


Introduction and background
National Health Service (NHS) Talking Therapies (TT) (formerly known as Improving Access to Psychological Therapies, or IAPT) is a programme that provides both high and low intensity evidence-based therapies, primarily for anxiety and depression, within the NHS in England (NHS, 2023a). The programme began in 2008, and approximately 1.9 million people are referred per annum, with 1.2 million people accessing treatment, and 671,000 completing a course of treatment (NHS, 2023b). It forms a key part of the NHS Mental Health Implementation Plan (Murdoch et al., Reference Murdoch, Farmer and Cumiskey2019), the NHS Five Year Forward View for Mental Health (Farmer and Dyer, Reference Farmer and Dyer2016), and the NHS Long Term Plan (NHS, 2019), and is underpinned by NICE guidelines (NHS, 2023a).
Referral into TT takes place via four main pathways: self-referral, community/voluntary service referral, primary care referral, and secondary care referral (NHS, 2023a). High intensity therapy, or Step 3 therapy, typically consists of 12–20 weekly sessions of standard cognitive behavioural therapy (CBT), undertaken by a high intensity therapist. Low intensity therapy (Step 2) is briefer, is administered in a variety of formats including CBT by psychological wellbeing practitioners, and typically consists of up to six weekly sessions (Martin et al., Reference Martin, Iqbal, Airey and Marks2022; Shafran et al., Reference Shafran, Myles-Hooton, Bennett and Öst2021).
Personality difficulties are persistent patterns of emotional, cognitive, and behavioural responses that deviate from social norms and lead to challenges in functioning. Unlike personality disorders, which are more severe, personality difficulties may still cause distress but not to the extent of a full personality disorder (Tyrer and Johnson, Reference Tyrer and Johnson1996). Prior research has shown that personality difficulties are a common co-occurrence in those with depression and anxiety disorders (Lamph et al., Reference Lamph, Baker, Dickinson and Lovell2021). A high prevalence of personality difficulties has been identified in high intensity TT populations; in a study of 3689 individuals attending high intensity treatment in SW England, Mars et al. (Reference Mars, Gibson, Dunn, Gordon, Heron, Kessler, Wiles and Moran2021) found that over 80% endorsed three or more personality difficulties (placing them at ‘high risk’ of being diagnosed with a personality disorder).
Furthermore, personality difficulties may be associated with poorer treatment outcomes for anxiety and depression (Martin et al., Reference Martin, Iqbal, Airey and Marks2022; Newton-Howes et al., Reference Newton-Howes, Tyrer, Johnson, Mulder, Kool, Dekker and Schoevers2014), even when accounting for demographic variables and baseline symptom severity (Goddard et al., Reference Goddard, Wingrove and Moran2015). Specifically, the likelihood of recovery and reliable improvement appears to be reduced among those with personality difficulties, regardless of treatment type (Mars et al., Reference Mars, Gibson, Dunn, Gordon, Heron, Kessler, Wiles and Moran2021). Appropriate training and supervision for staff on the assessment and treatment of individuals with personality difficulties may therefore be particularly important to optimise treatment outcomes (Goddard et al., Reference Goddard, Wingrove and Moran2015).
With this in mind, we developed and delivered an online educational workshop (led by co-author B.D.) to enhance the skills, knowledge, and confidence of therapists in treating clients with concurrent personality difficulties. The workshop was delivered by two experienced CBT trainers and had three over-arching aims: (1) to provide up-to-date education about personality difficulties, including how these features relate to therapy outcomes and clinical guidance; (2) to build therapists’ skills, knowledge, and confidence in meeting the needs of clients when delivering CBT for anxiety or depression, including structuring sessions, managing the therapeutic alliance, and building client skills in emotional management; and (3) building resilience to support therapists in working with more complex clients, including validating therapist experiences. The underpinning vision of the workshop was to support therapists in finding flexibility within protocols while still adhering to the CBT treatment model. For a more detailed description of the workshop, please see the study protocol of Warbrick et al. (Reference Warbrick, Dunn, Moran, Campbell, Kessler, Marchant, Farr, Ryan, Parkin, Sharpe, Turner, Sylianou, Sumner and Wood2023).
Aims and objectives
We aimed to assess the acceptability and potential utility of the workshop for therapists, and to determine the effectiveness of the workshop on improving treatment engagement and clinical outcomes of clients with depression/anxiety and concurrent personality.
Method
Study design
We used a mixed-methods design incorporating three components: (1) a pre–post non-randomised quantitative study of client outcomes, using routinely collected pseudonymised data collected by all TT services; (2) a cross-sectional online survey of therapists who attended the workshop; and (3) semi-structured qualitative interviews with a purposefully selected sample of therapists.
Study populations and recruitment
The study took place in a single NHS-TT healthcare provider in Southwest England (Vita Health Group, 2024). Managers at the provider were initially engaged to secure staff engagement in the workshop and associated study. The client population were Step 3 (high intensity) CBT clients of the Bristol TT service, with common mental disorders (mild to moderate depression and anxiety disorders) who were accessing treatment during the 6-month period pre- or post- therapist training. These patients could have started treatment prior to the period, but only those sessions falling within the study period were used.
Quantitative data on client outcomes
The workshop was run in two sessions in Bristol in October 2022, and was offered to all 90 practitioners working within the service, of whom 46 attended (51%) and completed the survey. The first workshop session was held on 12 October 2022, and the second session was held on 19 October 2022. Clients were included in the analyses of outcomes, if they were over 18 years, had a gender recorded, attended at least two sessions, and were included in the existing routinely collected clinical dataset. Clients were excluded if they had opted out via the NHS opt-out of the use of their data for research as per the service’s data protection policy.
We obtained standardised, routinely collected, pseudonymised high intensity sessions data on symptom scores and demographic data on 4861 high intensity clients who had been treated in the 6 months before or 6 months after the workshop. Therefore, the study data on clients covered those whose treatment commenced between 19 April 2022 and 19 April 2023. Our data extract included episodic data for each client treated within this period. The data extract also included data as far back as their first encounter with the service, as well as up until the end of their treatment, even if it was after the 6-month window. We did not receive data on whether clients had been ‘stepped up’. The client data were divided into two mutually exclusive cohorts, based on the training date of 19 October 2022. The first cohort (termed ‘pre-training cohort’ in the Results) contained 2273 clients who were seen in the 6 months prior to the training, and the second cohort of 2197 clients (termed ‘post-training cohort’ in the Results) were seen in the 6 months after the training. Clients who had treatment overlapping the training end date were allocated to the first cohort, therefore outcomes were assessed for these clients until the end of treatment. Clients who were treated post-training were also followed up to the end of their treatment. For 991 clients in the post-training cohort, their end of treatment scores were completed before 19 April 2023. For 1206 clients in the post-training cohort, their end of treatment scores were completed after April 2023 and this included a period of up to 1 November 2023.
Not all clients are assessed on all outcomes in each session, and some questionnaires, such as the phobia scale, are not applicable for all clients. Three clients were removed from the study dataset as their gender was unknown, 322 were removed as they only attended one session, and 66 were removed as they were under 18 years old, leading to a total sample size of 4470. We linked these data with employee data from TT on therapists, to allow us to adjust for therapist characteristics in the client outcomes analysis. The therapists were linked to the clients via a therapist identifier. However, the provider was unable to link information on whether therapists attended the training to the therapist dataset. The therapist survey results could not be linked to the client dataset due to the anonymity requirements of research ethics.
Quantitative data on staff attitudes
Managers at the provider were asked to send the staff survey two weeks prior to the training start date, and a post-training survey was later distributed automatically by the REDCap system, after the training had been completed on 19 October 2022. Study data were collected and managed using a REDCap survey hosted at the University of Bristol. The REDCap system is a secure data collection platform (Harris et al., Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde2009; Harris et al., Reference Harris, Taylor, Minor, Elliott, Fernandez, O’Neal, McLeod, Delacqua, Delacqua, Kirby and Duda2019), which also facilitates the consent process. Informed consent was taken via REDCap. Therapists were excluded from the survey if they did not intend to attend the online workshops.
Forty-six therapists participated in the survey, of whom 63% completed both pre- and post-training data collection points (n=29). Staff were asked to provide basic categorical demographic information, their years of experience, and to complete attitudinal measures about the management of clients with personality difficulties on a 5-point Likert scale (strongly disagree–disagree–neutral–agree–strongly agree). A copy of the attitudinal measures can be found in the Supplementary material (File 1). After the training, in addition to the attitudinal measures, staff were also asked to rate the value of the workshop on the same Likert scale, which provided a quantitative assessment about whether the training was deemed acceptable. In a related study, Warbrick et al. (Reference Warbrick, Dunn, Moran, Campbell, Kessler, Marchant, Farr, Ryan, Parkin, Sharpe, Turner, Sylianou, Sumner and Wood2023) defined a threshold of 60% or more of therapists answering agree/strongly agree on these items, as being indicative of acceptability, and we adopted an identical threshold in this study.
Qualitative data from staff
Qualitative interviews were conducted over the telephone, on MS Teams or Zoom, following University of Bristol guidelines, dependent upon the preferences of the interviewee.
Six staff participated in individual qualitative interviews. A semi-structured topic guide focused on the acceptability and usefulness of the workshop to therapists, and the impact of the workshop on how therapists engaged with clients. Following verbal recorded informed consent, interviews were audio recorded, transcribed, anonymised and analysed. Additional qualitative data were sourced from the follow-up staff survey after the training, with open-ended questions asking about how therapists found the workshop, what could be improved and what they might do differently because of the workshop, with a space for any other comments.
Data analysis
Quantitative data analysis
For the client outcome data, we examined the differences within each cohort on the following clinical outcomes:
-
(1) Depressive symptoms (Patient Health Questionnaire, PHQ-9) (Kroenke et al., Reference Kroenke, Spitzer, Williams and Löwe2010); higher scores (ranging between 0 and 27) indicate more severe depression.
-
(2) Anxiety symptoms (General Anxiety Disorder-7, GAD-7) (Toussaint et al., Reference Toussaint, Hüsing, Gumz, Wingenfeld, Härter, Schramm and Löwe2020); higher scores (ranging between 0 and 21) indicate more severe anxiety.
-
(3) Social functioning (the Work and Social Adjustment Scale, WSAS) (Mundt et al., Reference Mundt, Marks, Shear and Greist2002; Zahra et al., Reference Zahra, Qureshi, Henley, Taylor, Quinn, Pooler, Hardy, Newbold and Byng2014); higher scores (ranging between 0 and 40) indicate higher levels of impairment to functioning due to a specified condition.
-
(4) Specific phobia symptoms (Marks and Matthews, Reference Marks and Matthews1979); higher scores (ranging between 0 and 24) indicate higher avoidance of outlined situations, which include: ‘social situations due to a fear of being embarrassed or making a fool of myself’; ‘certain situations because of a fear of having a panic attack or other distressing reaction,’ and ‘certain situations because of a fear of particular objects or activities’.
It is important to note that routinely, in NHS TT services, the specific questionnaires that clients are asked to complete are based on their clinical needs, and therefore, not all clients complete all measures. Therefore, denominators for the symptom outcome domains varied. For each outcome, within each cohort, the last recorded score within a given cohort was subtracted from the first recorded score to obtain a within-cohort change (difference) in score. These differences were censored at the end of treatment for both cohorts. To ensure that the pre-training cohort only included clients whose therapists had not been exposed to the training, we dropped individuals from the pre-training cohort if they completed their treatment after the workshop. The differences in the score change between cohort groups (difference-in-difference) were then compared. Cohort groups, i.e. whether a client had undergone treatment in the 6 months before the training, or in the 6 months after the training, was considered the main exposure in the model. An improvement in score is denoted by a negative coefficient, indicating a reduction in symptom score.
For each outcome, we specified multi-level linear regression models, with clients at level 1, nested in therapists at level 2. The final adjusted model included the exposure, which was cohort, and also gender, age, length of therapy in months, number of sessions attended, ethnicity, and therapist years qualified. Therapist years qualified was specified to vary at level 2, the therapist level. To ensure consistency in results, we analysed the null models on the same population as the adjusted models. We also calculated an effect size with Cohen’s d (Lakens, Reference Lakens2013).
The intraclass correlation (ICC), was calculated for each model. The ICC measures the degree of variability between individual therapists (Hox, Reference Hox2010). A low ICC can be interpreted as showing little difference in the outcome when a client is treated by any given therapist, i.e. the variation in the outcome between therapists is low. A higher ICC can be interpreted as a higher degree of variability between the therapists, i.e. there is a greater difference in the outcome when a client is treated by a given therapist and that therapists are more distinct from one another in terms of their client outcomes. All data were analysed using Stata version 17.
For the therapist survey results, mean and median responses to the items on the attitudinal scales were calculated and the presence of changes in staff attitudes were explored using the Wilcoxon signed-rank test (Kirkwood and Sterne, Reference Kirkwood and Sterne2002).
Qualitative data analysis
Initially an inductive thematic analysis approach was used to analyse interview transcripts and qualitative comments (n=29) from the staff survey, with 17% of interviews double coded, using NVivo software. These thematic results were then grouped according to the different elements of capability, motivation and opportunity, in line with one of the key models that the training was based on – the behaviour change wheel (Michie et al., Reference Michie, van Stralen and West2011; Warbrick et al., Reference Warbrick, Dunn, Moran, Campbell, Kessler, Marchant, Farr, Ryan, Parkin, Sharpe, Turner, Sylianou, Sumner and Wood2023). Broader contextual issues that arose through the thematic analysis were then categorised according to intervention functions and policy categories as set out in the behaviour change wheel (Michie et al., Reference Michie, van Stralen and West2011). Capability, opportunity, and motivation (the ‘COM-B’ system) forms the hub of the wheel, with nine intervention functions and seven categories of policy that could enable those interventions (Michie et al., Reference Michie, van Stralen and West2011).
Results
Client outcome data
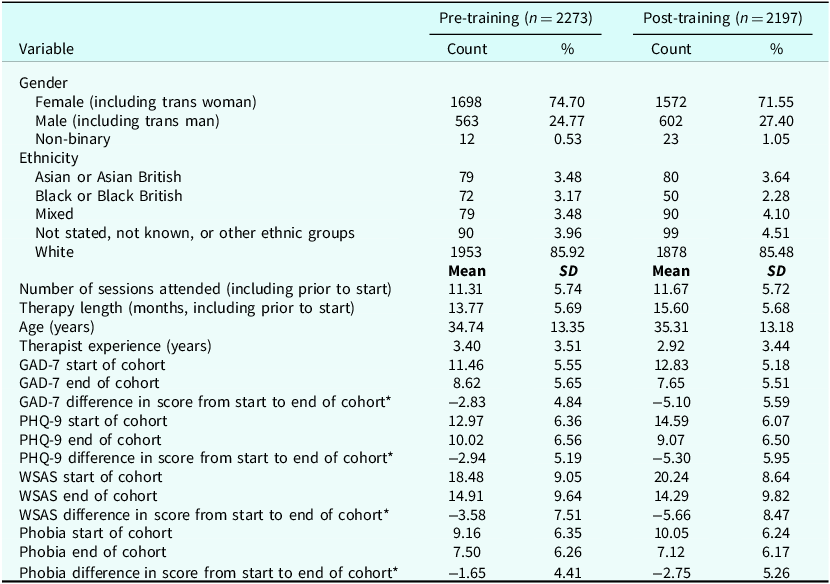
In both cohorts, the majority of clients were white and female (including trans women; Table 1). The mean client age was 34.74 years (SD 13.35) in the pre-training cohort and 35.31 years (SD 13.18) in the post-training cohort. Clients in the pre-training cohort attended a mean of 11.31 sessions (SD 5.74) and in the post-training cohort, mean attendance was 11.67 sessions (SD 5.72). In the pre-training cohort, the range of treatment was 2–38 sessions (median number of sessions: 11; IQR of 7–15). In the post-training cohort, the range of treatment was 2–30 sessions (median number of sessions: 12; IQR of 7–16).
Descriptive statistics of pre-training and post-training cohorts; cohorts are mutually exclusive

* The difference in score is calculated for each individual client in the dataset, from first and last measured scores in the defined cohort time period. Therefore, the number represents the mean of the differences in individual scores, rather than the difference between the overall mean scores at the start and end of the cohorts.
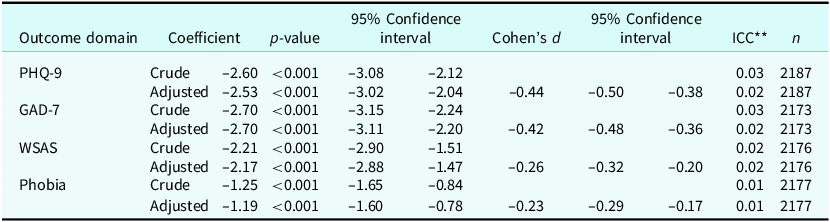
Table 2 shows the final adjusted regression coefficients for each outcome, as well as Cohen’s d, a measure of effect size, calculated for the final adjusted models. There was a –2.53-point difference (95% CI –3.02, –2.04, p<0.001) in the PHQ-9 score change between the pre-training and post-training cohort, adjusted for age, gender, ethnicity, length of therapy (months), number of sessions attended, and years of therapist experience. The associated effect size was –0.42 (95% CI –0.50, –0.38). Furthermore, we detected a –2.70-point difference (95% CI –3.11, –2.20, p<0.001) for GAD-7 score change between the two cohorts, with an associated Cohen’s d of –0.42 (95% CI –0.48, –0.36). There was a –2.17-point difference in score (95% CI –2.88, –1.47, p<0.001) for the WSAS, with an associated effect size of –0.26 (95% CI –0.32, –0.20). Similarly, there was a smaller –1.19-point difference (95% CI –1.60, –0.78 p<0.001) in the phobia score change between the pre- and post-training cohorts. For phobia, the associated effect size was –0.23 (95% CI –0.29, –0.17).
Null and adjusted* estimates for the multilevel difference in difference models for the cohort effect

* Model adjusted for gender, age, length of therapy in months, number of sessions attended, ethnicity, and therapist years qualified, varying at level 2. ** ICC, intraclass correlation.
Staff survey – quantitative findings
Forty-six therapists both attended the workshop and responded to the survey. Seventeen therapists only completed the survey before training and were therefore excluded from the pre–post analyses. The majority of therapists were female (73.9%), white (89.1%), and had eight years or more of experience (43.5%).
For therapists who responded to surveys at both time points, there were significant differences (p<0.001) between mean scores on questions relating to the appropriateness of managing clients with personality difficulties in the TT setting, measures of confidence in anticipating necessary relationships and therapeutic alliances, and managing emotional and interpersonal features of clients with personality difficulties (see Fig. 1). More detailed information on therapist responses can be found in the Supplementary material (File 2).
Mean therapist responses to attitudinal measures of personality difficulties, pre- and post-training, with 95% confidence interval; *p-value of Wilcoxon signed rank <0.05; **p-value of Wilcoxon signed rank <0.001.

For ratings of the workshop itself, all items, bar one, had mean ratings of 4 (agree) or above on clinical usefulness, presentation, theoretical interest, and recommendation to other IAPT therapists (see Fig. 2). The item on application of the workshop to their own practice had a mean rating of 3.9 (i.e. just below cut-point for ‘agree’); however, more than 60% of therapists agreed or strongly agreed with each item on the feedback survey. This indicates that the workshop is acceptable.
Therapist workshop rating (only taken post-training).

Staff – qualitative findings
Results are presented using the behaviour change wheel as thematic categories (Michie et al., Reference Michie, van Stralen and West2011). File 3 of the Supplementary material outlines the different aspects of the wheel explicitly, detailing capability, motivation and opportunity, and broader contextual influences, with example quotes from the interviews and staff survey.
Therapists reported that as a result of attending the training, they had enhanced their understanding of personality difficulties. They felt more confident about the knowledge and skills required to build a positive relationship with clients who had personality difficulties, as well as more confident in their ability to manage therapeutic ruptures and building clients’ interpersonal effectiveness. Staff were also positive about the impact of training on multiple components of treatment, specifically: building clients’ emotion regulation skills, setting boundaries, focusing on clients’ strengths, acknowledging past trauma, undertaking a formulation and managing the end of therapy:
‘That’s a change in my practice that I’ve started to implement already, so from session one or two I may identify relationship difficulties and say, “I’m always going to do my best for you in your therapy, but I’m a human being so I may not always get it totally right” … I’ve found that that’s been a nice way to open up the discussion and let them know that it’s okay to address those things and to discuss it, rather than, “Oh, it’s a rejection. The relationship is ruined”, and then have to drop out of therapy.’ (Interview 01)
In terms of changes in practice, five respondents reported interacting differently with clients in response to the training, leading to positive outcomes:
‘Well, the two people I’m thinking of, it’s been really good because they both went into recovery … they’ve been able to make progress with some of their wider goals with what they want in their lives, and move into some more independence … I think that’s been useful.’ (Interview 06)
Although some staff reported finding training very helpful, this was not unanimous, and others reported that they were still not confident in managing clients with personality difficulties:
‘I have left the workshop feeling as though I have access to a lot of useful information however still not entirely convinced that I have the skills to be able to successfully administer a piece of CBT to someone presenting with traits of a personality difficulties.’ (Survey 11)
Some respondents felt that treating clients with co-occurring personality difficulty was clearly ‘within remit’ of their work and acknowledged that these clients were already being seen. Yet there were also concerns expressed about the capacity of therapists to manage the needs of clients with personality difficulties:
‘Others have said, we still don’t think that we know what we’re doing. We still don’t have the tools that we need to do this personality difficulties work and is this actually the right place? Do we have the capacity for this?’ (Interview 05)
Others highlighted the need for more carefully tailored supervision in supporting them to manage clients with concurrent personality difficulties:
‘Typically supervision is not restorative in IAPT and there is a constant focus on targets, therefore taking on more complexity adds to burnout even if therapist implement good self care behaviours.’ (Survey 38)
The fact that all staff and managers joined the training together, was felt to be helpful. Some therapists were welcome of including clients with personality difficulties; however, there were also concerns about the appropriateness and capacity of the services to support these clients effectively:
‘We’re quite tight on getting people to follow models, and alarmed by therapist drift … some of what was being presented was about encouraging what isn’t necessarily following the model totally tightly because for this group it may not be the most effective thing for them and relying on your therapeutic judgement, and a part of me was like “oh god, this is a bit scary” because we’ve spent quite a lot of time really encouraging people to follow the evidence-base rather than the felt-sense.’ (Interview 03)
Whilst the workshop was designed to increase therapists’ knowledge and understanding and impart skills, qualitative data also highlighted the importance of wider interventions to enable appropriate treatment for clients with personality difficulties. These included developing the social context of IAPT work, for example enabling a more person-centred approach, and support for therapists to directly respond to the needs of clients with personality difficulties (Michie et al., Reference Michie, van Stralen and West2011). There were detailed comments on how IAPT services often demanded the following of protocols, and how much flexibility the service could allow, given the way the services have been set up and commissioned. Staff shortages and waiting lists were also mentioned in this context. The need for a broader range of therapies, and more time, and the fact that current performance measures may be inappropriate for clients with personality difficulties were also discussed:
‘IAPT services [are] predicated on short term therapy and with people with personality difficulties it has gone on years … Getting someone fully recovered in 12 sessions, it’s good luck with that one.’ (Interview 02)
In response to a question about whether the training should be rolled out nationally (asked in all interviews), five interviewees agreed, and one disagreed. Those who agreed saw the training as a helpful component of their professional development. Reticence about this related to ‘opening the floodgates’ (Interview 05) to clients with personality difficulties and concerns that the training might be a ‘sticking plaster’ (Interview 03) when more radical structural change may be needed within services.
Discussion and conclusions
In this mixed methods evaluation of a novel online staff training initiative, several key findings emerged. Firstly, the online training proved feasible to deliver and was highly acceptable for staff. The analysis of client outcome data indicated that the training initiative was associated with promising clinical effects on clients, with medium size effects on the domains of depression and anxiety and smaller, but still statistically significant effects on social functioning and phobic symptoms. The survey of staff attitudes indicated that the training was perceived by staff to enhance their clinical skills and confidence in managing clients with concurrent personality difficulties. The therapists’ perspectives of clients with personality difficulties improved after the training. This was particularly apparent in the attitudinal change in relation to whether TT was the appropriate service for clients with personality difficulties. The training was highly acceptable to therapists. Findings from the qualitative interviews mirrored these findings and also provided granular descriptions of how training had impacted multiple aspects of treatment, including setting boundaries, acknowledging past trauma, undertaking a formulation and managing the end of therapy.
Previous literature has suggested that in delivering CBT treatment for depression and anxiety, in clients with personality difficulties, the therapeutic relationship needs greater focus (Van Velzen and Emmelkamp, Reference Van Velzen and Emmelkamp1996). Our findings concur with this. In another study of clients’ perspectives about what was important in the treatment experience, having time to share emotional content, develop a therapeutic relationship and link past experiences to current problems were all highlighted as being key in determining successful treatment (Lamph et al., Reference Lamph, Baker, Dickinson and Lovell2021).
The staff we interviewed highlighted important constraints they experienced in working with clients with personality difficulties, including overly manualised treatment processes, a lack of appropriate supervision and performance measures that did not account for concurrent personality difficulties. These findings concur with other research conducted in primary care (Lamph et al., Reference Lamph, Baker, Dickinson and Lovell2019). Whilst the training attempted to tackle staff attitudes (Romeu-Labayen et al., Reference Romeu-Labayen, Tort-Nasarre, Rigol Cuadra, Giralt Palou and Galbany-Estragués2022), and a lack of skills and confidence in working with this patient group (Lamph et al., Reference Lamph, Baker, Dickinson and Lovell2019), wider contextual constraints limited the extent to which therapists were confident in working in this area. Tackling these contextual constraints and fully meeting the needs of clients with concurrent personality difficulties will possibly require the adoption of more flexible treatment protocols (allowing for more flexible and possibly longer courses of treatment), as well as the adoption of outcome measures capturing the complex emotional needs of clients with personality difficulties.
This study’s strengths include its use of mixed methods to allow for the triangulation of findings via multiple sources of data. The qualitative interviews allowed for a deeper understanding of the results obtained from the therapist survey. The routinely collected, validated client dataset allowed us to specify robust multi-level models, to account for potential therapist-level differences. However, the study also has limitations. In terms of the analysis of client data, we were unable to determine whether, for any individual client, their therapist had attended the training programme or not, as this was not recorded in the routine database. Notwithstanding, we adjusted for therapist experience in the statistical models and although this variable does not equate with attendance at the training, it did allow us to examine therapist-level effects on the outcomes. We used the WSAS total score in our analyses and in principle, this can be artificially lower for those who are unemployed. However, sensitivity analyses excluding individuals without scores in the work domain, revealed no change in the overall pattern of results. Furthermore, we were unable to characterise the personality status of the client cohorts. We had originally planned to include the SAPAS score (Moran et al., Reference Moran, Leese, Lee, Walters, Thornicroft and Mann2003) in the analysis, as these data are sometimes collected in clients. However, only 10% of the first cohort and 5% of the second cohort had recorded SAPAS scores. Yet, although the proportions with SAPAS data were small, in both cohorts, the mean SAPAS score exceeded 4, indicating that the cohorts were likely to include a sufficient proportion of individuals meeting the threshold for ‘high risk’ of personality disorder (Moran et al., Reference Moran, Leese, Lee, Walters, Thornicroft and Mann2003). Finally, as this was a non-randomised evaluation, we were unable to establish whether the differences in client outcomes were causally related to the training.
Clinical/future research
This mixed methods study analysed both client and therapist data to examine the acceptability and feasibility of a workshop developed to help TT therapists develop skills, confidence, and knowledge to work with clients with personality difficulties. The effects we detected on client outcomes should be replicated in further evaluations, ideally in the form of a randomised controlled trial. The training workshop is now being tested by a multi-site observational study (see Warbrick et al., Reference Warbrick, Dunn, Moran, Campbell, Kessler, Marchant, Farr, Ryan, Parkin, Sharpe, Turner, Sylianou, Sumner and Wood2023). Adapting CBT practices with the TT remit may help therapists work more confidently with clients with more complex needs.
Key practice points
-
(1) Online training for therapists, on the management of clients with concurrent personality difficulties, is both feasible to deliver and is acceptable to therapists.
-
(2) Such online training may be associated with important changes in the clinical outcomes of clients.
-
(3) Online training may enhance the knowledge, skills, and confidence of high intensity therapists in working with clients with concurrent personality difficulties.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1754470X25100482
Data availability statement
The client data that support the findings of this study are available from NHS Talking Therapies. Restrictions apply to the availability of these data, which were used under a bespoke data sharing agreement for this study. The therapist data are not publicly available because it contains information that could compromise the privacy of the research participants.
Acknowledgements
None.
Author contributions
Emily Eyles: Conceptualization (supporting), Data curation (lead), Formal analysis (lead), Investigation (lead), Methodology (lead), Project administration (lead), Software (lead), Writing - original draft (lead), Writing - review & editing (lead); Michelle Farr: Conceptualization (supporting), Data curation (lead), Formal analysis (lead), Investigation (lead), Methodology (lead), Project administration (supporting), Software (equal), Writing - original draft (equal), Writing - review & editing (equal); Barnaby Dunn: Conceptualization (supporting), Methodology (supporting), Project administration (supporting), Supervision (supporting), Writing - review & editing (supporting); Maria Theresa Redaniel: Conceptualization (equal), Data curation (equal), Formal analysis (equal), Funding acquisition (lead), Investigation (lead), Methodology (lead), Project administration (equal), Resources (lead), Software (equal), Supervision (equal), Writing - original draft (supporting), Writing - review & editing (supporting); Laura Amy Warbrick: Conceptualization (supporting), Methodology (supporting), Project administration (supporting), Writing - review & editing (supporting); David Kessler: Conceptualization (supporting), Investigation (supporting), Project administration (supporting), Supervision (supporting), Writing - review & editing (supporting); Richard Cooper: Conceptualization (supporting), Data curation (supporting), Investigation (supporting), Project administration (supporting), Resources (supporting), Writing - review & editing (supporting); Paul Moran: Conceptualization (lead), Funding acquisition (equal), Investigation (lead), Methodology (lead), Project administration (equal), Supervision (lead), Writing - original draft (equal), Writing - review & editing (lead).
Financial support
This research was funded by the National Institute for Health and Care Research Applied Research Collaboration West (NIHR ARC West) at University Hospitals Bristol and Weston NHS Foundation Trust (core NIHR infrastructure funded: NIHR200181). The views expressed in this article are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. Laura Warbrick’s time on this project was supported by a National Institute for Health and Care Research (NIHR) Three Schools Mental Health pre-doctoral training fellowship (grant reference: MHf011). Barney Dunn’s time on this project was supported by the Office for Life Sciences and the NIHR Mental Health Translational Research Collaboration, hosted by the NIHR Oxford Health Biomedical Research Centres. The views expressed here are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health or Social Care, or the Office for Life Sciences.
Competing interests
The authors declare none.
Ethical standards
Ethics for the study were obtained via the NHS Health Research Authority East of England – Cambridge Central Research Ethics Committee (REC reference: 22/EE/0034). This research has conformed to the Declaration of Helsinki. The authors have abided by the Ethical Principles of Psychologists and Code of Conduct set out by the BABCP and BPS.





 Open access
Open access
Comments
No Comments have been published for this article.