


The World Health Organization (WHO) defines burnout as an occupational syndrome resulting from the chronic accumulation of work-related stress that is inadequately managed, characterised by diminished energy levels, negativism and reduced professional efficacy. 1 Burnout and psychological distress have both become increasingly prevalent across all stages of the UK medical workforce, beginning in medical school and persisting through postgraduate training to consultancy. Reference Gemine, Davies, Tarrant, Davies, James and Lewis2,Reference Garcia, Abreu, Ramos, Castro, Smiderle and Santos3 The COVID-19 pandemic served as a significant inflexion point, exacerbating pressures such as excessive workloads, disrupted training pathways and inadequate pastoral support. Reference Gemine, Davies, Tarrant, Davies, James and Lewis2,Reference Ghahramani, Lankarani, Yousefi, Heydari, Shahabi and Azmand4,Reference Agata, Grzegorz, Ilona, Violetta and Katarzyna5 Post-pandemic disruptions and frustration among the medical workforce have exacerbated unresolved stress that may have contributed to industrial action, increased attrition and the potential migration of early-career doctors abroad. Reference Khan6–Reference Cook, Tandanu, Rehman, Whiteman, Osunronbi and Mukhtar8 Although much of the existing literature focuses on burnout and well-being among resident doctors, medical students are also experiencing increasing psychological strain early in their careers, driven by financial pressures, academic demands and poor work–life balance. Reference Bhugra, Molodynski and Ventriglio9–Reference Rehman, Sarwar, Kungwengwe, Choudhury, Whiteman and Brennan11
Resident doctors and medical students face distinct challenges that may increase their susceptibility to burnout. For doctors, prolonged training and balancing clinical, academic and professional demands contribute to stress and burnout. Medical students, meanwhile, experience stress linked to examinations, financial pressures, relocation and identity development. Reference Cotobal Rodeles, Martín Sánchez and Martínez-Sellés12 A clearer understanding of burnout among resident doctors and medical students, along with the interrelated factors, is essential for developing accurate screening and support tools. Reference Maslach and Leiter13,Reference Rotenstein, Torre, Ramos, Rosales, Guille, Sen and Mata14
This study aimed to evaluate self-reported burnout and related stressors among UK resident doctors and medical students, identify associated risk and protective factors, and estimate the economic impact of resident burnout-related absenteeism.
Method
Study design
The questionnaires were developed based on a systematic literature review, electronic interviews with residents and students, and a Delphi review process (see Supplementary Methods, Supplementary Tables 1–4).
Setting
Data collection was carried out between February and April 2025, using a decentralised recruitment strategy via the UK Plastic Research Collaborative network. Regional leads from UK foundation schools, local deaneries and medical schools distributed the questionnaire using institutional mailing lists, digital learning environments, societies and social media platforms. All participants were required to read the information sheet and provide informed consent for the data used in the research before proceeding.
Participants
This national cross-sectional study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Reference Vandenbroucke, von Elm, Altman, Gøtzsche, Mulrow and Pocock15 Eligible participants included all postgraduate doctors in training across all 18 UK foundation schools and medical students aged 18 years or older enrolled at UK medical schools listed by the Medical Schools Council at the beginning of the 2024 to 2025 academic year. 16,17 Doctors in specialty training beyond consultant level, and individuals previously withdrawn from medical education or training, were excluded.
Variables
Predictor domains included demographic factors (gender and age group), workplace and training characteristics (training stage, region, and specialty or career interest), lifestyle behaviours (perceived recovery, diet quality, physical activity and substance use), relational support (time and frequency spent with family or close contacts) and attitudinal factors (willingness to recommend medicine as a career and intention to leave the profession). Mental health and direct burnout measures were excluded from predictor models to avoid collinearity with outcome variables and latent class membership.
Data measurement
The primary objective of this study was to assess self-reported burnout rates among respondents, measured as a binary outcome. Secondary objectives included identifying risk and protective factors for burnout, evaluating self-reported intentions to leave medicine, assessing satisfaction with work–life balance and evaluating the perceived impact of geographical relocation and financial stress on well-being. As well as determining the economic cost of burnout among resident doctors through absenteeism.
Definitions
Composite indices were developed to quantify key lifestyle and well-being domains. Perceived recovery (recovery index) was derived from average sleep duration and fatigue frequency: sleep duration was scored on a five-point scale (1 = ≤3 h, 5 = ≥8 h) and fatigue frequency was scored on a five-point scale (1 = never, 5 = always), then reverse-coded so that less frequent fatigue contributed positively (reverse-coded fatigue = 6 − fatigue score). The recovery index was calculated as sleep score plus reverse-coded fatigue score, producing a total score ranging from 2 to 10, with higher scores indicating better perceived recovery (longer sleep and less frequent fatigue). For analysis, recovery scores were grouped into low (≤5), moderate (6–7) and high (≥8) categories. Diet quality integrated fruit and vegetable intake with reverse-coded consumption of sugary foods and ultra-processed foods; physical activity merged exercise frequency with daily step count; and substance use captured any reported nicotine use or elevated alcohol consumption. These constructs were selected based on evidence linking lifestyle behaviours to burnout among healthcare workers. Reference Lin, Woolery-Lloyd, Young and Kenya18,Reference Hall, Johnson, Watt, Tsipa, O’Connor and Harris19
Ethical approval
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. 20 The study received ethical approval from the Research Ethics Office of King’s College London for the Resident Doctors questionnaire (MRSU-24/25-46643) and the Medical Students questionnaire (MRSU-24/25-47084).
Statistical methods
Statistical analyses were conducted using Stata version 19 (StataCorp, Texas, USA; www.stata.com). Descriptive statistics were reported as frequencies and percentages for categorical variables and as medians with interquartile ranges for ordinal variables. Group comparisons were assessed using the Wilcoxon rank-sum test. Logistic regression was used for binary outcomes, multinomial regression for nominal outcomes and ordinal regression for ordered outcomes. Composite indices for perceived recovery, diet quality and physical activity were constructed by aggregating relevant questionnaire items. Internal consistency and dimensionality of these indices were evaluated using Spearman correlations, Cronbach’s alpha and, where appropriate, principal component analysis. Resulting indices were categorised into low, moderate or high groups based on empirical thresholds or tertile splits.
Human capital approach
The economic burden of burnout among resident doctors in the UK was estimated using a human capital approach, valuing productivity losses attributable to absenteeism. The analysis was conducted under the assumption that approximately 75 000 resident doctors (including foundation, core and specialty trainees) are currently employed within the National Health Service (NHS). 21
Productivity losses were modelled based on sickness absence associated with stress-related disorders, for which national data indicate an average of 21.1 working days lost per affected worker per year. 22 Salary data were drawn from the NHS ‘nodal pay points’ for the financial year 2024/25. After averaging across training grades, the representative annual salary was £57 215, corresponding to a daily wage of £227.04, assuming 252 working days per year. 23 Per-person productivity losses were calculated by multiplying the daily wage by the number of days lost owing to burnout-related absence, yielding an estimated loss of £4790.544 per affected resident. Aggregate costs were obtained by multiplying this figure by the estimated number of resident doctors affected at prevalence scenarios ranging from 10 to 80%.
The analysis was undertaken from a human capital perspective, assuming that each day of absence corresponds to a full day of lost output. No adjustment was made for the potential mitigating effects of staff redeployment or substitution through locum coverage; as such, the estimates presented are likely to represent an upper bound of the economic burden. To contextualise the magnitude of these costs, we expressed the total productivity losses as a share of national economic output. The proportion of UK gross domestic product (GDP) lost was calculated by dividing the estimated aggregate productivity costs by total UK GDP in 2024 (£2.56 trillion) and multiplying by 100. GDP estimates were obtained from the UK Office for National Statistics. 24
Results
Main findings
A total of 2793 responses were received, including 1439 (51.5%) from resident doctors and 1354 (48.5%) from medical students. Overall, 70% (n = 1008) of resident doctors and 65.7% (n = 889) of medical students reported experiencing burnout during their training. After adjustment for non-responder bias (Supplementary Results, Supplementary Tables 5 and 6) in age and gender, the prevalence of burnout among resident doctors and medical students increased to 77.9–78.9% and 78.6–78.7%, respectively. Despite the high prevalence of burnout, 56.8% (n = 573) of resident doctors and 79.3% (n = 705) of medical students were unaware of the support services available to manage burnout (Supplementary Tables 7–10). Overall, 30.7% (n = 442) of resident doctors and 13.7% (n = 186) of medical students reported an intention to leave medicine within the next 5 years (Supplementary Tables 11 and 12).
To further explore potential contributing factors to reporting burnout among UK resident doctors and medical students, a multivariate analysis was conducted to examine the influence of age, gender, region and various lifestyle factors. The analysis identified several key demographic and lifestyle factors associated with self-reported burnout. Female resident doctors and medical students demonstrated a higher likelihood of reporting burnout (residents: odds ratio 1.53, 95% CI 1.08–2.17, P = 0.017; students: odds ratio 2.10, 95% CI 1.42–3.11, P < 0.001). No statistically significant associations were identified between burnout and the training stages in both cohorts, but resident doctors working in a medical specialty reported higher rates of burnout (odds ratio 3.04, 95% CI 1.64–5.65, P < 0.001).
Several lifestyle factors showed associations with self-reported burnout. Lack of time with family was a significant risk factor for burnout reporting among both resident doctors (odds ratio 1.97, 95% CI 1.39–2.79, P < 0.001) and medical students (odds ratio 2.14, 95% CI 1.48–3.10, P < 0.001). However, a high recovery index was protective among resident doctors (odds ratio 0.17, 95% CI 0.05–0.50, P = 0.001). Similarly, maintaining a high-quality diet (odds ratio 0.58, 95% CI 0.41–0.83, P = 0.003) was a protective factor among students.
Resident doctors’ and medical students’ satisfaction with work–life balance was assessed. In total, 37.6 % (n = 541) of resident doctors and 20.6% (n = 280) of medical students were not satisfied with their current work–life balance. Residents in academic pathways (odds ratio 1.72, 95% CI 1.28–2.31, P < 0.001) reported better work–life balance compared with others. Lifestyle factors were strongly associated with better work–life balance among resident doctors, including high recovery (odds ratio 9.56, 95% CI 6.33–14.44, P < 0.001), high physical activity (odds ratio 2.04, 95% CI 1.73–2.40, P < 0.001) and high-quality diet (odds ratio 1.21, 95% CI 1.02–1.44, P = 0.033). Among medical students, high physical activity (odds ratio 2.61, 95% CI 2.12–3.20, P < 0.001), high-quality nutrition (odds ratio 1.59, 95% CI 1.36–1.85, P < 0.001) and high recovery (odds ratio 3.95, 95% CI 3.01–5.19, P < 0.001) were similarly protective (Supplementary Tables 13 and 14).
Relocation stress was then analysed, with 85.1% (n = 1224) of resident doctors and 62.6% (n = 849) of medical students reporting relocation-related stress. Resident doctors working in acute care (odds ratio 2.75, 95% CI 1.50–5.03, P = 0.001) and surgery (odds ratio 2.13, 95% CI 1.44–3.13, P < 0.001) were more likely to report that relocation adversely affected them. Observation of regional differences identified that medical students based in Wales (odds ratio 1.43, 95% CI 1.29–1.58, P < 0.001) and South-West England (odds ratio 1.66, 95% CI 1.49–1.85, P < 0.001) were more likely to experience relocation stress (Supplementary Tables 15 and 16).
Financial stress was also highly prevalent, with 53.9% (n = 775) of resident doctors and 57.8% (n = 784) of medical students reporting financial stress. Female residents had higher odds of experiencing financial stress (odds ratio 1.29, 95% CI 1.06–1.58, P = 0.012). Several specialties were associated with increased financial strain, including surgery (odds ratio 2.02, 95% CI 1.43–2.85, P < 0.001) and primary care (odds ratio 2.11, 95% CI 1.37–3.24, P = 0.001). Regional variation was significant, with residents in Scotland (odds ratio 0.24, 95% CI 0.14–0.41, P < 0.001) being significantly less likely to report financial stress (Supplementary Tables 17 and 18).
Economic implications
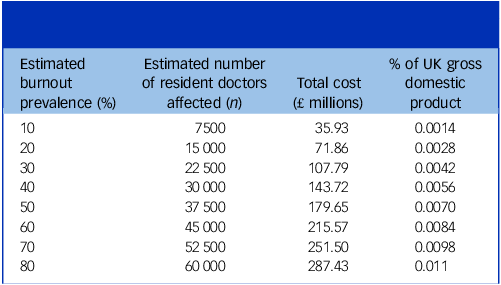
Using a human capital approach, the annual cost of individual-level absenteeism due to burnout among UK resident doctors is estimated at £4790.54. At the prevalence of burnout observed in our study (70% of 75 000 resident doctors), this translates into an annual economic loss of approximately £251.5 million through absenteeism, equivalent to 0.0098% of UK GDP, as shown in Table 1. Depending on the assumed prevalence, the total cost ranges from £35.93 million to £287.43 million (0.0014–0.011% of UK GDP).
Estimated economic impact of burnout among resident doctors in the UK

Discussion
Key results
This study identified a high prevalence of self-reported burnout among UK resident doctors and medical students, with more than half of respondents in both groups affected. The associated economic burden is substantial, with burnout-related absenteeism estimated to cost up to £287.43 million annually. These findings are concerning, as they suggest that psychological strain may emerge early in medical training. Reference Prendergast, Cardoso Pinto, Harvey and Muir25 Both residents and students reported considerable financial pressures, relocation difficulties and challenges maintaining work–life balance, all of which likely compound overall psychological distress. Similar trends have been observed across the European Union, where the WHO Mental Health Survey reported high levels of psychological distress among healthcare professionals, exacerbated by adverse working conditions and occupational stress that undermine mental health and well-being. 26 Collectively, these findings indicate that burnout in this population may reflect the cumulative impact of multiple psychosocial stressors rather than a single, isolated phenomenon.
Generalisability
Resident doctors and medical students face distinct stressors that heighten their vulnerability to burnout, including demanding clinical workloads, academic pressures and financial strain. The high prevalence observed in this cohort is likely multifactorial, reflecting the interplay between clinical demands and wider psychosocial and economic factors. These findings reinforce that burnout is a complex, context-dependent phenomenon shaped by individual circumstances and multiple stressors rather than a discrete construct.
Burnout prevalence in our cohort was markedly higher than recent USA estimates from the American Medical Association (34.5% in residents) (Supplemental Reference 1), suggesting important cross-national differences in training environments, training length and systemic pressures that may drive burnout. The current UK resident recruitment climate may further amplify existing stressors, contributing to the higher potential burnout observed compared with countries such as the USA. Heightened competition for postgraduate training intensifies these pressures, compelling early-career doctors and medical students to pursue research, audits and leadership roles during limited personal time to enhance their applications. 27 Competition in postgraduate training may shape burnout trajectories between students and residents. Medical students may experience early anticipatory stress when striving to remain competitive, potentially sacrificing self-care, which can carry forward or worsen in foundation training, as additional clinical, academic and financial pressures emerge. Reference Lin, Woolery-Lloyd, Young and Kenya18,Reference Hall, Johnson, Watt, Tsipa, O’Connor and Harris19 Residents face sustained clinical demands, speciality examinations, lengthy training pathways and uncertainty around securing subsequent training posts, all of which, combined with financial responsibilities, further compound stress and may carry over into higher specialty training.
Higher burnout among residents in medical specialties may reflect heavy service demands and perceived deficiencies in training and support. The Royal College of Physicians 2025 survey found low satisfaction with medical training and widespread perceptions of unfair recruitment and excessive service provision in medicine (Supplemental Reference 2). These factors likely contribute to burnout through emotional exhaustion and reduced professional fulfilment, highlighting the need for targeted specialty-level training and workforce reforms. This culture of competitiveness coupled with inadequate training may compromise mental and physical health, reduce opportunities for rest and recovery, and may contribute to burnout. Financial pressures from attending courses and conferences, as well as from obtaining additional qualifications, can strain personal finances and disrupt work–life balance. Reference Jerjes and Majeed28,Reference Stroman, Weil, Butler and McDonald29 Burnout in this context may therefore represent the cumulative impact of multiple stressors extending beyond the workplace. Importantly, previous research has linked burnout to a heightened intention among clinicians to leave the profession. Reference Ligibel, Goularte, Berliner, Bird, Brazeau and Rowe30
Collectively, these overlapping influences underscore the need to interpret burnout within a broader framework of well-being, recognising that self-reported symptoms may arise from interconnected academic, relocation, financial and lifestyle-related pressures. Lifestyle factors such as regular physical activity, adequate sleep and balanced nutrition were associated with lower burnout and improved work–life balance, consistent with existing evidence on the protective role of health-promoting behaviours. Although lifestyle factors such as exercise, sleep and nutrition are often bidirectional as these factors can both contribute to, but also result from, burnout. Reference Cecil, McHale, Hart and Laidlaw31,Reference Taylor, Scott and Owen32 Accommodating these behaviours during medical training, alongside institutional initiatives providing targeted financial, psychological and social support, may help prevent burnout, support those already affected and improve retention. Recognising burnout as a dynamic process rather than a fixed outcome highlights the importance of comprehensive, system-level strategies to support the well-being of resident doctors and medical students. Reference Madigan and Curran33
Interpretation
Our findings highlight that many resident doctors and medical students, particularly those experiencing burnout, were unaware of existing well-being support services. This finding highlights a potential communication and accessibility gap between institutions and individuals, suggesting that visibility of resources is equally important as their availability. Increasing awareness and accessibility of these services is therefore essential to ensure that at-risk individuals can seek timely support before burnout progresses to more severe psychological distress. One proposed solution, developed through an iterative co-design process by a multidisciplinary team comprising psychiatrists, general practitioners, surgical specialists, medical students and resident doctors, is a ‘stepped-support’ and ‘traffic light’ framework that provides evidence-based guidance on preventing burnout and links burnout severity to appropriate levels of support for resident doctors and medical students, as shown in Figs 1 and 2 below, respectively (Supplementary Methods). Starting from self-guided resources and escalating to professional counselling or crisis services, these posters could be standardised nationally or adapted locally before being incorporated into local hospitals’ or universities’ well-being initiatives and inductions. Their effectiveness could be validated through local and national quality improvement programmes, using pre- and post-implementation measures of awareness, help-seeking confidence, service utilisation/referrals and burnout scores to assess impact and inform iterative refinement. Efforts to increase awareness are undoubtedly laudable, although they may prove to be futile unless similar efforts are made to dismantle barriers and reject mental health-related stigma within medical school and residency. Without such active cultural change, resident doctors and medical students living with burnout are at risk of suffering in silence despite the availability of effective interventions.
Illustrative poster incorporating a ‘traffic light’ framework that provides evidence-based key burnout support services available to UK resident doctors. RCPCH, Royal College of Paediatrics and Child Health; RCR, Royal College of Radiologists; RCPath, Royal College of Pathologists; RCS, Royal College of Surgeons; RCEM, Royal College of Emergency Medicine; RCOG, Royal College of Obstetricians and Gynaecologists; RCP, Royal College of Physicians; RCOphth, Royal College of Ophthalmologists; RCPsych, Royal College of Psychiatrists; RCoA, Royal College of Anaesthetists; A&E, Accident and Emergency Department; BMA, British Medical Association.

Illustrative poster incorporating a ‘stepped-support’ framework that provides evidence-based self-care advice and key burnout support services available to UK medical students.

A focused approach to identifying the key stressors affecting resident doctors and medical students is essential to guide targeted and effective interventions. Financial strain remains a major concern, heightened by rising living costs and ongoing industrial action over pay erosion and workforce pressures. 34 Recent announcements of further strikes by the British Medical Association underscore the persistent financial and occupational uncertainty that contributes to psychological distress among doctors and students. 35 Interestingly, the lower financial stress reported by Scottish residents may relate to the recent pay discussions and improved industrial relations with the Scottish Government (Supplemental Reference 3). Recent pay restoration in Scotland and reduced strike action may have mitigated financial stress among residents, whereas ongoing disputes in England, with associated salary sacrifice, may exacerbate financial strain. These findings suggest that constructive workforce negotiations and pay stability may have measurable effects on trainee well-being. Supervisors and educators should remain aware of these non-clinical external pressures and offer appropriate guidance and support, and should be aware of local services that can help support residents and students (Figs 1 and 2). Furthermore, the progressive loss of autonomy throughout medical training, including limited control over training location and career trajectory, potentially increases vulnerability to burnout. Reference Cook, Tandanu, Rehman, Whiteman, Osunronbi and Mukhtar8,27,36 Frequent relocations and geographical instability can disrupt social networks and erode a sense of security, contributing to burnout and related stress. These risks should be recognised early in training, with mechanisms in place to identify individuals requiring additional support and to provide timely interventions during rotations.
At a policy level, early identification and support for resident doctors and medical students experiencing burnout aligns with the NHS Long-Term Workforce Plan’s emphasis on sustaining a healthy, resilient workforce. 37 Addressing burnout early in medical education represents an opportunity to improve retention and performance, reduce psychological morbidity, and mitigate future attrition within the NHS. The considerable economic implications of burnout among resident doctors should not be overlooked. In our analysis, burnout among resident doctors was estimated to cost the UK £251 million annually through absenteeism. Even when applying the lower prevalence rates reported by the General Medical Council’s workforce survey, and without accounting for absenteeism among the wider healthcare workforce, the estimated annual cost remains £215 million. 21 This cost falls within the broader context of work-related stress in the UK, estimated at £28 billion each year. Safeguarding the NHS workforce’s well-being, therefore, represents not only a professional responsibility, but also an economic imperative. Investing in staff well-being has been shown to generate significant returns, with each pound spent on mental health producing an estimated 4.7-fold increase in productivity. 38 In the current NHS climate, these potential gains represent an important opportunity to strengthen both staff well-being and patient care. Furthermore, these findings highlight the need to review training standards, particularly in high-burnout specialties such as medicine, and for Royal Colleges to implement targeted strategies to improve training quality and recruitment. In parallel, constructive engagement between resident doctors and government is required to address financial pressures that may otherwise compound burnout and threaten workforce retention.
From a practicality point of view, low-cost awareness interventions such as the stepped-support framework are highly feasible and scalable, whereas higher-impact reforms addressing workload, training quality, and financial pressures require coordinated policy action and sustained engagement from educators, Royal Colleges, NHS management and government. However, implementation may be constrained by entrenched cultural barriers within medical training, including stigma surrounding mental health and reluctance to seek support, highlighting the need for parallel cultural and structural change.
Strengths and limitations
The questionnaire was rigorously developed, informed by a systematic literature review, consultation with medical students and a Delphi cycle. This methodological approach aimed to ensure content validity and contextual relevance for the UK resident doctor and medical student population. Furthermore, the large sample size provided sufficient power to detect meaningful associations in understanding the complex determinants of burnout, including demographic, geographical and lifestyle factors. Several limitations should be noted. The sample size, although significant, does not fully represent all resident doctors or medical students in the respective region, and should be interpreted with caution. The use of self-reported data introduces potential bias, and the absence of a validated burnout scale limits cross-study comparability. Burnout prevalence was assessed using a binary self-report measure that aligns with a contextual definition reflecting the lived experiences of UK trainees, but differs from established questionnaires such as the Oldenburg and Copenhagen Burnout Inventories, which focus on exhaustion and disengagement and may underestimate burnout risk in medical populations. 39,Reference Tipa, Tudose and Pucarea40 Although these instruments assess general domains of exhaustion and disengagement, they are not specific to the medical context and may underestimate burnout risk within these populations. However, within the preset survey, a definition of burnout was provided that captured the ICD-11 key symptoms relating to burnout including exhaustion, depersonalisation and reduced personal efficacy, and this was the definition applied throughout the survey and study. 1 Furthermore, lifestyle factors such as exercise, nutrition and sleep likely have a bidirectional relationship with burnout. These behaviours may contribute to the development or exacerbation of burnout; however, they may also deteriorate as a consequence of burnout-related stress, fatigue and reduced capacity for self-care. As a result, the cross-sectional nature of this study limits the ability to determine the directionality or causality of the observed associations. Data were collected over a defined 3-month period (February to April 2025), which may not fully capture potential seasonal variation in burnout; however, this approach is consistent with prior national workforce surveys that similarly employ short, cross-sectional sampling windows. 21,34,35 Moreover, the survey did not collect further responses on reasons for leaving medicine, nor did we capture respondents’ status as UK or international students, limiting our ability to explore these factors in relation to burnout. The economic analysis also has inherent methodological limitations. Salary estimates were based on average NHS nodal pay points rather than a grade-weighted distribution, which may not represent the different grade levels of resident doctors and contract types in the system. Absenteeism estimates were drawn from national data on stress- and mental health-related disorders, and used as a proxy for burnout-related absenteeism. In contrast, reliable data on presenteeism were unavailable, which likely led to an underestimate of the economic burden. The human capital framework assumes that each lost day represents a full day of foregone output and does not account for labour substitution or organisational adaptation, which may introduce upward biases in the cost estimate.
In conclusion, this study highlights the high prevalence and multifactorial nature of burnout among UK resident doctors and medical students. Limited awareness of available well-being services suggests ongoing barriers to access and communication that require institutional attention. Burnout in this population likely reflects a combination of psychosocial and systemic stress, including financial strain, relocation challenges and poor work–life balance, rather than occupational factors alone. If unaddressed, these pressures may worsen mental health, reduce workforce retention and compromise patient care.
Improving the visibility and accessibility of well-being services, alongside financial and relocation support, can help mitigate stress and promote well-being. A coordinated, multi-level strategy focused on early identification and prevention of burnout throughout medical training is critical to sustaining the resilience of the UK healthcare workforce.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10666
Data availability
The data that support the findings of this study are available upon reasonable request to the corresponding author, U.R.
Acknowledgements
We would like to thank the WARM Study Collaborators Group for distributing the questionnaires across the UK.
Author contributions
U.R. and K.J.C. contributed to study conceptualisation, methodology, investigation, resources, data curation, formal analysis, writing the original draft and reviewing and editing the manuscript. They are also joint first authors and contributed equally. L.A. contributed to study methodology, literature review and reviewing and editing the manuscript. G.K., M.H. and I.P. contributed to formal analysis, data curation and reviewing and editing the manuscript. R.Y.C., A.J., M.S.S. and M.P. contributed to the study investigation, writing the original draft and reviewing and editing the manuscript. S.A. and K.C. contributed to the study investigation and reviewing and editing the manuscript. S.F., N.C., P.B., A.H. and M.L. contributed to study supervision, project administration and reviewing and editing the manuscript.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.





 Open access
Open access
eLetters
No eLetters have been published for this article.