


Introduction
This exploratory study aimed to empower people with serious mental illness to create and implement individualized supported decision-making plans and strategies and study the associated impact on their decision-making processes and progress. This article presents our findings and discusses their implications, including the potential role of supported decision-making in facilitating the participation of individuals with serious mental illness in clinical research, as well as directions for future research.
Supported decision-making is a decision-making framework recognized in both legislation and case law. It is intended to enable individuals with cognitive disabilities to exercise their right to make their own decisions at the time a decision needs to be made, while receiving support from trusted persons. Supported decision-making contrasts with guardianship, conservatorship, and other legal mechanisms that restrict decision-making authority.Reference Blanck 1 Although no standardized model exists, supported decision-making typically involves collaboration with friends, family members, and/or professionals who assist the individual in understanding the situations and choices they face, so they may understand, make, and effectively communicate their own decisions.Reference Dinerstein 2
Supported decision-making can range from informal guidance, like advice from friends,Reference Carney 3 to formal arrangements documented legally, such as Powers of Attorney, Psychiatric Advanced Directives, or supported decision-making agreements,Reference Hallmark and Martinis 4 and may include structured groups, like micro-boards or circles of support, that operate as a type of personal Advisory Council.Reference Kohn, Blumenthal and Campbell 5 All supported decision-making relationships share three key features: (1) they are based on a set of guiding principles that emphasize people’s legal right to make decisions to the maximum of their capabilities; (2) they recognize that people’s desire for or use of support in making decisions does not mean that they need someone to make decisions for them; and (3) they acknowledge that there are many ways to support people with disabilities in making decisions and the support used should be consistent with the person’s abilities, interests, preferences, and needs.Reference Dinerstein 6
Research and scholarship document that people with disabilities — including those whose cognitive capabilities are so limited that they are on the “margins of autonomy”Reference Peterson, Karlawish and Largent 7 — can use supported decision-making to make life choicesReference Harding and Tascioglu 8 such as deciding whether to engage in social and romantic relationshipsReference Boni-Saenz 9 or consenting to medical and mental health care,Reference Sapolsky 10 legal representation,Reference Gooding, McSherry and Arstein-Kerslake 11 and capacity assessments.Reference Jayes, Austin and Brown 12
Research and practice on supported decision-making focus predominantly on people with intellectual and developmental disabilities. However, supported decision-making is a valuable tool for people with serious mental illnessReference Jeste 13 who, above and beyond any decision-making limitations caused by their disabilities, face the risk of having their decision-making authority taken away because of the societal perception that they are “unstable” and cannot make rational decisions.Reference Ringer and Holen 14 Consequently, they may be subjected to guardianship and/or conservatorship, a judicial proceeding where a court removes their legal right to make some or all decisions, or face situations in clinical settings and day-to-day life where their decisions are not respected. 15 Serious mental illness is typically defined as a group of mental, behavioral, or emotional disorders that result in serious functional impairment, substantially interfering with or limiting one or more major life activities. These disorders often involve psychotic symptoms or lead to serious disruptions in areas such as work, relationships, and self-care. 16
Some people with mental health disabilities have concomitant cognitive impairments that affect their ability to consider and make decisions. 17 However, many others have temporary or episodic conditions where they have full capacity to make decisions during periods of stability but are limited in or unable to make decisions during times of crisis.Reference Palmer 18 Additional barriers to decision-making for people with serious mental illness include: (1) feeling uninformed and/or not being supported; (2) fear of lacking competency; (3) poor past experiences; (4) cultural factors; (5) social exclusion; (6) not wanting to be in a decisional conflict; and (7) fear of being viewed as “difficult.”Reference Pathare and Shields 19
Research indicates that patients with serious mental illness want support making everyday, medical, and mental health care decisions to address these and other problems.Reference Velligan 20 These desires could be met, and the above concerns addressed, by developing and implementing individualized supported decision-making relationships and strategies.Reference Jeste 21
The purpose of this study was to better understand the experience of people with serious mental illness in using supported decision-making, and best practices in creating and implementing supported decision-making strategies. Specifically, we address three research questions:
-
1. When empowered by knowledge of supported decision-making and identification of a support person, do individuals with serious mental illness use supported decision-making?
-
2. When empowered by knowledge of supported decision-making and identification of a support person, do individuals with serious mental illness benefit from supported decision-making?
-
3. When empowered by knowledge of supported decision-making and identification of a support person, are individuals with serious mental illness able to decide when and how they want to use supported decision-making?
Finally, this article also considers the implications of our findings for clinical research participation among people with serious mental illness. Given the unique challenges and barriers this population faces in decision-making, understanding how supported decision-making can support their autonomy in clinical research contexts is critical. We discuss how individualized supported decision-making strategies may enhance informed consent processes, participation, and respect for the decision-making rights of people with serious mental illness in research settings.
Methods
The study coached individuals through developing and implementing a supported decision-making plan and collected quantitative and qualitative data about the individual’s experience and associated outcomes of interest. The study is based on a convenience sample of 31 individuals aged 18 and above diagnosed with serious mental illness, specifically schizophrenia, schizoaffective disorder, and bipolar disorder. Each of the project’s 4 research partners recruited between 4 and 13 participants and conducted a series of 4 standardized interview sessions between mid-2019 and the end of 2020. Interviews lasted 60 to 90 minutes, and participants were compensated for each interview they completed.
Two of the four research partners, University of California San Diego and University of California Los Angeles Medical School — Semel Institute in Los Angeles, recruited participants currently receiving psychiatric care at their respective research sites. The other two collaborators, State University of New York (SUNY) Downstate Medical School in New York City and University of Southern California (USC) Outpatient Clinics in Los Angeles County, recruited people more broadly using emails, flyers, and personal invitations.
This study was approved by the Institutional Review Board (IRB) at the University of Southern California, and the IRB approval was obtained prior to recruitment. Interviewers provided each participant with a written consent form, reviewed the contents with them in detail, and obtained their signature to confirm informed consent. Participants were also given a copy of the signed consent form for their reference. They were informed that their participation was entirely voluntary, their identity would not be revealed, and that they could withdraw from the study at any time without penalty or loss of benefits. All data were de-identified by the research sites before being sent to the Burton Blatt Institute, where they were securely stored on a protected drive.
Intervention
After collecting baseline data on the study participants’ decision-making strategies, the interviewers guided each participant through a structured protocol designed to pinpoint life areas where the participant needed support. With guidance from the interviewer, the participant identified individuals they knew who could support them in making decisions in those areas. The participant then developed and implemented supported decision-making plans. By analyzing the post-decision phase, the study aimed to uncover the role of supported decision-making in enhancing quality of life.
In the first session, the interviewer gathered demographic information including age, gender, race/ethnicity, previous and current employment status, and living situation. The participant’s mental health diagnosis was confirmed using the “Diagnostic Screening” tool. This tool was developed by Dr. Michele Pato for use by the SUNY Downstate Psychiatry Research Center in diagnosing patients. For this study, Burton Blatt Institute (BBI) and Saks Institute for Mental Health Law, Policy, and Ethics (Saks Institute) took 10 items from this scale and used it to confirm participants’ diagnoses. There are 10 items in this scale to determine if a person has been diagnosed with or treated for schizophrenia or schizoaffective disorder, bipolar, or manic depression with psychosis.
Participants were asked to come to the second, third, and fourth interview with their primary support person. Participants typically identified a close family member or partner/spouse as their primary supporter. The second interview focused on creating an informal supported decision-making plan. With the supporter listening, participants responded to “When Do I Need Support,” a questionnaire designed to help the participant identify life areas where they want support making decisions. This form included 35 topics divided into ten life areas, including: communication, personal care, staying safe, home and friends, health choices, partners, money, jobs, travel, and citizenship. It was adapted by BBI and Saks Institute staff from “When Do I Want Support? Supported Decision-Making Self Assessment Tool” with permission from the American Civil Liberties Union. 22 The tool was originally developed by University of Missouri-Kansas City Institute for Human Development, University Center for Excellence in Developmental Disabilities as the “Missouri Stoplight Tool.” Participants were given 6 mutually exclusive options (“I can do this alone”, “I want to do this alone”, “I can do this with support”, “I want to do this with support”, “I want someone else to do this for me”, “I need someone else to do this for me”). If a participant expressed a need for support, the interviewer asked how they currently make decisions in that area and how a support person could assist them. Participants were also encouraged to identify others in their life — such as a primary care doctor, therapist, case manager, or friend — who could provide support with specific decision-making areas like job seeking, finances, or medical issues.
Building on these responses, the interviewer worked with the participant to create a supported decision-making plan identifying: (1) life areas where they need/want support; (2) their primary supporter; (3) other members of their support team; (4) the type of support they want; and (5) the frequency of support team meetings.
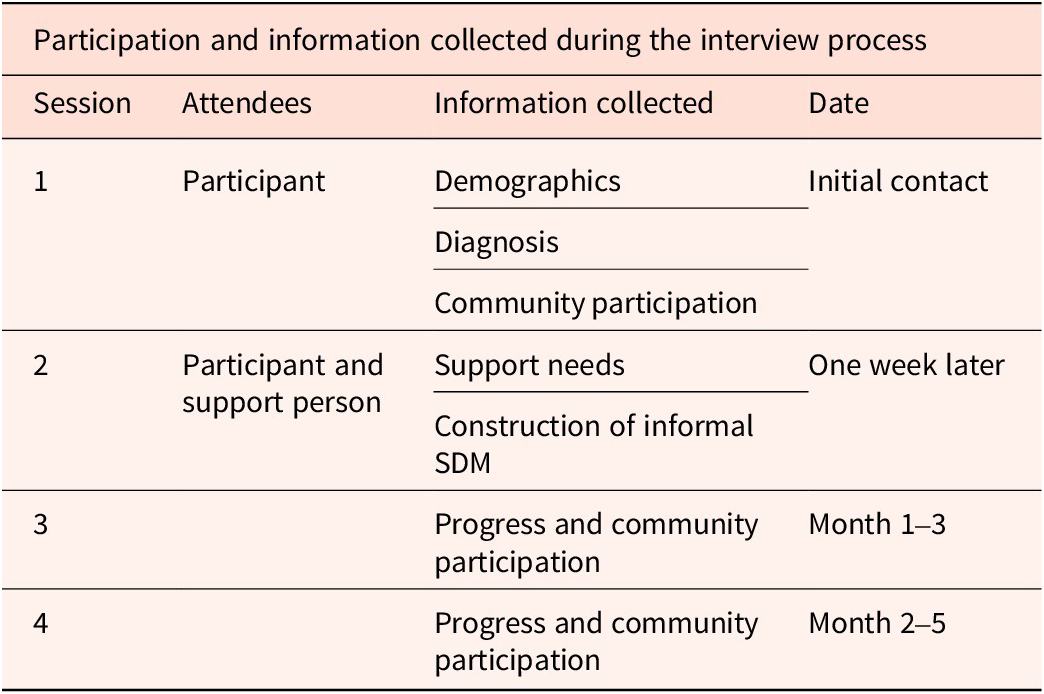
In the third and fourth sessions, interviewers prompted participants to report progress and challenges in each of their supported decision-making focus areas, satisfaction with using supported decision-making in making decisions, and possible uses of supported decision-making in future decision-making. Support persons were present during the third and fourth sessions. See Table 1 for a description of the interview protocol.
Interview Protocol Structure

Table 1: Long description
The table has four columns labeled Session, Attendees, Information collected, and Date. The main header spans all columns and reads Participation and information collected during the interview process. Session 1 lists Participant as attendee, with Demographics, Diagnosis, and Community participation as information collected, and Initial contact as the date. Session 2 lists Participant and support person, with Support needs and Construction of informal S D M as information collected, and One week later as the date. Session 3 and Session 4 have no attendees listed, both collect Progress and community participation, with dates Month 1 to 3 and Month 2 to 5 respectively.
Participants
As mentioned, two of the four research partners recruited participants currently receiving psychiatric care at their respective research sites. The other two collaborators recruited people more broadly using emails, flyers, and personal invitations. This sampling approach differs from the broader population of individuals affected by serious mental illness. Compared to the population of individuals with serious mental illness reported by the Substance Abuse and Mental Health Services Administration, 23 our sample reflects the population’s gender and age distribution but includes a disproportionately high number of African American and Hispanic participants, and our sample exhibits higher levels of education and unemployment at the time of the study. While these sample characteristics present some limitations, the findings nevertheless offer valuable insights into the experiences and potential benefits of supported decision-making for people with serious mental illness.
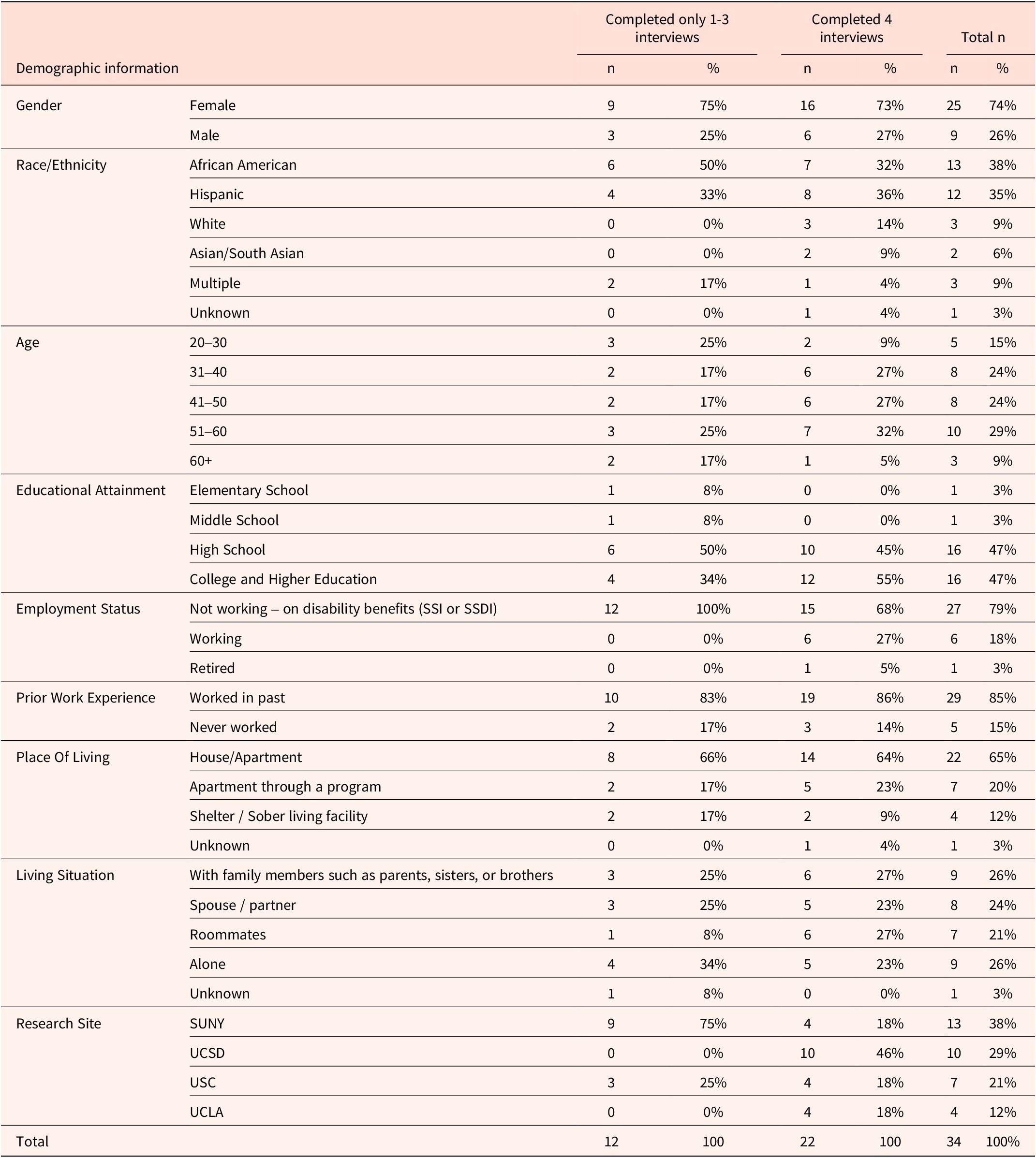
Demographic characteristics of the participants are shown in Table 2.
Demographic Information About Participants

Table 2: Long description
The table presents demographic information for participants grouped by those who completed only one to three interviews, those who completed four interviews, and totals. For gender, females comprised 75 percent of the one to three interview group, 73 percent of the four interview group, and 74 percent overall. Males made up 25 percent, 27 percent, and 26 percent, respectively. For race or ethnicity, African American participants were 50 percent, 32 percent, and 38 percent; Hispanic participants were 33 percent, 36 percent, and 35 percent; White participants were 0 percent, 14 percent, and 9 percent; Asian or South Asian were 0 percent, 9 percent, and 6 percent; Multiple races were 17 percent, 4 percent, and 9 percent; Unknown was 0 percent, 4 percent, and 3 percent. Age groups: 20 to 30 years were 25 percent, 9 percent, and 15 percent; 31 to 40 years were 17 percent, 27 percent, and 24 percent; 41 to 50 years were 17 percent, 27 percent, and 24 percent; 51 to 60 years were 25 percent, 32 percent, and 29 percent; 60 plus years were 17 percent, 5 percent, and 9 percent. Educational attainment: elementary school was 8 percent, 0 percent, and 3 percent; middle school was 8 percent, 0 percent, and 3 percent; high school was 50 percent, 45 percent, and 47 percent; college and higher education was 34 percent, 55 percent, and 47 percent. Employment status: not working on disability benefits was 100 percent, 68 percent, and 79 percent; working was 0 percent, 27 percent, and 18 percent; retired was 0 percent, 5 percent, and 3 percent. Prior work experience: worked in past was 83 percent, 86 percent, and 85 percent; never worked was 17 percent, 14 percent, and 15 percent. Place of living: house or apartment was 66 percent, 64 percent, and 65 percent; apartment through a program was 17 percent, 23 percent, and 20 percent; shelter or sober living facility was 17 percent, 9 percent, and 12 percent; unknown was 0 percent, 4 percent, and 3 percent. Living situation: with family members was 25 percent, 27 percent, and 26 percent; spouse or partner was 25 percent, 23 percent, and 24 percent; roommates was 8 percent, 27 percent, and 21 percent; alone was 34 percent, 23 percent, and 26 percent; unknown was 8 percent, 0 percent, and 3 percent. Research site: S U N Y was 75 percent, 18 percent, and 38 percent; U C S D was 0 percent, 46 percent, and 29 percent; U S C was 25 percent, 18 percent, and 21 percent; U C L A was 0 percent, 18 percent, and 12 percent. Totals for each group are 12, 22, and 34 participants, respectively. Note: due to rounding, some sections may not add up to 100 percent.
Note: Due to rounding, some sections may not add up to 100%.
Twenty-two participants engaged in all four sessions with project staff, created and implemented their supported decision-making plans, and reported on their progress and experiences. Researchers conducted a total of 111 interviews.
Analysis
During the interviews, participants were asked to respond to a combination of quantitative and qualitative questions designed to capture their baseline decision-making process and identify areas in which they need or want support. We calculated the prevalence of each answer to multiple-choice questions, including the demographic questionnaire and levels of support needed for 35 items within 10 topic areas. While analyzing participants’ need for support in making decisions, we grouped their answers into 2 categories: “no support needed” (I can do this alone, I want to do this alone) and “need some support” (I can do this with support, I want to do this with support, I need someone else to do this for me, I want someone else to do this for me). We analyzed the qualitative data by coding each comment based on the nature of the response within categories of current decision-making strategies, areas of needed support, potential role of supporter, and satisfaction with using the supported decision-making plan. We produced reports for each of the categories and identified crosscutting themes.
Findings
1. Using and Benefiting from Supported Decision-Making
1a. Need for Supported Decision-Making
Before creating their supported decision-making plans, participants were asked to discuss their decision-making strategies and areas of life where they need support. Almost one-quarter of respondents (24%) said they generally make decisions by themselves and almost two-thirds (64%) said they consult with supporters before making important decisions. A smaller number (12%) of respondents reported they need someone else to make decisions for them.
Even among those who initially described themselves as independent decision makers, many stated that they seek others’ input for significant decisions involving their health, money, or housing. One participant, Erin, (31, female, Hispanic) (all names are pseudonyms) described her process as: “Like everyone else. Actually, when I was reading this, I was like, I kind of already do the supportive decision method. I use my family as a sounding board and my friends as sounding boards if it’s an important decision, and I usually just decide what to do on my own.”
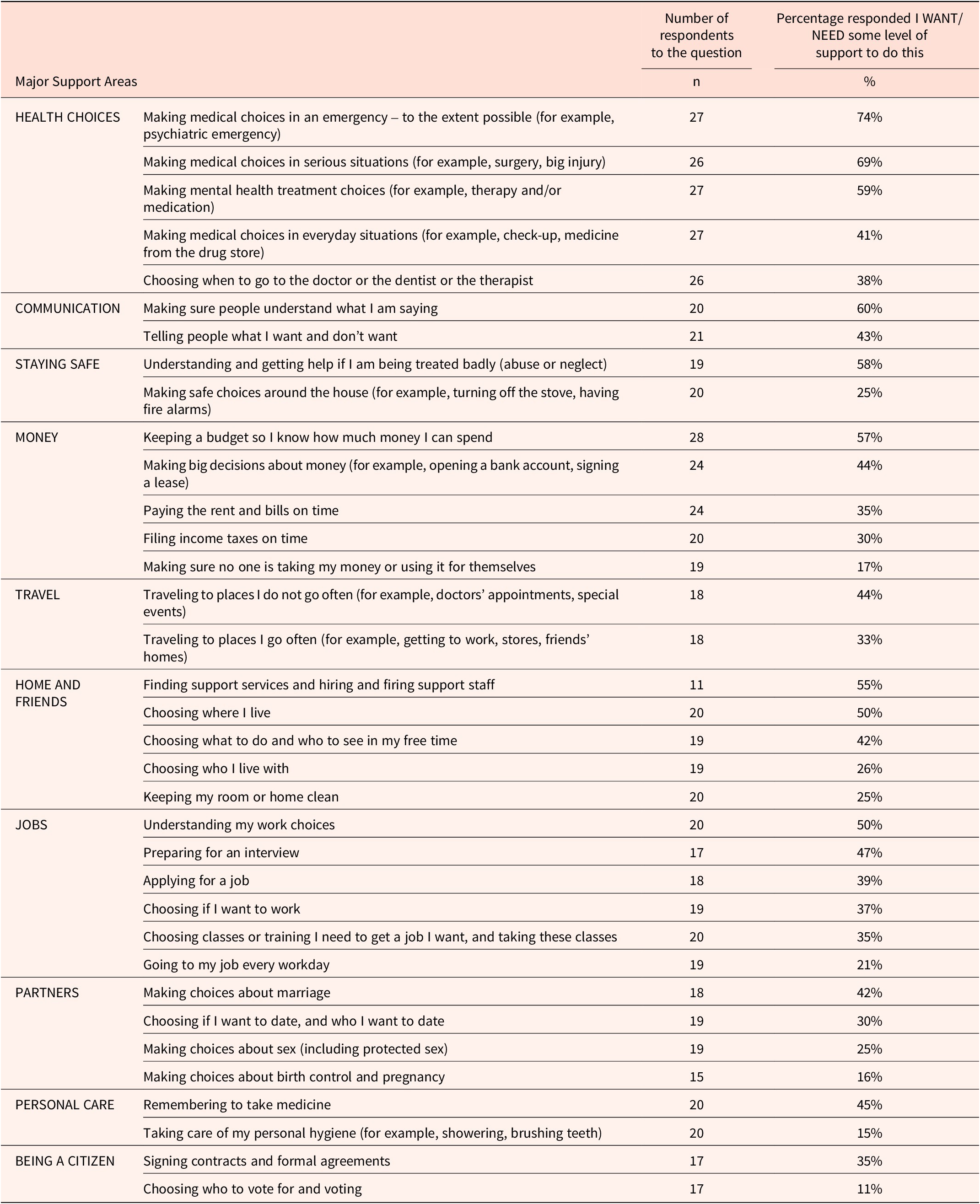
Participants were also asked to rate their need for support in 10 major life areas and a total of 35 specific decisions within those areas. Decisions about clinical research participation were not included among the 10 life areas. Participants were requested to describe the type of support they needed (Table 3) from supporters or other parties such as doctors. This activity was a precursor intended to highlight life areas participants should consider when developing their supported decision-making plans.
Type of Support Needed by Participants

Table 3: Long description
From the top row downward, the first column lists major support areas: Health Choices, Communication, Staying Safe, Money, Travel, Home and Friends, Jobs, Partners, Personal Care, and Being a Citizen. For each area, the next column details specific support needs. For Health Choices, needs include making medical choices in emergencies (27 respondents, 74 percent), serious situations (26, 69 percent), mental health treatment (27, 59 percent), everyday medical choices (27, 41 percent), and choosing when to visit health professionals (26, 38 percent). Communication includes making sure people understand (20, 60 percent) and expressing wants (21, 43 percent). Staying Safe covers understanding and getting help for abuse or neglect (19, 58 percent) and making safe choices at home (20, 25 percent). Money includes budgeting (28, 57 percent), big financial decisions (24, 44 percent), paying bills (24, 35 percent), filing taxes (20, 30 percent), and preventing financial exploitation (19, 17 percent). Travel is divided into unfamiliar places (18, 44 percent) and familiar places (18, 33 percent). Home and Friends includes finding support staff (11, 55 percent), choosing where to live (20, 50 percent), free time choices (19, 42 percent), choosing housemates (19, 26 percent), and keeping home clean (20, 25 percent). Jobs covers understanding work choices (20, 50 percent), interview preparation (17, 47 percent), applying for jobs (18, 39 percent), choosing to work (19, 37 percent), job-related training (20, 35 percent), and job attendance (19, 21 percent). Partners includes marriage choices (18, 42 percent), dating (19, 30 percent), sexual choices (19, 25 percent), and birth control or pregnancy (15, 16 percent). Personal Care includes remembering medicine (20, 45 percent) and hygiene (20, 15 percent). Being a Citizen includes signing contracts (17, 35 percent) and voting (17, 11 percent). Percentages indicate the proportion of respondents who want or need some level of support for each item.
Participants reported the need for support in “Making medical choices in serious situations” and “Making medical choices when there is a psychiatric emergency.” Some participants indicated a desire to create a plan for emergency situations in collaboration with their support person. One participant, Hermina, a 32-year-old Hispanic woman, elaborated: “My boyfriend and I actually discussed reaching out to the doctor in case I start having a manic episode or just an episode in general, so he now has her phone number, or at least her name, and he knows what to ask for.”
When asked who they wanted to support them during an emergency, almost all participants (95%) said they want their psychiatrist or physician to make the decision but wanted their supporters to help them ask questions, understand the answers, and provide a calming influence.
More than half of the participants (57%) said they need some level of support managing money. Most participants had low incomes, were on governmental disability benefits, and/or were living in supportive or subsidized housing. Most participants wanted their support person to help them develop and keep to a budget.
Most participants said they did not need support making decisions about transportation but sometimes needed their support person to drive them because they did not have access to transportation or due to their medical condition. As Sara, a 44-year-old White female explains, “It really depends on if I’m symptomatic or not. I can do it alone when I’m not, and I want to do it alone when I’m not, but I go in and out of having driving privileges.” This refers to periodic loss or restriction of legal driving privileges due to her medical condition or treatment status.
Out of 34 participants, 26 (76%) stated that they are not working currently due to their disabilities. Almost half (47%) of the participants stated that they need support to prepare for a job interview. Specifically, participants stated that they need motivation, encouragement, and advice from their support person before an interview. Participants who wanted support said that they would like to work with a counselor or someone with more knowledge about jobs.
Participants identified their need for support in effectively conveying their thoughts and intentions across multiple decision areas, including health, safety, community living, and interpersonal relationships. Participants frequently expressed concerns about their ability to communicate effectively with medical professionals, particularly during the acute phases of their serious mental illness. As one participant, Laura, a 27-year-old African American woman, stated: “Sometimes it’s hard for me to advocate for myself, and it’s good for me to have an advocate so they can say exactly what I mean if I’m not explaining it correctly[…] It’s mostly [with] doctors.”
Participants voiced their fear of losing control in challenging situations and recognized the need for a supporter to calm them and facilitate effective communication. As Manuella, a 59-year-old Hispanic woman explained:
It gets me depressed when somebody treats me bad because what I have learned through therapy is to be assertive, to talk, to talk. I usually keep it quiet and I start ruminating on things. Then I get upset. So, talking to my counselor about it, she tells me to put boundaries and to talk in a nice way but to be assertive. “You’ve got to talk. You’ve got to talk.” So nowadays, that’s what I’m doing. I’m protecting myself.
When participants were asked how their support person can help in these kinds of situations, answers included, “clarifying what I am saying or what they are saying to me,” “Giving advice about the situation,” “Advocating,” and “Encouraging.” Participants typically identified a close family member or partner/spouse as their primary supporter.
Although participants had the opportunity to identify additional supporters for different life areas, they often relied on their primary supporter even when that person may not have had the expertise needed to help with every decision. In addition, because of the close relationship between the participant and supporter, some “household” decisions — such as those involving money and intimate relationships — directly involved the interests or actions of the supporter. Thus, the participant may not have felt comfortable involving additional supporters in the decision-making process.
1b. Perceived Benefits of Supported Decision-Making
During their second interview, participants developed an individualized supported decision-making plan, focused on their decision-making strengths, limitations, interests, and preferences, with the help of the interviewer and their supporter. In subsequent interviews, participants reported on the progress they were making in implementing supported decision-making strategies.
Participants expressed satisfaction with their supported decision-making experience and identified benefits of and positive emotions towards the supported decision-making process. Zuri, a 44-year-old South Asian/Indian woman stated:
I don’t want to be dependent; I don’t want to be independent; I want to be interdependent and live in a community, and I don’t want to be left alone, isolated, alienating myself from the rest of the world. I want to make sure that I am part of the community, that I’m contributing, and I feel valued for what I bring to the table. But given my mental condition and disability, it’s not been easy to do, to be appreciated, because I can go on tangents, like on a euphoric trip somewhere, and I’ve lost myself and I’ve lost people. So I want to live in a community. I don’t want to live alone.
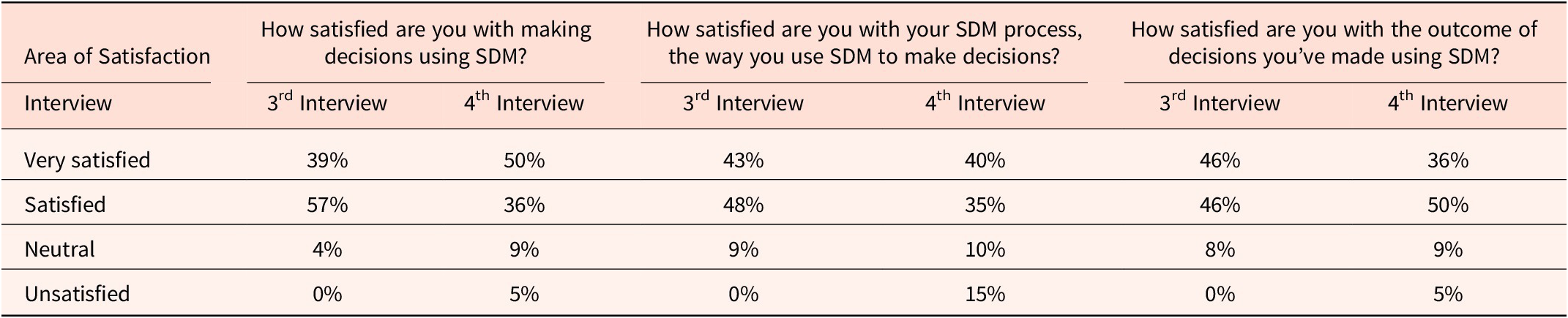
After their supported decision-making session with their supporters, several participants were pleasantly surprised to realize that beyond their spouse, partner or family members, other individuals such as friends or case managers could provide meaningful support. Supported decision-making also helped participants take action where they had previously struggled. Table 4 shows the number of participants who expressed satisfaction with supported decision-making, with the majority being “very satisfied” or “satisfied.” We note that some participants reported reduced satisfaction in the last interview.
Satisfaction with Supported Decision Making

Table 4: Long description
The table has four rows for satisfaction levels: Very satisfied, Satisfied, Neutral, Unsatisfied. The first column lists these levels. The next six columns are grouped in pairs under three domains: satisfaction with making decisions using S D M, satisfaction with the S D M process, and satisfaction with outcomes of decisions made using S D M. Each domain has data for the third and fourth interviews. For ‘Very satisfied’, percentages are 39 and 50 for making decisions, 43 and 40 for process, 46 and 36 for outcomes. For ‘Satisfied’, values are 57 and 36 for making decisions, 48 and 35 for process, 46 and 50 for outcomes. For ‘Neutral’, values are 4 and 9 for making decisions, 9 and 10 for process, 8 and 9 for outcomes. For ‘Unsatisfied’, values are 0 and 5 for making decisions, 0 and 15 for process, 0 and 5 for outcomes. The highest satisfaction is seen in the ‘Satisfied’ and ‘Very satisfied’ categories, with a slight increase in ‘Unsatisfied’ responses in the fourth interview, especially for the process domain.
2. Understanding When and How to Use Supported Decision-Making
In their second interview, participants shared how they were able to understand and decide when and how to use supported decision-making in different areas of their lives on their own. Most participants who used supported decision-making strategies applied them to make decisions on issues that arose in the course of their lives, even when those issues were unrelated to their plan. Only one in five (20%) said they used supported decision-making in all of the areas they chose. This suggests that a dynamic approach to supported decision-making may be more useful than a prescriptive one assigning specific supported decision-making methodologies to specific life areas.
When describing their decision-making processes, respondents drew attention to two significant differences. First, they distinguished between the type of support they needed during periods of mental health stability compared with the support they needed during acute phases of their condition. Second, they made a distinction between routine day-to-day decisions and more substantial or complicated decisions.
During periods of stability, participants reported they were generally capable of making most decisions without needing others to decide for them. However, many still valued and relied on practical or emotional support, especially in certain areas like health care, even outside of crisis situations.
For example, almost half of the participants reported needing support for everyday medical decisions, even when not in crisis. They wanted their support persons to help them throughout the broader medical process, not just with decisions themselves, including: (1) encouraging and motivating them to go to appointments; (2) accompanying them to the appointments, listening to doctors, asking clarifying questions, and helping clarify the doctors’ instructions and follow-up calls; and (3) driving them to appointments and picking up their medicine(s) from the pharmacy. This type of support differs from what is needed during acute phases of illness, when participants described relying more heavily on their supporters for help interpreting information, making decisions, or advocating on their behalf when they were unable to do so themselves.
Participants frequently expressed the need for support when communicating with their health care providers. This need arises for several reasons: (1) they may become flustered or upset, making it difficult to follow what the provider is saying; (2) providers may dismiss or disbelieve their concerns, assuming they are unable to think clearly; and (3) due to the stigma surrounding mental health issues, they may delay seeking care or struggle to follow through with treatment plans (further discussed below as a barrier). Interestingly, despite these experiences, some participants still wanted providers to take a more active role in decision-making. This may reflect a complex interplay of perceived expertise, trust in medical authority, and the challenges of navigating care while managing symptoms or stigma.
Many participants highlighted differences in their decision-making approaches based on the importance or complexity of the issue, often describing how they relied more on others for higher-stakes decisions. One participant, Nadine, a 20-year-old African American woman, said: “If it’s a big decision, I will consult with [my partner], because I tend to second guess myself. When it comes to regular decisions, I just ask myself the pros and the cons of it, so I weigh the pros, I weigh the cons, and I just go ahead and make my decision. If I’m going back and forth, I’ll consult with him and his mom and then we’ll come to a conclusion.”
3. Barriers and Differences in Using Supported Decision-Making Strategies
Some participants faced barriers when making decisions even when empowered to use supported decision-making through our intervention facilitated by researchers. For example, some participants reported a reluctance to engage in proactive decision-making or to act upon their decisions because they worry about the reaction of people around them.
This fear of stigma and discrimination manifested in various ways. For example, several respondents reported that fear of discrimination influenced their decision not to pursue employment opportunities. One participant, Bailee, a 52-year-old Native American/Hispanic woman, said “I want to try to work, but I don’t know if they give jobs to schizophrenia people [sic]. Some people in the world are skeptical about it, or worried about it.”
Stigma appeared to shape medical decisions as well. Participants sometimes avoided seeing a doctor or did not want others to know they were going through a medical or mental health emergency. Esther, a 44-year-old Hispanic woman, explains: “It’s more of a stigma thing; I don’t want people to know. If I do go, I do go; if I don’t, I don’t.”
Economic factors also presented a barrier to supported decision-making use by limiting people’s real options to decide where and how they live, concomitantly limiting their opportunities to use and benefit from supported decision-making. While supported decision-making supports individuals in making informed choices, these economic constraints reflect broader social service and policy challenges that affect available options. For example, several participants had low incomes, which limited their choices in where to live; often the only neighborhoods they could afford were less safe, far from family and friends, and offered limited transportation, making it difficult to participate in activities or visit loved ones.
Similarly, many study participants relied on government services that limited their choices about where to live and whether to work. Subsidized housing was only available in certain areas, and many feared losing Social Security benefits if they earned income. These structural constraints represent macro-level barriers that limit real options, thereby restricting opportunities to engage in supported decision-making, which is inherently focused on micro-level choices. For example, eight participants had housing through a mental health or subsidized housing program, and five were staying in a shelter or sober living facility, programs that often provided little input or choice regarding living situation. Participants reported that they sometimes were relocated without prior notification and have limited input in selecting roommates.
Even those who were not in such a program felt restricted about their housing choices due to affordability. One participant, Mary, a 57-year-old African American woman, said: “Choosing where I live. You know, these days people don’t have choices about where they live. You gotta take an apartment where you can find it at […] This new one I am staying, they just moved me; I had no choice.”
These findings demonstrate a key limitation of supported decision-making. Individuals must have real choices to make to use and benefit from supported decision-making. When societal, economic, or other macro-level factors constrain or remove these choices or fail to offer options aligned with a person’s preferences and interests, supported decision-making’s utility is inherently limited.
Another barrier to supported decision-making can be the supporter. For most participants, their primary support person was a partner (43%) or a close family member (33%). Others identified friends or a therapist, while some reported having no consistent support person. While having a close family member as a primary support person can be beneficial in health care settings — since these individuals are often readily available and familiar with the situation — it also presents challenges. Supporters may lack the necessary expertise or face personal challenges of their own, such as physical or mental health issues, housing instability, or financial difficulties. These factors can limit their ability to prioritize the needs of the decision-maker or may be compounded by complex family dynamics, which in turn can shape the type and quality of support they are able to provide. As a result, participants expressed concerns that their supporters often did not have the necessary knowledge to assist with certain decisions. As Esther stated: “I guess it could be better. I could have people with more knowledge or who are experts in certain fields that I’m trying to acquire and be successful in. Obviously, my roommate and my mother have no clue about mental illness or drug and alcohol for me to ask them for any decision on that.”
Finally, participants reported that their emotional and mental states varied across time and circumstances. As a result, it was sometimes hard for them to identify the times when they needed support to make decisions. Sarah, a 44-year-old White woman, expressed this situation as: “I think it’s important to note that because symptoms are not static, there are some times in my life when I can and am completely capable of making these decisions on my own, but when I am symptomatic, my ability to make decisions is compromised. That’s when [my partner] is able to help me.”
Discussion
This study explored the ways in which adults with serious mental illness understand and use supported decision-making across multiple domains of daily life.Reference Shogren and Wehmeyer 24 Participants consistently reported that supported decision-making enhanced their sense of agency and provided practical support for navigating complex decisions, particularly in healthcare settings. The findings extend prior research by demonstrating that people with serious mental illness actively use supported decision-making not only during periods of crisis but also during stable phases of illness, adapting the type and intensity of support to the decision at hand.
A central contribution of this study is the recognition that participants did not use supported decision-making in rigid or prescriptive ways. Rather, they applied supported decision-making strategies flexibly, calling upon supporters as needed in relation to the importance, complexity, or emotional difficulty of a decision.Reference Enck 25 This pattern mirrors how individuals without psychiatric disabilities make decisions in everyday life, supporting theoretical frameworks of relational autonomy that emphasize the dynamic role of social relationships and context in shaping decision-making.Reference Mackenzie and Stoljar 26
Despite these benefits, several barriers limited participants’ ability to fully use and benefit from supported decision-making. First, the episodic nature of serious mental illness created fluctuations in decision-making capacity. Participants described feeling confident during stable periods but struggled to make or communicate decisions during acute phases of illness.
Importantly, 95% of participants expressed a preference for clinicians to lead decision-making during emergencies, with trusted supporters in advisory roles. This finding complicates traditional interpretations of autonomy that prioritize individual control at all times. Instead, it reveals that individuals with serious mental illness may view autonomy as context-sensitive, valuing professional expertise and trusting relationships when experiencing limited cognitive capacity. This highlights the importance of developing supported decision-making models that accommodate dynamic shifts in decisional preferences.
Second, stigma and discrimination emerged as recurring barriers. Several participants expressed reluctance to disclose their diagnosis to employers or healthcare providers, fearing dismissal, disbelief, or outright rejection. These concerns not only constrained participants’ willingness to engage supporters in sensitive decisions but may also influence preferences for delegating certain decisions, particularly when navigating systems that have historically diminished their input.
Third, structural and economic factors constrained participants’ real options. Limited income, reliance on government benefits, and restrictions imposed by subsidized housing programs often left individuals with few meaningful choices. As participants explained, being relocated without input or having limited control over housing circumstances restricted their ability to engage in true decision-making, regardless of the presence of supportive relationships. These findings demonstrate that supported decision-making can only be effective when individuals have access to real and viable options.
Another important finding is the distinction between wanting support to make decisions and preferring others to make decisions on one’s behalf. While we grouped both under “needing some support,” we acknowledge that these are conceptually distinct: one reflects a desire for assistance in making decisions whereas the other reflects a preference to delegate decision authority.
Additionally, participants frequently emphasized the value of non-cognitive forms of support, such as emotional encouragement, motivation, and validation. These findings challenge supported decision-making models that focus narrowly on enhancing cognitive understanding or processing and suggest the need for more holistic frameworks that address the full spectrum of support needs among individuals with serious mental illness.
Finally, while most participants expressed high satisfaction with supported decision-making strategies over time, some reported decreased satisfaction between the third and fourth interviews. Though our data did not provide specific explanations, it is plausible that external factors, such as increased stress or disruptions related to the COVID-19 pandemic, may have contributed to this reduction in satisfaction.
Study Challenges and Limitations
This study has some limitations. The sample was recruited through a convenience approach, which may limit generalizability. Also, because serious mental illness is episodic, participants’ support needs and decision-making capacities fluctuated over time, complicating efforts to assess consistency in supported decision-making use.
In addition, some interviews were conducted with both the individual with serious mental illness and their support person present. While we only recorded participants’ views, the presence of a support person may also have influenced participants’ responses, particularly in sensitive areas where social desirability or concerns about conflict could shape answers.
Finally, while many participants relied on family or close friends as primary supporters, these individuals often lacked expertise in complex domains such as healthcare, legal rights, or financial planning. Despite these challenges, the study provides valuable insights into the real-world implementation of supported decision-making for people with serious mental illness.
Implications for Clinical Research
A distinctive contribution of this study lies in its implications for the participation of individuals with serious mental illness in clinical research. Historically, research protocols have excluded individuals with serious mental illness from clinical trials due to concerns about their capacity to provide informed consent.Reference Humphreys, Blodgett and Roberts 27 However, our findings support emerging evidence that supported decision-making can provide the necessary supports to enable informed and voluntary participation in research.
Participants in this study demonstrated that, when provided with encouragement, clarification, and trusted supporters, they were able to understand, deliberate, and make informed decisions across a wide range of life domains. This aligns with prior studies showing that individuals with serious mental illness can successfully participate in research and capacity evaluations when provided with peer support or decision-making tools.Reference Fortuna 28
Our findings suggest that clinical research protocols should incorporate supported decision-making strategies at multiple stages of the research process. Informed consent procedures, for example, can be adapted to include the use of plain-language materials, allow extended time for decision-making, and encourage the involvement of a trusted supporter who can assist the potential participant in understanding the study and its risks and benefits.Reference Silverman 29 In addition, formal supported decision-making agreements could explicitly include research participation as a decision-making domain, particularly for individuals whose decision-making abilities fluctuate due to the episodic nature of serious mental illness.
Beyond the consent process, supported decision-making could also support participants throughout the full course of clinical trial involvement. Trusted supporters could assist with ongoing decision-making around continued participation, adherence to treatment protocols, or managing side effects. Incorporating supported decision-making into the broader research context may help individuals navigate the complexities associated with clinical research while maintaining their sense of agency and trust in the process.
Given participants’ variable capacities over time, protocols should also consider the episodic nature of serious mental illness by integrating capacity assessments with supported decision-making plans that specify preferred supports during symptomatic periods. This approach not only strengthens autonomy but enhances ethical research practices by tailoring consent and participation processes to the individual.
Finally, future research should explore whether the type of trial or level of risk involved influences preferences around decisional delegation. For example, participants may feel more comfortable delegating decisions for high-risk studies while preferring greater autonomy in low-risk contexts. Understanding these preferences can inform the design of flexible and participant-centered research protocols.
Beyond clinical research settings, these findings hold important implications for healthcare practice and policy. This study provides an essential foundation for informing laws, policies, guidelines, and clinical practices that protect the rights of people with serious mental illness. The findings emphasize the importance of understanding how supported decision-making functions during both stable periods and times of crisis, offering critical insights for healthcare providers and researchers. As such, future research should focus on identifying opportunities and best practices for medical and mental healthcare providers to explore and integrate supported decision-making into their practices, empowering people with serious mental illness to be full and equal participants, and the primary decision-makers, in their healthcare.
Implications for Future Research
Our findings highlight several critical areas for future research. First, there is a need to better distinguish between participants’ preferences for decisional support, where an individual retains decision-making authority but seeks assistance, and decision-making delegation, where authority is formally or informally transferred to another person. In our study, participants used the broad language of “support,” but their underlying motivations varied. Some preferred assistance in understanding and weighing options, while others expressed a preference for someone else, often a clinician, to make decisions on their behalf, particularly during times of crisis. These preferences may be influenced by prior experiences of stigma or dismissal, and future studies should investigate how these factors shape individuals’ decisions to delegate rather than direct their own care or participation in research.
Second, future research should expand the conceptual understanding of what constitutes effective support in supported decision-making. Much of the existing literature has focused on cognitive enhancement such as improving understanding, and other articles in this symposium focus on support leading to authentic decisions.Reference Pan, Dinerstein and Wendler 30 However, our findings indicate that many participants valued affective and motivational forms of support just as much. As such, future studies should explore how supported decision-making models can be adapted to include non-cognitive forms of support, and how these may impact outcomes for people with serious mental illness across various contexts.
Third, future research should examine how supported decision-making strategies can be effectively integrated into clinical research protocols, particularly those involving individuals with serious mental illness. This includes identifying best practices for when and how to involve supporters, designing informed consent processes, and evaluating whether supported decision-making improves participant comprehension, retention, and satisfaction. In addition, empirical research is needed to assess the feasibility and effectiveness of maintaining supporter involvement throughout the entire course of a clinical trial, not just during the consent process.
Finally, longitudinal research designs are essential to capture how individuals with serious mental illness use supported decision-making over time, including during transitions between stability and crisis. Such studies could provide insight into how advance planning, flexible supported decision-making agreements, and dynamic support networks can be used to uphold autonomy, even when decisional or cognitive capacity fluctuates. Future research should also explore the role of provider training, system-level policies, and legal recognition in shaping the implementation and impact of supported decision-making across healthcare and research environments.
Conclusion
Overall, this study demonstrated that supported decision-making offers a promising framework for enhancing autonomy, communication, and participation in decision-making among people with serious mental illness. Participants reported high levels of satisfaction with supported decision-making and described it as a flexible and empowering process that could be adapted to everyday and complex decisions alike. However, the effectiveness of supported decision-making is limited by stigma, structural barriers, and economic constraints that reduce the range of real choices available. By integrating supported decision-making into healthcare, social services, and clinical research, professionals can better support individuals with serious mental illness as full and equal participants in their lives and communities.
Human subjects
The Saks Institute for Mental Health Law, Policy, and Ethics (Saks Institute) at the USC Gould School of Law was responsible for securing the data key with the names of the study participants and their ID numbers. The principal investigators at each of the four sites sent this information to the Saks Institute after assigning random (non-sequential) ID numbers. All subjects were deidentified. All names identified with the quotes in this paper are pseudonyms to protect individual privacy in accordance with approval to the Saks Institute by the USC Institutional Review Board. The Burton Blatt Institute was not involved in the data collection for this study and only reviewed deidentified data.
Competing interests
The authors have no conflicts to disclose.
Funding statement
This study was funded by the Saks Institute. This study was also in part funded by the Burton Blatt Institute by Syracuse University research funding to Dr. Blanck.

 Open access
Open access