


Mental health problems, especially emotional disorders, are common in children and young people (CYP) and their prevalence has been increasing in recent years. Reference Taxiarchi, Anderson, Abel, Ford, Newlove-Delgado and McManus1 This has meant that, in most countries, the need and demand for specialist child and adolescent mental health services (CAMHS) considerably outweigh service capacity and provision. Emotional disorders such as depression and anxiety disorders are associated with considerable distress for affected CYP and their families. They significantly impact day-to-day functioning across a range of domains and settings including home, school/education, employment, relationships and wider engagement in activities. Reference Clayborne, Varin and Colman2–Reference Pollard, Reardon, Williams, Creswell, Ford and Gray4 They are also a risk factor for persistent and other mental health difficulties, self-harm and suicidality. Reference Costello and Maughan5,Reference Weavers, Heron, Thapar, Stephens, Lennon and Bevan Jones6 Despite this, there are inequalities in access to services, particularly reflecting sociodemographic and socioeconomic factors. Reference Mannes, Coughlan, Yoon, Morgan, Drayak and Crozier-Roche7–Reference Trethewey, Mathews, Russell and Newlove-Delgado10 However, studies investigating inequalities with regard to access, receipt of care and clinical outcomes for CYP with emotional difficulties referred to specialist mental health services have not used multi-site prospective longitudinal designs: they have, instead, relied on survey or administrative data. However, routine administrative data-sets have shortcomings, with challenges reflecting data quality and completeness. By contrast, the present study uses both participant-reported and service-related data specifically collected from records, with very high rates of completion and excellent data integrity. An advantage of carrying out such research in UK settings is that mental health services are freely available at the point of delivery, which means that affordability factors do not impact the findings. This study uses longitudinal data from a large randomised controlled trial (standardised diagnostic assessment for children and young people with emotional difficulties, STADIA), which investigated the impact of introducing a standardised diagnostic assessment tool into CAMHS. Reference Sayal, Wyatt, Partlett, Ewart, Bhardwaj and Dubicka11 The focus is on CYP with emotional difficulties referred to CAMHS. This study aims to investigate the roles of (a) sociodemographic (sex, age, ethnicity), Reference Edbrooke-Childs and Patalay9,Reference Trethewey, Mathews, Russell and Newlove-Delgado10,Reference Sayal, Yates, Spears and Stallard12–Reference Mathews, Ford, White, Ukoumunne and Newlove-Delgado14 (b) socioeconomic (neighbourhood deprivation), Reference Mannes, Coughlan, Yoon, Morgan, Drayak and Crozier-Roche7,Reference Trethewey, Mathews, Russell and Newlove-Delgado10 (c) care-related (previous referral or emotional disorder diagnosis) Reference Hansen, Christoffersen, Telleus and Lauritsen15 and (d) clinical (symptoms, impairment) Reference Trethewey, Mathews, Russell and Newlove-Delgado10,Reference Sayal, Wyatt, Partlett, Ewart, Bhardwaj and Dubicka11,Reference Wickersham, Westbrook, Colling, Downs, Govind and Kornblum13,Reference Mathews, Ford, White, Ukoumunne and Newlove-Delgado14 factors in influencing access to services, receipt of clinical care and clinical outcomes.
Method
Setting and participants
This secondary analysis uses data from STADIA, which was a multi-site, randomised controlled trial investigating the use of a standardised diagnostic assessment tool, as an adjunct to usual care, in CAMHS (i.e. multidisciplinary secondary care mental health services for CYP). Reference Day, Wyatt, Bhardwaj, Dubicka, Ewart and Gledhill16 The trial comparator arm was usual care only. The current study is reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. STADIA took place in 8 large National Health Service (NHS) mental health trusts (sites) spread across England, focusing on 1225 children aged 5 to 17 years and with emotional difficulties referred to CAMHS. Recruitment to the trial ran from 2019 until 2021, and 18-month follow-up was completed by 2023. The trial primary participant providing data varied by CYP age: for 5- to 10-year-olds, this was the parent/carer; for 11- to 15-year-olds, the parent/carer was the primary participant and, with their permission, the young person could also provide data; for 16- to 17-year-olds, the young person was the primary participant and, with their permission, the parent/carer could also provide data. Randomisation took place following collection of baseline data, on average taking 7.6 days (mean) from referral receipt. For further information about the trial procedures and patient and public involvement activities throughout the trial, please see the protocol and full trial paper and report. Reference Sayal, Wyatt, Partlett, Ewart, Bhardwaj and Dubicka11,Reference Day, Wyatt, Bhardwaj, Dubicka, Ewart and Gledhill16,Reference Sayal, Wyatt, Thomson, Holt, Ewart and Bhardwaj17 All participants gave informed consent before taking part. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and with the Helsinki Declaration of 1975 as revised in 2013. All procedures involving participants were approved by the South Birmingham Research Ethics Committee (ref. no. 19/WM/0133).
Data collection and measures
The following data were collected.
Participant-reported
Participant-reported questionnaires were completed at baseline and 12-month follow-up. These included measures assessing sociodemographic and socioeconomic factors (at baseline only) and CYP mental health:
-
(a) sociodemographic: CYP age, sex and ethnicity;
-
(b) socioeconomic: postcode of CYP primary residence (which was linked to the Index of Multiple Deprivation (IMD) quintile, as a proxy for neighbourhood deprivation (https://imd-by-postcode.opendatacommunities.org/imd/2019);
-
(c) whether there had been a previous referral to CAMHS;
-
(d) the Mood and Feelings Questionnaire (MFQ), which is a 33-item measure of depression with well-established reliability and validity (score range 0–66; scores ≥27 suggest moderate–severe depression); Reference Angold, Costello, Messer and Pickles18–Reference Daviss, Birmaher, Melhem, Axelson, Michaels and Brent20
-
(e) the Strengths and Difficulties Questionnaire (SDQ), which is a 25-item mental health measure with well-established reliability and validity. Reference Goodman21,Reference Goodman22 The total difficulties score (range 0–40) incorporates emotional, conduct, hyperactivity/inattention and peer problems; the impairment scale (0–10) reflects distress and impact on home life, friendships, learning and leisure activities. Reference Goodman21 Both these measures capture co-occurring difficulties. Validated cut-off scores indicate the likelihood of having a mental health disorder. Reference Goodman22 For example, where the criteria for both symptoms (either parent-rated total difficulties score of ≥20 or self-rated score of ≥17) and impairment (score of ≥2) are met for a probable disorder (i.e. caseness), there is a >20-fold increased likelihood of having a mental health disorder. Reference Sayal and Taylor23 For CYP in the trial intervention arm, baseline SDQ was collected within the standardised diagnostic assessment tool (Development and Well-Being Assessment). Reference Goodman, Ford, Richards, Gatward and Meltzer24
Service-related
The following data were collected from CAMHS records by site researchers, using case record forms, at baseline and at 12- and/or 18-month follow-up:
-
(a) at baseline: (i) previous referral to CAMHS; (ii) previous or existing documented diagnosis of an emotional disorder;
-
(b) acceptance of: (i) the index referral (i.e. the referral leading to trial entry) by 12 months; (ii) any referral (including re-referrals) by 18-month follow-up; referral acceptance is defined as being offered an appointment in CAMHS; Reference Sayal, Wyatt, Partlett, Ewart, Bhardwaj and Dubicka11
-
(c) by 18-month follow-up: (i) receipt of a clinical diagnosis of an emotional disorder (such as depression, any anxiety disorder, etc.: see main trial paper and report for full list of disorders and details of adjudication procedures); Reference Sayal, Wyatt, Partlett, Ewart, Bhardwaj and Dubicka11,Reference Sayal, Wyatt, Thomson, Holt, Ewart and Bhardwaj17 (ii) any treatment/intervention offered.
Predictor measures
Predictor variables included CYP age, sex, ethnicity and IMD quintile, previous CAMHS referral, previous/existing diagnosis of emotional disorder in CAMHS records and MFQ and/or SDQ scores (please see Statistical analysis section below).
Outcome measures
-
(a) Referral acceptance: (i) index referral accepted by 12-month follow-up; (ii) any referral accepted by 18-month follow-up;
-
(b) clinical care (if referral accepted within 18 months): (i) receipt of a confirmed clinical diagnosis of an emotional disorder; (ii) any treatment/intervention offered;
-
(c) clinical outcomes: (i) MFQ parent or CYP cut-off score ≥27 at 12-month follow-up; (ii) SDQ caseness (i.e. parent total score ≥17 or CYP total score ≥20, and parent or CYP impairment score ≥2) at 12-month follow-up.
Statistical analysis
The following analyses were undertaken using Stata version 18 for Windows (StataCorp LLC, College Station, Texas, USA; https://www.stata.com/products/windows/).
-
(a) Baseline characteristics were presented descriptively, using frequencies and percentages for categorical variables and means and standard deviations for continuous variables.
-
(b) Individual associations between predictor and outcome variables were estimated using mixed-effects logistic regression models, adjusting for the trial intervention arm as a fixed effect and site as a random effect. Odds ratios and 95% confidence intervals are presented.
-
(c) Finally, associations were calculated between baseline predictor variables (including CYP age (as a categorical variable (5–10 or 11–17 years) for the clinical outcomes, reflecting the methodology of the trial data collection), sex, ethnicity (White versus Black, minority ethnic or dual/mixed heritage) and deprivation index quintile (the reference group was the first (most deprived) quintile)) and outcome variables of interest, using mixed-effects multivariable logistic regression models (additionally adjusting for the trial intervention arm as a fixed effect and site as a random effect). In addition, the following were performed.
-
(i) For service-related outcomes (referral acceptance and clinical care), additional predictor measures included (I) baseline symptom severity, as a binary measure, using MFQ (parent or CYP score ≥27) and SDQ (parent total score ≥17 or CYP total score ≥20); (II) baseline impairment (parent or CYP SDQ impairment score ≥2); (III) previous CAMHS referral; and (iv) previous emotional disorder diagnosis.
-
(ii) For clinical outcomes (MFQ cut-off and SDQ caseness), the respective models also adjusted for (I) index referral acceptance by 12 months and (II) baseline severity as a binary measure, i.e. MFQ (parent or CYP baseline MFQ score ≥27) or SDQ score (parent total score ≥17 or CYP total score ≥20 and impairment score ≥2 at baseline). As an additional analysis, for participants with 12-month follow-up data we also explored whether baseline sociodemographic and socioeconomic factors were associated with baseline MFQ cut-off and SDQ caseness (see Appendix Table 1 available at https://doi.org/10.1192/bjp.2026.10617).
-
-
(d) Sensitivity analyses were performed for all outcomes – the same mixed-effects logistic regression models were used, with the addition of an age category (5–10 or 11–17 years) and sex interaction.
Results
The sample consisted of 1225 children and young people (mean age 11.95 years (s.d. 3.1)); 58% were female, 86% were from White ethnicity backgrounds, 31% had previously been referred to CAMHS, 6% had a previous/existing documented diagnosis of an emotional disorder and there was a relatively even spread across the 5 deprivation index quintiles (ranging from 17 to 23% in each quintile). Service-related outcome data were collected for 99% of the sample, and 12-month follow-up MFQ and SDQ data completed in relation to 73 and 75%, respectively.
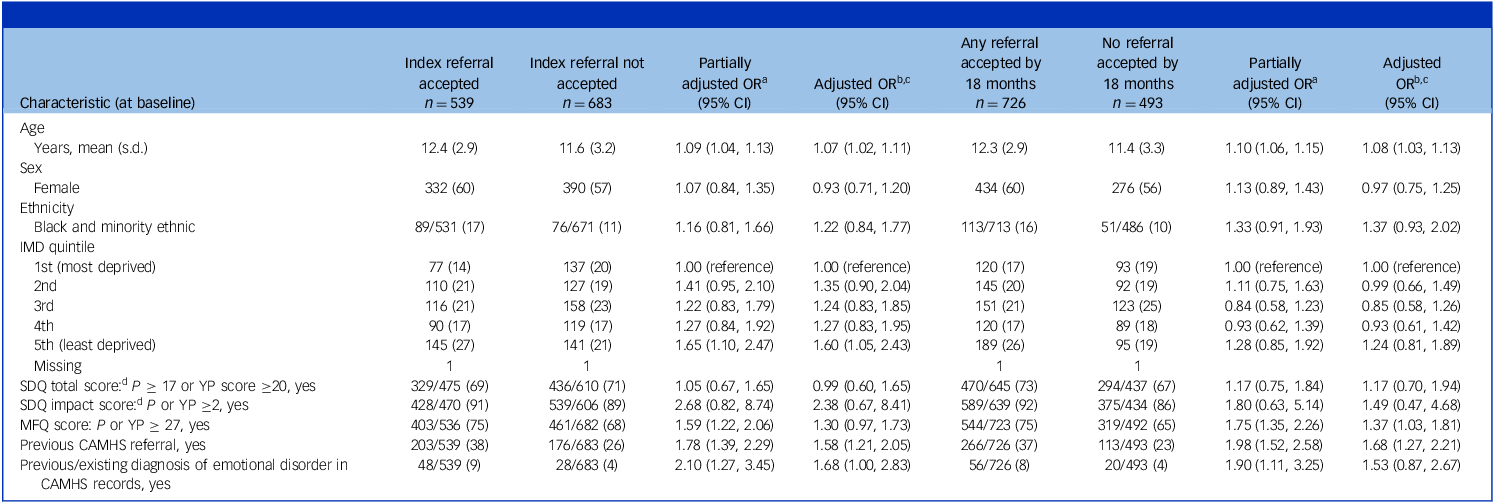
As shown in Table 1, 44% of index referrals were accepted by 12 months and, on multivariable analyses, the main predictors were older CYP age, previous referral to CAMHS, previous/existing diagnosis of an emotional disorder and living in the least deprived neighbourhood quintile. By 18 months, 60% of the sample had had referrals accepted and the main predictors were older age, previous CAMHS referral and scoring above cut-off on MFQ.
Predictors of referral acceptance

Figures represent number (percentage) of participants unless otherwise stated.
OR, odds ratio; IMD, Index of Multiple Deprivation; SDQ, Strengths and Difficulties Questionnaire; MFQ, Mood and Feelings Questionnaire; YP, young person; CAMHS, Child and Adolescent Mental Health Services.
a. Odds ratios obtained from mixed-effects logistic regression, also adjusting for intervention allocation as a fixed effect and site as a random effect.
b. The full model also adjusts for all other predictor variables as fixed effects, as well as intervention allocation as a fixed effect and site as a random effect.
c. The numbers of observations (1199 and 1196, respectively) are less than the total sample due to missing data within the following variables: ethnicity, IMD score and MFQ score.
d. Due to baseline SDQ being collected within Development and Well-Being Assessment, completion rates were lower within the intervention group. Participants who did not complete the SDQ were found to be representative of the remainder of the trial population, and therefore missing baseline SDQ scores (total and impact) were imputed using the mean score of the remainder of the sample to permit inclusion in the analysis models.
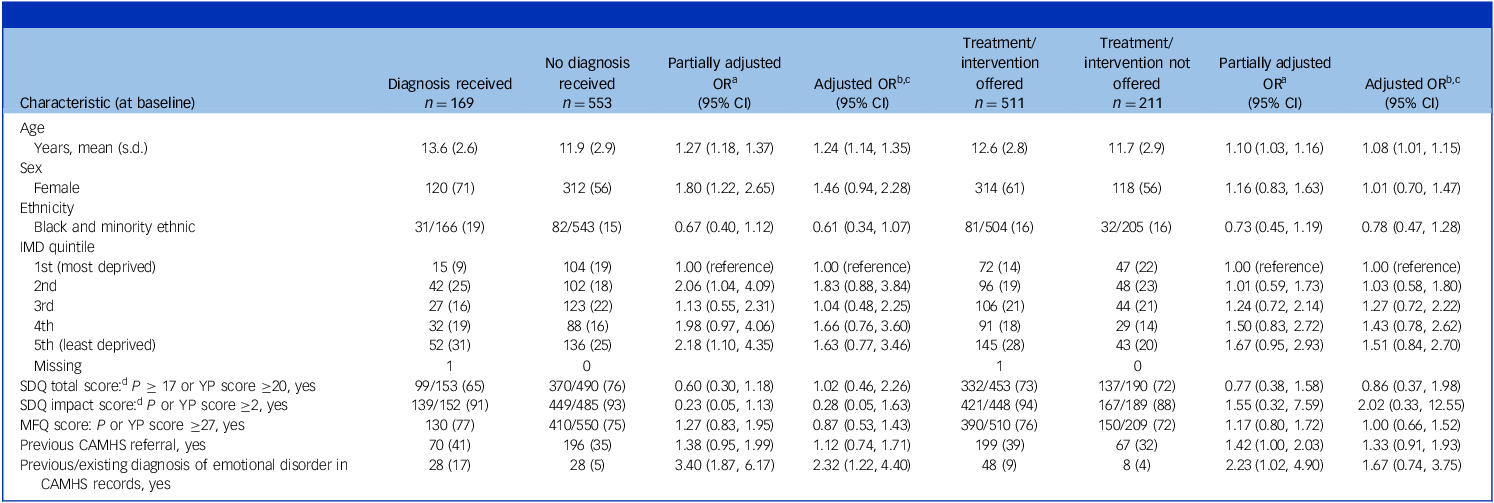
Table 2 shows that, among those whose referral was accepted within 18 months, 23% received a clinical diagnosis of an emotional disorder and, overall, 71% had been offered treatment/intervention from CAMHS. Predictors of receiving a clinical diagnosis were older age and having a previous/existing diagnosis at the time of referral; the only predictor of being offered any treatment/intervention was older age.
Predictors of receipt of emotional disorder diagnosis and treatment/intervention offered, within 18 months (if referral accepted)

Figures represent numbers (percentage) of participants unless otherwise stated.
OR, odds ratio; IMD, Index of Multiple Deprivation; SDQ, Strengths and Difficulties Questionnaire; MFQ, Mood and Feelings Questionnaire; YP, young person; CAMHS, Child and Adolescent Mental Health Services.
a. Odds ratios obtained from mixed-effects logistic regression, also adjusting for intervention allocation as a fixed effect and site as a random effect.
b. Full model also adjusts for all other predictor variables as fixed effects, as well as intervention allocation as a fixed effect and site as a random effect.
c. The number of observations (707) is less than the total sample due to missing data within the following variables: ethnicity, IMD score and MFQ score.
d. Due to baseline SDQ being collected within Development and Well-Being Assessment, completion rates were lower within the intervention group. Participants who did not complete the SDQ were found to be representative of the remainder of the trial population, and therefore missing baseline SDQ scores (total and impact) were imputed using the mean score of the remainder of the sample to permit inclusion in the analysis models.
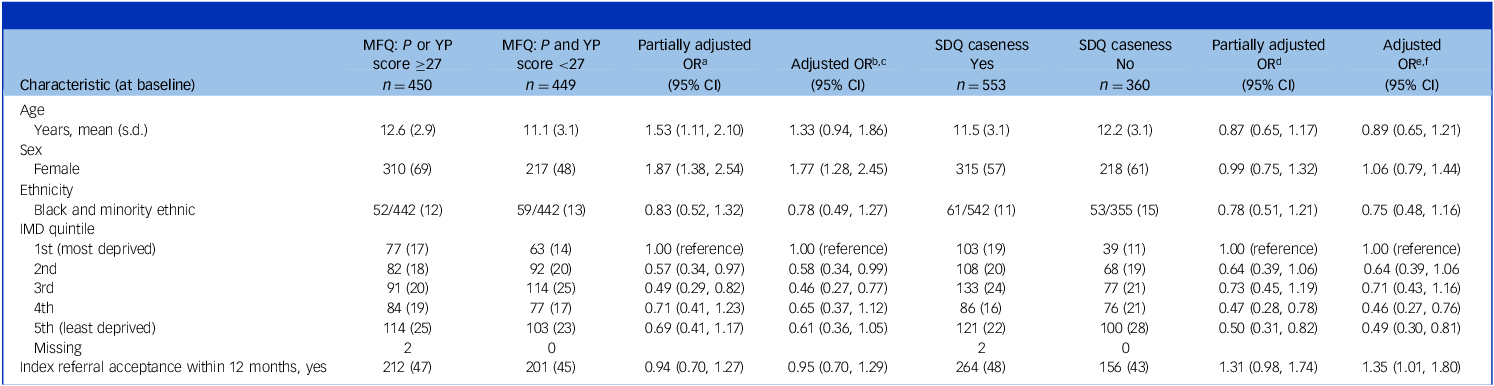
In relation to clinical outcomes, among those with participant-reported 12-month follow-up data, 70% scored above the MFQ cut-off for depression at baseline and 50% at 12-month follow-up. As shown in Table 3, the main predictors of scoring above cut-off at follow-up were female sex and living in the most deprived neighbourhood quintile (compared with the second and third quintiles). In terms of meeting SDQ caseness criteria, 67% scored above cut-off at baseline and 61% at 12-month follow-up. The main predictors of scoring above cut-off at follow-up were living in the most deprived neighbourhood quintile (compared with the fourth and fifth quintiles) and acceptance of the index referral
Predictors of scoring above MFQ cut-off and meeting SDQ caseness criteria at 12-month follow-up

Figures represent numbers (percentage) of participants unless otherwise stated. Mean (s.d.) age is presented for information only, with age treated categorically (5–10, 11–17 years) in the analyses.
MFQ, Mood and Feelings Questionnaire; SDQ, Strengths and Difficulties Questionnaire; YP, young person; OR, odds ratio; IMD, Index of Multiple Deprivation.
a. Odds ratios obtained from mixed-effects logistic regression, also adjusting for intervention allocation and baseline MFQ score as fixed effects and site as a random effect.
b. Full model also adjusts for all other predictor variables as fixed effects, as well as intervention allocation as a fixed effect and site as a random effect.
c. The number of observations (882) is less than the total sample due to missing data within the following variables: ethnicity, IMD score and MFQ score.
d. Odds ratios obtained from mixed-effects logistic regression, also adjusting for intervention allocation and baseline parent SDQ total score ≥17 or child SDQ total score ≥20, impact score ≥2 as fixed effects and site as a random effect.
e. Full model also adjusts for all other predictor variables as fixed effects, as well as intervention allocation as a fixed effect and site as a random effect.
f. The number of observations (897) is less than the total sample due to missing data within the following variables: ethnicity and IMD score. Due to baseline SDQ being collected within Development and Well-Being Assessment, completion rates were lower within the intervention group. However, participants who did not complete the SDQ were found to be representative of the remainder of the trial population, and therefore missing baseline SDQ scores (total and impact) were imputed using the mean score of the remainder of the sample for the analysis models.
Across all analyses there was no evidence of an age–sex interaction, and the main findings were unchanged.
Discussion
Main findings
This longitudinal study investigated the roles of sociodemographic, socioeconomic and clinical factors in influencing access to and receipt of care, and clinical outcomes, for CYP with emotional difficulties who had been referred to CAMHS. Our findings highlight considerable inequalities in access to care and services for CYP with mental health difficulties. It is possible that some of our findings might reflect the limited funding and capacity of CAMHS and the pressure to manage waitlists and waiting times. Reference Newman, Sayal, Ewart, Lang, Bhardwaj and Dubicka25 However, a relatively consistent finding from our study related to CYP living in the most deprived neighbourhoods – they were less likely to have their index referral to CAMHS accepted and were more likely to have worse mental health outcomes at 12-month follow-up. These associations persisted after adjusting for sociodemographic and clinical factors, as well as other potential confounder variables, including study site (the latter reflecting that service-related factors such as site/service variation in referral acceptance rates and waiting times, as well as geographical region, had been taken into account). Children and young people living in more deprived neighbourhoods were less likely to be seen, and therefore to receive timely help. Reference Mannes, Coughlan, Yoon, Morgan, Drayak and Crozier-Roche7 Possible reasons for this might be that their problems were less likely to be detected by triaging or assessing professionals, or were attributed to socioeconomic factors rather than relating to their mental health, acting as a barrier to care for CYP with probable emotional disorders.
Surprisingly, there were few clinical predictors (such as symptom severity or functional impairment) of receiving help, apart from severity of depression at baseline predicting acceptance of referral by 18 months (although not acceptance of the index referral by 12 months). This association with late/eventual referral acceptance highlights delays in accessing care, and therefore potentially receiving evidence-based interventions, when problems are severe. Although other markers of severity or chronicity, such as having had a previous referral Reference Hansen, Christoffersen, Telleus and Lauritsen15 (and, if this was rejected, consequent delays and multiple referrals before receiving help) Reference Newman, Sayal, Ewart, Lang, Bhardwaj and Dubicka25 or previous/existing diagnoses, were associated with referral acceptance, this was not the case for participant-reported symptoms or impairment. Among those whose referral was accepted by 18 months, 23% received a clinical diagnosis of an emotional disorder and 29% were not offered a treatment/intervention from CAMHS. And, similarly, clinical factors such as severity and functional impairment were not associated with treatment/interventions being offered.
With regard to 12-month clinical outcomes, it was striking that the proportion of the sample meeting clinical caseness criteria changed very little over time (67 v. 61%), highlighting the persistent and chronic nature of the difficulties that these CYP were experiencing. Although the proportion scoring above clinical cut-off for depression reduced from 70 to 50%, this figure still reflects that half of these CYP had clinically significant depression symptoms 1 year after being referred to CAMHS. Female sex and residing in the most deprived neighbourhood quintile (compared with the second and third quintiles) were associated with scoring above the depression cut-off at 12-month follow-up. Furthermore, living in the most deprived neighbourhood quintile (compared with the fourth and fifth (the most affluent) quintiles) was associated with meeting clinical caseness criteria at 12-month follow-up. Also, in the multivariable analyses, acceptance of the index referral within 12 months was associated with meeting clinical caseness criteria at follow-up (albeit 95% confidence intervals were very close to 1). This potentially counterintuitive finding might reflect delays in the index referral being accepted, or possibly unmeasured or residual confounding, despite adjustment for baseline severity and impairment.
Relationship with the literature
Over the past two decades there have been increases in the prevalence of emotional disorders, such as anxiety and depression, among CYP, with older CYP and females being more likely to have emotional disorders. Reference Taxiarchi, Anderson, Abel, Ford, Newlove-Delgado and McManus1 Our data indicate that older CYP are also more likely to be seen by CAMHS. Worse outcomes for females in terms of persistent depression symptoms might reflect the fact that the onset and persistence of depression are more likely in females. Reference Weavers, Heron, Thapar, Stephens, Lennon and Bevan Jones6 In terms of deprivation, recent data from one NHS trust found that CYP from the most deprived areas were twice as likely to have their referrals rejected, Reference Mannes, Coughlan, Yoon, Morgan, Drayak and Crozier-Roche7 and national data also suggest that 5- to 10-year-olds (but not 11- to 16-year-olds) living in more deprived neighbourhoods are less likely to have contact with a mental health specialist. Reference Trethewey, Mathews, Russell and Newlove-Delgado10
Our data also tentatively suggest that those CYP whose referral was accepted fared worse – they were more likely to meet clinical caseness criteria at 12-month follow-up. Taken at face value, this is a puzzling finding given that it was present after adjusting for confounder variables (factors associated with referral acceptance (predictor) and caseness (outcome)), such as baseline severity and sociodemographic and socioeconomic factors. However, there are mixed findings in the literature as to whether routine services help and make a difference to clinical outcomes following receipt of care, with some studies indicating improvements but others finding limited or no effect, or even worse outcomes. Reference Angold, Costello, Burns, Erkanli and Farmer26–Reference Verhage, Jansen, Almansa, Wunderink, Grietens and Reijneveld31 A recent longitudinal data registry study in Finland found that over half of former CAMHS patients went on to require adult mental health services by the age of 29 years. Reference Healy, Lang, O’Hare, Metsala, O’Connor and Lockhart32 Our study was able to investigate only whether a referral had been accepted, so we are unable to say how much contact the CYP had with CAMHS and which professional(s) they saw. And, given that, for CYP receiving care for psychosocial problems or those with diagnosed depression, Reference Wickersham, Westbrook, Colling, Downs, Govind and Kornblum13,Reference Verhage, Jansen, Almansa, Wunderink, Grietens and Reijneveld31 data indicate that between a third and a half are in contact with services for over 1 year (suggesting the persistence of caseness), perhaps 12 months is too soon to expect improvements. Nevertheless, given the uncertainty in the literature as to whether routine CAMHS make a difference to outcomes, our finding requires further exploration and investigation in future research – for example, it might be that referral acceptance, but with delays in subsequently receiving help, carries an implication for CYP and families that their problems are more intractable.
Methodological issues
Our study has a number of notable strengths. First, it reflects a real-world study of predictors and outcomes in a nationally representative help-seeking sample, and is therefore generalisable to CYP with emotional difficulties referred to mental health services. The underpinning STADIA trial had a broad geographical spread of sites across England (therefore covering a wide range of services and service models, and socioeconomic areas), and the sample was demographically representative of CYP seen by CAMHS, including ethnicity, Reference Edbrooke-Childs, Rashid, Ritchie and Deighton30 ensuring the generalisability of the findings. Second, the study benefited from a large sample size with excellent rates of retention and follow-up (99% for service-related outcomes and 73–75% for participant-reported outcomes), focused on the full range of emotional disorders as well as utilising measures (SDQ) capturing co-occurring difficulties, and our analyses adjusted for a range of important confounders. Data were collected from service records and CYP and/or parent reports. Third, the study ran from 2019 to 2023, spanning the COVID-19 pandemic period, and incorporated data collection over a 12- to 18-month follow-up duration. This enabled an up-to-date investigation of CYP mental health reflecting the pre-, in- and post-pandemic periods. Because the study spanned the pandemic, and although it is possible that pre-existing inequalities in access to care and outcomes were exacerbated over this period, their longer-term impact may persist over time. There has been an increase in both need and demand for services even since 2023. 33 Fourth, as described in the main trial report, Reference Sayal, Wyatt, Thomson, Holt, Ewart and Bhardwaj17 patient and public involvement was very strongly integrated and embedded throughout the research.
In terms of limitations, despite there being a large sample size with 14% of CYP being of Black, minority ethnic or dual/mixed heritage ethnicity (in keeping with national demographic figures), cell sizes were relatively modest for individual ethnic minority groups, which meant their combination into an aggregate group, limiting the ability to fully investigate ethnicity-related differences in risk. The IMD reflects an aggregate neighbourhood measure based on postcode, which is not necessarily the same as individual household-level socioeconomic status. As a longitudinal study, there was some attrition over time involving participant-reported data. The observational design also means that, despite best efforts to adjust associations for potential confounding factors, there may have been residual confounding present. Finally, the focus of this paper is on longitudinal observational data because the underpinning trial was not designed to investigate the effectiveness of services per se – this means that we did not collect data on the number of appointments offered or attended, the match between identified presenting needs and the offer and receipt of appropriate interventions, nor the level of adherence with treatments/interventions. Nevertheless, our caseness outcome is important given that one of the aims of mental health service input is to reduce symptom severity and impairment in the short to medium term.
Clinical and policy implications
The population prevalence of emotional disorders in 5- to 16-year-olds is estimated at around 6%. Reference Taxiarchi, Anderson, Abel, Ford, Newlove-Delgado and McManus1 However, in this clinically referred sample with emotional difficulties and among those whose referral was accepted for assessment by secondary care mental health services, it is striking that only 23% received a clinical diagnosis of an emotional disorder. It is also striking that clinical severity and impairment did not predict diagnosis receipt. This raises questions about what information clinicians gather and take into account in their assessments, and their weighing up of this information, when making diagnostic decisions. Reference Thomson, Newman, Ewart, Bhardwaj, Dubicka and Marshall34
Similarly, in general, neither clinical severity nor impairment were associated with referral acceptance (the only exception was scoring above the MFQ cut-off point influencing referral acceptance by 18 months). In terms of the sociodemographic predictors studied, it is perhaps not surprising that older CYP were more likely to have their referral accepted and to be offered help. However, the corollary of this is that younger children (particularly those aged 5–10 years) are less likely to be seen and receive help. It might be that this younger age group are overlooked because resources are limited and their mental health difficulties are perceived as being less acute or risky. However, neglecting under-11s in this way might be a short-sighted approach because opportunities for offering help in a more timely and preventative way are missed, particularly given that this is a clinically referred (i.e. help-seeking) group of children with high levels of mental health needs.
In terms of socioeconomic risk factors, previous research has shown an association between parental unemployment and the presence of CYP emotional disorders. Reference Taxiarchi, Anderson, Abel, Ford, Newlove-Delgado and McManus1 The findings from our study demonstrate that neighbourhood-level indicators of socioeconomic deprivation are associated with a range of inequalities in relation to accessing care and clinical outcomes. CYP living in the most deprived neighbourhoods were least likely to have their index referral accepted (even after adjusting for other variables, including site). Although this association no longer held for referral acceptance by 18 months, this finding still suggests that socioeconomic deprivation contributes to delays in eventually receiving help (i.e. the index referral was less likely to be accepted, but a referral was eventually accepted at a later point). Further compounding this inequality and highlighting a ‘treatment gap’, our data show that CYP living in the most deprived neighbourhoods had worse clinical outcomes at 12 months, perhaps reflecting lack of, or delayed, receipt of care. Given their risk of worse clinical outcomes (i.e. still meeting clinical caseness criteria 1 year after being referred to CAMHS), these CYP should be receiving timely, not delayed, help.
An improved understanding of socioeconomic inequalities is essential to inform intervention efforts to ameliorate them in practice. Even after adjusting for other potential explanatory or confounding factors, the persistence of the association of socioeconomic factors with adverse outcomes highlights the need to address system change in access and care. Although there are aspirations to improve access to care, service pressures around managing waitlists and waiting times carry the risk of unintended consequences of rejecting referrals and signposting elsewhere. Unfortunately, our current service models seem to require CYP to develop significant mental health difficulties in the first instance, which then need to be noticed by others, followed by attempts to navigate complex referral processes with systems seemingly designed to gatekeep resources through rejection of referrals and signposting them out towards externally provided early intervention/voluntary sector services. Reference Newman, Sayal, Ewart, Lang, Bhardwaj and Dubicka25 Even if referrals are accepted, our linked qualitative work highlights that clinicians feel guilty about the long waits for help. Reference Newman, Sayal, Ewart, Lang, Bhardwaj and Dubicka25 Future research initiatives and efforts should aim to inform service redesign that enables more timely access to evidence-based interventions for emotional disorders (for example, perhaps the provision of evidence-based digital interventions, Reference Creswell, Taylor, Giles, Howitt, Radley and Whitaker35 or those more readily accessible in community neighbourhood settings such as community hubs or education settings), to minimise health inequalities and barriers to care.
Finally, acceptance of the index referral was not associated with severity or impact of difficulties at baseline, but was associated with meeting criteria for caseness at follow-up. At face value, this finding (greater likelihood of worse outcomes if the referral is accepted) seems counterintuitive. Possible reasons for this include (a) methodological factors (e.g. acceptance of the index referral was measured over a 12-month period and ultimate acceptance, following clinical information-gathering at triage, may have reflected increases in the severity or chronicity of difficulties over this time); (b) linked with this, service- or care-related factors may have limited opportunities for improvement (e.g. long waits before being seen, receiving insufficient number of sessions or not being offered appropriate or evidence-based interventions); (c) the potential role of stigma or self-labelling resulting from the impact on self-perceptions because of needing specialist services; and/or (d) residual confounding, particularly given that 95% confidence intervals were very close to one. Nevertheless, it cannot fully be ruled out that perhaps, for some young people, outcomes are worse than they should have been because the receipt of help is too late or not sufficiently tailored to their needs. This finding also needs to be interpreted within the context that 1 year following referral to CAMHS, mental health caseness and severity of depression were high in at least half of the sample.
In terms of service implications, our findings suggest that current structures and models of mental health services are difficult to access and navigate, potentially disjointed, and inequitable. The socioeconomic findings identified in this study are particularly striking – CYP living in the most deprived areas were more likely to have their CAMHS referral rejected and to have worse clinical outcomes. Systems and services should better support children living in relative poverty.
Overall, there was not much improvement over time, especially in terms of continuing to meet caseness criteria: delays in being seen exacerbate severity, and potential treatment resistance, leading to worse outcomes. There is an urgent need for policy-makers, and service-funders and commissioners, to pay attention to these findings (see Fig. 1 for a schematic summary flow diagram) and reconsider current service models, to enable timely access to appropriate and evidence-based care for CYP with significant mental health problems.
Schematic flow diagram summarising the pathways, outcomes and obstacles identified and policy implications to minimise inequalities and barriers to care. CAMHS, Child and Adolescent Mental Health Services; MFQ, Mood and Feelings Questionnaire.

Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10617
Data availability
Anonymised trial data may be shared with researchers external to the trial research team in accordance with the Nottingham Clinical Trials Unit’s (NCTU) data-sharing procedure. The data-sets containing individual participant data analysed during the STADIA trial will be available upon request from NCTU (ctu@nottingham.ac.uk) a minimum of 6 months following publication of the National Institute for Health and Care Research (NIHR) threaded publication. Access to the data will be subject to review of a data-sharing and -use request by a committee, including the Chief Investigator and Sponsor, should reflect a proposed collaboration with the STADIA trial team and will be granted only upon receipt of a data-sharing and -use agreement. Any data shared will be anonymised, which may impact on the reproducibility of published analyses. The analytic code used in this analysis are available upon reasonable request. The materials used in this research (e.g. STADIA trial Case Report Forms) are available in the main trial publication (https://doi.org/10.1111/jcpp.14090).
Acknowledgements
We thank all the children, young people and parents/carers participating in the trial, and the research sites involved in recruiting participants and data collection. The authors also thank the wider STADIA team for their input, including our Patient and Public Involvement Advisory Panels and Naomi Thorpe (Library and Knowledge Services, Nottinghamshire Healthcare NHS Foundation Trust), for the evidence searches.
Author contributions
K.S.: acquisition of funding, study design, manuscript writing and revision; G.H.: data analysis, manuscript writing and editing; C.P.: data analysis, manuscript editing and revision; L.W.: coordination of data collection, manuscript editing; A.B. and J.G.: acquisition of funding, manuscript editing and revision.
Funding
The STADIA trial was funded by the NIHR Health Technology Assessment programme (grant reference no. 16/96/09). K.S. is an NIHR senior investigator. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.