


Adverse childhood experiences (ACEs) are widely recognised as risk factors for psychiatric disorders in adulthood. Reference Arango, Dragioti, Solmi, Cortese, Domschke and Murray1,Reference Hogg, Gardoki-Souto, Valiente-Gómez, Rosa, Fortea and Radua2 Childhood neglect represents a critical yet underexplored dimension of ACEs. Unlike other forms of maltreatment, such as physical or sexual abuse, which typically involve more identifiable acts, neglect is characterised by prolonged absence of care and support, making it more difficult to detect and quantify.
According to the World Health Organization, neglect is defined as the failure to meet a child’s fundamental needs, encompassing physical health, education, emotional development, nutrition, shelter and safety. 3 It can be categorised into various subtypes based on children’s unmet needs, often with overlapping descriptions, such as physical, emotional, environmental, supervisory, medical, developmental and educational neglect, but also abandonment. Reference Barron, Jenny and Jenny4,Reference Brandon, Bailey, Belderson and Larsson5 The two most recognised subtypes are physical neglect and emotional neglect. Physical neglect refers to the failure to provide adequate food, shelter, clothing, medical care or supervision necessary for a child’s well-being. Emotional neglect involves a persistent lack of emotional responsiveness, support or affection from caregivers, potentially impairing a child’s psychological and social development. Reference Barron, Jenny and Jenny4
Despite these classification efforts, there is still no universally accepted definition of childhood neglect, leading to substantial variability in its assessment and interpretation. Consequently, prevalence estimates vary widely, complicating efforts to establish its true epidemiological burden. Global studies report neglect prevalence rates ranging from as low as 1.4% to as high as 80.1%, Reference Stoltenborgh, Bakermans-Kranenburg and van IJzendoorn6 reflecting substantial methodological, regional and socioeconomic differences. Reference Clément, Bérubé and Chamberland7–Reference Prevoo, Stoltenborgh, Alink, Bakermans‐Kranenburg and van IJzendoorn10
Given the well-established long-term effects of neglect on mental health, Reference Anda, Felitti, Bremner, Walker, Whitfield and Perry11–Reference Jackson, Frederico, Cleak and Perry13 estimating its prevalence in psychiatric populations is of critical importance. However, this task is even more challenging because of the inherent clinical complexity of these populations, including variability in symptom presentation and comorbidities that may influence recall and reporting. Reference Hardt and Rutter14–Reference Wielaard, Stek, Comijs and Rhebergen16 Although the association between other forms of childhood maltreatment – such as physical and sexual abuse – and psychiatric disorders has been extensively documented, Reference Hogg, Gardoki-Souto, Valiente-Gómez, Rosa, Fortea and Radua2 the specific contribution of neglect remains less defined. A limited number of studies have investigated its association with specific psychiatric disorders, often without distinguishing between neglect subtypes, and have consistently reported increased risk for major depressive disorder (MDD), Reference Infurna, Reichl, Parzer, Schimmenti, Bifulco and Kaess17,Reference Norman, Byambaa, De, Butchart, Scott and Vos18 anxiety disorders, Reference Norman, Byambaa, De, Butchart, Scott and Vos18 schizophrenia spectrum disorders, Reference Norman, Byambaa, De, Butchart, Scott and Vos18,Reference Varese, Smeets, Drukker, Lieverse, Lataster and Viechtbauer19 eating disorders, Reference Pignatelli, Wampers, Loriedo, Biondi and Vanderlinden20 substance use disorders and personality disorders. Reference Norman, Byambaa, De, Butchart, Scott and Vos18 To reinforce the role of neglect as a key environmental factor contributing to psychiatric vulnerability, a recent systematic review and meta-analysis examined the prevalence of different neglect subtypes across a wide range of psychiatric disorders. Reference Carvalho Silva, Oliva, Barlati, Perusi, Meattini and Dashi21 Although this study did not restrict inclusion to controlled designs, it reported consistently high prevalence rates across diagnostic groups, with some clinical conditions (i.e. MDD, bipolar disorder, schizophrenia spectrum disorders and eating disorders) showing significantly lower rates than others.
Building on this evidence, the primary aim of this work was to quantify the association between childhood neglect, including emotional neglect, physical neglect and unspecified neglect, and major psychiatric disorders in adulthood. This relationship was assessed by estimating odds ratios derived from studies comparing clinical populations (adults diagnosed with psychiatric disorders) and control groups. A secondary aim was to explore the association between neglect subtypes and specific psychiatric disorders, to provide a more comprehensive understanding of how different forms of neglect contribute to distinct psychopathological trajectories.
Method
Protocol and registration
The review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Reference Moher, Liberati, Tetzlaff and Altman22 The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; identifier: CRD42024620183; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=620183).
Search strategy and selection criteria
A systematic search strategy was conducted across three major databases (PubMed, EMBASE and PsycINFO) to identify relevant studies published between 1 January 1994 and 30 September 2024. Search terms combined keywords related to childhood neglect (e.g. ‘childhood neglect’, ‘emotional neglect’, ‘physical neglect’) with terms referring to psychiatric disorders (e.g. ‘mental disorder’, ‘psychiatric diagnosis’ and disorder-specific terms), using database-specific controlled vocabulary when applicable. Eligible studies assessed childhood neglect using validated instruments or structured clinical interviews and diagnosed psychiatric disorders using internationally recognised diagnostic tools (e.g. DSM-IV, DSM-IV-TR, DSM-5, ICD-10, ICD-11).
When assessment tools did not distinguish between emotional neglect and physical neglect, or when only a combined neglect score was reported, data were categorised as unspecified neglect to differentiate them from those explicitly referring to emotional neglect or physical neglect.
The psychiatric diagnoses included post-traumatic stress disorder (PTSD), anxiety disorders, obsessive–compulsive disorder (OCD), MDD, eating disorders, bipolar disorder, mood disorders, schizophrenia spectrum disorders, personality disorders and mixed psychiatric disorders.
All details on the search strategy, complete structured queries and selection criteria are provided in the Supplementary Material, available at https://doi.org/10.1192/bjp.2026.10693.
Data extraction and quality assessment
From the included studies, the following data were systematically extracted: full bibliographic reference, study design, participant age, proportion of female participants, psychiatric diagnosis, diagnostic category, diagnostic tools used, type of control group, neglect measurement tools, type of neglect assessed (unspecified neglect, emotional neglect and/or physical neglect) and statistical information required for meta-analytical computations. The latter included the number of patients and controls exposed to neglect and the sample size of each population.
For diagnostic categorisation, when studies included only one clinical sample, the diagnosis and diagnostic category were considered equivalent (e.g. MDD alone was categorised as major depressive disorder). For studies involving multiple clinical samples with similar diagnoses, broader diagnostic categories were used to group patients (e.g. ‘mood disorders’ encompassed depressive conditions beyond MDD, ‘eating disorders’ included mixed samples of eating-related conditions and ‘personality disorders’ covered various personality related diagnoses).
Controls were classified based on clinical assessment as either clinically assessed or non-clinically assessed, depending on whether structured diagnostic tools were used to confirm the absence of psychiatric disorders.
Data extraction was performed independently by two reviewers. Discrepancies were resolved through discussion and, when necessary, consultation with a third reviewer.
To evaluate methodological quality and assess the risk of bias in the included studies, the Joanna Briggs Institute critical appraisal checklist for analytical cross-sectional and case–control studies was employed. Reference Aromataris, Lockwood, Porritt, Pilla and Jordan23 Additional details about data extraction and quality assessment of the included studies are described in the Supplementary Material.
Statistical analysis
All meta-analyses were performed in R version 4.4.2 for macOS (R Foundation for Statistical Computing, Vienna, Austria; see https://www.r-project.org/), using the meta, Reference Balduzzi, Rücker and Schwarzer24 metafor Reference Viechtbauer25 and dmetar Reference Harrer, Cuijpers and Ebert26 packages.
For each eligible outcome (i.e. reported in at least three controlled studies), a random-effects model based on the inverse variance method with Hartung–Knapp–Sidik–Jonkman adjustment Reference Hartung27 was applied to estimate the pooled odds ratios from raw data. Between-study variance (τ 2) was calculated with the restricted maximum likelihood method. Reference Viechtbauer28 Heterogeneity was assessed by Cochran’s Q-statistic and I 2-estimation, Reference Higgins, Thompson, Deeks and Altman29 and categorised as low, moderate or high based on conventional thresholds.
Forest and L’Abbè plots were used to visualise results and between-study heterogeneity. Outliers and influential studies were identified using a combination of visual and quantitative diagnostics, including inspection of forest plots for confidence interval overlap, leave-one-out analyses and influence diagnostics such as Baujat plots Reference Viechtbauer and Cheung30 and, when applicable, graphic display of heterogeneity (GOSH) plots. Reference Harrer, Cuijpers and Ebert26,Reference Olkin, Dahabreh and Trikalinos31 These procedures focused on identifying studies exerting disproportionate influence on between-study heterogeneity and pooled effect estimates. Finally, an adjusted model and the corresponding forest plot were created excluding outliers and influential studies for a sensitivity analysis.
A contour-enhanced funnel plot and Egger’s test were used to detect publication biases. Reference Egger, Smith, Schneider and Minder32,Reference Peters, Sutton, Jones, Abrams and Rushton33 Duval and Tweedie’s trim-and-fill procedure Reference Duval and Tweedie34 was employed to calculate the bias-corrected effect size.
A subgroup analysis using a random-effects model (without Hartung–Knapp–Sidik–Jonkman adjustment within subgroups) was conducted to evaluate the impact of the type of psychiatric diagnosis on the pooled odds ratios.
Potential moderators, including year of publication, age and gender of patients and controls, psychiatric diagnosis, control type, neglect assessment tool and total risk of bias score, were explored via meta-regression analysis.
Missing values were imputed using the multivariate imputation by chained equations package Reference Buuren and Groothuis-Oudshoorn35 and applying the Breiman’s random forest algorithm.
Each moderator was tested in a simple regression model, and the most relevant predictors were identified via multimodel inference based on corrected Akaike information criterion. Reference Harrer, Cuijpers and Ebert26,Reference Anderson36–Reference Viechtbauer38 A more detailed description of the statistical analyses employed is reported in the Supplementary Material.
Results
Study selection and study characteristics
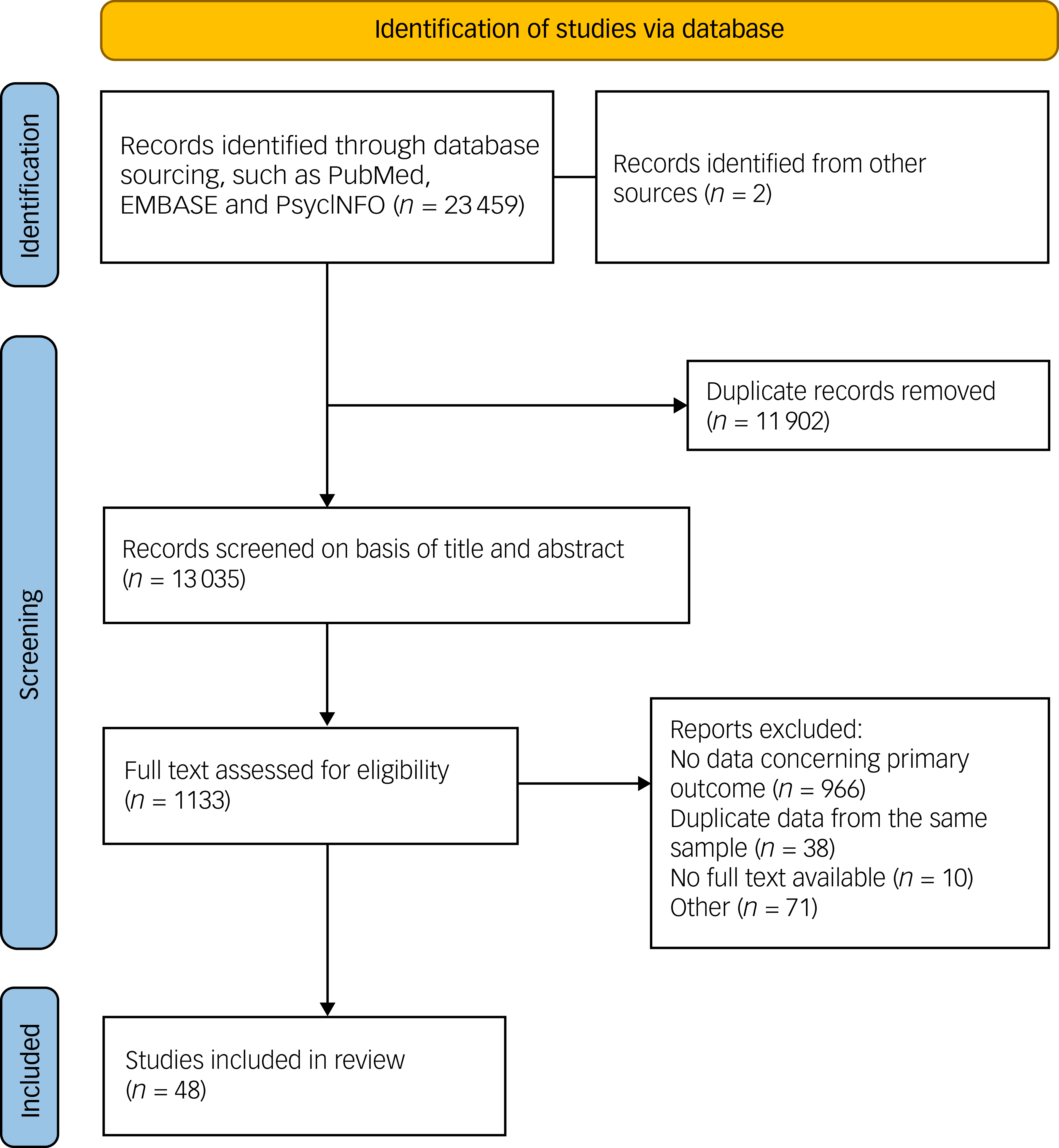
Of the 23 459 records initially identified, 48 studies met the inclusion criteria and were included in the meta-analysis. The flow chart diagram of the study selection procedure is displayed in Fig. 1. Additional details about the selection procedures and references for the included studies are available in the Supplementary Material.
Flow diagram chart showing the study selection procedure.

Fig. 1 Long description
Flow diagram chart showing the study selection procedure. The process begins with the identification of studies via database sourcing, such as PubMed, EMBASE, and PsycINFO, resulting in 23,459 records. Additionally, 2 records are identified from other sources. Duplicate records, totaling 11,902, are removed. The remaining 13,035 records are screened based on title and abstract. Following this, 1,133 full texts are assessed for eligibility. Reports are excluded for various reasons: 966 for no data concerning the primary outcome, 38 for duplicate data from the same sample, 10 for no full text available, and 71 for other reasons. Ultimately, 48 studies are included in the review.
The characteristics of the included studies, such as population size, place of recruitment, sample sizes, participant age, female proportion, psychiatric diagnoses, diagnostic tools and neglect assessment measures, are summarised in Table 1.
Characteristics of included studies (n = 48 studies)

Table 1 Long description
The table presents a detailed summary of 48 studies, focusing on various characteristics such as population size, place of recruitment, sample sizes, participant age, female proportion, psychiatric diagnoses, diagnostic tools, and neglect assessment measures. Each row corresponds to a different study, listing authors, year, country, number of cases and controls, age in years for both cases and controls, female proportion, diagnosis, diagnostic tool, and neglect assessment measures. Notable studies include those by Aas in 2023, Bromberger in 2022, and Bruffa in 2018, among others. The table provides a comprehensive overview of the methodologies and findings related to psychiatric diagnoses and neglect assessment across different regions and populations.
CTQ, Childhood Trauma Questionnaire; MDD, major depressive disorder; CECA.Q, Childhood Experiences of Care and Abuse Interview, Questionnaire version; ACE-Q, Adverse Childhood Experiences Questionnaire; BPD, borderline personality disorder; VES, Victimization Experience Schedule; OCD, obsessive–compulsive disorder; BED, binge eating disorder; BDD, body dysmorphic disorder; TAQ, Traumatic Antecedents Questionnaire; PTSD, post-traumatic stress disorder; LSC, Life Stressor Checklist; ITI, International Trauma Interview; NPD, narcissistic personality disorder; ELS, Early Life Stress Questionnaire; SPD, schizotypal personality disorder.
Across the clinical populations, a total of 18 061 participants were enrolled, with a pooled mean age of 36.3 years (95% CI 33.8–38.8) and a pooled proportion of females of 64.4% (95% CI 0.56–0.72). The control group comprised 37 394 participants, with a pooled mean age of 35.6 years (95% CI 33.2–37.9) and a proportion of females of 63.6% (95% CI 0.56–0.71).
Regarding diagnostic categories, MDD was the most frequently examined condition, appearing in 22 studies, followed by schizophrenia spectrum disorders in 15 studies and bipolar disorder in nine studies. Less frequently investigated categories included eating disorders, mood disorders and personality disorders. Additional psychiatric conditions, such as OCD, body dysmorphic disorder and PTSD, were each represented by a single study.
Among the included studies, the majority provided detailed assessments of both emotional neglect and physical neglect (39 and 38 studies, respectively), whereas only 10 studies reported unspecified neglect.
Information on study characteristics, including sociodemographic variables, psychiatric diagnoses, neglect assessment instruments and recruitment settings, is provided in the Supplementary Material.
Odds ratio estimations
The pooled odds ratio was 3.63 (95% CI 2.19–6.01, p < 0.001) for unspecified neglect, 3.26 (95% CI 2.51–4.25, p < 0.001) for physical neglect and 3.36 (95% CI 2.58–4.38, p < 0.001) for emotional neglect. Heterogeneity rates were substantial for all three estimations: I 2 = 91.7%, 95% CI 87.9–94.4%, Q = 157.53, p < 0.001 for unspecified neglect; I 2 = 86.7%, 95% CI 83.1–89.6%, Q = 323.88, p < 0.001 for physical neglect; I 2 = 84.3%, 95% CI 79.8–87.8%, Q = 281.11, p < 0.001 for emotional neglect.
Forest plots reporting pooled odds ratio analyses for unspecified neglect, physical neglect and emotional neglect, including all diagnostic subgroups, are available in Supplementary Figs 1–3, respectively.
Sensitivity analysis
Despite the high heterogeneity of the estimations, only one outlier was identified for unspecified neglect, Reference Mall, Platt, Temmingh, Musenge, Campbell and Susser64 whereas a larger number of outliers were detected for physical neglect (n = 8) Reference Bromberger, Chang, Colvin, Kravitz and Matthews40,Reference Hemmings, Lochner, van der Merwe, Cath, Seedat and Stein51,Reference Luo, Li, Zhang, Hu, You and Wang62,Reference Stapp, Williams, Kalb, Holingue, Van Eck and Ballard76–Reference Üçok, Noyan, Gülöksüz, Saka, Alptekin and Atbaşoğlu78,Reference Velikonja, Velthorst, McClure, Rutter, Calabrese and Rosell80,Reference Xie, Wu, Zheng, Guo, Yang and He84 and emotional neglect (n = 9). Reference Bromberger, Chang, Colvin, Kravitz and Matthews40,Reference Goltermann, Winter, Meinert, Sindermann, Lemke and Leehr48,Reference Stapp, Williams, Kalb, Holingue, Van Eck and Ballard76–Reference Üçok, Noyan, Gülöksüz, Saka, Alptekin and Atbaşoğlu78,Reference Velikonja, Velthorst, McClure, Rutter, Calabrese and Rosell80,Reference Xie, Zou, Xie, Hu, Tang and Cai83–Reference Yin, Guo, Xin, Zheng, Xue and Li85
After excluding these outliers, odds ratios increased marginally for unspecified neglect (odds ratio 4.09, 95% CI 2.53–6.61) and physical neglect (odds ratio 3.44, 95% CI 2.90–4.09), whereas a slight decrease in odds ratio was observed for emotional neglect (odds ratio 3.19, 95% CI 2.65–3.84). Additionally, heterogeneity was significantly reduced, reaching moderate levels for unspecified neglect (I 2 = 70.3%, Q = 40.43, p < 0.001) and physical neglect (I 2 = 47.6%, Q = 66.79, p = 0.001), and low levels for emotional neglect (I 2 = 57.9%, Q = 83.05, p < 0.001).
Influential studies were identified through combined inspection of Baujat plots, influence diagnostics and GOSH plot analyses. The number of studies was modest: one for unspecified neglect, Reference Mall, Platt, Temmingh, Musenge, Campbell and Susser64 five for physical neglect Reference Hemmings, Lochner, van der Merwe, Cath, Seedat and Stein51,Reference Luo, Li, Zhang, Hu, You and Wang62,Reference Stapp, Williams, Kalb, Holingue, Van Eck and Ballard76–Reference Üçok, Noyan, Gülöksüz, Saka, Alptekin and Atbaşoğlu78 and four for emotional neglect. Reference Bromberger, Chang, Colvin, Kravitz and Matthews40,Reference Stapp, Williams, Kalb, Holingue, Van Eck and Ballard76,Reference Takım, Sarı and Gokcay77,Reference Xie, Wu, Zheng, Guo, Yang and He84 Full details of the influence diagnostics and the corresponding plots are available in the Supplementary Material.
The exclusion of these studies did not result in substantial differences in odds ratios for any of the three neglect subtypes (odds ratio 4.09, 95% CI 2.19–6.01 for unspecified neglect; odds ratio 3.57, 95% CI 2.89–4.40 for physical neglect; odds ratio 3.53, 95% CI 2.85–4.37 for emotional neglect). However, heterogeneity rates increased again, reaching moderate to substantial levels across all categories (I 2 = 70.3%, Q = 40.43, p < 0.001; I 2 = 66.4%, Q = 112.98, p < 0.001; I 2 = 79.2%, Q = 192.45, p < 0.001, for unspecified neglect, physical neglect and emotional neglect, respectively).
Publication bias
A certain skewness for small studies was observed for unspecified neglect, physical neglect and emotional neglect (funnel plots reported in the Supplementary Material), confirmed by the Egger’s regression test (intercept 3.62, p = 0.003 for unspecified neglect; intercept 1.80, p < 0.001 for physical neglect; intercept 1.55, p = 0.002 for emotional neglect).
The trim-and-fill procedure significantly reduced the three pooled odds ratios. However, this was coupled with a notable increase in heterogeneity rates, which returned to substantial levels (odds ratio 1.48, 95% CI 0.71–3.09, I 2 = 93.1% Q = 290.03, p < 0.001 for unspecified neglect; odds ratio 1.95, 95% CI 1.44–2.66, I 2 = 88.2%, Q = 507.27, p < 0.001 for physical neglect; odds ratio 2.19, 95% CI 1.60–3.00], I 2 = 88.6%, Q = 510.05, p < 0.001 for emotional neglect).
Subgroup analysis according to diagnostic categories
The subgroup analysis for unspecified neglect was constrained by the limited number of available studies (Fig. 2). One diagnostic group, borderline personality disorder (BPD), included only a single study, whereas the other three groups (MDD, bipolar disorder, schizophrenia spectrum disorders) presented three or more studies. The random-effects model showed a significant between-group effect within most diagnoses, except for bipolar disorder (odds ratio 5.89, 95% CI 1.24–27.90, p = 0.140). The strongest association with unspecified neglect was observed for MDD (odds ratio 4.14, 95% CI 1.73–9.89, p = 0.015). Within-group heterogeneity remained at moderate-to-high levels.
Forest plot reporting odds ratios for unspecified neglect in the diagnostic subgroups, including bipolar disorder, major depressive disorder (MDD), schizophrenia spectrum disorders and borderline personality disorder (BPD). N, number of participants in the case and control groups.

Fig. 2 Long description
The table presents a comparison of odds ratios for unspecified neglect across different psychiatric disorders. It includes data for bipolar disorder, major depressive disorder (MDD), schizophrenia spectrum disorders, and borderline personality disorder (BPD). The table has multiple rows and columns, with column headers such as Study, Cases, Controls, Odds ratio, and Weight. Each row lists specific studies, the number of cases and controls, and the calculated odds ratios with their 95% confidence intervals. Notable trends include varying odds ratios across different disorders, with bipolar disorder showing an odds ratio of 5.89, MDD showing 4.14, schizophrenia spectrum disorders showing 1.83, and BPD showing 3.63. The table also includes heterogeneity statistics for each disorder subgroup.
Regarding physical neglect (Fig. 3), two diagnostic groups (PTSD and OCD) were represented by only one study each, and three additional categories (personality disorders, eating disorders, mood disorders) were examined only in two studies. The remaining diagnostic groups (MDD, bipolar disorder, schizophrenia spectrum disorders) had three or more studies available. The random-effects model indicated significant differences across subgroups, with the strongest associations observed between physical neglect and MDD (odds ratio 3.30, 95% CI 2.15–5.07, p < 0.001), bipolar disorder (odds ratio 2.80, 95% CI 0.99–7.91, p < 0.001) and schizophrenia spectrum disorders (odds ratio 3.47, 95% CI 2.12–5.69, p < 0.001). A substantial within-group heterogeneity was observed with I 2-values around 80% or higher.
Forest plot reporting odds ratios for physical neglect in the diagnostic subgroups, including schizophrenia spectrum disorder (SSD), major depressive disorder (MDD), personality disorder, bipolar disorder, obsessive–compulsive disorder (OCD), eating disorders, body dysmorphic disorder (BDD), post-traumatic stress disorder (PTSD) and mood disorders. N, number of participants in the case and control groups.

Fig. 3 Long description
The table presents odds ratios for physical neglect in different diagnostic subgroups, including schizophrenia spectrum disorder, major depressive disorder, personality disorder, bipolar disorder, obsessive-compulsive disorder, eating disorders, body dysmorphic disorder, post-traumatic stress disorder, and mood disorders. It includes columns for cases and controls, with unspecified neglect counts, odds ratios, confidence intervals, and weights. Notable trends include higher odds ratios for personality disorders and bipolar disorder compared to other disorders. The table summarizes the heterogeneity and overall odds ratios for each subgroup.
The subgroup analysis for emotional neglect (forest plot in Fig. 4) encompassed two diagnostic categories represented by only one study each (body dysmorphic disorder and OCD), two additional diagnostic subgroups including two studies each (eating disorders and mood disorders) and the remaining subgroups with at least three studies. The random-effects model indicated significant associations between emotional neglect and MDD (odds ratio 3.71, 95% CI 2.21–6.21, p < 0.001), bipolar disorder (odds ratio 3.68, 95% CI 1.12–12.04, p < 0.001), schizophrenia spectrum disorders (odds ratio 2.54, 95% CI 1.82–3.54, p < 0.001) and personality disorders (odds ratio 5.29, 95% CI 0.52–53.91, p = 0.003). Within-group heterogeneity was moderate to high, with I 2-values ranging from 74.3 to 85.5%.
Forest plot reporting odds ratios for emotional neglect in the diagnostic subgroups, including schizophrenia spectrum disorder (SSD), major depressive disorder (MDD), personality disorder, bipolar disorder, obsessive–compulsive disorder (OCD), eating disorders, body dysmorphic disorder (BDD) and mood disorders. N, number of participants in the case and control groups.

Fig. 4 Long description
The table presents a forest plot reporting odds ratios for emotional neglect in different diagnostic subgroups, including schizophrenia spectrum disorder, major depressive disorder, personality disorder, bipolar disorder, obsessive-compulsive disorder, eating disorders, body dysmorphic disorder, and mood disorders. The table consists of multiple rows and columns, with each row representing a study and each column providing data on cases, controls, odds ratio, confidence interval, and weight. Notable trends include varying odds ratios across different disorders, with some showing higher odds ratios and others lower. The table highlights the heterogeneity within and between subgroups, providing insights into the relationship between emotional neglect and various mental health conditions.
Evaluation of moderators of the heterogeneity
The moderator effect of psychiatric diagnosis was confirmed by simple meta-regression for all types of neglect (F = 11.972, p < 0.001 for unspecified neglect; F = 10.204, p < 0.001 for physical neglect; F = 9.689, p < 0.001 for emotional neglect). bipolar disorder (b = 1.801, 95% CI 0.82–2.79, t = 4.072, p = 0.002), BPD (b = 2.275, 95% CI 0.64–3.91, t = 3.093, p = 0.011) and MDD (b = 1.427, 95% CI 0.69–2.17, t = 4.310, p = 0.002) were associated with significantly higher outcomes for unspecified neglect. Bipolar disorder (b = 1.030, 95% CI 0.37–1.69, t = 3.182, p = 0.003), eating disorders (b = 1.478, 95% CI 0.29–2.67, t = 2.516, p = 0.017), MDD (b = 1.196, 95% CI 0.78–1.61, t = 5.864, p < 0.001), personality disorders (b = 2.134, 95% CI 0.55–3.72, t = 2.737, p = 0.001) and schizophrenia spectrum disorders (b = 1.274, 95% CI 0.75–1.80, t = 4.917, p < 0.001) showed a significant positive association with physical neglect. Significant positive associations with emotional neglect were found for bipolar disorder (b = 1.293, 95% CI 0.55–2.04, t = 3.509, p = 0.001), eating disorders (b = 1.526, 95% CI 0.21–2.84, t = 2.354, p = 0.024), MDD (b = 1.299, 95% CI 0.85–1.75, t = 5.877, p < 0.001), personality disorders (b = 1.657, 95% CI 0.52–2.80, t = 2.942, p = 0.006) and schizophrenia spectrum disorders (b = 1.023, 95% CI 0.44–1.61, t = 3.562, p = 0.001).
Among other variables, the type of assessment tool used to assess neglect exposure (F = 5.974, p = 0.011 for unspecified neglect; F = 27.170, p < 0.001 for physical neglect; F = 29.061, p < 0.001 for emotional neglect), country of enrolment (F = 7.155, p = 0.009 for unspecified neglect; F = 4.598, p < 0.001 for physical neglect; F = 4.034, p < 0.001 for emotional neglect) and type of control group (F = 10.836, p = 0.001 for unspecified neglect; F = 22.352, p = 0.001 for physical neglect); F = 24.493, p < 0.001 for emotional neglect) were significant moderators for the three types of neglect.
Notably, regarding age, a correlation was found for physical neglect only (F = 3.148, p = 0.035): higher patient age was significantly linked to lower outcomes (b = −0.113, 95% CI −0.21 to −0.01, t = −2.297, p = 0.027), as was higher control age (b = −0.112, 95% CI −0.22 to −0.003, t = −2.070, p = 0.045), with a significant positive effect for the interaction between patient and control ages (b = 0.003, 95% CI 0.0004–0.005, t = 2.348, p = 0.024). No other significant moderations were identified for gender, year of publication or risk-of-bias assessment. Detailed regression analyses and corresponding plots are reported in the Supplementary Material.
To refine the interpretation of regression results, a multimodel inference approach based on corrected Akaike information criterion criteria was applied for each neglect subtype.
For unspecified neglect, the analysis indicated that country of enrolment and diagnostic category were the most influential predictors, both achieving the highest importance score (1.00). Neglect assessment tool and control group type also showed high importance (0.95 and 0.94, respectively). Although some interactions between predictors, such as country:diagnosis (0.70) and diagnosis:neglect tool (0.66), displayed moderate importance, none exceeded the importance threshold of 0.8 (26), suggesting that predictors largely exert independent effects.
For the other neglect subtypes, the most important predictors identified were patient age (0.47) and control group age (0.44) for physical neglect, and control type (0.37) and neglect assessment tool (0.23) for emotional neglect. All of these values fell well below the threshold, and no meaningful interactions were observed, indicating limited explanatory power for both subtypes. Details and corresponding plots are available in the Supplementary Material.
Risk of bias
Overall, the methodological quality of the included studies was moderate. Most studies were classified as having a moderate risk of bias (68.8%), whereas 18.8% showed high risk of bias and only 12.5% were rated as low risk. In general, studies demonstrated low risk of bias in key domains, including the use of standardised and reliable measures of neglect and consistent exposure assessment across cases and controls. However, common limitations were related to inadequate matching between cases and controls and insufficient identification or control of confounding factors. Detailed risk of bias assessments are provided in the Supplementary Material.
Discussion
The current meta-analysis comprehensively examined the association between unspecified neglect, emotional neglect and physical neglect and different psychiatric disorders, comparing affecting individuals with their respective control groups. To the best of our knowledge, this is the first meta-analysis specifically designed to investigate the association between neglect subtypes across distinct psychiatric disorders. The previous meta-analytic work conducted by Norman and colleagues Reference Norman, Byambaa, De, Butchart, Scott and Vos18 examined the impact of ACEs, including neglect, on mental health outcomes. However, their analysis treated neglect as a single undifferentiated category and did not provide an overall estimate for psychiatric disorders, Reference Norman, Byambaa, De, Butchart, Scott and Vos18 thus precluding a direct comparison with the present findings.
Data from 48 studies were included. The pooled odds ratios for the 3 subtypes of neglect exceeded 3, indicating a strong association with psychiatric disorders. These findings suggest that individuals exposed to neglect during childhood were over three times more likely to have a psychiatric disorder compared to those without such exposure, consistently across all neglect subtypes.
The analyses revealed consistently high heterogeneity across all three forms of childhood neglect, with I 2-values exceeding 80%. These substantial levels of heterogeneity reflect the methodological diversity among studies, including differences in sample demographics, diagnostic criteria and the tools used to assess neglect.
Substantial heterogeneity was observed across neglect subtypes, likely reflecting methodological variability in sampling, diagnostic procedures and assessment tools. However, sensitivity analyses and correction for potential publication bias did not materially alter the pooled estimates, supporting the robustness of the associations despite between-study differences.
The second level analysis for heterogeneity, conducted by meta-regression, highlighted another noteworthy finding regarding the relationship between participant age and physical neglect. Specifically, higher age in both patient and control groups were linked with a weaker association between physical neglect and psychiatric disorders. This trend of decreasing odds ratios with increasing age may be partly explained by recall bias. Over time, memories of specific events, particularly those involving physical neglect, such as inadequate access to food, clothing or medical care, may become less salient or more difficult to be accurately retrieved. Reference Simpson, Eskandaripour, Levine and Taler87 Moreover, the progressive fading of physical neglect memories over time aligns with research indicating that early-life neglect can impair memory processes. Studies have shown that physical neglect during childhood is associated with episodic memory deficits and a reduced ability to recall associative memories, particularly later in life. Reference Wang, Yang, Yu, Song, Zhao and Gao88 Additionally, neglect has been linked to alterations in autobiographical memory specificity, with evidence suggesting that neglected children exhibit a diminished capacity to recall detailed personal experiences. Reference Lawson, Valentino, Speidel, McDonnell and Cummings89
Both the recall bias and cognitive decline associated with ACEs could result in underreporting among older participants, potentially leading to the lower observed associations. However, the absence of a similar age effect for emotional neglect offers an interesting counterpoint. Unlike physical neglect, emotional neglect often involves relational disruptions that are less likely to fade from memory, potentially because of their persistent impact on identity and interpersonal functioning, explaining the lack of an age-related decline in the association between emotional neglect and psychiatric outcomes.
Cultural and generational differences in the perception of physical neglect may also explain the observed age trend. Older generations, having experienced widespread hardship, such as food scarcity or inadequate clothing, may have normalised these conditions rather than perceiving them as neglect. In contrast, younger individuals, raised with different societal expectations, may be more likely to recognise and report such experiences. Notably, one epidemiological study found that older age was a significant predictor of physical neglect, with the highest rates observed in individuals aged 70 years and older (46%). Reference Witt, Brown, Plener, Brähler and Fegert90 The authors attributed this finding to the unique sociohistorical circumstances of this generation that lived through World War Two. The lower representation of this older age group in more recent studies, attributable to demographic shifts, may explain why contemporary studies, including this meta-analysis, found a decline in physical neglect reporting with increasing participant age. Notably, this age-related pattern was consistent across both patient and control groups, suggesting that younger individuals may universally exhibit greater sensitivity to experiences of physical neglect. These findings underscore the importance of considering cultural and demographic context as moderating factors in studies of childhood neglect, emphasising the need to explore how generational shifts and memory processes influence the reporting and impact of neglect.
Subgroup analyses were conducted to identify differences between neglect subtypes among specific psychiatric diagnoses.
Subgroup analyses confirmed that the association between childhood neglect and psychiatric disorders was evident across multiple diagnostic categories, reinforcing its transdiagnostic relevance.
MDD exhibited the strongest and most stable associations across all neglect subtypes: the pooled odds ratios suggest that exposure to neglect increases the likelihood of developing MDD three to four times. These findings align with previous meta-analyses that consistently report strong associations between childhood neglect and depression. Reference Norman, Byambaa, De, Butchart, Scott and Vos18,Reference Mandelli, Petrelli and Serretti91,Reference Nelson, Klumparendt, Doebler and Ehring92 Although prior estimates were generally somewhat lower than those observed in the present analysis, the direction and overall magnitude of the association remain comparable, reinforcing the stability of the link between neglect and depression across studies. Importantly, recent literature emphasises that neglect, particularly emotional neglect, is more strongly associated with depression than other forms of childhood maltreatment. Reference Infurna, Reichl, Parzer, Schimmenti, Bifulco and Kaess17,Reference Humphreys, LeMoult, Wear, Piersiak, Lee and Gotlib93 This distinction suggests that the lack of care, emotional validation and consistent support during critical developmental periods may uniquely impair attachment, emotional regulation and resilience, all of which are key factors in the pathogenesis of MDD. Reference Nilsson, Nygaard, Ebsen and Østergård94–Reference Struck, Krug, Feldmann, Yuksel, Stein and Schmitt96
Bipolar disorder and schizophrenia spectrum disorders were also significantly associated with childhood neglect, with all three neglect subtypes showing elevated odds of psychiatric diagnosis compared with controls. The association between neglect and bipolar disorder is particularly noteworthy given the well-established genetic and neurobiological underpinnings of the disorder. Although the high odds ratio may initially seem unexpected, growing evidence indicates that childhood trauma, including neglect, significantly influences the clinical course of bipolar disorder, shaping its presentation and progression rather than serving as a primary aetiological factor. This has been documented by several studies highlighting the impact of ACEs on critical aspects of bipolar disorder. For instance, meta-analytic data revealed that patients with bipolar disorder and a history of childhood maltreatment (not limited to neglect) experience more severe manic, depressive and psychotic symptoms, along with higher rates of comorbid psychiatric conditions. Reference Agnew-Blais and Danese97 Maltreatment is also linked to earlier onset of bipolar disorder, a higher likelihood of rapid cycling and increased risk of suicide attempts. Reference Agnew-Blais and Danese97,Reference Duarte, Belzeaux, Etain, Greenway, Rancourt and Correa98 Moreover, given the strong heritability of bipolar disorder, it is plausible to speculate that the presence of the disorder in caregivers may contribute to difficulties in providing stable and consistent caregiving, potentially leading to neglectful environments. Reference Iacono, Beaulieu, Hodgins and Ellenbogen99 These challenges, associated with the emotional and functional impairments of bipolar disorder, could help explain the high incidence of neglect observed in individuals with this condition. Reference Carvalho Silva, Oliva, Barlati, Perusi, Meattini and Dashi21,Reference Zhang, Lin, Yang, Zhang, Pan and Lu100 These findings suggest that although neglect may not be considered an aetiological factor, it seems to act as a catalyst for more complex clinical presentations of bipolar disorder.
The association between neglect and schizophrenia spectrum disorders aligns with the meta-analysis conducted by Varese and colleagues, reinforcing the evidence that neglect is a significant environmental factor linked to schizophrenia and psychosis, with a dose–response relationship. Reference Varese, Smeets, Drukker, Lieverse, Lataster and Viechtbauer19,Reference Inyang, Gondal, Abah, Minnal Dhandapani, Manne and Khanna101 As observed in bipolar disorder, childhood neglect has been associated with worse clinical trajectories of schizophrenia spectrum disorders. Patients with a history of neglect often exhibit greater severity in both positive and negative symptoms, tend to be more resistant to treatment and are significantly affected in terms of functional outcomes. Reference Bailey, Alvarez-Jimenez, Garcia-Sanchez, Hulbert, Barlow and Bendall102–Reference Grindey and Bradshaw104 Notably, the stronger association with physical neglect found in this meta-analysis aligns with previous studies specifically linking physical neglect to more severe negative symptoms in schizophrenia spectrum disorders, including flattened affect, reduced social engagement and diminished motivation. Reference Bailey, Alvarez-Jimenez, Garcia-Sanchez, Hulbert, Barlow and Bendall102,Reference Chase, Melbourne, Rosen, McCarthy-Jones, Jones and Feiner105–Reference Popovic, Schmitt, Kaurani, Senner, Papiol and Malchow107 Furthermore, these studies highlight a strong correlation between physical neglect and functional and social impairments in adults with schizophrenia spectrum disorders, reinforcing its long-term impact on disability and overall quality of life.
Other psychiatric disorders also showed significant associations with childhood neglect, although estimates were less stable because of the limited number of studies and greater heterogeneity.
Eating disorders showed significant associations with both physical neglect and emotional neglect. Notably, this meta-analysis is the first to examine the link between childhood neglect and the eating disorders category as a whole. Previous studies have typically focused on specific eating disorders diagnoses or investigated the broader constructs of ACEs, without isolating neglect as a distinct exposure. Consequently, direct comparisons with the current findings are limited. Nevertheless, some parallels can be drawn with existing literature to contextualise these results. Coffino and colleagues found that food neglect was significantly associated with specific eating disorders, including anorexia nervosa and binge eating disorder, highlighting the relevance of food-related neglect as a distinct form of childhood adversity. Reference Coffino, Grilo and Udo108 Similarly, Quilliot and colleagues identified emotional neglect as a key predictor of binge eating disorder, Reference Quilliot, Brunaud, Mathieu, Quenot, Sirveaux and Kahn109 and Caslini and colleagues reported a significant association between child maltreatment and eating disorders. Reference Caslini, Bartoli, Crocamo, Dakanalis, Clerici and Carrà110 These findings, along with the high prevalence of childhood neglect in eating disorders populations, reinforce the strong connection between early adversity and disordered eating behaviours. Reference Pignatelli, Wampers, Loriedo, Biondi and Vanderlinden20,Reference Carvalho Silva, Oliva, Barlati, Perusi, Meattini and Dashi21
Personality disorders demonstrated exceptionally strong associations with both physical neglect and emotional neglect. It is essential to note the wide-ranging effect sizes observed in this analysis, which result not only from heterogeneity in the included data, but also from the inherent complexity of the personality disorders category itself. When compared with previous findings, this meta-analysis presents notably higher effect sizes for the association between neglect and personality disorders. Previous population-based and clinical studies have reported more modest but consistent associations for physical neglect and emotional neglect across personality disorders clusters, Reference Afifi, Mather, Boman, Fleisher, Enns, MacMillan and Sareen111,Reference Johnson, Smailes, Cohen, Brown and Bernstein112 with evidence suggesting that different neglect subtypes may relate to distinct personality phenotypes. Reference Johnson, Smailes, Cohen, Brown and Bernstein112
The relationships between childhood neglect and OCD, body dysmorphic disorder and PTSD were investigated based on single studies, precluding meta-analytic synthesis. Although these findings provide initial insights, the reliance on single studies underscores the need for further research to validate and expand these associations.
Notably, for PTSD, the exceptionally high odds ratio observed for physical neglect suggests a particularly strong link, although the limited availability of comparative studies complicates interpretation. However, McLaughlin and colleagues reported a lower but significant association, reinforcing neglect as a risk factor for PTSD development following a traumatic event. Reference McLaughlin, Koenen, Bromet, Karam, Liu and Petukhova113 Further supporting these findings, a more recent study identified emotional neglect as a significant contributor to the development of complex PTSD. Reference Leiva-Bianchi, Nvo-Fernandez, Villacura-Herrera, Miño-Reyes and Parra Varela114 Although this finding should be interpreted with caution, support from previous studies allows speculation on the role of childhood neglect in shaping severe and chronic trauma responses, often resulting in disorders characterised by high multimorbidity and significant functional impairment.
The findings of this meta-analysis must be interpreted in light of several methodological challenges, primarily concerning the studies included.
A key issue is the high heterogeneity observed across studies, partly attributable to moderate to high risk of bias in a substantial portion of the included works. The risk-of-bias analysis highlights the general lack of high-quality evidence in this field, with significant concerns in specific areas. Notably, many studies failed to adequately match cases and controls on relevant criteria or control for relevant confounders, potentially contributing to variability in effect estimates. Another important consideration in interpreting these findings is the potential influence of recall and reporting bias, exacerbated by the limitations of self-report measures used to assess childhood neglect. Reference Hardt and Rutter14,Reference Reuben, Moffitt, Caspi, Belsky, Harrington and Schroeder15 Unlike more overt forms of maltreatment, such as physical or sexual abuse, neglect often lacks discrete, easily recalled events, making it more challenging to identify and report accurately. This limitation is particularly pronounced in psychiatric populations, where cognitive, emotional, and social functioning may further influence responses, amplifying these biases. Indeed, many of the included studies did not adequately address the real-world clinical characteristics of psychiatric disorders. In bipolar disorder, distinctions between euthymic and symptomatic states at the time of assessment, as well as differences between bipolar disorder type 1 and type 2, were often overlooked. Similarly, in schizophrenia spectrum disorders, several studies did not distinguish between the different disorders within the schizophrenia spectrum or consider whether patients had positive or negative symptoms at the time of data collection. These methodological gaps not only contributed to the substantial heterogeneity observed across studies, but may have also introduced variability in the estimates of neglect prevalence in these populations, warranting caution in interpreting the results.
A major challenge in studying childhood neglect is its accurate measurement using standardised and validated assessment tools, particularly in psychiatric populations. Although the meta-regression identified assessment tool as a significant moderator of the outcome, many of the instruments used in the included studies are either rarely used or not specifically validated for use in psychiatric populations, raising concerns about the consistency and accuracy of neglect measurement in this context. Beyond exposure assessment, the characterisation of control groups also emerged as a relevant methodological factor. Studies using non-clinically assessed controls showed larger odds ratios than those employing clinically assessed controls screened with standardised diagnostic tools, possibly reflecting less reliable classification of psychiatric status when based on self-report and a consequent inflation of effect estimates. Future research would benefit from prospective longitudinal designs assessing neglect exposure in childhood and following individuals over time, thereby reducing reliance on retrospective recall. In addition, the use of multi-informant approaches, integration with administrative or child protection records and the adoption of standardised clinical interviews for both exposure assessment and control group characterisation may enhance the reliability and validity of findings. Such methodological improvements are essential to improve study comparability and to clarify the temporal and potentially causal relationships between childhood neglect and psychiatric disorders. Finally, prevalence estimates of neglect in the general population remain highly variable, influenced by regional and socioeconomic differences. Reference Stoltenborgh, Bakermans-Kranenburg and van IJzendoorn6,Reference Moody, Cannings-John, Hood, Kemp and Robling9 This variability complicates comparisons between psychiatric and non-clinical populations and challenges the estimation of the true magnitude of neglect’s association with psychiatric disorders.
A key strength of this meta-analysis is its focus on studies with controlled designs, including healthy control groups. This methodological approach allowed for a more precise comparison of neglect prevalence between psychiatric and non-clinical populations, providing a clearer estimate of its association with psychiatric conditions.
Nevertheless, the findings of this study should be interpreted in light of the inherent limitations of meta-analyses. First, heterogeneity was high in most analyses, reflecting substantial variability both within and between clinical diagnostic categories. Although sensitivity analyses, subgroup analyses and meta-regressions were conducted to address this variability, other potential effect modifiers – not examined in the current study – may have contributed to the observed heterogeneity. Second, treating psychiatric diagnoses as discrete categories may have oversimplified real-world clinical presentations, limiting the ability to fully capture their complexity. Furthermore, for some disorders, neglect prevalence was based on a limited number of studies, restricting the accuracy and generalisability of the findings. For OCD, PTSD and body dysmorphic disorder, only a single study was available for analysis, whereas other diagnostic categories, such as anxiety disorders or substance use disorders, were entirely absent.
Despite these limitations, the consistency and magnitude of the associations observed across diagnostic categories carry important clinical implications. The findings suggest that childhood neglect should not be considered a peripheral background variable, but rather, a clinically meaningful vulnerability factor across a broad range of psychiatric conditions. Routine and structured assessment of neglect exposure in psychiatric evaluations may enhance case formulation, improve risk stratification and support trauma-informed treatment planning.
At a broader level, the transdiagnostic relevance of neglect underscores the importance of early identification and preventive strategies. Strengthening family support systems, parental mental health services and child protection interventions may represent critical public health priorities aimed at reducing long-term psychiatric burden and disability.
In conclusion, the results of this meta-analysis confirm a significant and consistent association between childhood neglect and the development of major psychiatric disorders. Notably, for disorders with the most comprehensive data, including MDD, bipolar disorder, schizophrenia spectrum disorders, eating disorders and personality disorders, odds ratios exceeded 2, indicating a stronger likelihood of these conditions among individuals exposed to childhood neglect. Moreover, different forms of neglect may be differentially associated with specific psychiatric trajectories, influencing symptom severity, onset patterns and comorbidities. These findings reaffirm neglect as a critical environmental factor associated with psychiatric pathology.
Although odds ratios quantify the strength of association, they do not establish causation. Childhood neglect should be understood within a multifactorial framework of psychiatric illness, in which genetic vulnerability, neurodevelopmental processes and environmental influences interact over time. Neglect is neither a necessary nor sufficient condition for psychiatric disorders. Many individuals exposed to neglect do not develop mental illness and, conversely, such disorders occur in individuals without a history of neglect. Emerging evidence suggests that early neglect may contribute to psychiatric vulnerability through mechanisms such as stress system dysregulation, neurodevelopmental alterations in fronto-limbic circuits and epigenetic modifications. Reference Jackson, Frederico, Cleak and Perry13,Reference Norman, Byambaa, De, Butchart, Scott and Vos18,Reference Teicher and Samson115,Reference Nemeroff116 Beyond psychiatric outcomes, childhood neglect has also been associated with broader health consequences, including increased risk of metabolic, cardiovascular and neuroendocrine dysregulation, Reference Jackson, Frederico, Cleak and Perry13,Reference Norman, Byambaa, De, Butchart, Scott and Vos18 underscoring its systemic and long-term impact on health.
Overall, recognising childhood neglect as a transdiagnostic risk factor has important implications for research, clinical assessment and public health strategies aimed at reducing long-term psychiatric burden and associated medical comorbidity.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10693
Data availability
The data, analytic code and materials that support the findings of this study are available from the corresponding author, S.C., upon reasonable request.
Acknowledgements
The authors thank Dr Chiara Lops of Clinical Psychology Unit, Città della Salute e della Scienza di Torino, Turin, Italy, for providing support in the study selection and data extraction phases.
Author contributions
M. Merola contributed to the investigation and writing the original draft of the manuscript. S.C., S.B. and A.M. contributed to study conceptualisation and supervision, and reviewing and editing the manuscript. R.C.S., G.P., M. Merola, M. Meattini and V.M. contributed to the investigation and data curation. N.C. contributed to the study methodology. L.O. and B.L.A. contributed to study supervision and reviewing and editing the manuscript. F.O. contributed to the study methodology, formal analysis, supervision and writing the original draft of the manuscript.
Funding
The assistant researcher position of G.P. is funded by the European Rresearch Area on Personalised Medicine (ERA-PerMed) Toward PrecisiOn Medicine for the Prediction of Treatment (PROMPT) project (Italian Ministry of Health grant number ERP-2020-23671059). The postdoctoral student position of V.M. was partly funded by the Piano Nazionale di Ripresa e Resilienza (PNRR) (grant number DM 117/2023). A.M. is supported by the Italian Ministry of Health under grant Ricerca Corrente 2025 (RC-2025). None of these funding sources contributed directly to the design, execution or publication of the present study.
Declaration of interest
None.







 Open access
Open access
eLetters
No eLetters have been published for this article.