

Introduction
One day as a young doctor, on my way out of the hospital, I bumped into one of my former Senior registrars who is now a consultant. ‘Maria!’ he said, ‘You look very nice.’ He gave me the long top-down look and lingered on the lower half of my body. I politely replied, ‘thank you’. ‘How is work going?’ ‘Fine.’ ‘What are you up to?’ And as he asked that follow up question, he continued to inappropriately stare at the lower half of my body. I tilted my head, staring right into his face with that look that is supposed to tell anyone actually looking at my face that, ‘I can see what you are doing, and you better stop it now.’ And then I answered, ‘Work and school as usual.’ He obviously had not even seen my facial expression. His stare was still on the lower half of my body. ‘I see. You look so good. Listen … Maria … You are married and I am married. Why don’t we get a room and make each other feel good?’ I stood there staring at him in disbelief, but he was clearly not registering. He is looking at me but he either can’t see what my face is saying or couldn’t care less. He continues, ‘Enh? You obviously do not have HIV and neither do I so … let’s just do that. We help each other out.’
I am too shocked to respond just yet. I am asking myself, what did I just miss? How did our conversation move from a greeting straight to the bed? How did a man with whom I always had purely academic conversations give himself permission to speak to me about all this? I felt violated. I was angry, disgusted and humiliated as to why I was not being seen as a professional.
This was my personal experience starting out as a young doctor. These kinds of experiences prompted us to work on this project to share real life stories of sexual harassment, bringing awareness and insight into this immorality, and pave the way for policy creation on sexual harassment in the workplace.
Gender in Society
Zambia is a landlocked, resource-rich country with sparsely populated land in the centre of Southern Africa. It shares its border with eight countries (Angola, Botswana, Democratic Republic of the Congo, Malawi, Mozambique, Namibia, Tanzania, and Zimbabwe) that serve as an expanded market for its goods. Its population, much of it urban, is estimated at about 17.9 million and growing rapidly at 2.8% per year, partly because of high fertility, resulting in the population doubling close to every twenty-five years. (1) Girls and women continue to remain vulnerable because of many age- and sex-specific social barriers and gender inequalities. High Gender-Based Violence (GBV) prevalence in Zambia, particularly in rural areas, is due to existing cultural norms and unequal power relations at the household level. The 2013/14 Zambia Demographic Health Survey (ZDHS) reports that from all women who had experienced any type of physical or sexual violence, only 43% sought help to stop the violence, 9% never sought help but told someone, and 42% did not seek help and never told anyone. (2) Where help was sought, GBV survivors most frequently sought it from their own family (69%) or from the husband or partner’s family (43.2%), while formal structures of support were hardly approached for help (e.g., police – 7.8%; medical staff – 1.5%; social work – 2.2%). Unfortunately, there are no cases of sexual harassment in the workplace from any sector which have been referred to the National Prosecution Authority (NPA), except for one in the recent past.
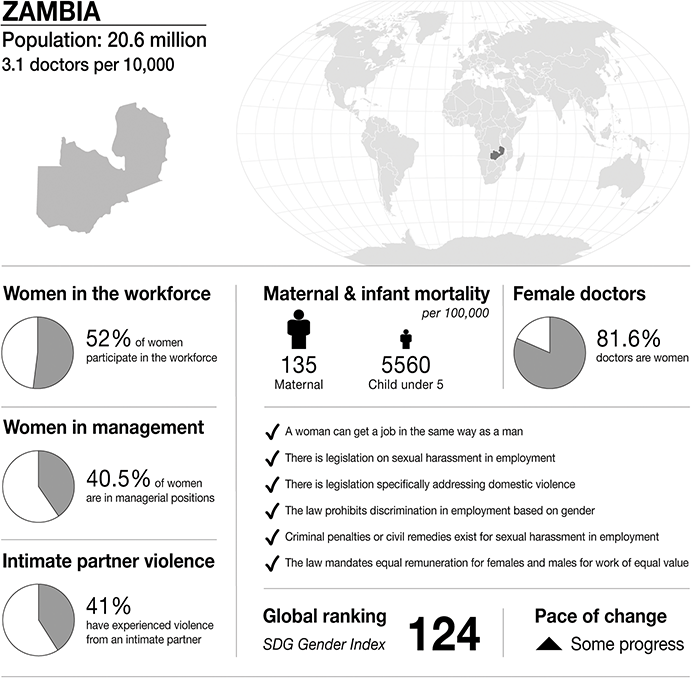
Infographic Zambia. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.
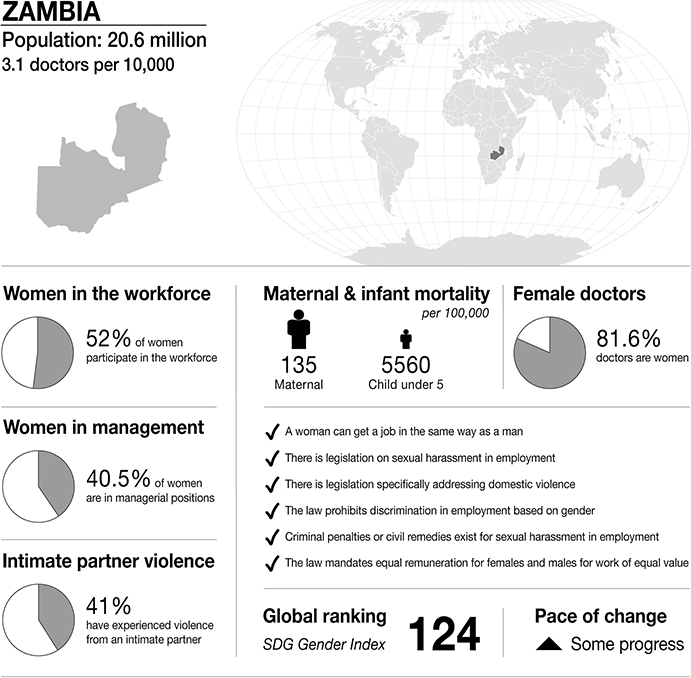
Figure 30.1 Long description
The infographic provides information about Zambia, with a population of 20.6 million and 3.1 doctors per 10,000 people. It highlights several gender-related statistics. 52 per cent of women participate in the workforce. 40.5 per cent of women are in managerial positions. 41 per cent of women have experienced intimate partner violence. Maternal mortality is 135 per 100,000. Infant mortality under 5 is 5560 per 100,000. 81.6 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Zambia:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– the law mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 124, and there is some progress.
Gender in Medicine
There has been a notable change in the number of women in medicine in Zambia, from one female medical student entering medical school about fifty years ago to some universities recording over 50% female medical student entry recently. Despite this great achievement we have great underrepresentation of women at the leadership level in the health sector in general. Over almost sixty years of independence, there has been no female doctor who has ever served as Minister of Health. Those doctors that have been ministers are male. Zambia has ten provinces: all provincial health offices are headed by male doctors. It is almost the same picture at the district level, where we have less than 10% representation in the 110 districts. Women remain underrepresented at the various levels of leadership in the health sector in Zambia in research, academia and hospital management.
On the other hand, in the private sector, including private hospitals, non-governmental organisations and international organisations, female doctors are heading these organisations, some with more than 100 employees. One of the reasons women abstain from leadership positions in Zambia is because workplace policies do not support the parental and family roles that women have. Women are slowly getting more support from partners in our society but women in leadership roles need more than just supportive partners. Our workplace systems need to be more inclusive and diverse for us to see a meaningful change. Women in the health sector in Zambia continue to be underrepresented in positions of authority. They are merely restricted to lower ranks of management.
A recent study showed that firms with female CEOs experience 48.3% less sexual harassment. An increase of one female director is associated with a 18.2% decrease in the sexual harassment rate. (Reference Au, Tremblay and You3) Of course, more is involved in reducing sexual harassment in workplaces. Increasing female leadership in the health sector is one way to start through deliberate collaborative and innovative leadership.
Medical Education
For a long time, there was just one public medical school in the country, but in the recent past we have seen an increase in the number of both public and private medical schools. The duration of training for a medical doctor varies between six and seven years depending on the institution. There are also a number of medical students that train in other countries like China and Russia, after which they come back home to practise medicine. The faculty under these universities are responsible for assessing competencies both at undergraduate and postgraduate levels. All newly trained and inducted medical doctors have a mandatory one-and-a-half-year internship as junior resident medical officers. On completion they may choose to undergo specialty training for another four years on average in their field of choice or remain as general medical officers. Certain fields tend to attract more women for specialisation, like paediatrics, and obstetrics and gynaecology, although the overall number of males is always higher. Other than a few private hospitals and non-governmental organisations (NGOs), the government, through the Ministry of Health, is the main employer of all medical doctors in Zambia. However, at the hospital level, the hierarchy in the department starts with the head of department, consultants, senior registrars, registrars, then the interns, and learning in the clinical environment is by apprenticeship. Therefore, the seniors play a major role in the career progression of the junior colleagues because they impart skills and knowledge, and complete the appraisals of students and junior doctors’ performance, in the form of logbooks. This, unfortunately, means doctors in junior positions, including students, are vulnerable to hierarchical abuse. Culturally, a junior may never offer criticism or any form of feedback to the superiors regarding their clinical learning environment for fear of jeopardising their career progression. Even though there no actual studies to indicate the level of abuse in the Zambian context, other studies have found that inappropriate behaviour, harassment, and belittlement of physicians-in-training was perpetrated mostly by fellow physicians in superior positions. (Reference Szafran, Woloschuk, Torti and Palacios Mackay4)
Law
Zambia has laws which prohibit sexual harassment in the workplace. These are the Gender Equity and Equality Act no. 22 of 2015, the Anti-Gender-Based Violence Act no. 1 of 2011 and the Penal Code. These acts provide criminal and civil sanctions. (5) The law generally deals with cases of sexual harassment very seriously, as the offence has a very strict punishment with a minimum of three years’ imprisonment and a maximum of fifteen years’ imprisonment. However, the evidentiary rules in offences of a sexual nature are quite onerous as they require corroboration. The evidence of the victim has to be corroborated by independent evidence which tends to establish the identity of the perpetrator and the commission of the offence. These corroborative rules are in place to guard against the danger of false implications. These rules are onerous as most incidents of sexual harassment occur in private, and in the absence of evidence such as text messages or an eyewitness it becomes difficult to prove a case beyond reasonable doubt.
There are specialised police, prosecution, and judiciary departments mandated to deal with cases of sexual harassment; however, the evidentiary requirements are the major impediment that may lead to perpetrators not being charged. Victims can receive support from One Stop Centres, which offer multi-disciplinary support in the form of counselling and legal advice. The police and the prosecution service also provide counselling and legal support as do non-governmental organisations. There are risks of retaliation and further harassment on a victim who reports, as most institutions both private and public do not have safety mechanisms that protect a victim from backlash. The medical doctors do not have an institution mandated to defend them in civil or criminal cases nor do they have insurance which would cover such costs. Women who report sexual harassment are often viewed as weak or are blamed for having seduced the man, for example, by their way of dressing. Additionally, many panels to resolve such issues are led by men who are less knowledgeable about sexual harassment.
Medical Regulation
In order for medical doctors to practise in Zambia, they have to register with the Health Profession’s Council of Zambia (HPCZ). The Council has the mandate to register and regulate all health facilities in Zambia, both public and private, and training institutions teaching health sciences. The HPCZ is a statutory regulatory body established under the Health Professions Act No. 24 of 2009 of the Laws of Zambia. The functions of the HPCZ as enshrined in the Act, among others, include the registration of health practitioners and regulation of their professional conduct. (6)
Professional misconduct may warrant disciplinary action, as spelt out in the organisation’s ethical code of conduct which states in part that personnel (health practitioners) exhibiting dishonest behaviour or corrupt practices, and indecent or violent behaviour, may lead to disciplinary proceedings even if the offence is not directly connected with the health practitioner’s profession. Some of the disciplinary measures include cancellation of registration, censure or counsel to the practitioner or otherwise imposition of fines. (7) Clearly there is no mention of sexual harassment of colleagues in this document. The role of colleagues and other professional bodies is not clearly spelt out in how an erring member should be disciplined. On the progressive side, the Public Service Management Division (PSMD), which is the regulator of all public workers doctors, including doctors, has recently revised the disciplinary code and procedures for handling offences in the public service, as of May 2023. Any form of sexual harassment on first breach results in instant dismissal from public service. (8)
Case Report
Prelude
Following ethics approval (#1652–2021), a survey using Google form documents that did not capture any personal information or identifiers was sent to the membership of the Medical Women Association of Zambia. Eight responded to the questionnaire and reported to have experienced sexual harassment, which happened between one to more than ten years ago. The sexual harassments which have been experienced by the survivors include inappropriate texting (3), inappropriate touching (3), inappropriate comments (7), physical contact (2) and rape (1). Three of the survivors are currently working in the same department as the perpetrators. Only one perpetrator was the same rank as the survivor, while the rest of the perpetrators were senior to the survivors at the time of the harassment.
Most survivors attributed organisational culture, followed by social context and personal vulnerabilities, as factors they thought contributed to the sexual harassment. Below are quotes from the survivors’ perspectives on what they consider put them at risk of such horrendous acts.
I’m not an assertive person … S1
He said it was what others were doing … S2
I am not sure why they felt they had to do that. I thought we had a professional and cordial relationship … S3 (this survivor experienced two different sexual harassments by two different doctors)
They appeared to use their connection to a much senior doctor … S4 (perpetrator thought the woman would comply because it gave her a point of connection with a senior doctor)
The comments and texts started in the workplace. Apparently, it was normal to talk about a woman’s body like just any other object and the jesting was perceived as normal … S5
According to ‘research’ he sleeps with every beautiful girl at work … S6
Seniors know juniors can’t report them for such, if they do it’s his word against mine … S7
He was going to sign my internship logbook for me to go for specialty training … S8
The Assault
Here we highlight the narratives given by two of the survivors.
One of the respondents (S5) narrated this.
In my unit at work, we planned a party to relax and socialize outside the work environment. One of the male doctors offered to host this party at his house. However, at the end of the party, I thought that I had drunk a little too much and was unsure I would drive home safely. The party host offered that I could spend a night at their house and go home the next day when sober. I woke up in the middle of the night and couldn’t believe what was happening; he was right on top of me, having penetrative sexual intercourse without my consent. I cried myself to sleep as I let him finish what he was doing. He raped me!!! Initially, I thought it was my fault because I had too much to drink, but then being in the company of people I knew, I thought I was safe and let my guard down. When I confronted him about it somehow, he turned it around to say I was to blame; I led him on.
However, this was plain simple: it was rape.
The second survivor (S6) explained an incident as having brewed from ward rounds.
He (head of the department) started making advances on the ward telling me how beautiful I am in front of everyone … I thought it was a joke … I never cared.
At the end of each rotation, junior residents get signed out before rotating through another specialty. As this junior officer went to the head of department’s office to be signed off, he grabbed her and started touching her breasts and asked for sex; but she found a way to escape and never looked back.
Limbo
An analysis of the responses reveals an alarming trend of systemic sexual harassment by male doctors of female doctors who were in the majority of the cases subordinates of the perpetrators. More than half of the respondents considered reporting the case; however, only two did report. Reports were made to the immediate supervisor and to the Ministry of Health. In both cases nothing came out of the reports, one respondent was told that it was normal for new young doctors to be approached by seniors and in the second one the complaint report went missing. There were no sanctions, nor was accountability meted out on the perpetrators for the reported cases. The only satisfaction that respondents got from reporting was that they experienced no further acts of harassment.
The major challenges faced by the respondents which prevented reporting were fear of reprisals and of being labelled difficult, in addition, respondents thought they would not be believed. Previous attempts by other female doctors to report had resulted in the whole hospital knowing of the incident: the lack of confidentiality and protection against retaliation were major deterring factors for non-disclosure. Other key considerations were that respondents did not want to create work tensions with perpetrators with whom they still had to work. Moreover, the lack of documented evidence of incidents of harassment contributed to the non-reporting, as respondents believed their word alone would not suffice. Knowledge of whom to report to was not known to all: only half of respondents knew where to go. Some respondents hoped for the incidents of sexual harassment to naturally go away, and half of the respondents stated that they did not have the personal strength to report as the process of doing so would be cumbersome and emotionally draining.
Exposure
Two of the survivors reported that they had experienced retaliation from the perpetrators and colleagues. And as a result, the survivor had to leave that hospital and find employment elsewhere. Three survivors had actually experienced thoughts of how they would cope with a sense of betrayal in the event that colleagues talked about them, and one of these narrated that she did not care only for her career. On the other hand, another survivor narrated the ordeal her friend went through when she reported a rape case at her institution, and we infer here that this friend unfortunately did not participate in our current survey, and hence we cannot comment on the specifics of the experience. This loss of anonymity and gossip has some repercussions on how the survivors would cope with the sense of betrayal. This survivor did not report her case, and she does not think she would recommend anyone to report a rape case at her hospital.
The social stigma and backlash can be worse than the event itself. I think part of my healing was because I wasn’t reminded of it every day by random strangers.
None of the survivors in this survey ever thought they needed to respond to critics or people talking about them if it came to light that their cases were exposed. One of the survivors alluded to thoughts of self-blame and said people have often misunderstood her friendliness. On the contrary, another survivor knew she would be criticised but the critics would not be correct to blame her for being female around men who are ill mannered. Some of the survivors did consider how they would cope working in an environment amidst the gossip and would have preferred to get a transfer. While another actually moved:
yes, I moved, ran away from all. It’s almost as if I was spoiling things for everybody …
Aftermath
After the incidents, the respondents expressed different feelings; some respondents felt the incident made them stronger. ‘I feel strong as I had a clear plan on how to gather evidence about the harassment and to report it.’ Another one responded, ‘A strong doctor.’ There was self-blame as well. ‘I always think I am a coward. I should have fought.’ Not reporting the incident meant they could go on without anybody knowing.
The impact the incident had on their personal and professional life was profound. It has led to suspicion and mistrust of male colleagues: ‘I am suspicious of male colleagues. I always prefer to work with female doctors on projects.’ A loss of respect as well:
Each time I work with a different male senior I am very closed up and scared he might be another individual to harass me. Meeting the perpetrators at work makes me have negative feelings towards them and I don’t respect them anymore.
Avoidance of male colleagues as well: ‘I am distant with male colleagues, and I am not usually comfortable in situations where I find myself alone with a male colleague.’
Respondents also described recovery in various ways that meant some state of forgetting, forgiveness or feeling comfortable about themselves and feeling comfortable in the company of male colleagues. Agonisingly, some have failed to recover. One described recovery as ‘Not happening as I see him with his smirk on his face.’ Others reached a place of recovery through counselling and prayer. Sadly, most have not fully recovered, and this remains a work in progress. Some respondents have used their experience to counsel others and raise awareness on the issue, seeking the benefit of others.
Discussion
The enactment of the Gender Equality and Equity Act, 2015 (No. 22 of 2015) was a key milestone in the progress towards gender equality and equity. Additionally, Zambia first adopted the National Gender Policy in 2000, and this was reviewed in 2014. This is great progress towards the elimination of sexual harassment in the workplace. The Gender Equity and Equality Act prohibits sexual harassment. The Employment Code, under the provisions of section 95(1), makes it mandatory for the employer to have a policy on harassment. (9) The key findings from this case study are that perpetrators of sexual harassment in the workplace among female doctors are mainly superiors, it is underreported, and the few reported cases yielded no repercussions on the perpetrators.
Medicine is dominated by males, and they hold most of the leadership positions. We found that most of the respondents were harassed by their superiors, people they held in high esteem due to the hierarchical nature of the field. Heads of department should be go-to people when sexual harassment has occurred; however, we found that they are key perpetrators themselves. So where do women run to? Female-led organisations have reported reduced rates of sexual harassment. (Reference Au, Tremblay and You3) The lack of clear work policies on sexual harassment to protect and support women has been a major barrier to prevention and supporting the survivors. The perception that sexual harassment is normal, as was seen with some of the responses, is wrong. Perpetrators and the so-called channels of communication, most of which are unfortunately headed by men, attribute the blame to the survivor, which they must then carry. A female reporting sexual harassment is shamed by society and this is a major hindrance to reporting: women feel like there is no point in reporting as they will just be exposed and blamed.
Zambia has been progressive in fulfilling its obligations to prevent discrimination against women by enacting laws which provide protection both in the private and public spheres. Despite these efforts, implementation of these laws has not been comprehensive or widespread, thus leaving women vulnerable to sexual harassment. Very few institutions, both private and public, have implemented the provisions of the law relating to workplace sexual violence. The public service, which employs most of the female doctors, recently revised its disciplinary code and procedures for handling offences; (8) however, they have not incorporated protective measures against retaliation, to appoint designated sexual harassment focal point persons to whom victims can report in a confidential manner and to enforce strict penalties against perpetrators. This inadequacy can be seen from the responses in the survey. Further, the prohibitive corroborative rules on sexual violence also deter victims from reporting as victims often do not have evidence of the harassment apart from their word.
In order to remedy these shortcomings, there is a need to have workplace sexual harassment policies in both the public and private sectors brought into conformity with the law. These policies should provide for confidential reporting, protection of victims and accountability of perpetrators. This should also be coupled with the corroborative evidentiary rules in the criminal justice sector being relaxed to encourage more victims to report cases to the police for prosecution.
From preliminary discussions with male colleagues, the first step in winning this fight is psychoeducation. The male doctors in Zambia seem unaware of what sexual harassment is for starters and only think it is recognizable when an overt request for sex is made, if there is physical touch, or worse still, when rape occurs. This is heartbreaking, to say the least. In addition, the impact is even less acknowledged. Perpetrators either have no knowledge or are dismissive of the impact of sexual harassment. The fact that it infringes on the career progression of the much-needed medical doctor in a nation where we still lack enough medical staff is tragic. It is also counterproductive to all the efforts being made to empower women at workplaces.
Sexual harassment results in mental health problems such as depression, anxiety, insomnia, post-traumatic stress disorder, low self-esteem, poor concentration, poor interpersonal relationships, anger outbursts and substance abuse. (Reference Adler, Vincent-Höper, Vaupel, Gregersen, Schablon and Nienhaus10–Reference Friborg, Hansen, Aldrich, Folker, Kjær, Nielsen, Rugulies and Madsen12) Sexual harassment also has a negative impact on work, resulting in absenteeism, demotivation, poor engagement, disintegration of teams, (13; Reference Dobbina and Kalevb14) transfers even to areas where staff might be less skilled or less passionate to work, and resignation. In addition, there has been an association between sexual harassment and the development of physical problems such as headache, dizziness, sleep disturbances, physical exhaustion, poor appetite, stomach-aches, and weight changes (both weight gain and loss). (9; Reference Gebregziabher Kahsay, Negarandeh, Dehghan Nayeri and Hasanpour15)
There is a need for mass psychoeducation and training sessions to improve the picture for women, because currently, such types of training are not readily available. These trainings should be targeted at both male and female physicians. It will help us get to a place where recognition of the impact is acknowledged. Recognition that sexual harassment negatively impacts wellbeing is insufficient without follow-up care interventions for the victims. This is vital. As discussions and training on sexual harassment begin, they tend to cause victims to experience re-traumatisation. Therefore, interventions should include readily available psychosocial support for victims in order to have an effective and comprehensive intervention. These interventions can include group therapy, brief interventions, individual therapy, and trauma-focused counselling.
The level of sensitivity to sexual harassment by an organisation determines the policies that are put in place. There has been notable general awareness of gender issues in Zambia. It has been noted that male-dominated professions report more sexual harassment against females. Thus, it is paramount for the Ministry of Health, which is the main employer for doctors, to define sexual harassment for its personnel. Strong policy statements of no tolerance of sexual harassment should be made by the Ministry of Health. Orientation of new staff must include education on sexual harassment for both female and male workers. Once workers understand what constitutes sexual harassment, it is easier for them to avoid sexual harassment behaviours and understand reporting mechanisms. The Ministry of Health should also develop strategies to provide support to victims of sexual harassment, like retaliation and counselling.
The Medical Women Association of Zambia (MWAZ) is the only association that focuses on providing a voice to address the interests and concerns of medical women and students. The Association represents an important platform through which membership can leverage opportunities and address challenges that influence their individual and professional development, with the ultimate goal of increasing medical women’s ability to positively impact the Zambian health care system. Issues regarding sexual abuse of female doctors working in Zambia are part of the core business of MWAZ. The association needs to ensure their members are working in a safe environment free from sexual abuse.
The most important role for MWAZ is to ensure the presence of sexual harassment policies in all workplaces in the health sector. The policies must be clear in definition of sexual harassment, and provide a clear reporting channel which protects the victim from retaliation. Currently, MWAZ, in collaboration with the Zambia Medical Association (ZMA), has made marked progress in formative works that are fundamental in the development of the policy document on sexual harassment of doctors. Support for the victim after the incident in the form of counselling must be assured. Periodic anonymous surveys with standard validated tools which can be adapted to the local context should be implemented to understand where and how sexual harassment is occurring and come up with strategies to curb it. More women should aspire and acquire the necessary skills to take up leadership roles.
Female medical students are affiliate members, and awareness of sexual harassment needs to start at the student level. A clear definition of sexual harassment must be taught to students. Orientation on sexual abuse in the workplace at induction into the medical field must be done. Further ongoing training on what constitutes sexual harassment among all members and affiliate members is key and should be done. MWAZ must have a committee on sexual harassment which ensures policies exist in workplaces and acts as an alert system for all female doctors who experience sexual harassment. The association must collaborate with associations with legal experts should legal redress be required. Only when female doctors work in a safe environment can they attain their full potential.
Sexual harassment is costly to the individual and the organisation. Robust training for both male and female doctors is required to break what has been described as an entrenched organisational culture of sexual harassment. Female doctors continue to be vulnerable to sexual harassment by male doctors due to many factors. The impact spans from reduced self-esteem and mental trauma to reduced productivity and change of career plan as the work environment is perceived as unsafe. Our reflection on the current situation of sexual harassment and abuse of women doctors in Zambia would be incomplete without including the perspectives from survivors on making workplaces safe for female doctors. Respondents recommended sexual harassment and violence workplace policies, highlighting raised awareness, a well-defined channel of reporting that is easily accessible to all doctors, confidentiality, action against perpetrators and support for victims. It is therefore important that the employer protects the employee from sexual harassment.

 Open access
Open access