlled by nothing other than his own choice (or arbitrium).”Reference O’Shea12 The superintendents of institutions and the physician-researchers that worked closely with them were not only charged with managing the daily lives of the people under their custodial responsibility, but were also the public facing “experts on the conditions and individuals housed within the institution’s walls.”Reference Carlson13 They were understood as the expert arbiters of what, for instance, constituted an elevated risk of exposure to hepatitis in a research setting as opposed to the risks wards were exposed to in their everyday institutional lives, even as these same men were also in charge of the everyday living and sanitary conditions that allowed hepatitis to spread.
Both of these features of domination were present in institutionalized settings such as Willowbrook. People with IDD were often left under the power of people who enjoyed wide discretion to make arbitrary judgments about who would be subjected to research and on what terms. Note that the wrongness of domination does not require that the dominated party must have decisional capacity. That is, a person does not need to have the “ability to understand information relevant to making an informed, voluntary decision to participate in research” to be subject to the arbitrary will of another.14 The concern is not that there is some possibility of interference in your capacity to make your own decisions, but rather that someone else has the power to make decisions for you in a way that can be arbitrary and is largely unaccountable.
Being subject to such power can lead to psychological insecurity and servility on the part of the dominated, who are incentivized to behave in ways that could garner the good graces of those who wield power over them.Reference O’Shea15 Cashed out in this way, the oppressive nature of dominating relationships cannot be ameliorated by good intentions or empathy on the part of the dominating party. As long as someone is subjected to the arbitrary decisions of an unaccountable other, without recourse to contest these choices, they are being dominated. Vulnerability to domination is not unique to people with IDD, but this population may be particularly vulnerable due to their impaired cognition and their reliance on the support others provide in their daily lives.
While particularly pronounced in the institutionalized setting, dominating relations of power were a pervasive feature of research at the time. By the 1950s, the National Institutes of Health (NIH) already put in place ethical guidelines for their intramural research; however, when it came to those outside the NIH, “the prevailing position of NIH … was that extramural researchers should be guided by their own professional judgment.”Reference Bonnie16 Researchers thus enjoyed broad discretionary power over their research subjects to impose their own will and their own conception of what constitutes ethically appropriate and socially valuable research onto others. This discretionary power was explicitly justified by some of the ethicists and influential researchers at the time as an inherent feature of the research enterprise. For instance, in 1967, at a Colloquium at the American College of Physicians, Walsh McDermott criticized the recent FDA regulations and the Declaration of Helsinki for codifying the primacy of individual rights over the public good, stating:
“There is no escape from the fact that, if the future good of society is to be served, there will be times when the clinical investigator must make an arbitrary judgment with respect to the individual … Society may not have given us a clear blueprint for clinical investigation, but it has long given us immense trust to handle moral dilemmas of other sorts, including many in which, in effect, we have to play God.”Reference McDermott17
2. Protection
Relying primarily on the self-regulation by researchers and the pressure posed from professional and reputational concerns proved unwise. The revelations of the gross human rights abuses taking place throughout the 20th century in the name of science, such as Tuskegee, led to a public reckoning in the US about the aims of research and the appropriate limits on what researchers should be allowed to do. In this section, we suggest that while the protections that were put in place offered some safeguards against the most egregious of ethical abuses, they did not fully attend to the possibility of domination within the research context and so did not cover all the potential ways in which people, especially those in the most vulnerable social positions, continue to be subject to the arbitrary will of others. This is particularly pronounced when we pay attention to the way that regulatory protections regarding people determined to lack decisional capacity were defined and justified.
A National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research convened in 1974. After four years of deliberation, the commission issued the Belmont Report, which identifies the basic ethical principles and guidelines for human subjects research in the US. The Belmont Report articulated three pillars of ethical research: Respect for Persons, Beneficence, and Justice. Growing out of this guidance, US human subject protection regulations were created including the federal regulations known as the “Common Rule,” which establishes standards, institutions, and procedures for ethical recruitment, selection, and protection of participants for human subjects research.18
The Common Rule attempted to operationalize the three ethical principles of the Belmont Report into practice. Notably, in the Belmont Report, respect for persons was broken up into two guiding values, first, “that individuals should be treated as autonomous agents, and second, that persons with diminished autonomy are entitled to protection.”19 For individuals with consent capacity, including for those individuals with IDD, respect for persons is operationalized by the Common Rule and by other regulations as the requirement of informed consent to research.20 When it comes to people who are determined to lack capacity to consent to a particular research study, the Belmont Report does not distinguish between what counts as respecting them and what counts as acting beneficently towards them. In contexts where the individuals who are determined to lack capacity do not stand to benefit from the research and face the risk of harm, protection may just mean exclusion. The Belmont Report states that “the extent of protection afforded should depend upon the risk of harm and the likelihood of benefit.”21 Individuals determined to lack capacity may accordingly only be allowed to participate in contexts where they face minimal risks or where they personally stand to benefit from research participation.
This protective position of the Belmont Report plays out in what research is generally allowed to be conducted on persons determined to lack capacity today. Through a combination of federal regulations and professional ethical guidance, people who lack capacity are generally only permitted to participate in research under the following conditions:
1. Necessity Requirement: People determined to lack capacity can be included only when the study cannot be successfully conducted without their enrollment, and
2. Minimal Risk Requirement: If research participation offers no prospect of direct benefit, people determined to lack capacity can be included only when study participation is no more risky than what they would typically encounter in their daily life.Reference Wendler22
3. Benefit Requirement: If the research is more than minimal risk, people determined to lack capacity can be included only when study participation offers the prospect of direct benefit to them.Reference Mintz, Wasserman, Reynolds and Wieseler23
4. Surrogate Authorization Requirement: People determined to lack capacity can be included only through a process of surrogate approval of a legally authorized representative.24
Of these conditions, only the Surrogate Authorization Requirement is formalized as a legal mandate in the US federal regulations for clinical research.Reference Segal25 The other conditions, while not legally required according to US federal regulations, are promulgated by patient advocacy groups,Reference Association26 international research ethics guidelines,27 and are sometimes enforced through state and local law or institutional policy.28 Taken together, these conditions provide safeguards that may drastically limit the sort of research that can involve adults with decisional incapacity. According to these conditions, people with intellectual disabilities determined to lack decisional capacity cannot participate in research that is above minimal risk with no prospect of benefit, even if it is something that they express interest in pursuing or if it aligns with the research priorities for which they themselves or others with similar conditions have self-advocated, or even if it were the type of activity that a surrogate would approve of on their behalf.Reference Loomes29
A number of critics have argued that these ethical guidelines and the regulations that have been set up on their basis are overly protective, leading to unjust exclusions of IDD individuals from research participation. Specifically, the argument goes, they do not appropriately recognize that members of the IDD community frequently value participation in disability-related research because of the prospect of benefit for the broader disability community, even if there is no prospect of their directly benefitting from the research.30 Moreover, this value may be durable, persisting even in cases where capacity to consent is impaired or lost.31 Even if someone is determined to lack decisional capacity, it can still be wrongfully paternalistic to only authorize research participation according to what would be in their best interest (i.e., considering only the risk-benefit ratio).Reference Howard, Grill and Hanna32 This is because even if people are determined to lack decisional capacity, they still retain agential capacities that could be disrespected if disregarded.Reference Howard, Wendler, Wasserman and Cureton33
However, attention to the value of non-domination also reveals how these same ethical protections, while overly protectionist in some contexts, may also not resolve the danger of domination within research on other dimensions. Admittedly, the safeguards put in place by federal regulations — particularly requiring independent ethical oversight by Institutaional Review Boards (IRBs) and the involvement of surrogate decision-makers known in federal regulations as legally authorized representatives (LARs) — have been effective tools in curbing the dominating power of researchers. Federal requirements for IRB review turned what was sometimes a voluntary ethical consultative process to one in which researchers were required to justify their study design, inclusion criteria, and research risks and benefits for prior approval by an independent ethical oversight committee that is diverse in its makeup and must include at least one member not affiliated with the institution.34 Regulations surrounding surrogate decision-making also include criteria for full information and opportunities for discussion, which curbs researchers’ ability to withhold crucial information about the research in the recruitment process.35
Nonetheless, despite more effective ethical research protections, both minimally risky research and research purporting to hold “direct benefit” can still be conducted under conditions of domination. When respect for persons determined to lack decisional capacity is operationalized purely through either excluding participation altogether or through buttressing the authority of surrogate decision-makers, the research participants may still be unable to escape domination in the research context.
Researchers, parents, and other surrogates may be well-intentioned but still lack insight into or regard for the research priorities and values of the potential participant. Researchers may share surrogate biases, or they may play on surrogate fears, and enroll people who lack decisional capacity in research that, while minimally risky, ultimately goes against the participants’ evaluative perspective. We use the term “evaluative perspective” here to be maximally inclusive of a person’s way of seeing and navigating the world that is stable and distinctive given their embodied experience and particular history. This perspective includes a person’s view of what is good for them, but it also can include other habits of mind and behavior, such as manifest aversions and passions, all of which may go beyond their welfare interests. Many of these features of our evaluative perspective need not be subject to critical appraisal or reflective endorsement, but they play key roles in our deliberation and it would be insulting of our agential capacities for others to disregard them.36
So while current ethical guidance may guard against much of the dominating power of the researchers, it doesn’t resolve the possibility that when recruited to authorize some types of research, the surrogates themselves could be empowered to make decisions arbitrarily that undermine the basic interests of the participants, as we hope to show with the following two cases.
First, minimally risky research can still be dominating. Consider the following example from 2014, of a polarizing rollout for a biorepository project, which aimed to genetically sequence 10,000 samples from Autistic people to be made available for future research through a vetted approval process.Reference Villanueva and Majumder37 Such a research study clearly met ethical standards according to research regulations — it involved no more than minimal risk and surrogate consent. However, Villanueva and Majumber chronicle the controversy surrounding the rollout. The project, which was sponsored by Autism Speaks, in partnership with industry and medical collaborators, was named “MSSNG,” with the two missing ‘I’s intended to convey the missing information about Autism Spectrum Disorder. Notably, at the time of the rollout, Autism Speaks, the nonprofit behind the project, still included the hope for a “cure for Autism” in its organizational mission statement, which was subsequently removed in 2016. On the same day that the MSSNG project was announced, “the hashtag #NotMssng emerged on Twitter.”38 Many of the Twitter users who posted their criticisms of the project with the hashtag #NotMssng, communicated a very different understanding of the project’s name and message. Namely, that “MSSNG” expressed the view that there is something missing or deficient about Autistic people. Critical posts of the project wholeheartedly rejected the idea that autism was something to be cured or that there is anything amiss about being Autistic, e.g.:
“We are here, We are healthy, We are intelligent, We are #NotMssng. Please listen to us for once Autism Speaks instead of hurting us!”
“@autismspeaks Autism has no cure because it is hard-wired in the brain. If you eradicate autism, you eradicate autistic people. #NotMssng”
“I am Autistic and I am #NotMssng! I am right here and I can speak for myself”
Autistic people who are most vocal on social media may not be representative of the larger Autism community, and in particular may not represent the evaluative perspective of Autistic people who are unable to communicate through assistive technology or who have been determined to lack decisional capacity. However, Villanueva and Majumber cite further evidence that in comparison to the general population, a larger proportion of Autistic people, particularly those self-reporting being nonverbal/selective mute or experiencing learning challenges, are more likely to reject the goal of finding a “cure for autism.”39
Imagine an Autistic adult, who is determined to lack decisional capacity, but whose parents, acting as her legally authorized representative, enroll her in the MSSNG project, and she donates a genetic sample. This person has now contributed to a project not only run by an organization professing specific values that she may or may not endorse, but also that creates a database for research activity potentially in service of aims she may find objectionable. In light of known disagreement within the Autism community, if her parents are empowered to enroll her in the project without even needing to consider whether her views are aligned with at least a significant minority of the Autism community, then her participation is established under conditions of domination.
Second, the direct benefit requirement, while overly protectionist on many fronts, also does not wholly guard against the possibility for domination. A compelling example revolves around the outcome measures used in trial design for research on autism, which generally measure reduction of observed autistic traits (such as poor eye contact or hand flapping). This in effect imposes “passing demands” on subjects; contrary to providing benefit, such demands may in fact cause considerable harms.Reference Ne’eman40 For example, current research efforts on pharmacological agents that would modulate the vasopressin system in both children and in adults aim to examine whether use of such agents results in “improved social functioning.”Reference Parker41 Outcomes are assessed using outcome measures (such as the Social Responsiveness Scale, Second Edition) that include repetitive behaviors or avoidance of eye contact; improved social functioning involves observed reduction of such “deficiencies” in social functioning.
However, identifying reduction of such traits as a “direct benefit” of a research study builds a controversial evaluation of benefit and harm into the study design, one which is not responsive to many Autistic individuals’ understanding of what it would be to benefit from an intervention.Reference Ne’eman42 Where legally authorized representatives have standing to enroll an individual in such trials without accountability to the individual’s own perspective on what constitutes genuine impediments to social functioning, they may be enrolling an individual who would not see themselves as benefited by reduction of certain behaviors — again, securing their participation under conditions of domination.
One might object that these examples merely reflect the risks that any individual takes when enrolling in research; the decision to participate in research is always marked by some degree of uncertainty about the interface of the study with one’s values and commitments. However, the classification of research as “minimally risky” or “directly beneficial” is a judgment that comes not from the participant, but from the study team and IRB. What is incorporated into judgments of risks and benefits is rarely comprehensive and may be unresponsive to harms or risks distinctive to the study population.43 As Villanueva and Majumber argue, while risk of bodily harm is low when it comes to donating a blood sample to a biorepository, there are dignitary risks associated with participation: “The violations and harms associated with having one’s genetic material used without one’s explicit consent for research to which one has fundamental moral objections are substantial.”44
Under current regulations, a participant with decisional capacity has the opportunity to evaluate and contest the purported value of a research project and its alignment with the participant’s own judgments of what is important or good. But a participant who lacks decisional capacity is not awarded this protection. In the cases of MSSNG and vasopressin trial enrollment, we do not know whether the enrolled participants determined to lack decisional capacity agree or disagree with the critiques of these projects because there is no requirement for the legally authorized representative and research team to try and find out.45 It appears to operate on a presumption that if a participant lacks capacity to consent to research participation, then they also lack capacity to form judgments about whether the study aims and design aligns with their values — but this presumption is not necessarily true.Reference Jaworska46
Some research particularly studying IDD populations may have higher risks or may not hold prospect of direct benefit for the participants but aligns better with the values and research priorities of members of the IDD community. Some research may be classified as minimally risky or directly beneficial, but engage such individuals in aims whose value they would forcefully reject. How do we fully realize the goal of inclusive and non-paternalistic research practices, but also guard against reintroduction of the potential domination of a vulnerable population outlined in the cases above?
3. The Non-Domination Approach to Informal Supported Decision-Making
One recent proposal for balancing protection and inclusion of people with IDD in the research setting is the introduction of supported decision-making as an alternative to surrogate decision-making in certain research contexts.Reference Wendler and Kim47 Supported decision-making has been implemented in other legal settings outside of research and is defined as process by which individuals (the “principals”) who lack decisional capacity to make decisions independently may be able to make voluntary and fully informed choices with the assistance of others whom they select to help them in the process (the “supporters”).Reference Kohn, Dinerstein and Wright48 Many states have implemented laws to govern the supported decision-making model, dictating that in the supported decision-making relationship, it is the principal and not the supporter that is the decision-maker.Reference Wright49 In this way, formal supported decision-making is a legal tool for achieving decisional and legal capacity. In jurisdictions without laws governing supported decision-making, supported decision-making can still be implemented, but informally — the principal may not be recognized as the decision-maker by law, but is recognized as such by the supporter.
Here, we develop a model of informal supported decision-making to ethically guide and delineate the role of the legally authorized representative (LAR) in the research setting. Rather than being a process designated solely for those individuals who can attain decisional capacity to consent to research with the assistance of a supporter, we think many others can benefit from supported decision-making. We argue that in certain research settings, for individuals who are unable to engage in formal supported decision-making (because the jurisdiction in which they reside does not recognize formal supported decision-making or because their disability ensures they cannot achieve decisional capacity even with support) and thus will still need the involvement of an LAR in the informed consent process for research, informal supported decision-making still has ethical purchase. In such situations, the LAR should see their role as that of a supporter rather than as a surrogate. This means that the prospective participant would be included in the informed consent process according to the norms of supported decision-making even if the process does not result in the prospective participant’s achievement of decisional or legal capacity.50
This section will thus develop how informal supported decision-making can apply to individuals with IDD who lack decisional capacity (even with additional supports) and thus require the involvement of an LAR. Such persons may not legally qualify as appropriate candidates for formal supported decision-making as enumerated in state laws.Reference Weisbord and Horton51 The idea is to use the model of supported decision-making as an ethical guide for a more collaborative process by which LARs and researchers can directly engage such prospective research participants. While this is our focus in this section, we think that a model of supported decision-making guided by the non-domination approach can be applicable more broadly to anyone who needs or wants decisional support.
Previously we have developed and defended a process of supported decision-making guided by the non-domination approach in the clinical setting.Reference McCarthy and Howard52 We argued that, in the clinical setting, the value of non-domination centers on ensuring that the principal’s own perspective on what they need and what is good or important guides the entirety of decision-making. In this paper, we hope to translate this process into the clinical research setting to highlight how it differs from and improves upon current practices related to surrogate decision-making to counteract the possibility of domination in the research setting.
The central objective of our non-domination approach is to treat supported decision-making as a fundamentally collaborative decision-making process between the prospective research participant (the principal), their supporter, and the researchers — a collaboration that is grounded in and justified by the principal’s evaluative perspective. Given the commitment to supported decision-making as collaborative at its base, our non-domination approach does not require the principal and supporter to approximate independent, “unsupported” decision-making. In many clinical situations, patients often seek out and rely on the deliberative support of clinicians, family members, and friends. The process in which IDD patients make these decisions should not be categorically different. Regardless of whether individuals prefer making decisions independently or with the support of trusted others, they should never be subject to the domination of others in their deliberative process. This is true in both the clinical and the research setting.
Given this, in the research setting, the non-domination approach is concerned with precluding the possibility that the informed consent process yields a decision which is insufficiently responsive to the prospective participant’s perspective. The non-domination approach to supported decision-making, then, focuses on articulating the constraints and requirements of the process that are necessary for forging the right kind of relation between the prospective participants’s evaluative perspective and the resulting decision. This requires that time and attention be dedicated to eliciting the potential participant’s actual evaluative perspective. This creates an expectation in the research team that they have an independent responsibility to explore and elicit elements of the potential participant’s perspective, as opposed to simply deferring to the LAR’s interpretation.
On the non-domination approach to informal supported decision-making, the goal is to reach a decision endorsed by the principal, who in this case is a prospective research participant. A person without decisional capacity can still endorse a decision made on their behalf. A decision is endorsed by the principal if it satisfies the following conditions:
-
1. The resulting decision can be publicly justified in terms of the principal’s evaluative perspective;
-
2. The principal has been given opportunity to contest the decision; and
-
3. The principal cannot be interpreted as contesting.
Endorsement concerns the relationship between the resulting decision and the principal’s actually elicited evaluative perspective. But there is another important feature of the non-domination approach to supported decision-making: there must be affirmation that the principal desires the identified supporter to remain in this role. Because the supporter for individuals with IDD frequently is central to interpreting the principal’s actual evaluative perspective for the sake of a decision-making process, we must safeguard against the possibility that the resulting decision tracks an interpretation of the principal’s evaluative perspective by an individual that the principal themselves would not accept as the appropriate individual to serve that interpretive function — that is, as the appropriate supporter. This possibility threatens the principal’s capacity to endorse not only the resulting decision, but also the decision-making process.
Precluding this possibility requires two further conditions:
-
4. There are periodic opportunities throughout the decision-making process for the principal to contest the supporter’s authority to engage in supported decision-making; and
-
5. The principal’s refusal to have a particular individual serve as a supporter does not require justification on the principal’s part.
Taken together, these five conditions are central to establishing supported decision-making processes that ground the resulting decision in the principal’s own evaluative perspective.Reference Pan, Dinerstein and Wendler53 But the non-domination approach allows that interpretation of the principal’s evaluative perspective could be a collaborative and constructive project by the principal and their supporter.
The non-domination approach to supported decision-making has several strengths for the research context. First, the non-domination approach requires that for any participant, their own evaluative perspective be part of the foundation of the resulting decision to participate.54
Second, the non-domination approach emphasizes the importance of publicity within the collaboration. It is not enough that the supporter be able, if called upon, to justify the resulting decision in terms of the principal’s evaluative perspective. Non-domination requires that principals actually have the opportunity to contest and to continue the process of deliberation. Also, when prospective participants are determined to lack capacity and an LAR is involved, third parties play an indispensable role in supported decision-making as safeguards for the principal against the possibility of the LAR making decisions divorced from the principal’s evaluative perspective. In the research setting, third parties, researchers, and IRBs, as well as community advocates, may play a key role in ensuring that the LAR is indeed acting as a supporter for the prospective participant in making decisions that grow out of a potential participant’s own distinctive evaluative perspective.55
Third, a non-domination approach to supported decision-making requires that the potential participant be given periodic opportunity to affirm that the supporter is the right person to entrust in the role of supportive decision-making. Such periodic opportunities are important both for individuals with IDD who have decisional capacity but choose to engage with a supporter in the decision-making process and those who have been determined to lack capacity and must rely on an LAR to authorize their research participation. In the research setting, even if the potential participant may not be found to have decisional capacity for consenting to research, their capacity to trust others to support their decision-making should still be respected and supported.
Finally, at the heart of the non-domination approach is a focus on the role of contestation in supported decision-making. Contestation is important on three levels. First, the act of contestation itself (regardless of whether or not it is backed up with justification) is evidence that the choice does not conform to a principal’s distinctive evaluative perspective. Second, it can undermine a person’s welfare when others make decisions that a person explicitly contests; that is, there are psychic costs to realizing that one’s refusals are being dismissed and disregarded. When it comes to forced research participation, these psychic costs compound on other harms, including harms to one’s bodily integrity and additional physical harm and discomfort caused either by the research intervention itself or resistance to the intervention. These psychic and physical costs persist even if the dismissals are justified paternalistically on grounds of what is best for the potential participant. Third, the capacity to contest is a constitutive feature of one’s agential capacities and should be seen as separate from one’s capacity to provide informed consent. It is, after all, the principal and not the supporters who will intimately experience the consequences of the decision, and so they have a unique and irreducible right to refuse some choice.Reference Wright56 Even if a person’s agential capacities fall below what is taken to be one of the thresholds required for being able to make one’s own decisions in some domain, it is possible for their agential capacities to be insulted and disrespected. And this insult occurs regardless of whether or not the person realizes that their contestations have been disregarded.57
The emphasis on contestation is particularly compelling in the research context, as the relevant decisions for potential participants and supporters are binary in nature — to enroll or not to enroll; to withdraw or to continue. This is fundamentally different from the clinical context, in which the process of medical decision-making frequently involves constructing a set of potential pathways in response to the patient’s clinical condition and their evaluative perspective. Because the decision-making space in consent to research is so focused, the interpretive project of the LAR (acting in their supporting role) is equally focused; the prospects for unaccountability to the participant’s evaluative perspective in the supporter’s work is more constrained.
The non-domination approach to supported decision-making is additionally valuable in the research context because it promotes the goals of respect for persons and protection of individuals who are members of vulnerable populations. Under current regulations, the role of the LAR comes into play once a specific risk-benefit assessment has been confirmed. Studies must be classified either as minimally risky or as having prospect of direct benefit in order to enroll IDD individuals. These are necessary general determinations, the backdrop against which the consent process occurs. Regulatory bodies have little to say, however, about the process for determining whether the individual participant would see the study as being minimally risky or directly beneficial. The non-domination approach to supported decision-making targets precisely this gap in guidance.
4. Is This Just Substituted Judgment by Another Name?
An important challenge to the non-domination approach we sketched out in the previous section is whether it articulates an account of actual supported decision-making or is just surrogate decision-making and substituted judgment by another name. Specifically, this approach may seem to require very little active engagement from the potential participant who lacks decisional capacity. If an LAR develops an account of the prospective participants’s evaluative perspective that stands up to scrutiny, then as long as the prospective participant does not take up the provided opportunity to contest the LAR’s work, a decision could go forward. Thus it can be suggested that the non-domination approach only secures a requirement of participant assent or nondissent to an LAR’s substituted judgment.
While we acknowledge that the non-domination approach does not secure maximal independent engagement from the prospective participant, we argue that there are two essential differences between our vision of informal supported decision-making and a model of “Substituted Judgment + Assent”, and that considerations of non-domination secure the collaborative approach to supported decision-making (see figure 1).
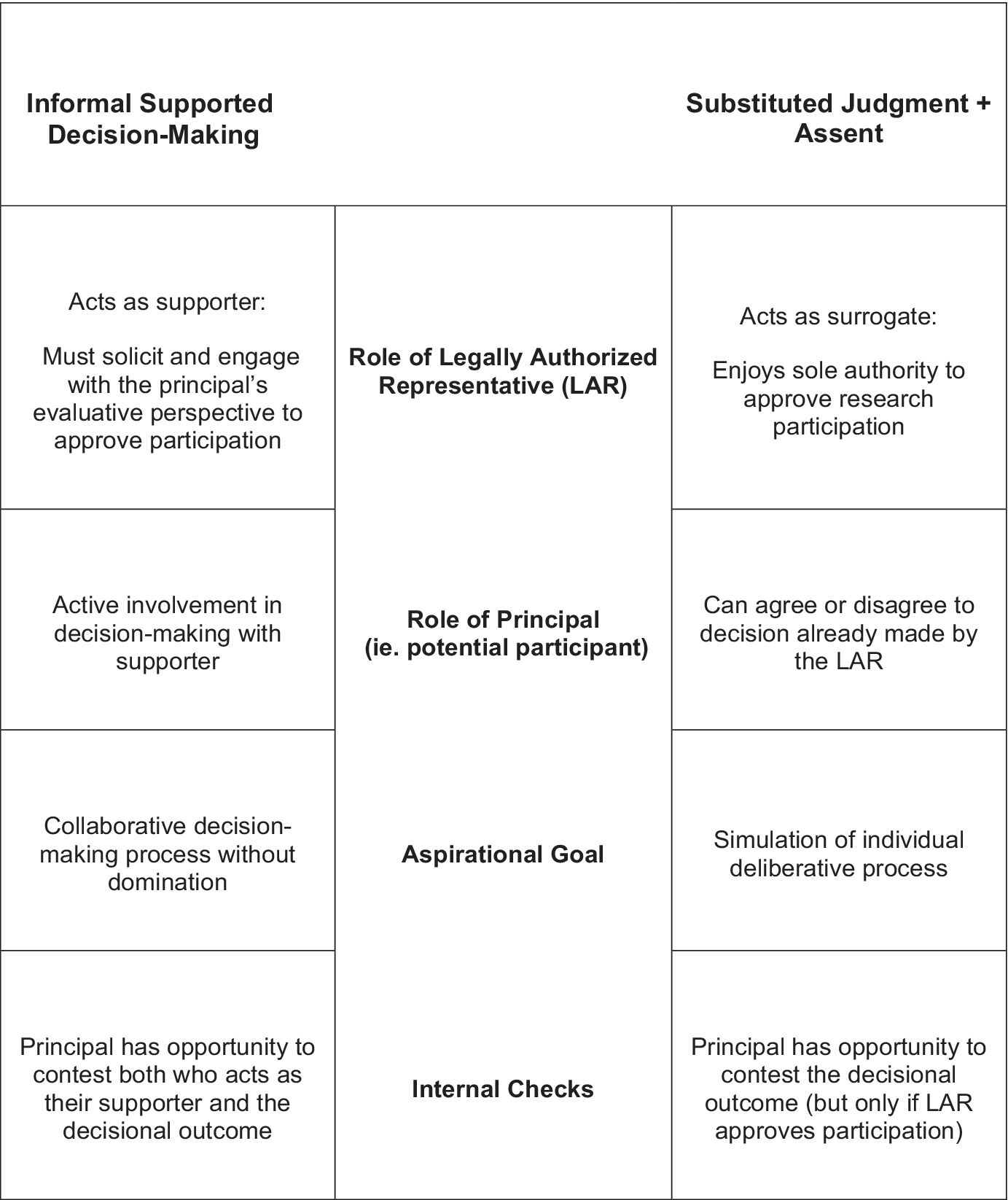
Table contrasting the core features of informal supported decision-making with the core features of substituted judgment with assent.

Figure 1. Long description
From top to bottom, the table has four horizontal sections. The first row compares the role of the legally authorized representative. Informal supported decision-making: acts as supporter, must solicit and engage with the principal’s evaluative perspective to approve participation. Substituted judgment plus assent: acts as surrogate, enjoys sole authority to approve research participation. The second row compares the role of the principal. Informal: active involvement in decision-making with supporter. Substituted: can agree or disagree to decision already made by the L A R. The third row compares aspirational goals. Informal: collaborative decision-making process without domination. Substituted: simulation of individual deliberative process. The fourth row compares internal checks. Informal: principal has opportunity to contest both who acts as their supporter and the decisional outcome. Substituted: principal has opportunity to contest the decisional outcome but only if L A R approves participation.
In informal supported decision-making for individuals with IDD who lack decisional capacity, the prospective participant is an indispensable part of the deliberative process itself. In their role as the principal, it is their evaluative perspective that is actively solicited and is part of the starting point for deliberation; it alone is capable of ruling out an otherwise permissible course of action. This authority derives from the demands of respect for the principal’s agential capacities. Consequently, appropriate recognition of the principal’s standing in decision-making requires starting with them, eliciting from them an understanding of their evaluative perspective to the greatest extent possible.58 In contrast, substituted judgment supposes that the LAR has primary responsibility, and so authority, to articulate the prospective participant’s evaluative perspective. While it would be good if LARs engaged with the potential participants in their decision-making, there is no requirement in a substituted judgment approach for surrogate deliberation to be anchored in direct engagement with the participant.
The role of the prospective participant’s contestation in terms of our attitude towards the participant’s evaluative perspective also differs. Substituted judgment presumes that the participant’s evaluative perspective is knowable and articulable, independent of what has been directly elicited from the participant. On substituted judgment + Assent, contestation by the participant could be treated as erroneous, as a failure to endorse a decision that appropriately aligns with the participant’s evaluative perspective.
By contrast, the non-domination approach to supported decision-making does not cleave contestation from the articulation of the evaluative perspective. An evaluative perspective is rarely a perfectly coherent set with which a decision could align. Rather, decisions are often a point at which internal conflicts or contradictions within one’s own evaluative perspective emerge, and the decision-making process is the resolution of such conflicts by way of reaching a decision.59 Resolution of internal conflicts within one’s evaluative perspective in the context of a decision is an agential capacity necessary for independent decision-making, and it demands respect even if the individual is not fully capable of unsupported decision-making. Contestation should not, on the non-domination approach, be seen as the participant’s failure to grasp their own evaluative perspective. This isn’t to say that misunderstandings, confusion, and errors in reasoning never occur. But the non-domination approach to supported decision-making tells us that the only way we can discern whether we are in a state of error is by revisiting the work of eliciting the participant’s evaluative perspective. Presuming error is not justifiable, because it is the participant’s evaluative perspective at the center of supported devision-making.
Moreover, in supported decision-making, the prospective participant’s authority around contestation extends not only to the decision itself, but to the supporter’s authority. Specifically, the participant has authority to contest their own continued representation by the current LAR (as their supporter). Moreover, removal of a supporter does not require justification by the principal. This creates an asymmetry in the shared authority between the potential participant and their supporters in supported decision-making. The supporter is held publicly accountable to justify the decisional outcome on terms that are grounded in the evaluative perspective of the principal — not merely in their welfare interests. The principal, on the other hand, needn’t offer up any justification in order to legitimately contest a particular decision outcome or refuse to have a particular person play the role of their supporter. In contrast, substituted judgment, at least for many people with IDD, does not recognize the potential participant’s standing to contest the authority of the LAR; rather, any removal of the LAR would have to be the product of clear legal justification.
To illustrate these differences, let us revisit the MSSNG case. A parent reads about the MSSNG initiative. This parent knows their adult child values engaging in community initiatives to improve quality of life for Autistic individuals. They conclude that enrollment in this minimally risky research project would align with their child’s evaluative perspective, fully unaware of the nuanced concerns raised by the broader Autistic community. They engage the research team about potential participation. The potential participant’s capacity to consent to research is evaluated and they are deemed to lack capacity; their parent is identified by the team as the LAR. After undertaking the informed consent process, the LAR decides that the risks of the trial are wholly tolerable for the purported benefit of making a meaningful contribution to disability-related research, and they agree to enroll their child in the trial. Their child does not contest this enrollment.
A substituted judgment approach would empower an LAR to consider only the risks and benefits presented in the consent process by the research team, unknowingly disregarding the broader critiques of the potential research applications in this specific case within the Autistic community. Because there is no requirement that deliberation and disclosure be undertaken with the incapacitated subject, the opportunity for key information that could be the site of contestation does not rise to the attention of the participant. Often the requirement of assent is incorporated into the substituted judgment model, where the potential participant may be given the opportunity to agree to the decision that the LAR has made on their behalf.60 But importantly, this takes place only after the surrogate has agreed to authorize participation. Moreover, the adult child has no opportunity to contest their parent’s identification as the LAR, even if there are individuals within their community who they would trust to ask questions or recognize red flags that their parent may not.
By contrast, the supported decision-making approach requires the research team to begin their consent process with the potential participant themselves. Every process of supported decision-making should begin from an assumption that the participant has an insight that they can provide about research involvement. Key information would be disclosed directly to the potential participant that may elicit reactions prompting further inquiry by the team and LAR as to whether this project really aligned with the participant’s perspective. Moreover, the expectation would be that the team would afford the participant initial and subsequent opportunities to affirm that their parent was the correct LAR. If the participant would prefer a different individual, this would be elicited before the consent process even began. Moreover, as more information is disclosed and the participant has the opportunity to observe their parent’s response to and interpretation of germane information, the non-domination approach affords the participant the opportunity to contest the continued appointment of their parent as LAR.
Finally, on the non-domination approach, opportunities for contestation may be implemented beyond the decision point of whether or not to participate in the trial. When it comes to studies, such as the MSSNG biorepository, where “identity-based concerns” arise among a large swath of the affected community regarding the overarching value and aims of the research, safeguards can be be put in place to allow donors to withdraw their sample in the future.61 This would not be a requirement for all biorepository research involving participants who lack decisional capacity, just the studies where there is already evidence of polarization within the affected community.
On our interpretation, giving participants the power to contest who acts as their LAR and guiding LARs to act as supporters rather than surrogates in the research context would not go against any of the current requirements of the Common Rule, which are largely silent on the selection process of the LAR and on the norms that should guide the LAR’s decision-making process.62 However, federal guidance states that the LAR selection process and the informed consent process more generally should conform to the “laws of the jurisdiction in which the research is conducted (e.g., local or state law).”63 In some instances, if the participant contested the appointment of the identified LAR, there may not be another individual that state law would allow to consent on the participant’s behalf, which means that this contestation of the LAR would preclude research participation.
For those jurisdictions where there are currently no laws governing supported decision-making, we think our approach can be incorporated into ethical guidance for those charged with making decisions on behalf of others. Even in juridictions with laws that recognize formal supported decision-making processes, our recommendations can have ethical purchase. Our approach should not supplant the decision-making authority of any person with IDD who is already legally recognized as the decision-maker through a formal supported decision-making process. Rather, the approach we have sketched can give guidance to how to informally support others in these jurisdictions who do not qualify for supported decision-making. Insofar as our recommendations conflict with current state and local laws regarding supported decision-making or human subjects protection, laws should be implemented to empower participants to be directly involved in the decisions made on their behalf.
We acknowledge that non-domination may not guarantee active participation in a form that renders the supported decision-making process to look like a simulation of independent decision-making. However, this is only a problem insofar as one thinks that independent decision-making is morally preferable to shared decision-making. Given that we envision supported decision-making as a fundamentally collaborative endeavor, one complementary with the ideal of shared decision-making for individuals without intellectual or developmental disabilities making serious medical decisions, the failure of non-domination to secure a process that looks like independent decision-making does not cause as much concern.
Central to the non-domination approach, however, is a recognition that securing the ability for individuals with IDD to make decisions to participate in research goes beyond optimization of supported decision-making at the time of consent. The emphasis on contestation shows that there must be structural checks in research design and planning to ensure periodic opportunities for contestation. An Autistic adult who is enrolled in a vasopressin trial and who then learns about the contents of the outcome measures tracking their progress should be empowered to extricate themselves from continued participation if leaving the study is consistent with their preferences based on what they have learned.
We recognize that supported decision-making in the research context does not guard against all the ways in which people with IDD may be dominated in their lives. For instance, the process just sketched for supported decision-making doesn’t address the ways in which adult children with decisional incapacity may find it difficult to contest their parents as the appropriate decision-making supporters, nor does it guarantee that potential participants will have the information or supports available to go against the decisions that a loved one endorses. The non-domination approach encourages us, therefore, to see supported decision-making as just one tool among many to protect and empower IDD persons as research participants.
Disclosures
Dana Howard received NIH support for attending a supported decision-making workshop.

 Open access
Open access